
An Introduction of Healthcare Market in China
29
-
Upload
ziqian-wang -
Category
Healthcare
-
view
982 -
download
1
Transcript of An Introduction of Healthcare Market in China

IntroductionofHealthcareMarketinChinaAnoverviewofthehealthcaremarketThehierarchyofthemedicalsystemPublichospitalsPhysicians’workconditionandsalariesOutpatientpatientconsultation
MedicalInsuranceSysteminChinaThedevelopmentofthesystemUniversalhealthcareinsurance
ContinuedMedicalEducationforPhysiciansinChinaCEMpolicyandcreditsystemMajorissuesofCMEactivitiesAccreditationcriteriafornationalCMEcourses
TableofContents
2

Anoverview ofthehealthcaremarket inChina1
• From2004to2011,healthcaremarketinChinaincreasedby18%annually
• ThepublicexpenseonhealthcareinChinaisstillquitelow,accountingforonly5%oftotalGDP.Thispercentagecouldincreaseto6,5– 7%by2020.
• Themarketislargelymonopolizedbythepublichospitals:
44%
18%
38%
Government Otherorganisations Private
Thenumber ofpublichospitalsaccountsfor62%overthetotalnumber
Thetotalamountofserviceprovided byprivatehospitalsonlyaccounts for9%in2011
Only1%oftheprivate–ownedhospitalsarethesocalled« Tier3Ahospitals »inChina
3
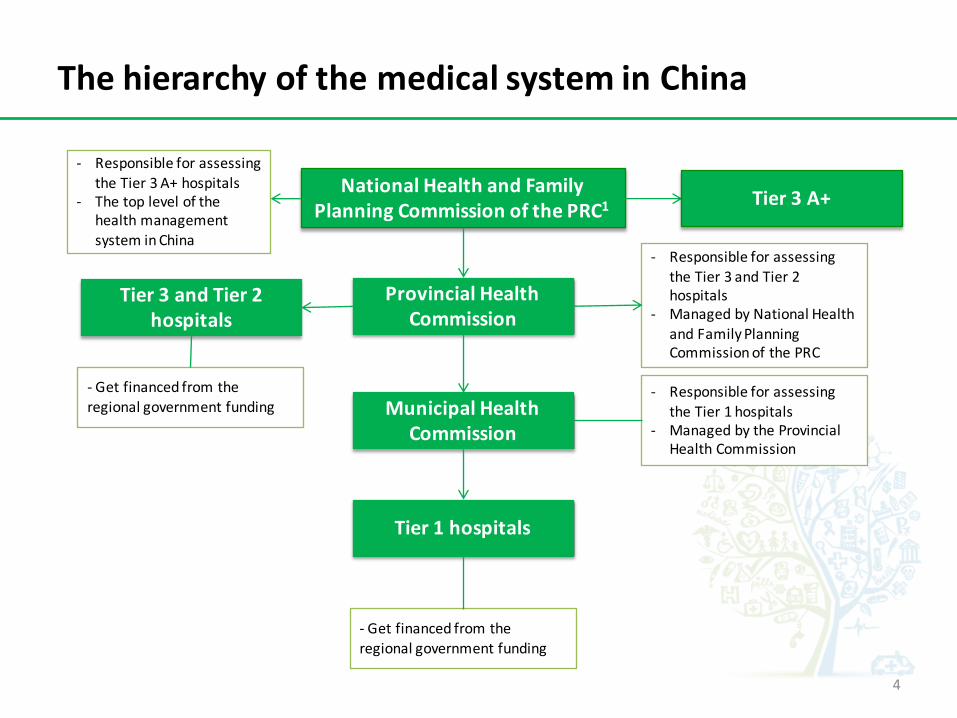
ThehierarchyofthemedicalsysteminChina
NationalHealthandFamilyPlanningCommissionofthePRC1
ProvincialHealthCommission
MunicipalHealthCommission
Tier1hospitals
- ResponsibleforassessingtheTier1hospitals
- ManagedbytheProvincialHealthCommission
- Getfinancedfromtheregionalgovernmentfunding
Tier3andTier2hospitals
- Getfinancedfromtheregionalgovernmentfunding
Tier3A+
- ResponsibleforassessingtheTier3andTier2hospitals
- ManagedbyNationalHealthandFamilyPlanningCommissionofthePRC
- ResponsibleforassessingtheTier3A+hospitals
- ThetoplevelofthehealthmanagementsysteminChina
4
PublichospitalsinChina1
• The public hospitals in China are not pure non-profit organisations (In reality)– Public funding only covers part of hospitals operational expenses– Public hospitals have to and are allowed to generate and keep the profits in order to cover all their
operational expenses.– However, public hospitals have to declare the total amount of salaries as well as the bonus they distributed
to doctors to Health Commissions. Health Commissions will assess this amount with other relatinggovernmental departments to set the total amount of salaries that hospitals could distribute to doctors inthe next year. The bonus distributed under this amount is allowed.
– Hospitals’ research expenses are mainly from some specific public funding, aiming at supporting thescientific researches. Hospitals can apply for these funds from the National Health Commission or fromother governmental organisations.
• However, in theory, China’s hospitals should be non-profit organisations, meaning that they have to distributeall their incomes back to the public funding. However, since the financial supports from the public funding aretoo limited, which can hardly support public hospitals’ daily operations, it has become an unspoken rule in thehealth system in China that public hospitals have to find their ways to generate profits in order to maintain theirday-to-day operation. Different from what the public believes, many public hospitals in China are suffering fromlosses every year.
• Cashgeneratorsinpublichospitals– Registrationfees– Treatment fees– Inspectionfees– Drugsales
5

ClassificationofChinesehospitals
• InChina,hospitalsareclassifiedinto3tiers,whichareTier1,2and3.• Eachtierwillbefurtherclassifiedintothreesub-tiers,whichare甲 (Jia =A),乙(Yi=B),丙
(Bing=C).
Tier 3 3B
3A
3C
Tier 2 2 B
2 A
2 C
Tier 1 1 B
1 A
1C
Tier 3A+2
- Comprehensiveorgeneralhospitals1 atthecity,provincialornationallevelwithabedcapacityexceeding500.
- Responsibleforofferingspecialistservice,conductingscientificresearchtosolvemajormedicalchallengesandprovidingmedicaleducationfor1and2tierhospitals.
- Mainlynationalandprovincialmajorhospitalsoraffiliatedhospitalsofmajormedicaluniversities.
- Regionalhospitalsprovidingmedicalservicesacrossseveralcommunities.
- Providemedicaltrainingsandlimitedmedicaleducationtotier1hospitals.
- Hospitalsmainlyaffiliatedwithmediumorsmallcities,countiesordistrictsinbigcities.
- Directlyprovidemedicalservicetocommunitiesregardingdiseaseprevention, recoveringandotherhealthcareservices
- Townshiphospitalsinruralareasandcommunityhospitalsinbigcities
- Hospitalswiththemostadvanced facilitiesandabletoprovidemedicalservicestothetopgovernmentalleaders
- AssessedbyNationalHealthCommission
Haveverystronginfluenceonlower- tierhospitalswithregardtonewdrugpublicizing
RarelyexistinbigcitiessuchasBeijingandShanghai
6
Chinesephysicians’workconditionsandsalaries1
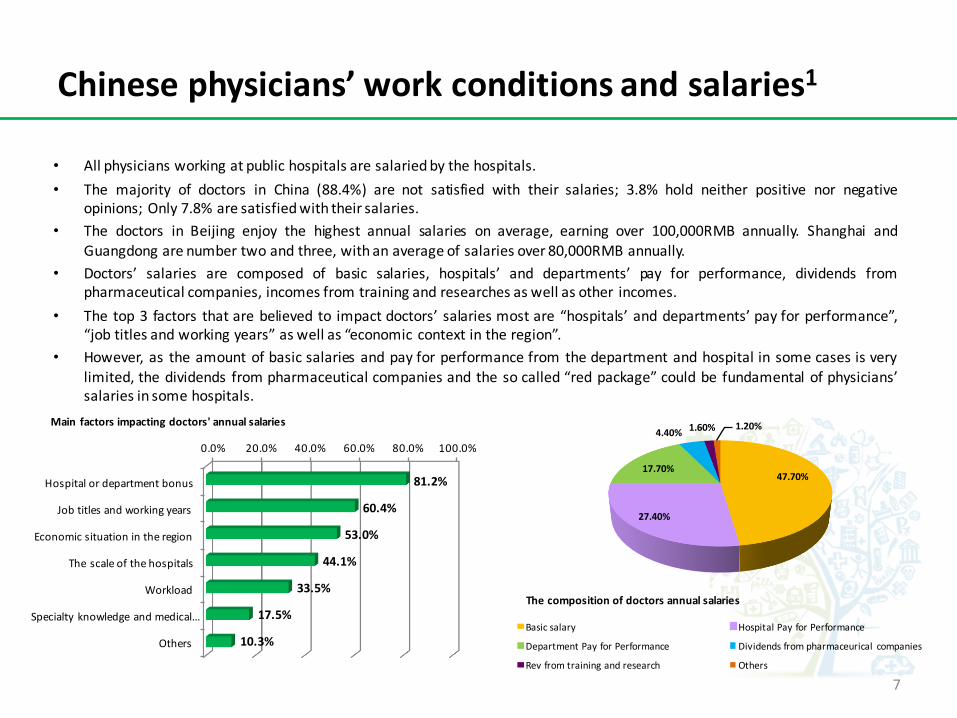
• All physicians working at public hospitals are salariedby the hospitals.• The majority of doctors in China (88.4%) are not satisfied with their salaries; 3.8% hold neither positive nor negative
opinions; Only 7.8% are satisfiedwith their salaries.• The doctors in Beijing enjoy the highest annual salaries on average, earning over 100,000RMB annually. Shanghai and
Guangdong are number two and three, with an average of salaries over 80,000RMB annually.• Doctors’ salaries are composed of basic salaries, hospitals’ and departments’ pay for performance, dividends from
pharmaceutical companies, incomes from training and researches as well as other incomes.• The top 3 factors that are believed to impact doctors’ salaries most are “hospitals’ and departments’ pay for performance”,
“job titles and working years” as well as “economic context in the region”.• However, as the amount of basic salaries and pay for performance from the department and hospital in some cases is very
limited, the dividends from pharmaceutical companies and the so called “red package” could be fundamental of physicians’salaries in some hospitals.
47.70%
27.40%
17.70%
4.40% 1.60% 1.20%
Basicsalary HospitalPayforPerformance
DepartmentPayforPerformance Dividendsfrompharmaceurical companies
Revfromtrainingandresearch Others
Thecompositionofdoctorsannualsalaries
0.0% 20.0% 40.0% 60.0% 80.0% 100.0%
Hospitalordepartmentbonus
Jobtitlesandworkingyears
Economicsituationintheregion
Thescaleofthehospitals
Workload
Specialtyknowledgeandmedical…
Others
81.2%
60.4%
53.0%
44.1%
33.5%
17.5%
10.3%
Main factorsimpactingdoctors'annualsalaries
7

Chinesephysicians’workconditionandsalaries1
0 1000 2000 3000 4000 5000 6000 7000 8000 9000
CardiothoracicsurgeryNeurologyGeriatries
GastroenteralogyIntensiveCareMedicine
AnesthesiologyUrology
OncologyEmergency
InternalMedicine-CardiovascularStamatologyResparitoryNephrology
GeneralSurgeryInfectious Disease
OrthopedicsPediatrics
PhysicalMedicineandRehabilitationGeneralNeurosurgery
HematologyOBGYN
Immunology - RheumatologyMentalhealth
OtorhinolaryngologyImaging&radiology
EndocrinologyOphthalmology
Dermatology&sexuallytransmitteddiseaseGeneralmedicine
SurgeryTraditionalChineseMedicine
GPs
889888778874874386368627856384918454842583848346832882938243
805180007979795279097836783377847764775576227615757975107453
66885938
• Thetop5departmentsearningthehighestannualsalariesareDepartmentsofCardiothoracicsurgery,Neurology,Geriatries,GastroenteralogyandIntensiveCareMedicine.
• Thebottom5departmentsearningthelowestannualsalariesareDepartmentsofDermatology&SexuallyTransmittedDiseases,GeneralMedicine,Surgery,TraditionalChineseMedicineaswellasGPs.
• Moreover,nearly73%ofChinesephysiciansworkover9hoursperday.
• 100%ofphysiciansworkingovertimeatTier3AhospitalsinbigcitiessuchasBeijingandShanghai
Rankingofthedepartments byannualsalaries/Euros2
27.0%
67.5%
4.9% 0.5%
below8hrs 9- 12hrs 13- 16hrs over16hrs
Physicians’workinghourperday
8

OutpatientconsultationinChina
Step1•Thepatientcanbrieflyexplainhis/herhealthproblemstothenurseattheconsultationdesk,whowillprovidesguidanceontowhichdepartmentsofspecialtiespatientscouldgoforconsultation.However,thefinaldecisionwillbemadebypatients.(Optional)
Step2•Thepatientasksanappointmentwiththephysicianstheywouldliketovisitandpaysfortheregistrationfees
Step3•Ifitwasthefirsttimethatthepatientscometothishospital,theyhavetobuyaconsultationnotebookusedforphysiciansonlyinthishospitaltowritedownpatients’medicalrecords(Thisnotebookcannotbeusedacrossdifferenthospitals)
Step4•Waitsfortheconsultationaccordingtothetimerangegivenontheregistrationticket
Step5•Aftertheconsultation,physicianswillgivetheprescriptionstopatients.
Step6•Patientspayforallmedicinesontheprescriptionsinthehospitalandtaketheinvoice.
Step7•Gotothemedicinecollectiondeskinthehospitaltocollectalltheirmedicineswiththeinvoice.
Issue1:InChina,patientsdon’tgothroughtheprocessfortheconsultationwithGPsandapproachtothespecialtiesaccordingtotheirguidance.Infact,theyasktheappointmentswithsomespecialtiesbasedontheunderstandingoftheirownillness,leadingtothewasteofprofessionalresourcesinmanyregards:- Gotospecialtiestodealwithissues
thatGPscoulddealwith- Approachthewrongspecialtiesdueto
thewrongconceptionontheirowndiseases
Issue2:LimitedProfessionalResourcesvsExtremelyHighDemand- Thetopphysiciansarehighly
concentratedinafewTier3AhospitalsinsomebigcitiessuchasBeijingandShanghai.Patientscomingfromalltheotherregionsinthecountryplungeintothislimitednumberofhospitals.
Issue3:- TheconsultationfeesinChinaareverylow,normallyrangingfrom3-70RMBinpublichospitals,anequivalentof0,35–8,25euros.Duetothelackofpublicfundsfromthegov andtheverylowconsultationfees,manypublichospitalstruetodrugstoincreasetheirprofits.
9

IntroductionofHealthcareMarketinChinaAnoverviewofthehealthcaremarketThehierarchyofthemedicalsystemPublichospitalsPhysicians’workconditionandsalariesOutpatientpatientconsultation
MedicalInsuranceSysteminChinaThedevelopmentofthesystemUniversalhealthcareinsurance
ContinuedMedicalEducationforPhysiciansinChinaCEMpolicyandcreditsystemMajorissuesofCMEactivitiesAccreditationcriteriafornationalCMEcourses
TableofContents
10
ThedevelopmentofthemedicalinsurancesysteminChina
• 1950s- 1970s:1
– Halfabillionpeople– Mostofthemareyoung– 36%agelessthan15– 80%rural– 1/3Illiterate– Livingabsolutelyinpoverty– Ruralresidenceshaveaccesstobasichealthservicesundercooperativemedicalschemes– Urban:workunitbasedhealthinsuranceeitherthroughtheLabor InsuranceSystemortheGovernmentInsurance
System
• 1980s– 1990s:– Urbanarea:implementationofuserfeesaspublicfundingdeclined– Ruralarea:thedissolutionofruralcooperativesandassociationofcooperativemedicalschemeswiththeradicalism
oftheCulturalRevolutioncausedinsurancecoveragelevelsinruralareastodrop to7%ofcountiesby1999– ThemajorityofChina’spopulationdidnothavehealthinsurancebetween1980and2000– Supply-sidesubsidiestypicallycovered lessthan10%ofproviderexpenses,withtheremainderearnedthroughfee-
for-servicepaymentfromuninsuredpatients.
• Nowadays:– Apopulation of1,3397bnby2010
• Aging:13,3%overage60andonly16,6%belowage15• Half(49,7%)urban;96%literate
Demographicchange:
11
ThedevelopmentofmedicalinsurancesysteminChina
• ThetransitionofdiseaseburdeninChina– China’s primaryburdenofdisease hasshifteddefinitively frominfectious tochronicnon-
communicable disease– However,theburdenforsome infectiousdiseases suchasTBremainslarge– Cancer,heartconditions andcerebrovasculardiseases arenowtopkillers
– Hypertension istheleadingpreventablerisk factorforprematuremortalityinChina,accountingfor2,33deathsin2005
– Byin2007– 2008,theage-standardizedprevalenceofdiabetesamongadultsinChinawas9,7percent,withthemajorityofpatientsundiagnosed anduntreated
– China’s healthsystemfacesthechallengeoftransitioningfromfocus onacutecareandcontrolofcommunicable diseasetoasystemsupporting preventionandcost-effectivemanagementofchronicdisease
12

UniversalHealthcare
InsuranceSystem
UrbanResidence UrbanWorkers RuralResidence OtherHealthcareInsurance
OverviewofChina’sUniversalHealthcareInsuranceSystem
Population Coverage:237million
Population coverageratein2010:97%
Targetpeople: Urbanworkersandretiringworkers
Population coverage:194million
Population coverageratein2010:97%
Targetpeople:Children,students,unemployedurbanresidence
Population coverage:836million
Population coverageratein2010:95%
Targetpeople: farmers
Population coverage:2600million
Population coveragerate:100%
Targetpeople:civilservantsandsoldiers
13
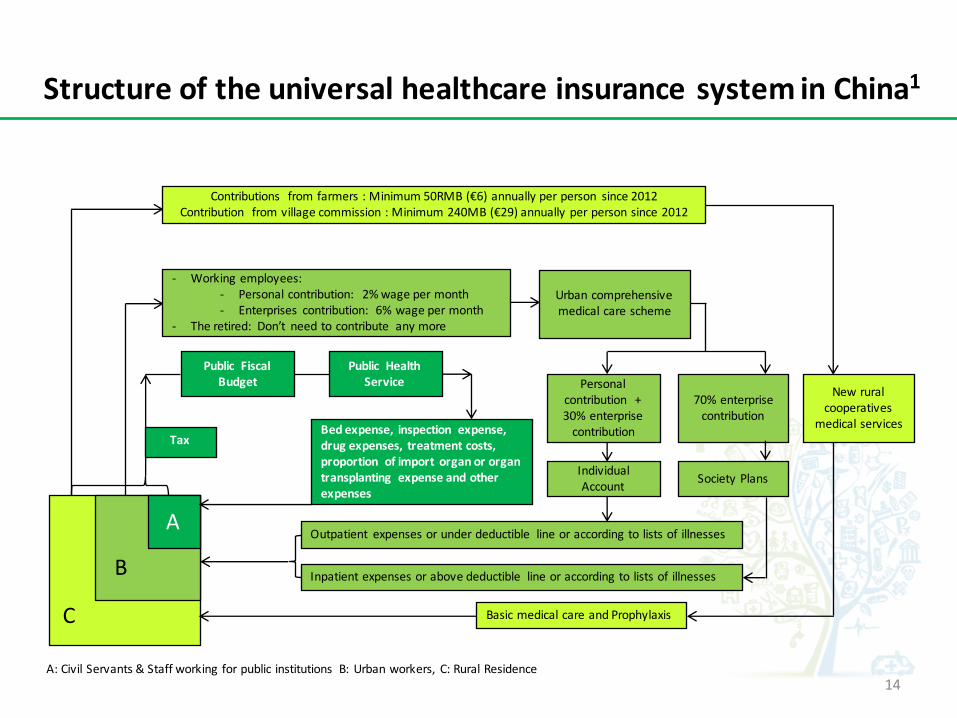
StructureoftheuniversalhealthcareinsurancesysteminChina1
A
Tax
Public FiscalBudget
Public HealthService
Bedexpense,inspection expense,drugexpenses,treatmentcosts,proportion ofimport organororgantransplanting expenseandotherexpenses
- Workingemployees:- Personalcontribution: 2%wagepermonth- Enterprises contribution: 6%wagepermonth
- Theretired: Don’t needtocontribute anymore
Urbancomprehensivemedicalcarescheme
Personalcontribution +30%enterprisecontribution
70%enterprisecontribution
IndividualAccount SocietyPlans
Outpatient expensesorunderdeductible lineoraccordingtolistsofillnesses
Inpatientexpensesorabovedeductible lineoraccordingtolistsofillnesses
Contributions fromfarmers:Minimum50RMB(€6)annuallyperperson since2012Contribution fromvillagecommission:Minimum240MB(€29)annuallyperpersonsince2012
Newruralcooperatives
medicalservices
BasicmedicalcareandProphylaxis
B
C
A:CivilServants&Staffworkingforpublicinstitutions B:Urbanworkers, C:RuralResidence14

HealthcareinsurancepoliciesinChina• Allthehealthcareinsurancefunds areadministratedbyprovincial governments,leadingtoanissue that
patientshavetopaybytheirownmoney forallhealthcarecostsandcannotgetimmediatereimbursement.Sometimes, thereimbursementacrossprovinces candelaybyseveralmonths.
• Thehealthcareinsurancepolicies varybycities,forexamplethethreshold oftheamountthatpatientscangetreimbursed.Itmainlydepends onthelocaleconomiccontext.
• Healthcareinsurancepolicies inBeijing:– Bothindustries andpublic organisationshavetopaythemedicalexpenses byindividuals untilthe
expenses reachathreshold (variesbytiersofthehospitals). Patientscangetreimbursementwhentheirmedicalexpenses areoverthisamount.
– ThepartofmedicalexpensescoveredbyUniversalhealthinsurancesystemwillbepaidbyhospitalsfirst.Andhospitalswillgetreimbursed afterwards.
HospitalTypes MedicalExpenses Individual InsuranceTier3 X- 10000 80% 20%
10000- 30000 85% 15%30000- 40000 90% 10%Over40000 95% 5%
Tier2 X- 10000 82% 18%10000- 30000 87% 13%30000- 40000 92% 8%Over40000 97% 3%
Tier1 X- 10000 85% 15%10000- 30000 90% 10%30000- 40000 95% 5%Over40000 97% 3%
Healthinsurancepoliciesforurban workersinBeijing
ThisisthehealthcareinsurancepoliciesforUrbanworkersinBeijing(GroupBinthegraphonthepreviouspage).However,thepercentageofreimbursementforthisgroupofpeoplemaybealittledifferentfromwhatitisshownhere.Thehealthinsurancepoliciestothepublicinstitutionworkersandcivilservantsaswellasthattoruralresidencesaredifferentfromthisone.
15

IntroductionofHealthcareMarketinChinaAnoverviewofthehealthcaremarketThehierarchyofthemedicalsystemPublichospitalsPhysicians’workconditionandsalariesOutpatientpatientconsultation
MedicalInsuranceSysteminChinaThedevelopmentofthesystemUniversalhealthcareinsurance
ContinuedMedicalEducationforPhysiciansinChinaCEMpolicyandcreditsystemMajorissuesofCMEactivitiesAccreditationcriteriafornationalCMEcourses
TableofContents
16
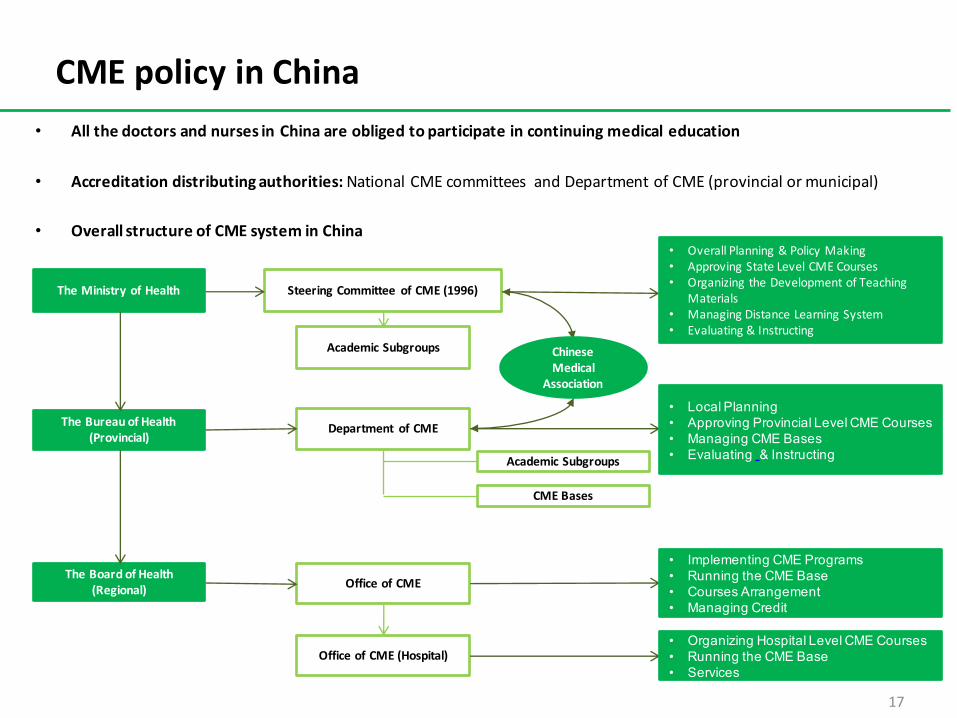
CMEpolicyinChina• All the doctors and nurses in China are obliged to participate in continuing medical education
• Accreditation distributing authorities:National CME committees and Department of CME (provincial or municipal)
• Overall structure of CME system in China
TheMinistryofHealth
TheBureauofHealth(Provincial)
TheBoardofHealth(Regional)
SteeringCommittee ofCME(1996)
AcademicSubgroups
Department ofCME
AcademicSubgroups
CMEBases
OfficeofCME
OfficeofCME(Hospital)
ChineseMedical
Association
• OverallPlanning&PolicyMaking• ApprovingStateLevelCMECourses• OrganizingtheDevelopmentofTeaching
Materials• ManagingDistanceLearningSystem• Evaluating&Instructing
• Local Planning • Approving Provincial Level CME Courses• Managing CME Bases• Evaluating & Instructing
• Implementing CME Programs• Running the CME Base• Courses Arrangement• Managing Credit
• Organizing Hospital Level CME Courses• Running the CME Base• Services
17

CMECreditSysteminChina
• According to the policy issued by Chinese National Health Commission, all doctors and nurses are obliged to earnat least 25 credits annually, including 5-10 credits in category I and 15 – 20 credits in category II. Doctors workingin health care organisations on provincial or municipal levels have to pass the exams and earn at least 10 creditsfrom CME programme on national level. Credits in Category I and Category II are not interchangeable.
• Credit Categories:– Category I:1. National CME programme: programmes assessed, authorized and published by national CME commission ;
programmes applied by national CME organisations and published by national CME commission.2. Provincial CME programme: programmes assessed, authorized and published by provincial CME
commission; programmes applied by provincial CME organisations and published by provincial CMEcommissions; programmes applied by the sub – associations of Chinese Medical Association, ChineseStomatological Association, Chinese Preventive Medicine Association, Chinese Nursing Association, ChineseHospital Association and ChineseMedical Doctor Association and authorised by the associations mentionedabove
3. Promotional programmes: programmes aiming at providing healthcare workers with professional trainingsdesigned for emergency events and other necessary trainings such as those on professional ethics in theindustry; programmes authorised by national health commission and provincial health commission.
– Category II: self – study, publishing medical papers, conducting medical researches and other academicactivities.
18
CMEcreditsysteminChina
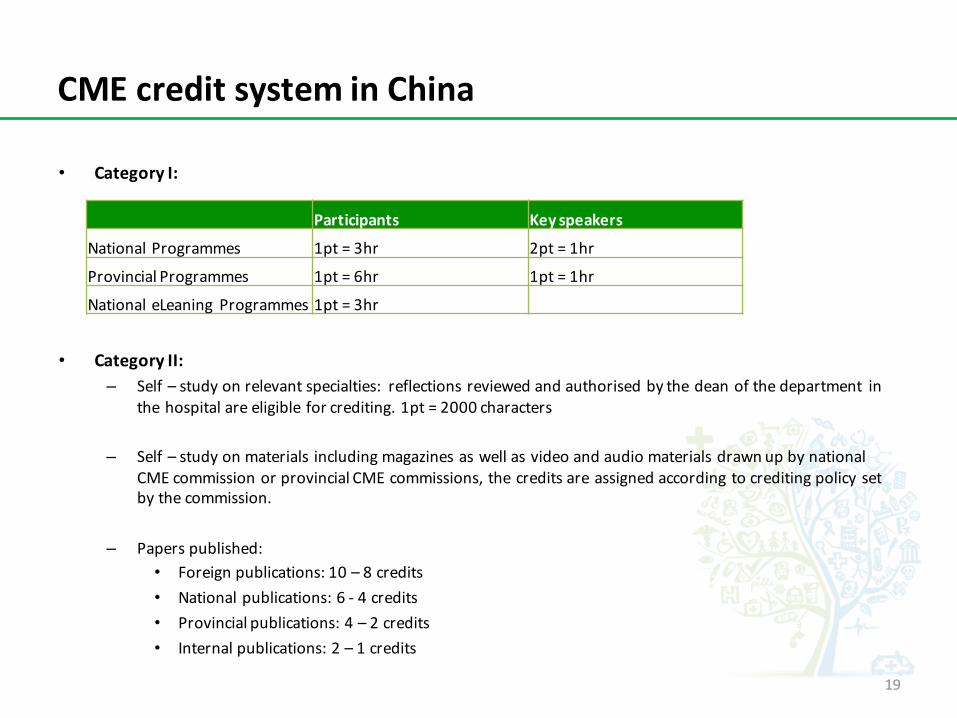
• CategoryI:
• CategoryII:– Self– studyonrelevantspecialties: reflectionsreviewedandauthorisedbythedeanofthedepartment in
thehospitalareeligibleforcrediting.1pt=2000characters
– Self– studyonmaterials includingmagazinesaswellasvideoandaudiomaterialsdrawnupbynationalCMEcommissionorprovincialCMEcommissions,thecreditsareassignedaccordingtocreditingpolicysetbythecommission.
– Paperspublished:• Foreignpublications:10– 8credits• Nationalpublications:6- 4credits• Provincialpublications:4– 2credits• Internalpublications:2– 1credits
Participants Keyspeakers
NationalProgrammes 1pt=3hr 2pt=1hr
ProvincialProgrammes 1pt=6hr 1pt=1hr
NationaleLeaning Programmes 1pt=3hr
19

CMEcreditsysteminChina
– Authorizedscientificmedicalresearches:creditswillbeassignedtoresearchersbasedontheirrankinginthescientificresearchesby theirresponsibilities:
• Nationalresearches:Ranking:1,2,3,4,5– Credits:10,9,8,7,6• Provincialresearches:Ranking:1,2,3,4,5– Credits:8,7,6,5,4• Municipalresearches:Ranking:1,2,3,4,5– Credits:6,5,4,3,2
– Publishmedicalliterarywork• Reportsoninternationalandnationalmedicalconferences:1pt– 3000characters• Publishmedicaltranslatingarticles:1pt– 1500characters
– Scientificconferences,instructiononoperationsandpromotionofnewtechnologiesorganisedbythehealthorganisationswherehealthworkerswork:(Participantscanonlybegrantedupto10ptsperyear)
• Speakers:2pt– 1time• Participants:0,5pt– 1time
– ClinicalPathologySymposium,casestudyorganisedbyseveraldepartments:(participantscanonlybegrantedupto10ptsperyear)
• Speaker:1pt– 1time• Participants:0,5pt– time
– HowcreditsassignedineLearningmedicaleducationisbasedon thespecificregulationsetbyprovincialormunicipalhealthcommissions.
• Authorisedmedicaltraininginsuperiormedicalorganisations(includingtrainingabroad)over6months:– Iftheconcerningpeoplepassallnecessaryexams,itisregardedthattheygetalltherequired25creditsintheyear.
20
CreditregistrationsanddistributionofCMEmedicalcertificates
• Credits registrations:– The organisers of the programmes grant credits to the participants. Participants’ working organisations are
responsible for registration.– Provincial and municipal health organisations are responsible for printing and distributing the CME
registration cards or implementing the electronic information system, both of which should include the CMEprogramme number, data, name of the programme, entities of the concerning organisations, credits, resultsas well as the corporate stamps. The registration cards should be under the management of physicians ornurses themselves and could be used as the proofs for their enrolment of the CME activities.
– Organisations responsible for CMEs should make a record of participants’ performance and the total numberof credits they earn. This record should be taken as one of the most important criteria in the annualappraisal. The qualification of CME should be the prerequisites amid of the recruiting, promotion, and re-registration.
• Supervision on credits registrations:– Certificates to national and provincial CME programmes are made respectively by national or provincial CME
committees. Authorized associations or organisations could also make such certificates, but based on theformat regulated by the national CME committee.
– Regarding the certificates to Distance Learning of CME in category I, organisers should first provideparticipants with relevant learning materials. After the materials have been evaluated by the Department ofCME on provincial level, the Department could grant the certificates to the concerning participants.
– The CME activities, which are organised on national level or by the authorized associations and arepublished by the national health commission, should be under the supervision of the Department of CME inthe particular province where the events are held. The organisers are obliged to report the CME materials tothe Department. 21

CMEcoverageinChina
• ThecoveragerateofCMEhasreached85%by2010,successfullyachieving thegoalofthe11th 5-yearnationalplaninChina.Itisexpected thatthisratewillreach100%by2015accordingtothe12th 5-yearnationalplan.1
• It is also expected that the rural doctors’ pass rate in CME could reach 80% by 2015, and this ratecould reach 70% for those in remote rural areas or in western part of China.
• Untiltheendof2011,therewereupto750,000 healthworkersareenrolled intothenationalDistanceLeaning2 CMEprogrammes.Alongsidethenationalprogrammes,over3,000,000healthworkersparticipate intotheprovincialormunicipalDistanceLeaningCMEactivities.3
• According to a survey, 95% of clinical health workers say that Internet CME is the most preferredway for them to get involved into the CME activities. 3
• To develop Distance CME activities in China:– Only five units are licensed by the Chinese Ministry of Health for the Distance Learning of
CME. (National Level of distance CME activities)4
– Credits earned on Internet CME websites that are authorised on provincial or municipal levelmay be authenticated in other provinces or cities.
70%
80%
90%
100%
Y2010 Y2015
85%
100%
22

DistanceCMEactivities
• InternetCMEcourses• Satellitetransmission
23

618
554
357
224
203
137
118111
110
92
85
834 4
0
GeographyDistributionof CMECourses,2009
MajorissuesofthecurrentCMEsystems– ImbalanceDevelopmentAmongDifferentProvinces
24
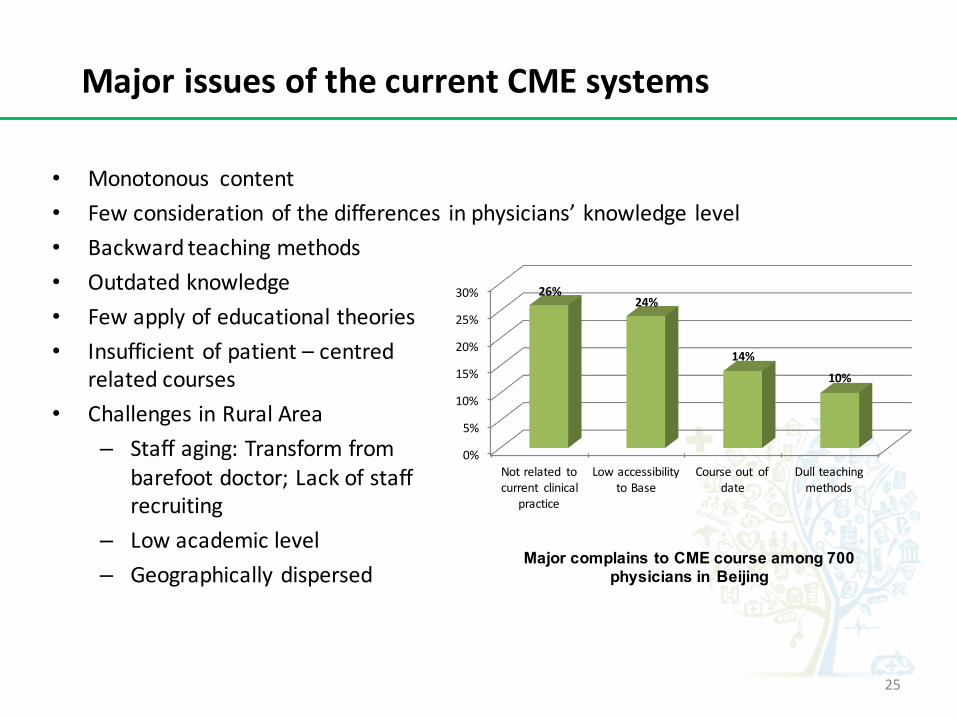
MajorissuesofthecurrentCMEsystems
Major complains to CME course among 700 physicians in Beijing
• Monotonous content• Fewconsiderationofthedifferences inphysicians’knowledge level• Backwardteachingmethods• Outdatedknowledge• Fewapplyofeducationaltheories• Insufficientofpatient– centred
relatedcourses• ChallengesinRuralArea
– Staffaging:Transformfrombarefootdoctor;Lackofstaffrecruiting
– Lowacademiclevel– Geographicallydispersed
0%
5%
10%
15%
20%
25%
30%
Notrelated tocurrent clinical
practice
LowaccessibilitytoBase
Courseout ofdate
Dullteachingmethods
26%24%
14%
10%
25

AccreditationcriteriafornationalCMEcourses• TheprerequisiterequirementstoapplyforthenationalCMEcourses(thecoursesmustfulfiloneofthe
requirementsbelow):CategoryICMEcourses– Courses introducethemostadvancedinthefieldwithChinaoraroundtheglobe– Thelatestprogressofinterdisciplinary– Theintroduction andthepublicisation oftheadvancedinternationaltechnology orresearchresults;
Ortheintroductionandpublicisation oftheadvancedtechnology orresearchresultsinChina.– Trainingandprogrammesdesigned forcopingwiththepublichealthemergenciesorfulfilling thekey
demands emergedamidtherevolutionary developments oftheChinese healthsystem.– Courses couldcompensatefortheblankinafieldinChinaandfocusesonatechnologyormethod
thatcouldgeneratesignificantsocialandeconomicbenefits
• Eligibility forcandidatestoapplyfordevelopingthenationalCMEcourses– Healthmedical,educationalandscientificorganisationscould applyfordeveloping thenationalCME
coursesbyfollowing theapplicationprocedure.Otherorganisationshavetofirstgettheapplicationeligibility firstfromtheNationalCMECommittee.
– PeopleinchargeofthenationalCMEcoursesshould haveDeputySeniorprofessional positions. Theprogrammesforwhichtheyareresponsible should berelatedtotheirspecialties.Oneperson canapplyforatmost2nationalCMEcourses underhis/her chargeinthesameyear.
26
AccreditationcriteriafornationalCMEcourses• ProceduretoapplyforthenationalCMEcourses
– TheorganisationshouldfirsthandintheapplicationformstotheprovincialormunicipalCMEcommittees.Aftertheassessment, theprovincialormunicipalCMEcommittees willrecommendtheCMEprogrammestonationalCMEcommittees.
– AssociationsalreadyhavingthequalificationstoapplyforthenationalCMEcourses,suchasChineseMedicalAssociation,ChineseStomatological Association,ChinesePreventativeMedicineAssociation,ChineseNursingAssociation,ChineseHospitalAssociation,ChineseMedicalDoctorAssociationandtheCMECommittee ofHealthofMinistry,shouldhandintheirproposalsofthenextyearCMEcoursestoNationalCMECommittee; TheaffiliatedorganisationsofNationalHealthCommissionshoulddirectlyapplyforthenextyearCMEcoursestoNationalCMECommittee.
– ProgrammesinitiatedbyNationalCMECommittee, NationalHealthandFamilyPlanningCommissionofPRCintheneedforthepublichealthemergencies andrevolutionarydevelopmentforChinesehealthsystemshouldbedirectlyappliedtoNationalCMECommittee.
– Theeligibilityfortheaccreditation ofthenationalCMEcoursesis2– year.Ifthecoursesareheldinthesecondyear,theorganisershouldhandinanapplicationtonationalCMEcommittee inordertoreservetheireligibilitytoorganisethecourseinthenextyear.
– Theapplicationtime forallnationalCMEcoursesisbetween JulyandSeptember.Theorganisershouldfillintheapplicationformandapplyfortheeligibilitytoconductthecoursesaccordingtotheapplicationprocedure.
• Accreditation– NationalCMECommittee andNationalHealthandFamilyPlanningCommissionwillreviewandpublishthe
accreditationresults.– NationalCMECommitteewillpublishtheresultsoftheaccreditednationalCMEcoursesfromtheendofthe
yeartoFebruaryinthenextyear.
27

AccreditationcriteriaasanorganisationtoprovidenationaldistanceCMEactivities• Theprerequisiterequirements
1. Theorganisationmusthaveacquiredtheauthorizationoftherelevantgovernmentaldepartmentstoworkinthefieldofreportinghealthrelatedinformation.
2. Haveatleast2yearexperiencetodevelopandorganiseonlineCMEcourses3. TheCMEsystem(developingsystem,educationoperationalsystem,learningsupport
system,educationmanagementsystem,internalqualityassurancesystem)isalreadyestablishedandundertheoperation.
4. Theorganisationhasenoughresourcestomeettheeducationdemands.Theorganisationshouldpossess theonlinemedialibrary,coursewarelibrary,questionbank,andlearning– materialdatabase.
5. Possessateamofeducationalstaffwithdifferentexpertise,includinginstructors,tutors,editorsanddevelopers.
6. ThedistanceeducationplatformshouldbeabletoadapttothecontinuingdevelopmentneedsofCME,possessoptimisedtechnology,andeffectivelydeveloptheinteractiveteachingmethod.
• Applicationtime– Eachyear,candidatesshouldhandintheapplicationsfrom1Marchto15Maytothe
NationalCMEDistanceEducationalCentre.
28
• AccreditationProcedure– Theassessmentofthecandidateswillbeorganisedonceeveryyearandtheprocedure
includesmaterialaudit,siteevaluationandresultverification.1. MaterialAudit:applicationsareregardedasinvalidinthesituationsbelow
• Itisimpossibletohaveaknowledgeofcandidateorganisation’sbasicsituation,orthecandidateorganisationsdon’tfulfilwillalltheprerequisiterequests
• Theapplicationmaterialsaredifferentfromtheproofmaterials2. Siteevaluation
• Theministryofhealthwillsendprofessionalstotheorganisationstoevaluatetherealsituation.
3. Resultsverificationa) TheNationalCMEDistanceEducationCentrewillpublishtheorganisationsthat
havesuccessfullypassedtheassessment.AndtheorganisationcanacquireboththeeligibilitytoapplyandorganisethedistanceCMEactivities.
b) Organisationsnotpassingtheassessmentdon’thavetheeligibilitytoapplyfortheNationalDistanceCMEactivities.
c) Organisationsnotpassingtheassessmenthavetoreapplyfortheeligibilityafteroneyear.
29
AccreditationcriteriaasanorganisationtoprovidenationaldistanceCMEactivities


















