Ajm Pericarditis Constrictiva
4
CLINICAL COMMUNICATIONS TO THE EDITOR Constrictive Pericarditis Masquerading as Chronic Idiopathic Pleural Effusion: Importance of Physical Examination To the Editor: We describe a patient who was labeled as having “idio- pathic pleural effusion” for several years. A careful physical examination clarified the diagnosis and resulted in a cura- tive procedure. CASE REPORT A 40-year-old Honduran woman was admitted to the car- diology service in late 2004. For 3 years she had dyspnea on exertion, lower extremity swelling, dry cough, and “three- pillow” orthopnea, but she denied paroxysmal nocturnal dyspnea, and her exercise capacity was very limited (New York Heart Association functional class III/IV). History In January 2002, diabetes mellitus, hypertension, and a right pleural effusion were diagnosed in the patient. Pulmonary function test results showed mixed restrictive-obstructive disease. Bronchoscopy findings were negative. Computed tomography of the chest showed a right-sided pleural effu- sion. Pleural biopsy showed chronic inflammatory changes, and the pleural fluid was a transudate. Four antituberculous medications were prescribed for a presumed diagnosis of tuberculosis, although diagnostic studies were not diagnos- tic, and the pleural fluid was a transudate. In 2003, all of these tests were repeated, and the results were negative. Physical Examination The patient had a paradoxical pulse of 15 to 20 mm Hg and a blood pressure of 110/66 mm Hg. The peaks of the jugular venous pulse (JVP) were higher than the angle of the man- dible even when the patient was sitting up. The troughs of the JVP showed prominent “x” and “y” descents (Figure 1A) that increased with inspiration (positive Kussmaul’s sign). A “pericardial knock” was present at the left lower sternal border. The cardiac impulse was not palpable, and there was no cardiac enlargement on percussion of the chest. There was dullness to percussion over the right lung base with absent breath sounds, hepatomegaly, and lower ex- tremity edema. Chest radiography showed a small right- sided pleural effusion and a normal-sized heart with no evidence of pericardial calcification. The electrocardiogram showed sinus rhythm, low-voltage QRS, and nonspecific T-wave abnormalities. The bedside clinical diagnosis was constrictive pericarditis, with no differential diagnosis (S.H.R.). The diuretic was discontinued. Transthoracic and transesophageal echocardiography/ Doppler showed no pericardial effusion. The pericardium appeared “minimally” thickened, biatrial enlargement was evident, and the left ventricle (LV) size and function were normal. Significant respiratory variations in the Doppler signals, obtained across the mitral and tricuspid inflows, could not be documented with confidence. Computed to- mography and magnetic resonance imaging of the heart reconfirmed the possible “minimal” pericardial thickening and showed no calcification or any other pathologic abnormalities. Cardiac catheterization showed near equalization of the right atrial (RA) and pulmonary artery (PA) wedge pres- sures and of the diastolic right ventricle (RV) and LV pressures (Figures 1A and B). The discordance between the RV and LV systolic pressures could not be convincingly demonstrated. Coronary arteriography showed no coronary arterial obstruction. At surgery, the pericardium had an abnormal fibrous appearance with diffuse thickening of 5 to 7 mm (Figure 2) and was easily removed. After pericardiectomy, the RV systolic pressure decreased from 42 to 30 mm Hg, and the RA pressure decreased from 20 to 14 mm Hg. The postop- erative course was uneventful, and the patient was dis- charged on the eighth day with no medications. At the 6-month postoperative evaluation, the patient was asymptomatic. DISCUSSION This patient had a diagnosis of chronic idiopathic pleural effusion for 3 years even though the pleural fluid was a transudate. The most common cause of a transudate pleural effusion is heart failure. 1 Pleural effusions occur in 44% to Dr. Rahimtoola is on the Speaker’s Bureau of Merck and Pfizer and has received honoraria from three companies that manufacture prosthetic heart valves. Requests for reprints should be addressed to Shahbudin H. Rahimtoola, MD, University of Southern California, 2025 Zonal Avenue, Los Angeles, CA 90033. E-mail address: [email protected]. 0002-9343/$ -see front matter © 2006 Elsevier Inc. All rights reserved. The American Journal of Medicine (2006) 119, e1-e4
-
Upload
fabiandionisio -
Category
Documents
-
view
8 -
download
1
Transcript of Ajm Pericarditis Constrictiva

C
CCI
T
pet
CAdepdY
HIpfdtsamttt
PTavdt
rv
MC
0
The American Journal of Medicine (2006) 119, e1-e4
LINICAL COMMUNICATIONS TO THE EDITOR
1sstTwtsesTc(
Daenscmraa
rspRda
aasRec6a
DTet
onstrictive Pericarditis Masquerading ashronic Idiopathic Pleural Effusion:mportance of Physical Examination
o the Editor:
We describe a patient who was labeled as having “idio-athic pleural effusion” for several years. A careful physicalxamination clarified the diagnosis and resulted in a cura-ive procedure.
ASE REPORT40-year-old Honduran woman was admitted to the car-
iology service in late 2004. For 3 years she had dyspnea onxertion, lower extremity swelling, dry cough, and “three-illow” orthopnea, but she denied paroxysmal nocturnalyspnea, and her exercise capacity was very limited (Nework Heart Association functional class III/IV).
istoryn January 2002, diabetes mellitus, hypertension, and a rightleural effusion were diagnosed in the patient. Pulmonaryunction test results showed mixed restrictive-obstructiveisease. Bronchoscopy findings were negative. Computedomography of the chest showed a right-sided pleural effu-ion. Pleural biopsy showed chronic inflammatory changes,nd the pleural fluid was a transudate. Four antituberculousedications were prescribed for a presumed diagnosis of
uberculosis, although diagnostic studies were not diagnos-ic, and the pleural fluid was a transudate. In 2003, all ofhese tests were repeated, and the results were negative.
hysical Examinationhe patient had a paradoxical pulse of 15 to 20 mm Hg andblood pressure of 110/66 mm Hg. The peaks of the jugularenous pulse (JVP) were higher than the angle of the man-ible even when the patient was sitting up. The troughs ofhe JVP showed prominent “x” and “y” descents (Figure
Dr. Rahimtoola is on the Speaker’s Bureau of Merck and Pfizer and haseceived honoraria from three companies that manufacture prosthetic heartalves.
Requests for reprints should be addressed to Shahbudin H. Rahimtoola,D, University of Southern California, 2025 Zonal Avenue, Los Angeles,A 90033.
eE-mail address: [email protected].
002-9343/$ -see front matter © 2006 Elsevier Inc. All rights reserved.
A) that increased with inspiration (positive Kussmaul’sign). A “pericardial knock” was present at the left lowerternal border. The cardiac impulse was not palpable, andhere was no cardiac enlargement on percussion of the chest.here was dullness to percussion over the right lung baseith absent breath sounds, hepatomegaly, and lower ex-
remity edema. Chest radiography showed a small right-ided pleural effusion and a normal-sized heart with novidence of pericardial calcification. The electrocardiogramhowed sinus rhythm, low-voltage QRS, and nonspecific-wave abnormalities. The bedside clinical diagnosis wasonstrictive pericarditis, with no differential diagnosisS.H.R.). The diuretic was discontinued.
Transthoracic and transesophageal echocardiography/oppler showed no pericardial effusion. The pericardium
ppeared “minimally” thickened, biatrial enlargement wasvident, and the left ventricle (LV) size and function wereormal. Significant respiratory variations in the Dopplerignals, obtained across the mitral and tricuspid inflows,ould not be documented with confidence. Computed to-ography and magnetic resonance imaging of the heart
econfirmed the possible “minimal” pericardial thickeningnd showed no calcification or any other pathologicbnormalities.
Cardiac catheterization showed near equalization of theight atrial (RA) and pulmonary artery (PA) wedge pres-ures and of the diastolic right ventricle (RV) and LVressures (Figures 1A and B). The discordance between theV and LV systolic pressures could not be convincinglyemonstrated. Coronary arteriography showed no coronaryrterial obstruction.
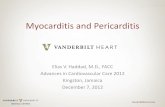
At surgery, the pericardium had an abnormal fibrousppearance with diffuse thickening of 5 to 7 mm (Figure 2)nd was easily removed. After pericardiectomy, the RVystolic pressure decreased from 42 to 30 mm Hg, and theA pressure decreased from 20 to 14 mm Hg. The postop-rative course was uneventful, and the patient was dis-harged on the eighth day with no medications. At the-month postoperative evaluation, the patient wassymptomatic.
ISCUSSIONhis patient had a diagnosis of chronic idiopathic pleuralffusion for 3 years even though the pleural fluid was aransudate. The most common cause of a transudate pleural
ffusion is heart failure.1 Pleural effusions occur in 44% to
5titt
PPIe
aifldimaaf
Fvitfi re the
e2 The American Journal of Medicine, Vol 119, No 7, July 2006
0% of patients with constrictive pericarditis.2,3 Previously,he most common cause of constrictive pericarditis was annfection (especially tuberculosis), but at the present timehe common cause is previous cardiac surgery, secondary toherapeutic mediastinal irradiation and idiopathic.4
athophysiology and Clinical Signs of Constrictiveericarditisn constrictive pericarditis, the heart is enclosed in a thick-
igure 1 A: Right atrial (RA) and pulmonary artery (PA) weariation, the PA wedge pressure is higher at times, but the mean Rs 20 mm Hg. The “x” descent is more prominent than the “y” desceracings show that the diastolic pressures are similar (difference isrst and fourth diastolic periods. Diastolic RV and LV pressure a
ned, rigid pericardium resulting in a restricted and fixed (
mount of space in the heart (Figure 3). On inspiration thencreased venous return to the RA results in an increasedow to the RV, but all of the blood cannot be accommo-ated in the RA and RV. This has two effects: (1) The JVPs increased and increases further on inspiration (Kuss-aul’s sign),5 and the hepatic venous flow and pressures are
lso increased. The JVP has a sharp “x” descent because ofccelerated atrial relaxation and a prominent “y” descentrom early rapid, but short, resistance-free filling of the RV
direct left atrial) pressures are elevated. Because of respiratorysure is 18 mm Hg and the mean pulmonary artery wedge pressureSimultaneous left ventricle (LV) and right ventricle (RV) pressurem) and exhibit the ventricular “square root” sign best seen in the
same as atrial pressures (18-20 mm Hg).
dge (inA presnt. B:
�2-3 m
Figure 1). The latter also results in RV pressure having an

ep“isddstipbaavpcipcditata
rHmisKhirccmt
ahatsDDttmvstincpmmaccto
thRiso
Fncirpc
Fr
e3Constrictive Pericarditis
arly rapid diastolic decrease and increase followed by a flatressure in mid- and late diastole, producing the ventricularsquare root sign” (Figure 1B). The RV systolic pressure isncreased, as is RV output. (2) The interventricular septumhifts to the LV. Pulmonary venous flow is reduced from aecreased RV output in the previous expiration. These con-itions result in a decrease of LV cavity, LV systolic pres-ure, and systemic arterial pressure and flow. In expiration,his process is reversed. Pulmonary venous (PV) return isncreased because of the increased RV output from therevious inspiration, and the interventricular septum shiftsack into the RV. As a result, LV systolic pressure, volume,nd stroke volume (LVSV) are increased, and systemicrterial pressure is increased. The RV systolic pressure,olume, and stroke volume (RVSV) are reduced. Theseathophysiologic changes explain the observed signs ofonstrictive pericarditis, namely, Kussmaul’s sign; paradox-cal pulse; echocardiographic/Doppler velocities in the he-atic veins; tricuspid and mitral inflow velocities; and dis-ordant changes in systolic pressures in the RV and LV. Iniastole, the pressures in both atria and both ventricles aredentical or very similar. Thus, by careful examination ofhe JVP one can know the mean pressures in the whole heartt the patient’s bedside. The other two conditions in whichhis last phenomena occurs are cardiac tamponade and largetrial septal defect or single (common) atrium.
Changes in venous return to the heart in healthy personsesult in a normal decline of arterial pressure of 4 to 6 mmg. In pulsus paradoxus, arterial pressure is greater than 10m Hg. The term “paradoxical” is thus a misnomer because
t is an exaggeration of the normal variation of blood pres-ures with respiration. It was described as “paradoxical” byussmaul5 in 1873 “because of the discrepancy betweeneart action and arterial pulse, and partly because the pulsen spite of apparent irregularity shows in reality a regularepeating decrease or disappearance.” Pulsus paradoxus oc-urs in 30% of patients with constrictive pericarditis. Otherauses include acute/chronic obstructive lung disease, pul-onary embolus, tense ascites, RV infarction, and circula-
igure 2 Abnormally thickened (5-7 mm) pericardium that wasemoved by pericardiectomy.
ory shock.5,6 a
Pericardial knock occurs 0.06 to 0.10 seconds after theortic component of the second heart sound,7 and the thirdeart sound usually occurs 0.12 to 0.16 seconds after theortic component of the second heart sound. On occasionhe two occur at approximately the same time (0.10-0.12econds). The diagnostic finding on echocardiography andoppler studies is the characteristic respiratory variation inoppler flow velocities. This includes an increase in the
ricuspid E velocity on inspiration (which is also present inhe hepatic veins), an increase of more than 25% in theitral E velocity, and a decrease in the tricuspid and hepatic
enous diastolic flow velocity on expiration.6,8 The higherpatial resolution of computed tomography (and its sensi-ivity to diagnose calcification) and magnetic resonancemaging help in determining the pericardial thickness. Mag-etic resonance imaging is said to be able to show a peri-ardium thicker than 4 mm.9 Moreover, in up to 18% ofatients the pericardium may be of normal thickness (� 2m).4 LV systolic function is usually normal. Later abnor-al LV systolic function results from associated coronary
rtery disease or calcium spicules from the calcified peri-ardium that extends into the epicardial layer of the myo-ardium and results in myocardial damage and necrosis. Ifhe pericardium is not calcified, the surgeon can easily “peelff” the pericardium from the heart.
The definitive therapy is pericardiectomy. Medicalreatment is directed to treat the underlying cause. Theigh filling pressure is needed for rapid early filling of theV and LV. The RV and LV are filled almost completely
n the first one-third of diastole; thus, the RV and LVtroke volume is more or less fixed, and the cardiacutput is largely determined by an increase of heart rate.
igure 3 Diagrammatic illustration of the abnormal hemody-amics. The sizes of the circles represent the increases and de-reases of venous return. The sizes of the arrows represent thencreases and decreases of flow. The broken arrows indicate ret-ograde flow. The thick black line outside the heart represents rigidericardium. SVC � superior vena cava; IVC � inferior venaava; HV � hepatic vein. Please see text for additional
bbreviations.
Amm
wpmncse
D
R12
3
4
5
6
7
8
9
e4 The American Journal of Medicine, Vol 119, No 7, July 2006
ttempts to “normalize” venous pressure and heart rateay result in a disastrous decrease of cardiac output andust be avoided.In summary, constrictive pericarditis is an abnormality
ith an anatomic construct that has a characteristicathophysiology and classic physical signs. The abnor-alities may be difficult to document or interpret by
oninvasive tests, especially if the pericardium is notalcified. Our patient illustrates that imaging modalitieshould not be a substitute for a thorough physicalxamination.
Mohammed W. Akhter, MDIsmael N. Nuño, MD
Shahbudin H. Rahimtoola, MD, DSc (Hon)The Griffith Center, Division of Cardiovascular Medicine,
epartment of Medicine, Department of Cardiothoracic Surgery,LAC�USC Medical Center, University of Southern California,
Keck School of Medicine,Los Angeles, Calif.
doi:10.1016/j.amjmed.2005.09.011
eferences. Light RW. Pleural effusion. N Engl J Med. 2002;346:1971-1977.. Wychulis AR, Connolly DC, McGoon DC. Surgical treatment of peri-
carditis. J Thorac Cardiovasc Surg. 1971;62:608-617.. Bertog SC, Thambidorai SK, Parakh K, et al. Constrictive pericarditis:
etiology and cause-specific survival after pericardiectomy. J Am CollCardiol. 2004;43:1445-1452.
. Talreja DR, Edwards WD, Danielson GK, et al. Constrictive pericarditisin 26 patients with histologically normal pericardial thickness. Circu-lation. 2003;108:1852-1857.
. Kussmaul A. Uber Schwieligie Mediastino-Pericardits und den Para-doxenpuls. B Klin Wschr. 1873;10:433. Cited in: Fowler NO. Theparadoxical pulse (pulsus paradoxus). In: The Pericardium in Healthand Disease. New York: Futura Publishing Company, Inc.; 1985:235-245.
. Goldstein JA. Cardiac tamponade, constrictive pericarditis, and restric-tive cardiomyopathy. Curr Probl Cardiol. 2004;29:503-567.
. Tyberg TI, Goodyer AVN, Langou RA. Genesis of pericardial knock inconstrictive pericarditis. Am J Cardiol. 1980;46:570-575.
. Oh JK, Hatle LK, Seward JB, et al. Diagnostic role of Doppler echo-cardiography in constrictive pericarditis. J Am Coll Cardiol. 1994;23:154-162.
. Wang ZJ, Reddy GP, Gotway MB, et al. CT and MR imaging of
pericardial disease. Radiographics. 2003;23:S167-S180.