ALTARUM - Preventing Epidemics. Protecting Peoplehealthyamericans.org/assets/files/Prevention...
17
Recommendations to Promote Health and Well-Being Among Aging Populations Prepared for Trust for America’s Health Altarum Institute September 2012 ALTARUM
Transcript of ALTARUM - Preventing Epidemics. Protecting Peoplehealthyamericans.org/assets/files/Prevention...

Recommendations to Promote Health and Well-Being Among Aging Populations Prepared for Trust for America’s Health
Altarum Institute
September 2012
ALT
ARU
M

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 1
Introduction
Altarum Institute supports Trust for America’s Health (TFAH) in its efforts to protect health and prevent disease in every community. We are pleased to provide recommendations to promote health and well-being among our nation’s rapidly growing aging population, more specifically Baby Boomers (ages 48–66) and older adults (age 65 and older). As described in a June 2012 paper submitted to TFAH, these age groups are less often the target for community-based wellness and prevention initiatives. Addressing this gap is consistent with the goal of the National Prevention Strategy to increase the number of Americans who are healthy at every stage of life. To that end, we offer proven and promis-ing community-based prevention strategies that can be implemented to place Baby Boomers and older adults on a path to healthier, more meaningful lives. These recommen-dations are intended for consideration as TFAH develops its 2012 federal policy report with proposed actions for the next Presidential Administration and Congress.
Baby Boomers
Recommendation 1. Accelerate the Imple-mentation, Spread, and Scale-Up of Proven Community-Based Prevention Programs
IssueThere are 79 million members of the Baby Boom generation and all of these individuals will have reached the age of 65 by 2030.1 As a result of advances in health care and technology, Boomers are slated for longer life spans than previous generations. However, many of these later years may be spent with increasing disability and compromised quality of life due to chronic illnesses such as heart disease, cancer, stroke, and diabetes. Chronic conditions are responsible for 70 percent of all deaths (1.7 million people)2 and 75 percent of health care costs each year.3 More than half of Baby Boomers ages 50–64 already report having a chronic condition,4 and nearly all (91 percent) of adults age 75 and older suffer from one or more.5 Just four health behaviors account for the most risk for preventable chronic conditions:
poor diet, physical inactivity, smoking, and alcohol misuse. Tremendous opportunity exists to engage millions of at-risk Baby Boomers in programs and initiatives that can reduce behavioral risk factors for chronic disease and help them maintain or improve their health and well-being. Although evidence-based efforts have demonstrated effectiveness, information about how to activate and sustain participation of adults likely to benefit from these programs is limited.
RecommendationThe next Administration and Congress should accelerate the implementation, spread, and scale-up of proven community-based prevention programs. Community leaders across the public and private sectors need funding and incentives to implement these programs and improve their availability. They also need education and training to encourage aware-ness and utilization of effective prevention approaches. Policymakers should increase support for research to better understand the impact and outcomes of wellness and prevention initiatives and how to scale them up and embed them in sustained practices. State- and community-level data will be especially important to guide and sustain improvement. Evaluations and systematic analyses of interventions should also be aimed at offering guidance to align programs with the unique needs of individuals and communities. Additionally, policymakers should test innova-tive payment structures in which public and private payers directly support community-based prevention programs.
Altarum has done both internally-funded and client-funded work to explore community-based programs that focus on wellness and prevention. Leading programs in this domain include:
▲▲ Diabetes prevention programs addressing lifestyle improvements have been shown to prevent and in some cases reverse chronic conditions, including diabetes and hypertension. Participants in one study achieved 58 percent risk reduction overall and 71 percent risk reduction among people age 60 and older, demonstrating that Boomers and older adults can indeed change their behavior.6 Such evidence-based initiatives can be effectively translated into practice in the general community.7
▲▲ Group Lifestyle Balance is a comprehensive behavior change program aiming to prevent diabetes and the metabolic syndrome through healthy eating and physi-cal activity. Research has found that the program can
Top Priorities for Baby Boomers▲■ Community-based
prevention
▲■ Chronic disease self-management
▲■ Workplace wellness initiatives
▲■ Health and financial planning for old age

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 2
help significantly reduce weight, cholesterol, and blood pressure and gains were maintained after program completion.8
▲▲ Coordinated Approach to Child Health (CATCH) Healthy Habits is an intergenerational physical activity and nutrition program that uses a nationally recognized evidence-based curriculum. Volunteers age 50 and older facilitate the program for students in Kindergarten through fifth grade. Studies have shown increased vegetable consumption, likelihood of reading nutrition labels, and physical activity level for adults who learn and teach the material, as well as nutrition, physical activity, and school performance benefits for children.9
ImpactThe success of these and other community-based interven-tions suggests that chronic conditions can be prevented or delayed by empowering people to make healthy lifestyle choices. More widespread implementation of these pro-grams can change the future health trajectory and quality of life for millions of Baby Boomers. Avoiding or delaying onset of disease and disability for these individuals could not only preserve their health and well-being but also reduce or postpone the need for costly medical services. Additionally, with more research related to outcomes and effectiveness, the quality of these programs will improve. Overall, greater adoption of evidence-based prevention initiatives can help improve health outcomes and may reduce the economic burden of chronic disease.
Recommendation 2. Enhance Knowledge and Adoption of Chronic Disease Self-Man-agement Programs
IssueAlthough a considerable proportion of Baby Boomers already suffer from chronic diseases, there are opportunities to prevent their conditions from worsening (or reverse them altogether) and assist in understanding and coping with their conditions. Numerous interventions and programs aim to help patients become more active in their own health by learning how to self-monitor symptoms and self-manage conditions and medications. However, research in this area is still fairly limited, and there is broad variation in the design, implementation, and evaluation of these efforts.10 This presents a challenge for providers and patients alike as it becomes difficult to communicate effectively and set
program goals and expectations. Poor integration or align-ment of these programs with other health improvement efforts can undermine their potential impact and benefit.
RecommendationPolicymakers should enhance knowledge and adoption of chronic disease self-management programs. As with preven-tion programs, there is no one-size-fits-all self-management approach. Interventions must be appropriately tailored to match the needs of patients and communities. However, investments in comparative-effectiveness research could provide a better understanding of how different programs work, what program features might be optimal, and examples of promising or best practices. With this enhanced knowledge, community partners may then consider devel-oping general standards to harmonize their approaches in administering programs. These standards may be broadly related to patient characteristics or diagnoses, for example, and should still allow for customization to meet specific patient and community needs. Additional actions should be taken to facilitate collaboration across medical and nonmedical organizations, including health care and aging services providers, public health departments, employers, and advocacy groups. These stakeholders should be encour-aged to improve alignment of their education, outreach, and messaging efforts and generate accord regarding ways to maximize patient self-management of chronic conditions.
Policymakers may consider promoting adoption of proven evidence-based strategies such as the Stanford Chronic Disease Self-Management Program. This program is offered to people with chronic health problems in community settings by trained workshop leaders who also have chronic condi-tions. Participants learn about and share coping techniques, exercise and nutrition, medication and treatment, and effective communication. The program has produced sustained health and financial benefits, including fewer emergency room and outpatient visits, reduced health distress, and improved self-efficacy.11 It has been implemented widely as funded by the Centers for Disease Control and Prevention (CDC), the Admin-istration for Community Living (ACL), and health systems such as Kaiser Permanente. Disease-specific self-management programs, including the Arthritis Self-Management Program and the Diabetes Self-Management Program, are structured similarly and have also had a positive impact.

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 3
Impact
Self-management programs targeted and implemented with fidelity can generate health and financial improve-ments. These programs can provide Baby Boomers with the education, skills, and self-efficacy needed to choose healthy behaviors and live well with their conditions. In turn, they may potentially prevent future health complications, reduce utilization of health care services, and lower overall costs to the health care system. Increased research and evaluation of these programs strengthens the evidence base and provides useful information to a diverse mix of stakeholders, helping them coordinate their patient education and outreach efforts better.
Recommendation 3. Promote the Adop-tion of Evidence-Based Workplace Wellness Initiatives
IssueThe workplace holds promise to support working Baby Boomers in improving health and well-being by encourag-ing healthy behaviors and empowering them with health information and decision support to manage their own care. Research studies including a 2011 Altarum review12 have yielded mixed evidence on the outcomes and effectiveness of workplace wellness programs. Most have reported improvements in employee health and productivity associ-ated with the implementation of wellness interventions. Evidence also suggests that employers adopting wellness programs may experience positive financial returns.13 How-ever, inconsistencies in study results and gaps in knowledge limit the extent to which workplace wellness research conclusions may be generalized to most or all employers.14
RecommendationConsistent with Altarum’s recommendations to the Bipar-tisan Policy Center (BPC), which were provided to inform the BPC’s June 2012 Lots to Lose report,15 we recommend promoting the adoption of evidence-based workplace well-ness initiatives. Specifically, policymakers should consider establishing a database of evidence related to disease prevention, wellness, and health promotion initiatives in the workplace. This database should be populated with prospec-tive, ongoing, and completed studies and best practices of workplace wellness programs. Additionally, they should encourage the use of tools and resources to evaluate the economics of workplace wellness programs. For example,
CDC offers financial guidance and Cost Calculators through its Healthier Worksite Initiative.16 More in-depth tools would allow employers to examine different investment scenarios; estimate return on investment; and allocate and manage resources before, during, and after the implementation of wellness programs. Finally, policymakers should explore strategies to engage employees in health care decisionmak-ing and help to achieve desired outcomes. These may include the use of financial and nonfinancial incentives, combined with options and tools to place the consumer “in the driver’s seat” of his or her health.
ImpactWorkplace wellness interventions grounded in evidence are more likely to be successfully adopted and sustained. A registry and ongoing evidence review and synthesis for workplace wellness research would add to and improve the quality of evidence in this area. Improved access to analytical tools and resources will provide employers with an accurate understanding of the costs and benefits of wellness programs. Additionally, engaging consumers maintains employee buy-in, a critical factor for program success. All of these efforts ensure greater success in bringing programs to scale and potentially influencing the health behaviors of many working Baby Boomers.
Recommendation 4. Support Public Educa-tion and Community-Based Initiatives That Encourage Planning for Old Age
IssueMost Baby Boomers are not adequately prepared for their “golden years.” The economic downturn has taken a particu-larly heavy toll on this generation. In addition to struggling with job losses and plunging home values, many Boomers serve as a financial crutch for both their aging parents and their children. The majority feel that they will need to delay retirement and half of Boomers are not confident that they will ever be able to retire.17 According to a recent poll, 25 per-cent of Boomers have no retirement savings and 26 percent have no personal savings.18 Just as their funds are depleting, Boomers face the reality of needing long-term care (LTC) services in the coming years, the costs of which can be substantial ($47,000 for the average person according to one study19). Since most prefer to age in place, they must also reserve funds to make age-friendly home adjustments such as chair lifts and no-step showers. Health-related planning is as important as (and intricately linked to) financial planning.

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 4
Boomers must take steps to plan for care and treatment in their later years, yet most people do not engage in advance care planning or complete advance directives. Without these measures, end-of-life care is often inconsistent with patient preferences, resulting in unnecessary suffering and wasted resources.20
RecommendationAlthough financial and health care planning are not part of the traditional menu of public health prevention strategies, they are essential components of ensuring healthy aging, security, and quality of life in later years. Policymakers should support public education and outreach initiatives that encourage advance planning for old age. This includes developing new and strengthening existing educational resources, such as the National Clearinghouse for Long-Term Care Information. This clearinghouse provides a broad range of resources to assist individuals and families in understand-ing, planning, and paying for LTC services, such as: financial planning scenarios, housing and home modification considerations, public and private insurance options, home equity and reverse mortgage information, legal and advance care planning resources, and different methods of obtaining services. Similarly, policymakers may enhance support for the Own Your Future Awareness Campaign, a federal-state effort to build knowledge about the importance of LTC planning. New outreach strategies leveraging social media platforms and technologies could expand the reach and impact of these initiatives.
Policymakers should also support broader application of community-based interventions that have demonstrated effectiveness in promoting advance care planning. Particular attention should be paid to uses of health information technology to initiate planning and share patient informa-tion. Program examples follow:
▲▲ Respecting Choices is an evidence-based program that provides training and support to help communities adopt advance care planning as an ongoing process of communication among providers, families, caregiv-ers, and patients, rather than a one-time product or event (e.g., completion of a living will). The widely implemented program has been effective in facilitating advance directive completion and matching treatments to patient wishes at the end of life.21
▲▲ Physicians Orders for Life-Sustaining Treatment (POLST) is an advance care planning tool that translates patient goals and preferences into his or her care plan through
physician orders. The POLST form accompanies the patient across care settings, including through electronic health records, making care plan communica-tions more visible and “routine” and helping to foster care coordination and continuity. Studies have shown positive results.22
ImpactAs they look ahead to old age, people in mid-life need to recognize that they may develop conditions and cognitive problems that impair their ability to make complex decisions. Planning ahead is central to ensuring active participation in financial and health-related decisionmaking. Greater emphasis on public education and outreach can provide Baby Boomers with the tools and resources that they need to understand their current and future needs, evaluate options, identify short- and long-term action items, and plan accord-ingly for old age. Increased use of advance care planning, in particular, can minimize anxiety and manage expectations for Boomers—as well as their families, caregivers, and provid-ers—as they grow older and experience changing health care needs. Having structured and informed conversations early helps ensure that they receive care aligned with their goals and wishes later. All these anticipatory steps can help Boomers to maintain control and autonomy, contributing to greater enjoyment of life as they age.
Quick Facts About Baby Boomers▲■ Boomers are likely to embrace health care
innovations to lower costs.
▲■ Boomers are concerned with staying fit and healthy. Messages that provoke a sense of empowerment and self-efficacy will have a big impact.
▲■ More than 65 million Boomers are online. The Internet and social media are powerful tools to influence their health behaviors and promote active living.
▲■ Boomers are diverse and most receptive to information that is tailored to their needs, preferences, and experiences.
Adapted from the CDC’s Audience Insights: Communicating to Boomers (1946-1962)

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 5
Older Adults
Recommendation 5. Increase Support for Policies and Programs Aimed at Preventing Falls Among Older Adults
IssueFalls are the leading cause of fatal injuries, nonfatal injuries, and trauma-related hospital admissions for older adults. Every year, one-third of seniors experience an accidental fall, resulting in more than 2 million injuries, 650,000 hospitalizations, and 20,000 deaths. These incidents are associated with direct medical costs exceed-ing $28 billion. In addition, falls have a substantial impact on quality of life for older adults. Many develop a fear of falling that causes them to limit their physical activity and social interactions, creating a “domino effect” that results in reduced mobility, physical weakness and decline, and feelings of isolation and depression.23
RecommendationGiven the magnitude of this public health problem, poli-cymakers should elevate falls prevention as a priority and support policies and programs that aim to reduce risk factors among older adult populations. This may be accomplished in multiple ways. For instance, increased funding may be provided to Area Agencies on Aging for broader imple-mentation of community-based falls prevention programs. Certain falls prevention strategies, such as home safety assessments, could also be integrated into existing senior outreach services and programs, such as Meals on Wheels. Medicare policy alternatives could reimburse for falls prevention services and, additionally, the U.S. Department of Housing and Urban Development could modify its proce-dures to incorporate falls prevention. The U.S. Department of Health and Human Services (HHS) is currently supporting evaluation and research of injury prevention programs, which includes developing strategies to reduce falls among older adults.24 These efforts should continue, and outcomes should be broadly disseminated.
Examples of proven evidence-based falls prevention strate-gies follow:
▲▲ A 2008 CDC report25 offers 14 specific falls preven-tion interventions with rigorous scientific evidence. Exercise-based programs focused on improving balance and coordination, muscle strength, range of motion, endurance, and aerobic capacity. Home modification programs featured regular visits to patient homes to identify hazards and unsafe behaviors, recommend home modifications (e.g., installing grab bars and shower seats) and behavior changes, and demonstrate the use of safety devices and mobility aids. Finally, multifaceted interventions involved assessments of environmental, behavioral, and physical risk factors; implementation of exercise programs; hazard reduc-tions; and training and guidance to further reduce risk of falls.
▲▲ FallProof is a group-based program that targets older adults who are beginning to experience balance-related problems. The program adopts a multidimensional approach, using state-of-the-art technology in order to assess the most suitable training program for partici-pants. FallProof has been proven to reduce the risk of falling26 and was recognized by the Health Promotion Institute of the National Council on Aging (NCOA) in 2006 as a “Best Practice” program in health promotion.
▲▲ Matter of Balance aims to reduce fear of falling, stop the fear of falling cycle, and increase activity levels among community-dwelling older adults. Using a lay leader model approved by ACL and NCOA, Matter of Balance acknowledges the risk of falling but emphasizes practi-cal coping strategies to reduce this fear. Studies indicate that participants experience a sustained reduction in falls, increased activity levels (due to a decreased fear of falling), and improved mobility.27
ImpactMaking falls prevention a national priority will reduce the incidence of falls and fall-related deaths and injuries among older adult populations. These efforts have the potential to save billions in health care costs currently associated with falls. Seniors benefit from falls prevention services and interventions in many ways. Through improved physical strength and coordination, as well as changes to their behav-ior and home environments, they reduce their risk of falling
Top Priorities for Older Adults▲■ Falls prevention
▲■ Physical activity
▲■ Proper nutrition
▲■ Depression prevention
▲■ Affordable and accessible housing

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 6
and feel more confident engaging in activities and events. This creates more opportunities for communication with peers, a key component in preventing depression. Overall, an increased emphasis on falls prevention helps seniors to stay active, functional, and independent.
Recommendation 6. Enhance Opportunities for Physical Activity Among Older Adults
IssuePhysical activity offers a multitude of health benefits to people at every stage of life. For older adults, it plays a crucial role in preserving strength, flexibility, and balance, thereby preventing falls and fall-related injuries.28 Other benefits for seniors include protecting against depression29; helping to maintain a healthy body weight; reducing the risk or progression of chronic diseases; reducing disabilities and functional impairments; and extending years of active, independent, and high-quality living.30 Despite these proven advantages, the majority of older adults do not achieve the recommended amount of physical activity, and many are inactive altogether. They may refrain for a number of reasons, such as health and safety concerns, lack of trans-portation, and costs associated with the activity.31 These sedentary lifestyles are contributing to a growing population of overweight and obese seniors.32 Moreover, the health care costs related to inactivity are substantial and suggest a potential to lower costs by improving physical activity among older adults.33
RecommendationAltarum recommends that policymakers enhance oppor-tunities for physical activity among older populations. Specifically, they should implement policies and targeted strategies that support active living for seniors. This involves identifying and addressing the barriers that currently prevent seniors from participating in physical activity; ramping up education and outreach efforts; and promot-ing community-based, multicomponent physical activity programs that incorporate strength, endurance, balance, and flexibility training. Group-based programs offered in community settings such as senior centers offer added social benefits, such as peer interaction and support. Importantly, policymakers need to support a broad continuum of pro-grams, ranging from low to high intensity levels, available to people of all abilities, cultures, and ethnic backgrounds.
Policymakers may spread and bring to scale the following programs, for example:
▲▲ Active Choices is a program to help older adults meet their physical activity needs. Participants are assigned a trained activity coach to help develop an individualized exercise plan, provide monthly phone support, monitor progress, and offer exercise tips and modifications. Research has shown increased moderate-to-vigorous physical activity, decreased stress and depressive symp-toms, and increased satisfaction with body appearance and function.34
▲▲ EnhanceFitness and EnhanceWellness are award-winning, community-based health programs for older adults. EnhanceFitness offers a certified instructor who leads participants in warmups, aerobics, cooldowns, strength training, stretching, and balance exercises. EnhanceWellness is implemented by a wellness team that helps participants to reach their self-determined health goals. The programs have shown positive outcomes and can be effectively replicated. 35, 36, 37
▲▲ Strong for Life is a home-based exercise program with an easy-to-follow exercise routine designed to improve strength, function, and balance in older adults with or without limitations. Research has shown that participants achieve lasting exercise adherence, improvements in lower-extremity strength and gait, and a reduction in disability.38
▲▲ Active Living Every Day helps people with sedentary lifestyles become and stay physically active. The program is offered in a variety of settings such as worksites, hospitals, and retirement communities. This evidence-based course uses established behavior change models to empower people to overcome bar-riers to physical activity. Studies have shown improved physical functioning39 and other physical and mental health benefits.40
▲▲ Fit & Strong! is an award-winning, multicomponent, evidence-based physical activity program for older adults. This program targets older adults with osteo-arthritis and has demonstrated improved functional and physical activity, reduced pain, and increased self-efficacy. These benefits have been sustained over the long term.41

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 7
ImpactEmpowering seniors to make physical activity a regular part of their lives minimizes the adverse health effects and costs associated with sedentary lifestyles. For example, more of our nation’s older adults will reduce their risk of developing a range of chronic and disabling health conditions. For seniors with existing chronic diseases, physical activity helps them to treat and manage their conditions. Additionally, fewer older adults will experience falls and related injuries, since physical activity serves as a strong ally to protect against falling. Seniors will also prevent or relieve symptoms of depression and improve their mental well-being through active lifestyles. Overall, promoting physical activity among the older adult population will help to optimize health, function, and quality of life for millions of seniors.
Recommendation 7. Promote Healthy Diet and Nutrition Among Older Adults
IssuePoor nutrition is a significant problem for older adults. Roughly 60 percent of hospitalized adults over the age of 65 experience malnutrition, which can result in increased hospitalization rates, length of stay, hospital readmission, and in-hospital mortality.42 A reduction in appetite and food intake referred to as “anorexia of aging” is common among seniors and affects even those who are in good health.43 This is caused by a number of physiological, psychological, social, and environmental factors ranging from changes in taste and smell to feelings of loneliness and depression. Inad-equate diet can lead to nutrient deficiencies and weight loss, further associated with a long list of health effects including dehydration,44 bone fractures and deterioration,45 oral health problems,46 reduced muscle mass and strength, functional and cognitive limitations, poor recovery from illness, loss of energy, and frailty.47 Low-income and homebound seniors are especially vulnerable to malnutrition, as they have limited resources and access to nutritional foods. Food assistance programs such as the Supplemental Nutrition Assistance Program (SNAP) could play an important role in reaching these populations, yet only one-third of eligible seniors participate in SNAP due to barriers including limited mobility, stigma, and general lack of understanding of the program.48
RecommendationThe next Presidential Administration and Congress should promote healthy diet and nutrition among older adults. Many strategies can be employed to achieve this. For example, home-delivered meal services can make significant strides in improving nutrition for older adults, particularly those who are homebound. Studies have shown that people who receive these services are better nourished, have increased energy levels, and experience fewer symptoms of depression.49 These programs, such as Meals on Wheels, should be encouraged and expanded to reach greater numbers of vulnerable older adults. Other nutrition education programs promoting the use of dietary supplements, such as multivitamins and nutritional drink supplements, have also been effective.50 Policymakers may also increase support for programs such as SNAP or the federally funded Commodity Supplemental Food Program, which aims to supplement the diets of older adults, and address barriers related to low participation rates. They should also facilitate partnerships across agencies such as the U.S. Department of Agriculture (USDA) and the ACL to coordinate nutrition education and assistance efforts and maximize impact. Finally, policymakers should promote awareness of existing community-based programs such as the following:
▲▲ Healthy Eating for Successful Living, endorsed by NCOA, educates seniors about nutrition and lifestyle changes to promote health and prevent chronic disease develop-ment or progression. Main components of the program include self-assessment and management of dietary pattern, goal setting, problem solving, group support, and education. The program has been well-received and addresses the cultural and literacy needs of diverse populations.51
▲▲ The federal Senior Farmers’ Market Nutrition Program awards grants to states, U.S. territories, and Indian tribal governments to provide low-income seniors with coupons that can be exchanged for eligible foods (e.g., fruits, vegetables, herbs) at farmers’ markets, roadside stands, and community agriculture programs. Evaluations have demonstrated increased access to fresh fruits and vegetables, increased consumption, and satisfaction with the program.52 Studies have also shown that home delivery of foods to homebound seniors increased intake.53
▲▲ Eat Smart, Live Strong is a nutrition education program designed to improve fruit and vegetable consump-tion and physical activity among adults ages 60–74

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 8
who participate in or are eligible for USDA Food and Nutrition Service nutrition assistance programs. The intervention, based on the Dietary Guidelines for Americans, MyPyramid, and a review of promising practices, helps communities to improve the health of low-income older adults.
ImpactProper nutrition plays a vital role in the health and well-being of older adults. Implementing evidence-based strategies to promote nutrition among seniors, especially those most at risk, will produce a range of positive outcomes for this population. For example, these actions prevent and reduce food insecurity, ensuring that more seniors have access to the healthful foods, nutrients, and supplements that they need. Rates of malnutrition among older adults will drop along with related costs and conditions. Community-based nutrition programs and services also help seniors to ward off potential health problems and achieve greater levels of energy and socialization.
Recommendation 8. Promote Primary and Secondary Prevention of Depression Among Older Adults
IssueDepression, sadness, and “feeling blue” can be mistakenly accepted as part of the normal aging process. In actuality, depression is a serious public health problem affecting more than 6 million people age 65 and older.54 It is linked with suffering and reduced quality of life—for the affected individuals as well as their friends and families—and can lead to declines in physical, mental, and social functioning. In general, depressed seniors visit health care providers and hospitals more frequently, have longer lengths of stay, and take more medications, all of which result in high health care costs.55 One study56 found that costs for seniors with depression were nearly double the costs for those without ($20,046 vs. $11,956). Risk factors for depression may include bereavement, disability, chronic conditions, and low levels of physical activity.57 Depression is the single greatest risk factor for suicide among older adults. Adults age 65 and older experience higher suicide rates than the general population and accounted for 16 percent of suicide deaths in 2004.58 Alarmingly, as many as 75 percent of older adults who commit suicide visit a physician within the month before their death,59 underscoring the need for prevention, early diagnosis, and treatment of depression.
RecommendationPolicymakers should promote the prevention and early detection of depression among older adults. Screening for depression is already part of each periodic health examina-tion Medicare covers, but Medicare should monitor the compliance and the effectiveness of the tools and documen-tation that practitioners are using. The Substance Abuse and Mental Health Services Administration identifies a number of programs and services that have demonstrated positive effects in preventing depression in older adults, such as community-based exercise programs; targeted educational classes (e.g., multicomponent mind-body wellness courses); and life review programs aimed at reflection, reminiscence, and improvement of overall life satisfaction.60 Such proven strategies should be disseminated more broadly, accompa-nied by enhanced communication efforts to raise awareness about the public health implications of depression among senior populations. Policymakers may also consider increas-ing funding and support to federal, state, and local agencies to encourage collaboration in research and demonstration projects aimed at prevention of depression and suicide among older adults.
Secondary prevention strategies are also important in the early detection and management of depression. Examples of programs that have demonstrated effectiveness follow:
▲▲ PEARLS (Program to Encourage Active Rewarding Lives for Seniors) teaches depression management techniques to older adults with depression. The program offers in-home counseling sessions that focus on brief behavioral techniques (e.g., problem solving treatment, social and physical activation, pleasant event planning). Evidence shows significant reduction and in some instances elimination of depression, improved functional and emotional well-being, and reduced use of health care services such as hospitalizations.61
▲▲ Healthy IDEAS (Identifying Depression, Empowering Activities for Seniors) is a community-based program designed to detect and reduce the severity of depressive symptoms in older adults with chronic health conditions and functional limitations. The program includes screen-ing, education, empowerment, and linkages to health care providers. Research has shown reduced depression severity, reduced pain, and increased activity levels.62

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 9
ImpactIncreased prevention and early diagnosis of depression will have a positive effect on the lives of millions of older Americans. Efforts aimed at improving the emotional and psychological well-being of seniors reduce risk factors for depression and reduce symptoms for those already suffer-ing. Seniors will also benefit from other physical and mental health improvements, as many programs and services to prevent or treat depression focus on promoting healthy lifestyles. Lower rates of depression will result in reduced health care utilization and costs associated with the disorder. Moreover, as more seniors learn effective strategies to combat stress and feelings of helplessness, they reduce their risk of suicidal behavior. This expected outcome is consistent with research showing significant reductions in suicide risk through the prevention and management of depression.63
Recommendation 9. Increase Affordable and Accessible Housing Options for Older Adults
IssueWhile 90 percent of older adults want to stay in their homes as long as possible,64 the costs of maintaining a home can be prohibitive for seniors with declining health and functional capacity. Homes must often be revamped to accommodate limitations related to vision, hearing, memory, and mobility. These modifications can add thousands of out-of-pocket dollars, forcing many to forgo them altogether. Supportive services that help seniors with daily living activities, such as cooking and bathing assistance, can also be costly and are not paid by Medicare on a long-term basis.65 Many grapple with these cost burdens while living in or close to poverty. Half of older adults have incomes less than $18,500, and roughly 10 million have incomes less than $10,800.66 Federal housing programs such as Section 202 can help people age comfortably in their communities. However, demand is high, wait lists are long, and funding cuts over the past several years have slowed the construction of new feder-ally subsidized housing units.67 Other affordable housing developments for seniors are also in short supply. Most of the communities in which older adults have built memories, relationships, and connections over the years simply do not meet their housing needs. Many end up moving prematurely into institutions or nursing homes where annual costs far exceed the costs of home- or community-based care.68 As the general population ages and the number and propor-tion of older adults increases, this problem will become ever more acute.
RecommendationAltarum recommends increasing the amount of afford-able and accessible housing options for older adults. The supply of federally subsidized housing for seniors should at least meet current needs, and further expansion should be considered to plan for future demands. Policymakers should also explore new and existing models that combine housing and supportive services for older adults. These may be supported by both public and private funding. Examples include assisted living residences, Naturally Occurring Retirement Communities, “Village” models (e.g., Beacon Hill Village),69 and Continuing Care Retirement Communities. More studies of these models, focusing on their shared and unique characteristics, will shed light on those that may be most effectively implemented in other communities. The success of housing models and programs will rely strongly on community partnerships. Therefore, opportunities for collaboration across a range of organizations—from universities to government agencies—should be examined.
The Center for Housing Policy70 suggests a number of policy changes and recommendations that can be implemented to enhance housing choices for seniors. Some examples include property tax relief programs and housing vouchers to make senior homes more affordable, Medicaid and Medicare policy changes to support home and community care, required use of age-friendly design principles in government subsidized housing, and flexible building and zoning regulations to offer more shared living arrangement options.
Additionally, policymakers should support programs that connect seniors with available benefit programs to help cover the cost of housing expenses. For example, NCOA’s Economic Security Initiative and BenefitsCheckUp initiatives offer tools and assistance to improve the overall economic security of lower-income older adults. BenefitsCheckUp has helped more than 3 million people find nearly $12 billion in federal, state, and private benefits to assist with a variety of expenses including food, housing, utilities, medications, legal issues, and in-home services.71
ImpactThe availability of affordable and accessible housing enables seniors to age in place, consistent with their preferences and generally at a lower cost to the community. Improved access to services and programs will help them to make necessary adjustments to their homes and lifestyles without the severe costs that can “break the bank” for so many older

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 10
adults. These housing options play a role in averting or delaying placement in nursing homes. Overall, adequate housing affects the ability of older adults to maintain control and independence, contributing to greater satisfaction and well-being.
Communities and Environments
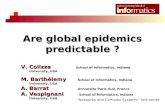
Some of the recommended prevention strategies in this paper are important for both Baby Boomers and older adults. For example, healthy eating and exercise are key components of community-based wellness and prevention initiatives and chronic disease self-management programs. These factors can help Baby Boomers to avoid, delay, and manage chronic conditions. Nutrition and physical activity remain important as Boomers enter into their senior years, for the same reasons as well as their added role in protect-ing against falls and depression. Prevention strategies are often interconnected and influenced by many factors at the individual, community, and environmental levels, including lifestyles, social networks, work environments, and housing (see Figure 1). Altarum addresses several determinants of health throughout this paper. The relationship between health and social and economic factors is at the core of our final recommendation below.
Figure 1. Determinants of Health
Source: Dahlgren, G. & Whitehead, M. (1991). Policies and strategies to promote social equity in health. Stockholm: Institute for Future Studies.
Recommendation 10. Support the Creation of Healthy Communities for People of All Ages and Abilities
IssueThe design of our built environment—such as homes, schools, businesses, parks, and roads—has a profound impact on our health and well-being.72 For example, cities and neighborhoods can engender healthy behaviors by offering safe sidewalks, bike paths, and walking trails. Others can rely mostly on automobiles, limiting opportunities for people to be active and contributing to harmful effects such as air pollution and car accidents. Public health and com-munity leaders are paying increased attention to our built environments. The impending swell of the U.S. population over the next 20 years, requiring the construction of 59 million new housing units according to some projections,73 challenges leaders to rethink the ways in which places are designed, resources are spent, and services are delivered. This presents an enormous opportunity to reshape our communities as well as a pressing need for research and guidance on how to create environments that protect and improve public health.74
RecommendationAltarum recommends that policymakers support the creation of healthy communities for people of all ages and abilities. “Livable,” “lifelong,” “age-friendly,” “sustainable,” and “intergenerational” are terms popularly used to describe this concept. They share the basic premise of ensuring that com-munities and environments meet the needs of all residents. Policymakers should consider laws, policies, and programs that pave the way for these healthy built environments. States such as Michigan have made significant progress in enacting policy and environmental changes to engage residents in healthy lifestyle behaviors. Altarum has worked extensively with the Michigan Department of Community Health to evaluate initiatives, including (1) Building Healthy Communities, which aims to reduce unhealthy eating, increase physical activity, and increase tobacco-free environ-ments; and (2) Complete Streets, which aims to ensure that roadways are designed and operated to enable safe access for users of all ages and abilities. Several other states have supported livable communities through the implementa-tion of policies pertaining to land use, transportation, and housing.75 These efforts should be evaluated to identify promising practices that may be used by other state and local government entities.

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 11
Other ongoing community-driven projects can offer lessons to help prioritize and kick-start community transformation efforts. The Atlanta Regional Commission’s Lifelong Com-munities Initiative is an award-winning example.76 Through this initiative community members with diverse expertise (e.g., health, design, engineering, marketing, development, economics) have worked together to convert suburban sprawl into communities that appeal to all residents. The challenges and interventions needed to retrofit different urban and suburban settings are detailed in case studies.
Additionally, policymakers should address the dearth of current research related to community design and human health. Agencies including CDC77 and the National Institutes of Health78 have identified specific research recommenda-tions in this area, both emphasizing the importance of coordination across multiple disciplines and both federal and nonfederal organizations. Support should be provided to these and other agencies, such as the Environmental Protection Agency, to conduct studies to better understand the elements and impact of healthy communities.
Impact
The design and development of healthy communities affects people across the lifespan, from early childhood to older adulthood. Community environments are especially important determinants of health for older adults and those with disabilities who spend the majority of time near their
homes. Environments that offer a range of transportation options, a mix of housing choices, convenient services and amenities, and access to nutritious foods and open spaces will improve health in many ways. For example, they promote physical activity and healthy diet, improve air and water quality, and enable social connections and neighborli-ness, making life more enjoyable and fulfilling at every stage. They also improve coordination and collaboration across organizations and maximize resources. More research, poli-cies, and practices aimed at promoting healthy communities help to build and strengthen our national infrastructure for prevention and wellness.
Summary Table of Recommendations
Altarum’s recommendations align with and reinforce National Prevention Strategy recommendations and federal actions aimed at improving the health of all Americans. As shown in the table below, many Altarum recommendations correspond directly with the National Prevention Strategy (e.g., falls prevention), and others are more broadly connected (e.g., planning for old age, affordable housing). Opportunities remain to ensure that the unique needs of aging adults, including Boomers and seniors, are explicitly incorporated into National Prevention Strategy implementation plans.
Altarum Recommendation
National Prevention Strategy Recommendation
National Prevention Strategy Federal Action
Accelerate the implementation, spread, and scale-up of proven community-based prevention programs
Enhance knowledge and adoption of chronic disease self-management programs
Promote the adoption of evidence-based workplace wellness initiatives
Engage and empower people and communities to plan and implement prevention policies and programs
Provide people with tools and information to make healthy choices
Promote positive social interactions and support healthy decisionmaking
Support implementation of community-based preventive services and enhance linkages with clinical care
Support workplace policies and programs that increase physical activity
Promote and expand research efforts to identify high-priority clinical and community preventive services and test innovative strategies to support delivery of these services
Support research and programs that help people make healthy choices

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 12
Altarum Recommendation
National Prevention Strategy Recommendation
National Prevention Strategy Federal Action
Support the creation of healthy communities for people of all ages and abilities
Enhance opportunities for physical activity among older adults
Increase affordable and accessible housing options for older adults
Support public education and community-based initiatives that encourage planning for old age
Enhance cross-sector collaboration in community planning and design to promote health and safety
Identify and implement strategies that are proven to work and conduct research where evidence is lacking
Facilitate social connectedness and community engagement across the lifespan
Encourage community design and development that supports physical activity
Facilitate access to safe, accessible, and affordable places for physical activity
Design and promote affordable, accessible, safe, and healthy housing
Enhance capacity of state, tribal, local, and territorial governments to create healthy, livable, and sustainable communities
Support healthy housing while addressing unsafe housing conditions and health-related hazards
Promote healthy diet and nutrition among older adults
Increase access to healthy and affordable foods in communities
Help people recognize and make healthy food and beverage choices
Implement programs and regulations to increase access to healthy food and eliminate food insecurity
Increase support for policies and programs aimed at preventing falls among older adults
Promote and strengthen policies and programs to prevent falls, especially among older adults
Develop and test innovative and promising strategies to prevent injuries and violence
Promote primary and secondary prevention of depression among older adults
Provide individuals and families with the support necessary to maintain positive mental well-being
Promote early identification of mental health needs and access to quality services
Improve access to high-quality mental health services and facilitate integration of mental health services into a range of clinical and community settings
Provide easy-to-use information about mental and emotional well-being for consumers, especially groups that experience unique stressors
Source for National Prevention Strategy recommendations and federal actions: National Prevention Council. (2012, June). National Prevention Council action plan: Implementing the National Prevention Strategy.
Conclusion
This paper details top prevention priorities for Baby Boomers and older adults. Altarum offers proven community-based wellness and prevention strategies, as well as promising approaches, to steer them toward better health and well-being. Many focus on equipping both age groups with the tools and support that they need to choose healthy behaviors, such as healthy eating and physical activity. These lifestyle interventions can prevent, delay, and better manage chronic health conditions and disabling conditions. They also lead to social and mental health benefits and
show potential for considerable cost savings. For Boomers, we offer financial and health planning as an important way to anticipate and prepare for old age. While no one can “prevent” growing old, everyone can take measures to avoid unnecessary suffering and crippling LTC expenses. For older adults, we highlight their susceptibility to fall-related injuries and depression and offer evidence-based strategies to address these issues. Finally, we recognize the inextricable link between health and our surrounding environment. We offer strategies to reshape the landscape of our communities to promote, protect, and improve health for people of all ages and abilities.

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 13
Endnotes
1. Pew Research Center. (2010, December). Baby boomers approach age 65 – glumly. Retrieved from http://pewresearch.org/pubs/1834/baby-boomers-old-age-downbeat-pessimism.
2. Centers for Disease Control and Prevention. Chronic disease prevention and health promotion. Retrieved from http://www.cdc.gov/chronicdisease/index.htm.
3. National Council on Aging. Healthy aging fact sheet. Retrieved from http://www.ncoa.org/press-room/fact-sheets/healthy-aging-fact-sheet.html.
4. Collines, S. R., Davis, K., Schoen, C., Doty, M. M., & Kriss, J. L. (January 2006). Health coverage for aging baby boomers: Findings from the Commonwealth Fund survey of older adults. The Commonwealth Fund. Retrieved from http://www.commonwealthfund.org/Publications/Fund-Reports/2006/Jan/Health-Coverage-for-Aging-Baby-Boomers--Findings-from-The-Commonwealth-Fund-Survey-of-Older-Adults.aspx.
5. National Council on Aging. Healthy aging fact sheet. Retrieved from http://www.ncoa.org/press-room/fact-sheets/healthy-aging-fact-sheet.html.
6. Brink, S. (2009). The Diabetes Prevention Program: How the participants did it. Health Affairs (Project Hope), 28(1), 57–62.
7. Ackermann, R., & Marrero, D. (2007). Adapting the Diabetes Prevention Program lifestyle intervention for delivery in the community: The YMCA model. The Diabetes Educator, 33(1), 69.
8. Kramer, M., McWilliams, J., Chen, H., & Siminerio, L. (2011). A community-based diabetes prevention program: evaluation of the group lifestyle balance program delivered by diabetes educators. The Diabetes Educator, 37(5), 659–668.
9. Werner, D., Teufel, J., Holtgrave, P., & Brown, S. (2012). Active generations: an intergenerational approach to preventing childhood obesity. The Journal of School Health, 82(8), 380-386.
10. Pearson, M. L., Mattke, S., Shaw, R., Ridgely, M. S., & Wiseman, S. H. (2007, November). Patient self-management support programs: An evaluation. AHRQ Publication No. 08-0011. RAND Health. Retrieved from http://www.ahrq.gov/qual/ptmgmt/ptmgmt.pdf.
11. Lorig, K., Mazonson, P., & Holman, H. (1993). Evidence suggesting that health education for self-management in patients with chronic arthritis has sustained health benefits while reducing health care costs. Arthritis & Rheumatism, 36(4), 439–446.
12. Korda, H., Eldridge, G. N., Kloc, M., & Schuster, J. L. (2011). Enabling employee wellness: What do we know about what works? Altarum Institute issue brief.
13. Goetzel, R., & Ozminkowski, R. (2008). The health and cost benefits of work site health-promotion programs. Annual Review of Public Health, 29, 303–323.
14. Osilla, K. C., Van Busum, K., Schnyer, C., Larkin, J. W., Eibner, C., & Mattke, S. (2012). Systematic review of the impact of worksite wellness programs. American Journal of Managed Care, 18(2), e68–e81.
15. Bipartisan Policy Center. (2012, June). Lots to lose: How America’s health and obesity crisis threatens our economic future. Retrieved from http://bipartisanpolicy.org/projects/lotstolose.
16. Centers for Disease Control and Prevention. Healthier Worksite Initiative: Cost Calculators. Retrieved from http://www.cdc.gov/nccdphp/dnpao/hwi/programdesign/costcalculators.htm.
17. AARP. (2012, August). Boomers’ “anxiety index” high, voter survey reveals. Retrieved from http://www.aarp.org/politics-society/government-elections/info-08-2012/aarp-2012-voter-survey.html.
18. AARP. (2011, February). Boomers report no savings at all. Retrieved from http://www.aarp.org/work/retirement-planning/info-02-2011/many_boomers_report_no_savings_at_all.html.
19. Kemper P., Komisar, H. L., & Alecxih, L. (2005). Long-term care over an uncertain future: What can current retirees expect? Inquiry, 42(4), 335–350.
20. U.S. Department of Health and Human Services, Assistant Secretary for Planning and Evaluation. (2008, August). Advance directives and advance care planning: Report to Congress. Retrieved from http://aspe.hhs.gov/daltcp/reports/2008/ADCongRpt-C.pdf.
21. Hammes, B. J. & Rooney, B. L. (1998). Death and end-of-life planning in one Midwestern community. Archives of Internal Medicine, 158(4), 383–390.
22. Hickman, S. E., Tolle, S. W., Brummel-Smith, K., & Carley, M. M. (2004). Use of the POLST (Physician Orders for Life-Sustaining Treatment) program in Oregon nursing facilities: Beyond resuscitation status. Journal of the American Geriatrics Society, 52, 1424–1429.
23. National Council on Aging. Falls prevention fact sheet. Retrieved from http://www.ncoa.org/press-room/fact-sheets/falls-prevention-fact-sheet.html.

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 14
24. National Prevention Council. (2012, June). National Prevention Council action plan: Implementing the National Prevention Strategy. Retrieved from http://www.healthcare.gov/prevention/nphpphc/2012-npc-action-plan.pdf.
25. Stevens, J., & Sogolow E. (2008). Preventing falls: What works. A CDC compendium of effective community-based interventions from around the world. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control.
26. Rose, D. (2011). Reducing the risk of falls among older adults: The FallProof Balance and Mobility Program. Current Sports Medicine Reports, 10(3), 151–156.
27. Healy, T. C., Peng, C., Haynes, P., McMahon, E., Botler, J. & Gross, L. (2008). The Feasibility and Effectiveness of Translating A Matter of Balance into a Volunteer Lay Leader Model. Journal of Applied Gerontology, 27 (1), 34-51.
28. Gregg, E., Pereira, M., & Caspersen, C. (2000). Physical activity, falls, and fractures among older adults: A review of the epidemiologic evidence. Journal of the American Geriatrics Society, 48(8), 883–893.
29. Strawbridge, W., Deleger, S., Roberts, R., & Kaplan, G. (2002). Physical activity reduces the risk of subsequent depression for older adults. American Journal of Epidemiology, 156(4), 328–334.
30. Cress, M., Buchner, D., Prohaska, T., Rimmer, J., Brown, M., Macera, C., ... Chodzko-Zajko, W. (2005). Best practices for physical activity programs and behavior counseling in older adult populations. Journal of Aging And Physical Activity, 13(1), 61–74.
31. Belza, B., Walwick, J., Shiu-Thornton, S., Schwartz, S., Taylor, M., & LoGerfo, J. (2004). Older adult perspectives on physical activity and exercise: Voices from multiple cultures. Preventing Chronic Disease, 1(4), A09.
32. McTigue, K., Hess, R., & Ziouras, J. (2006). Obesity in older adults: A systematic review of the evidence for diagnosis and treatment. Obesity (Silver Spring, Md.), 14(9), 1485–1497.
33. Elsawy, B., & Higgins, K. (2010). Physical activity guidelines for older adults. American Family Physician, 81(1), 55–59.
34. Wilcox, S., Dowda, M., Griffin, S., Rheaume, C., Ory, M., Leviton, L., ... Mockenhaupt, R. (2006). Results of the first year of active for life: Translation of 2 evidence-based physical activity programs for older adults into community settings. American Journal of Public Health, 96(7), 1201–1209.
35. Leveille, S., Wagner, E., Davis, C., Grothaus, L., Wallace, J., LoGerfo, M., & Kent, D. (1998). Preventing disability and managing chronic illness in frail older adults: A randomized trial of a community-based partnership with primary care. Journal of the American Geriatrics Society, 46(10), 1191–1198.
36. Tomioka, M., Sugihara, N., & Braun, K. (2012). Replicating the EnhanceFitness physical activity program in Hawai`i’s multicultural population, 2007–2010. Preventing Chronic Disease, 9, E74.
37. Moore-Harrison, T., Johnson, M., Quinn, M., & Cress, M. (2009). An evidence-based exercise program implemented in congregate-meal sites. Journal of Physical Activity & Health, 6(2), 247–251.
38. Jette, A., Lachman, M., Giorgetti, M., Assmann, S., Harris, B., Levenson, C., ... Krebs, D. (1999). Exercise—it’s never too late: The strong-for-life program. American Journal of Public Health, 89(1), 66–72.
39. Baruth, M., Wilcox, S., Wegley, S., Buchner, D., Ory, M., Phillips, A., ... Bazzarre, T. (2011). Changes in physical functioning in the Active Living Every Day program of the Active for Life Initiative (R). International Journal of Behavioral Medicine, 18(3), 199–208.
40. Wilcox, S., Dowda, M., Griffin, S., Rheaume, C., Ory, M., Leviton, L., ... Mockenhaupt, R. (2006). Results of the first year of active for life: Translation of 2 evidence-based physical activity programs for older adults into community settings. American Journal of Public Health, 96(7), 1201–1209.
41. Hughes, S., Seymour, R., Campbell, R., Huber, G., Pollak, N., Sharma, L., & Desai, P. (2006). Long-term impact of Fit and Strong! on older adults with osteoarthritis. The Gerontologist, 46(6), 801–814.
42. Furman, E. F. (2006). Undernutrition in older adults across the continuum of care. Journal of Gerontological Nursing (32)1, 22–27.
43. Hays, N., & Roberts, S. (2006). The anorexia of aging in humans. Physiology & Behavior, 88(3), 257–266.
44. Mentes, J. (2006). Oral hydration in older adults: greater awareness is needed in preventing, recognizing, and treating dehydration. The American Journal of Nursing, 106(6), 40–49.
45. Lane, N. (2006). Epidemiology, etiology, and diagnosis of osteoporosis. American Journal of Obstetrics and Gynecology, 194(2 Suppl), S3–S11.
46. Saunders, M. (1997). Nutrition and oral health in the elderly. Dental Clinics of North America, 41(4), 681–698.

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 15
47. Johnson, M. A., Park, S., Penn, D., McClelland, J. W., Brown, K., & Adler, A. (2008.) Nutrition education issues for older adults. The Forum for Family and Consumer Issues, 13(3).
48. Food Research and Action Center. Seniors and SNAP/Food Stamps. Retrieved from http://frac.org/initiatives/addressing-senior-hunger/seniors-and-snapfood-stamps/.
49. Gollub, E., & Weddle, D. (2004). Improvements in nutritional intake and quality of life among frail homebound older adults receiving home-delivered breakfast and lunch. Journal of the American Dietetic Association, 104(8), 1227–1235.
50. Mitchell, R., Ash, S., & McClelland, J. (2006). Nutrition education among low-income older adults: A randomized intervention trial in Congregate Nutrition sites. Health Education & Behavior: The Official Publication of the Society For Public Health Education, 33(3), 374–392.
51. National Council on Aging. (2005). Using the evidence base to promote healthy aging: the model programs project. Retrieved from http://www.ncoa.org/improve-health/center-for-healthy-aging/content-library/IB_ModelProgramsProject.pdf.
52. Kunkel, M., Luccia, B., & Moore, A. (2003). Evaluation of the South Carolina seniors farmers’ market nutrition education program. Journal of the American Dietetic Association, 103(7), 880–883.
53. Johnson, D., Beaudoin, S., Smith, L., Beresford, S., & LoGerfo, J. (2004). Increasing fruit and vegetable intake in homebound elders: The Seattle Senior Farmers’ Market Nutrition Pilot Program. Preventing Chronic Disease, 1(1), A03.
54. National Alliance on Mental Illness. (2009). Depression in older persons fact sheet. Retrieved from http://www.ncoa.org/improve-health/center-for-healthy-aging/content-library/Depression_Older_Persons_FactSheet_2009.pdf.
55. Centers for Disease Control and Prevention and National Association of Chronic Disease Directors. (2008). The state of mental health and aging in America. Issue brief no. 1. Atlanta, GA: National Association of Chronic Disease Directors. Retrieved from http://www.cdc.gov/aging/pdf/mental_health.pdf.
56. Unützer J, Schoenbaum M, Katon, W., Fan, M., Pincus, H., Hogan, D., & Taylor, J. (2009). Health care costs associated with depression in medically ill fee-for-service Medicare participants. Journal of the American Geriatric Society, 57(3), 375–584.
57. Substance Abuse & Mental Health Services Administration. Depression and anxiety prevention for older adults. Retrieved from http://www.ctrsctraining.com/pdfs/Depression_Booklet.pdf.
58. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web-based Injury Statistics Query and Reporting System (WISQARS).
59. Conwell, Y. (2001). Suicide in later life: A review and recommendations for prevention. Suicide and Life Threatening Behavior, 31(Suppl), 32–47.
60. Substance Abuse & Mental Health Services Administration. Depression and anxiety prevention for older adults. Retrieved from http://www.ctrsctraining.com/pdfs/Depression_Booklet.pdf.
61. Ciechanowski, P., Wagner, E., Schmaling, K., Schwartz, S., Williams, B., Diehr, P., ... LoGerfo, J. (2004). Community-integrated home-based depression treatment in older adults: A randomized controlled trial. JAMA, 291(13), 1569–1577.
62. Quijano, L. M., Stanley, M. A., Petersen, N. J., Casado, B. L., Steinberg, E. H., Cully, J. A., & Wilson, N. L. (2007). Healthy IDEAS: A depression intervention delivered by community-based case managers serving older adults. Journal of Applied Gerontology, 26, 139–156.
63. Madhusoodanan, S., Ibrahim, F., & Malik, A. (2010). Primary prevention in geriatric psychiatry. Annals of Clinical Psychiatry: Official Journal of the American Academy of Clinical Psychiatrists, 22(4), 249–261.
64. AARP. (2010, November). Home and community preferences of the 45+ population. Retrieved from http://assets.aarp.org/rgcenter/general/home-community-services-10.pdf.
65. Center for Housing Policy. (2012). Housing an aging population: Are we prepared? Retrieved from http://www.nhc.org/media/files/AgingReport2012.pdf.
66. AARP Public Policy Institute. The new reality: Important facts about America’s seniors. Retrieved from http://assets.aarp.org/rgcenter/ppi/econ-sec/fs230-economic.pdf.
67. AARP. (2006). Section 202 supportive housing for the elderly. Retrieved from http://www.aarp.org/home-garden/housing/info-2006/fs65r_housing.html.
68. MetLife Mature Market Institute. (2011, October.) Market survey of long-term care costs. Retrieved from https://www.metlife.com/assets/cao/mmi/publications/studies/2011/mmi-market-survey-nursing-home-assisted-living-adult-day-services-costs.pdf.
69. Spillman, B., Biess, J., & MacDonald, G. (2012, April). Housing as a platform for improving outcomes for older renters. Urban Institute. Retrieved from http://www.urban.org/publications/412553.html.

Altarum Institute September 2012
Recommendations to Promote Health and Well-Being Among Aging Populations 16
70. Center for Housing Policy. (2012). Housing an aging population: Are we prepared? Retrieved from http://www.nhc.org/media/files/AgingReport2012.pdf.
71. National Council on Aging. BenefitsCheckUp. Retrieved from http://www.benefitscheckup.org/find-help/.
72. Dannenberg, A., Jackson, R., Frumkin, H., Schieber, R., Pratt, M., Kochtitzky, C., & Tilson, H. (2003). The impact of community design and land-use choices on public health: A scientific research agenda. American Journal of Public Health, 93(9), 1500–1508.
73. Nelson, A. C. (2004, December). Toward a new metropolis: The opportunity to rebuild America. Washington, DC: Brookings Institution.
74. Srinivasan, S., O’Fallon, L., & Dearry, A. (2003). Creating healthy communities, healthy homes, healthy people: Initiating a research agenda on the built environment and public health. American Journal of Public Health, 93(9), 1446–1450.
75. National Conference of State Legislatures and the AARP Public Policy Institute. (2011, December). Aging in place: A state survey of livability policies and practices. Retrieved from http://www.aarp.org/home-garden/livable-communities/info-11-2011/Aging-In-Place.html.
76. Atlanta Regional Commission. Lifelong communities. Retrieved from http://www.atlantaregional.com/aging-resources/lifelong-communities-llc.
77. Dannenberg, A., Jackson, R., Frumkin, H., Schieber, R., Pratt, M., Kochtitzky, C., & Tilson, H. (2003). The impact of community design and land-use choices on public health: A scientific research agenda. American Journal of Public Health, 93(9), 1500–1508.
78. Srinivasan, S., O’Fallon, L., & Dearry, A. (2003). Creating healthy communities, healthy homes, healthy people: Initiating a research agenda on the built environment and public health. American Journal of Public Health, 93(9), 1446–1450.