AIM of Age Friendly Health System Initiative
12
MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020 1 Age‐Friendly Healthcare in the New Normal Mobility: Keeping Aging FUN Montana Geriatric Education Center Colleen Hergott, PT, DPT, GCS October 20,2020 Objectives 1) Describe the benefits of physical activity promotion and fall risk screening for the older adult to help maintain mobility 2) Identify ways to assess mobility in the older adult 3) Identify ways to act on mobility findings to design and provide appropriate care for older adults AIM of Age‐Friendly Health System Initiative Follow an essential set of evidence‐based practices 1 Cause no harm 2 Align with What Matters to the older adult and their family caregivers 3 Institute for Healthcare Improvement Institute for Healthcare Improvement Two Key Drivers of Age‐Friendly Health Systems Mobility: being able to move
Transcript of AIM of Age Friendly Health System Initiative

MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
1
Age‐Friendly Healthcare in the New NormalMobility: Keeping Aging FUN
Montana Geriatric Education Center
Colleen Hergott, PT, DPT, GCS
October 20,2020
Objectives
1) Describe the benefits of physical activity promotion and fall risk screening for the older adult to help maintain mobility
2) Identify ways to assessmobility in the older adult
3) Identify ways to act on mobility findings to design and provide appropriate care for older adults
AIM of Age‐Friendly Health System Initiative
Follow an essential set of evidence‐based practices
1
Cause no harm
2
Align with What Matters to the older adult and their family caregivers
3
Institute for Healthcare Improvement
Institute for Healthcare Improvement
Two Key Drivers of Age‐Friendly Health Systems
Mobility: being able to move
MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
2
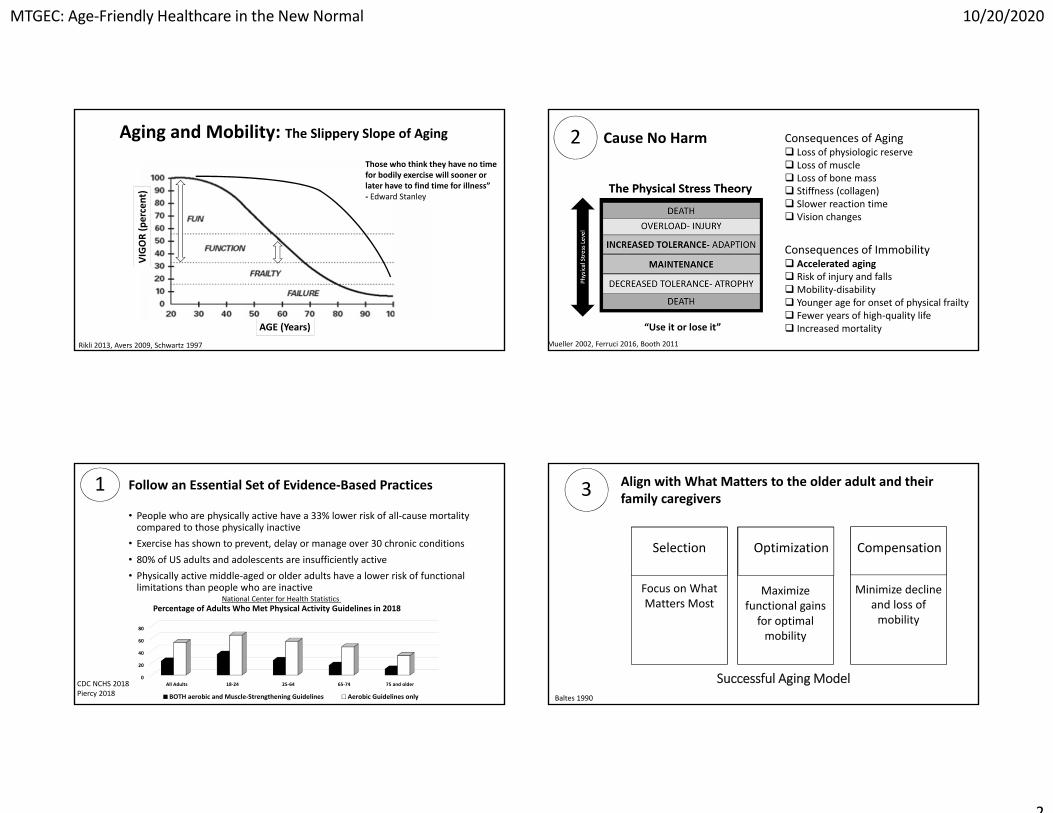
Aging and Mobility: The Slippery Slope of AgingThose who think they have no time for bodily exercise will sooner or later have to find time for illness” ‐ Edward Stanley
Rikli 2013, Avers 2009, Schwartz 1997
VIGOR (percent)
AGE (Years)
0
20
40
60
80
All Adults 18‐24 25‐64 65‐74 75 and older
Percentage of Adults Who Met Physical Activity Guidelines in 2018
BOTH aerobic and Muscle‐Strengthening Guidelines Aerobic Guidelines only
• People who are physically active have a 33% lower risk of all‐cause mortality compared to those physically inactive
• Exercise has shown to prevent, delay or manage over 30 chronic conditions• 80% of US adults and adolescents are insufficiently active• Physically active middle‐aged or older adults have a lower risk of functional limitations than people who are inactive
1 Follow an Essential Set of Evidence‐Based Practices
National Center for Health Statistics
CDC NCHS 2018Piercy 2018
Consequences of Aging Loss of physiologic reserve Loss of muscle Loss of bone mass Stiffness (collagen) Slower reaction time Vision changes
Cause No Harm
Consequences of Immobility Accelerated aging Risk of injury and fallsMobility‐disability Younger age for onset of physical frailty Fewer years of high‐quality life Increased mortality
2
Mueller 2002, Ferruci 2016, Booth 2011
“Use it or lose it”
Successful Aging Model
Focus on What Matters Most
SelectionSelection
Maximize functional gainsfor optimal mobility
OptimizationOptimization
Minimize decline and loss of mobility
CompensationCompensation
Focus on What Matters Most
Selection
Maximize functional gainsfor optimal mobility
Optimization
Minimize decline and loss of mobility
Compensation
3 Align with What Matters to the older adult and their family caregivers
Baltes 1990
MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
3
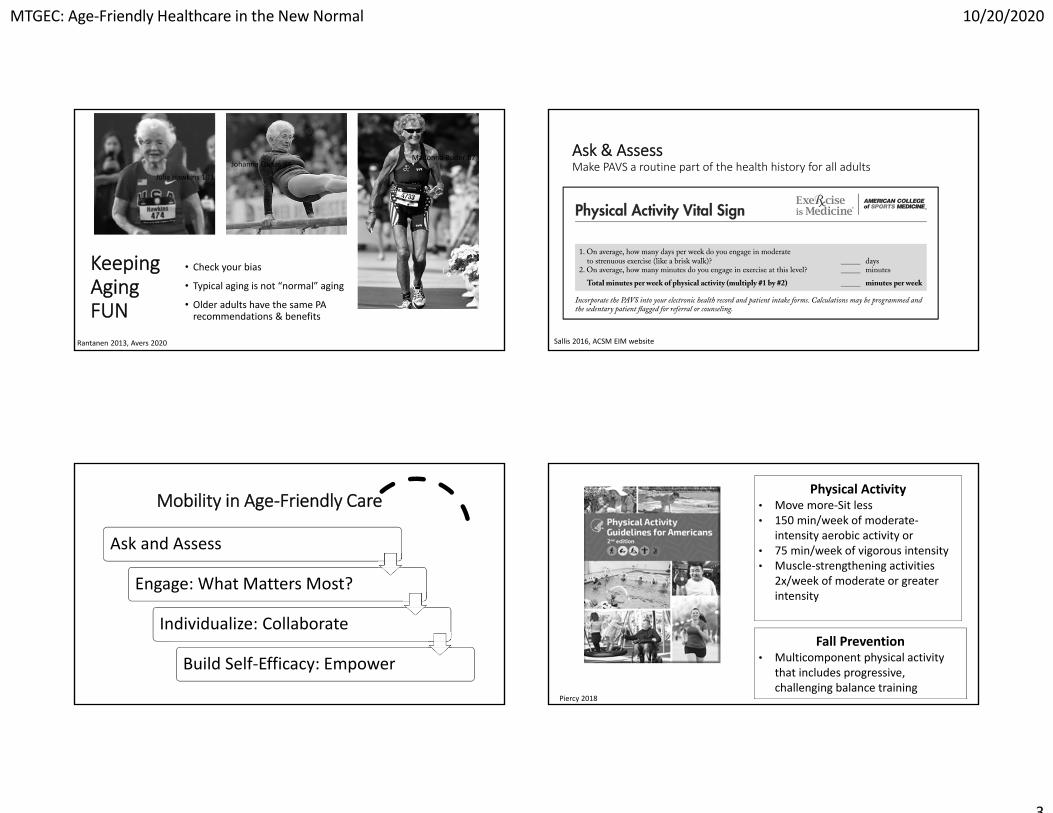
Keeping AgingFUN
• Check your bias
• Typical aging is not “normal” aging
• Older adults have the same PA recommendations & benefits
Julia Hawkins 103
Madonna Buder 87Johanna Quaas 94
Rantanen 2013, Avers 2020
Mobility in Age‐Friendly Care
Ask and Assess
Engage: What Matters Most?
Individualize: Collaborate
Build Self‐Efficacy: Empower
• Physical activity can be quickly & efficiently assessed through the Physical Activity Vital Sign (PAVS or EVS).
• Simple 2‐item questionnaire determines weekly minutes of moderate‐intensity physical activity (PA). Is patient meeting PA recommendations (150 mins/wk)?
• Most effective when embedded as a “vital sign” in electronic medical record (EMR).
Ask & AssessMake PAVS a routine part of the health history for all adults
Sallis 2016, ACSM EIM website
Physical Activity • Move more‐Sit less• 150 min/week of moderate‐
intensity aerobic activity or• 75 min/week of vigorous intensity • Muscle‐strengthening activities
2x/week of moderate or greater intensity
Fall Prevention • Multicomponent physical activity
that includes progressive, challenging balance training
Piercy 2018

MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
4
Build self‐efficacy with positive messaging
• It is MY choice.• PA is a privilege not a punishment.• Feel better, function better, sleep
better.• Being active is a gift to yourself. • Every minute counts. • Permission to do any and all
movement. • Day is a treasure hunt to find
opportunities to move. • Snack mentality for PA.• Be active for enjoyment, fun, pleasure. • Can feel good while doing it.
Segar 2015
0 Minutes:Running late? Too many other concerns on the patient’s list? Relax. Discuss physical activity at the next visit. Hopefully, office staff will have assessed exercise and provided resources.
1 Minute for Brief Advice:Quickly congratulate patients who are getting 150 minutes or more of moderate or greater physical activity. Advise patients who are getting <150 minutes of the importance of physical activity, especially linking benefits to patient’s concerns, problems, and diagnosis.
What Can Busy Providers Do to Encourage PA?
ACSM EIM
2 Minutes for Activity Rx: Review key messages about the importance of physical activity.Offer a generic Exercise Prescription.Suggest useful resources (e.g. smart phone apps, wellness tele‐coaching, community programs, chair exercise DVDs)
5 Minutes for Brief PA Counseling: Assess readiness for change re: exercise habits.Ask what the patient might want to do to be more active and barriers to prevent it ‐‐ brainstorm on how to get around them.Explain how exercise can affect diseases they have (or are at risk for) and how they can go about incorporating activity into their life.
What Can Busy Providers Do to Encourage PA?
ACSM EIM
Exercise is Medicine: Rx for Health Series~30 medical conditions (also in Spanish)

MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
5
1. It is never too late to start2. Supervised strength training is not a
high‐risk activity3. Reduces the effects of chronic
conditions4. Improves balance and reduces risk of
falling5. Reduces lower back pain6. Enhances mental well being raising
self‐esteem and self‐confidence
Muscle‐Strengthening Activities
Check your bias!
YMCA website, Avers 2009
Collaboration Matters
Richards 2015, Orro 2012, Elliot 2018, Karani 2016, Yeom 2009
APTA’s New Public Awareness Campaign Promotes Physical Activity
#Choose PT APTA website
Create a Physical Activity Network
Places
• Parks and Trails• Churches• Fitness Centers• Community Centers
• Senior Centers
Programs
• Area Agency on Aging
• YMCA• SilverSneakers• EBPs•Web‐based programs
People
• Exercise Professionals
• PT (GCS)• OT (BCG)• Registered Dieticians (CSG)
• Pharmacists (BCGP)
3

MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
6
Customizable for YOUR Community!
ACSM EIM Website
Keep Aging FUNAvoiding Harm
through Prevention
Physical activity is an effective means of slowing age‐related deterioration in mobilityIndividual risk factors for mobility decline should be assessed and addressed earlyPreventative and rehabilitative interventions should be considered to optimize the opportunities for good mobility with age Target risk by groups:
• Young people can slow aging declines by being active• Middle‐aged people can prevent future risk for mobility decline by increasing physiological reserve
• Older people who are recovering from an injury or disease should receive rehabilitation
Rantakokko 2013
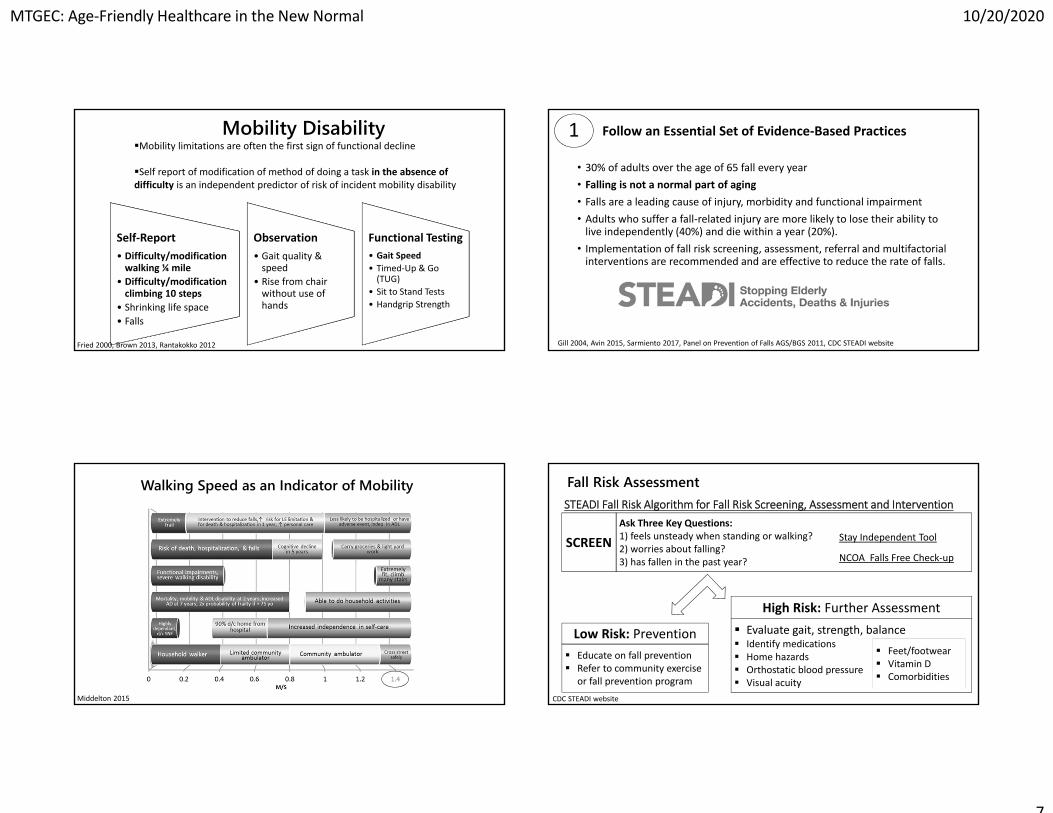
Preclinical Disability
Mobility limitations are often the first sign of functional decline: How do we identify in time to intervene?
Gill 2006, Gill 2014
Slippery Slope of AgingSchwartz 1997
VIGOR (percent)
AGE (Years)
Mobility disability is the gap between an individual’s physical ability and environmental challenges Mobility encompasses the person’s physical ability to move as well as the ability to adapt to the environment Disability can range from preclinical (limitation only exists in highly challenging environments) to severe Loss of independent mobility is associated with higher rates of functional disability, nursing home placement and mortality among older adults
Mobility Disability
Life Space is a measure of mobility capturing an individual’s
typical movement in their environment
Shrinking life space is a behavioral adaptation to declining physiological reserve and capacity
Fried 2000, Brown 2013
MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
7
Self‐Report• Difficulty/modification walking ¼ mile
• Difficulty/modification climbing 10 steps
• Shrinking life space• Falls
Observation• Gait quality & speed
• Rise from chair without use of hands
Functional Testing• Gait Speed• Timed‐Up & Go (TUG)
• Sit to Stand Tests• Handgrip Strength
Mobility DisabilityMobility limitations are often the first sign of functional decline
Self report of modification of method of doing a task in the absence of difficulty is an independent predictor of risk of incident mobility disability
Fried 2000, Brown 2013, Rantakokko 2012
Middelton 2015
Walking Speed as an Indicator of Mobility
• 30% of adults over the age of 65 fall every year• Falling is not a normal part of aging• Falls are a leading cause of injury, morbidity and functional impairment • Adults who suffer a fall‐related injury are more likely to lose their ability to live independently (40%) and die within a year (20%). • Implementation of fall risk screening, assessment, referral and multifactorial interventions are recommended and are effective to reduce the rate of falls.
1 Follow an Essential Set of Evidence‐Based Practices
Gill 2004, Avin 2015, Sarmiento 2017, Panel on Prevention of Falls AGS/BGS 2011, CDC STEADI website
Ask Three Key Questions: 1) feels unsteady when standing or walking?2) worries about falling?3) has fallen in the past year?
SCREEN Stay Independent Tool
NCOA Falls Free Check‐up
Educate on fall prevention Refer to community exercise
or fall prevention program
Low Risk: Prevention Evaluate gait, strength, balance Identify medications Home hazards Orthostatic blood pressure Visual acuity
High Risk: Further Assessment
Feet/footwear Vitamin D Comorbidities
STEADI Fall Risk Algorithm for Fall Risk Screening, Assessment and Intervention
CDC STEADI website
Fall Risk Assessment
MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
8
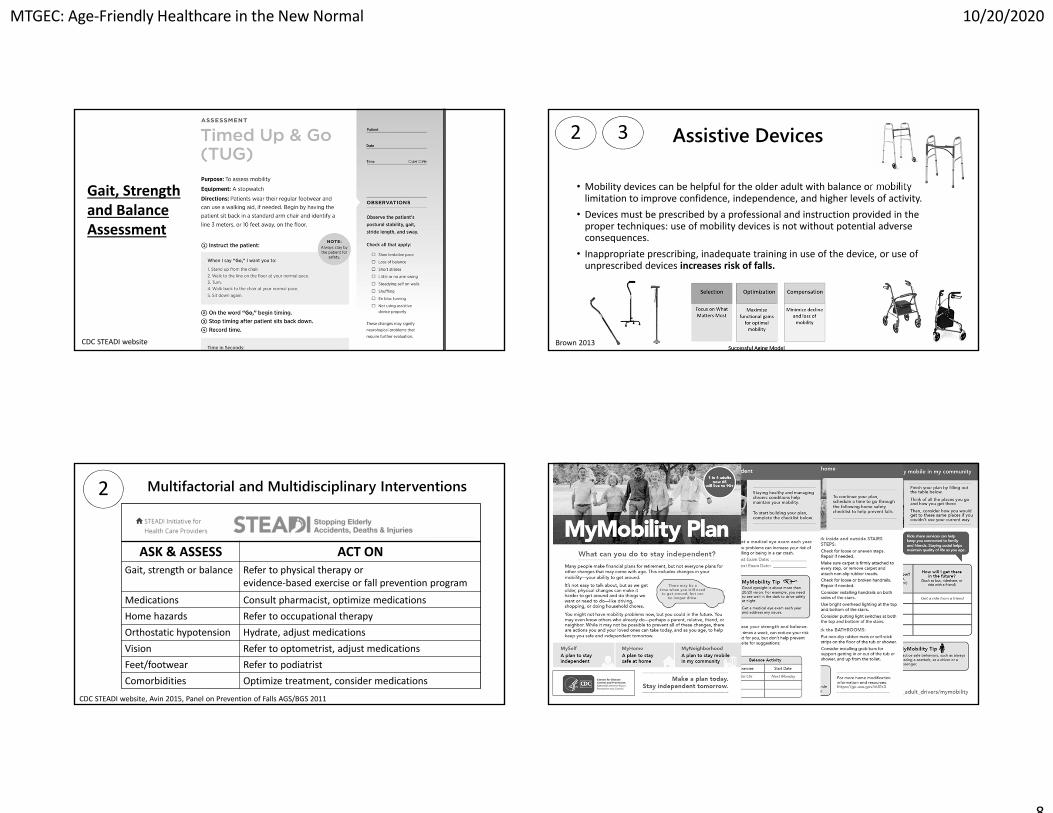
Gait, Strength and BalanceAssessment
CDC STEADI website
ASK & ASSESS ACT ONGait, strength or balance Refer to physical therapy or
evidence‐based exercise or fall prevention program
Medications Consult pharmacist, optimize medicationsHome hazards Refer to occupational therapyOrthostatic hypotension Hydrate, adjust medicationsVision Refer to optometrist, adjust medicationsFeet/footwear Refer to podiatristComorbidities Optimize treatment, consider medications
2 Multifactorial and Multidisciplinary Interventions
CDC STEADI website, Avin 2015, Panel on Prevention of Falls AGS/BGS 2011
• Mobility devices can be helpful for the older adult with balance or mobility limitation to improve confidence, independence, and higher levels of activity.
• Devices must be prescribed by a professional and instruction provided in the proper techniques: use of mobility devices is not without potential adverse consequences.
• Inappropriate prescribing, inadequate training in use of the device, or use of unprescribed devices increases risk of falls.
Assistive Devices32
Brown 2013

MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
9
5%
30%
35%
Care Management
Intervention Care
Care Prevention
Wellness30%
HighRisk
Rising‐Risk
Low‐Risk
Healthy
Action
Initiate Action to Engage the ‘Rising-Risk’Slow, stop or even reverse the progress of mobility‐disability
before ‘High‐Risk’ Care Management
3
Stump 1997
Frailty: a state of increased vulnerability and functional impairment caused by cumulative declines across multiple systems
Natural aging produces a strength decline of 10% a decade
Weakness is the most common initial manifestation of the frailty phenotype
80% of transitions to frailty involve adding exhaustion
Clegg 2011
Slippery Slope of AgingSchwartz 1997
VIGOR (percent)
AGE (Years)
Mobility
Ask and Assess
Engage: What Matters Most?
Individualize: Collaborate
Build self‐efficacy: Empower
Collaboration Matters
Care ManagementRequires Collaboration
Richards 2015, Orro 2012, Elliot 2018, Karani 2016, Yeom 2009

MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
10
37
Health System Connections: The importance of professional collaboration to build a continuum of care
• Identify risk factors impacting mobility
• Identify impairments and develop interventions to optimize and/or compensate
• Address activity limitations
• Improve participation
Address factors associated with reduced mobility
● Balance ● Weakness● Aerobic endurance● Falls● Pain/injury● Use of assistive device● Environmental hazards● Medications● Depression
38
Clinical‐Community Connections: The importance of community collaboration to build a continuum of care
• Fall prevention• Increase physical activity• Promote health
• Motivate behavior change
• Enhance engagement and reduce social isolation
Address factors associated with reduced mobility
● Physical activity/exercise● Fall prevention● Chronic disease self‐management● Nutrition● Pain self‐management● Depression● And more...
NCOA website, Hergott 2020
• Limited access to healthcare services during the pandemic• Increased risk of poor outcomes for those with chronic conditions• COVID‐19 induced shrinking life space and mobility disability
• Loneliness• Loss of social support • Reduced access to services• Increased sedentary behavior• Exacerbation of chronic conditions• Exacerbation of mental health issues (depression, stress, anxiety, substance abuse)
Address secondary consequences of the pandemic
Connections in the “New Normal”: The importance of building a continuum of care during COVID‐19
Narici 2020, Hergott 2020
What are EBPs? How have they changed in the “New Normal”?
Track Health Promotion Program Guidance During COVID‐19
About Evidence‐based Programs NCOA website
Evidence‐based programs (EBPs) offer proven ways to promote health and prevent disease among older adults. They are based on research and provide documented health benefits.
There are four broad categories of evidence‐based programs which can be found at the NCOA website: • falls prevention• general wellness and physical activity• chronic disease self‐management • behavioral health.

MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
11
Where do you find EBPs in your community?
• Area Agency on Aging• YMCA• Churches• Senior Centers• Community Centers• Private Gyms
Virtual Expansion of Physical Activity & Fall Prevention Programs
National Institute on Aging Go4Life
YouTube: Dr. Paul Lam
Virtual Expansion of Physical Activity & Fall Prevention Programs
Age‐Friendly MobilityKeeping Aging FUN
Ask & Assess: Utilize self‐report and functional assessments
Engage: What Matters Most?
Individualize: Utilize resources to find the
best solution to increase mobility for each older
adult
Collaborate: Connect your patients to
people & places that promote mobility (4Ms) for all older
adults
Empower: Aging is inevitable, but
mobility‐disability can be avoided by building self‐efficacy
Be a Role Model: fitness‐ patient care‐
health system

MTGEC: Age‐Friendly Healthcare in the New Normal 10/20/2020
12
Bibliography
1) Avers, D. (2020). We Can Do Better: Aging and the Value of Physical Therapy: 2020 Carole B. Lewis Distinguished Lecture: Address to the APTA Geriatrics Membership at the Combined Sections Meeting, Denver, CO, February 13, 2020. Journal of Geriatric Physical Therapy, 43(3), E31‐E44.2) Avers, D., & Brown, M. (2009). White paper: strength training for the older adult. Journal of Geriatric Physical Therapy, 32(4), 148‐152.3) Avin KG, Hanke TA, Kirk‐Sanchez et al (2015) Management of falls in community ‐dwelling older adults: Clinical guidance statement from the academy of geriatric PT of the APTA. PT 95 (6) 815‐834 4) Baltes, P. B., & Baltes, M. M. (1990). Psychological perspectives on successful aging: The model of selective optimization with compensation5) Booth F, Laye M, Roberts. (2011) Lifetime Sedentary living accelerates some aspects of secondary aging. J Appl Physiol111:1497‐1504.6) Brown, C. J., & Flood, K. L. (2013). Mobility limitation in the older patient: a clinical review. Jama, 310(11), 1168‐1177.7) Clegg, A., & Young, J. (2011). The frailty syndrome. Clinical medicine, 11(1), 72.8) Elliott, S., & Leland, N. E. (2018). Occupational therapy fall prevention interventions for community‐dwelling older adults: A systematic review. American journal of occupational therapy, 72(4), 7204190040p1‐7204190040p11.9) Ferrucci, L., Cooper, R., Shardell, M., Simonsick, E. M., Schrack, J. A., & Kuh, D. (2016). Age‐related change in mobility: perspectives from life course epidemiology and geroscience. Journals of gerontology series a: biomedical sciences and medical sciences, 71(9), 1184‐1194.10) Fried, L. P., Bandeen‐Roche, K., Chaves, P. H., & Johnson, B. A. (2000). Preclinical mobility disability predicts incident mobility disability in older women. Journals of Gerontology‐Biological Sciences and Medical Sciences, 55(1), M43.11) Gill TM, Allore HG, Holford TR et al. (2004). Hospitalization, restricted activity, and the development of disability among older persons. JAM 292; 2115‐2124.
Bibliography
12) Gill, T. M., Allore, H. G., Hardy, S. E., & Guo, Z. (2006). The dynamic nature of mobility disability in older persons. Journal of the American Geriatrics Society, 54(2), 248‐254.13) Gill, T. M., Guralnik, J. M., Pahor, M., Church, T., Fielding, R. A., King, A. C., ... & Allore, H. G. (2016). Effect of structured physical activity on overall burden and transitions between states of major mobility disability in older persons: secondary analysis of a randomized trial. Annals of internal medicine, 165(12), 833‐840.14) Hergott C. Clinical‐community connections during COVID‐19: How are community programs adapting to keep older adults active and healthy at home? Webinar presented at: APTA. 15) Karani, M. V., Haddad, Y., & Lee, R. (2016). The role of pharmacists in preventing falls among America’s older adults. Frontiers in public health, 4, 250. 16) Middleton, A., Fritz, S. L., & Lusardi, M. (2015). Walking speed: the functional vital sign. Journal of aging and physical activity, 23(2), 314‐322.17) Mueller, M. J., & Maluf, K. S. (2002). Tissue adaptation to physical stress: a proposed “Physical Stress Theory” to guide physical therapist practice, education, and research. Physical therapy, 82(4), 383‐403.18) Narici, M., De Vito, G., Franchi, M., Paoli, A., Moro, T., Marcolin, G., ... & Di Girolamo, F. G. (2020). Impact of sedentarism due to the COVID‐19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. European Journal of Sport Science, 1‐2219) Orrow, G., Kinmonth, A. L., Sanderson, S., & Sutton, S. (2012). Effectiveness of physical activity promotion based in primary care: systematic review and meta‐analysis of randomised controlled trials. Bmj, 344, e1389 20) Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society. (2011). Summary of the updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. Journal of the American Geriatrics Society, 59(1), 148‐157.
Bibliography21) Piercy, K. L., Troiano, R. P., Ballard, R. M., Carlson, S. A., Fulton, J. E., Galuska, D. A., ... & Olson, R. D. (2018). The physical activity guidelines for Americans. Jama, 320(19), 2020‐2028
22) Rantakokko, M., Mänty, M., & Rantanen, T. (2013). Mobility decline in old age. Exercise and sport sciences reviews, 41(1), 19‐25.
23) Rantanen, T. (2013). Promoting mobility in older people. Journal of Preventive Medicine and Public Health, 46(Suppl 1), S50 Richards, E. A. (2015). The evolution of physical activity promotion. AJN The American Journal of Nursing, 115(8), 50‐54.
24) Rikli, R. E., & Jones, C. J. (2013). Development and validation of criterion‐referenced clinically relevant fitness standards for maintaining physical independence in later years. The Gerontologist, 53(2), 255‐267.
25) Sallis, R. E., Matuszak, J. M., Baggish, A. L., Franklin, B. A., Chodzko‐Zajko, W., Fletcher, B. J., ... & Puffer, J. C. (2016). Call to action on making physical activity assessment and prescription a medical standard of care. Current sports medicine reports, 15(3), 207‐214.
26) Sarmiento K, Lee R. (2017) STEADI: CDC approach to make older adult fall prevention part of every primary care practice. J Safety Re 63: 105‐109
27) Schwartz RS. (1997). Sarcopenia and physical performance in old age: introduction. Muscle & Nerve, S10‐12.
28) Segar, M. (2015). No sweat: how the simple science of motivation can bring you a lifetime of fitness. Amacom.
29) Stump, T. E., Clark, D. O., Johnson, R. J., & Wolinsky, F. D. (1997). The structure of health status among Hispanic, African American, and white older adults. Journals of Gerontology Series B, 52, 49‐60. 30) Yeom, H. A., Keller, C., & Fleury, J. (2009). Interventions for promoting mobility in community‐dwelling older adults. Journal of the American Academy of Nurse Practitioners, 21(2), 95‐100.
Website Bibliography1) About evidence‐based programs. National Council on Aging website. https://www.ncoa.org/center‐for‐healthy‐aging/basics‐of‐evidence‐based‐programs/about‐evidence‐based‐programs/. Accessed Aug 25, 2020.
2) ACSM EIM. Exercise is Medicine website. https://www.exerciseismedicine.org/support_page.php/health‐care‐providers/. Accessed Sep 6, 2020.
3) Centers for Disease Control and Prevention. Early Release of Selected Estimates Based on Data From 2018 National Health Interview Survey. Division of Health Interview Statistics, National Center for Health Statistics; 2018. Available from: https://www.cdc.gov/nchs/nhis/releases/released201905.htm#7a. Accessed Sep 5, 2020.
4) Center for Disease Control STEADI website. https://www.cdc.gov/steadi/index.html. Accessed Sep 6, 2020.
5) Institute for Healthcare Improvement: http://www.ihi.org/Engage/Initiatives/Age‐Friendly‐Health‐Systems/Pages/default.aspx. Accessed Sept 5, 2020.
6) Lam, P. Tai Chi for Rehabilitation YouTube. https://www.youtube.com/watch?v=6nCaiM9yd9w. Accessed Sep 6, 2020.
7) National Association of Area Agencies on Aging. n4a Web site. https://www.n4a.org. Accessed Sep 1, 2020.
8) National Institute on Aging Go4Life website. https://www.nia.nih.gov/health/exercise‐physical‐activity. Accessed on Sep 6, 2020.
9) Physical Activity Guidelines for Americans 2018. HHS.gov website. https://www.hhs.gov/fitness/be‐active/physical‐activity‐guidelines‐for‐americans/index.html. Accessed Sep 7, 2020.
10) SilverSneakers website. https://tools.silversneakers.com/. Accessed Sep 6, 2020.
11) Your Y at home for active older adults. YCMA website. https://www.ymca.net/your‐y‐at‐home‐for‐active‐older‐adults. Accessed Sept 6, 2020.
12) #Choose PT website. https://www.choosept.com/physicalactivity. Accessed Sep 6, 2020.