Afdalia Cardio_pericarditis Akut
30
BY BY : AFDALIA AFDALIA C111 0 C111 07 1 1 14 14 SUPERVISOR SUPERVISOR : DR. PENDRIK TANDEAN, SPPD-KKV.FINASIM DR. PENDRIK TANDEAN, SPPD-KKV.FINASIM ACUTE PERICARDITIS
description
perikarditis akut
Transcript of Afdalia Cardio_pericarditis Akut

BYBY ::
AFDALIAAFDALIA
C111 0C111 077 1 11414
SUPERVISORSUPERVISOR ::
DR. PENDRIK TANDEAN, SPPD-KKV.FINASIMDR. PENDRIK TANDEAN, SPPD-KKV.FINASIM
ACUTE PERICARDITIS

Patient Identity
• Name : Mr. Y
• Age : 41 years old
• Address : Takallar Pattalasang
• Medical record : 536023
• Admitted : January 1th 2013

History Taking
Chief complaint: Chest painHistory taking: Experienced since 2 days ago before admitted to
the hospital, feel like stab and penetrate to the back. The patient feel comfortable when in bend position and the pain was not improved by rest. Shortness of breath (-) accompanied by sweating, nausea. PND (-), DOE (-)
Fever (+), since 2 days before admitted to the hospital, Headache (-)
Epigastric pain (-), Cough (-)No history of previous chest pain,Defecation & urination normal

History of illness
Hypertension history (-), DM (-), heart disease (-)
History of smoking (-) Post. Op urolithiasis December 2012

Physical Examination
• General Status :
Moderate-illness/normal Body
Weight/conscious
• Vital Sign : Blood Pressure : 110/70 mmHg Pulse : 88 bpm, regular Respiratory rate : 20 tpm,
abdominothoracal Body temperature : 36,8º C

Head Examination• Eyes : anemic -/-, icterus -/-• Lip : cyanosis (-)• Neck : lymphadenopathy (-), JVP R +2 cmH2O
Chest Examination• Inspection : symmetric R=L, normochest• Palpation : mass (-), tenderness (-), VF R=L• Percussion : sonor• Auscultation : breath sound : vesicular
additional sound : ronchi - /- wheezing -/-

Cardiac Examination
• Inspection : IC not visible• Palpation : IC not palpable • Percussion : Normal • Auscultation : Heart sound I/II regular,
murmur (-)

Abdominal Examination - Inspection : flat and following
breath movement- Auscultation : peristaltic sound (+) ,
normal- Palpation : liver and spleen
unpalpable- Percussion : tympani, ascites (-)
Extremities - Oedema : pretibial -/-
dorsum pedis -/-


Interpretation
- Rhythm : Sinus rythm- Hearth Rate : 85 x/minute- P wave : 0,08- PR Interval : 0,12 ms- QRS Complex : 0,08- Axis : Normoaxis- ST Segment : - L1+aVL = ST Depresion
- - II, III, aVF = ST Elevation Inferior
- - V1+V2 = ST Elevation Septal- - V3+V4 = ST Elevation Anterior- - V5+V6 = ST Elevation Lateral
Conclusion : Sinus rhythm, HR 85x/minute, normoaxis, ST elevation
mostly in all leads.

LABORATORY FINDINGS
(01/01/2013)
• Routine Blood Test
RBC : 4,40 x106/mm3
WBC : 24,1 x103/mm3
HB : 12,1 g/dlHCT : 37,41 %PLT :386.103/mm3
• Biochemical blood test
GDS : 118 mg/dl Ureum : 78 mg/dlCreatinin : 5,4 mg/dlSGOT : 24 U/L SGPT : 35 U/LTot.Chol: 96 mg/dl HDL : 6 mg/dlLDL : 32 mg/dl TG : 195 mg/dl

Electrolyte (01/01/2013) Sodium : 138 mmol/L Potassium : 4,4 mmol/L Chloride : 110 mmol/L
Cardiac Enzyme (03/01/2013) CK-MB : 151 U/L Trop. T : 1,5

WORKING DIAGNOSIS
CHEST PAIN e.c SUSPC. ACUTE PERICARDITIS

PLANNING
Thorax PAEchocardiography

MANAGEMENT
O2 2 L/minIVFD NaCl 0.9% 500cc/24h/ivCeftriaxone 2 gr/24h/ivIbuprofen 4x400 mg

Acute pericarditis

DEFINITION
•Acute pericarditis is an inflammation of the pericardium characterized by chest pain, pericardial friction rub, and serial electrocardiographic (ECG) changes (see an example of such an ECG below).
•Happened more man than woman

Causes
• Idiopathic (idio and pathy) – 86%Infective (viral or bacterial) – 7%Following a myocardial infarction or
cardiac surgery (Dressler’s syndrome)Radiation therapyNeoplastic disease (commonly lung or
breast) – 6%Connective tissue disease

PATHOPHYSIOLOGY
Pericardial tissue damaged by bacteria or other substances releases chemical mediators of inflammation (prostaglandins, histamines, bradykinins, and serotonin) into the surrounding tissue, thereby initiating the inflammatory process. Friction occurs as the inflamed pericardial layers rub against each other. Histamines and other chemical mediators dilate vessels and increase vessel permeability. Vessel walls then leak fluids and protein (including fibrinogen) into tissues, causing extracellular edema. Macrophages already present in the tissue begin to phagocytize the invading bacteria and are joined by neutrophils and monocytes. After several days, the area fills with an exudate composed of necrotic tissue and dead and dying bacteria, neutrophils, and macrophages. If the cause of pericarditis isn't infection, the exudate may be serous (as with autoimmune disease) or hemorrhagic (as seen with trauma or surgery). Eventually, the contents of the cavity autolyze and are gradually reabsorbed into healthy tissue.

RISK FACTORS
Pericarditis occurs in people of all ages. However, men between the ages of 20 and 50 are more likely to get it.People who are treated for acute pericarditis may get it again. This may happen in 15 to 30 percent of people who have the condition. A small number of these people go on to develop chronic pericarditis.

CLINICAL FEATURES
Chest painRetrosternal chest painmore likely to be sharp and pleuritic with coughing, inspiration, swallowingworse by lying supine, relieved by sitting and leaning forwardCan often radiate to the neck, arms, or left shoulder.
Sudden in onset Pleuritic and sharp in nature Exacerbated by inspiration Mild feverDyspnea, orthopnea, tachycardiaPericardial friction rub Present in 85% of cases of pericarditis Pericardial friction rub is audible throughout the respiratory cycle, whereas the pleural rub disappears when respirations are on hold.

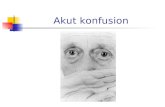
ECG (acute pericarditis)

EKG in Pericarditis
Widespread upward concave ST-segment elevation and PR-segment depression
If the ratio of ST-segment elevation to T-wave amplitude in V6 > 0.24, acute pericarditis is almost always present.
The EKG changes have 4 phases during the course of illness

Treatment
Bed rest as long as fever and pain persistTreatment of the underlying cause, if it can be
identifiedNonsteroidal anti-inflammatory drugs,
corticosteroidsAntibacterial, antifungal, or antiviral therapyNSAID (aspirin, indomethacin) are generally
accepted as effective for relieving symptoms of chest pain
NSAID ketorolac tromethamine rapid resultsColchicine may be a useful adjunct in those who
do not respond to NSAIDs alone

Complication
Pericardial effusionCardiac TamponadeConstrictive pericarditis

Prognosis
Pericarditis is usually a benign disorderDiagnosis relates to underlying causeBut any cause can lead to an effusion and
tamponade which can lead to deathPericarditis can also progress to pericardial
constriction and heart failure

Deferential diagnosis
MIAngina PectorisPulmonary Emboli


Pericarditis vs AMI
PericarditisPericarditis MIMI
ST segmentST segment Diffuse,concave elevation in all Diffuse,concave elevation in all leads except aVRleads except aVR++ V6 w/o V6 w/o reciprocal changesreciprocal changes
Height Not > 5mmHeight Not > 5mm
Localized, convex, with Localized, convex, with reciprocal changes in infarctreciprocal changes in infarct
Height may be > 5 mmHeight may be > 5 mm
PR depressionPR depression FrequentFrequent Almost neverAlmost never
Q wavesQ waves Not usual, unless with infarctNot usual, unless with infarct Common with q wave infarctCommon with q wave infarct
T wavesT waves Inverted after J returns to Inverted after J returns to baselinebaseline
T inversions and ST ↑ are not T inversions and ST ↑ are not seen simultaneously on the seen simultaneously on the same EKG same EKG
Inverted while ST still elevatedInverted while ST still elevated
T inversions and ST ↑ can be T inversions and ST ↑ can be seen simultaneously on the seen simultaneously on the same EKG same EKG
ArrhythmiasArrhythmias RareRare FrequentFrequent
Conduction Conduction disturbancesdisturbances
RareRare FrequentFrequent

THANK YOU