All About Orthopedics September 24th, 2021
13
9/22/2021 1 All About Orthopedics September 24 th , 2021 Chase Woodward, MD, MPH Orthopedic Spine Surgeon Classification of Scoliosis • Congenital • Neuromuscular • Syndrome related • Idiopathic (accounts for 80% of scoliosis) ‐ Infantile (age 0‐3 years, 0.5%) ‐ Juvenile (age 3‐10 years, 10.5%) ‐ Adolescent (age 10‐18 years, 89%) 1 2
Transcript of All About Orthopedics September 24th, 2021

9/22/2021
1
All About Orthopedics
September 24th, 2021
Chase Woodward, MD, MPHOrthopedic Spine Surgeon
Classification of Scoliosis
• Congenital
• Neuromuscular
• Syndrome related
• Idiopathic (accounts for 80% of scoliosis)
‐ Infantile (age 0‐3 years, 0.5%)
‐ Juvenile (age 3‐10 years, 10.5%)
‐ Adolescent (age 10‐18 years, 89%)
1
2

9/22/2021
2
Anatomy of idiopathic scoliosis
Definition: Cobb > 10 degrees
3D deformity: coronal, sagittal, axial
Three curves:• Proximal thoracic• Main thoracic• Thoracolumbar
Flexibility of curve
“Spinal balance” – C7 plumb line
Determining skeletal maturity
Anatomy of idiopathic scoliosis
Definition: Cobb > 10 degrees
3D deformity: coronal, sagittal, axial
Three curves:• Proximal thoracic• Main thoracic• Thoracolumbar
Flexibility of curve
“Spinal balance” – C7 plumb line
Determining skeletal maturity
3
4

9/22/2021
3
Anatomy of idiopathic scoliosis
Definition: Cobb > 10 degrees
3D deformity: coronal, sagittal, axial
Three curves:• Proximal thoracic• Main thoracic• Thoracolumbar
Flexibility of curve
“Spinal balance” – C7 plumb line
Determining skeletal maturity
PT
MT
TL
Anatomy of idiopathic scoliosis
Definition: Cobb > 10 degrees
3D deformity: coronal, sagittal, axial
Three curves:• Proximal thoracic• Main thoracic• Thoracolumbar
Flexibility of curve
“Spinal balance” – C7 plumb line
Determining skeletal maturity
5
6
9/22/2021
4
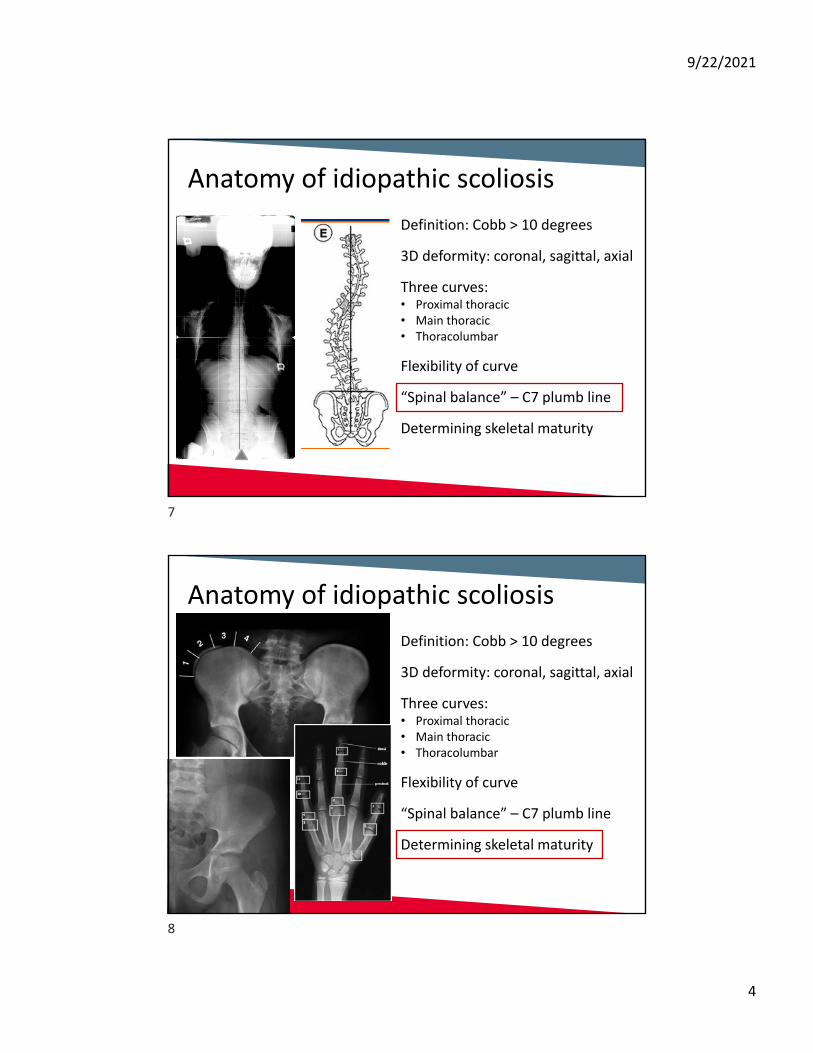
Anatomy of idiopathic scoliosis
Definition: Cobb > 10 degrees
3D deformity: coronal, sagittal, axial
Three curves:• Proximal thoracic• Main thoracic• Thoracolumbar
Flexibility of curve
“Spinal balance” – C7 plumb line
Determining skeletal maturity
Anatomy of idiopathic scoliosis
Definition: Cobb > 10 degrees
3D deformity: coronal, sagittal, axial
Three curves:• Proximal thoracic• Main thoracic• Thoracolumbar
Flexibility of curve
“Spinal balance” – C7 plumb line
Determining skeletal maturity
7
8
9/22/2021
5
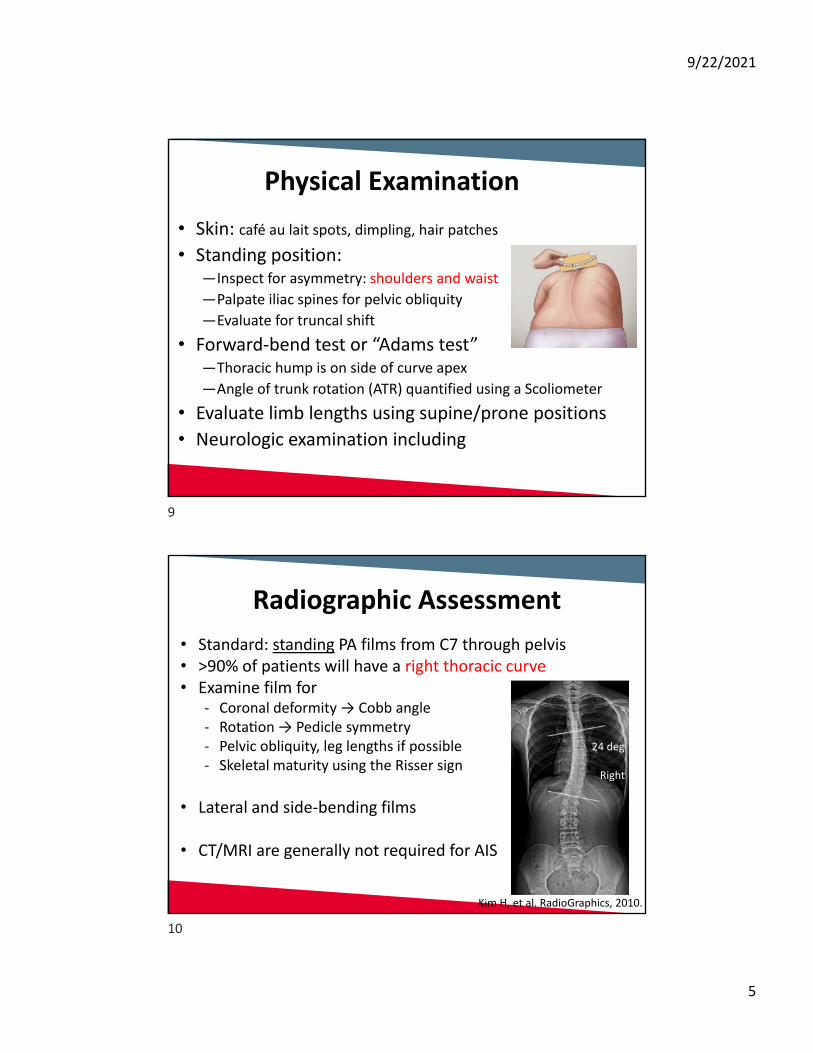
Physical Examination
• Skin: café au lait spots, dimpling, hair patches
• Standing position: —Inspect for asymmetry: shoulders and waist
—Palpate iliac spines for pelvic obliquity
—Evaluate for truncal shift
• Forward‐bend test or “Adams test”—Thoracic hump is on side of curve apex
—Angle of trunk rotation (ATR) quantified using a Scoliometer
• Evaluate limb lengths using supine/prone positions
• Neurologic examination including
Radiographic Assessment
• Standard: standing PA films from C7 through pelvis• >90% of patients will have a right thoracic curve• Examine film for
‐ Coronal deformity → Cobb angle‐ Rota on → Pedicle symmetry ‐ Pelvic obliquity, leg lengths if possible‐ Skeletal maturity using the Risser sign
• Lateral and side‐bending films
• CT/MRI are generally not required for AIS
Right
24 deg
Kim H, et al. RadioGraphics, 2010.
9
10
9/22/2021
6
Risk Factors for Curve Progression
• Patient sex—Need for surgical correction is 8x more common in girls
• Remaining skeletal growth—Highest risk of progression during growth spurt—Risser grade <1 confers greater risk—Risser grade >2 is protective
• Curve location—A curve apex above T12 is a risk factor
• Curve magnitude at initial diagnosis—More severe curves and double curves carry higher risk
Indications for Referral
• Scoliometer measurement >7 degrees
• Cobb angle between 20‐30 deg in pre‐teens (premenarchal girls or boys <14 years old)
• Cobb angle >30 deg in any patient
• Progression of Cobb angle >5 deg on serial XR
11
12

9/22/2021
7
Indications for Referral
• Scoliometer measurement >7 degrees
• Cobb angle between 20‐30 deg in pre‐teens (premenarchal girls or boys <14 years old)
• Cobb angle >30 deg in any patient
• Progression of Cobb angle >5 deg on serial XR
*OR ANY PATIENT YOU WANT US TO EVALUATE*
Treatment Strategies
1. Watchful waiting (observation)Cobb angle <20 degreesFollow‐up radiographs at 3‐12 month intervals (depends on maturity)
2. BracingPatient has not yet reached skeletal maturity (Risser 2 or less)Cobb angle 20‐30 degreesGoal is to prevent curve progression until skeletal maturity reached
3. SurgeryCobb guidelines: skeletally immature >40 deg, mature with >50 degConsider deformity, skeletal maturity, risk for progression, curve patternInstrumented deformity correction and fusion
13
14

9/22/2021
8
242 patients were included in primary analysis (combined cohorts)116 patients enrolled in the randomized cohort: observation vs TLSO
Treatment failure: curve progressed to > 50 degreesTreatment success: skeletal maturity prior to progression
TRIAL STOPPED DUE TO BRACING SUCCESS
2013
Posterior Spinal Fusion
• Goals: deformity correction, spinal balance, stability
• Pedicle screw and rod instrumentation
• Osteotomies for rigid deformities
• Duration: 4‐6 hours
• Blood loss: 600‐1200cc
15
16

9/22/2021
9
Safety Measures
• Intraoperative CT navigation for instrumentation
• Spinal cord monitoring
• Blood salvage systems
• Tranexamic acid
17
18

9/22/2021
10
Postop and Rehabilitation
Hospital stay: 3 nights
Back to school: 2 weeks
Feeling “good”: 6‐12 weeks
Return to sports: 6‐12 months
“Selective” fusion
14 yo girl, Lenke 1AN, 70 degree thoracic Three years postop: T3‐L1 fusion
19
20
9/22/2021
11
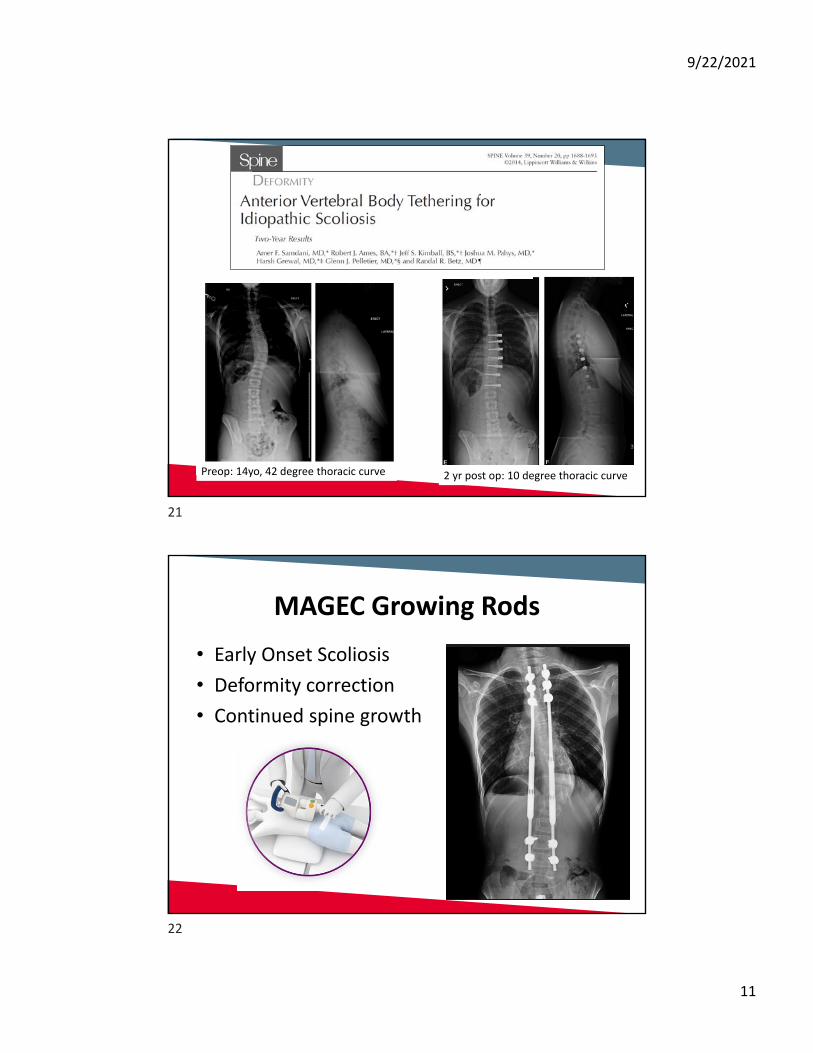
Preop: 14yo, 42 degree thoracic curve 2 yr post op: 10 degree thoracic curve
MAGEC Growing Rods
• Early Onset Scoliosis
• Deformity correction
• Continued spine growth
21
22

9/22/2021
12
Sources• Betz RR, Lenke LG. Adolescent idiopathic scoliosis. In: Vaccaro AR, Betz RR, Zeidman SM, eds: Principles and
Practice of Spine Surgery. Philadelphia: Mosby, 2003.• Danielsson AJ, Nachemson AL. Back pain and function 23 years after fusion for adolescent idiopathic
scoliosis: a case‐control study‐ part II. Spine. 2003;28:E373‐383.• Hresko MT. Idiopathic scoliosis in adolescents. J Engl J Med 2013;368:834‐41.• Kim H, et al. Scoliosis imaging: what radiologists should know. Radiographics 2010;30:1823‐1842.• Koumbourlis AC. Scoliosis and the respiratory system. Paediatric Respiratory Reviews. 2006;7:152‐160.• Lenke LG, et al. Adolescent idiopathic scoliosis: a new classification to determine the extent of spinal
arthrodesis. J Bone Joint Surg Am 2001;83:1169‐1181.• Lenke LG, et al. Curve prevalence of a new classification of adolescent idiopathic scoliosis (AIS): does
classification predict treatment? Spine 2002;27: 604‐611• Newton PO, Wenger DR. Idiopathic and congenital scoliosis. In: Morrissy RT, Weinstein SL, eds: Lovell and
Winter’s Pediatric Orthopaedics. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2001.• Newton PO, Wenger DR. Pediatric spinal deformity. In: Fardon DF, Garfin SR, eds: Orthopedic Knowledge
Update: Spine 2, American Academy of Orthopedic Surgeons, 2002:361.• Richards BS, Vitale MG. Screening for idiopathic scoliosis in adolescents: an information statement. J Bone
Joint Surg Am. 2008;90:195‐8• Ward K, et al. Validation of DNA‐based prognostic testing to predict spinal curve progression in adolescent
idiopathic scoliosis. Spine. 2010;35:1455‐64.• Weinstein SL, et al. Effects of bracing in adolescents with idiopathic scoliosis. N Engl J Med 2013;369:1512‐
21.
THANK YOU
Chase Woodward, MD, MPH
Orthopedic Spine Surgeon
September 24th, 2021
23
24

9/22/2021
13
25