Allelo typing of Endometriosis with Adjacent Ovarian ...dometriosis, and in three cases (cases 78,...
7
[CANCER RESEARCH 58. 1707-1712. April 15. 1998] Allelo typing of Endometriosis with Adjacent Ovarian Carcinoma Reveals Evidence of a Common Lineage1 Xiuxian Jiang, Sarah J. Morland, Andrew Hitchcock, Eric J. Thomas, and Ian G. Campbell2 Obsieirics and Gynecology. University of Southampton, Princess Anne Hospital, Southampton SOI6 SÕA [X. J., S. J. M., E. J. T., I. G. C.], and Department of Hislopalhology, Southampton General Hospital. Southampton SOln 6YD [A. H.ÃOE. United Kingdom ABSTRACT Endometriosis is a common gynecological disease in which tissue sim ilar to the endometrium proliferates at sites outside the uterine cavity. Malignant transformation of endometriosis to endometrioid and clear cell ovarian carcinomas has been documented in histológica!studies, but no molecular genetic evidence exists to support that endometriosis is the clonal precursor of such malignancies. We examined 14 cases of endo metriosis synchronous with ovarian cancer for loss of heterozygosity on 12 chromosome arms, X chromosome inactivation, and TP53 mutation to determine whether they shared genetic alterations. In all four of the cases where the carcinoma had arisen within endometriosis and in five of the seven cases where the carcinoma was adjacent to the endometriosis, common genetic lesions were detected, consistent with a common lineage. A 77*53mutation was also detected in one case of endometriosis adjacent to carcinoma. These findings support the numerous histológica! observa tions that endometrioid and clear cell ovarian carcinomas may arise through malignant transformation of endometriotic lesions. INTRODUCTION Endometriosis is a common gynecological disease in which endo- metrial-like glandular epithelium and stroma is found at locations outside the uterine cavity, most commonly the ovary. The most likely origin of the disease is implantation of viable endometrium refluxed into the peritoneal cavity during menstruation (1). Although endo metriosis generally follows a benign course, it does exhibit some characteristics reminiscent of malignancy, including local invasion and métastases.A relationship between endometriosis and endometri oid and clear cell cancers of the ovary have long been suspected based on their frequent co-occurrence in surgical specimens (2-5). Based on histológica! observations and clinically documented cases, the fre quency of malignant transformation of ovarian endometriosis is about 1%, but the actual frequency is probably significantly higher. In a long-term follow-up of over 20,000 Swedish women hospitalized for endometriosis, Brinton et al. (6) observed a 1.9 relative risk of ovarian cancer. The risk increased dramatically to 4.2 (95% confidence inter val, 2.0-7.7) among subjects with a long-standing history of ovarian endometriosis. Many of the risk factors associated with both endometriosis and ovarian cancer are the same and include earlier menarche, more regular periods, shorter cycle lengths, and lower parity. For endo metriosis, the increased risk is consistent with an increased opportu nity for menstrual contamination of the peritoneal cavity, whereas for ovarian cancer, these factors are thought to increase the number of ovulations and therefore the potential for malignant transformation of damaged epithelium. However, it is possible that part of the increased ovarian cancer risk is due to an increased risk of endometriosis- associated endometrioid and clear cell subtypes. This idea is sup- Received 9/18/97; accepted 2/18/98. The costs oÃ-publication of this article were defrayed in part by the payment of page charges. This article must therefore he hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 Supported by grants from Wellbeing and The Wessex Medical Trust. 2 To whom reprints should be addressed, at Obstetrics and Gynaecology. University of Southampton. Level F. Princess Anne Hospital, Coxford Road. Southampton SO 16 5YA. UK. ported by Rosenblatt and Thomas (7), who found that tubai ligation, which prevents menstrual reflux and is protective for endometriosis, was also protective for clear cell and endometrioid ovarian cancers (relative risks of 0.2 and 0.32) but not serous and mucinous cancers. Although much of the data are circumstantial, there does appear to be a strong case for suggesting that endometriosis has malignant poten tial and is the precursor of some, and possibly all, endometrioid and clear cell ovarian cancers. The first molecular genetic evidence that at least a subset of endometriotic lesions may be premalignant came from our analysis for LOH1 at candidate ovarian TSG loci in a series of 40 cases of endometriosis (8). We detected LOH on chromosome arms 9p. llq, and 22q in 28% of cases, suggesting that the development of endo metriosis might require the inactivation of the same set of TSGs involved in ovarian tumorigenesis. In this study, we have extended these findings by analyzing for genetic alterations present in endo metriosis synchronous with ovarian carcinoma to determine whether the carcinoma had arisen de novo or by clonal expansion from the endometriosis. MATERIALS AND METHODS Source of Specimens. Fourteenarchivalparaffin-embeddedspecimensof ovarian endometriosis synchronous with ovarian carcinoma were accessed through the Department of Pathology, Southampton General Hospital. Histo- logical diagnosis was confirmed by a specialist gynecological pathologist (A. H.) and are summarized in Table 1. Additionally. 17 endometrioid ovarian carcinomas without evidence of synchronous endometriosis were accessed either as fresh tumor biopsies or as archival paraffin-embedded specimens. Microdissection and DNA Extraction. DNA was extractedfromselected regions by microdissection as described previously (8). Briefly, serial 10-fj.m- thick sections were dewaxed in xylene and hydrated in 95% ethanol. One section was stained with H&E and mounted with a coverslip and used as a template. The remaining sections were mounted onto slides but left unstained for tissue removal. The areas of interest were scraped off using a 21-gauge needle under a dissecting microscope. For each case, cells were dissected from at least four consecutive sections. Clonality Analysis. Clonalityanalysis was performedby assessing the X chromosome inactivation pattern of the human androgen receptor (AR)gene as described previously (8). LOH Analysis. The following markerswere usedto assess for LOHon the following chromosome regions: 2q (D2S95), 4q (D4S395), 4q (D4SÃOE75), 5p (D5S406), 5ql3.1-14 (D5S424), 5q (D5S346). 5q22.3-3l.3 (D5S399), 6ql4 (D6S300). 6ql4-15 (D6S284). 7pl3 (D7S69I). 7pl5-pter (D7S48ÃOE), 9p21 (D9SI7I, D9SI6I). \\q23-ler (Dl 1SI336 und Dl 1S1328), 17pl3.1 (TP53CA), 17q21 (DI7S855), 17q21 (D17S806). 22ql3 (D22S304. PDGFB. D22S284, D22S302, CYP2D6, and D22S274) and Xql 1.2-12 (AR). The sequences of the primers were obtained from various databases accessed through the National Center for Human Genome Research (http://www.nih.gov). Details of the PCR conditions and analysis of PCR products have been described previously (8). SSCP and Sequencing Analysis of TP53. PCR amplificationof exons 5-8 of TP53 were performed in the carcinoma and endometriosis components of all 14 cases using the primers and conditions described previously (9-11). Statistical Calculations. The probabilityof common LOH events occur ring as independent events were calculated according to Jacobs et al. (12) with 1The abbreviations used are: LOH. loss of heterozygosily; TSG, tumor suppressor gene. 1707 on August 3, 2020. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Transcript of Allelo typing of Endometriosis with Adjacent Ovarian ...dometriosis, and in three cases (cases 78,...

[CANCER RESEARCH 58. 1707-1712. April 15. 1998]
Allelo typing of Endometriosis with Adjacent Ovarian Carcinoma Reveals Evidenceof a Common Lineage1
Xiuxian Jiang, Sarah J. Morland, Andrew Hitchcock, Eric J. Thomas, and Ian G. Campbell2
Obsieirics and Gynecology. University of Southampton, Princess Anne Hospital, Southampton SOI6 SÕA [X. J., S. J. M., E. J. T., I. G. C.], and Department of Hislopalhology,Southampton General Hospital. Southampton SOln 6YD [A. H.Ì.United Kingdom
ABSTRACT
Endometriosis is a common gynecological disease in which tissue similar to the endometrium proliferates at sites outside the uterine cavity.Malignant transformation of endometriosis to endometrioid and clear cellovarian carcinomas has been documented in histológica!studies, but nomolecular genetic evidence exists to support that endometriosis is theclonal precursor of such malignancies. We examined 14 cases of endometriosis synchronous with ovarian cancer for loss of heterozygosity on 12chromosome arms, X chromosome inactivation, and TP53 mutation todetermine whether they shared genetic alterations. In all four of the caseswhere the carcinoma had arisen within endometriosis and in five of theseven cases where the carcinoma was adjacent to the endometriosis,common genetic lesions were detected, consistent with a common lineage.A 77*53mutation was also detected in one case of endometriosis adjacent
to carcinoma. These findings support the numerous histológica!observations that endometrioid and clear cell ovarian carcinomas may arisethrough malignant transformation of endometriotic lesions.
INTRODUCTION
Endometriosis is a common gynecological disease in which endo-metrial-like glandular epithelium and stroma is found at locations
outside the uterine cavity, most commonly the ovary. The most likelyorigin of the disease is implantation of viable endometrium refluxedinto the peritoneal cavity during menstruation (1). Although endometriosis generally follows a benign course, it does exhibit somecharacteristics reminiscent of malignancy, including local invasionand métastases.A relationship between endometriosis and endometrioid and clear cell cancers of the ovary have long been suspected basedon their frequent co-occurrence in surgical specimens (2-5). Based on
histológica! observations and clinically documented cases, the frequency of malignant transformation of ovarian endometriosis is about1%, but the actual frequency is probably significantly higher. In along-term follow-up of over 20,000 Swedish women hospitalized for
endometriosis, Brinton et al. (6) observed a 1.9 relative risk of ovariancancer. The risk increased dramatically to 4.2 (95% confidence interval, 2.0-7.7) among subjects with a long-standing history of ovarian
endometriosis.Many of the risk factors associated with both endometriosis and
ovarian cancer are the same and include earlier menarche, moreregular periods, shorter cycle lengths, and lower parity. For endometriosis, the increased risk is consistent with an increased opportunity for menstrual contamination of the peritoneal cavity, whereas forovarian cancer, these factors are thought to increase the number ofovulations and therefore the potential for malignant transformation ofdamaged epithelium. However, it is possible that part of the increasedovarian cancer risk is due to an increased risk of endometriosis-associated endometrioid and clear cell subtypes. This idea is sup-
Received 9/18/97; accepted 2/18/98.The costs oÃpublication of this article were defrayed in part by the payment of page
charges. This article must therefore he hereby marked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
1Supported by grants from Wellbeing and The Wessex Medical Trust.2 To whom reprints should be addressed, at Obstetrics and Gynaecology. University of
Southampton. Level F. Princess Anne Hospital, Coxford Road. Southampton SO 16 5YA.UK.
ported by Rosenblatt and Thomas (7), who found that tubai ligation,which prevents menstrual reflux and is protective for endometriosis,was also protective for clear cell and endometrioid ovarian cancers(relative risks of 0.2 and 0.32) but not serous and mucinous cancers.Although much of the data are circumstantial, there does appear to bea strong case for suggesting that endometriosis has malignant potential and is the precursor of some, and possibly all, endometrioid andclear cell ovarian cancers.
The first molecular genetic evidence that at least a subset ofendometriotic lesions may be premalignant came from our analysisfor LOH1 at candidate ovarian TSG loci in a series of 40 cases of
endometriosis (8). We detected LOH on chromosome arms 9p. llq,and 22q in 28% of cases, suggesting that the development of endometriosis might require the inactivation of the same set of TSGsinvolved in ovarian tumorigenesis. In this study, we have extendedthese findings by analyzing for genetic alterations present in endometriosis synchronous with ovarian carcinoma to determine whetherthe carcinoma had arisen de novo or by clonal expansion from theendometriosis.
MATERIALS AND METHODS
Source of Specimens. Fourteenarchivalparaffin-embeddedspecimensofovarian endometriosis synchronous with ovarian carcinoma were accessedthrough the Department of Pathology, Southampton General Hospital. Histo-logical diagnosis was confirmed by a specialist gynecological pathologist(A. H.) and are summarized in Table 1. Additionally. 17endometrioid ovariancarcinomas without evidence of synchronous endometriosis were accessedeither as fresh tumor biopsies or as archival paraffin-embedded specimens.
Microdissection and DNA Extraction. DNA was extractedfromselectedregions by microdissection as described previously (8). Briefly, serial 10-fj.m-thick sections were dewaxed in xylene and hydrated in 95% ethanol. Onesection was stained with H&E and mounted with a coverslip and used as atemplate. The remaining sections were mounted onto slides but left unstainedfor tissue removal. The areas of interest were scraped off using a 21-gaugeneedle under a dissecting microscope. For each case, cells were dissected fromat least four consecutive sections.
Clonality Analysis. Clonalityanalysis was performedby assessing the Xchromosome inactivation pattern of the human androgen receptor (AR)gene asdescribed previously (8).
LOH Analysis. The following markerswere usedto assess for LOHon thefollowing chromosome regions: 2q (D2S95), 4q (D4S395), 4q (D4SÌ75),5p(D5S406), 5ql3.1-14 (D5S424), 5q (D5S346). 5q22.3-3l.3 (D5S399), 6ql4(D6S300). 6ql4-15 (D6S284). 7pl3 (D7S69I). 7pl5-pter (D7S48Ì),9p21(D9SI7I, D9SI6I). \\q23-ler (Dl 1SI336 und Dl 1S1328), 17pl3.1 (TP53CA),17q21 (DI7S855), 17q21 (D17S806). 22ql3 (D22S304. PDGFB. D22S284,D22S302, CYP2D6, and D22S274) and Xql 1.2-12 (AR). The sequences of theprimers were obtained from various databases accessed through the NationalCenter for Human Genome Research (http://www.nih.gov). Details of the PCRconditions and analysis of PCR products have been described previously (8).
SSCP and Sequencing Analysis of TP53. PCR amplificationof exons5-8 of TP53 were performed in the carcinoma and endometriosis componentsof all 14 cases using the primers and conditions described previously (9-11).
Statistical Calculations. The probabilityof common LOH events occurring as independent events were calculated according to Jacobs et al. (12) with
1The abbreviations used are: LOH. loss of heterozygosily; TSG, tumor suppressor
gene.
1707
on August 3, 2020. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

CaseAgePathologyTissuesourceHistology'@Locations'StageGrade3847E,
no atypiaECWithinlaIPP7876E,
E, severe atypiaECWithin WithinlaIIP
PP10868E,
E, severe atypiaEC/MCWithin WithinlaIIP
PP26734E
E, severe atypiaECWithin WithinlaIIp
PP841E,noatypia
ECAdjacentNANAPP3059E,no atypia
EC/CCAdjacent3IIIPF3654E,noatypia
ECAdjacentlaIPF13680E,noatypia
ECAdjacentIIllPF20265E,no atypia
ECAdjacent2IPF28757E,no atypia
ECAdjacent1IPPPE6
9NA 47E,
no atypiaECE, no atypiaECAdjacent
Right ovaryLeftovaryNA NANA NAP
PP
P7055E,no atypia
EC/CCRightovary
LeftovaiylaIPF9060E,noatypia
MCLeftovary RightovarylcIP P
. @:@‘ •@
.-
@ @--
ENDOMETRIOSIS AND O@ARlAN CANCER
Table I Clinical and pathologicalfeatures of endometriosis synchronous withovarian carcinoma
after menopause, consistent with the loss of gonadal hormone support.However, 6 of our 14 cases showed clear histological features ofactive endometriosis (endometrial glands and stroma), including an80-year-old patient.
In four cases (cases 38, 78, 108, and 267), the carcinoma waspresent within the endometriotic cyst and was of endometrioid ormixed endometrioid and mucinous subtypes. Three of these cases alsocontained areas of endometriosis with cytological atypia (cases 78,108, and 267). In seven cases, the carcinoma was located adjacent tothe endometriosis (cases 8, 30, 36, 136, 202, 287, and PE6) and wereof the endometrioid or mixed endometrioid and clear cell subtypes. Inthe remaining three cases, the carcinoma and endometriosis werepresent in contralateral ovaries and were of endometrioid, mucinous,or mixed endometrioid and clear cell subtypes.
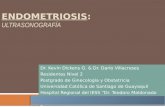
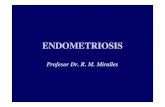
Microtlissection and DNA Extraction. Areas of carcinoma, endometriosis, and in three cases (cases 78, 108, and 267) atypicalendometriosis were carefully microdissected from surrounding normal areas as illustrated for case 38 in Fig. 1. In cases of mixed ovariancancer subtypes, only areas of endometrioid carcinoma were microdissected. Cells were microdissected from at least four consecutivesections for each case. In case PE6, there were several endometrioticcysts adjacent to the carcinoma (Fig. 2). DNA was extracted fromthree of these endometriotic cysts (El, E2, and E3). El was analyzedfor clonality, LOH, and TP53 mutation, whereas E2 and E3 wereanalyzed for TP53 mutation only.
7
,e@ A@@
Fig. I. Top, H&E-stained ovarian endometrioid ovarian carcinoma arising from withinan endometriotic cyst (case 38) before microdissection. EC, endometrioid carcinoma; E.endometriosis. Bottons@same section as Top after microdissection. Arrows, the dissectedcell populations, which were subjected to DNA analysis. EC-a, endometrioid carcinomaarea after dissection; E-a, endometriosis area after dissection.
a E, endometriosis; EC, endometrioid ovarian carcinoma; MC, mucinous carcinoma;
CC, clear cell carcinoma; NA, not available; P. formalin-fixed, paraffin-embedded tissue;F, fresh tissue.
b Adjacent, carcinoma and endometriosis were present in the same slide; Within,
carcinomas were arising within the endometriotic cyst.
the modification ofAbeln a al. (13) using the formula P = p(LOH ofthe sameallele) X p(LOH at the same locus) X p(same clonality). Where n deposits oftissue have LOH for a polymorphism, the probability ofeach deposit losing thesame allele as an independent event is (½)@ @.If the endometriosis with andwithout atypia is considered as a single deposit, then in this study n = 2, andthe probability of the endometriosis and carcinoma losing the same allele as anindependent event is (½)2 _ I 0.5. However, this is an overestimate because
it does not take into account the probability of an LOH occurring at a specific
locus. Thus, if LOH is present in endometriosis, the probability of LOHoccurring at the same locus in the carcinoma as an independent event is thefraction of the locus-specific LOH frequencies. For the clonality study, because one X chromosome is inactivated in all cells, the probability that ndeposits of a tumor have the same X chromosome inactivated as an independent event is simply (½)@@ (½)2_ I 0.5.
RESULTS
Histological Features of Cases with Synchronous Endometriosisand Ovarian Cancer. Fourteen cases of ovarian endometriosis synchronous with ovarian carcinoma (Table 1), presenting between 1991and 1995, were analyzed. In each case, histological diagnosis wasconfirmed by a specialist gynecological pathologist (A. H. ). Eightcases (cases 38, 70, 78, 90, 108, 267, 8, and 9) were identified afterreviewing 220 endometriosis pathology reports. The remaining sixcases (cases 30, 36, 136, 202, 287, and PE6) were identified afterreexamination of tissue slides from 19 ovarian endometrioid carcinomas cases. In none of these six cases was the presence of synchronousendometriosis noted in the pathological report.
An interesting feature of these patients was that the majority (9 of13, 70%) were >50 years of age and likely to be postmenopausal. Inthe vast majority of women, endometriotic implants become atrophic
I
E
@,
. ,
_.4.)
._,
i-@.. B-a
,@@@
1708
on August 3, 2020. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

ENDOMETRIOSIS AND OVARIAN CANCER
Ei
E3
X
F\g. 2. Case PE6 showing an endomctrioid ovarian carcinoma (77) with severaladjacent endometriotic cysts (EI, £2.and E3).
DNA derived from paraffin-embedded tissue is commonly dam
aged and/or present in minute amounts and can cause PCR artifacts(such as random preferential alÃeleamplification), which can confusethe interpretation of LOH and clonality assays. A critical factor ineliminating such artifacts is to extract DNA from as many cells aspossible to maximize the DNA yield. The smallest number of cells weused was on the order of 400 cells (for example, cyst 3 in Fig. 2 has—100 cells, and four sections were extracted). Because the DNA was
extracted into a final volume of 30 /il, each 1 ¡Aused per PCR
reaction contained —12genomes. This represents the smallest number, and in most cases, DNA was extracted from at least 2()(X)-5(X)()
cells. To distinguish preferential alÃeleamplification from true LOH,all experiments were repeated at least three times, and a locus wasonly scored as showing LOH when it was observed on every occasion.As a further control, the normal DNA controls included not onlypurified high molecular weight blood DNA but also normal archivalendometrium or normal areas from the same slide as the endometri-
osis. Only when LOH was observed consistently in independentexperiments and no loss was observed in the normal archival DNAwas a locus scored as showing LOH.
Clonality Analysis. Assessment of clonality was only possible forcases 9, 108, and PE6; the endometriosis and carcinoma areas weremonoclonal (Table 2). In cases 106 and PE6, the same X chromosomeinactivation pattern was observed in the endometriosis and adjacentcarcinoma, whereas in case 9, where the carcinoma and endometriosiscomponents were present on contralateral ovaries, the X-inactivation
involved the opposite alÃeles.LOH Analysis. LOH analysis was performed on all components of
the 14 cases of endometriosis synchronous with ovarian carcinomaand the 17 solitary ovarian endometrioid ovarian carcinomas using 25microsatellite markers on the following chromosome regions: 2q, 4q,5p, 5q, 6q, 7p, 9p, llq, 17p, 17q, 22q, and Xq. These regions wereselected for the study either because they are thought to harbor TSGsinvolved in the development of ovarian and other epithelial cancers(14-15) or have been reported to be specifically involved in endo
metrioid ovarian cancer (16).The LOH results for the 14 cases of endometriosis synchronous
Table 2 Allelotype of endometriosis and synchronous ovarian carcinotntl
2q4qCase38
EEC/CCE78
AtyECE108
AtyEC/MCE267
AtyEC8
EEC30
EEC/CC36
EEC136
EEC202
EEC287
EECPE
E6EC9
EEC70
EEC/CC90
EMCSite''wwwwwwwaaaaaaaRLLRLRClonality'NININDNDNDDNWSameSameNININIDNWDNWDNWDNWDNWDNWDNWDNWDNWDNWNINISameSameDIFFDIFFNDNDDNWDNW95HHLHLHHHHHLHH395HHHHHHHLLHHHLHHHHHH175HHHHLLHHHHHHHHHH5p406
424HHHHHHLH
HHLHHHLLLHHLLHHHHHH5q346HLHHHHLHHLLHLHH6q399HHHHHHLHHHLHHHL300HHHHHHHHLLHLHHHLHHHH284HHHHHHHLLLHHLH7p691HHHHHHHHHHLHHHH481HHHHHHHLHLHHHLHHHH9p171HHHHLHHHHHHLLHHHHHHHLHL161LLHLLLLLHHHLHLHHHHHLHHHHLOHllq1328LLLHHHHHHL1336LLHHHHHHHHHHHHHHLHHa17pTP53HHHHHHLHLHHHH17q855HHHHHHHIIHHHHLHLHHHLHLHLHH806
304PDGFBHLLLLLHHHHHHHLHH284HIIHHHHHHHLHHHLHIIHHHHHH22q302CYP2DHHHHIIHH
IIHMHHLLHHL
HHLHH27h
274HHLLLHHHHIILIILHHHLHHHHXqARHHLHHHHHHHHLHHTP531'NNNNNNNNNNMNNNMNNNNNNNNM'NNNNNNN
" H, heterozygous; L, loss of heterozygosity; blank space, not informative; E, endometriosis; Aty. endometriosis with atypia; EC, endometrioid carcinoma; CC. clear cell carcinoma;
MC, mucinous carcinoma.*The location of the endometriosis with atypia and/or carcinoma relative to the endometriosis. w. within; a. adjacent.c Clonality w;th respect to the endomelriosis: Same, endometriosis and carcinoma are monoclonal and show the same X chromosome inaction: DIFF. endometriosis and carcinoma
are monoclonal but show the opposite X chromosome inactivation pattern; NI, not informative; DNW, did not work; ND, not done.d N, no TP53 mutation as assessed by SSCP; M. TP53 mutation as detected by SSCP and confirmed by direct sequence analysis.'The TP53 mutation was present in cyst E3 only. The LOH data were derived from cyst El.
1709
on August 3, 2020. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Table 3 Stage and grade of endometrioid ovarian carcinoma with andwithoutsynchronousendometriosisThe
cases of early stage (stage 1) and late stage (stages 2 and 3) and low grade (gradeI) and high grade(grades II and ifi) were analyzed by y@test at a significance ofP <0.05:P
= 0.349 for stage and P = 0.005 forgrade.Stage
GradeI
2 3 I IIIIISolitary
EC― 56% 25% 19% 0 67%33%9/164/16 3/16 0/15 10/155/15EC
with E― 82% 9% 9% 55% 27%18%9/11I/Il 1/li 6/11 3/112111Total
67% 19% 15% 22% 48%26%18/275/27 4/27 6/27 13/277/27a
@ endometrioid carcinoma; E, endometriosis. Only 16 cases were availableforsta'e
and 15 for grade.Only 11 cases were available for stage and grade.
END0ME'rRIosIsANDOVARIANCANCER
Nb N E I TP53 Mutation Analysis. TP53 mutations were detected in the
‘Ida.'. carcinoma components of cases 30 (CGT>TGT, codon 273) and 267
@ (l-bp deletion in codon 152), but these were not detected in the
—@ .@ adjacent endometriosis components. However, in case PE6 where the
carcinoma was surrounded by three apparently independent endometriotic cysts (Fig. 2), a Tyr-to-Cys mutation in codon 220 was
C::@:: detected in endometriosis cyst E3 but surprisingly not in the adjacentcarcinoma. Only one TP53 mutation (GTC>GAC codon 157) wasdetected among the 17 cases of solitary endometrioid ovarian cancers.
LOH in Endometrioid Ovarian Carcinoma. A total of 31 endoNb N E T metrioid ovarian carcinomas were analyzed and comprised the 14
cases synchronous with endometriosis and 17 without evidence of. —. T synchronous endometriosis. Comparison of the grade and stage (Table
w-.@ 3) demonstrated that the cases with synchronous endometriosis were
more frequently early stage and low grade than those without associated endometriosis, although only the association with grade was
d9S171 statistically slgmficant ( test, P = 0.005).The locus-specific LOH frequencies did not differ significantly
between the groups with and without endometriosis so the LOHfrequencies were combined (Table 4). LOH among the carcinomaswas common with 29 of 31 (94%) showing LOH with at least onemarker. LOH was detected on all chromosome arms with frequenciesbetween 14% for chromosome 5p and 54% for chromosome 9p. Thefrequency of LOH with respect to tumor grade and stage for bothgroups were assessed, but because the numbers in each group weresmall, no statistically significant correlations were evident. However,LOH on chromosome arms 5q, 9p, llq, l7p, 22q, and Xq wererelatively common in grade 1 (40%—80%)and/or stage I (33%—57%)tumors, suggesting these are early events in endometrioid tumorigenesis.
LOH in Endometriosis. We have reported previously LOH analysis of 40 cases of solitary endometriosis using a limited number ofchromosome arms. We extended the LOH analysis to include all ofthe markers used for the synchronous cases, and the results aresummarized in Table 4. To calculate the overall frequency of LOH inendometriosis, the results for the 14 endometriosis cases synchronouswith ovarian carcinoma have been included in the calculations.
Twenty-three of the 54 (43%) endometriosis cases demonstratedLOH with one or more markers on chromosome arms 4q (2%), Sq(10%), 6q (7%), 9p (21%), 1lq (19%), and 22q (19%). Nine cases(17%) showed LOH on two chromosome arms and two (4%) showedLOH on three chromosome arms.
Comparison of LOll in Endometriosis and Endometrloid Carcinoma. A comparison of the LOH frequencies detected in solitaryendometriosis, endometriosis synchronous with carcinoma and solitary endometrioid ovarian carcinoma is shown in Table 4. The overallLOH frequency among all of the endometriosis cases was lower and
NbN E T NbN E A T N E T
@@ .@
Case 38Case 78CasePE6d22S274d11S1328d5S424
NbNEAT NET N E T
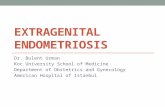
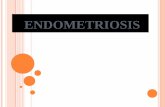
Fig. 3. LOH analysis. The case number and microsatellite marker used are indicatedbelow each autoradiograph. Nb, normal DNA extracted from blood lymphocytes; N, DNAextracted from normal stromal areas of the paraffin section; E, endometriosis DNA; A,endometriosis with atypia DNA; T, ovarian tumor DNA.
with ovarian carcinoma are summarized in Table 2. Among thecarcinoma components, a total of 65 LOH events were detected, withall showing LOH with at least one marker. Seventeen of these LOHevents, occurring in nine cases (case 30, 36, 38, 78, 108, 136, 202,267, and PE6), were also detected in the associated endometriosis,examples of which are shown in Fig. 3. In all 17 instances, the LOHinvolved the same allele as the associated carcinoma, consistent witha common lineage. There was only one LOH event detected inendometriosis that was not also present in the carcinoma (Fig. 3), butthis occurred in case 90, where the endometriosis and carcinoma werefrom contralateral ovaries. None of the three cases where the endometriosis and carcinoma were from contralateral ovaries displayedany common LOH. Five of the seven cases with carcinoma adjacentto the endometriosis displayed common LOH events. All four caseswith the carcinoma arising within the endometriotic cysts (cases 38,78, 108, and 267) displayed at least two common LOH events. Inparticular, case 38 harbored three common LOH events on 9p, 1lq,and 22q. The LOH on 9p and 22q appeared to encompass an identicalregion in the endometriosis and carcinoma because adjacent microsatellite markers were heterozygous.
In some cases, the LOH detected in the endometriosis componentsinvolved smaller regions than observed in the associated carcinoma.In particular, LOH on chromosome Sq in cases 36 and PE6 wasobserved only with marker D5S346 and D5S424, respectively,whereas the carcinoma had LOH with all of the Sq markers.
The probability that these common LOH occurred as independentevents were calculated according to Jabobs et a!. (12) with themodification of Abeln et a!. (13), which takes into account theprobability of LOH occurring at a specific locus. The locus-specificprobabilities were derived from the observed LOH frequencies observed in our 3 1 cases of endometrioid ovarian cancer and wereestimated to be 0.29 on 4q, 0.46 on Sq. 0.29 on 6q, 0.54 on 9p, 0.37on 1lq, and 0.47 on 22q. The probability of independent origin amongthe nine cases with common LOH ranged from P 0.23 for case 202,where only one common LOH event was observed, to P 0.01 forcase 38 in which three common LOH events were observed. In six ofthe nine cases, the probabilities were P 0.05 or less, indicating thatit is very unlikely that these occurred by chance. Additionally, theseprobability estimates do not take into account the fact that the regionsof LOH in some cases appeared to be identical in each component.
Case 108d22S274
Case9O Case9d68284 PDGFB
1710
on August 3, 2020. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Study EC CC EC/CC S M Other― Total
Fukunaga et aL (5) 13/31 27/50 0/0 6/63 2/35 6/45 54/224Dc Ia Cuesta et al. (4) 9/23 7/17 4/8 0/10 1/18 1/3 22179Vercellini et aL (2) 30/114 8/36 8/36 8/220 6/94 3/52 63/556McMeekin et al. (3) 28191 0/0 0/0 0/0 0/0 0/0 28/91Totalsc 98/259 42/103 12/44 14/293 9/147 10/100 167/950(%) (38%) (41%) (27%) (4%) (6%) (10%) (17%)
a EC, endometrioid carcinoma; CC, clear cell carcinoma; EC/CC, mixed endometrioid and clear cell carcinoma; 5, serous; M, mucinous.b@ includesserousborderline,mucinousborderlinetumors,and mixed mUlleriantumors.C Total for each column.
ENDOME'FRIOSISAND OVARIAN CANCER
Table 4 LOH in solitary endometriosis, endometriosis synchronous with ovariancancer, and endometrioid carcinoma
We detected only three TP53 mutations among the total of 56(5%)endometrioid ovarian carcinomas, which indicates that the TP53 mutation is of less relevance in the development of this histologicalsubtype. The low frequency of mutation in the carcinomas was reflected in the absence of TP53 mutations in any of the 40 solitaryendometriotic cysts we examined in a previous study (8) and in only1 of 14 of the cases reported here. This mutation was detected in cystE3 from case PE6 and was particularly intriguing because it was notdetected in the adjacent carcinoma or endometriotic cysts. This wasunexpected because an endornetriotic cyst harboring a TP53 mutationseemed the most likely precursor of an adjacent carcinoma. LOHanalysis has not been performed on this cyst; therefore, it is notpossible to determine whether it shares some other common geneticalterations that could establish a relationship between the adjacentcarcinoma.
Our previous LOH analysis of 40 solitary endometriotic cystsdemonstrated that about one-third of these harbored deletions onchromosomes 9p, llq, or 22q (8). In this study, we examined additional chromosomes and confirmed that LOH is relatively common onchromosomes 9p (10 of 48, 21%), 1lq (8 of 43, 22%), and 22q (10 of53, 15%), and we also detected LOH on chromosome arms Sq (S of47, 12%) and 6q (3 of 45, 8%). If endometriosis is the precursor ofendometrioid and clear cell ovarian cancers, then LOH on thesechromosomes should also be common in the cancers. Comparison ofthe LOH frequencies (Table 4) revealed a striking trend of increasingLOH on chromosome Sq, 6q, 9p, llq, and 22q in solitary endornetriosis, endometriosis with associated carcinoma, and endometrioid
ovarian carcinoma.As a result of these studies, we are in a position to propose a
preliminary model for the development and malignant transformationof endometriosis. The first step is the implantation and proliferation ofectopic endometriurn. It is not clear whether this is dependent on theacquisition of genetic alterations, but by the time these implants havedeveloped into small endometriotic cysts, over one-third will harborLOH, predominantly on chromosomes 9p, 1lq, or 22q. Because themajority of endometriotic cysts remain benign, these genetic alterations may only be involved in the maintenance of the endometrioticcysts, with other mutations in other genes being required for thepromotion to a premalignant state. The detection of LOH on chromosome Sq in 6% of solitary cysts and 25% of cysts with synchronous
carcinoma suggests that one of these genes may reside on chrornosome Sq. LOH on chromosome 6q first appears in endometriosis withadjacent carcinoma (27% of these cases), and this might be associatedwith malignant transformation. It is interesting to note that Tibiletti eta!. (21) has shown that deletions involving chromosome 6q are verycommon in early ovarian cancers of all histological types and hassuggested that this may be one of the earliest lesions in the pathogen
esis of ovarian cancer. LOH on chromosomes Sq, 9p, 1lq, and 22q arealso common in early-stage and/or low-grade endornetrioid ovariancancers, consistent with the LOH pattern observed in endometriosis.
LOHa
ChromosomearmsSolitary
E(40 cases)E
with EC(14 cases)EC (31cases)2q0%(0/21)0%(0/6)40%(6/15)4q0%
(0/34)8% (1/12)29%(8/28)5p0%(0/21)0% (0/4)14%(1/7)Sq6%(2/35)25% (3/12)46%(13/28)@i0%(0/34)27% (3/1 1)29%(7/24)7p0%(0/24)0%(0/l1)28%(5/18)9p17%
(6/35)31% (4/13)54%(14/26)llql8%(6/33)20%(2/10)37%(10127)lip0%
(0/17)0% (0/6)42%(8/19)17q0%(0/30)0% (0/12)46%(12/26)22q15%(6/40)31% (4/13)47%(14/30)Xq0%(0/22)0% (0/6)38% (6/16)
a E, endometriosis; EC, endometrioid ovarian cancer.
involved fewer loci than the solitary carcinomas. Among the solitaryendometriosis cases, LOH was only detected on chromosome anus5q, 9p, 1lq, and 22q. LOH was also detected at these loci in theendometriosis cases with associated carcinoma, but the frequencieswere consistently higher than in the solitary cases. LOH was alsodetected on chromosome arms 4q and 6q in the endometriosis caseswith carcinoma. Interestingly, the chromosome arms showing thehighest LOH frequencies among the endometriosis cases (Sq, 9p, 1lq,and 22q) were also among those showing frequent LOH in low gradeand early stage endometrioid ovarian cancers.
DISCUSSION
Histological and epidemiological observations have consistentlydemonstrated an association between endometriosis and ovarian cancer (2—5,17—20),and although much of the data are circumstantial,there is a strong case for suggesting that endometriosis has malignantpotential and may be the precursor of some, and possibly all, endometrioid and clear cell ovarian cancers. Our goal has been to test thishypothesis by analyzing for genetic alterations in endometriosis contiguous with, or adjacent to, ovarian carcinoma.
The finding of common LOH events in 9 of 11 (82%) cases ofendomeiriosis with adjacent or contiguous carcinoma supports theview that they have a common genetic lineage. These common geneticalterations are very unlikely to have occurred as independent eventsbased on statistical analysis and because in some cases they encompassed the same small chromosomal segment. The possibility that theareas of endometriosis in these cases represented differentiated cornponents ofthe carcinomas is not supported by the fact that in all cases,the endometriosis harbored fewer genetic alterations than the carcinoma,as wouldbe expectedif it werethe precursorof the tumor.Theonly cases where a common lineage could not be established werethose cases in which the endometriosis and carcinoma were obtainedfrom contralateral ovaries.
Table 5 Summary of reported incidence of endometriosis with ovarian cancer
Endometriosis associated with histological subtype― Endometriosiscontiguous
with carcinoma
13/547/22
not studied15/2835/104(34%)
1711
on August 3, 2020. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

ENDOMETRIOSISAND OVARIANCANCER
The data presented here support the view that endometriosis canundergo malignant transformation and raise the questions of howfrequently transformation occurs and what proportion of endometrioid and clear cell ovarian carcinomas arise via this route. Thefrequency with which endometriosis undergoes transformation isdifficult to determine, but based on histological observations, it hasbeen estimated to occur in about 1% of all cases. Epidemiological
studies of women with endometriosis have generally involved fewpatients and have been of insufficient duration to assess the magnitude of risk of developing a carcinoma. In the largest study, 62women were followed for a mean of 8. 1 years (22), one of whom(1 .6%) developed an ovarian carcinoma within an endometrioticcyst, which is broadly in line with the risk estimated from histological observations.
The proportion of endometrioid and clear cell ovarian carcinomas arising via endometriosis is also difficult to assess. Numerousstudies have established that between 30 and 40% of endometrioidand clear cell ovarian cancers contain histologically identifiableareas of endometriosis (Table 5), with about one-third showing adirect transition to malignancy. Even this remarkably high figure islikely to be an underestimate, because in many instances, evidenceof the precursor endometriotic lesion would be destroyed by outgrowth of the carcinoma. Interestingly, when we reexamined 19cases of endometrioid ovarian cancer, in which only 2 cases werereported as carcinoma with endometriosis, an additional 6 caseswith endometriosis in the same ovary were found. This suggeststhat the presence of endometriosis may be routinely omitted inpathological reports, thereby underestimating its biological significance.
It is possible to estimate the proportion of ovarian cancer thatmay arise via an endometriotic precursor, assuming that endometriosis affects about 10% of women (23), and 1% of these caseswill undergo malignant transformation. Based on these estimates,about 1 in a 1000 women would be expected to develop anendometrioid or clear cell ovarian cancer from endometriosis. Thisestimate is remarkably similar to the incidence observed in clinical
practice, where about 1% of women develop ovarian cancer, of
which -@10—15% are of endometrioid or clear cell type (i.e., 1 of1000 to 1 of 1500 women). Although these calculations are basedon best estimates, it is consistent with the hypothesis that endometriosis is the precursor of the majority, if not all, endometrioidand clear cell ovarian cancers.
In summary, we have shown that genetic alterations are relatively common in endometriosis, implying that TSG alterations arelikely to be involved in the proliferation and maintenance ofendometriotic implants. The finding of common genetic abnormalities in endometriosis synchronous with ovarian carcinoma reinforces the histological and epidemiological data, suggesting thatendometriosis is the precursor of all endometrioid and clear cellovarian cancers. However, the absolute risk of malignant transformation is small, and the vast majority of endometriotic lesionsfollow a benign course. The challenge now is to identify the smallsubset of endometriosis cases with the greatest risk of malignanttransformation.
1712
ACKNOWLEDGMENTS
We thank the staff of the Princess Anne Hospital, who participated incollection of tumor and endometriosis samples, and especially Maggie Barronand Narell Thomas.
REFERENCES
1. Thomas, E. J. Endometriosis: still an enigma. Br. J. Obstet. Gynaecol., 100: 615—617,1993.
2. Vercellini, P., Parazzini, F., Bolis, 0., Carmnelli,S., Dindelli, M., Vendola, N.,Luchini, L., and Crosignani, P. G. Endometriosis and ovarian cancer. Am. J. Obstet.Gynecol., 169: 181—182,1993.
3. McMeekin, D. S., Burger, R. A., Manetta, A., Disaia, P., and Berman, M. L.Endometrioid adenocarcinoma of the ovary and its relationship to endometriosis.Gynecol. Oncol., 59: 81—86,1995.
4. De la Cuesta, R. S., Eichhorn, J. H., Rice, L. W., Fuller, A. F., Jr., Nih-ui, N., andGoff, B. A. Histologic transformation of benign endometriosis to early epithelialovarian cancer. Gynecol. Oncol., 60: 238—244, 1996.
5. Fukunaga. M., Nomura, K., Ishikawa, E., and Ushigome, S. Ovarian atypical endometriosis: its close association with malignant epithelial tumours. Histopathology(Oxf.), 30: 249—255,1997.
6. Brinton, L. A., Gndley, 0., Persson, I., Baron, J., and Bergqvist, A. Cancer risk aftera hospital discharge diagnosis of endometriosis. Am. J. Obstet. Gynecol., i76:572—579,1997.
7. Rosenblatt, K. A., and Thomas, D. B. Reduced risk of ovarian-cancer in women witha tubal-ligation or hysterectomy. Cancer Epidemiol. Biomark. Prey., 5: 933—935,1996.
8. Jiang, X., Hitchcock, A., Bryan, E. J., Watson, R. H., Englefield, P., Thomas, E. J.,and Campbell, I. 0. Microsatellite analysis of endometriosis reveals loss of heterozygosity at candidate ovarian tumor-suppressor gene loci. Cancer Res., 56: 3534—3539,1996.
9. Milner, B. J., Allan, L. A., Eccles, D. M., Kitchener, H. C., Leonard, R. C. F., Kelly,K. F., Parkin, D. E., and Haites, N. E. p53 mutation is a common genetic event inovarian carcinoma. Cancer Res., 53: 2128—2132, 1993.
10. Campbell, I. G., Nicolai, H. M., Foulkes, W. D., Senger, G., Stamp, 0. W., Allan, G.,Boyer, C., Jones, K., Bast, R. C., Solomon, E., Trowsdale, J., and Black, D. M. Anovel gene encoding a B-Box protein within the BRCA1 region at 17q21.l. Hum.Mol. Genet., 3: 589—594,1994.
11. Foulkes, W. D., Stamp, G. W. H., AfZaI, S., Lalani, N., McFarlane, C. P., Trowsdale,J., and Campbell, I. G. MDM2 overexpression is rare in ovarian carcinoma irrespective of TP53 mutation status. Br. J. Cancer, 72: 883—888, 1995.
12. Jacobs, I. J., Kohler, M. F., Wiseman, R. W., Marks, J. R., Whitaker, R., Kems, B. A.,Humphrey, P., Berchuck, A., Ponder, B. A., and Bast, R. C., Jr. Clonal origin ofepithelial ovarian carcinoma: analysis by loss of heterozygosity, p53 mutation, andX-chromosome inactivation. J. Natl. Cancer Inst., 84: 1793—1798,1992.
13. Abeln, E. C. A., Kuipersdijkshoom, N. J., Berns, E., Henzenlogmans, S. C., Fleuren,G. J., and Comelisse, C. J. Molecular-genetic evidence for unifocal origin of advanced epithelial ovarian-cancer and for minor clonal divergence. Br. J. Cancer, 72:1330—1336,1995.
14. Cliby, W., Ritland, S., Hartmann, L., Dodson, M., Halling, K. C., Keeney, G.,Podratz, K. C., and Jenkins, R. B. Human epitheial ovarian cancer allelotype. CancerRes., 53: 2393—2398, 1993.
15. Osborne, R. J., and Leech, v. Polymerase chain reaction allelotyping of humanovarian cancer. Br. J. Cancer, 69: 429—438,1994.
16. Orphanos, V., McGown, G., Hey, Y., Thorncroft, M., Santibanezkoref, M., Russell,S. E. H., Hickey, I., Atkinson, R. J., and Boyle, J. M. Allelic imbalance of chromosome 6q in ovarian-tumors. Br. J. Cancer, 7i: 666—669,1995.
17. Sampson, J. A. Endometrial carcinoma of the ovary, arising in endometrial tissue inthat organ. Arch. Surg., iO: 1—72,1925.
18. Scott, R. B. Malignant changes in endometriosis. Obstet. Gynecol., 2: 283—289,1953.19. Mostoufizadeh, M. 0. H., and Scully, R. E. Malignant tumour arising in endometri
osis. Clin. Obstet. Gynecol., 23: 951—963,1980.20. Heaps, M. H., Nieberg, R. K., and Berek, J. S. Malignant neoplasms arising in
endometriosis. Obstet. Gynecol., 75: 1023—1028,1990.21. Tibile@,M.G.,Bemasth,B.,Furlan,D.,Rva,C.,Tmbia,M.,Buraggi,G.,Franchi,M.,
Boils, P., Madam, A., Frigerio, L, Capella, C., and Taramelli, R. Early involvement of 6qhi surface epithelial ovarian-tumors. Cancer Res@, 56: 4493-4498, 1996.
22. Seidman, J. D. Prognostic importance of hyperplasia and atypia in endometriosis. tnt.J. Gynecol. Pathol., 15: 1—9,1996.
23. Mabmood, T. A., and Templeton, A. Prevalence and genesis of endometriosis. Hum.Reprod., 6: 544—549,1991.
on August 3, 2020. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1998;58:1707-1712. Cancer Res Xiuxian Jiang, Sarah J. Morland, Andrew Hitchcock, et al. Reveals Evidence of a Common LineageAllelotyping of Endometriosis with Adjacent Ovarian Carcinoma
Updated version
http://cancerres.aacrjournals.org/content/58/8/1707
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/58/8/1707To request permission to re-use all or part of this article, use this link
on August 3, 2020. © 1998 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from