
Aldo NaOcl Chx Biofilms
5
Biofilm Dissolution and Cleaning Ability of Different Irrigant Solutions on Intraorally Infected Dentin Aldo E. del Carpio-Perochena, DDS,* Clovis M. Bramante, DDS, PhD,* Marco A.H. Duarte, DDS, PhD,* Bruno Cavalini Cavenago, DDS,* Marcelo H. Villas-Boas, DDS,* Marcia S. Graeff, MSc, † Norberti Bernardineli, DDS, PhD,* Flaviana Bombarda de Andrade, DDS, PhD,* and Ronald Ordinola-Zapata, DDS, MSc* Abstract Introduction: The aim of this study was to evaluate the biofilm dissolution and cleaning ability of different irrigant solutions on intraorally infected dentin. Methods: One hundred twenty bovine dentin speci- mens were infected intraorally by using a removable orthodontic device. Thirty samples were used for each irrigant solution: 2% chlorhexidine and 1%, 2.5%, and 5.25% sodium hypochlorite (NaOCl). The solutions were used for 5, 15, and 30 minutes and at 2 experi- mental volumes, 500 mL and 1 mL. The samples were stained by using acridine orange dye before and after the experiments and evaluated by using a confocal microscope. The percentage of biofilm, isolated cells, and noncolonized dentin was measured by using a grid system. Differences in the reduction or increase of the studied parameters were assessed by using nonparametric methods (P < .05). Results: The higher values of biofilm dissolution and noncolonized dentin were found in the 30-minute NaOCl group and in the 5-minute and 15-minute groups of 5.25% NaOCL. The use of 2% chlorhexidine solution did not improve the bi- ofilm dissolution or increase the cleaning of the dentin in comparison with the NaOCl solutions (P < .05). Conclusions: Two percent chlorhexidine does not dissolve the biofilms. Thirty minutes of NaOCl are neces- sary to have higher values of biofilm dissolution and to increase the cleaning of the dentin independently of the concentration in comparison with the 5-minute and 15- minute contact times. (J Endod 2011;-:1–5) Key Words Acridine orange, bacteria, confocal laser scanning microscopy, dentin, irrigant solutions, oral biofilms B acteria and their products in avascular and necrotic root canal systems are the main etiologic factor of apical periodontitis (1). Biofilms can be defined as cells attached to a surface embedded in an exopolysaccharide matrix that fills the space between cells (2). Biofilms can resist alkali stress (3) and have increased resistance to antibacterial agents (4). Because of the irregularities of the root canal anatomy, antimicrobial irrigant solu- tions are used to dissolve necrotic tissue and to assist in the microbial control stage (5). The results of clinical studies have shown that at least 50% of root canals can retain bacteria after endodontic procedures with sodium hypochlorite (NaOCl)–based or chlorhexidine-based protocols (6, 7). Clinical advantages of chlorhexidine are antimicrobial activity (8), substantive effect (9), and low toxicity. Despite the fact that NaOCl and chlorhexidine have shown no differences in their antimicrobial activity in clinical research, the cleaning ability of these compounds and direct comparisons by using microscopic methods are scarce. Residual organic biofilm can act as a source of toxins and might also interfere with the obturation process in noninstrumented areas such as fins (10). Confocal laser scanning microscopy (CLSM) for the study of oral biofilms has been reported in earlier studies (11, 12). A potential advantage is the absence of dehydration or sputter-coating of the sample. This advantage allows for analysis of an infected sample before and immediately after antimicrobial treatment. Thus, this study aimed to evaluate under controlled conditions of the biofilm dissolution and cleaning dentin, the effect of different concentrations of NaOCl and 2% chlorhexidine on intraorally developed biofilm. The influence of time was also studied. The hypothesis of the study was that biofilm dissolution depends on the irrigant solutions and contact time. Materials and Methods The irrigant solutions used in this study were 1% and 2.5% NaOCl (CloroRio, S ~ ao Jos e do Rio Preto, SP, Brazil), 5.25% NaOCl (Farmacia Espec ıfica, Bauru, SP, Brazil), and 2% chlorhexidine (Villevie, Joinville, SC, Brazil). One hundred twenty dentin sections (4 Â 4 Â 2 mm) were obtained from previ- ously sterilized bovine radicular dentin. The samples were treated with 2.5% NaOCl for 15 minutes and 17% ethylenediaminetetraacetic acid for 3 minutes. Three samples were examined under the scanning electron microscope to verify the cleaning protocol. Eight to 12 dentin samples were fixed in each experimental procedure on a removable ortho- dontic device to allow the biofilm development (13). To standardize the rate of biofilm development, one healthy volunteer (heavy plaque–former) used the intraoral device for 72 hours. The subject maintained his routine consumption of food and drink From the *Department of Endodontics and † Integrated Research Center (CIP), Bauru Dental School of Bauru, University of S~ ao Paulo, Bauru, S~ ao Paulo, Brazil. This work was supported by FAPESP process 2009/03217-5, 2010/16002-4. Address requests for reprints to Dr Ronald Ordinola-Zapata, Faculdade de Odontologia de Bauru, USP, Al. Oct avio Pinheiro Brisolla, 9-75, CEP 17012-901, Bauru, S~ ao Paulo, Brazil. E-mail address: [email protected] 0099-2399/$ - see front matter Copyright ª 2011 American Association of Endodontists. doi:10.1016/j.joen.2011.04.013 Basic Research—Technology JOE — Volume -, Number -, - 2011 Biofilm Dissolution and Cleaning Ability of Different Irrigant Solutions 1
-
Upload
gabykarina -
Category
Documents
-
view
224 -
download
0
description
vcd
Transcript of Aldo NaOcl Chx Biofilms

Biofilm Dissolution and Cleaning Ability of Different IrrigantSolutions on Intraorally Infected DentinAldo E. del Carpio-Perochena, DDS,* Clovis M. Bramante, DDS, PhD,*
Marco A.H. Duarte, DDS, PhD,* Bruno Cavalini Cavenago, DDS,* Marcelo H. Villas-Boas, DDS,*
Marcia S. Graeff, MSc,† Norberti Bernardineli, DDS, PhD,*
Flaviana Bombarda de Andrade, DDS, PhD,* and Ronald Ordinola-Zapata, DDS, MSc*
Abstract
Introduction: The aim of this study was to evaluate thebiofilm dissolution and cleaning ability of differentirrigant solutions on intraorally infected dentin.Methods: One hundred twenty bovine dentin speci-mens were infected intraorally by using a removableorthodontic device. Thirty samples were used for eachirrigant solution: 2% chlorhexidine and 1%, 2.5%, and5.25% sodium hypochlorite (NaOCl). The solutionswere used for 5, 15, and 30 minutes and at 2 experi-mental volumes, 500 mL and 1 mL. The samples werestained by using acridine orange dye before and afterthe experiments and evaluated by using a confocalmicroscope. The percentage of biofilm, isolated cells,and noncolonized dentin was measured by usinga grid system. Differences in the reduction or increaseof the studied parameters were assessed by usingnonparametric methods (P < .05). Results: The highervalues of biofilm dissolution and noncolonized dentinwere found in the 30-minute NaOCl group and in the5-minute and 15-minute groups of 5.25% NaOCL. Theuse of 2% chlorhexidine solution did not improve the bi-ofilm dissolution or increase the cleaning of the dentin incomparison with the NaOCl solutions (P < .05).Conclusions: Two percent chlorhexidine does notdissolve the biofilms. Thirty minutes of NaOCl are neces-sary to have higher values of biofilm dissolution and toincrease the cleaning of the dentin independently of theconcentration in comparison with the 5-minute and 15-minute contact times. (J Endod 2011;-:1–5)
Key WordsAcridine orange, bacteria, confocal laser scanningmicroscopy, dentin, irrigant solutions, oral biofilms
Bacteria and their products in avascular and necrotic root canal systems are the mainetiologic factor of apical periodontitis (1). Biofilms can be defined as cells attached to
a surface embedded in an exopolysaccharidematrix that fills the space between cells (2).Biofilms can resist alkali stress (3) and have increased resistance to antibacterial agents(4). Because of the irregularities of the root canal anatomy, antimicrobial irrigant solu-tions are used to dissolve necrotic tissue and to assist in the microbial control stage (5).
The results of clinical studies have shown that at least 50% of root canals can retainbacteria after endodontic procedures with sodium hypochlorite (NaOCl)–based orchlorhexidine-based protocols (6, 7). Clinical advantages of chlorhexidine areantimicrobial activity (8), substantive effect (9), and low toxicity. Despite the factthat NaOCl and chlorhexidine have shown no differences in their antimicrobial activityin clinical research, the cleaning ability of these compounds and direct comparisons byusing microscopic methods are scarce. Residual organic biofilm can act as a source oftoxins and might also interfere with the obturation process in noninstrumented areassuch as fins (10).
Confocal laser scanningmicroscopy (CLSM) for the study of oral biofilms has beenreported in earlier studies (11, 12). A potential advantage is the absence of dehydrationor sputter-coating of the sample. This advantage allows for analysis of an infectedsample before and immediately after antimicrobial treatment. Thus, this study aimedto evaluate under controlled conditions of the biofilm dissolution and cleaning dentin,the effect of different concentrations of NaOCl and 2% chlorhexidine on intraorallydeveloped biofilm. The influence of time was also studied. The hypothesis of the studywas that biofilm dissolution depends on the irrigant solutions and contact time.
Materials and MethodsThe irrigant solutions used in this study were 1% and 2.5% NaOCl (CloroRio, S~ao
Jos"e do Rio Preto, SP, Brazil), 5.25% NaOCl (Farmacia Espec"ıfica, Bauru, SP, Brazil),and 2% chlorhexidine (Villevie, Joinville, SC, Brazil).
One hundred twenty dentin sections (4! 4! 2 mm) were obtained from previ-ously sterilized bovine radicular dentin. The samples were treated with 2.5% NaOCl for15minutes and 17% ethylenediaminetetraacetic acid for 3minutes. Three samples wereexamined under the scanning electron microscope to verify the cleaning protocol. Eightto 12 dentin samples were fixed in each experimental procedure on a removable ortho-dontic device to allow the biofilm development (13). To standardize the rate of biofilmdevelopment, one healthy volunteer (heavy plaque–former) used the intraoral devicefor 72 hours. The subject maintained his routine consumption of food and drink
From the *Department of Endodontics and †Integrated Research Center (CIP), Bauru Dental School of Bauru, University of S~ao Paulo, Bauru, S~ao Paulo, Brazil.This work was supported by FAPESP process 2009/03217-5, 2010/16002-4.Address requests for reprints to Dr Ronald Ordinola-Zapata, Faculdade de Odontologia de Bauru, USP, Al. Oct"avio Pinheiro Brisolla, 9-75, CEP 17012-901, Bauru, S~ao
Paulo, Brazil. E-mail address: [email protected]/$ - see front matter
Copyright ª 2011 American Association of Endodontists.doi:10.1016/j.joen.2011.04.013
Basic Research—Technology
JOE — Volume-, Number-,- 2011 Biofilm Dissolution and Cleaning Ability of Different Irrigant Solutions 1

and used the intraoral device except during regular oral hygiene prac-tices. The ethical human committee approved the protocol (064/2009).After the infection process the samples were observed by using CLSM(Leica TCS-SPE, Germany) in the epifluorescence mode. Specimensthat showed absence of biofilm structures were discarded.
Thirty samples were used for each irrigant solution. The experi-ments were performed by immersing the dentin sample in the irrigantsolutions by using 24-well tissue culture plates. The samples weredivided into 3 groups (n = 10) according to the contact time (5, 15,and 30 minutes) and subdivided into 2 subgroups (n = 5) accordingto the volume of the irrigant solutions used (500 mL or 1 mL). The ir-rigant solutions in the 15-minute and 30-minute groups were refreshedevery 5 minutes to simulate clinical condition. One additional dentinsample in each group was treated with 1 mL distilled water for 30minutes to serve as control.
Before contact with the irrigant solutions, the samples werestained with 100 mL of 0.01% acridine orange for 15 minutes andthen rinsed with 100mL of distilled water; such dye has been used previ-ously in biofilm research for bacterial identification (14, 15) because ofits ability to bind with bacterial RNA/DNA emitting red and greenfluorescence (16). After the staining procedure, the specimens wereimmediately analyzed by the CLSM technique.
All the samples were observed by using the 10! and 40! oil lens(CLSM Leica TCS-SPE; Microsystems GmbH, Mannheim, Germany).Three 40! confocal pictures were obtained from the central point ofthe sample before the experiment by using a 1-mm step-size in a formatof 512 ! 512 pixels. After the experiments, the NaOCl samples weretreated with 100 mL of 5% sodium thiosulfate. Chlorhexidine-treatedsamples were washed with 100 mL of distilled water. A pilot studyshowed that sodium thiosulfate does not have dissolution ability andimproves the quality of the stain process. Then the samples were imme-diately stained with the acridine orange dye, and 3 post-treatment 40!pictures were recorded from the middle of the sample. Each 40!picture represented an area of 275 ! 275 mm2.
The evaluation was performed by using the Adobe Photoshop(Adobe Systems, San Jose, CA) software, as previously described(17). The following terminology was used to quantify the content ofthe confocal pictures: biofilm, the presence of cells embedded in anextracellular matrix attached to the dentin; isolated cells, very sparseindividual bacteria not embedded in an extracellular matrix; noncolon-ized dentin, the dentin presents absence of microbial structures.
For quantification purposes the confocal pictures were dividedinto 100 squares by using a digital grid (Fig. 1). The percentage of bio-film, isolated cells, or noncolonized dentin was calculated by placing thedigital grid over the maximum projection confocal images to allowcounting the points in the picture that coincided with either biofilmareas or areas showing dentin (17). Each digital square representedan area of 27.5 ! 27.5 mm2. Two single evaluators with experiencein confocal/biofilm research classified the content of each of the 100squares individually in each preirrigation and postirrigation picture.Appropriate interobserver reproducibility was confirmed by using thePearson correlation coefficient. The values of r ranged from 0.89–1.00, showing high correlation between the measurements.
The preliminary analysis of the raw pooled data did not showa normal distribution. Thus, the Kruskal-Wallis and Dunn tests wereused for multiple comparisons among the groups and time. The influ-ence of volume was determined by using the Mann-Whitney U test. Thelevel of significance was set at P < .05, and Prisma 5.0 (GraphPad Soft-ware Inc, La Jolla, CA) was used as the analytical tool.
ResultsA total of 720 experimental pictures were evaluated. The Mann-
Whitney U test showed the absence of differences between the 500-mL and 1-mL groups. It means that the results were not dependenton the irrigant volume. Consequently, the data were pooled to providea single median of 10 samples (30 pictures) per group.
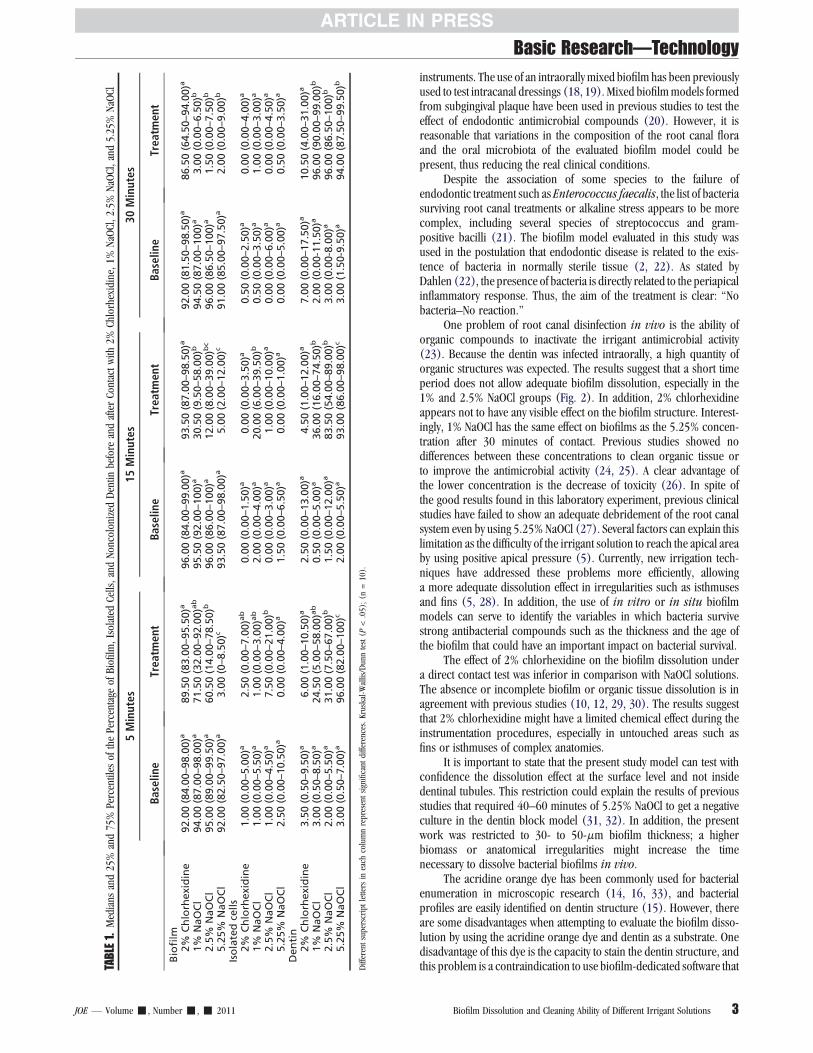
Overall, the preoperative biofilm thickness ranged from 30–50mm, without statistical significances among the groups (data notshown). The medians and 25%–75% percentiles of the studiedparameters of biofilm, isolated cells, and noncolonized dentin arepresented in Table 1. No significant differences in the preoperativeparameters as a percentage of area covered by biofilm, isolated cells,or dentin were found among the groups (P > .05) (Table 1). Thehigher values of biofilm dissolution were found in the 30-minuteNaOCl group and in the 5-minute and 15-minute groups of 5.25%NaOCL. The 2% chlorhexidine–treated samples showed the highestvalues for the biofilm parameter in comparison with all the NaOClgroups (P < .05), except the 5-minute group of 1% NaOCl (P >.05). The higher increment of noncolonized dentin was found after30 minutes of NaOCl (P > .05). There was a significant increment ofthe isolated cells in 1% NaOCl–15-minute group as a result ofincomplete biofilm disorganization (P < .05).
An intragroup time comparison showed that time does not have aneffect on 2% chlorhexidine or 5.25% NaOCl in all the parameters tested(P > .05). In the 1% and 2.5% NaOCl groups, time significantly alteredthe parameters of biofilm and noncolonized dentin (P < .05). In bothcases, the 5-minute period was significantly different from the 15-minuteperiod, and this group was significantly different from the 30-minutegroups with one exception; 5 minutes of 1% NaOCl had the same effecton the noncolonized dentin parameter as 15 minutes (P > .05). Repre-sentative pictures of the experimental groups are shown in Fig. 2.
DiscussionDissolution of biofilms by irrigant solutions is crucial because
a significant area of the root canal system is inaccessible to endodontic
Figure 1. Confocal picture of representative intraorally infected dentin withthe digital grid overlapped that is used for quantification purposes. The pictureshows areas of intense biofilm colonization and the presence of isolated cells(arrow). Bar represents 20 mm.
Basic Research—Technology
2 del Carpio-Perochena et al. JOE— Volume-, Number-,- 2011
instruments. The use of an intraorally mixed biofilm has been previouslyused to test intracanal dressings (18, 19). Mixed biofilmmodels formedfrom subgingival plaque have been used in previous studies to test theeffect of endodontic antimicrobial compounds (20). However, it isreasonable that variations in the composition of the root canal floraand the oral microbiota of the evaluated biofilm model could bepresent, thus reducing the real clinical conditions.
Despite the association of some species to the failure ofendodontic treatment such as Enterococcus faecalis, the list of bacteriasurviving root canal treatments or alkaline stress appears to be morecomplex, including several species of streptococcus and gram-positive bacilli (21). The biofilm model evaluated in this study wasused in the postulation that endodontic disease is related to the exis-tence of bacteria in normally sterile tissue (2, 22). As stated byDahlen (22), the presence of bacteria is directly related to the periapicalinflammatory response. Thus, the aim of the treatment is clear: ‘‘Nobacteria–No reaction.’’
One problem of root canal disinfection in vivo is the ability oforganic compounds to inactivate the irrigant antimicrobial activity(23). Because the dentin was infected intraorally, a high quantity oforganic structures was expected. The results suggest that a short timeperiod does not allow adequate biofilm dissolution, especially in the1% and 2.5% NaOCl groups (Fig. 2). In addition, 2% chlorhexidineappears not to have any visible effect on the biofilm structure. Interest-ingly, 1% NaOCl has the same effect on biofilms as the 5.25% concen-tration after 30 minutes of contact. Previous studies showed nodifferences between these concentrations to clean organic tissue orto improve the antimicrobial activity (24, 25). A clear advantage ofthe lower concentration is the decrease of toxicity (26). In spite ofthe good results found in this laboratory experiment, previous clinicalstudies have failed to show an adequate debridement of the root canalsystem even by using 5.25% NaOCl (27). Several factors can explain thislimitation as the difficulty of the irrigant solution to reach the apical areaby using positive apical pressure (5). Currently, new irrigation tech-niques have addressed these problems more efficiently, allowinga more adequate dissolution effect in irregularities such as isthmusesand fins (5, 28). In addition, the use of in vitro or in situ biofilmmodels can serve to identify the variables in which bacteria survivestrong antibacterial compounds such as the thickness and the age ofthe biofilm that could have an important impact on bacterial survival.
The effect of 2% chlorhexidine on the biofilm dissolution undera direct contact test was inferior in comparison with NaOCl solutions.The absence or incomplete biofilm or organic tissue dissolution is inagreement with previous studies (10, 12, 29, 30). The results suggestthat 2% chlorhexidine might have a limited chemical effect during theinstrumentation procedures, especially in untouched areas such asfins or isthmuses of complex anatomies.
It is important to state that the present study model can test withconfidence the dissolution effect at the surface level and not insidedentinal tubules. This restriction could explain the results of previousstudies that required 40–60 minutes of 5.25% NaOCl to get a negativeculture in the dentin block model (31, 32). In addition, the presentwork was restricted to 30- to 50-mm biofilm thickness; a higherbiomass or anatomical irregularities might increase the timenecessary to dissolve bacterial biofilms in vivo.
The acridine orange dye has been commonly used for bacterialenumeration in microscopic research (14, 16, 33), and bacterialprofiles are easily identified on dentin structure (15). However, thereare some disadvantages when attempting to evaluate the biofilm disso-lution by using the acridine orange dye and dentin as a substrate. Onedisadvantage of this dye is the capacity to stain the dentin structure, andthis problem is a contraindication to use biofilm-dedicated software thatTA
BLE
1.Medians
and25%and75%Percentiles
ofthePercentage
ofBiofilm,Isolated
Cells,andNoncolonizedDentin
before
andafterContactwith
2%Chlorhexidine,1%
NaOCl,2.5%
NaOCl,and5.25%NaOCl
5Minutes
15Minutes
30Minutes
Baseline
Treatm
ent
Baseline
Treatm
ent
Baseline
Treatm
ent
Biofilm
2%
Chlorhexidine
92.00(84.00–98.00)a
89.50(83.00–95.50)a
96.00(84.00–99.00)a
93.50(87.00–98.50)a
92.00(81.50–98.50)a
86.50(64.50–94.00)a
1%
NaOCl
94.00(87.00–98.00)a
71.50(32.00–92.00)ab
95.50(92.00–100)a
30.50(9.50–58.00)b
94.50(87.00–100)a
3.00(0.00–6.50)b
2.5%
NaOCl
95.00(89.00–99.50)a
60.50(14.00–78.50)b
96.00(86.00–100)a
12.00(8.00–39.00)b
c96.00(86.50–100)a
1.50(0.00–7.50)b
5.25%
NaOCl
92.00(82.50–97.00)a
3.00(0–8.50)c
93.50(87.00–98.00)a
5.00(2.00–12.00)c
91.00(85.00–97.50)a
2.00(0.00–9.00)b
Isolatedcells
2%
Chlorhexidine
1.00(0.00–5.00)a
2.50(0.00–7.00)ab
0.00(0.00–1.50)a
0.00(0.00–3.50)a
0.50(0.00–2.50)a
0.00(0.00–4.00)a
1%
NaOCl
1.00(0.00–5.50)a
1.00(0.00–3.00)ab
2.00(0.00–4.00)a
20.00(6.00–39.50)b
0.50(0.00–3.50)a
1.00(0.00–3.00)a
2.5%
NaOCl
1.00(0.00–4.50)a
7.50(0.00–21.00)b
0.00(0.00–3.00)a
1.00(0.00–10.00)a
0.00(0.00–6.00)a
0.00(0.00–4.50)a
5.25%
NaOCl
2.50(0.00–10.50)a
0.00(0.00–4.00)a
1.50(0.00–6.50)a
0.00(0.00–1.00)a
0.00(0.00–5.00)a
0.50(0.00–3.50)a
Dentin
2%
Chlorhexidine
3.50(0.50–9.50)a
6.00(1.00–10.50)a
2.50(0.00–13.00)a
4.50(1.00–12.00)a
7.00(0.00–17.50)a
10.50(4.00–31.00)a
1%
NaOCl
3.00(0.50–8.50)a
24.50(5.00–58.00)ab
0.50(0.00–5.00)a
36.00(16.00–74.50)b
2.00(0.00-11.50)a
96.00(90.00–99.00)b
2.5%
NaOCl
2.00(0.00–5.50)a
31.00(7.50–67.00)b
1.50(0.00–12.00)a
83.50(54.00–89.00)b
3.00(0.00-8.00)a
96.00(86.50–100)b
5.25%
NaOCl
3.00(0.50–7.00)a
96.00(82.00–100)c
2.00(0.00–5.50)a
93.00(86.00–98.00)c
3.00(1.50-9.50)a
94.00(87.50–99.50)b
Differentsuperscriptlettersineach
columnrepresentsignificantdifferences.Kruskal-Wallis/Dunntest(P
<.05);(n
=10).
Basic Research—Technology
JOE — Volume-, Number-,- 2011 Biofilm Dissolution and Cleaning Ability of Different Irrigant Solutions 3

can allow a more accurate volumetric quantification of the residualbiomass. As stated by Bryce et al (12), ‘‘the use of dentin to grow bio-films can result in difficulties with background fluorescence from thedentin, which autofluoresces, potentially obscuring software basedbacterial counting’’. For this reason, volumetric analysis was discarded,and 2-dimensional semiquantification was used. The methodology usedis not so different from scanning electron microscope evaluation (10),with the advantage that the samples can be observed before the exper-imental protocol, allowing verification of an adequate standardization ofthe dentin infection before contact with the irrigant solutions. One limi-tation of this method is the possibility of overlapping, mainly betweenthe categories, biofilm/isolated cells. However, the proportion of iso-lated cells was very low, between 0%–7% of the total area evaluated,and they were only more prevalent in the 1% NaOCl 15-minute groupas a result of incomplete biofilm dissolution. In addition, the cleaningability of the irrigation solutions on dentin can be clearly confirmed byevaluating the statistical increment of noncolonized dentin in thedifferent experimental periods, which is also a good indicator thatthe biofilm/bacteria dissolution has occurred, because dentin can beeasily differentiated from biofilm or cells.
The advantage of direct observation by using microscopic tech-niques is clear; the sample is not dispersed as in culture technique,and this allows information on the proportion of the colonized surfacein the infected tissue. Future studies with the live/dead technique canallow studying the vitality of persister cells on dentin specimens. More-over, the effect of the biofilm thickness appears to be important with thismodel. In addition, the influence of anatomical variables needs to befurther determined.
Under the conditions of this study, it can be concluded that NaOClsolutions were more effective than 2% chlorhexidine to eliminate bio-films. Thirty minutes of NaOCl are necessary to have the higher values ofbiofilm dissolution and to increase the cleaning of the dentin mainly in1% and 2.5% concentrations, thus accepting the tested hypothesis.
Under clinical conditions, a lower contact time in the apical third mightbe insufficient to allow a total disintegration of intraradicular biofilm.
Acknowledgments
The authors deny any conflicts of interest related to this study.
References1. Ricucci D, Siqueira JF Jr. Biofilms and apical periodontitis: study of prevalence and
association with clinical and histopathologic findings. J Endod 2010;36:1277–88.2. Costerton JW. The biofilm primer. Berlin/New York: Springer; 2007.3. Chavez de Paz LE, Bergenholtz G, Dahlen G, Svensater G. Response to alkaline stress
by root canal bacteria in biofilms. Int Endod J 2007;40:344–55.4. Dunavant TR, Regan JD, Glickman GN, Solomon ES, Honeyman AL. Comparative
evaluation of endodontic irrigants against Enterococcus faecalis biofilms. J Endod2006;32:527–31.
5. Susin L, Liu Y, Yoon JC, et al. Canal and isthmus debridement efficacies of two irri-gant agitation techniques in a closed system. Int Endod J 2010;43:1077–90.
6. McGurkin-Smith R, Trope M, Caplan D, Sigurdsson A. Reduction of intracanalbacteria using GT rotary instrumentation, 5.25% NaOCl, EDTA, and Ca(OH)2.J Endod 2005;31:359–63.
7. Siqueira JF Jr, Rocas IN, Paiva SS, Guimaraes-Pinto T, Magalhaes KM, Lima KC.Bacteriologic investigation of the effects of sodium hypochlorite and chlorhexidineduring the endodontic treatment of teeth with apical periodontitis. Oral Surg OralMed Oral Pathol Oral Radiol Endod 2007;104:122–30.
8. Rocas IN, Siqueira JF Jr. Comparison of the in vivo antimicrobial effectiveness ofsodium hypochlorite and chlorhexidine used as root canal irrigants: a molecularmicrobiology study. J Endod 2011;37:143–50.
9. Lenet BJ, Komorowski R, Wu XY, et al. Antimicrobial substantivity of bovine rootdentin exposed to different chlorhexidine delivery vehicles. J Endod 2000;26:652–5.
10. Clegg MS, Vertucci FJ, Walker C, Belanger M, Britto LR. The effect of exposure toirrigant solutions on apical dentin biofilms in vitro. J Endod 2006;32:434–7.
11. Shen Y, Stojicic S, Qian W, Olsen I, Haapasalo M. The synergistic antimicrobial effectby mechanical agitation and two chlorhexidine preparations on biofilm bacteria.J Endod 2010;36:100–4.
Figure 2. (A, B) Representative confocal pictures before and after treatment with 2% chlorhexidine (15 minutes); biofilm structure is not affected. The effect of 5and 15 minutes of 1% NaOCl on biofilm dissolution can be seen in (D) and (F). Preoperative pictures are shown in (C) and (E). After 5 minutes there is partialdissolution of the biofilm structure and visible loss of the biomass. However, deep biofilm layers are still covering the dentin structure (D). After 15 minutes of 1%NaOCl, dentin structure is visible, but residual biofilm structures are persistent (F). After 5 minutes of 5.25% NaOCl, no biofilm structure could be found in thissample (H); only remnant isolated cells are visible (*). Preoperative picture is shown in (G). All bars represent 20 mm.
Basic Research—Technology
4 del Carpio-Perochena et al. JOE— Volume-, Number-,- 2011

12. Bryce G, O’Donnell D, Ready D, Ng YL, Pratten J, Gulabivala K. Contemporary rootcanal irrigants are able to disrupt and eradicate single- and dual-species biofilms.J Endod 2009;35:1243–8.
13. Zaura-Arite E, van Marle J, ten Cate JM. Confocal microscopy study of undis-turbed and chlorhexidine-treated dental biofilm. J Dent Res 2001;80:1436–40.
14. George S, Kishen A. Effect of tissue fluids on hydrophobicity and adherence ofEnterococcus faecalis to dentin. J Endod 2007;33:1421–5.
15. George S, Kishen A, Song KP. The role of environmental changes on monospeciesbiofilm formation on root canal wall by Enterococcus faecalis. J Endod 2005;31:867–72.
16. Vitkov L, Hannig M, Krautgartner WD, et al. Ex vivo gingival-biofilm consortia. LettAppl Microbiol 2005;41:404–11.
17. Fornari VJ, Silva-Sousa YT, Vanni JR, Pecora JD, Versiani MA, Sousa-Neto MD. Histo-logical evaluation of the effectiveness of increased apical enlargement for cleaningthe apical third of curved canals. Int Endod J 2010;43:988–94.
18. Barthel CR, Zimmer S, Zilliges S, Schiller R, Gobel UB, Roulet JF. In situ antimicro-bial effectiveness of chlorhexidine and calcium hydroxide: gel and paste versusgutta-percha points. J Endod 2002;28:427–30.
19. Virtej A, MacKenzie CR, Raab WH, Pfeffer K, Barthel CR. Determination of the perfor-mance of various root canal disinfection methods after in situ carriage. J Endod2007;33:926–9.
20. Shen Y, Qian W, Chung C, Olsen I, Haapasalo M. Evaluation of the effect of two chlo-rhexidine preparations on biofilm bacteria in vitro: a three-dimensional quantitativeanalysis. J Endod 2009;35:981–5.
21. Chavez de Paz LE. Redefining the persistent infection in root canals: possible role ofbiofilm communities. J Endod 2007;33:652–62.
22. Dahlen G. Microbiological diagnostics in oral diseases. Acta Odontol Scand 2006;64:164–8.
23. Pappen FG, Qian W, Aleksejuniene J, Leonardo Rde T, Leonardo MR, Haapasalo M.Inhibition of sodium hypochlorite antimicrobial activity in the presence of bovineserum albumin. J Endod 2010;36:268–71.
24. Bystrom A, Sundqvist G. The antibacterial action of sodium hypochlorite and EDTAin 60 cases of endodontic therapy. Int Endod J 1985;18:35–40.
25. Baumgartner JC, Cuenin PR. Efficacy of several concentrations of sodium hypochlo-rite for root canal irrigation. J Endod 1992;18:605–12.
26. Spangberg L, Engstrom B, Langeland K. Biologic effects of dental materials: 3—toxicity and antimicrobial effect of endodontic antiseptics in vitro. Oral Surg OralMed Oral Pathol 1973;36:856–71.
27. Nair PN, Henry S, Cano V, Vera J. Microbial status of apical root canal system of humanmandibular first molars with primary apical periodontitis after "one-visit" endodontictreatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:231–52.
28. Burleson A, Nusstein J, Reader A, Beck M. The in vivo evaluation of hand/rotary/ultrasound instrumentation in necrotic, human mandibular molars. J Endod2007;33:782–7.
29. Okino LA, Siqueira EL, Santos M, Bombana AC, Figueiredo JA. Dissolution of pulptissue by aqueous solution of chlorhexidine digluconate and chlorhexidine digluc-onate gel. Int Endod J 2004;37:38–41.
30. Chavez de Paz LE, Bergenholtz G, Svensater G. The effects of antimicrobials onendodontic biofilm bacteria. J Endod 2010;36:70–7.
31. Sen BH, Safavi KE, Spangberg LS. Antifungal effects of sodium hypochlorite and chlo-rhexidine in root canals. J Endod 1999;25:235–8.
32. Retamozo B, Shabahang S, Johnson N, Aprecio RM, Torabinejad M. Minimumcontact time and concentration of sodium hypochlorite required to eliminateEnterococcus faecalis. J Endod 2010;36:520–3.
33. Harrison JJ, Ceri H, Yerly J, et al. The use of microscopy and three-dimensionalvisualization to evaluate the structure of microbial biofilms cultivated in the CalgaryBiofilm Device. Biol Proced Online 2006;8:194–215.
Basic Research—Technology
JOE — Volume-, Number-,- 2011 Biofilm Dissolution and Cleaning Ability of Different Irrigant Solutions 5


















