Adolescent Bariatric Surgery - October 2009
50
Adolescent Bariatric Adolescent Bariatric Surgery Surgery Kirk Reichard MD, MBA, FACS, FAAP
-
Upload
cardiacinfo -
Category
Health & Medicine
-
view
1.090 -
download
1
description
Transcript of Adolescent Bariatric Surgery - October 2009

Adolescent Bariatric SurgeryAdolescent Bariatric Surgery
Kirk Reichard MD, MBA, FACS, FAAP

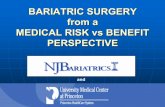
CDC Obesity Trends
1998
2007
1990
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%

Pediatric Obesity


Severe Pediatric Obesity
BMI > 40
BMI Z score >2.5
Children with severe obesity start with early onset morbid obesity– 4 yo who weighs >80 lbs– 8 yo who weighs > 160lbs

How much extra weight?
BMI 25 BMI 40 BMI 45 BMI 50
15 yo Female
Ht: 64 inches145 235 265 290
15 yo Male
Ht: 69 inches170 270 305 340
A gain of 10 extra pounds (physiologic 5-10lbs/yr) per year between kindergarten and high school = BMI of 40

Prevalence
Between 1 to 3%
of adolescents have BMI >40
750,000 adolescents in the United States with BMI>40
More common disease than cystic fibrosis, juvenile diabetes, and childhood cancer combined

BMI Tracking
Children (age 12) with BMI>99% followed into adulthood (age 27)– 100% BMI>30– 90% with BMI>35– 65% with BMI>40
Freedman et al. Cardiovascular Risk Factors and Excess Adiposity Among Overweight Children and Adolescents: The Bogalusa Heart Study. Journal of Pediatrics. 2007; 15: 12-7

Obesity Complications

Pediatric Metabolic Syndrome
Explains the relationship between obesity and CV Disease– Central Obesity– Insulin resistance– Dyslipidemia– Hypertension– Glucose intolerance
Cook, S, et al. Arch Pediatr Adolesc Med. 2003;157:821-827.
MS = 3 or more

Pediatric Metabolic Syndrome
Cali, A. M. G. et al. J Clin Endocrinol Metab 2008;93:s31-s36

Pediatric Metabolic Syndrome
Weiss, R. et al. N Engl J Med 2004;350:2362-2374
CRP goes up (BAD!)
Adiponectin goes down (also BAD!)

Cardiovascular Risk Factors
≥1 ≥ 2 ≥ 3 ≥ 4
50-85% 36% 9% 2% 0%
85-95% 51% 19% 5% 1%
95-99% 70% 39% 18% 5%
>99% 84% 59% 33% 11%
Risk Factors:Triglycerides
Cholesterol
HDL
Insulin (fasting)
Systolic BP
Diastolic BP
Freedman et al. Cardiovascular Risk Factors and Excess Adiposity Among Overweight Children and Adolescents: The Bogalusa Heart Study. Journal of Pediatrics. 2007; 15: 12-7

Berenson GS, Srinivasan SR, Bao W, Newman WP III, Tracy RE, Wattigney WA. Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults: the Bogalusa Heart Study. N Engl J Med. 1998; 338: 1650–1656.
Atherosclerosis vs Cardiovascular Risk Factors

Pediatric Obesity and Mortality
Neovius, M, et al. BMJ 2009;338:b496

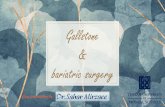
The Cost of Obesity
Wee, et al., Am Journal of Public Health, January, 2005

0
20000
40000
60000
80000
100000
120000
140000
160000
180000
200000
<25 25-30 30-35 >35
BMI
$Males
Females
Daviglus, et.al, JAMA, December 8, 2004
The Cost of Obesity

Cost of Childhood Obesity
Thompson Medstat Research Brief, , 2006

Childhood Obesity
Thompson Medstat Research Brief, , 2006

Childhood Obesity
Thompson Medstat Research Brief, , 2006

duPont WTM Cohort
92 patients treated in 2005 with BMI over 40.– 55 with BMI 40-45– 20 with BMI 45-50– 13 with BMI 50-55– 4 with BMI >55

duPont Morbidity Rates
Acanthosis/ Hyperinsulinism: 71%– Diabetes: 4%
Asthma: 48% Dyslipidemia: 45% PCOS: 35% of females Psych (Depression, Anxiety, Bipolar): 29% Nonalcoholic Steatohepatitis: 24% Hypertension: 22% Sleep Disordered Breathing: 20% Ortho (SCFE, Blounts): 8%

duPont Weight Management
BMI>40 Patients by Age (n=95)
0
5
10
15
20
25
30
<= 12 13 14 15 16 17 18 19+
Years of Age (Avg=17.2, Range 8-23)
Fre
qu
ency

duPont Weight Management
Diagnosis Codes
0
500
1000
1500
2000
2500
0 1 2 3 4 5 6 7+
# of Diagnosis codes (Median=2.3, Range 1-15)
En
co
un
ters

duPont Weight Management
Weight Change
8
5
50
28
0 10 20 30 40 50 60
<5% decrease
3-5% decrease
No change
Increased BMI
% of Patients

duPont Weight Management
# Unique Patients 95
Inpatient and Outpatient Encounters 6576Hospital Discharges 63Avg Encounters per Unique Pt 69.2Ranges of Encounters per Unique Pt. 5-425
Charges per Unique Patient $52,939Total Charges $5,029,205

Adult Bariatric Surgery
NIH Consensus Panel- 1991– Failure of Medical and Dietary Treatments– Substantial excess morbidity and Mortality
Surgery Indicated for selected pts:– Documented failure of non-surgical weight loss – BMI> 40– BMI> 35 with at least 2 co-morbidities– Adults Age 18+

“Who would have thought it? An operation proves to be the most effective therapy for adult-onset
diabetes mellitus”
Pories WJ, Swanson MS, MacDonald KG, et al 1995;222:339-350

Bariatric Procedures
Bypass of part of the intestine– Roux-en-Y Gastric
Bypass– Duodenal switch, etc.

Adult Bariatric- RYGBP
Outcomes– 50-75% Excess Wt Loss (3+ years)
Complications– GI Leak (5%), Bleeding (3.5%), Wound (9%), Pulm (6%),
DVT/PE (3%)– Stenosis, bowel obstruction (up to 20% each), Ulcers, Gall
Stones, Iron and vitamin deficiency– Mortality 0.5-2%

Bariatric Procedures Restrictive
– Decrease size of stomach, early Satiety
– Vertical Banded Gastroplasty, Sleeve Gastroplasty
– Lap-Band Laparoscopic Adjustable Gastric Banding*
*FDA approved for age 18+ only

Lap Band® Adverse Events
Intra operative– Conversion to open 1(0.1%)– Iatrogenic gastrostomy 1(0.1%)
Early Post-operative– Hemorrhage 1(0.1%)– Port infection 6(0.6%)– Stomal obstruction 14(1.4%)– Perforation 3(0.3%)
Late– Mechanical dysfunction 5 (0.4%)– Erosion 2(0.2%)– Slippages 23(2.3%)
Ponce, et al., 2005

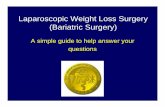
Comparing Weight-Loss Results
Source: O’Brien et al. Obesity is a Surgical Disease: Overview of Obesity and Bariatric Surgery, ANZ J Surg, 2004; 74: 200-204.
Gastric Bypass
LAP BAND®

Adolescent Bariatric Surgery
50% of bariatric surgeons have done a bariatric procedure on an adolescent in the past year
Most not done in a pediatric setting Estimated 1,000 – 10,000 bariatric procedures
done in children < 18 yearly.

Adolescent Bariatric Surgery
Inge, et al., Pediatrics, 2004– Multidisciplinary Pediatric Panel– Lack of evidence-based guidelines– More restrictive criteria:
BMI>40 with severe co-morbidity (Type II DM, Obstructive sleep apnea, Pseudotumor cerebri)
BMI>50 with less severe co-morbidity

Adolescent Bariatric Surgery Contraindications
Physical immaturity Medically Treatable Cause of Obesity Inability to participate in follow-up Patient cognitively unable to participate in decision Active psychiatric/ behavioral issues that would preclude
participation Substance Abuse Current or planned pregnancy (within 2 years)
Inge, et al.

Adolescent Bariatric SurgeryOutcomes
Meta-analysis November 2008
Procedure Number Outcome Evidence Rating
Band 8 studies
352 Pts
Wt Loss
Co-morbiditiesMod/Weak
Weak
Bypass 5 Studies
131 Pts
Wt Loss
Co-morbidities
Mod/Weak
Insuff/weak
Other 5 Studies
158 Pts
Wt. Loss
Co-Morbidities
Insuff
Insuff
Treadwell, J, et al, Ann Surg 2008;248: 763-776

Adolescent Bariatric Surgery Outcomes
APSA Adolescent Bariatric Study Group, Adolescent Lap-Band® Group, Teen LABS (NIH)
ASMBS Pediatric Committee
Teen LABS (NIH)
FDA trials
DuPont has been granted an Investigational Devise Exemption (IDE) from the FDA for Lap Band use

DuPont Adolescent Lap-Band FDA Study
FDA, CRRC, IRB approved trial
14-17 years of age
BMI>40
Co-morbidity
Obesity for at least 5 years
At least 6 months supervised treatment
Commit to 5 year follow-up

Adolescent Lap-Band® Exclusions
Age less than 14 years
History of inflammatory bowel disease
Chronic use of anti-inflammatory medication
Pregnancy or planning pregnancy
Uncontrolled eating disorder
Uncontrolled mental health disorder

Our Treatment Program
Family Behavioral Therapy
Individualized
Multidisciplinary
Well balanced hypocaloric diet
Home exercise regimen
Surgical option is not primary focus

Team Composition
Weight management team with adolescent experience– Pediatrician– Surgeon– Nutritionist– Psychologist– Exercise Physiologist– Study Coordinator: organization of data

Adolescent Lap-Band® Preoperative Program
Monthly visits for 6 months
Evaluative Component
Completion of Preoperative Workbook
Improve: – Fitness– Nutrition– Family Functioning– Psychological Functioning
Protein sparing fast for 2 weeks

Adolescent Lap-Band® post-op issues
Visits every 3-6 weeks for adjustments Long-term Compliance is Critical
– Family/ peer support– Band Adjustments– Ongoing nutritional support– Exercise– Behavior Modification
Transition to “adult” life

duPont Lap Band® Results
26 Patients to date21 FemaleAverage age 16 years old

duPont Lap Band® Results- Excess Weight Loss
0
10
20
30
40
50
60
70
0 6 12 18
Months
%E
WL

duPont Lap Band® Results- Metabolic Syndrome

Adverse Events
No perioperative complications
Hospital Stay: <48 hours.
No adverse events requiring a second operation
No adolescents asking for their band to be removed
No pregnancies
None lost to follow-up

What We Have Learned
Morbid obesity in adolescents is a disease state even without any other medical comorbidities
Modest to Significant Lifestyle changes result in weight stability but only clinically significant weight loss (5-10% decrease in BMI) in a small percentage of patients
Severe calorie restriction (<1000 calories/day) will result in weight loss
All weight loss options require lifestyle changes

Questions
Is there any long term benefit (medical or psychological) in doing obesity surgery in childhood instead of early adulthood
What (if any) surgical procedure is best to do in children
What should we do with severely morbidly obese children who have limited decisional capacity or with non stable family units
.