
©AMSP 20081 Suicidal Behavior, Alcohol, and Alcohol Use Disorders Timothy W. Lineberry, M.D....
38
©AMSP 2008 1 Suicidal Behavior, Alcohol, and Alcohol Use Disorders Timothy W. Lineberry, M.D. Assistant Professor, Psychiatry Mayo Clinic
-
Upload
louisa-warner -
Category
Documents
-
view
223 -
download
0
Transcript of ©AMSP 20081 Suicidal Behavior, Alcohol, and Alcohol Use Disorders Timothy W. Lineberry, M.D....
©AMSP 2008 1
Suicidal Behavior, Alcohol, and Alcohol
Use Disorders
Timothy W. Lineberry, M.D.
Assistant Professor, Psychiatry
Mayo Clinic

©AMSP 2008 2
US Prevalence Suicidal Behavior
%/yr #/yr
Thoughts 3.3 9,900,000
Attempts0.6
(4.6 Lifetime)
1,800,000
(13,800,000)
Suicide ~ 0.01 >32,000

©AMSP 2008 3
%/yr
(Lifetime)
#/yr
(Lifetime)
Hazardous 25 75,000,000
Abuse5
(18)
15,000,000
(54,000,000)
Dependence4
(13)
12,000,000
(39,000,000)
US Prevalence Alcohol Use Disorders

©AMSP 2008 4
This Lecture will Cover
• Definitions
• Relationship
• Screening & identification
• Assessment & management
©AMSP 2008 5
Hazardous Drinking
• Men 5 drinks/day or 15 drinks/week
• Women 4 drinks/day or 8 drinks/week
• “At risk” for alcohol-related problems
• NOT alcohol abuse or dependence
©AMSP 2008 6
Alcohol Abuse
– 12-month pattern of problems in 1 of:
• Inability to meet obligations
• Physically hazardous situations
• Legal problems
• Social or interpersonal problems
– Not alcohol dependence

©AMSP 2008 7
Alcohol Dependence
• 12-month pattern of problems in 3 of:
– Tolerance: use = same effect– Withdrawal: Use to relieve/avoid withdrawal– Use larger amounts/longer than intended– Desire to or unsuccessful efforts to cut down time spent in alcohol-related activities– Give up important social activities– Continued use despite persistent problems

©AMSP 2008 8
Major Depressive Disorder (MDD)
• MDD lifetime prevalence: ♀ 15%: ♂ 8%
• Must represent change in function
• Subjective report or observation of others
• > 5 symptoms nearly daily for 2-weeks
• Must have at ≥ 1 of following 2
1. Depressed mood most of the day
2. ↓ interest/pleasure in most activities
©AMSP 2008 9
Additional MDD Criteria
• Weight ↓ or ↑ or appetite ↓ or ↑
• Sleep ↓ or ↑
• Psychomotor agitation or retardation
• Fatigue or ↓ energy
• Feelings of worthlessness or inappropriate guilt
• ↓ Ability to think/concentrate or indecisiveness
• Recurrent SI or thoughts of death
©AMSP 2008 10
Suicide-related Behavior
• Ideation = thoughts of
• Attempt = deliberate self-harm
• Completion = death from attempt

©AMSP 2008 11
This Lecture will Cover
• Definitions
• Relationship
• Screening & identification
• Assessment & management
©AMSP 2008 12
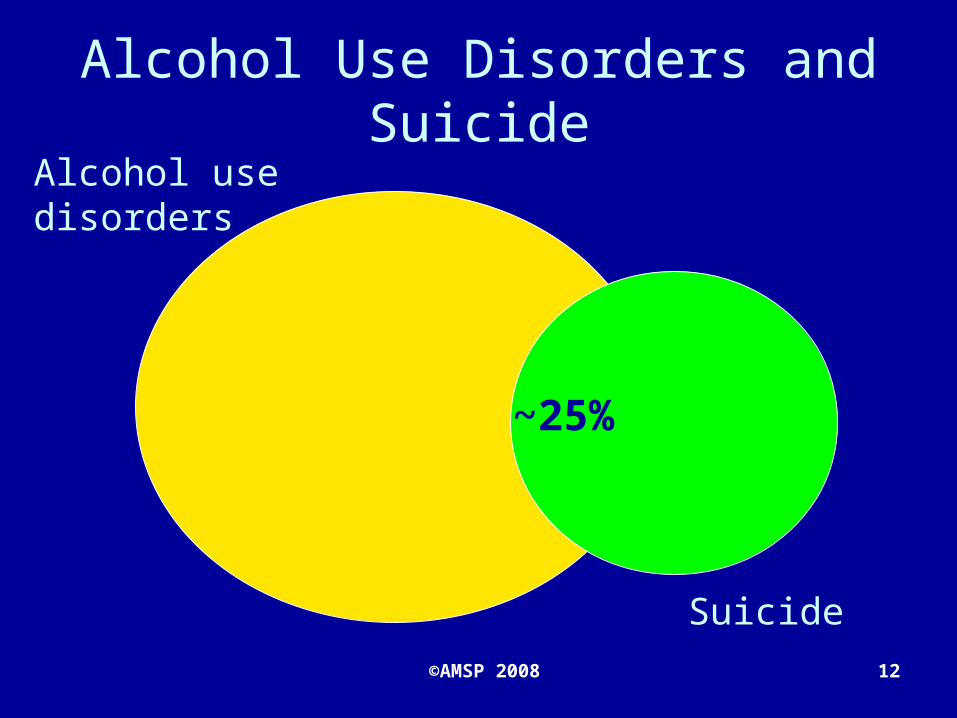
Alcohol Use Disorders and Suicide
Alcohol use disorders
Suicide
~25%

©AMSP 2008 13
Alcohol Dependence and Suicide
• Suicidal ideation ↑ 3-5X
• Suicide attempts ↑ 4-6X
• Lifetime suicide rate 7-10%
©AMSP 2008 14
Major Depression
• ~40% of suicides have MDD• 20% with MDD attempt in lifetime • Lifetime suicide rate varies with
severity of depressive illness–Psych. hospitalized + SI: 9%–Hospitalized without SI: 4%–Outpt. depression: 2%

©AMSP 2008 15
Depression and suicideDepression
Suicide
~40%

©AMSP 2008 16
Which came First?
• 80% of patients with alcohol dependence report lifetime depressive symptoms
• Sustained heavy alcohol use induces depressive symptoms

©AMSP 2008 17
“Independent” MDD
• Predates alcohol dependence diagnosis or occurs in times of sustained abstinence
• More likely to have family history of MDD
• 15% of alc dependence patients

©AMSP 2008 18
Alcohol Induced MDD
• Temporary sxs associated with use
–Typically resolve in ~ 4 weeks
• Resolve with sustained abstinence
• Family history of MDD less likely
• 26% of alc dependence patients

©AMSP 2008 19
Alcohol Dependence and MDD
MDDAlcohol Dependence
Alcohol Induced 26%
Independent 15%

©AMSP 2008 20
Depression + Alcohol Dependence
Suicide rate
• Independent depression ↑ suicide attempt rate vs. alcohol induced
• Increasing age risk for both
• Depression and alcohol use disorder make up ~65% of all suicides
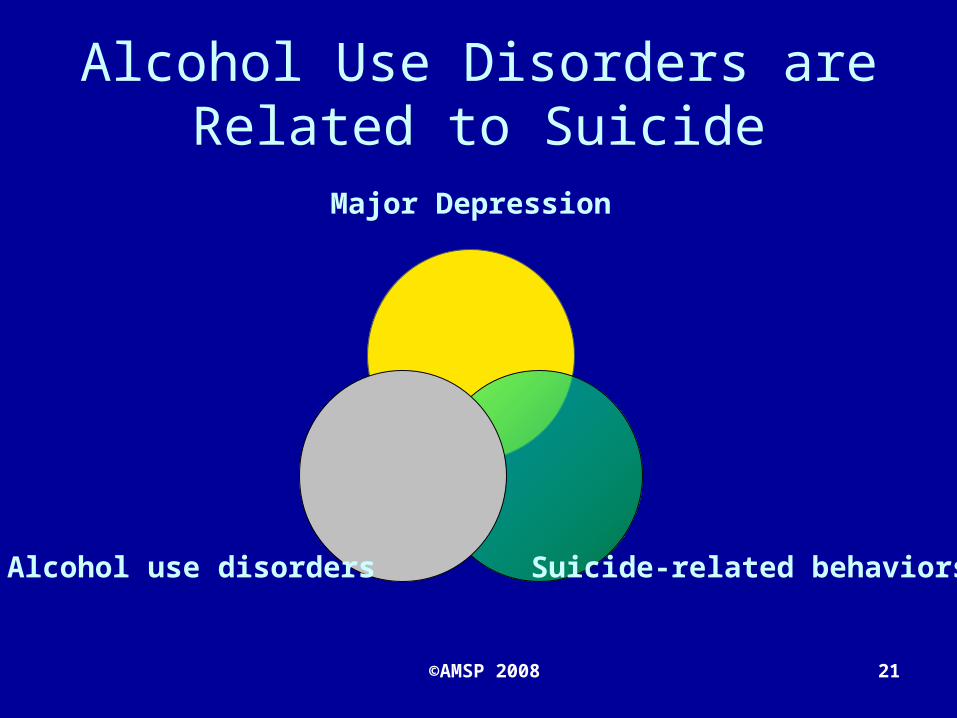
©AMSP 2008 21
Major Depression
Suicide-related behaviorsAlcohol use disorders
Alcohol Use Disorders are Related to Suicide
©AMSP 2008 22
This Lecture will Cover
• Definitions
• Relationship
• Screening & identification
• Assessment & management
©AMSP 2008 23
Ask Everyone!
• <25% patients routinely screened for alcohol use
• ~ 40% with MDD missed by primary MD
• 35% with known MDD asked about suicide
• MDs report discomfort with asking
• MDs miss obvious clinical patterns
©AMSP 2008 24
Patients Expect
• To be asked about alcohol use
• To be asked about emotional problems
• Guidance about use and risky behaviors
• Judge MD skill based on their attention to

©AMSP 2008 25
Evidence Based Screening
• Screening ≠ diagnosis• Screening tools include
– History– Survey– Physical exam– State markers (laboratory)
• + Screen requires full evaluation

©AMSP 2008 26
CAGE
• Cut down, Annoyed, Guilt, Eye-opener
• Positive test > 2 yes answers • Sensitivity → 50-80%• Specificity → ~ 80%• Doesn’t screen for hazardous
drinking
©AMSP 2008 27
AUDIT
• 10-item survey
• Developed by W.H.O.
• Score of > 8 = positive test for hazardous drinking/ ↑ chance of alc. dx
• Sensitivity → ~70%
• Specificity → 80%
• 3-item survey
• Sensitivity/specificity
= to 10-item AUDIT
• Positive score
– Men > 4
– Women ≥ 3
AUDIT-C
©AMSP 2008 28
Physical Examination
3 drinks/day risk of hypertension
Hepatosplenomegaly (liver/spleen size
)Peripheral neuropathy: 15% w/alc
dep
©AMSP 2008 29
State Markers
• Blood tests
• Change with heavy sustained alcohol use
– Gamma-glutamyl transferase (GGT)
– Carbohydrate Deficient Transferrin (CDT)
– CBC w/Mean Corpuscular Volume (MCV)
– Aspartate transaminase (AST)

©AMSP 2008 30
2 Question Depression Screening
• In the past month… 1. Have you been bothered by feeling
down, depressed, or hopeless? 2. Have you been bothered by little
interest/pleasure in doing things?• ≥ 1 yes = positive test• Sensitivity: 96%; specificity: 57%• Remember! screening ≠ diagnosis
©AMSP 2008 31
This Lecture will Cover
• Definitions
• Relationship
• Screening & identification
• Assessment & management
©AMSP 2008 32
Manage At Risk Patients
Positive screenHistory, survey, physical exam, state markers
Full evaluation
Use diagnostic criteria
Evidence-based treatments

©AMSP 2008 33
Define MDD in Alcohol Use
Timeline interview
Carefully assess lifetime MDD sxs
Sxs present w/sustained abstinence?
Family history of depression?
©AMSP 2008 34
Evidence Based Treatments
• Motivational Interviewing
• Cognitive Behavioral Therapy
• Disulfiram
• Naltrexone
• Acamprosate

©AMSP 2008 35
SAFE-T Suicide Risk Assessment
Risk factors
Protective factors
Suicide inquiry
Assess risk & level of care
Document
©AMSP 2008 36
Intent
Plan
Suicidal ideation
Thoughts of death
Hopelessness
Stepwise assessment
©AMSP 200841

©AMSP 2008 37
Assess Risk and Level of Care
• Clinical judgment
• Low risk → outpt follow-up
• Moderate → psychiatry/ER
• High → hospitalization
©AMSP 2008 38
Summary
• Definitions
• Relationship
• Screening & identification
• Assessment & management


















