Analysis of Health-Related Quality-of-Life Instruments Measuring the Impact of Bariatric Surgery
14
Analysis of Health-Related Quality-of-Life Instruments Measuring the Impact of Bariatric Surgery Systematic Review of the Instruments Used and their Content Validity Raed Tayyem, 1 Abdulmajid Ali, 1 John Atkinson 2 and Colin R. Martin 3 1 General Surgery Department, The Ayr Hospital, Ayr, UK 2 University of the West of Scotland, Paisley Campus, Paisley, UK 3 University of the West of Scotland, Ayr Campus, Ayr, UK Contents Abstract .................................................................................. 73 1. Overview of Obesity and Health-Related Quality of Life (HR-QOL).............................. 74 2. Literature Review ....................................................................... 75 2.1 Methods .......................................................................... 75 2.2 Potential Sources of Bias ............................................................. 76 2.3 Search Results ..................................................................... 76 3. Content Validity ........................................................................ 77 4. Generic vs Obesity-Specific HR-QOL ....................................................... 77 5. Discussion ............................................................................. 78 6. Conclusion ............................................................................ 82 Abstract The worldwide prevalence of obesity has been steadily rising, reaching alarming levels. Obesity, particularly morbid obesity, carries significant health risks to the lives of affected patients, including physical, psychological, and social co-morbidities. Bariatric surgery provides the only effective and sustainable approach to treat morbid obesity and reverse its adverse effects. The reduction in well-being due to poor health in obesity may have adverse effects on health-related quality of life (HR-QOL). There are numerous studies reporting HR-QOL in bariatric patients; however, there is a paucity of studies examining the psychometric properties of the HR-QOL instruments used. The main aim of this review is to identify the instruments used in assessing HR-QOL in bariatric patients and evaluate their content validity. We believe that this is the first systematic review of its kind to look in depth at various generic- and obesity-specific HR-QOL instruments that were used in bariatric surgery, and to analyze their content validity. A systematic and structured search of Ovid databases (1980–2009) was conducted using terms synonymous with bariatric surgery, combined with terms synonymous with HR-QOL instruments. A total of 112 relevant studies REVIEW ARTICLE Patient 2011; 4 (2): 73-87 1178-1653/11/0002-0073/$49.95/0 ª 2011 Adis Data Information BV. All rights reserved.
-
Upload
john-atkinson -
Category
Documents
-
view
212 -
download
0
Transcript of Analysis of Health-Related Quality-of-Life Instruments Measuring the Impact of Bariatric Surgery

Analysis of Health-Related Quality-of-LifeInstruments Measuring the Impact ofBariatric SurgerySystematic Review of the Instruments Used and their ContentValidity
Raed Tayyem,1 Abdulmajid Ali,1 John Atkinson2 and Colin R. Martin3
1 General Surgery Department, The Ayr Hospital, Ayr, UK
2 University of the West of Scotland, Paisley Campus, Paisley, UK
3 University of the West of Scotland, Ayr Campus, Ayr, UK
Contents
Abstract. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 731. Overview of Obesity and Health-Related Quality of Life (HR-QOL). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 742. Literature Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75
2.1 Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 752.2 Potential Sources of Bias . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 762.3 Search Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 76
3. Content Validity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 774. Generic vs Obesity-Specific HR-QOL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 775. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 786. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 82
Abstract The worldwide prevalence of obesity has been steadily rising, reachingalarming levels. Obesity, particularly morbid obesity, carries significanthealth risks to the lives of affected patients, including physical, psychological,and social co-morbidities. Bariatric surgery provides the only effective andsustainable approach to treat morbid obesity and reverse its adverse effects.
The reduction in well-being due to poor health in obesity may have adverseeffects on health-related quality of life (HR-QOL). There are numerous studiesreportingHR-QOL in bariatric patients; however, there is a paucity of studiesexamining the psychometric properties of the HR-QOL instruments used.The main aim of this review is to identify the instruments used in assessingHR-QOL in bariatric patients and evaluate their content validity. We believethat this is the first systematic review of its kind to look in depth at variousgeneric- and obesity-specific HR-QOL instruments that were used in bariatricsurgery, and to analyze their content validity.
A systematic and structured search of Ovid databases (1980–2009) wasconducted using terms synonymous with bariatric surgery, combined withterms synonymous withHR-QOL instruments. A total of 112 relevant studies
REVIEWARTICLEPatient 2011; 4 (2): 73-87
1178-1653/11/0002-0073/$49.95/0
ª 2011 Adis Data Information BV. All rights reserved.

were identified, detailing the use of eight generic, nine obesity-specific, andnumerous other condition-specific instruments.
A conceptual framework comprising 20 domains pertinent to bariatricsurgery and morbid obesity was proposed, against which the identifiedgeneric- and obesity-specific instruments were assessed. The results of thisassessment showed that neither the generic nor the specific instruments wereadequate instruments in terms of content validity.
Given the lack of adequate HR-QOL instruments in the rapidly developingfield of bariatric surgery, we suggest building a new bariatric-specific instru-ment informed by the proposed framework, which will then enable clinicians toassess the full impact of morbid obesity and bariatric surgery on HR-QOL.
1. Overview of Obesity andHealth-Related Quality of Life (HR-QOL)
Although there is no universally accepted defi-nition[1,2] or measurement[2] of quality of life (QOL),it is basically agreed that QOL is concerned with thefunctioning and well-being of the physical, mental,and social aspects of one’s life.[3,4]
QOL is multidimensional, and could be sub-divided into health-related (HR-QOL) and non-health- or environment-based domains. The aspectsof life measured by HR-QOL have the potentialto improve with treatment. On the other hand,the aspects of non-health QOL that can adverselyaffect health are unlikely to improve with ap-propriate medical care.[5]
Obesity is a chronic, complex, multifactorialcondition[6-8] associated with a body mass index(BMI) ‡30 kg/m2[9] and results in increased mor-bidity[10-12] and mortality.[13,14] Morbid obesitycharacterized by a BMI ‡40 kg/m2[15] will furtherincrease health risks,[16-18] including detrimentaleffects on HR-QOL.[19-21]
In the US, two-thirds of adults are overweight,one-third of adults are obese,[9] and approximately5% of the population are morbidly obese.[10] Obe-sity and associated medical conditions cost thehealth system in the US a staggering $US100billion per year,[15] which is roughly equal to 10%of overall medical expenditure.[22] The socioecono-mic impact of the obesity epidemic is similar tothat of poverty, smoking, or alcohol abuse.[23]
The prevalence of obesity is expected to doubleevery 5–10 years.[20] The UK has the fastest in-crease in obesity in Europe, which costs the UK
economy d7 billion and the NHS d2 billion peryear (estimated costs for the year 2006–7).[24]
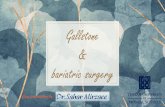
Obesity potentially carries detrimental effectson HR-QOL in three main aspects, includingphysical, psychological, and social aspects, as il-lustrated in a proposed graphical model of themechanism relatingHR-QOL and obesity (figure 1).Behavioral modification interventions and phar-macotherapy result in weight loss of 4–8%,[25,26]
which is not sustainable for more than a year,[27,28]
and will relapse and fail in 90% of patients within5 years.[29] Bariatric surgery, on the other hand,achieves significant and sustainable weight re-duction,[30,31] with resolution of obesity-relatedco-morbidities and reduction in mortality.[32-34]
Bariatric surgery – whether restrictive, malab-sorptive, or restrictive-malabsorptive – can be per-formed laparoscopically, safely, and effectively.[35,36]
Bariatric surgery has the potential to improvethe HR-QOL of obese patients. Results of studiesin which patients’ experiences and perspectiveshave been evaluated will help clinicians to betterunderstand what outcomes of bariatric surgeryare important to the patient. Consequently, re-sources can be directed towards treatments mostvalued by patients.[37] Surgeons usually makeimplicit subjective judgment of their patients’HR-QOL when performing bariatric procedures;however, few of them will use explicit HR-QOL in-struments.[38] In addition, where patient-recordedoutcomes such as HR-QOL have been measured assecondary endpoints of clinical trials, the results ofthese instruments have rarely been translated intoformal clinical assessment,[39] and they have rarelymodified the overall interpretation of the trial.[40]
74 Tayyem et al.
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

Like any other psychometric instrument, anHR-QOL instrument should produce meaning-ful data with satisfactory psychometric proper-ties, including validity, reliability, specificity,sensitivity, and responsiveness to change. Con-tent validity is the extent to which items in aninstrument assess relevant aspects of the targetedconcepts.[37]
Few papers have tried to analyze the con-tent validity of obesity-specific HR-QOL in-struments.[41-43] The purpose of this systematicreview is to identify instruments used to assessHR-QOL in bariatric surgery and morbid obe-sity, which is a special subset of obesity, and toanalyze and explore their suitability with refer-ence to the proposed framework. As far as weknow, this is the first attempt at a systematicreview of the literature to analyze HR-QOL in-struments used in bariatric surgery and assesstheir content validity.
2. Literature Review
2.1 Methods
A comprehensive electronic search was per-formed of Ovid databases (Ovid MEDLINE,
EMBASE, PsycINFO, EBM Reviews: CochraneDatabase of Systematic Reviews – CDSR, andEBM Reviews: Cochrane Central Register ofControlled Trials – CCTR) for all relevant clin-ical studies including controlled trials writtenin the English language, reporting HR-QOL asone of the primary or secondary endpoints, andpublished between 1980 and October 2009. Acomprehensive description of the search meth-odology listing all search terms and inclusion andexclusion criteria is outlined in table I.1. An electronic search was conducted to includeall relevant studies by applying the followingterms in the citation, abstract and title fields:(i) terms synonymous with ‘bariatric surgery’;and (ii) terms synonymous with ‘HR-QOL’; and(iii) terms synonymous with ‘instrument’.2. Application of the inclusion parameters onthe database search result.3. Application of the exclusion parameters onthe database search result.4. Manual abstract screening.
Data extraction included the type of HR-QOLinstrument used and the number of different in-struments used (if more than one instrument wasused). Full articles were retrieved if their abstractswere not clear regarding the required data. Full
Obesity
Chronic inflammatory statePsychological
factorsSocialfactors
Behavioralfactors
Physical factors
Gut hormone modulation
Calcium and vitamin D
Socialco-morbidities
Physicalco-morbidities
Psychologicalco-morbidities
PoorHR-QOL
Fig. 1. Graphic model illustrating a proposed relationship between obesity and physical, psychological, and social co-morbidities. Thedemonstrated vicious cycle clearly carries detrimental effects on health-related quality of life (HR-QOL). The various factors contributing to thedevelopment of obesity are also shown in this model.
HR-QOL Instruments in Bariatric Surgery 75
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

articles of six abstracts were unavailable at the timeof writing.[44-49] Abstract screening and data ex-traction was carried out by a single reviewer (RT).
An experienced bariatric team (two bariatricsurgeons, a clinical psychologist, a bariatric spe-cialist nurse, and a bariatric dietician) in collab-oration with two university professors with interestin the subject created a preliminary conceptualframework relying on patients’ experiences andcriteria. The domains of the instruments identi-fied during the review were recorded. This helpedfurther refine and finalize the preliminary frame-work, as shown in figure 2.
2.2 Potential Sources of Bias
The methodology of this review followed astructured and comprehensive approach; however,one possible source of error could be publicationbias where studies with negative results are notpublished. Another source of bias is that a smallnumber of the full articles were not available.
2.3 Search Results
The search strategy was conducted in a system-atic and structured way to include all the relevantarticles. A total of 613 citations were obtained in
Table I. Search methodology showing the terms, inclusion criteria, and exclusion criteria used in the database search
Terms synonymous with bariatric
surgery
‘Bariatric surgery’ or ‘bariatric procedure’ or ‘bariatric operation’ or ‘bariatric’ or ‘obesity surgery’
or ‘gastric bypass’ or ‘gastroplasty’ or ‘sleeve gastrectomy’ or ‘gastric sleeve’ or ‘gastric band’ or
‘lap-band’ or ‘gastric balloon’ or ‘duodenal switch’ or ‘bilio-pancreatic diversion’
Terms synonymous with health-related
quality of life
‘Quality of life’ or ‘qol’ or ‘health related quality of life’ or ‘health-related quality of life’ or ‘hqol’ or
‘hrqol’ or ‘hrql’ or ‘health status’ or ‘well-being’ or ‘functional status’
Terms synonymous with instrument ‘Instrument*’ or ‘measure*’ or ‘question*’ or ‘tool*’ or ‘scale*’ where (*) denoted truncated term
Inclusion parameters Clinical trials, controlled clinical trials, or randomized controlled trials, year 1980–2009, and
‘morbid obesity’ or ‘morbidly obese’
Exclusion parameters Non-English publication and animal studies
Physicalaspects
Psychologicalaspects
Social aspects
Maritallife
Physicalactivity
Energyand
vitalityOther
symptoms
Familyrelationships
Work andemployment
Eatingactivity
Pain
Environmentand
accommodation
Friendship
Finance
Moodand
emotion
Sleep
Sexualactivity
Appearance
Mentalstatus
MobilityPhysicalhealth
Social activities andsocial relationships
HR-QOL
Self-esteem andself-respect
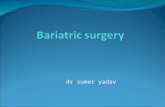
Fig. 2. Proposed conceptual framework demonstrating the potential domains of health-related quality of life (HR-QOL) that might be ad-versely affected by obesity.
76 Tayyem et al.
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

the first stage, 271 of which met the inclusioncriteria by the end of the second stage. It was sur-prising that, to date, less than 4% of all the publishedliterature regarding bariatric surgery for morbidobesity (7148 citations) included one or more in-struments to assess HR-QOL (271 citations).
During the third stage, 145 studies were ex-cluded and 126 abstracts were retrieved for fur-ther assessment. By the end of manual abstractscreening in the fourth stage, 14 studies were ex-cluded, leaving 112 studies for the review (figure 3).The majority of studies included in the review wererandomized controlled trials, non-randomized con-trolled clinical trials, and uncontrolled clinical trials.
Data extraction in the fifth stage revealed thatthe instrument type was not explicitly mentioned in22 studies, leaving 90 studies for the analysis. A totalof 42 differentHR-QOL instrumentswere identifiedin this systematic review, which were categorizedinto three groups: eight generic, nine obesity-specific,and 25 other condition-specific instruments.
Most of the studies used a single instrument tomeasureHR-QOL (70%), whereas 30% of the stud-ies used more than one instrument. Table II showsthat the most commonly used instrument categoryis other condition-specific instruments (36%), fol-lowed by obesity-specific instruments (34%). Thegeneric instruments were least used (30%).
Overall, the most commonly used instrumentswere theMAQOL (Moorehead-Ardelt Quality of
Life instrument; 21%), followed by the SF-36 (36-Item Short-Form Health Survey; 20%), GI-QLI(Gastrointestinal Quality of Life Index; 9%),Euroqol EQ-5D (5-Item European Quality ofLife; 5%), and IWQOL-Lite (Impact of Weighton Quality of Life-Lite version; 4%).
3. Content Validity
The provisional framework was thoroughlyre-edited during the literature search, resulting in20 potential domains of HR-QOL that might beadversely affected by obesity and improved bybariatric surgery. The identified domains weredistributed almost equally among the three mainaspects of the framework, with six domains in thephysical aspect, seven domains in the psychologicalaspect, and seven domains in the social aspect, asillustrated in the proposed conceptual framework(figure 2). This framework was used in analyzingthe content validity of the identified instruments.
Generic and obesity-specific instruments iden-tified in this review were compared against thedomains in the proposed conceptual framework.Table III compares the content validity of theHR-QOL instruments commonly used in bari-atric surgery against the domains in the proposedframework. Three generic instruments are notincluded because they are rather historical andnot in current use, and two obesity-specific in-struments are not included because they have notbeen used in clinical practice following their de-velopment and validation. Table III clearly showsthat the commonly used instruments are far fromperfect, because they are lacking important do-mains as informed by the proposed framework.
4. Generic vs Obesity-Specific HR-QOL
A condition-specific HR-QOL instrument ispreferable to a generic instrument when consid-ering a specific condition or disease, because acondition-specific instrument will provide a mea-surement that displays greater content validity,and a better attribution factor. The concept of theattribution factor can be explained by the fol-lowing example. When using generic instruments,obese patients will rate their health, sleep, social
Potentially relevant studies(n = 613)
Met inclusion criteria(n = 271)
Abstract reviewed for manualscreening (n = 126)
Irrelevant studies(n = 14)
Met exclusion criteria(n = 145)
Did not meet inclusioncriteria (n = 342)
Total number of studies includedin the systematic review
(n = 112)
Fig. 3. Flow diagram of the search results after the application ofthe search methodology.
HR-QOL Instruments in Bariatric Surgery 77
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

activity, etc. without direct reference to their obe-sity, leaving their rating susceptible to externalinfluence from other conditions or factors. Con-versely, with obesity-specific instruments, onlythe impact of obesity on the various aspects of thepatients’ lives will be rated.[37]
Despite increased recognition of the advan-tages of condition-specific instruments and thelimitations of generic instruments, relatively fewobesity-specific instruments have been developedand are ready for use. Moreover, the use ofobesity-specific HR-QOL instruments in bariatricsurgery has still not become common practice asevident by the literature search, which showedthat <4% of all the published literature regarding
bariatric surgery for morbid obesity included oneor more instruments to assess the HR-QOL.
Table IV provides an annotated description ofHR-QOL instruments commonly used in bari-atric surgery.
5. Discussion
QOL is subjective, dynamic, and multidimen-sional. The multidimensional character can bedivided into health-related and non-health-relateddomains, as discussed in the introductory section.The subjectivity of QOL arises from the fact thatindividuals rate their own QOL from their uniqueperspective based on their own feelings, experi-
Table II. Types of health-related quality-of-life instruments and how often they were used in bariatric surgery
Instrument category Times used
Generic
36-Item Short-Form Health Survey (SF-36)[50-77] 28
5-Item European Quality of Life (EuroQoL EQ-5D)[54,56,68,78-81] 7
Miscellaneousa 7
Subtotal 42
Obesity-specific
Moorehead-Ardelt Quality of Life instrument (MAQOL)[51,52,56,57,64,65,79,82-103] 29
Impact of Weight on Quality of Life-Lite version (IWQOL-Lite)[67-70,104,105] 6
Swedish Obese Subjects Obesity Psychosocial Problem (SOS-OP) module[43,106,107] 3
Miscellaneousb 9
Subtotal 47
Other condition-specific
Gastrointestinal Quality of Life Index (GI-QLI)[51,64,108-117] 12
Visual Analog Scale (VAS)[53,118-121] 5
Symptom Check List – 90 Revised (SCC-90R)[92,122-124] 4
Miscellaneousc 30
Subtotal 51
Total 140
a Miscellaneous includes Nottingham Health Profile (NHP),[120,121] World Health Organization Quality Of Life (WHOQOL-BREF),[125]
Manchester Short Assessment of Quality of Life (MANSA),[126] Lancashire Quality of Life Profile,[122] Goldberg General Health
Questionnaire (GHQ-12),[79] and Gothenburg Quality of Life Scale.[127]
b Miscellaneous includes Obesity Specific Quality of Life (OSQOL) instrument,[43,128] Health Related Quality of Life (HRQL),[129,130] Obesity
and Weight-Loss Quality-of-Life (OWLQOL) instrument,[43,131] Obesity Adjustment Survey Short Form (OAS-SF),[132] Obesity Related
Well-Being Scale (ORWELL 97) questionnaire,[133] and Bariatric Quality of Life Index (BQL).[51]
c Miscellaneous includes Psychosocial Stress and SymptomQuestionnaire (PSS-Q),[134,135] Incontinence Impact Questionnaire (IIQ-7),[136,137]
Urogenital Distress Inventory (UDI),[136,137] Kobashi Prolapse Symptom Inventory Quality of Life (PSI-QOL),[137] Oswestry Disability Index
(ODI),[53,118] Gastroesophageal RefluxDiseaseQuality of Life (GERD-QOL),[138,139] Beck Depression Inventory (BDI),[140,141] Cleveland Clinic
Foundation Fecal Incontinence Scale (CCF-FI),[142] Eating Disorder Inventory (EI),[143] Binge Eating Scale,[144] Eating Behavior Self-Efficacy
Scale Questionnaire,[145] Eating Disorder Examination questionnaire,[146] Stunkard and Messick Eating Inventory,[83] Three-Factor Eating
Questionnaire (TFEQ),[144,147] Questionnaire of Eating and Weight Patterns (QEWP),[147,148] Rosenberg Self-Esteem Scale (RSE),[149]
Roland Morris Disability Questionnaire,[118] Waddell Disability Index,[118] Apgar Family Function Questionnaire,[146] Hospital Anxiety
Depression Scale (HAD),[76] Pelvic Floor Disorder Questionnaire,[150] and International Consultation on Incontinence Questionnaire.[151]
78 Tayyem et al.
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

Table IV. Annotated description of health-related quality-of-life (HR-QOL) instruments commonly used in bariatric surgery
Instrument name Description
Moorehead-Ardelt Quality of Life instrument (MAQOL) Bariatric Analysis and Reporting Outcome System (BAROS) evaluates the
results of bariatric surgery by analyzing three domains: weight loss, changes
in co-morbidities, and HR-QOL.[82] The system has been used in many
countries since its introduction in the late 1990s.[83] The QOL instrument
used in BAROS is the validated[160] MAQOL instrument, which is a simple
quick six-item questionnaire[50]
Impact of Weight on Quality of Life (IWQOL) Has 74 items developed by Duke University to measure eight domains:
health, social interpersonal interaction, work, mobility, self-esteem, sexual
life, daily living activities, and comfort with food.[129,156] There are some
concerns regarding its reliability and validity.[22] The IWQOL has been
reduced to a 31-item psychometrically sound and clinically sensitive
instrument (IWQOL-Lite)[104]
Swedish Obese Subjects Obesity Psychosocial Problem
(SOS-OP) module
A special module composed of eight items and developed for use in the SOS
study.[130] The covered domains include physical activity, social activity,
appearance, and sexual functioning[159]
Obesity Specific Quality of Life (OSQOL) A validated 11-item instrument covering four domains: physical state, vitality
and desire to do things, relations with other people, and psychological
state[128,129]
Health Related Quality of Life (HRQL) A validated 55-item instrument looking at five domains: general well-being,
health distress and depression, self-esteem with three major levels of
functioning (self-regard, physical appearance, and work productivity),
physical activity, and social activities.[129,130] Unfortunately, this lengthy time-
consuming instrument is unreliable when administered serially in patients
with stable weights[22]
Obesity and Weight-Loss Quality-of-Life (OWLQOL)
instrument and Weight-Related Symptom Measure (WRSM)
Has two parts: part one records the patient’s feelings about their weight,
including 17 items, and part two records 20 items about weight-related
symptoms and how much they bother the patient.[131,157,158] Both have been
shown to display good internal consistency, test-retest reliability, and
convergent validity[129]
Obesity Adjustment Survey An instrument with a huge collection of 95 items from the Mental Health
Inventory, the Sickness Impact Profile, and the Eating Inventory, which was
condensed into a shorter 20-item survey[22,132]
Obesity Adjustment Survey Short Form (OAS-SF) A sensitive and valid measure of obesity, although it is limited as it only
measures the psychological distress aspect of HR-QOL[22,129,132]
Bariatric Quality of Life Index (BQL) A 30-item measure of well-being in bariatric surgery patients, which is a
validated instrument ready for clinical use[51]
Obesity Related Well-Being Scale (ORWELL 97)
questionnaire
A simple, valid,[129] and reliable measure of obesity HR-QOL that can be
used in current clinical practice. It consists of measuring two subscales:
ORWELL 97-1, which is related to psychological status and social
adjustment, and ORWELL 97-2, which is related to physical symptoms and
impairment[133]
36-Item Short-Form Health Survey (SF-36) One of the most commonly used generic HR-QOL instruments, which has
been used in thousands of studies.[22] It is used in health economics as a
variable in the QALY calculation to determine the cost effectiveness of a
health treatment. A shorter validated version, the SF-12, composed of 12
items, is also available for use. The SF-36 instrument has been throughmany
years of development and refinement, producing well validated and reliable
results. The SF-36 is a multipurpose health survey, which consists of 36
validated items distributed among eight scaled domains:[152] vitality, physical
functioning, bodily pain, general health perceptions, physical role functioning,
emotional role functioning, social role functioning, and mental health
Continued next page
80 Tayyem et al.
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

ences, and priorities. Individuals’ assessment oftheir own QOL will change over time, dependingon their priorities, experiences, and circumstancesat a given time, which explains the dynamic prop-erty of QOL.[37] The concept of subjectivity anddynamicity of QOL may explain why patients’ andclinicians’ ratings of the same objective situationhave been found to differ significantly, with therating rarely well matched.[161]
To maintain adherence to treatment and to de-velop new treatments that may be more acceptableto patients, it is crucial to understand howconditionsand interventions can affect QOL in a way pertinentto patients. An HR-QOL instrument can be usedto generate quality-adjusted life-years (QALYs),which would be utilized in estimating the costeffectiveness of the treatment.HR-QOLassessmentcan also aid in the process of decision making whencomparing different treatment options.[3]
In bariatric surgery, objective measurement ofweight loss has been the standard common prac-tice; however, subjective assessment of HR-QOLhas been less standardized. Several generic andobesity-specific HR-QOL instruments have beendeveloped and used in bariatric surgery. Al-though some of their psychometric properties
have been satisfactory, their content validity asshown in this review has not. Content validity is afundamental concept of an instrument’s validity,as there is no point saying that an instrument hasexcellent reliability, sensitivity, and responsive-ness if it does not measure what it is supposed tomeasure, i.e. the target concept or domain.
During this study, a conceptual frameworkwith 20 domains was constructed. This frameworkcould provide better insight into the problems ofobesity, and equally importantly, a window to ex-plore the patient experience after the operation –whether that experience be good, as anticipated(e.g. weight loss, resolution of co-morbidities), orbad (e.g. complications).
Obesity-specific HR-QOL instruments identi-fied during the literature search did not includeall the domains of the conceptual framework.Generic instruments, although considerably lon-ger than the obesity-specific instruments, containedirrelevant domains and still missed some of thedomains of the conceptual framework. Therefore,the currently available instruments, whether genericor obesity-specific, may underestimate the fullimpact of obesity on HR-QOL. This has beenacknowledged by previous researchers, as they
Table IV. Contd
Instrument name Description
5-Item European Quality of Life (EuroQoL EQ-5D) Another commonly used validated health survey. It is a short generic
instrument composed of five items including mobility, self-care, usual
activities, pain/discomfort, and anxiety/depression. It provides a single index
value that can be used in clinical and economical evaluation of healthcare[153]
Nottingham Health Profile (NHP) A validated HR-QOL instrument that has been used in bariatric surgery. It
consists of 38 items covering six domains: energy, pain, emotional reaction,
sleep, social isolation, and physical mobility. A major advantage of this
instrument is that it has been validated against a large population, which
makes it possible to compare results with a reference population. Another
advantage is that the instrument results can be reduced to one single value
that can be used as a utility index[22]
World Health Organization Quality of Life (WHOQOL 100) Assesses generic HR-QOL over a 2-week recall period. It includes 100 items,
which have been reduced to 26 validated items in the WHOQOL-BREF
instrument; covers four domains of physical health, mental health, social
relationships, and environment[154]
Manchester Short Assessment of Quality of Life (MANSA) Used to assess HR-QOL, developed by Priebe et al.[126] in 1999. It is a brief
instrument for assessing HR-QOL, focusing on satisfaction with life as a
whole and with life domains.[126] It has 14 specific life domains looking at
employment, financial situation, family relationships, accommodation,
sexuality, mental health, and physical health. It has satisfactory psychometric
properties, including validity and reliability[155]
QALY = quality-adjusted life-year; QOL = quality of life.
HR-QOL Instruments in Bariatric Surgery 81
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

administered more than one HR-QOL instru-ment in their studies, which is time consumingand difficult for both the patient and the clini-cian. Moreover, the use of multiple instrumentsmay increase the number of irrelevant items,and still not pick up all the domains of theframework.[37]
The findings from the current review contrastwith those of Stucki et al.,[43] although this isunsurprising since that review focused on thecontent of obesity-specific measures within therealm of generic utilization in a broad range ofpopulations encountering health concerns due toobesity. The current review focuses specificallyon the content and application of HR-QOLmeasures within the context of bariatric surgery.Furthermore, whereas the elegant review ofStucki et al.[43] compared instrument content withthe International Classification of Functioning,Disability and Health (ICF), the current reviewdeveloped a conceptual framework against whichboth generic and disease-specific measures wereassessed. Unsurprisingly, therefore, the con-clusions from both studies are different in that theuse of the conceptual framework within the cur-rent review emphasizes the requirement for anovel HR-QOL tool to be developed specificallyfor use within the bariatric clinical setting, giventhat the current instruments available would ap-pear inadequate. This contrasts with Stuckiet al.,[43] since the content comparisons were in-trinsically and fundamentally related to and de-termined by orientation to the ICF.
This review may represent the first step tobuilding a valid and true ‘bariatric’-specific instru-ment, as opposed to the majority of the currentlyavailable instruments, which are ‘obesity’-specificinstruments and might be unable to fully assessthe bariatric patient pre- and post-operatively.One potential limitation of the review concernsthe conceptual framework developed by the au-thors. It may be seen from this introduction thatthe authors present a conceptual frameworkstrictly focused on obesity and QOL. The devel-opment of a preliminary framework before goingto the literature could potentially introduce twotypes of bias: initial bias, as the framework couldbe influenced by the experience and knowledge of
the researcher, and ongoing bias as, once theframework is developed, it will influence the re-searcher’s thinking and may result in some issuesbeing overestimated and others being ignored.Whereas this is contextually sensitive to the pur-poses of the review, such an orientation may in-evitably introduce a degree of bias within the lit-erature search, since the focus of these elements isnecessarily circumscribed within the overarch-ing domain of bariatric surgery. This has beenaddressed by revisiting and refining the con-ceptual framework during the literature review.The assertions made, therefore, must be viewedas specific and not general.
6. Conclusion
Various aspects of the morbidly obese pa-tient’s life can be adversely affected, althoughmuch remains to be understood to be able tomeasure it scientifically and accurately. In thissystematic review of the literature, we foundthat most of the literature in bariatric surgeryeither did not report HR-QOL outcome, or theHR-QOL outcome was not given the appro-priate weight and importance. Whenever a HR-QOL instrument was used, the generic and othercondition-specific instruments were used notice-ably more frequently than the obesity-specificinstruments.
Over the years, several generic and obesity-specific instruments have been developed and usedin bariatric surgery; however, all had limitations.Content validity, which is a vital element when itcomes to deciding the type of instrument to beused, has been unsatisfactory and substandard forall the instruments we identified. Obese patientsneed to be given the opportunity to decide the se-verity of impairment of their HR-QOL, based ontheir own experience and criteria. Only then canthe full impact of morbid obesity and bariatricsurgery be assessed. We propose a conceptualframework detailing all the pertinent domains thatmight be affected, which can be used to develop anew bariatric-specific instrument. Such an instru-ment would display excellent content validity andcover all the potential aspects that might be af-fected by morbid obesity or bariatric surgery.
82 Tayyem et al.
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

Acknowledgments
No sources of funding were used to conduct this review orprepare this manuscript. The authors have no conflicts of in-terest that are directly relevant to the content of this review.
References1. Foster JH. Quality of life measurement and alcoholism:
another arm to nursing practice? Clin Eff Nurs 2006; 9:295-301
2. Costanza R, Fisher B, Ali S, et al. An integrative approachto quality of life measurement, research, and policy. S A PI E N S 2008; 1 (1): 17-21
3. Fallowfield L. What is quality of life? 2nd ed. HaywardMedical Communications, a division of Hayward GroupLtd [online]. Available from URL: http://www.medicine.ox.ac.uk/bandolier/painres/download/whatis/WhatisQOL.pdf [Accessed 2009 Oct 15]
4. US National Library of Medicine NLM, National Institutesof Health. National Information Center on Health ServicesResearch and Health Care Technology. HTA 101: glossary[online]. Available from URL: http://www.nlm.nih.gov/nichsr/hta101/ta101014.html [Accessed 2009 Oct 16]
5. Spilker B, Revicki DA. Taxonomy of quality of life. In:Spilker B, editors. Quality of life and pharmacoeconomics inclinical trials. Philadelphia (PA): Lippincott-Raven, 1999:25-32
6. Esposito K, Giugliano G, Scuderi N, et al. Role of adipo-kines in the obesity-inflammation relationship: the effectof fat removal. Plast Reconstr Surg 2006; 118: 1048-57
7. Doucet E. Gastrointestinal peptides after bariatric surgeryand appetite control: are they in tuning? Curr Opin ClinNutr Metab Care 2008; 11: 645-50
8. Major GC, Chaput JP, Ledoux M, et al. Recent develop-ments in calcium-related obesity research. Obes Rev 2008;9: 428-45
9. Pohl JF, Stephen M, Wilson DP. Pediatric obesity: impactand surgical management. South Med J 2006; 99: 833-44
10. DeMaria EJ. Bariatric surgery for morbid obesity. N Engl JMed 2007; 356: 2176-83
11. Presutti RJ,GormanRS, Swain JM. Primary care perspectiveon bariatric surgery. Mayo Clin Proc 2004; 79: 1158-66
12. Calle EE, Rodriguez C, Walker-Thurmond K, et al. Over-weight, obesity, and mortality from cancer in a prospectivelystudied cohort ofUS adults. NEngl JMed 2003; 348: 1625-38
13. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric sur-gery: a systematic review and meta-analysis. JAMA 2004;292: 1724-37
14. Brolin RE. Bariatric surgery and long-term control ofmorbid obesity. JAMA 2002; 288: 2793-6
15. Ellison SR, Ellison SD. Bariatric surgery: a review of theavailable procedures and complications for the emergencyphysician. J Emerg Med 2008; 34: 21-32
16. Wolf AM, Colditz GA. Current estimates of the economiccost of obesity in theUnited States.Obes Res 1998; 6: 97-106
17. Mokdad AH, Marks JS, Stroup DF, et al. Actual causes ofdeath in the United States, 2000. JAMA 2004; 291: 1238-45
18. Gould JC, Garren MJ, Gutowski KA. Bariatric surgery.Clin Obstet Gynecol 2006; 49: 375-88
19. Buchwald H. Overview of bariatric surgery. J AmColl Surg2002; 194: 367-75
20. Colquitt J, Clegg A, Loveman E, et al. Surgery for morbidobesity. Cochrane Database Syst Rev 2005; 4: CD003641
21. Treadwell JR, Sun F, Schoelles K. Systematic review andmeta-analysis of bariatric surgery for pediatric obesity.Ann Surg 2008; 248: 763-76
22. Livingston EH, Fink AS. Quality of life: cost and future ofbariatric surgery. Arch Surg 2003; 138: 383-8
23. Peter S, Craft R, Tiede J, et al. Impact of advanced age onweight loss and health benefits after laparoscopic gastricbypass. Arch Surg 2005; 140: 165-8
24. Butland B, Jebb S, Kopelman P, et al. Foresight tacklingobesities: future choices project report, 2nd ed. Govern-ment Office for Science [online]. Available from URL:http://www.foresight.gov.uk/Obesity/17.pdf [Accessed 2009Oct 17]
25. Wee CC. A 52-year-old woman with obesity: review ofbariatric surgery. JAMA 2009; 302: 1097-104
26. Matarasso A, Roslin MS, Kurian M. Bariatric surgery:an overview of obesity surgery. Plast Reconstr Surg 2007;119: 1357-62
27. McTigue KM, Harris R, Hemphill B, et al. Screening andinterventions for obesity in adults: summary of the evi-dence for the U.S. Preventive Services Task Force. AnnIntern Med 2003; 139: 933-49
28. Balsiger BM, Luque de LE, SarrMG. Surgical treatment ofobesity: who is an appropriate candidate?Mayo Clin Proc1997; 72: 551-7
29. Salem L, Jensen CC, Flum DR. Are bariatric surgicaloutcomes worth their cost? A systematic review. J AmColl Surg 2005; 200: 270-8
30. Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med2005; 142: 547-59
31. Sjostrom L, Lindroos AK, Peltonen M, et al. Lifestyle,diabetes, and cardiovascular risk factors 10 years afterbariatric surgery. N Engl J Med 2004; 351: 2683-93
32. Gould JC, Garren MJ, Starling JR. Laparoscopic gastricbypass results in decreased prescription medication costswithin 6 months. J Gastrointest Surg 2004; 8: 983-7
33. Sjostrom L, Narbro K, Sjostrom CD, et al. Effects ofbariatric surgery on mortality in Swedish obese subjects.N Engl J Med 2007; 357: 741-52
34. Ashrafian H, le Roux CW, Darzi A, et al. Effects of bari-atric surgery on cardiovascular function. Circulation2008; 118: 2091-102
35. Nguyen NT, Wilson SE, Wolfe BM. Rationale for lap-aroscopic gastric bypass. J Am Coll Surg 2005; 200: 621-9
36. Cummings DE, Overduin J, Foster-Schubert KE. Gastricbypass for obesity: mechanisms of weight loss and diabetesresolution. J Clin Endocrinol Metab 2004; 89: 2608-15
37. Reaney M, Martin C, Speight J. Understanding and as-sessing the impact of alcoholism on quality of life. Patient2008; 1: 151-63
38. Tayyem R, Ali A, Atkinson J, et al. Bariatric surgery andhealth related quality of life. In: Preedy V, Watson R,
HR-QOL Instruments in Bariatric Surgery 83
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

Martin C, editors. International handbook of behaviour,diet, and nutrition. New York: Springer, 2011
39. Spitzer RL, Kroenke K, Linzer M, et al. Health-relatedquality of life in primary care patients with mental dis-orders: results from the PRIME-MD 1000 Study. JAMA1995; 274: 1511-7
40. Contopoulos-Ioannidis DG, Karvouni A, Kouri I, et al.Reporting and interpretation of SF-36 outcomes in ran-domised trials: systematic review [abstract]. BMJ 2009;338: a3006
41. Kolotkin RL, Meter K, Williams GR. Quality of life andobesity. Obes Rev 2001; 2: 219-29
42. Duval K, Marceau P, Perusse L, et al. An overview ofobesity-specific quality of life questionnaires. Obes Rev2006; 7: 347-60
43. Stucki A, Borchers M, Stucki G, et al. Content comparisonof health status measures for obesity based on the inter-national classification of functioning, disability andhealth. Int J Obes (Lond) 2006; 30: 1791-9
44. Picot J, Jones J, Colquitt JL, et al. The clinical effectivenessand cost-effectiveness of bariatric (weight loss) surgery forobesity: a systematic review and economic evaluation.Health Technol Assess 2009; 13: 1-357, iii
45. van Hout GC, Boekestein P, Fortuin FA, et al. Psycho-social functioning following bariatric surgery. Obes Surg2006; 16: 787-94
46. Munoz DJ, Lal M, Chen EY, et al. Why patients seekbariatric surgery: a qualitative and quantitative analysisof patient motivation. Obes Surg 2007; 17: 1487-91
47. Phillips E. Design and demography of the United StatesSwedish Adjustable Gastric Band trial: a 3-year pro-spective study. Surg Obes Relat Dis 2008; 4: S63-72
48. Green AE, Dymek-Valentine M, Pytluk S, et al. Psycho-social outcome of gastric bypass surgery for patients withand without binge eating. Obes Surg 2004; 14: 975-85
49. Menderes A, Baytekin C, Haciyanli M, et al. Dermalipec-tomy for body contouring after bariatric surgery in Ae-gean region of Turkey. Obes Surg 2003; 13: 637-41
50. NguyenNT,GoldmanC,Rosenquist CJ, et al. Laparoscopicversus open gastric bypass: a randomized study of out-comes, quality of life, and costs. Ann Surg 2001; 234: 279-89
51. Weiner S, Sauerland S, Fein M, et al. The Bariatric Qualityof Life index: a measure of well-being in obesity surgerypatients. Obes Surg 2005; 15: 538-45
52. Tolonen P, VictorzonM,Makela J. Impact of laparoscopicadjustable gastric banding for morbid obesity on disease-specific and health-related quality of life. Obes Surg 2004;14: 788-95
53. Khoueir P, Black MH, Crookes PF, et al. Prospectiveassessment of axial back pain symptoms before andafter bariatric weight reduction surgery. Spine J 2009; 9:454-63
54. Sauerland S, Weiner S, Hausler E, et al. Validity of theCzech, German, Italian, and Spanish version of theMoorehead-Ardelt II questionnaire in patients withmorbid obesity. Obesity Facts 2009; 2 Suppl. 1: 57-62
55. van Hout GC, Fortuin FA, Pelle AJ, et al. Health-relatedquality of life following vertical banded gastroplasty. SurgEndosc 2009; 23: 550-6
56. Sauerland S, Weiner S, Doezalova K, et al. Mapping utilityscores from a disease-specific quality-of-life measure inbariatric surgery patients. Value Health 2009; 12: 364-70
57. Muller MK, Wenger C, Schiesser M, et al. Quality of lifeafter bariatric surgery: a comparative study of laparos-copic banding vs. bypass. Obes Surg 2008; 18: 1551-7
58. Nguyen NT, Slone JA, Nguyen XM, et al. A prospectiverandomized trial of laparoscopic gastric bypass versuslaparoscopic adjustable gastric banding for the treatmentof morbid obesity: outcomes, quality of life, and costs.Ann Surg. Epub 2009 Aug 27
59. Sutton D, Raines DA. Health-related quality of life fol-lowing a surgical weight loss intervention. Appl Nurs Res2010; 23: 52-6
60. Brancatisano A, Wahlroos S, Brancatisano R. Improvementin comorbid illness after placement of the Swedish Adjust-able Gastric Band. Surg Obes Relat Dis 2008; 4: S39-46
61. Wagner AJ, Fabry Jr JM, Thirlby RC. Return to workafter gastric bypass in Medicaid-funded morbidly obesepatients. Arch Surg 2007; 142: 935-40
62. Frezza EE, Shebani KO, Wachtel MS. Laparoscopic gastricbypass for morbid obesity decreases bodily pain, improvesphysical functioning, and mental and general health inwomen. J Laparoendosc Adv Surg Tech A 2007; 17: 440-7
63. Larsen JK, Zijlstra H, van RB, et al. Conversion to gastricbypass in patients with unsuccessful weight loss aftergastric banding may depend on mental quality of life.Obes Facts 2010; 3: 127-30
64. Weiner S, Sauerland S, Weiner R, et al. Quality of life afterbariatric surgery: is there a difference? Chir GastroenterolInterdisziplin 2005; 21: 34-6
65. Ballantyne GH. Measuring outcomes following bariatricsurgery: weight loss parameters, improvement in co-morbid conditions, change in quality of life and patientsatisfaction. Obes Surg 2003; 13: 954-64
66. de ZM, Lancaster KL, Mitchell JE, et al. Health-relatedquality of life in morbidly obese patients: effect of gastricbypass surgery. Obes Surg 2002; 12: 773-80
67. de ZM, Mitchell JE, Howell LM, et al. Two measures ofhealth-related quality of life in morbid obesity. Obes Res2002; 10: 1143-51
68. Kolotkin RL, Norquist JM, Crosby RD, et al. One-yearhealth-related quality of life outcomes in weight loss trialparticipants: comparison of three measures [abstract].Health Qual Life Outcomes 2009; 7: 53
69. Kolotkin RL, Crosby RD, Gress RE, et al. Two-yearchanges in health-related quality of life in gastric bypasspatients compared with severely obese controls. SurgObes Relat Dis 2009; 5: 250-6
70. Kolotkin RL, Crosby RD, Gress RE, et al. Health andhealth-related quality of life: differences between men andwomen who seek gastric bypass surgery. Surg Obes RelatDis 2008; 4: 651-8
71. Kolotkin RL, Crosby RD. Psychometric evaluation of theimpact of weight on quality of life-lite questionnaire(IWQOL-lite) in a community sample. Qual Life Res2002; 11: 157-71
72. O’Brien PE, Sawyer SM, Laurie C, et al. Laparoscopicadjustable gastric banding in severely obese adolescents:a randomized trial. JAMA 2010; 303: 519-26
84 Tayyem et al.
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

73. O’Brien PE, Dixon JB, Laurie C, et al. A prospective ran-domized trial of placement of the laparoscopic adjustablegastric band: comparison of the perigastric and parsflaccida pathways. Obes Surg 2005; 15: 820-6
74. O’Brien PE, Dixon JB, Brown W, et al. The laparoscopicadjustable gastric band (Lap-Band): a prospective studyof medium-term effects on weight, health and quality oflife. Obes Surg 2002; 12: 652-60
75. Dixon JB, DixonME, O’Brien PE. Quality of life after lap-band placement: influence of time, weight loss, and co-morbidities. Obes Res 2001; 9: 713-21
76. Carmichael AR, Sue-Ling HM, Johnston D. Quality of lifeafter the Magenstrasse and Mill procedure for morbidobesity. Obes Surg 2001; 11: 708-15
77. Horchner R, Tuinebreijer MW, Kelder PH. Quality-of-lifeassessment of morbidly obese patients who have under-gone a Lap-Band operation – 2-year follow-up study: isthe MOS SF-36 a useful instrument to measure quality oflife in morbidly obese patients? Obes Surg 2001; 11: 212-8
78. Sendi P, Brunotte R, Potoczna N, et al. Health-relatedquality of life in patients with class II and class III obesity.Obes Surg 2005; 15: 1070-6
79. Sanchez-Santos R, Del BarrioMJ, Gonzalez C, et al. Long-term health-related quality of life following gastric by-pass: influence of depression. Obes Surg 2006; 16: 580-5
80. Bilbao A, Mar J, Mar B, et al. Validation of the Spanishtranslation of the questionnaire for the obesity-relatedproblems scale. Obes Surg 2009; 19: 1393-400
81. Ackroyd R, Mouiel J, Chevallier JM, et al. Cost-effective-ness and budget impact of obesity surgery in patients withtype-2 diabetes in three European countries. Obes Surg2006; 16: 1488-503
82. Oria HE,Moorehead MK. Bariatric Analysis and ReportingOutcome System (BAROS). Obes Surg 1998; 8: 487-99
83. Oria HE,MooreheadMK. Updated Bariatric Analysis andReporting Outcome System (BAROS). Surg Obes RelatDis 2009; 5: 60-6
84. Suter M, Calmes JM, Paroz A, et al. Results of Roux-en-Ygastric bypass in morbidly obese vs superobese patients:similar body weight loss, correction of comorbidities, andimprovement of quality of life. Arch Surg 2009; 144: 312-8
85. ChangKH,CondonET,O’ConnorEJ, et al. Sustainedweightloss and improvement of quality of life after laparoscopicadjustable gastric banding for morbid obesity: a single sur-geon experience in Ireland. Ir J Med Sci 2010; 179: 23-7
86. Todkar JS, Shah SS, Shah PS, et al. Long-term effects oflaparoscopic sleeve gastrectomy in morbidly obese subjectswith type 2 diabetes mellitus. Surg Obes Relat Dis 2010; 6:142-5
87. Larrad-Jimenez A, Diaz-Guerra CS, de Cuadros BP, et al.Short-, mid- and long-term results of Larrad biliopan-creatic diversion. Obes Surg 2007; 17: 202-10
88. Kinzl JF, Schrattenecker M, Traweger C, et al. Quality oflife in morbidly obese patients after surgical weight loss.Obes Surg 2007; 17: 229-35
89. Peterli R,Wolnerhanssen BK, Peters T, et al. Prospective studyof a two-stage operative concept in the treatment of morbidobesity: primary lap-band followed if needed by sleeve gas-trectomy with duodenal switch. Obes Surg 2007; 17: 334-40
90. Silberhumer GR, Miller K, Kriwanek S, et al. Laparos-copic adjustable gastric banding in adolescents: the Aus-trian experience. Obes Surg 2006; 16: 1062-7
91. Puzziferri N, Austrheim-Smith IT, Wolfe BM, et al. Three-year follow-up of a prospective randomized trial com-paring laparoscopic versus open gastric bypass. Ann Surg2006; 243: 181-8
92. Mamplekou E, Komesidou V, Bissias C, et al. Psycho-logical condition and quality of life in patients with mor-bid obesity before and after surgical weight loss. ObesSurg 2005; 15: 1177-84
93. Gabriel SG, Karaindros CA, Papaioannou MA, et al. Bil-iopancreatic diversion with duodenal switch combinedwith laparoscopic adjustable gastric banding. Obes Surg2005; 15: 517-22
94. Pasnik K, Krupa J, Stanowski E. Vertical banded gastro-plasty: 6 years experience at a center in Poland. Obes Surg2005; 15: 223-7
95. Hell E, Miller KA, Moorehead MK, et al. Evaluation ofhealth status and quality of life after bariatric surgery:comparison of standard Roux-en-Y gastric bypass, verti-cal banded gastroplasty and laparoscopic adjustable sili-cone gastric banding. Obes Surg 2000; 10: 214-9
96. Miller K, Pump A, Hell E. Vertical banded gastroplastyversus adjustable gastric banding: prospective long-termfollow-up study. Surg Obes Relat Dis 2007; 3: 84-90
97. Souto KE,Meinhardt NG, Stein AT. Evaluation of qualityof life and metabolic improvement after jejunoileal bypassin a community of low socioeconomic status. Obes Surg2004; 14: 823-8
98. Guedea ME, Arribas del AD, Solanas JA, et al. Results ofbiliopancreatic diversion after five years. Obes Surg 2004;14: 766-72
99. Tolonen P, VictorzonM. Quality of life following laparoscop-ic adjustable gastric banding: the Swedish band and theMoorehead-Ardelt questionnaire. Obes Surg 2003; 13: 424-6
100. Victorzon M, Tolonen P. Bariatric Analysis and ReportingOutcome System (BAROS) following laparoscopic adjust-able gastric banding in Finland. Obes Surg 2001; 11: 740-3
101. Caniato D, Skorjanec B. The role of brief strategic therapy onthe outcome of gastric banding. Obes Surg 2002; 12: 666-71
102. Wolf AM, Falcone AR, Kortner B, et al. BAROS: an ef-fective system to evaluate the results of patients afterbariatric surgery. Obes Surg 2000; 10: 445-50
103. Favretti F, Cadiere GB, Segato G, et al. Bariatric Analysisand Reporting Outcome System (BAROS) applied tolaparoscopic gastric banding patients. Obes Surg 1998; 8:500-4
104. Kolotkin RL, Crosby RD, Kosloski KD, et al. Develop-ment of a brief measure to assess quality of life in obesity.Obes Res 2001; 9: 102-11
105. Kolotkin RL, Crosby RD, Williams GR. Health-relatedquality of life varies among obese subgroups. Obes Res2002; 10: 748-56
106. Ryden A, Karlsson J, Persson LO, et al. Obesity-relatedcoping and distress and relationship to treatment prefer-ence. Br J Clin Psychol 2001; 40: 177-88
107. Ryden A, Karlsson J, Sullivan M, et al. Coping and dis-tress: what happens after intervention? A 2-year follow-up
HR-QOL Instruments in Bariatric Surgery 85
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

from the Swedish Obese Subjects (SOS) study. PsychosomMed 2003; 65: 435-42
108. Champault A, Duwat O, Polliand C, et al. Quality of lifeafter laparoscopic gastric banding: prospective study (152cases) with a follow-up of 2 years. Surg Laparosc EndoscPercutan Tech 2006; 16: 131-6
109. Poves I, Cabrera M, Maristany C, et al. Gastrointestinalquality of life after laparoscopic Roux-en-Y gastric by-pass. Obes Surg 2006; 16: 19-23
110. Lee WJ, Yu PJ, Wang W, et al. Laparoscopic Roux-en-Yversus mini-gastric bypass for the treatment of morbidobesity: a prospective randomized controlled clinical trial.Ann Surg 2005; 242: 20-8
111. Lee WJ, Huang MT, Yu PJ, et al. Laparoscopic verticalbanded gastroplasty and laparoscopic gastric bypass:a comparison. Obes Surg 2004; 14: 626-34
112. Foster A, Laws HL, Gonzalez QH, et al. Gastrointestinalsymptomatic outcome after laparoscopic Roux-en-Ygastric bypass. J Gastrointest Surg 2003; 7: 750-3
113. Clements RH, Gonzalez QH, Foster A, et al. Gastro-intestinal symptoms are more intense in morbidly obesepatients and are improved with laparoscopic Roux-en-Ygastric bypass. Obes Surg 2003; 13: 610-4
114. Lee WJ, Wang W, Yu PJ, et al. Gastrointestinal quality oflife following laparoscopic adjustable gastric banding inAsia. Obes Surg 2006; 16: 586-91
115. Wang W, Wei PL, Lee YC, et al. Short-term results of lap-aroscopic mini-gastric bypass. Obes Surg 2005; 15: 648-54
116. Lee WJ, Yu PJ, Wang W, et al. Gastrointestinal quality oflife following laparoscopic vertical banded gastroplasty.Obes Surg 2002; 12: 819-24
117. Arcila D, Velazquez D, Gamino R, et al. Quality of life inbariatric surgery. Obes Surg 2002; 12: 661-5
118. Melissas J, Kontakis G, Volakakis E, et al. The effect of sur-gical weight reduction on functional status in morbidly obesepatients with low back pain. Obes Surg 2005; 15: 378-81
119. Govindarajan R, Ghosh B, Sathyamoorthy MK, et al.Efficacy of ketorolac in lieu of narcotics in the operativemanagement of laparoscopic surgery for morbid obesity.Surg Obes Relat Dis 2005; 1: 530-5
120. van Gemert WG, Adang EM, Kop M, et al. A prospectivecost-effectiveness analysis of vertical banded gastroplastyfor the treatment ofmorbid obesity.Obes Surg 1999; 9: 484-91
121. van Gemert WG, Adang EM, Greve JW, et al. Quality of lifeassessment of morbidly obese patients: effect of weight-reducing surgery. Am J Clin Nutr 1998; 67: 197-201
122. Guisado JA, Vaz FJ, Alarcon J, et al. Psychopathologicalstatus and interpersonal functioning following weight lossin morbidly obese patients undergoing bariatric surgery.Obes Surg 2002; 12: 835-40
123. Papageorgiou GM, Papakonstantinou A, Mamplekou E,et al. Pre- and postoperative psychological characteristicsin morbidly obese patients. Obes Surg 2002; 12: 534-9
124. Ryde NO, Hedenbro J, Frederiksen S. Weight loss aftervertical banded gastroplasty can be predicted: a pro-spective psychological study. Obes Surg 1996; 6: 237-43
125. Dinc G, Eser E, Saatli GL, et al. The relationship betweenobesity and health related quality of life of women in aTurkish city with a high prevalence of obesity. Asia Pac JClin Nutr 2006; 15: 508-15
126. Priebe S, Huxley P, Knight S, et al. Application and resultsof the Manchester Short Assessment of Quality of Life(MANSA). Int J Soc Psychiatry 1999; 45: 7-12
127. Isacsson A, Frederiksen SG, Nilsson P, et al. Quality of lifeafter gastroplasty is normal: a controlled study. Eur JSurg 1997; 163: 181-6
128. Le Pen C, Levy E, Loos F, et al. ‘‘Specific’’ scale comparedwith ‘‘generic’’ scale: a double measurement of the qualityof life in a French community sample of obese subjects.J Epidemiol Community Health 1998; 52: 445-50
129. Mathus-Vliegen EM, de Wit LT. Health-related quality oflife after gastric banding. Br J Surg 2007; 94: 457-65
130. Mathus-Vliegen EM, de WS, de Wit LT. Health-relatedquality-of-life in patients with morbid obesity after gastricbanding for surgically induced weight loss. Surgery 2004;135: 489-97
131. University ofWashington. Obesity andWeight-Loss Quality-of-Life Instrument (OWLQOL) [online]. Available fromURL: http://depts.washington.edu/yqol/docs/OWLQOL%20and%20WRSM%20combined%20measure.pdf [Ac-cessed 2009 Oct 17]
132. Butler GS, Vallis TM, Perey B, et al. The Obesity Adjust-ment Survey: development of a scale to assess psycho-logical adjustment to morbid obesity. Int J Obes RelatMetab Disord 1999; 23: 505-11
133. Mannucci E, Ricca V, Barciulli E, et al. Quality of life andoverweight: the obesity related well-being (Orwell 97)questionnaire. Addict Behav 1999; 24: 345-57
134. Buddeberg-Fischer B, Klaghofer R, Krug L, et al. Physicaland psychosocial outcome inmorbidly obese patients withand without bariatric surgery: a 4 1/2-year follow-up.Obes Surg 2006; 16: 321-30
135. Buddeberg-Fischer B, Klaghofer R, Sigrist S, et al. Impactof psychosocial stress and symptoms on indication forbariatric surgery and outcome in morbidly obese patients.Obes Surg 2004; 14: 361-9
136. Gerten KA, Richter HE, Burgio KL, et al. Impact of urinaryincontinence in morbidly obese women versus women seek-ing urogynecologic care. Urology 2007; 70: 1082-5
137. Kapoor DS, Davila GW, Rosenthal RJ, et al. Pelvic floordysfunction in morbidly obese women: pilot study. ObesRes 2004; 12: 1104-7
138. Woodard GA, Encarnacion B, Downey JR, et al. Pro-biotics improve outcomes after Roux-en-Y gastric bypasssurgery: a prospective randomized trial. J GastrointestSurg 2009; 13: 1198-204
139. Zainabadi K, Courcoulas AP, Awais O, et al. Laparoscopicrevision of Nissen fundoplication to Roux-en-Y gastricbypass in morbidly obese patients. Surg Endosc 2008; 22:2737-40
140. MunozDJ, Chen E, Fischer S, et al. Considerations for the useof the BeckDepression Inventory in the assessment ofweight-loss surgery seeking patients. Obes Surg 2007; 17: 1097-101
141. Dixon JB, Dixon ME, O’Brien PE. Depression in associa-tion with severe obesity: changes with weight loss. ArchIntern Med 2003; 163: 2058-65
142. Wasserberg N, HaneyM, Petrone P, et al. Fecal incontinenceamong morbidly obese women seeking weight loss surgery:an underappreciated association with adverse impact onquality of life. Int J Colorectal Dis 2008; 23: 493-7
86 Tayyem et al.
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)

143. Lang T, Hauser R, Buddeberg C, et al. Impact of gastricbanding on eating behavior and weight. Obes Surg 2002;12: 100-7
144. Guisado JA, Vaz FJ, Lopez-Ibor Jr JJ, et al. Eating be-havior in morbidly obese patients undergoing gastricsurgery: differences between obese people with and with-out psychiatric disorders. Obes Surg 2001; 11: 576-80
145. Zijlstra H, Larsen JK, van RB, et al. The association be-tween weight loss and self-regulation cognitions beforeand after laparoscopic adjustable gastric banding forobesity: a longitudinal study. Surgery 2006; 139: 334-9
146. Abiles V, Rodriguez-Ruiz S, Abiles J, et al. Psychologicalcharacteristics of morbidly obese candidates for bariatricsurgery. Obes Surg 2010; 20: 161-7
147. Bocchieri-Ricciardi LE, Chen EY, Munoz D, et al. Pre-surgery binge eating status: effect on eating behavior andweight outcome after gastric bypass. Obes Surg 2006; 16:1198-204
148. Dymek-Valentine M, Rienecke-Hoste R, Alverdy J. Assess-ment of binge eating disorder in morbidly obese patientsevaluated for gastric bypass: SCID versus QEWP-R.Eat Weight Disord 2004; 9: 211-6
149. Buser A, Dymek-Valentine M, Hilburger J, et al. Outcomefollowing gastric bypass surgery: impact of past sexualabuse. Obes Surg 2004; 14: 170-4
150. Wasserberg N, Petrone P, Haney M, et al. Effect of surgi-cally induced weight loss on pelvic floor disorders inmorbidly obese women. Ann Surg 2009; 249: 72-6
151. Laungani RG, Seleno N, Carlin AM. Effect of laparoscopicgastric bypass surgery on urinary incontinence in morbidlyobese women. Surg Obes Relat Dis 2009; 5: 334-8
152. QualityMetric. SF-36v2 Health Survey [online]. Availablefrom URL: http://www.qualitymetric.com/WhatWeDo/GenericHealthSurveys/SF36v2HealthSurvey/tabid/185/Default.aspx [Accessed 2009 Oct 17]
153. The EuroQol Group. EuroQol: a new facility for themeasurement of health-related quality of life. HealthPolicy 1990; 16: 199-208
154. The WHOQOL Group. Development of the World HealthOrganization WHOQOL-BREF quality of life assess-ment. Psychol Med 1998; 28: 551-8
155. Puschner B, Born A, Giessler A, et al. Adherence to med-ication and quality of life in people with schizophrenia:results of a European multicenter study. J Nerv Ment Dis2006; 194: 746-52
156. Kolotkin RL, Head S, HamiltonM, et al. Assessing impactof weight on quality of life. Obes Res 1995; 3: 49-56
157. University of Washington. Introducing the OWLQOL andWRSM instruments [online]. Available fromURL: http://depts.washington.edu/yqol/docs/OWLQOLWRSM_Info.pdf [Accessed 2009 Oct 17]
158. Niero M, Martin M, Finger T, et al. A new approach tomulticultural item generation in the development of twoobesity-specific measures: the Obesity and Weight LossQuality of Life (OWLQOL) questionnaire and theWeight-Related Symptom Measure (WRSM). Clin Ther2002; 24: 690-700
159. Karlsson J, Sjostrom L, SullivanM. Swedish obese subjects(SOS) – an intervention study of obesity: two-year follow-up of health-related quality of life (HRQL) and eatingbehavior after gastric surgery for severe obesity. Int JObes Relat Metab Disord 1998; 22: 113-26
160. MooreheadMK, Ardelt-Gattinger E, Lechner H, et al. Thevalidation of the Moorehead-Ardelt Quality of LifeQuestionnaire II. Obes Surg 2003; 13: 684-92
161. Walker J, Bradley C. Assessing the quality of life of ado-lescents with diabetes: using the SEIQoL, DQoL, patientand diabetes specialist nurse ratings. Pract Diab Int 2002;19: 141-4
Correspondence: Professor Colin R. Martin, University ofthe West of Scotland, Ayr Campus, Beech Grove, Ayr,KA8 0SR, UK.E-mail: [email protected]
HR-QOL Instruments in Bariatric Surgery 87
ª 2011 Adis Data Information BV. All rights reserved. Patient 2011; 4 (2)