Admissions from Cardiac Cath Lab to RICU
22
A Case of Hyperferritinemia due to HLH Michelle Fallon Antrim Area Hospital
-
Upload
nhs -
Category
Health & Medicine
-
view
243 -
download
2
Transcript of Admissions from Cardiac Cath Lab to RICU
A Case of Hyperferritinemia due
to HLHMichelle Fallon
Antrim Area Hospital
Case Summary
History:
41 year old man admitted to Antrim Area Hospital in June 2014
Generally unwell- headache, rigors, sore throat and unproductive cough
LRTI 2 weeks previously treated with amoxicillin
Noted weight loss of ½ stone past 2 months, night sweats
PMHx: Chronic back pain, no medications
Social Hx: Non-smoker, builder
Initial assessment
Examination:
Pyrexic 40.9 degrees, HR 140, BP 100/50
RR 30, Sats 90% RA, Chest clear
Jaundiced, hepato-splenomegaly, tender RUQ
No meningism or focal neurology
No lymphadenopathy or rash, throat clear
Initial investigations:
Hb 133, WCC 2.8, PLT 84, CRP 97, Deranged LFTs
U&E/Coagulation profile unremarkable
ABG compensated metabolic acidosis, Lactate 2.5
Clinical course
Initial management
Admitted to medical ward
Managed as sepsis/PUO
Broad spectrum antibiotics/IV fluids
Multiple Ix sent
Deterioration
Persistent pyrexia & worsening LFTs
Increasing oxygen requirements developed respiratory failure
CT CAP: Mediastinal hilar lymphadenopathy, bilateral small pleural effusions, perihilar air space and ground glass shadowing. Enlarged spleen.
Referred to ICU for respiratory support
ICU management
Differential diagnosis: Haematological malignancy, atypical CAP/sepsis, PCP, TB, viral hepatitis, HIV, etc
Required NIV, high oxygen requirements
Anti-microbial coverage
Did not require any other organ support
Hb drop 130 to 70= pancytopenic
Iron profile: Ferritin > 11,000 ng/ml
Required transfusion
Ix of note: LDH 795, EBV 16,000 copies
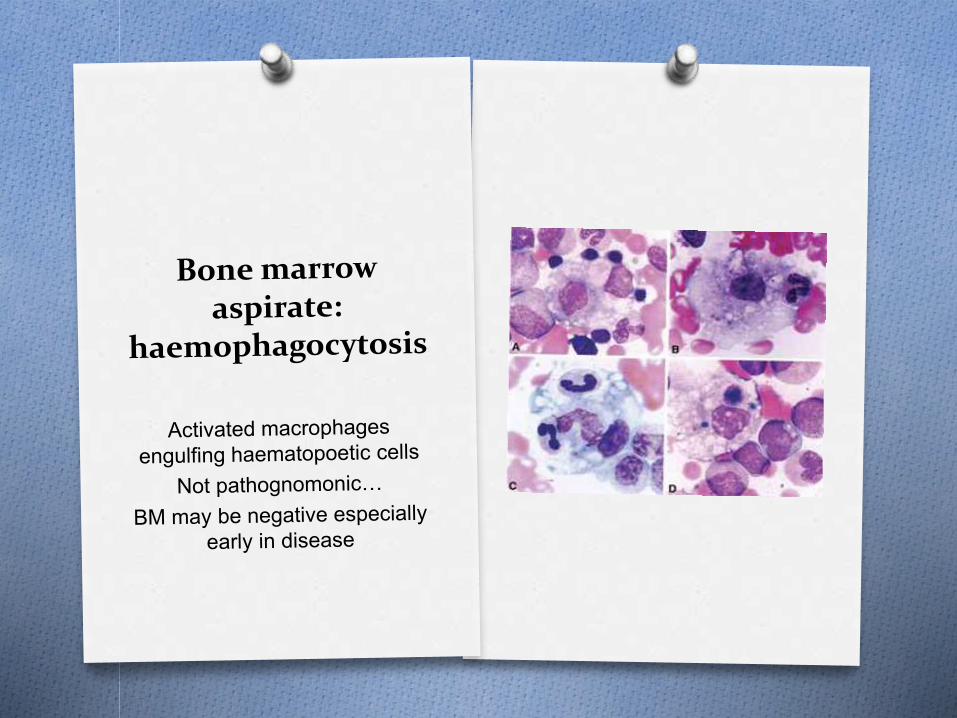
Bone marrow biopsy showed haemophagocytosis
Diagnosis: Acquired Haemophagocytic
Lymphohistiocytosis (HLH) secondary to
infection with Epstein Barr Virus
HaemophagocyticLymphohistiocytosis (HLH) Why do we need to know about this?
=rare haematological condition!
Causes SIRS/MODS and may resemble
sepsis
Patients may present to ICU
Likely under diagnosed
Fatal if not treated
Requires specific treatment
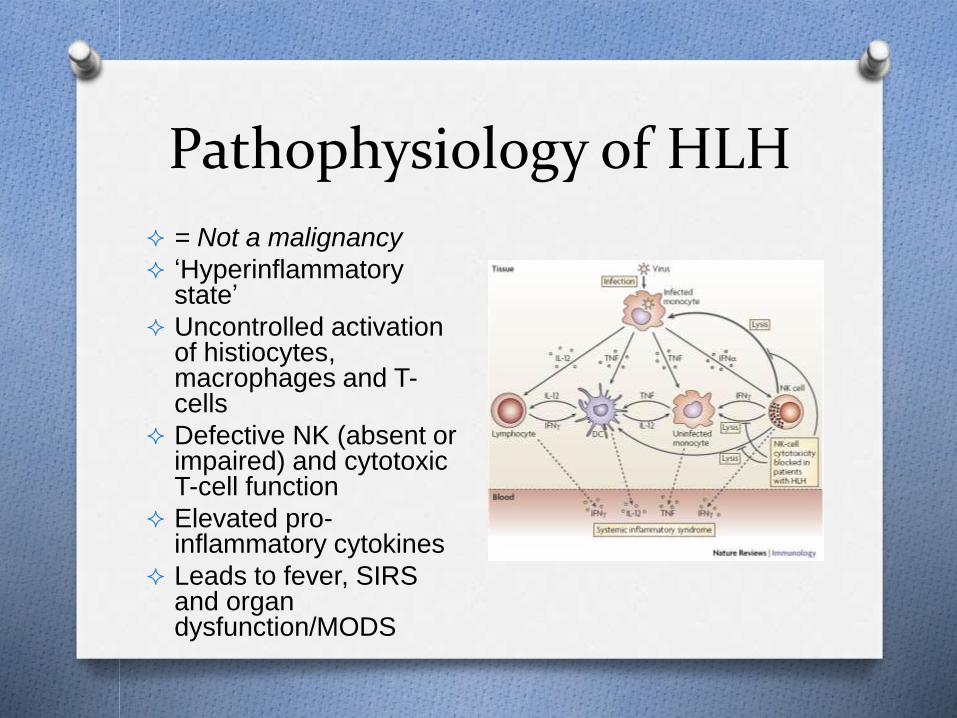
Pathophysiology of HLH
= Not a malignancy
‘Hyperinflammatorystate’
Uncontrolled activation of histiocytes, macrophages and T-cells
Defective NK (absent or impaired) and cytotoxic T-cell function
Elevated pro-inflammatory cytokines
Leads to fever, SIRS and organ dysfunction/MODS
Primary HLH
Familial/genetic HLH
Usually presents in infants < 12 months old
Sub-classified into FHL 1-5 depending upon protein abnormality/gene mutation
FHL 2 most common (= perforin mutation)
Immune deficiency syndromes associated with HLH= CHS-1, (Chediak-Higashi),GS-2 (Griscelli Syndrome), XLP
Can still be triggered by infection
Secondary HLH
Secondary or ‘acquired’ HLH associated
with:
Viral infections = classically due to EBV,
CMV
Other infections (bacterial, fungal, etc)
Malignancies
Rheumatological disorders (Macrophage
activating Syndrome= MAS)
Immune deficiency disorders
Diagnostic Criteria
International Histiocytosis Society 2004. Requires 5 of 8:
1. Fever
2. Splenomegaly
3. Cytopenia
4. Hypertriglyceridemia or hypofibrinogenemia
5. Haemophagocytosis (on BM or LN biopsy)
6. Hyperferritinemia
7. Elevated IL-2 (high soluableinterleukin-2-receptors)
8. Decreased NK cell activity
Henter et al (2007)
Ferritin
Hallmark of HLH is raised ferritin….
Ferritin is an iron binding molecule (L&H subunits)
Cytoplasmic levels of ferritin regulated by iron levels but also influenced by cytokines/inflammation
Hepatocytes, macrophages and Kupffer cells secrete ferritin
Often elevated as an acute phase reactant
Ferritin levels
Serum ferritin considered elevated if above:
> 200 ng/mL women
> 300 ng/mL men
Adams (2008) proportion of general
population will have a serum ferritin
between 200-1000 ng/mL
Causes of raised ferritin
Iron overload (haemochromatosis, transfusion, iron loading anaemia, porphyria)
Liver disease (acute/chronic)
Alcohol/Obesity (metabolic syndrome)
Autoimmune disease (RA, SLE etc)
HHCS (hereditary hyperferritinemia/cataract syndrome)
Still’s disease*
Antiphospholipid Syndrome*
Haemophagocytic syndrome/MAS*
Sepsis/septic shock*
* Associated with very high ferritin levels (Rosario et al 2013)
Critical illness and ferritin
Raised due to inflammatory process
Anaemia common (complex)
Typically in critically ill patients: raised ferritin/ low iron
Garcia et al (2007) reported that high ferritin levels were associated with increased mortality in children with septic shock
? Marker of severity of illness
Rosario et al (2013) proposed hyperferritinemia involved pathogenesis of disease rather than just a marker
Treatment of HLH
Common regimen: (HLH-2004 protocol)
Dexamethasone (chemo-immune therapy)
Cyclosporine A (CSA)
Etoposide (associated with increased survival in adults with secondary HLH, especially effective for EBV associated disease)
Other:
IVI immunoglobulin (IVIG)
HSCT (familial/genetic or severe/recurring)
Plasma exchange
IT methotrexate (CNS involvement)
Case reports- monoclonal antibodies
Patient progress
Transferred to haematology ward after 8 days in ICU
Commenced Dexamethasone/CiclosporineA/Etoposide
Ferritin levels decreased to 1896
Received GCSF/blood transfusion
Clinically improved
Discharged home (3/52 following admission)
Re-admission: a month later, severe back pain, neutropenia, ferritin increased to 4000, LDH 828. Dexamethasone dose increased.
Outcomes
Retrospective analysis of HLH-94 treatment protocol: 54% of 249 patients treated survived. George (2014).
Higher survival rates for MAS
Untreated the familial condition is fatal
Lack of recognition may contribute to higher mortality
Lin et al (2011) fall of ferritin levels of less than 50% associated with increased risk of death in children treated for HLH
Summary
Haemophagocytic Lymphohistiocytosis
(HLH) is rare but under recognized
Can cause SIRS/MODS and mimic sepsis
May present in critical care
Multiple causes of hyperferritinemia
Markedly elevated levels should prompt
consideration of HLH as a diagnosis
References: Adams, P. Management of Elevated Serum Ferrtin Levels. Gastroenterology and Hepatology 2008;
4(5): 333-334
Castillo, L et al. Secondary hemophaocytic lymphohistiocytosis and severe sepsis/systemic inflammatory response syndrome/multiorgan dysfunction syndrome/macrophage activation syndrome share common intermediate phenotypes on a spectrum of inflammation. Pediatric Critical Care Medicine 2009; 10 (3): 387-92
Demirkol, D et al. Hyperferritinemia in the critically ill child with secondary hemophagocyticlymphohistiocytosis/sepsis/multiple organ dysfunction syndrome/macrophage activation syndrome: what is the treatment?. Critical Care 2102; 16:R52
George, M. Hemophagocytic lymphohistiocystosis: a review of etiologies and management. Journal of Blood Medicine 2014; 5:69-86
Grom, A. Macrophage Activating Syndrome: A review of diagnosis, treatment and prognosis . The Rhuematologist 201
0Heming, N et al. Iron deficiency in critically ill patients: highlighting the role of hepcidin. Critical Care 2011; 15: 210
Henter J et al. Histiocyte Society HLH-2004: diagnostic and therapeutic guidelines for hemophagocyticlymphohystiocytosis. Pediatric Blood Cancer 2007;48(2):124-131
Lin T et al. Rate of Decline of Ferritin in Patients with HLH as a Prognostic Variable for Mortality. Paediatric Blood and Cancer 2011; 56(1) 154-155
Raschke, R et al. Haemophagocytic Lymphohistiocytosis: A Potentially Underrecognized Association With Systemic Inflammatory Response Syndrome, Severe Sepsis, and Septic Shock in Adults. Chest 2011; 4:140
Rosario, C et al. The Hyperferritinemic Syndrome: macrophage activating syndrome, Still’s disease, septic shock and catastophic antiphospholipid syndrome. BMC Medicine 2013; 11:185
Tothova, Z et al. Haemophagocytic Syndrome and Critical Illness: New Insights into Diagnosis and Management. J Intensive Care Med 2014 (Epub ahead of print)
Questions…?