Am J Clin Nutr 1978 Jelliffe 492 515
24
perspectives in nutrition 492 The American Journal of Clinical Nutrition 31: MARCH 1978, pp. 492-515. Printed in U.S.A. The volume and composition of human milk in poorly nourished communities A review1 Derrick B. Jelliffe and E. F. Patrice Jelliffe “How is it that poor men’s wives, who have no cold fowl or port wine on which to be coshered up, nurse their children without difficulty, whereas the wives of rich men, who eat and drink everything that is good, cannot do so, we will for the present leave to the doctors and mothers to settle between them.” Anthony Trollope (1847) The question of the composition and vol- ume of breast milk produced by mothers on different planes of nutrition at different phases of lactation is a major issue in pedi- atnic public health in the world, especially in resource-poor countries. Fundamentally, ultimate concerns are the nutritional adequacy of such milk for young infants in relation to calories, proteins, vi- tamins, and minerals, and the physiological and practical efficacy of supplementing the maternal on infant diets, when or if neces- sary. However, it must be stressed that infant feeding cannot be considered in relation to the dietary supply of nutrients alone, but rather in an ecological context. For exam- ple , with regard to breast feeding in less developed countries, the nutritional and health consequences of the prevention of diarnheab disease , the lactation contracep- tive phenomenon, and the economic and agnonomic considerations have to be borne in mind at the same time (77). Conversely, for the majority of the world, breast feeding cannot only be compared with adequate feeding with cow’s milk - that is with sufficient formula available and with reasonable home hygiene. From a practical point-of-view, it is more usually a comparison of breast feeding and formula feeding as they exist in the nutritional, hy- gienic, and economic circumstances usually found in villages and urban shanty towns in resource-poor, less developed countries, mainly in the subtropics and tropics (77). Considerations of the volume and com- position of breast milk in poorly nourished communities can only be made in relation to other ecological circumstances affecting both mother and baby (66, 77). However, this paper attempts to draw together the main relevant information from different parts of the world, in which widely varying cultural, genetic, economic, and nutritional circumstances prevail. Differences, when they exist, may be related mainly to nutri- tion, to physical overwork and/or to en- vironmental psychosocial stress. Other van- abbes such as maternal parasitic diseases and genetic physiological differences may be more relevant than presently appneci- ated. Variations in results in different stud- ies are difficult to interpret, especially those of minor degree, because of dissimilarities in times and methods of sampling and anal- ysis, in types and levels of maternal under- ‘From the School of Public Health, University of California, Los Angeles, California 90024. by guest on June 21, 2011 www.ajcn.org Downloaded from
-
Upload
mohammad-arshi-khan -
Category
Documents
-
view
19 -
download
4
Transcript of Am J Clin Nutr 1978 Jelliffe 492 515

perspectives in nutrition
492 The American Journal of Clinical Nutrition 31: MARCH 1978, pp. 492-515. Printed in U.S.A.
The volume and composition of human milk inpoorly nourished communitiesA review1
Derrick B. Jelliffe and E. F. Patrice Jelliffe
“How is it that poor men’s wives, who have no cold fowl or port wine on which to be
coshered up, nurse their children without difficulty, whereas the wives of rich men, who eatand drink everything that is good, cannot do so, we will for the present leave to the doctorsand mothers to settle between them.”
Anthony Trollope (1847)
The question of the composition and vol-ume of breast milk produced by mothers ondifferent planes of nutrition at differentphases of lactation is a major issue in pedi-atnic public health in the world, especiallyin resource-poor countries.
Fundamentally, ultimate concerns are thenutritional adequacy of such milk for younginfants in relation to calories, proteins, vi-tamins, and minerals, and the physiologicaland practical efficacy of supplementing thematernal on infant diets, when or if neces-sary.
However, it must be stressed that infantfeeding cannot be considered in relation tothe dietary supply of nutrients alone, butrather in an ecological context. For exam-ple , with regard to breast feeding in lessdeveloped countries, the nutritional andhealth consequences of the prevention ofdiarnheab disease , the lactation contracep-tive phenomenon, and the economic andagnonomic considerations have to be bornein mind at the same time (77).
Conversely, for the majority of the world,breast feeding cannot only be comparedwith adequate feeding with cow’s milk -
that is with sufficient formula available andwith reasonable home hygiene. From apractical point-of-view, it is more usually a
comparison of breast feeding and formulafeeding as they exist in the nutritional, hy-gienic, and economic circumstances usuallyfound in villages and urban shanty towns inresource-poor, less developed countries,mainly in the subtropics and tropics (77).
Considerations of the volume and com-position of breast milk in poorly nourishedcommunities can only be made in relationto other ecological circumstances affectingboth mother and baby (66, 77). However,this paper attempts to draw together themain relevant information from differentparts of the world, in which widely varyingcultural, genetic, economic, and nutritionalcircumstances prevail. Differences, whenthey exist, may be related mainly to nutri-tion, to physical overwork and/or to en-vironmental psychosocial stress. Other van-abbes such as maternal parasitic diseasesand genetic physiological differences maybe more relevant than presently appneci-ated. Variations in results in different stud-ies are difficult to interpret, especially thoseof minor degree, because of dissimilaritiesin times and methods of sampling and anal-ysis, in types and levels of maternal under-
‘From the School of Public Health, University ofCalifornia, Los Angeles, California 90024.
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

ri;u ProcIs.ocin�
Alveokts
lldk �Alveoko,
VOLUME AND COMPOSITION OF HUMAN MILK 493
nutrition, and in degrees of environmentalpsyshosocial stress.
Methods
Recent work has reemphasized the possibility ofvery considerable variations in findings as a result ofusing different biochemical methods . This is particu-
larly so with regard to protein (91).The actual obtaining of representative samples of
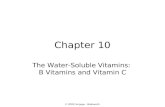
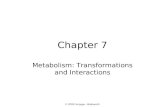
human milk poses unique problems as the normaldestination is the baby’s stomach and not a test-tubeor laboratory container. The ejection of breast milk ismediated by the psychosomatic let-down reflex (Fig.1). Milk production is proportional to the secretion ofanterior pituitary hormone , prolactin , resulting fromnipple stimulation (“prolactin reflex”) (Fig. 2), and tothe degree of intra-alveolar tension, related to empty-ing. Methods used must , therefore , avoid interferingwith normal mechanisms as much as possible, but infact, all do so considerably. As Hytten (48) noted,“the sucking of a baby has, for the mother, psycholog-ical overtones beyond the mere local stimulation ofthe areola and nipple; and the mechanical replacementof this local stimulus cannot hope to be an entirelyeffective substitute for the baby”.
Diurnal variations in milk volume and compositionhave been noted (50, 104, 105). The invariable andconsiderable difference in fat content between fore-and hind-milk (1 to 2 g/100 ml) means that the time ofsampling during a feeding can be significant.
In addition, in some areas of the world, seasonalvariation has been noted - for example, lower levels ofascorbic acid in the “hungry season” in parts of Africa(130). Such seasonal changes have long been recog-nized by dairy farmers. The stage of lactation is anothervariable, as is frequency, intensity and duration of
FIG. 1 . Letdown reflex: the key to successful lac-
tation. Sucking stimulation on the breast generates
nerve impulses that pass to the posterior pituitarythat secretes oxytocin . This passes via the bloodstreamto the breast, where it acts on the myoepithelial cells,surrounding the milk-containing alveoli, causing theircontraction. This expresses the milk from the alveoliinto the lacteals. The sequence is also known as the“milk ejection reflex.” Importantly, it can be inhibitedby anxiety (Fig. 3) and enhanced by confidence.
FIG . 2 . Prolactin reflex . Sucking stimulation onbreast generates nerve impulses which pass to the an-tenor pituitary, which secretes prolactin. This is car-ried in the bloodstream to the breast , where it acts inthe alveoli causing milk secretion . The prolactin pro-duced is proportional to the amount of sucking stim-ulus.
nipple stimulation (and reflex prolactin secretion).Important reducers of such stimulation are comple-mentary bottle feeds (allaitement mixte) and the early
introduction of semisolid foods.
Likewise , questions of total ouptut are often basedon day-time estimations. In fact, in traditional cultures,the baby sleeps by the mother’s side and must obtainconsiderable quantities as “night feedings” (A . Omo-
lulu, personal communication).Two methods can be used to try to measure the
volume produced - test feeding and expression (48):
Test feeding (test weighing)
In this venerable technique, the baby is weighedbefore and after each feeding. Difficulties are numer-ous and obvious. Results depend on the vigor of the
infant and the success of the mother-baby interaction.To ensure larger, more measurable samples, it may beconsidered preferable for mothers to nurse their babiesat prescribed intervals rather than on demand - asunder nonexperimental conditions at home . Expensive,
accurate scales are required to measure relatively smallweight increases in an uncooperative infant . There isconsiderable likelihood of interference with the emo-
tionally-sensitive let-down reflex in the unnatural, anx-iety-producing circumstances and embarrassment inev-itably created by the investigation, which often have
been carried out in hospitals. Practically, there may bea need for continuous surveillance to ensure that nofeeding takes place between weighings, and, as notedearlier, ideally this should be on a 24-hr basis, which isalmost never possible.
Expression
Milk may be expressed from the breast manuallyand by some form of mechanical or electrical pump.These methods can be used to estimate total output,and, of course, are required if samples are to beobtained for analysis.
The same difficulties exist as with test feeding.Indeed , anxiety can be greater with expression , espe-cially with an unfamiliar, uncomfortable apparatus,
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

494 JELLIFFE AND JELLIFFE
possibly combined with concern over feeding the baby
later with the expressed milk. Also, the influence of
expression on prolactin secretion , compared with suck-ling by the baby, is unknown.
Results
Comparative results have varied in differ-ent studies. In some, expression has givengreater volumes; in others, test weighing.Sometimes daily outputs have been calcu-bated from the amount obtained at onefeeding only. In all cases, it is apparent thatresults are only approximations.
Maternal nutrition
Comparisons are also made more difficultby variables in the nutritional status ofmothers, both between mothers in a partic-ubar group and between various communi-ties, and by the possibilities of differentdegrees of adaptation (53). The nutrientsinvolved, the degree and duration of depri-vation, methods of nutritional assessment,and the previous nutritional situation andstores can have many and varying combina-tions. There may, for example, be consid-enable difference between the nutritionalpast and present histories in poorer womenin Sao Paobo, Brazil, (106a) in Ibadan, Ni-genia (8-12), and in Southern India (37).
An aspect of the situation about whichnothing is known is the effect of the nutri-tional status of the pregnant mothers to-
wards the end of gestation on the sensitive,developing mammary glands of the femalefetus (89).
More directly, the physiological weightgain in pregnancy, about one-third due todeposition of subcutaneous fat (“lactationstores”2) ; can vary considerably from the1 2 .5 kg suggested for Western women to 5
kg (or even weight boss) reported in poorlyfed communities (53) . Dietary inadequacyin pregnancy may sometimes be compli-cated by associated hard work and by re-stnictive food customs. However, culturallydefined customs or physiological adjust-ments may bead to less energy expenditurein pregnancy and lactation.
Likewise, in all communities, lactationitself leads to weight loss. In very ill-fedmothers, this can sometimes be as much as7 kg after a year-even leading to thedevelopment of nutritional edema in very
poorly nourished women (4) . Recent stud-ies in Guatemala have suggested that fatloss may be the main mechanism by whichsuch mothers can continue to lactate (124a).
Many accounts from different parts ofthe world suggest that malnourished womenoften lactate with unexpectedly little clini-cabby obvious deterioration of their nutri-tional status. However, in recent years theremay be increasing evidence of shorter pe-nods of satisfactory lactation then previ-ously, at least in some parts of the world.The effect of maternal malnutrition may bepartly hormonal, with decreased secretionof cortisol and possibly prolactin (55a) . Cer-tainby the cumulative effects of sequentialreproductive cycles, including prolongedlactation, can bead to general “maternaldepletion,” as shown by progressive weightloss and a prematurely aged appearance(78 , 1 24a) . More specific nutrient deficien-cies may occur with repeated reproductivecycles - for example , an increasingly largegoiter, anemia, osteomalacia, or nutritionaledema (78).
Environmental psychosocial stress
Under-appreciated in the past has beenthe effect of environmental psychosocialstress from poverty and unemployment,from poor housing and crime , from ilbegiti-macy and family instability, and from cub-tural confusion and uncertainty on lactationperformance, probably manifested throughthe effect of anxiety on the bet-downreflex - and possibly on the secretion ofvarious hormones, such as contisob. This ismainly of concern in urban slums and shantytowns. Despite these differences, certaingeneral findings seem to be usual and enableprinciples to be suggested on which practicalaction can be based. These can be consid-ered under three headings-volume, com-position, and adequacy of breast milk inpoorly nourished communities.
Volume
Well-nourished mothers. To interpret theadequacy of yields of breast milk in mothers
2 An estimated average increase in body fat of 4 kg
(9 Ib) represents an energy store of some 35,000 kcal,
enough to subsidize lactation by nearly 300 kcal dailyfor 3 to 4 months (53).
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

TABLE 1Mean intake of breast milk in Swedish babies (1945).
TABLE 2Daily volume of breast milk in Swedish women (1975)
(91).
VOLUME AND COMPOSITION OF HUMAN MILK 495
in communities with defective nutrition, itis plainly important to compare results withthose from well-nourished communities.Unfortunately, such data are scanty, out-of-date , and difficult to compare because ofdifferences in technique and sampling, andbecause of recent back of interest in thewhole subject of lactation.
In scientific and international literature,the figure of 850 mb/day is usually quotedfor the volume of milk produced in the first6 months. However, review of the literatureof 20 to 25 years ago shows that this was anarbitrary estimate and selected as an easy-to-remember round number based on an“assumption” in 1950 in the United NationsCommittee on Calorie Requirements (34a).It has become sanctified by repetition insubsequent international reports (34b,150a) and in the United States, where thefirst (1953) recommended dietary allow-ances for babies were based on the assump-tion that 850 ml of breast milk would beproduced from 1 to 3 months and 1400from 4 to 6 months (139a).
Typical daily outputs of mature breastmilk in well-nourished women in the first 6months of life can often be less than antici-pated - between 600 to 700 mb/day ratherthan the 850 mb/day often quoted, accord-ing to a recent interpretation by Thomsonand Black (138) of the data collected byMorrison up to 1952 (101). However, muchvariation occurred between the results ofdifferent investigations, depending on themethods used and the type of subjects. Forexample, a Detroit series of studies andother early investigations contained profes-sional wet-nurses (104, 105), whose “con-ditioned” lactation performance can be par-ticulanly impressive.
Carefully conducted investigation of 363babies of normal Swedish mothers was un-dertaken 30 years ago by Wallgren (145),using test-weighing at home for 2 consecu-tive days (Table 1 ). Recently, L#{246}nnerdal etal. (91) estimated the yield of 53 mothersin the same country by test-weighing (Table2) . Despite different detailed techniquesand the intervening time between the stud-ies, the results are quite similar.
Very recent studies show the difficulty ininterpreting variation in results. For exam-ple, Picciano determined by test weighing
AgeVolume (mean)
Girls Boy’.
inc ml
1 576 645
2 704 7503 733 798
6 740 817
Monthpostpartum
No. ofmothers
Breast milkvolume
- ml
0-’/2 15 558±83
/2- l�/2 11 724 ± 117
1’/2-3’/2 12 752 ± 177
3’/2-6’/2 12 756 ± 140
the intakes of 26 healthy totally breast fedbabies in lllinois, with the following results(in mb/day) (lila).
Month Mean Mm. Max.
1 606.3 294.5 996.1
2 601.4 322.0 892.43 625.5 400.2 899.9
In Sweden, test weighing by mothers gavedaily volumes which were higher, with amean of 838 mb/day (134a).
Various studies have been undertakenwhich have sometimes shown minor varia-tions between the volume produced by eachbreast, and on different days or times ofnursing. Diurnal variation in the amountsecreted has also been noted, often withmaximal yields in the early morning andlowest yields towards evening.
Results concerning variation with age orparity of mother have been rightly termed“confused and inconclusive.” Variation involume of milk secreted between individualwomen is recognized as being considerable,although difficulties in making comparisonsare great, including variation in the weightand sucking vigor of the baby . Breast sizedoes not appear to be related to yield, beingmore an indication of mammary fat. How-ever, the influence of emotional factors onmilk yield has recently been reendorsed byLindbbad et al. (88b) who found that hospi-
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

496 JELLIFFE AND JELLIFFE
talization of healthy Swedish mothersmerely to collect samples of milk, bloodand feces caused a significant drop of 210mb/24 hr.
Variation in yield with “later” lactationis difficult to judge in webb-nourished corn-rnunities as, until the resurgence of interestin breast feeding of recent years, nursinginto the second semester of life or longerhas not been usual in Western industrializedcountries. Also, there seems little doubtthat the main stimulus responsible for thevolume of milk produced is the amount ofsucking at the breast, and hence of prolactinsecreted. This is shown by “induced bacta-tion” in some traditional societies and byrecently introduced “adoptive lactation” ornelactation in nonbactating American women,who wish to breast feed their adopted ba-bies. (143a) In both, frequent sucking at thebreast is the main factor in initiating andcontinuing milk secretion. Likewise, 24% ofa series of twins have been shown to besolely breast-fed adequately for 3 to 6months (1). Also, the “perpetual,” on atbeast very prolonged, high output by tnadi-tional wet-nurses is in part a reflection ofcontinuing vigorous sucking stimulus by suc-cessive hungry customers. In fact, the vol-ume of milk secreted has to be viewedagainst the pattern of infant feeding in theparticular family (or culture) and the con-sequent degree of sucking stimulus and itseffect on the pnolactin secretion.
The common concept of the “normal pat-tern” in Western-type cultures is of rise inoutput in the first month or so , followed bya decline thereafter to a plateau lastingapproximately until the baby is about 6months old, followed by a slow declinethereafter. Consideration of lactation pat-terns elsewhere and the previously men-tioned results in twins, in wet-nurses, ininduced lactation, and in nelactation, sug-gest that the Western pattern may not be abiological inevitable, but rather a responseto a particular pattern of sucking stimula-tion.
Very few studies have been undertakenon dietary effects on the volume of milkproduced in well-nourished women. By con-trast, numerous investigations have shownthat variation in water intake between wide
limits by the mother has no physiologicaleffect on the volume of milk secreted. Thisseems endocrinobogicalby explicable in lightof the renal antidiunetic, water-sparing ef-fect of pnolactin (77). The common beliefthat fluid intake affects milk yield probablyoperates more through a “sympatheticmagic” effect on confidence (“fluid in =
fluid out”), and hence on the psychosomatic“let-down reflex.” Conversely, in what hasbeen termed a “low solute , continuous con-tract species”, such as man, human milkwith an approximately 87% water contentis also the young baby’s source of fluid, aswell as nourishment, even in solely breastfed infants, including such a hot climate asJamaica (la).
Dominating considerations of the “nor-mab range” of milk volume secreted by well-nourished mothers are difficult questions ofsampling, very great differences in tech-nique and timing of collection of specimens,and individual variation between womenand in the same woman , both from day today and as lactation progresses . As a gener-abization, technique and method of calcuba-tion often appear to play a major robe inthe final figure brought forward.
Poorly nourished mothers. Estimations ofthe volume of breast milk produced havealso been undertaken in a variety of coun-tries in Asia and Africa, and in NewGuinea . The results have been extractedfrom published information and these ap-
proximations are presented in Table 3 . De-spite differences in methods of collection,sampling, and analysis, and bevels and formsof maternal undernutrition, it seems thatthe volumes produced were usually some-what below those reported from well-noun-ished countries in Europe and North Amer-ica.
Volumes reported varied greatly andseem to be lowest in communities with poorlevels of nutrition and with inadequate liv-ing conditions, whether urban (Cobombo,Sri Lanka (30)) or rural (New Guinea High-lands (5)) . However, working approxima-tions in round figures can be suggested:between 500 to 700 mb/day in the first 6months of life,400 to 600 mb/day in thesecond 6 months and 300 to 500 mb/day inthe second year. The few studies under-
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

VOLUME AND COMPOSITION OF HUMAN MILK 497
TABLE 3Approximate quantities of milk produced daily at different periods of lactation in some poorly nourished
communities0
Countryreference
1-6 months 6-12 months 12-24 months24 monthsand above
India(15,16) 600ml SOOml 350mlIndia (Baroda) (116, 117) 600 (3 mo)
. (350-1100)
735 (3 mo)
(540-1100)New Guinea (Chimbu) (142) 525 ml 525 ml 343 ml 343-142 mlBiak Island (60) 427 ml 390-430 ml 127-338 ml 243 mlNew Guinea (14) 720 ml 660 ml 705 ml 488 mlNew Guinea (5) 400 ml 400 ml 400 ml
Chimbu and Maprik
New Guinea (5) 600 ml 600 ml 600 mlBaiyer River
New Guinea (108) 350-480 ml 270-360 ml (12-18 mo)200-210 ml (12-24 mo)
230-300 ml
AjamaruNubuai 310-410 ml 250-340 ml (12-18 mo)
150-210 ml (18-24 mo)Egypt (45)
Healthy 922 mlMalnourished 733 ml
Sri Lanka (30) 475 ml 495 ml 506 mlNigeria (Benin) (81) 555 ml (2-3 mo) 590 ml (6-9 mo) 606 ml (13-18 mo)Uganda (122a) 660 ml (2-12 mo)
a Results not strictly comparable as varying collection techniques and methods of sampling used.
taken in the third year of lactation showvery considerable differences, varying from230 to 488 mb/day.
Also, it is well recognized in practice thatthe output of extremely malnourished moth-ers in families declines and ultimatelyceases, with fatal consequences for the nurs-ing baby (71). The nutritional point atwhich human lactation becomes seriouslyinhibited or ceases in famine circumstancesis not known , but early marasmus (in thefirst 9 months of life) a solely breast fedbabies may be occurring increasingly in thebabies of very poorly nourished womenliving in conditions of severe psychosocialstress - for example , in Karachi , Pakistan(89). Sometimes in some countries this maybe partly “contraceptive manasmus,” fromfurther interference with breast milk secre-tions by oral estrogen-containing contracep-tive pills. In pants of the world with seasonalfood shortages (“hungry seasons”), as inCentral Africa, the daily output may dropby 100 to 200 ml (l43a).
Supplementation. Limited studies havebeen carried out on the effect of supplemen-tation of the mother’s diet on output. Go-
palan showed an increase in volume se-creted, from 420 to 540 ml in poorly nour-ished Indian women after protein supple-mentation (from 61 g/day to 90 g/day (36)).Similar results were obtained in WesternNigeria by Bassir using a vegetable proteinsupplement-30 g of soya flour daily (10).Another study in India, where inadequatelynourished mothers were fed with milk bis-cuits, showed a rise in serum albumen par-abbebed by increase in albumen in the breastmilk, presumably by “spill-oven” (26b).Also , an early investigation in 1 93 1 , showedthat an increase in output could be achievedin New Zealand women by increasing thecalorie and/on the protein intake (27). Re-cently, a study in England seemed to sug-gest that poor lactation could be rebated toinadequate energy reserves - in the form ofsubcutaneous fat laid down in pregnancy,and calorie intakes in lactation. In theUnited Kingdom, slimming diets in lactatingmothers lead to “an immediate reduction inmilk supply” (148).
A recent detailed investigation was re-ported by Edozien and co-workers fromNigeria, (31b) when they showed that pro-
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

498 JELLIFFE AND JELLIFFE
tein supplementation of the lactatingmother’s diet increased the milk producedand weight in the baby, but not the proteincontent of the milk (Table 4). Similarly,Sosa et al. (128a) demonstrated a rapidincrease in milk production in a malnour-ished Guatemalan woman following an im-proved diet, particularly calories and pro-tein.
As usual , those concerned with the pro-duction of cow’s milk as a business, thedairy farmers, have infinitely more practicalknowledge than those concerned with hu-man milk and breast feeding. Thus, Lind-blad and colleagues quoted the followingaphorism from Morrison’s 1948 Handbookof Stockmen (101) which may not be com-pleteby correct for the human, but is cer-tainby generally so:
“Any inadequacy in the ration or fault inthe methods of care or management willgenerally manifest itself in the yield of milk,rather than by a change in its chemicalcomposition”
However, the effect of increasing the ma-ternal diet on human milk output may be
TABLE 4Effect of maternal dietary supplementation withprotein on the volume and protein content of breast
milkand weight gained by baby (Nigeria) 31b.0
Daily protein intake
Variable’�. 50g lOOg � 25g bOgnitially initially
No. of subjects 7 7 3 3
Totalmilksolids 13.8d 13.4 12.0 11.9
(g/lOOml) ±1.3 ±0.9 ±0.6 ±0.5Milk protein 1 .61 1 .57 1 .20 1.25
(g/lOOml) ±0.15 ±0.19 ±0.21 ±0.23
Milklactose 8.1 7.9 7.3 8.0(g/lOOml) ±0.9 ±1.0 ±1.4 ±1.8
Milkproduced 742 872� 817 1059�(g/day) ±16 ±32 ±59 ±63
Milkconsumed 617 719� 777 996�(g/day) ±15 ±10 ±38 ±74
Weightgainedby 30.4 45#{149}7e 10.5 32.2e
baby(g/day) ±3.6 ±2.0 ±3.6 ±10.1
0 Subjects were fed the initial diets for the first 14
days and then a diet providing 100 g protein per dayfor the next 14 days. Results for each subject represent
the mean values for milk samples collected duringdays 8 to 14 (for initial diet) and days 21 to 28 (fordiet providing 100 g protein per day). b Durationof lactation for all subjects was between 30 and 90
days. C Duration of lactation was over 100days. ii Results are mean values + SD. e Signifi-cantly different at the 0.05 level from the unsupple-mented subjects.
less than in dairy cows, but it should beremembered that such farm animals havebeen bred to produce much greater yieldsthan are required by the offspring (138).
Composition
The biochemical composition of humanmilk has been examined in different partsof the world . Approximate comparisons canbe made between various communities, andwith well-nourished mothers, for protein,fat, lactose, vitamins, and calcium, keepingin mind previously mentioned difficultiesposed by variations with sampling (periodin lactation cycle , time of day ; single , re-peated or 24 hr; seasons; one subject orpooled specimens, etc.), with laboratorytechniques and with bevels of difficulties inmaternal nutrition (Table 5) . Interpretationof such comparisons is made much greatenby recent realizations of the physiologicalvariations that occur in well-fed healthywomen successfully breast feeding their ba-bies.
Protein. The protein content of humanmilk has been described as varying between1 .0 to 1 .6 g/100 ml in well-nourishedwomen. In 1952, Morrison reported themean of European analyses to be 1 .6 g/l00ml and American 1 .2 g/lOO ml (101). Hesuggested that differences in methods ofestimation may be mainly responsible, andthat 1 .2 g/100 ml probably represented anoverall mean . A study in Britain showed1 .3 g/100 ml (29a). There seems little evi-dence for significant diurnal variation orfluctuation with age on parity.
However, very recent Swedish studies(1975) have shown the “true protein con-
tent” to be only 0.8 to 0.9% in apparentlywell-nourished women in that country,when determined by amino acid analysis(91). These investigators pointed out thatearlier analyses of breast milk were madewith the same methods as used for cow’smilk. In fact, it is now recognized that therelatively low protein, low solute character-istics of breast milk place the human as acontinuous contact, frequent suckling spe-cies in infancy, with rather slow growth,and also permits breast milk to be the onlysupply of water as well as nutrients.
Retrospective examination of analysesundertaken with similar methods in Brus-
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

VOLUME AND COMPOSITION OF HUMAN MILK 499
TABLE 5
Fat, lactose, protein, and calcium content of mature human milk from some well-nourished and poorlynourished communities”
Country (reference) Fat Lactose Protein Calcium
g/IOO ml mgIlOO ml
Well-Nourished
American(92) 4.5 6.8 1.1 34.0
British(87) 4.78 6.95 1.16 29.9
Australian (150) 28.6-30.7
British (29a) 4.2 7.4 1.3
Poorly-Nourished
Indian(17) 3.42 7.51 1.06 34.2
BantuS.Africa(144) 3.90 7.10 1.35 28.7Chimbu, New Guinea Highlands (142) 2.36 7.34 1.01
New Hebrides (111) 3.8 5.0 1.40 25.8
Wuppertal, Germany 3.59 1.20(Immediately Post World War II) (42)
Nauru(19) 1.60
Ibadan, Nigeria (88 months) (62) 1 .20 (0.59-1.79)New Guinea (Biak) (60) 0.83-0.9
Alexandria, Egypt (45)Healthy 4.43 6.65 1.09Malnourished 4.01 6.48 0.93
New Guinea (14) 2.3 6.48 0.93
Sri Lanka (30) 2.8 6.8 1.5Brazil (21)
Higheconomic 3.9 6.8 1.3 20.8Loweconomic 4.2 6.5 1.3 25.7
Pakistan (139) 1.2Tanzania (25) Often below 2%Nigeria(Ibadan)(102) 4.05 7.67 1.22
a Modified from Gopalan and Belavady (37), with added data.
sels, Belgium (129) in 1954 and in Tokyo,Japan (1 23) shows similar “low” levels for“true protein content” as with recent Swed-ish figures.
In poorer, technically developing coun-tries, the average protein content of themilk of inadequately nourished mothers,based on previously used methods of total
nitrogen assessment, is usually surprisinglyhigh-in fact, a low normal (1 .0 to 1 .1 g/100 ml), although the range may be quitewide (Table 5).
In some places with probably poorer flu-trition, analyses with older methods havesometimes shown the protein content to belower (0.8 to 0.9%). However, in a care-fully carried out study of poorly nourishedwomen in Karachi, Pakistan, the “true pro-tein content,” determined by an exchangechromatography after acid hydrolysis andadding up the calculated amino acid resi-dues, was 0.8 ± 0.1 g/100 ml (89). Theseresults are similar to those obtained by liketechniques in Sweden, Belgium, and Japan,
althoughwere lower.
Varying results have been obtained withestimations of the protein content with whatis termed by modern Western cultural defi-nition “prolonged lactation” - that is intothe second year of life and later. Some havefound a decline, some a rise, and others nomaterial change.
The effect of maternal dietary suppbemen-tation on protein content does not appearto have been investigated adequately. How-ever, in the protein supplementation studycarried out by Gopaban, the increased out-put of milk was associated with a come-sponding fall in protein concentration, withthe result that the total protein output in 24hr was not significantly altered (36, 37).Also, modern laboratory methods such asimmunoelectrophoresis, which enables ac-curate quantities and measurement of theindividual proteins of milk to be made werenot available at the time of earlier studies.
Recent investigations by L#{246}nnendal et al.
the lysine and methionine levels
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

500 JELLIFFE AND JELLIFFE
(91) have shown many unexplained vania-tions in healthy, well-fed women-for ex-ample, in “milk-specific proteins,” thosesynthesized by the mammary gland, no-
tabby ct-lactalbumin and lactoferrin . Thedecrease in total nitrogen in the first periodof lactation, for example in the first month,was mainly due to a dramatic drop in secre-tory IgA bevel.
Fat (lipid) . The significance of the fat con-tent of milk has been under-emphasized. Itis the main source of calories; it containsfat soluble vitamins, especially vitamin A;it is also the source of essential fatty acidsneeded for the growth and development ofthe central nervous system (24b). Lastly,the higher fat in the after-milk may act as aphysicochemical appetite control for thesuckling baby (44).
Earlier estimations of the fat content ofmilk in webb-nourished communities in theUnited States and Britain showed means of4.5 (93) and 4.78 g/100 ml (87), respec-lively. A more recent 1977 study showed amean of 4.2 g/100 ml (29a).
Results from poorly fed women in devel-oping countries have demonstrated consid-enable variation (Table 5). However, somerecent work has suggested that the fat maysometimes be considerably reduced, evendown to 1 g/100 ml (24b). Under thesecircumstances , the calorie content of themilk may be much decreased with signifi-cant lessening of energy intake (24a). Thesignificance of a bower fat content has to berelated to inadequate energy intake in pneg-nancy, with an inadequate subcutaneous“fat bank” (53), as well as to the diet inlactation itself.
The fatty acid pattern of breast milk canbe altered to some extent without affectingmilk volume or milk fat output by variationin the types of dietary fat (especially if theseare extreme) (25a) on by changes in thecalorie intake (57, 147). During energyequilibrium, milk fat resembles the fattyacid pattern of dietary fat, but when inade-quate calories are eaten, the fat in humanmilk follows the composition of human sub-cutaneous depot fat. The major factor influ-encing the fatty acid composition of milk isthe carbohydrate supply in the diet. Ulti-mately, the fatty acid composition of the
breast milk (or cow’s milk based formula)appears to be reflected in the fatty acids inthe infant’s subcutaneous fat.
The relevance of the fatty acid (and cho-lestenol) contents of human milk is currentlyunder consideration in relation to the deveb-opment of the central nervous system andatheroma in adults in industrialized coun-tries. In developing regions, the pobyenoicfatty acids may be diminished in the breastmilk of malnourished mothers, with possibleill-consequences in relation to brain growth(25).
Lactose. The third “proximate principle,”lactose, is generally recognized as beingmost constant in concentration and showsno diurnal variation. Morrison’s (101) fig-une based on 1010 samples examined invarious American and European studiesshowed a mean of 7.2 g/100 ml, while Konand Mawson found 6.9 g/100 ml in 586samples of mature milk (87). In poorlynourished mothers, lactose also does notseem to vary very much (Table 5) (range6.43 to 7.51 g/l00 ml), except in one studyin the New Hebrides where 5.0 g/100 mlwas reported (111).
Calories. The calorie intake from breastmilk is a product of the volume (as takenby the baby) and its caloric content, whichis primarily derived from fat. In well-fedcommunities, the caloric content variesgreatly. Macy and Kelly (92) give a meanfigure of 75 kcab/100 ml (range 45 to 119).The recent United Kingdom report showeda mean of 70 kcab/100 ml (29a).
In poorly nourished communities, boththe volume secreted and the fat, the maincalorie-containing constituent, (and othernutrients) may be less than in well-fed moth-ens.
Vitamins
Vitamin A . The concentration is influ-enced by the adequacy of the diet of themother in pregnancy and lactation. Thevitamin A content of breast milk is oftenmuch lower in poorer populations of somedeveloping countries (India , Ceylon , Indo-nesia, Jordan), where this nutrient is mar-ginal, than in Europe and North America.Maternal serum bevels are also low. Theintake is generally higher in the spring and
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

VOLUME AND COMPOSITiON OF HUMAN MILK 501
summer months due to greaten supplies ofdark green leafy and yellow vegetables.Particularly high levels of netinob (vitaminA) have been noted in Western Nigeria,presumably because of the widespread useof palm oil in cooking (102).
In a recent comparative investigation , thevitamin A content of breast milk was signifi-cantly higher in normal Swedish mothersthan in nonpnivileged Ethiopian mothers,whose milk showed greater concentrationsof f3-carotene (35).
Kcn and Mawson (87) found that supple-mentation with vitamin A, before and afterpartunition or later during lactation, bed tothe secretion of milk richer in vitamin Athan normally produced. In Central Amer-ica, Arroyave et al. (3) observed a rise inthe breast milk vitamin A levels after theintroduction of vitamin A fortified sugar.
Vitamin D. As well-known, levels of fat-soluble vitamin D are low in both humanand bovine milks. However, the recent dis-covery that breast milk contains a water-soluble conjugate of vitamin D with sub-phate (87a) producing the same anti-nachiticpotential as milk formulas fortified withconventional vitamin D explains the clini-cally well-recognized rarity of rickets in thebreast fed.
Thiamine. The thiamine content of breastmilk in areas with a high incidence of infan-tile beriberi has been found to be low, dueto insufficient maternal stores and intake incommunities with diets largely based onpolished rice (66) . Under these circum-stances, a specific form of malnutrition -
infantile beriberi - occurs exclusively in nor-mab-seeming breast fed babies, and is dueto a thiamine-deficient diet in the motherduring pregnancy and lactation . It is socharacteristic in time of onset that the 2 to5 month mortality has been suggested as anage-specific rate for this condition in theregions at risk.
Riboflavin. Human milk is a good sourceof riboflavin, provided the maternal diet isadequate. However, in South India, Gopa-ban and Belavady (37) found an average ofonly 17.2 p�g/100 ml of riboflavin in breastmilk, as compared with a value of about 25�g/100 ml found by Kon and Mawson inBritain (87).
Niacin. Although human milk is bow inactual niacin, it has a high potential niacinvalue because this vitamin may be synthe-sized from the amino acid, tryptophan.
Vitamin B12. Low bevels of vitamin B12have been found in the milk of poorervegetarian women in Bombay. Also, in var-ious parts of India the “syndrome oftremors” have been described in solelybreast fed babies, and has been ascribed todeficient B12 in the mother’s milk (59).
Vitamin C. The level of ascorbic acid inbreast milk is subject to variations in dietaryintake in developing countries, particularlywith the seasonal availability of fresh fruitsand vegetables. In webb-nourished mothers,human milk contains an average of 4 mg/100 ml of vitamin C. In Botswana (formerlyBechuanaband), Squires (130) found thecontent to be 1 .7 mg/100 ml in the dryseason and 2.7 mg/100 ml in the wet sea-sons. The subjects were poorly nourishedTswana women.
Since the ascorbic acid contant of breastmilk is greater than that of blood plasma,which is generally below 2.5 mg/100 ml,secretory activity in the mammary glandsmust play a part in determining the bevel ofvitamin C in milk. Apparent adaptation tolow maternal intakes of vitamin C has beennoted in Banoda, India (117) and the Phil-ippines (132). The possibility of placentalsynthesis in pregnancy has been suggested.Certainly both the placenta and the breastsmay be abbe to actively secrete ascorbicacid for the offspring. Levels of fobic acidand vitamin B6 seem to reflect maternalnutritional status (106a, 85).
Vitamin supplementation
Deodhar and Ramakrishnan (28) carriedout a dietary survey among women in SouthIndia with special reference to pantothenicacid, riboflavin, nicotinic acid, ascorbic acidand thiamin. Subsequently, the breast milkwas analyzed for the concentrations of thesame vitamins. A positive and significantcorrelation was found between dietary in-take and vitamin content of the milk for thevitamins investigated, which underlines theneed for an adequate diet for the lactatingwomen. The content of all the vitamins
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

502 JELLIFFE AND JELLIFFE
increased steadily with the dose of supple-mentation.
In a more recent investigation, supple-mentation with ascorbic acid, nicotinic acid,riboflavin, thiamin, pantothenic acid, cyan-ocobalamin, biotin, pyridoxine, and folicacid was undertaken. As a result, the vi-tamin content of the milk increased steadilywith the dose used in supplementation (29).
Calcium . Levels of calcium reported inthe milk of webb-fed mothers vary consider-ably. The calcium content in poorly nour-ished mothers has been reported to rangefrom “normal” levels to somewhat bow con-centrations (Table 5). Again, differences insampling and technique may be in partresponsible.
Levels of other minerals will not be con-sidered here, but are presented elsewhere(77). Early analyses are given by Morrisonand others (101). The question of the con-tent of trace minerals will be much underinvestigation in coming years, in relationboth to nutritional need and to possibleeffects of environmental pollution.
Adequacy
The nutritional adequacy of breast milkfor the infant can be roughly assessed bymeasuring 24-hr output and chemical corn-position , or by the recording of satisfactorygrowth, “good health” and absence of clini-cab malnutrition.
Adequacy of nutrients. The “nutrientneeds” of the baby during the exterogestatefetal stage are not derived only from thediet, but also from fetal stores acquired inutero, from the placental transfusion (iron)and, to a limited and variable extent fromultraviolet irradiation of the skin (vitaminD). The recommended daily dietary allow-ances (RDA) for babies are estimatedmainly “by analogy with breast fed infants,”and yet it is agreed increasingly that pres-entby available data on the composition ofhuman milk is incomplete and out-of-date.Fomon (34) rightly notes the need for moremodern studies, and remarks that “untilsuch data are available, many of our calcu-lations rebating to nutrients in human milkwill be likely to be misleading”. RecentSwedish studies (91) on the protein contentof breast milk give urgency to this comment.
In this regard, it is often insufficientlyappreciated that the RDA’s given for in-fants are themselves derived from estimatedintakes of breast fed babies, with an addi-tional safety factor added for the less certainsituation of infants fed on cow’s milk for-mulas (70). This is the case, for example,with the very high RDA of iron (1 0 mg/day) for the first 6 months of life , whichcan not be attained with human milk.
The derivation of RDA’s for infants areoften not understood by pediatricians ornutritionists, so that the advertising of corn-mercial baby foods can issue the followingappeal to “logic”:
“A stimulating exercise for professionals wouldbe sorting one’s beliefs about breast feeding intothose based on scientific fact and those stemmingfrom hearsay and emotion. One could thus moreobjectively counsel that growing membership in
lay organizations dedicated to breast feeding.Many sincerely believe that breast milk is allsufficient without any supplementation for at least
six months if not the full duration of breast feed-
ing. The fallacy of this concept is obvious if onecompares the nutrient content of breast milk withrecommended RDA for infants.”
The inanity of this comment is apparentespecially in view of the biological adapta-tion that has occurred over hundreds ofmibbenia. Carried to extremes, this argumentwould mean that breast milk was unfit forconsumption by human babies, without ad-ditional iron and vitamins.
The RDA’s of protein and calories sug-gested for infants have been derived frombreast milk estimations, feeding with cow’smilk based formulas and from the impon-tant, but special, studies by Fomon andMay (1958) on babies bottle fed ad bibiturnwith pasteurized breast milk (33). Based ontheir findings, it has been suggested thatinfants need: 1 st month - 836 mb/day (pro-tein 2.6 g/kg; cab 143kg); 6th month-990ml/day (protein 1 .7 g/kg; cal 90k).
However, as noted earlier, outputs inwell-nourished women actually nursing theirbabies often supply less than this, a commonrange being 600-700 mb/day for the first 6months (138). Among poorly nourishedtropical communities estimated volumesoften seem to range from 500-700 mb/dayduring the first six months (Table 4).
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

VOLUME AND COMPOSITION OF HUMAN MILK 503
As noted earlier, many of the constituentsof breast milk can be affected by inadequatematernal nutrition, depending upon its Se-verity, length and the mother’s previousnutritional status. Water soluble vitaminsare particularly influenced, including ascor-bic acid and riboflavin. Likewise, levels ofvitamin A and the pattern of fatty acidsreflect maternal diet and stores. The fatmay be reduced in some malnourishedcountries. The protein content of humanmilk in poorly nourished women is usuallywithin “normal” limits (1 .0 to 1 .1 g/100ml) or sometimes below this (0.7 to 0.9 g/100 ml) (Table 5).
By comparison with estimates of volumeand composition in well-fed mothers, infor-mation derived from poorly nourishedwomen suggests that their babies may some-times receive lesser intakes of nutrients.However, five factors need to be taken intoaccount before making too sweeping conclu-sions:
First, the figures on volume gained ingeneral studies are often those obtained byexpression or following test-feeding with theerrors implicit, and often having a risk ofunderestimations because of interferencewith the psychosomatic “bet-down reflex”and inadequate stimulation of prolactin pro-duction.
Second, such investigations are usuallybased on daytime output, when in mosttraditional cultures, babies sleep by themothers side with frequent night feedingsthe normol practice.
Third, there is a possibility of lower cab-ne intakes being needed by infants in trulytropical areas.
Fourth, smaller babies have a lesser needof nutrients, but also may have less suckingpotential.
Fifth, the data on which the RDA arebased are inadequate and approximate forinfants. The babies in the Fomon and Mayinvestigation (33) were receiving pasteur-ized breast milk from a feeding bottle, withan easier rate of flow and without the pos-sibly appetite-controlling function of highfat found in the hind-milk (44), and other“powerful self-regulatory controls withinthe infant” (110). In other words, the intakeof milk noted, and hence of calories and
protein recommended, are probably high.As noted earlier, the reported consumptionof milk in direct breast feeding studies areoften lower with apparently well-nourishedbabies.
Also, the difficulties with understandingthe nutritional and biochemical meaning ofresults obtained by analyses of single sam-ples are increased by recent increasedawareness of the physiological variation inhuman milk composition and by the needto recognize breast milk as a biologicalsystem with interacting nutrients, whichmodify each other’s absorption and utibiza-tion, rather than as a solution of indepen-dent chemicals. Recent work on the supe-nor absorption of zinc from human milkmay be noted in this respect (31a). In otherwords, the nutrients and their physiologicaleffects in the human baby vary greatly inthe breast fed and the bottle fed.
Physiological variations in the constitu-ents of milk from webb-nourished healthymothers with babies who are being success-fully breast fed can be between individualsand/or in the same individual at differenttimes. Similar differences are to be foundwith other aspects of body physiology - forexample , serum biochemistry.
Genetic variations in the composition ofcow’s milk have been recognized for dec-ades-fon example, the high fat content ofJerseys. Also, in the last 10 years on so,genetic variations in the milk of differentbreeds of cattle has been demonstrated intheir “milk protein systems,” notably in theforms of a SI casein and the /3-lactogbobulin(120). Despite the very barge amount ofnew scientific information that has becomeavailable recently, these authorities main-tam that “we have barely scratched thesurface of the complex behavior and prop-erties of the (cow’s) milk system” and other“fundamentals of dairy chemistry.” Thereare even fewer analyses of the detailedstructure of the protein systems in humanmilk (120). No information seems to beavailable concerning possible genetic differ-ence in milk composition on lactationab abil-ity in varying ethnic groups.
The level of some nutrients varies withbreast feeding itself on possibly in relationto the stage of maternal digestion. The fat
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

504 JELLIFFE AND JELLIFFE
content increases with an uninhibited bet-down reflex (with a possible appetite-con-trolling significance (44), and the prolactinproduced as a result of sucking appear tohave a controlling effect on mammary fatsynthesis (44). Periprandiab variation inconstituents secreted may also occur. Bloodbevels of sugar, fat, amino acids, and othernutrients will rise at different times afterthe mother’s meals according to their speedof digestion and absorption, and this maymake supplies to the breast’s secretory cellsfluctuate also.
Cyclical chronobiobogicab changes arecontinually occurring in all living organisms,from plankton to flowers to vertebrates. Inman , well-recognized cycles include thosethat occur each 24 hr (circadian rythms),each month (notably menstruation) andeach lifetime, as manifest by aging. Circa-dian changes in humans involved many as-pects of body physiology, including for ex-ample, the secretion of steroids, body tem-peratune , the rate of cell division and levelsof brain electrical activity.
Some chronobiobogical variations in theconstituents of breast milk are well-known,particularly the diurnal fluctuation in fatcontent (50). It also seems that, as withpregnancy, lactation can be considered as a“free-running biological cycle ,“ althoughopen-ended and without a clean-cut end-point. During this cycle, marked changes incomposition of human milk occur betweenthe cobostrurn , with its high protein (protec-tive immunogbobulins, etc., high zinc andpattern of fatty acids, and subsequent ma-tune milk. Later, chnonobiobogical changesin the lactation cycle are unclean and needinvestigation.
Lastly, the needs of individuals for allnutrients varies, and this is certainly thecase for infants. This individuality can bepartly taken cane of by the “demand andsupply” nature of the volume of milk pro-duced in breast feeding, with greaten suck-ing stimulus beading to greaten secretion. Inaddition, the composition may vary withthe individual need of the baby, possibly ona genetic basis or as a result of feedbackmechanisms acquired transplacentally bythe mother while the fetus was in utero.
Also, it is possible that stimuli from thenursing baby may affect the milk composi-tion, by as yet unappreciated mechanisms,such as alteration in the details of sucklingor even the weight of the baby. Thesesuggestions are speculative and seem fanci-ful. However, the ability of the female kan-garoo simultaneously to secrete milks ofquite different compositions from two nip-ples in response to differing stimulation ofthe young of varying stages of developmentmay be noted (77).
The physiological variation in composi-tion of human milk is unsurprising. Geneticvariations and cyclical changes occur in themilks of other mammals, and, as men-tioned, in other body fluids in man. Theexpectation that breast milk will be stan-dandized entity reflects a common fallacybased on “medical education, thought andpractice , for the past 1 00 years (which hasplaced emphasis on the constancy of physi-ological systems, (and) inter alia that con-stancy is a characteristic of life .“ Ratherthe normal healthy human being is an “os-cillating system” that is fluctuating chrono-biologically (127).
In the solely breast fed infants of webbnourished mothers with established lacta-tion and unimpaired let-down reflexes,growth is excellent in the first 4 to 6 monthsof life and nutritional deficiency is virtuallynonexistent, despite variation in milk corn-position between individuals and in any oneindividual. Breast feeding does not consistof ingesting milk obtained at a single time,but over a continuing period of time . Hu-man milk can, therefore, be considered asphysiologically variable in composition , me-sponding to various factors suggested earlierand doubtless to others, but uniformlyadapted to supply the nutrients required forthe infant, both as an individual and at theparticular stage of growth and development.
Finally, the question of possible disadvan-tages of rigidly constant formula composi-tion needs consideration. Such is the casewith regard to absence of a cobostrum-sur-rogate, but whether inability to match theflexible variability of breast milk is signifi-cant on not will only become more apparentwhen more detailed investigations are un-
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

VOLUME AND COMPOSITION OF HUMAN MILK 505
dertaken into the mechanisms and purposeof physiological chronobiological changes inhuman milk.
One conclusion seems inescapable - thatis that the present RDA for young babiesin the “exteno-gestate fetal” stage are inurgent need of reconsideration . In view ofthe unique biochemical components of hu-man milk (and their interactions), thedyadic nature of nutrition in early infancyand the difficulties of obtaining valid breastmilk samples, it would appear that theserevisions will pose considerable , perhapsinsuperable, difficulties in practice.
Adequacy by growth. It is apparent thatthe ultimate test of the adequacy of humanmilk output in breast feeding is not reflectedby estimates of volume produced or by thecomposition, but rather by assessment ofphysical growth, metabolic equilibrium, and“good health and nutrition.” From an im-mediate and rough point-of-view, adequategrowth is normally assessed anthropornetni-cabby, usually judged approximately by serialweight gain, and by the absence of necogniz-able nutritional deficiency, as the main prac-tical yardsticks. Laboratory tests for specificnutrients may rarely be possible , but in anycase, are often difficult to evaluate. Clinicalimpressions concerning “good health,”vigor and well-being are helpful, but impos-sible to measure objectively. Indeed, eventhe weight “standards of reference” used inthe assessment of growth may be inappro-priate in that they were collected in theUnited States and Europe in mainly bottle-fed babies. Biologically, standards areneeded derived from breast-fed infants.
There is sufficient evidence from widelyscattered areas, including such diversesources as the United States (58), and thePeople’s Republic of China (125), thatsolely breast fed infants do well and showsatisfactory gains in weight during the first6 months on so of life when the lactatingmothers are well nourished. From about 6months, flattening of the weight curve usu-ally indicates that the intake of calories andprotein are no longer adequate - in otherwords, that the baby has outgrown thebreast as a sole source of food.
The adequacy of unsupplemented human
milk (and the prolactin-mediated “supplyand demand” nature of breast feeding) isindicated by a recent investigation of 173pains of twins in Southern California (1).23 .7% pains were breast fed, and, of these,59.5% received no food other than humanmilk for three months or more, and 21.9%for 6 months on more (1). Growth is beinginvestigated in detail, but in general seemedcomparable to those bottle fed.
With the babies of poorly nourishedmothers in resource-poor, technically deveb-oping countries, difficulties in interpretinggrowth curves exist in relation to the preva-bence and significance of low birth weightsin the particular community, in the selectionof reference standards thought to be themost appropriate genetically for the partic-ular group, the significance of infections(including diarrhea with fluid loss) and theusual problem of sorting out weight gain inrelation to increases in fat, muscle on water-electrolyte retention.
Earlier evidence from various pants ofAfrica and India in the 1950’s indicatedthat breast feeding, with little or no supple-mentation, resulted in excellent growth forabout the first 5 to 6 months of life (36, 66,146).
However, as a generalization, more me-cent studies from such varied, but poorlynourished, parts of the world as NewGuinea (5), Ethiopia (32), and Tanzania( 1 1 3), often show comparable weight curvesto those of Western standards of referenceonly up to about 4 months of age. However,in some studies growth has continued to besimilar up to 5 months of age as in Malaysia(31), while in other investigations in Jordan(84), in northeastern Tanzania (1 13), andin Mexico (23 , 94) the weight gain in somebabies was reported to have become made-quate after only 3 months. It seems possi-ble , then , that decreasing lengths of satisfac-tory lactation are becoming evident inpoorer communities in some less developedcountries, perhaps especially in slum areas.
An additional problem is related to theeffect of oral contraceptives on reducingmilk secretion (especially with the earlierhigher dose of estrogens, and on the com-position. The possible range of significance
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

506 JELLIFFE AND JELLIFFE
of the latter is emphasized by recent reviewswhich reveal the complexity of oral contra-ceptive interactions with vitamin metabo-lism in general and difficulties in their inter-pretation (22, 73, 88).
Conclusions
The investigations summarized in thepresent account of knowledge concerningthe quantity and quality of human milk inboth well and poorly nourished communi-ties in different ecological circumstances arevery far from satisfactory . Understandably,studies have, on the whole, been piecemealwith different emphases and techniquesused in various investigations.
Although not usually appreciated, untilthe 1975 studies in Sweden (89, 91), NewZealand (100), and the 1977 report fromthe United Kingdom (29a), the most recentinvestigations in well-nourished communi-ties were made about a quarter of a centuryago.
Likewise , the technical difficulties of ob-taming representative samples, especiallyon a 24 hr basis, can be almost insuperable,especially in the field. Also the degrees ofseverity, chronicity and specificity of mater-nab malnutrition (and of maternal depletionfrom numerous previous reproductive cy-des) are rarely indicated, and indeed, withmany of these variables are difficult to cate-gomize. Lastly, the questions of genetic dif-fenences in lactation ability in different hu-man groups has never been explored ade-quately (138) and would be difficult toundertake, because of variation in diet andforms of environmental psychosocial stress.
At another level altogether is the factthat most research undertaken has beenconcerned with gross analyses of occasionalsamples, with no recognition of the degreeof variation seen normally of the morenewly recognized considerations mentionedelsewhere, such as the pattern of aminoacids, the different protein components, po-lyenoic fatty acids, pobyamines, and nucbeo-tides, and the presence of anti-infective sub-stances.
There is, in fact, a need for coordinatedcomparative modern studies into all aspectsof human lactation in webb-fed and in poorlynourished communities, using similar sam-
pling methods and analytic techniques.These would include preferably more thanone 24 hr sample, and include investigationscovering the volume and major nutrients aswell as more recently recognized biochemi-cab components and physio-chemical ele-ments (such as the forms of casein present)in different communities with various levelsof maternal oven- and under-nutrition, in-cluding women using oral contraceptives.These should also include longitudinal sam-ples to investigate the dimensions (and pun-pose) of physiological variation.
Generalizations
Nevertheless, present-day incompleteknowledge appears to warrant the followinggeneralizations for practical action:
1 ) Unsupplemented human milk is allthat is required to sustain growth and goodnutrition for the first six months of life inthe babies of well-nourished mothers, whohave, therefore, produced fetuses with op-
timal stores, who have themselves laid downadequate nutritional reserves, includingsubcutaneous fat, in pregnancy, and whoare well-fed during lactation (69).
2) The volume and composition of humanmilk in poorly nourished women is sumpnis-ingly good, possibly due to some metabolicadaptations, but probably usually to theircumulative nutritional detriment (“maternaldepletion”). However, it is often subopti-mal in quantity and in quality with lowervalues of fat (calories), water soluble vita-mins, vitamin A, and somewhat lower cab-cium and protein, than in webb-nourishedwomen.
3) Limited studies with supplementaryfeeding of poorly nourished lactatingwomen (and common sense probability)have suggested improvement in volume ofoutput and in nutritional quality of breastmilk to be feasible.
4) The adequacy of breast milk as thesole food for the baby is related to themother’s diet in pregnancy; to maternalpuempenal calorie reserves in the form ofsubcutaneous fat; to fetal stores, mainlyhepatic; to birth weight; and to the ironobtained from the placental transfusion.
5) Breast milk produced in so-called “latelactation” (e.g., 7 months to 2 years or
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

VOLUME AND COMPOSITION OF HUMAN MILK 507
more) is insufficient by itself for the risingnutrient needs (and declining stones) of therapidly growing infant, and forms a decreas-ing, but, valuable supplementary source of“complete” protein, and of fat, calcium andvitamins.3
Practical approaches
If growth, as evidenced by the weightcurve, becomes inadequate in solely breastfed babies at 4 months or earlier in poorcommunities in less developed countries, itis necessary to consider why this “failure tothrive” should be the case. Maternal nutri-tion is often considered as though it wasoccurring in isolation, with the mother as atempemamentless, disease-free “breast ma-chine” (88b). As Lindblad et al. (88b)noted:
“The most important variable behind lac-tation failure in poor women, namely milkvolume, does not seem to be primarily de-pendent on food intake, but the combinedstress of maternal disease , undernutritionand the increasingly difficult living condi-tions in rapidly developing city slum areas”
It follows, therefore, that diagnosis of anindividual in a community in relation tolactation failure must be concerned withfactors considered to be responsible in somemeasure, including maternal infections andenvironmental psychosocial stress. Never-theless, the two main forms of interferencewith lactation performance appear to bethrough’ the maternal reflexes and throughhem nutrition, so that the relative signifi-cance of these two requires consideration inany individual woman on community.
Interference with reflexes
Present-day infant feeding practices in theparticular area should be scrutinized toidentify possible practices which may beaffecting the two main maternal reflexesresponsible for the production and ejectionof milk - the prolactin and the bet-downreflexes (76a).
Various customs may be found in thetraditional culture on, more often, in im-ported Westernized practices in maternityunits (Table 6) which reduce sucking stimu-bus and, hence, diminish the pnolactin secre-tion (such as the separation of mother and
TABLE 6Puerperal practices in orthodox Western maternity
ward, which interfere with lactation, via the prolactin
and let-down reflexes. In other cultural circumstances,an analysis for practices facilitating or interfering with
these lactation reflexes needs to be undertaken (77).
Practice Effect
Delaying first breast feed
Sedated newborn (excess ma-ternal anesthesia)
Supplying prelacteal and comple-
mentary feedsRegularly, limited feeds (4 hr) Limitation of
(with no night feeds) sucking and
prolactin se-cretion
Separation of mother and infant
(“nurseries”)
Automatic free supply of formulaand infant food industry litera-
ture
Uninformed, confused mother
Tired mother (no food or drink)
Routine episiotomy (pain)Weighing before and after (test
feeds)Restricting visitors Anxiety and in-
terference withlet-down re-
Unsympathetic health staff (“an-
tidoula effect”)Automatic free supply of formula
and infant food industry litera-ture
baby in the maternity unit on the taboo onbreast feeding in public), and/on create un-certainty and anxiety and thus inhibit thebet-down reflex (Fig. 3). Conversely, minorchanges in regimen can be introduced with-out cost and make the initiation of lactationeasier (Table 7).
There is little doubt that disturbed reflexbehavior is often more important in thecausation of lactation failure than maternalsubnutmition, unless severe. In devising anappropriate program to improve breastfeeding, both aspects need consideration.Conversely, failure to gain weight in thebreast fed extemo-gestate fetus needs inves-tigation into the effects of the techniquesemployed on lactation reflexes.
3 Rohde in Indonesia comments that, in domesticterms, the output in the second year means that the
child is receiving at least one 8 oz glass of milk daily,
with 3 to 5 g of protein (supplementary to the usualvegetable protein weaning diet), essential fatty acidsand 200 to 500 IU ofvitamin A (121).
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

Puerperal care
508 JELLIFFE AND JELLIFFE
Inadequate maternal nutrition
If the infant is judged to be receivingbreast milk, which is insufficient in volumeand/or composition because of poor mater-nal nutrition, three approaches need to beconsidered:
Cow’s milk supplementation. A “logical”possible solution may seem to be the intro-duction of bottle feeds with cow’s milkbased formulas from just prior to the usualage of flattening of the weight curve.
In the circumstances of most resource-poor, less developed countries, this ap-
FIG. 3. The anxiety-nursing failure s)ndrome. Anx-iety, uncertainty or lack of interest can inhibit the let-
down reflex, often leading to failure of lactation.
proach (allaitement mixte) usually needs tobe avoided. It introduces the danger ofweanbing diarrhea at an early and vulnerableage . It decreases the secretion of breastmilk, as it interferes with sucking stimula-tion and proportional secretion of pituitaryprolactin. It interferes with lactation amen-orrhea. It is an additional endorsement bythe pediatric nutritionist of the unfortunateand unaffordable trend away from breastfeeding. Lastly, if viewed on a family or ona large-scale community basis, it has eco-nomic, agmonomic and food production con-sequences of very considerable dimensions.
Early introduction of semisolids. Again,under majority circumstances in the world,the risks of weanbing diarrhea are great ifunavoidably unclean semisolid foods areintroduced. Also, in average kitchen cm-cumstances in tropical countries and withthe foods most often available, it is usuallyvery difficult to prepare digestible, well-tol-emated and nutritionally adequate supple-mentany semisolid foods for an infant in thefirst semester of life. However, the intro-duction of semisobids by cup on by spoonwould have less effect on the prolactin reflexand hence on lactation performance thancow’s milk by bottle and can be based onthe use of mixtures of locally available
TABLE 7
Possible modifications in health services designed to promote breastfeeding in a community (77). (1978.)
Health service Modifications
Prenatal care Information on breastfeeding (preferably from breastfeeding mothers). Breast preparation.
Maternal diet. Emotional preparation for labor.
Avoid maternal fatigue/anxiety/pain (e.g. , allow to eat in early labor; avoid unnecessaryepisiotomy; relatives and visitors allowed; privacy and relaxed atmosphere; organization
of day with breastfeeding in mind). Stimulate lactation (e.g., no prelacteal feeds; firstbreast feeding as soon as possible; avoid unnecessary maternal anesthesia; permissiveschedule; rooming in). Lactation “consultants” (advisers-preferably women who have
breast fed); adequate “lying-in-period.” In hot weather, extra water to baby by dropperor spoon.
Premature unit Use of expressed breast milk (preferably fresh). Contact between mother and baby withearliest return to direct breastfeeding.
Children’s wards Accommodation in hospital (or nearby) for mothers of breast fed babies.
Home visiting Encourage, motivate, support.
Health center Supplementary food distribution (e.g., formula and wearning foods) according to defined,locally relevant policy.
General Supportive atmosphere from all staff. Avoid promotion of unwanted commercial infantfoods (e.g. , samples, posters, calendars, brochures, etc.). Adopt minimal bottle feedingpolicy and practical health education concerning “biological breastfeeding.”
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

VOLUME AND COMPOSITION OF HUMAN MILK 509
foods, nutritionally blended as “multi-mixes,” particularly based on cereal-legumeblends (79).
Supplementation of maternal diet.4 Cur-rent knowledge suggests that the most eco-nomical, safe , physiological, and practicablemethod of approaching the situation is bylaying maximum emphasis on feeding themother during both pregnancy and lacta-tion . Some nutrient stones may be neplen-ished rapidly (e .g . , vitamin C); some maytake months, particularly calories (subcuta-neous fat) and protein (muscle). An optimaldiet in pregnancy leads to improved fetalstores and a higher birth weight and morevigorous baby.
Adequate feeding, again based on “multi-mixes” of locally available foods (79) orsometimes on maternal dietary supple-ments, during pregnancy (as well as lacta-tion) can assist in insuring adequate mater-nab weight gain and sufficient nutrientstones, including calorie reserves in the form
I, of subcutaneous fat, as well as a newbornof good weight and with optimal nutritionalreserves. Similarly, an appropriate maternaldiet, again based on locally available foodmixtures, should be the emphasis duringlactation , with semisolids slowly introducedto the baby, probably from about the ageof 4 to 6 months onwards, depending onlocal circumstances, particularly the usualweight curve in infancy in the communityconcerned. Recent studies have shown thatthe main additional nutrients needed duringlactation are less than previously thought(137), and that they can usually be obtainedfrom economical, every-day foods (77).
Evidence for the adequacy of human milkas the sole food for young infants up to 6months is available, at beast in well-noun-ished communities. Theme is evidence ofimprovement in lactation performance, es-pecially the volume of milk produced, withdietary supplementation in less well-fed cm-cumstances, and deterioration with calorierestriction (148).
The message seems clean. As with somuch else concerning the health and nutri-tion of young children, the emphasis shouldbe in large measure on the mother.5 Byfeeding hem with locally available foods dur-ing pregnancy and lactation, it will be pos-sible to optimize the volume and composi-
tion of breast milk, to avoid the economic,infective and distributive complexities ofintroducing cow’s milk and bottle feedingunnecessarily, and also to avoid assistingstill further a decline in breast feeding on acommunity basis.
In addition, and at risk of oven-repetition,it must be emphasized again that thoseconcerned with infant feeding often do notgive adequate appreciation to the associatedeffects of great nutritional significance ofthe anti-infective, child spacing and eco-nomic significance of human milk and breastfeeding.
A quarter of a century ago in 1952, Mom-nison (101) concluded his painstakingly de-tailed analysis of available evidence con-cemning the “yield, proximate principles andinorganic constituents” of human milk bycommenting:
“It is clear that there is plenty of room forwork on every constituent. This review may serveto show where special care is needed in sampling
technique and the spacing of samples.”
The need for further investigations isgreaten at the present-day in view of theincreasing realization of the significance ofhuman milk on a world basis, but especiallyin resource-poor, less developed countries.Such studies need to take into account mod-ern knowledge of the psychophysiology andendocrinology of lactation, and, if feasible,should be undertaken on a collaborativeand comparative basis in various represent-ative ecobogies in different pants of the
4 In the still relatively affluent Western world, withfood increasing greatly in cost but still abundant,probably most mothers obtain their extra calories (and
probably most other nutrients also) with little extraexpense by taking somewhat larger portions of the
dishes in their everyday diet. However, guidance maybe needed in widening this diet, and one wonderswhether the Nutrition Section, Ministry of Agriculture,or other appropriate body, could suggest economicaland culturally acceptable additions to the diet duringlactation (and pregnancy). In other words, by advising
the mother not only that she needs more calories and
protein but also that these can be obtained by eating
more mashed potato (with milk) or bread-and-cheeseor similar low-cost everyday foods, rather than by
consuming large volumes of milk or other relatively
costly animal products.
The title of a recent paper by Sosa et al. (128a)
encapsulates this approach: “Feed the Nursing Mother:
Thereby the Infant”.
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

510 JELLIFFE AND JELLIFFE
Thanks are due to Ms. Indira Yalamanchili forassistance with library research.
world . Priority should be given to practicalissues of immediate application , particularlythe effect of improved maternal diet onlactation and, conversely, the breast’s abib-ity to biosynthesize nutrients and to supplythese to cover the infant’s needs on a contin-uing basis.
At the same time , within the labyrinth ofavailable data, sufficient knowledge alreadyexists to permit a rational practical approachto be suggested, based on the importantinformation available , on probability andon an understanding of the biological back-ground of man’s mammalian needs. AsOunsted and Sleigh (1 10) comment in arecent paper on “the infant’s self-regulationof food intake and weight gain” in theoffspring of presumably well-nourishedwomen: “The mange of optimal intake andgrowth mate varies widely, and the individualinfant’s needs would best be met, if he isallowed to take what he wishes, preferablyfrom his mother only.”
Infant feeding is a dyadic phenomenonfrom many points of view. Nutritionally, anadequate diet in pregnancy, including atten-tion to calories, leads to sufficient fetalstones, an optimal maternal fat bank( needed to cater for a sufficient volume ofmilk with a “normal” calorie content de-mived from fat), and a vigorous full-sizedneonate (88a) capable of inducing appnopni-ate prolactin secretion . Psychophysiobogi-cabby, the key moles of the maternal lactationreflexes are also vital to success.
In practice , it may be that Western pedi-atnc nutritionists find themselves in a mazeof often conjectural mathematical biochem-istry full of circular logic and doubtful data.(The recent halving of the RDA for caloriesfor lactating women seems to give expres-sion to the fundamental uncertainties.)
Theme is a need for new factual informa-tion, although difficulties in obtaining it willbe very great. In the well-fed, non-stressedmother it seems increasingly clean thatbreast feeding represents an unique titrationbetween the mother and baby - a trulydyadic adaptation.
References
1 . ADDY, H. A. The breast feeding of twins: anexploratory study . J . Trop . Pediat . Environ.Child Health 21: 231, 1975.
la.ALMR0rH, S. G. Water requirements of breast
fed infants in a warm climate. J. Trop. Pediat.Environ. Child Health, in press, 1978.
2. APPLEBAUM, R. M. The Modern Managementof Successful Breast Feeding. Pediat. Clin. NorthAm. 17: 203, 1970.
3. ARROYAVE, G., I. BEGHIN, M. FLORES, C. S.DE Gurno AND J. M. TICAS. Efectos del consumode azucar fortificada con retinol, en la madreembarazada y lactancte cuya dicta habitual esbaja en vitamina A. Estudio de la madre y delnino. Arch. Latinamer. Nutr. 24: 485, 1974.
4. BAILEY, K. V. Field surveys on lactating women.Trop. Geogr. Med. 14: 11, 1962.
5 . BAILEY, K . V. Quantity and composition ofbreast milk in some New Guinean populations.J. Trop. Pediat. 11: 35, 1965.
6. BARRIE, H. Modified milk for babies. J. Mat.Child Health 1 : 30, 1976.
7. BARRIE, H., E. MARTIN AND C. ANSELL. Milkfor babies. Lancet 2: 1330, 1975.
8. BASSIR, 0. Breast milk in Nigeria. J. Trop. Med.Hyg. 59: 138, 1956.
9 . BASSIR, 0 . Nutritional studies on breast milk of
Nigerian women (3). Variation in output of milk
with the stage of lactation. West Afr. Med. J. 5:88, 1956.
10 . BASSIR, 0 . Nutritional studies on breast milk ofNigerian women. Determination of the output ofbreast milk. West Afr. J. Biol. Chem. 1: 15,1957.
1 1 . BASSIR, 0. Nutritional studies on breast milk ofNigerian women. J. Trop. Pediat. 4: 3, 1958.
1 2 . BASSIR, 0 . Nutritional studies on breast milk ofNigerian women. Trans. Roy. Soc. Trop. Med.
Hyg. 53: 256, 1959.13. BEAL, V. Breast and formula feeding of infants.
J. Am. Dietet. Assoc. 55: 31, 1969.14. BECROFT, C. T. A longitudinal study of breast
feeding in the Highlands of New Guinea. Med.J. Australia 2: 598, 1967.
15. BELAvADY, B. Special report series no. 45. Stud-ies on lactation. Indian Coun. Med. Res. 1963.
16 . BELAVADY, B . Nutrition in pregnancy and lacta-tion. Indian J. Med. Res. 57: 63, 1969.
17. BELAvADY, B., AND C. GOPALAN. The effect ofdietary supplementation on the composition ofbreast milk. Indian J. Med. Res. 48: 518, 1960.
18. BOSTOCK, J. Evolutionary approaches to infantcare. Lancet 1: 1033, 1962.
19. Ba�y, G. W. Vitamin deficiency in infants.Trans. Roy. Soc. Trop. Med. Hyg. 22: 9, 1928.
20. CAMERON, M., AND Y. HOFVANDER. Manual on
Feeding Infants and Young Children. New York:Protein Advisory Group of the United Nations,1971.
21. CARNIERO, T. A., AND J. E. DULTA DE OLIv-
ERIA. Nutritional studies on human lactation in
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

VOLUME AND COMPOSITION OF HUMAN MILK 511
Brazil. J. Trop. Pediat. Environ. Child Health19: 384, 1974.
22. CHOPRA, J. G. The effect of steroid contracep.
tives on lactation. Am. J. Clin. Nutr. 25: 1202,
1972.
23. CHAVEZ, A., C. MARTINEZ, H. BouRGEs, M.CORONADO, M. LOPEZ AND S. BASTA. Childnutrition problems during lactation in poor ruralareas. Proc. IXth Int. Congr. Nutr. Mexico City,August, 1972, Vol 2, p. 90.
24. C�vIoTo, J., H. G. BRICH, E. R. DE LICARDIE
AND L. ROSALES. The ecology of infant weightgain in a pre-industrial society . Acta Paediat.Scnd. 56: 71, 1967.
24a.C�wFoRD, M. A., B. M. LAWRENCE AND A.E. MUMHAMBO. Breast feeding and human milkcomposition. Lancet 1: 99, 1977.
24b.Ca�wFoRD, M. A. AND A. J. SINCLAIR. Nutri-
tional influences in the evolution of the mamma-han brain. In: Lipids, Malnutrition and the Dc-
veloping Brain, edited by R. Elliott and J.Knight. Amsterdam: Associated Science Publi-cation, 1972.
25. CRAWFORD, M. A., P. SmvEN5, P. MSUYA AND
A. MANHAMBO. Lipid composition of human
milk: comparative studies on African and Euro-
pean mothers. Brit. J. Nutr. 33: 50A, 1974.25a.CUTHBERTSON, W. F. Essential fatty acid re-
quirements in infancy. Am. J. Clin. Nutr. 29:559, 1976.
26. EDOZIEN, J. C., M. A. R. KAGAN AND C. I.WASLIEN. Protein deficiency in man: results of aNigerian study. J. Nutr. 106: 312, 1976.
26a.DAVIES, D. P., AND T. I. EVANS. Failure tothrive at the breast. Lancet 2: 1 194, 1976.
26b.DEB, A. K., AND H. R. CAMA. Studies in humanlactation. Brit. J. Nutr. 16: 65, 1962.
27. DEEM, H. E. Observations on milk of New
Zealand Women. Arch. Disease Childhood 6:
53, 1931.
28. DEODHAR, A. D. , AND C. V. RAMAKRISHNAN.
Relation between dietary intake of lactatingwotnen and the chemical composition of milkwith regard to vitamin content. J. Trop. Pediat.
6: 44, 1960.29. DEODHAR, A. D., R. RAJALAKSHMI AND C. V.
RAMAKRISHNAN. Effects of dietary supplemen-
tation on vitamin contents of breast milk. ActaPaediat. 53: 42, 1964.
29a.Department of Health and Social Security. TheComposition of Mature Human Milk. ReportNo:12. London: H. M. Stationery Office, 1977.
30. Da SILVA, C. C. Common nutritional disordersof childhood in the tropics. Advan. Pediat. 12:213, 1964.
31 . DUODALE, A. E. The effect of the type of feedingon weight gain and illnesses in infants. Brit. J.Nutr. 26: 423, 1971.
31a.EcKERT, C. D., M. V. SLOAN, J. T. DUNCAN
AND L. S. HURLEY. Zinc binding: a difference
between human and bovine milk. Science 195:789, 1977.
31b.ED0zIEN, J. C., R. M. A. KHAN AND C. I.WASHIEN. Protein deficiency in man: results of a
Nigerian village study. J. Nutr. 106: 312, 1976.32. EKSMYR, R. A trial to change infant feeding
practices in an Ethiopian village . Addis Ababa:Ethiopian Nutrition Institute, 1969.
33. FOMON, S. J., AND C. D. MAY. Metabolic studiesof full term infants fed pasteurized human milk.Pediatrics22: 191, 1958.
34. FOMON, S. J. Infant Nutrition, (2nd ed). Phila-delphia: W. B. Saunders Company: 1974.
34a.Food and Agriculture Organization. Calorie Re-quirements. Rome: FAO Nutrition Studies No:5,p. 4. 1950.
34b.Food and Agriculture Organization. Calorie Re-quirements. Rome: FAO Nutrition StudiesNo:15, p. 12. 1957.
35. GEBRE MEHDIN, M., B. VAHLQUIST, Y.HOFVANDER AND L. UPPSALL. Breast milk com-positions in Ethiopian and Swedish women. Am.
J. Clin. Nutr. 29: 441, 1976.36. GOPALAN, C. Studies on lactation in poor Indian
communities. J. Trop. Pediat. 4: 87, 1958.37. GOPALAN, C., AND B. BELAVADY. Nutrition and
lactation. Federation Proc. 20, No. 1 , Part 3.1961.
38. GOPALAN, C., AND B. S. NARASINGA RAO. Nu-
tritional constraints on growth and developmentin current Indian dietaries. Indian J. Med. Res.59: lii, 1971.
39. GORDON, J. E., I. D. CHITKARA AND J. B.WYON. Weanling diarrhea Am. J. Med. Sci. 245:
345, 1963.40. GREENFIELD, H. The energy needs in pregnancy
and lactation. Paper presented at the Tenth Inter-national Congress of Nutrition, Kyoto, Japan,1975.
41 . GUNThER, M. Composition of human milk: fac-tors affecting it. Brit. J. Nutr. 6: 215, 1952.
42 . GUNThER, M . , AND J . E . STANIER. Special re-port series No. 275. Studies of undernutrition,Wuppertal. Med. Res. Coun. 1951.
43. HABICHT, J. P., H. DELAGADO, C. YARBOROUGH
AND R. E. KLEIN. Repercussions of lactation inthe nutritional status of mother and infant . Proc.IXth mt. Cong. Nutr. Mexico City, Vol. 2, p.106. 1972.
44. HALL, B. Changing composition of human milkand early development of appetite control. Lan-cet 1: 799, 1975.
45. HANAFY, M. M., M. R. A. MORSEY, Y. SEDDICK,
Y. A. I-Li�.aoB AND M. EL LOZY. Maternal nutri-tion and lactation performance . J . Trop. Pediat.Environ. Child Health 18: 187, 1972.
46. HARFOUCHE, K. J. The importance of breastfeeding. J. Trop. Pediat. 16: 135, 1970.
47. HONDA, T., N. KOHRI, T. KAWAKANI, H.
KOHNO, N. ORISHIMA AND K. OSUMI. A studyon aurantiasis in Japanese children . Proceedingof the Tenth International Congress of Nutrition.Kyoto, Japan: Victory-sha Press. 1976.
48. HYITEN, F. E. Collection of milk samples. Brit.Med. J. 1: 175, 1954.
49 . HYI-rEN, F. E . Variations in major constituentsduring a feeding. Brit. Med. J. 1: 176, 1954.
50. HYI-rEN, F. E. Diurnal variation in major con-
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

512 JELLIFFE AND JELLIFFE
stituentsofmilk. Brit. Med. J. 1: 179, 1954.51 . HYI-rEN, F. E. The functional capacity of the
breast. Brit. Med. J. 1: 912, 1954.52. HYI-rEN, F. E. The effect of differences in yield
and composition of milk on the infant’s weightgain and duration of breast feeding. Brit. Med.
J. 1: 1410, 1954.53. HYI-rEN, F. E., AND I. LEITCH. The Physiology
of Human Pregnancy (2nd ed). Oxford: Black-world Scientific Publications 1971.
54. HWANG, P., H. GUYDA AND H. FRIESEN. Aradioimmunoassay for human prolactin . Proc.Natl. Acad. Sci. 68: 1902, 1971.
55. IBRAHIM, A., AND N. EL-TANIL. The effect of anew low-dosage oral contraceptive pill on lacta-tion. Inter. Surg. 49: 561, 1968.
55a.GEISsLER, C., D. H. CALLOWAY, S. MARGEN
AND B. KENNEDY. Lactation adequacy, pre andpost-natal nutritional status and serum hormonallevels in Iranian women of low and middle socio-economic status. Federation Proc. 4: 896, 1975.
56. INGALLS, T. H., R. DRAPER AND H. M. TEEL.
Vitamin C in human pregnancy. Am. J. DiseasesChildren56: 1011, 1938.
57. INSULL, W., J. HIRSCH, T. JAMES AND E. H.AHRENS. The fatty acids of human milk. J. Clin.Invest. 38: 443, 1959.
58. JACKSON, R. L., R. WESTERFIELD, M. A.FLYNN, E. R. KIMBALL AND R. B. LEWIS.
Growth of “well born” American infants fedhuman and cow’s milk. Pediatrics 33: 643, 1964.
59. JADHAV, M. , J. K. G. WEBB, S. VAISHNAVA
AND S. J. BAKER. Vitamin B 12 deficiency inIndian infants. Lancet 2: 903, 1962.
60. JANSEN, A. A. J., R. KUYKEN, S. H. MALCOLM
AND J. J. L. WILLEMS. Quantity and compositionof breast milk in Biak Island. Trop. Geogr. Med.12: 138.
61 . JATHAR, V. S., S. A. KAMATH, M. N. PARIKH,
D. V. REGE AND R. S. SATOSKAR. Maternalmilk and serum vitamin B 12, folic acid andprotein levels in Indian subjects. Arch. DiseaseChildhood 45: 236, 1970.
62. JELLIFFE, D. B. The protein content of breastmilk of African women. Brit. Med. J. 2: 1131,1952.
63 . JELLIFFE, D . B . Infant feeding among the Yo-ruba of Ibadan. West African Med. J. 2: 114,1953.
64. JELLIFFE, D. B. Breast feeding in developingcountries: with special reference to West Bengal.Courrier6: 191, 1956.
65 . JELLIFFE, D. B. Child Nutrition in DevelopingCountries. Washington, D.C.: U. S. Govt. Print-cr5: 1966.
66 . JELLIFFE, D . B . Infant Nutrition in the Subtrop-ics and Tropics, (2nd ed.). Geneva: WHO Mon-
ograph no: 29, 1968.
67. JELLIFFE, D. B. Nutrition in early childhood.World Rev. Nutr. Dietet. 16: 1, 1972.
68. JELLIFFE, D. B . World trends in infant feeding.Am. J. Clin. Nutr. 29: 1227, 1976.
6� . JELLIFFE, D. B., J. M. GURNEY AND E. F. P.JELUFFE. Unsupplemented human milk and thenutrition of the exterogestate fetus. Proc. IXth
Intl. Nutr. Congr. Mexico City, Vol. 2, p. 77.1972.
70. JELLIFFE, D. B., A. E. IFEKWUNIGWE AND E.F. P. JELLIFFE. Recommended dietary allow-ances for infants. Ecol. Food Nutr. 4: 53, 1975.
71 . JELLIFFE, D. B., AND E. F. P. JELLIFFE. Theeffects of starvation on the function of the familyand of society. In: Nutrition and Relief Opera-tions in Times of Disaster edited by G. Blix andB. Vahlquist. Uppsala: Almquist and Wilsells:54, 1971.
72. JELLIFFE, D. B., AND E. F. P. JELLIFFE. Theuniqueness of human milk. Am. J. Clin. Nutr.24: 968, 1971.
73. JELLIFFE, D. B., AND E. F. P. JELUFFE. Lacta-
tion, conception and the nutrition of the nursingmother and child. J. Pediat. 81: 829, 1972.
74. JELLIFFE, D. B., AND D. JELLIFFE. Doulas,confidence and the science of lactation . J . Pediat.84: 462, 1974.
75. JELLIFFE, D. B., AND E. F. P. JELLIFFE. Humanmilk, nutrition and the world resource crisis.Science 183: 557, 1975.
76. JELLIFFE, D. B., AND E. F. P. JELLIFFE. Adap-
tive suckling. Ecol. Food Nutr. 5: 1, 1976.76a.JELLIFFE, D. B., AND E. F. P. JELLIFFE. Cultural
traditions and nutritional practices related topregnancy and lactation. In: The Nursing Dyad.Swedish Nutrition Foundation Symposium, Inpress.
77. JELLIFFE, D. B., AND E. F. P. JELLIFFE. HumanMilk in the Modern World. Oxford: OxfordUniversity Press: 1978.
78. JELLIFFE, D. B., AND I. MADDOCKS. Ecologicmalnutrition in the New Guinea Highlands. Clin.
Pediat. 3: 432, 1964.79. JELLIFFE, E. F. P. A new look at multi-mixes for
the Caribbean. J. Trop. Pediat. Environ. ChildHealth 17: 135, i971.
80. JELUFFE, E. F. P. Maternal nutrition and lacta-tion. In: Breast feeding and the mother. CibaFoundation No: 43, Amsterdam: Elsevier, 1976.
80a.JENSEN, K. 0., M. HAGGERTY AND K. E. Mc-MAHON. Lipids in human milk and infant formu-las: a review. Am. J. Clin. Nutr. In press.
81 . JOHNSON, E. J., H. S. GOYEA, E. OMAGHOMI
AND M. I. OGBEIDE. Breast milk intake of infantsin Benin City, Nigeria. J. Trop. Pediat. Environ.Child Health. In press. 1978.
82. KANAANEH, H. The relationship of bottle feed-ing to malnutritional gastroenteritis in a pre-in-dustrial setting. J. Trop. Pediat. Environ. ChildHealth 18: 302, 1972.
83. KARMARKAR, M. G., T. RAJALAKSHIMI AND C.B. RAMAKRISHNAN. Effect of dietary proteinand fat supplementation on protein, fat and es-sential amino acid contents of breast milk. ActaPaediat. 52: 473. Studies on human lactation: 1.
84. KIMMANCE, K . J . Failure to thrive and lactationfailure in Jordanian villages in 1970. J. Trop.Pediat. Environ. Child Health 18: 313, 1972.
85. KmK5Y, A., AND K. D. WEST. Relationshipbetween vitamin B6 and the content in humanmilk. Proceeding of the Tenth International Con-gress of Nutrition, Kyoto, Japan: Victory-sha
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

VOLUME AND COMPOSITION OF HUMAN MILK 513
Press, 1976, p. 607.86. KON, S. K., AND A. T. COWIE. Milk: The
Mammary Gland and its Secretion. New York:Academic Press, 1961.
87. KON, S. K., AND E. H. MAWSON. Milk: TheMammary Gland and its Secretion. Med. Res.Coun. Special Rep. Series, 1950.
87a.LAKDAWALA, D. R., AND E. M. WIDDOWSON.
Vitamin D in human milk. Lancet. 1: 167, 1977.88. LATHAM, M. D. The effect of lactation on human
fertility. Paper prepared for the Subcommitteeon Nutrition and Fertility, National Academy ofSciences, Washington, D.C. 1972.
88a.LECHTIG, A., J. P. H,�.rncrr AND C. YAR-
BROUGH. Influence of food supplementation dur-ing pregnancy on birth weight in a rural popula-tion in Guatemala. Nutrition 2: 44, 1975.
88b.LINDBLAD, B. S., AND A. LJUNGQUIST, M.GEBRE MELDIN, AND R. J. RAHIMT00LA. Foodand immunology: the composition and yield ofhuman milk in developing countries. Proc. Swed-ish Nutr. Symp. 1976.
89. LINDBLAD, B. S., AND R. J. RAHIMTOOLA. Apilot study of the quality of human milk in alower socio-economic group in Karachi, Pakistan.Acta Paediat. Scand. 63: 125, 1974.
90. Lurz, P., AND B. S. P�n. The amounts anddistribution of the nitrogenous components ofthe breast milk of British, Indian and Africanmothers, with special reference to the curd-wheyprotein ratio. Proc. Nutr. Soc. (Lond.) 17, iii,1958.
91 . LONNERDAL, B., E. FORSUM AND L. HAMBRAUS.
The protein content of human milk . Proceedingof the Tenth International Congress of Nutrition,Kyoto, Japan: Victory-sha Press, 1976, p. 698.
92 . MACY, I. G . Composition of human colostrumand milk. Am. J. Dis. Child, 78: 589, 1949.
93. Macv, I. G., AND G. J. KELLY. Human milkand cow’s milk in nutrition. In: Milk-The Mam-mary Gland and its Secretion, edited by S. K.Kon and A. T. Cowie. New York: AcademicPress, 1961, p. 265.
94. MARTINEZ, C. , AND A. CHAVEZ. Nutrition anddevelopment in infants of poor rural area . (1)Consumption of mother’s milk by infants. Proc.Internat. Nutr. Congr. 4: 139, 1971.
95. MALCOLM, L. A. A study of the Bundi people ofNew Guinea. Institute of Human Biology, Papuaand New Guinea Monograph series No. 1 , 1970.
96. MALCOLM, L. A. Growth and development inNew Guinea. A study of the Bundi people ofMadang. Madang: Institute of Human Biology,1970.
97 . MAY, J . Nutrition and lactation . Postgrad . Med.33: 380, 1963.
98. MCMILLAN, J. A., S. A. LANDEN AND F. A.05Kb. Iron sufficiency in human infants and theavailability of iron from human milk. Pediatrics58: 686, 1976.
99. MEYER, H. F. Breast feeding in the UnitedStates. Clin. Pediat. 7: No. 12, 708, 1968.
100. MICKELSON, K. N. P., J. C. HAWK, K. M.MORIARTY, R. E . MUMFORD, D . F. NEWSTEAD,
I. K. GRAY, S. V. RUMBALL AND I. THOMAS.
Composition of human milk. Proceedings of theTenth International Congress of Nutrition,Kyoto, Japan: Victory-sha Press, i976, p. 698.
101 . MORRISON, S. D. Human milk: yield, proximateprinciples and inorganic constituents. Aberdeen,Scotland: Commonwealth Agricultural Bureau
Tech. Comm. No.: 18, 1952.102 . NAISMJTh, D. J. Kwashiorkor in Western Ni-
geria. Brit. J. Nutr. 30: 567, 1973.103. NMswm, D. J., AND C. D. RITCHIE. The effect
of breast feeding and artificial feeding on bodyweight, skinfold measurements and food intakesof forty-two primiparons women. Brit. J. Nutr.32, li6A, 1975.
104. Nu.is, B., I. G. MACY, H. HUNSCHER AND M.BROWN. Variations in the composition of milk at
four hour intervals during the day and night.Am. J. Diseases Children 43: 828, 1932.
105. NIMS, B., I. G. MACY, H. HUNSCHER AND M.BROWN. Daily and monthly variations in milkcomponents as observed in two successive lacta-tion periods. Am. J. Diseases Children 43: 1062,
1932.106. NISHIMURA, H. Zinc deficiency in suckling mice
deprived of colostrum. J. Nutr. 49: 79, 1953.106a.NooUEIRA, D. M., A. BENEZIN, F. I. PEDROSO
AND B. STRUFALDI. Folic acid levels in humancolostrum and milk. 0. Hospital 70: 91 , 1966.
107. OGBEIDE, 0. Breast feeding in Mid-WesternState of Nigeria. Am. J. Clin. Nutr. 28: 88,1975.
108. OOMEN, H. A. P. C. The Papuan child as survi-vor. J. Trop. Pediat. 6: 103, 1961.
109. OOMEN, H. A. P. C. Nutrition and the Papuanchild. Noumea: South Pacific Commission Tech-nicalReportNo. 118, 1958.
1 10. OUNSTED, M., AND G. SLEIGH. The infant’s self-regulation of food intake and weight gain . Lancet2: 1393, 1975.
ill . PETERS, F. E. Chemical composition of NewHebridean human milk. Brit. J. Nutr. 7: 208,1953.
1 1 la.PICcIAN0, M. F. Iron content of breast milk. Inpress, 1978.
1 12. PICCIANO, M. F., AND H. GUThRIE. Copper,iron and zinc in mature human milk. Am. J.Clin. Nutr. 29: 242, 1976.
1 13. POEPLAU, W., AND C. SCHLAGE. Nutrition andHealth-Usumbara . In: Investigations into Healthand Nutrition in East Africa, Welfform Verlag,Munich 1969.
114. PRINSLOO, J. G., W. WrrrM�N, E. S. P. Sray-DOM, D. B. DE VILLIERS, A. S. WEH, F.LAUBSCHER AND M. A. BOTHA. Composition ofbreast milk from Bantu and White women onthe fifth postpartum day. Suppl. S. Aft. J. Nutr.44: 738, 1970.
1 15. QUEK, K. Q. Breast feeding-Southern Califor-nia. J. Trop. Pediat. Environ. Child Health 1978.In press.
1 16. RAJALAKSHMI, R., AND C. B. RAMAKRISHNAN.
Gestation and lactation performance in relationto nutritional status. Biochemistry Department,Baroda University, Baroda. 1969.
1 17. RAJALAKSHMI, R., G. SUBBULAKSHMI AND B.
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

514 JELLIFFE AND JELLIFFE
K0mARI. Ascorbic acid metabolism pregnancyand lactation. Baroda J. Nutr. 1: 117, 1974.
118. R’�o, K. S., M. C. SWAMINATHAN, S. SWARUP
AND V. N. PATWARDHAN. Protein malnutrition
in South India. Bull. World Health Org. 20:603, 1959.
1 1 9 . RAPHAEL, D . The lactation-sucking processwithin a matrix of social support. Ph.D. Thesis,Columbia University, New York, 1970.
120. RLBADEAU, DUMAS, B., F. GROSCLANDE AND J.C. MERCIER. Primary structure of the poly-morphs of casein. Mod. Prob. Paediat. 15: 46,1975.
121. ROHDE, J. E. Human milk in the second year.Paediat. Indonesiana. 14: 198, 1974.
122. READ, W. W. C., P. G. LUTZ AND A. TASHJUAN.
Human milk lipids: II the influence of dietarycarbohydrates and fact on the fatty acids ofmature milk. A study in four ethnic groups. Am.J. Clin. Nutr. 17: 180, 1965.
122a.RunSHAUsait, I. H. E. Factors affecting theintake of energy and protein by Ugandan pre-school children. Ecol. Food Nutr. 30: 213, 1974.
123. SArro, K., E. FURNICHI, S. KONDO, Q. KAWAN-
l5HI, I. NISHIKAWA, H. NAKAZATO, Y. NOGU-
CHI, T. DOI, A. NOGUCHI AND S. SHINoo. Stud-
ies on human milk. Snow Brand Milk Products,
Tokyo, Japan. 1975.124. SAMMOUR, M. B., M. E. A. RAMADAN AND M.
SALEH. Effect of chlormadinone on the composi-tion of human milk. Fertility and Sterility: 24:
301, 1973.
124a.ScHUTZ, Y., A. LECHTIG AND R. B. BRADFIELD.
Energy intakes, energy expenditure, and weightchanges in chronically malnourished women inGuatemala, Am. J. Clin. Nutr. in press.
1 25 . Shanghai Child Health Coordination Group.Measurement of the growth and development ofchildren up to 20 months in Shanghai. J. Trop.Pediat. Environ. Child Health 21 : 284, 1976.
1 26 . SCHWEDTFEGER, E . Der Aminosaurengehalt derMuttermilch. Naturwissenschafter, 52: 162,1965.
127. SiMpsoN, H. W. Chronobiological rhythms. Int.
J. Chronobiol. 1 : 19, 1973.127a.SouSA, P. L. R. The decline of breast feeding in
Brazil. J. Trop. Pediat. Environ. Child Health21: 212, 1975.
128. SIMPSON, I. A., AND A. Y. SHOW. The thiaminecontent of human milk in Malaya. J. Trop. Pc-diat. 2: 3, 1956.
128a.SoSA, R., M. KLAUS AND J. J. URRUTIA. Feedthe mother: thereby the infant. J. Pediat. 88:668, 1976.
129. SOUPART, P., 5. MOORE AND E. J. BIGwooD.
Amino acid composition of human milk. J. Biol.Chem. 206: 699, 1954.
130. SQUIRES, B. T. Ascorbic acid content of the milkof Tswana women. Roy. Soc. Trop. Med. Hyg.53: 170, 1950.
131 . STEWART, R. A. What is mother’s milk? Pediat.Basics 15: 3, 1976.
132. STRANSKY, E., D. F. DAUIS-LAWAS AND C.VIcE�rE. On ascorbic acid (vitamin C) deficiencyin the tropics. J. Trop. Med. Hyg. 53: 170,1950.
133 . Sn0M, J . The breast feeding of mature infantsduring the neonatal period and the influence ofsome factors on the same . Acta Paediat . 35 : 55,
1948.134. STUART, J. E., AND P. CONNELAN. Ascorbic
acid studies in Aborigines. Australian J. Pediat.9: 149, 1973.
134a.SVANBERG, U., M. GEBRE-MEHDIN, B. LJU-NGQUVIST AND M. OLSSON. Breast milk compo-sition in Ethiopian and Swedish mothers. IIIAminoacids and other nitrogenous substances.Am. J. Clin. Nutr. 30: 499, 1977.
135. TAITZ, L. S. Infantile overnutirition among arti-
ficially fed infants in the Sheffield region. Brit.
Med. J. 1: 315, 1971.136. THOMPSON, M. P., AND H. M. FAMELL. Genetic
variants of milk proteins. In: Lactation, A Corn-prehensive Treatise, vol. III, edited by B. L.Larson and V. R. Smith. New York: AcademicPress, 1977, p. 109.
137. THOMSON, A. M., F. E. HYI-rEN AND W. Z.BILLEQICZ. The energy cost of human lactation.Brit. J. Nutr. 24: 565, 1970.
138. THOMSON, A. M., AND A. E. BLACK. Nutritionalaspects of human lactation. Bull. World HealthOrg. 52: 163, 1975.
139. UNDERWooD, B. A., R. HEPNER AND H. ABDUL-
LAM. Protein, lipid, and fatty acids of humanmilk from Pakistani women during prolongedperiods of lactation. Am. J. Clin. Nutr. 23: 400,1970.
i39a.U. S. National Academy of Sciences. Recorn-mended dietary allowances. Washington, D.C.:Publication No: 302, 1953, p. 6.
140 . VAHLQUIST, B . Evolution of breast feeding inEurope. J. Trop. Pediat. Environ. Child Health21: 59, 1975.
141 . VAN GINNEKEN, J. K. Prolonged breast feedingas a birth spacing method. J. Trop. Pediat. Envi-ron. Child Health 21: 59, 1975.
142. VENKATACHALAM, P. 5. A study of diet, nutri-tion and health of people of the Chimbu area.Department of Public Health, Territory of Papuaand New Guinea, Monograph 4. 1962.
143. Vis, H. L. Influence of maternal health on thevolume and quality of breast milk. 6: 15, Bull.Internatl. Paediat. Assoc. 1976.
143a.WALa�rZKY, L. R., AND E. C. HERMAN. Relac-tation. Am. Family Phys. 14: 69, i976.
144. WALKER, A. R. P., U. B. ARVIDSSON AND W.L. DRAPER. Breast feeding and diet. Lancet 1:317, 1952.
145 . WALLOREN, A. Breast milk consumption ofhealthy full-term infants. Acta Paediat. 32: 778,1945.
146. WELBOURN, H. F. The danger period duringweaning. J. Trop. Pediat. 1: 334, 1955.
147. WELBY, M., M. W. O’H�LwRAN AND M. L.WELLBY. Maternal diet and lipid composition ofbreast milk. Lancet 2: 458, 1973.
148 . WHICHELOW, M . G . Success and failure in rela-tion to energy intake. Proc. Nutr. Soc. 35: 62A,1976.
148a.WHITEHEAD, R. G. Infant feeding in the devel-oping world, Lancet 2: 1 192, 1976.
149. WIDDOWSON, E. M., M. J. DAUNCEY, D. M. T.
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from

VOLUME AND COMPOSITION OF HUMAN MILK 515
GAJRDNER, J. H. P. JoNxIs AND M. PELIKAN-
FILIPKOVA. Body fat of British and Dutch infants.Brit. Med. J. 1: 653, 1975.
150. WINIKOFF, D. Calcium, magnesium and phos-phorus in the milk of Australian women. Med. J.Australia 2: 660, 1944.
150a.World Health Organization. Nutrition in Preg-nancy and Lactation. Tech. Rept. Geneva: SeriesNo: 302, 1965.
Addendum
Recent Bibliography
ALMROTH, S. G. Water requirements of breast-fedinfants in a hot climate. Quebec: Proc. Western Hemi-sphere Nutr. Congr., 1977.BELAVADY, B. Quality and composition of breast milkin undernourished mothers. Proc. Swedish Nutrition
Foundation Symposium; The Mother-Child Dyad. Inpress.BOURGES, H., C. MARTINEZ AND A. CHAVEZ. Effect
of dietary supplements on nutrient content of milkfrom mothers in rural Mexico. Quebec: Proc. WesternHemisphere Nutr. Cong., 1977.CALKINS, E. J., J. R. GARRICK AND M. F. PICCIANO.
Mineral intakes of breast-fed infants. Quebec: Proc.Western Hemisphere Nutr. Congr., 1977.HENNART, P., AND H. L. VIS. Breast feeding andpost-partum amenorrhea in Central Africa . (1 ) Milk
production in rural areas. J. Trop. Pediat. Environ.Child Health, in press.LAUBER, E. , AND M. REINHARDT. Studies on the
quality of breast milk during 23 months of lactation in
a rural community of the Ivory Coast . Am . J . Clin.
Nutr. , in press.
LECHTIG, A., J. P. HABIcHI, 0. WILSON, G. ARBoY-AVE, G. GUZMAN, H. DELGADO, R. MARTORALL, C.
YARBOROUGH AND R. KLEIN. Maternal nutrition, hu-man milk composition and infant nutrition in a ruralpopulation of Guatemala. Quebec: Proc. WesternHemisphere Nutr. Congr., 1977.VAUGHAN, L. A., C. W. WEBER AND S. R. KEMBER-
LING. Trace elements in human milk. Quebec: Proc.Western Hemisphere Nutr. Congr., 1977.SCHUlZ, Y., A. LECHTIG AND R. B. BRADFIELD.
Energy intakes, energy expenditures and weightchanges of chronically malnourished lactating womenin Guatema’a. Quebec: Proc. Western HemisphereNutr.Congr., 1977.
WRAY, J . D . Maternal nutrition , breast feeding andsurvival. Proc. Conference on Nutr. and Reprod.,February 13-16, 1977.
by guest on June 21, 2011w
ww
.ajcn.orgD
ownloaded from