
Adhesions and bands
50
INTESTINAL OBSTRUCTION
-
Upload
kcmct20 -
Category
Health & Medicine
-
view
1.369 -
download
2
Transcript of Adhesions and bands
INTESTINALOBSTRUCTION

ADHESIONS
Aetiology
Iatrogenic (Post operative) : Individual susceptibilityMay be induced by talc (powder from
gloves), cotton or linen (surgical mops, suture material)
Inflammatory / Infections : Following appendicitis and PIDFollowing peritonitis (specially biliary)Plastic type of peritoneal tuberculosis
Ischaemia :
Arterial or venous occlussionOccurs at sites of anastomosesIschaemia due to mobilisation of peritoneum
Irradiation : Radiation enteritis
Drugs : Practolol
Types
Fibrinous :EarlyEasy to do adhesiolysis / flimsyMay reduce over time
Fibrous : Occurs laterDifficult to do adhesiolysis / denseNo tendency to improve over timeOccurs due to associated ischaemia and
vascular ingrowth and replacement with mature fibrous tissue
Treatment - Medical
Monitor the vital signs : TPR / BP / IO / Abdominal girth chart
Nil Per Oral
Nasogastric tube (Ryle’s tube) insertion anddependent drainage. Intermittent (fourthhourly) aspiration
IV fluid supplement : Ringer’s lactate orNormal saline
Antibiotics if strangulation suspected
Reassess periodically
Treatment – Surgical
Indications :
When conservative treatment for 3 to 5days does not result in resolution
When strangulation is suspected / cannotbe ruled out
Treatment – Surgical Emergency exploratory laparotomy
Adhesiolysis / EnterolysisResect the strangulated bowel and do
end to end anastomosis
• Handle the bowel carefully (less abrasion)• Do not produce ischaemia of peritoneum• Do not mobilize and suture peritoneum• Do thorough peritoneal lavage with saline• Instillation of inhibitors - controversial
Treatment for recurrent intestinal obstruction due to adhesions
Repeat Adhesiolysis / Enterolysis Noble’s plication Charles – Phillips transmesentric plication Intestinal intubation
BANDS
Aetiology
Congenital :
Ladds bandsObliterated vitellointestinal duct
Mesodiverticular band
Inflammatory :A string band following bacterial peritonitis
Greater omentum adherent to the parietes
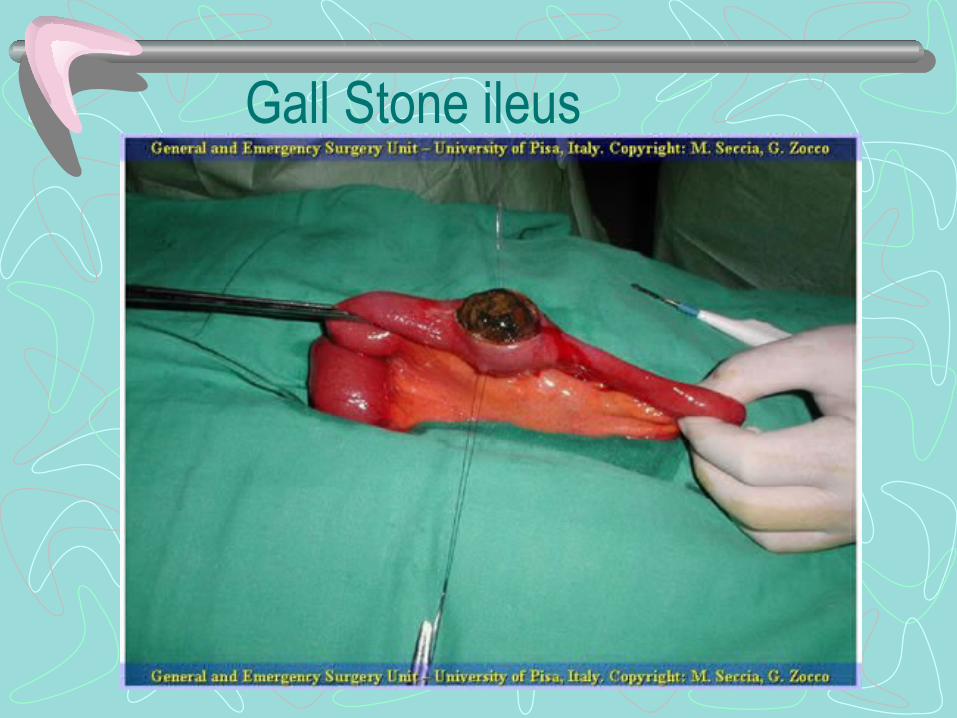
Gall Stone ileus

Definition
• Gall stone obstructing the lumen of bowel, usually the small intestine
Pathogenesis
• Gall stone erodes the wall of the gall balder and enters the duodenum
• Impaction 60 cm proximal to ileo-cecal junction
Clinical Features• Elderly female • Severe colicky pain • Recurrent attacks –ball valve
obstruction • Vomiting • Distension • Usually no constipation
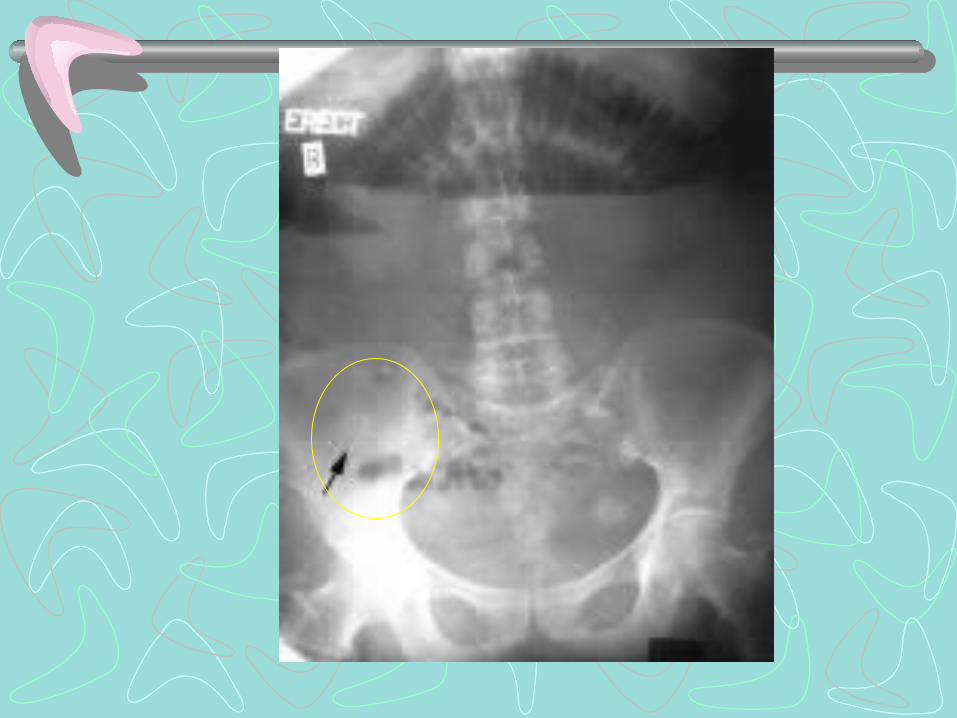
Investigations
• Routine • Plain x-ray abdomen
–Air fluid level with Air in the biliary tree- pneumobilia (diagnostic)
– Gall stone may or may not be seen

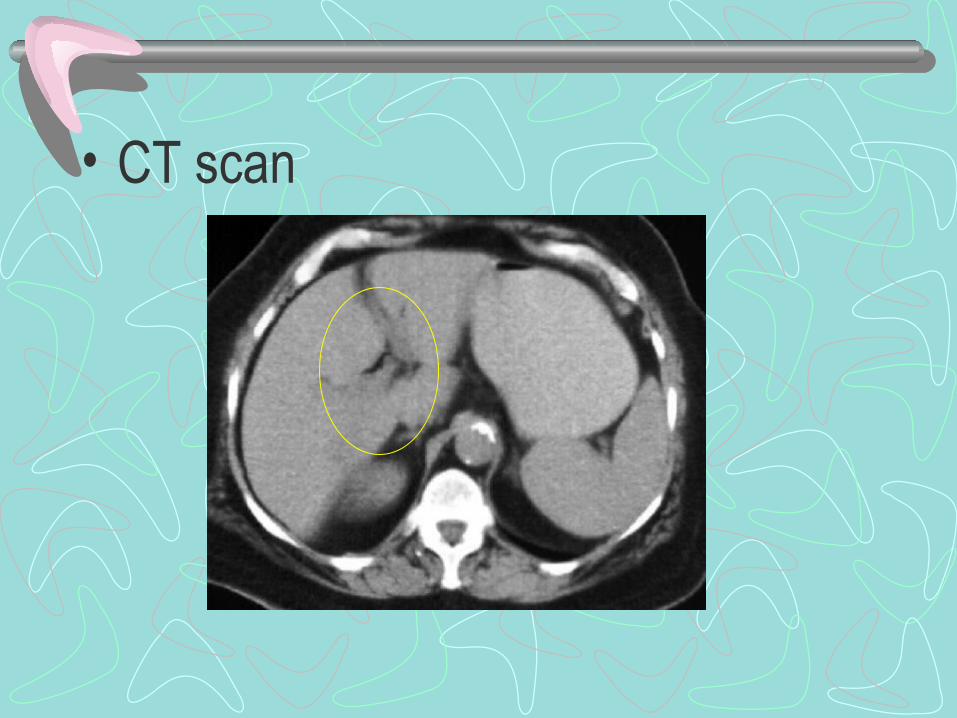
• CT scan
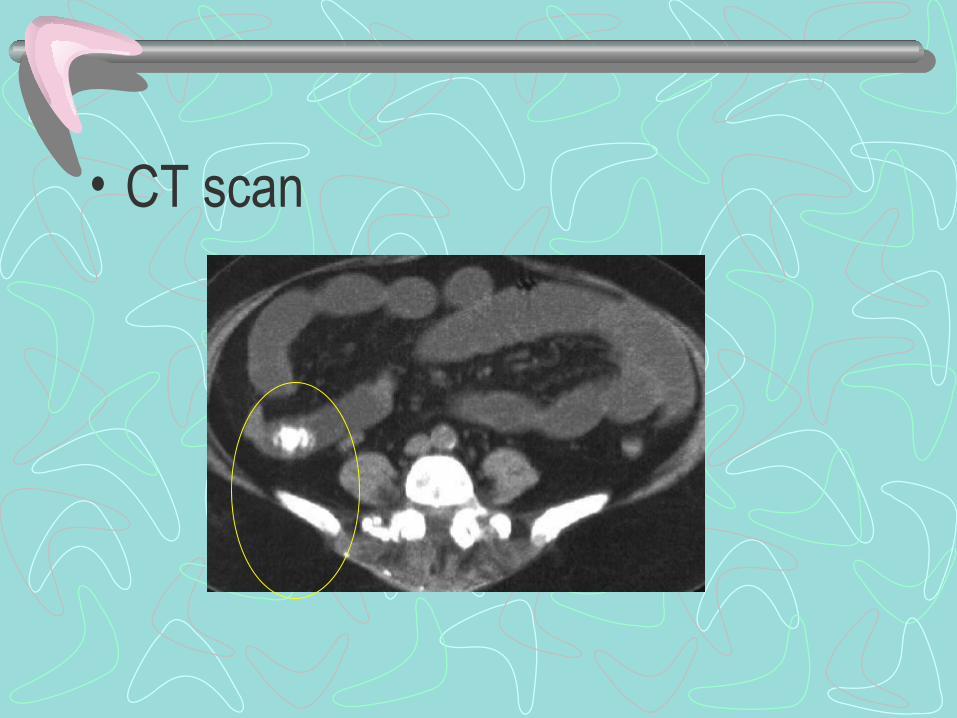
• CT scan
Treatment
• General measures
• Laparotomy – Explore by palpating bowel– Crush the stone without opening bowel– Enterotomy and removal
Do not explore gall bladder
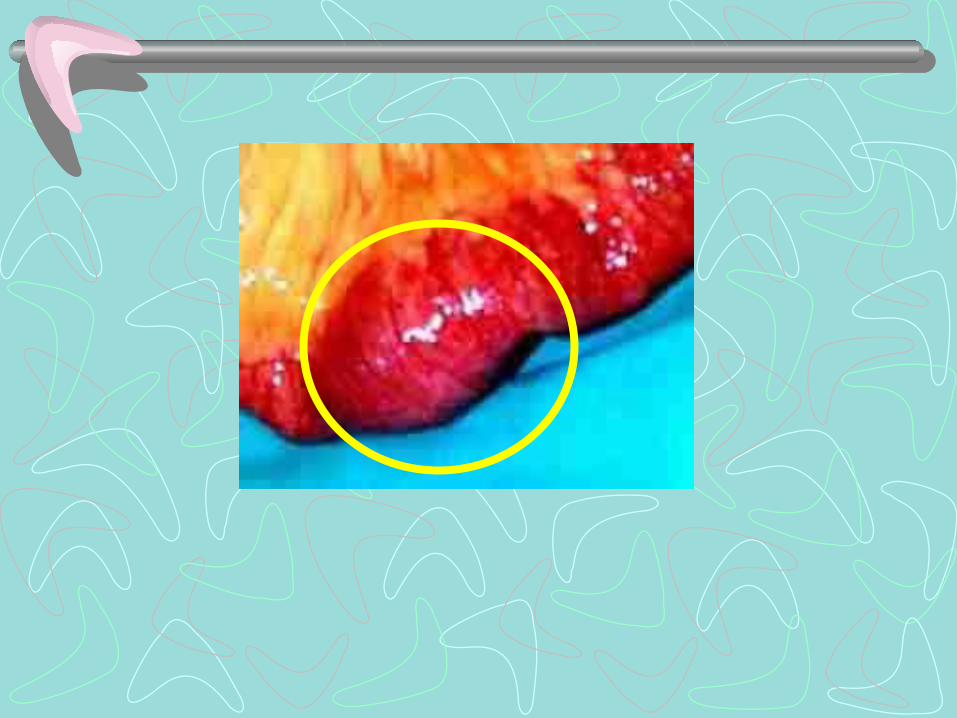
Intussusception
Definition:
Invagination of one portion of the gut within the other and it is usually proximal into the distal bowel;
Rarely retrograde.
- Telescoping


Etiology:Primary - Idiopathic • Seen in children; no lead point• Peak incidence 3 - 9 months• Hyperplasia of Payer’s patches in the terminal ileum - Secondary to weaning - URTI due to adenovirus or rotavirusAdults – Secondary • Meckel’s diverticulum, HS Purpura• Polyp (Peutz – Jegher syndrome)• Submucous lipoma , submucous haemorrhage• Malignancy of the colon - Lead point always
Types:
• Simple - Ileocolic, ileoileal, colocolic• Retrograde - Jejunogastric• Compound - Ileoileocolic• Multiple
• Chronic intussusception• Recurrent intussusception
Parts of the intussusception:
• Intussusceptum:Proximal bowel which enters inside – inner tube
• Intussuscipiens:Distal bowel which receives the intestine – outer tube
• Apex: Starting point or the part which advances• Neck:Narrowest portion
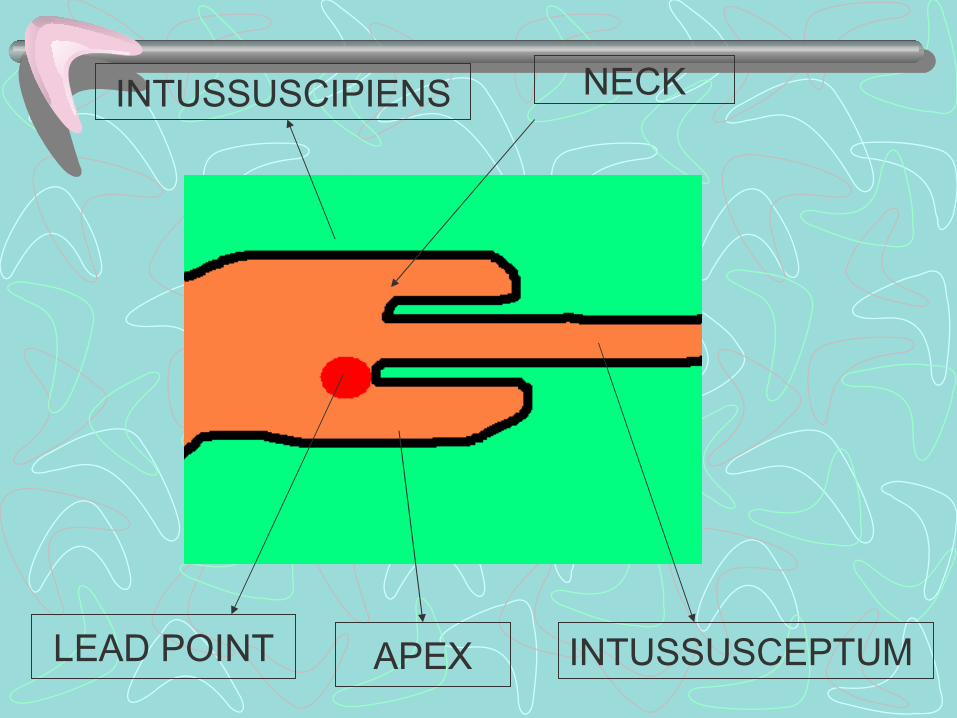
INTUSSUSCEPTUM
INTUSSUSCIPIENS NECK
APEXLEAD POINT

Pathology:• As the intussusception progresses the mesentery is
dragged through the neck• Mucosal ulcers and hemorrhages• Venous engorgement with oedema of the wall • Blood and mucous from the wall and will be discharged per
rectally – red currant jelly• Arteries get occluded and gangrene sets in • Perforation and peritonitis
• Strangulating obstruction (compound obstruction )
• Gangrene sets in at the neck • Inner layer blood supply get impaired
Clinical features
• Male child between 3 -9 months of age commonly affected• Colicky pain abdomen - onset is sudden and the child
screams with drawing up of the legs• Attack lasts for few minutes, recur every 15 minutes and
becomes progressively severe.• Vomiting may or may not be there• Facial pallor• Red current jelly stools• Dehydration, tachycardia
On examination
Abdomen• Visible peristalsis• Lump may be felt under the right or left coastal margin• Sausage shaped lump with the concavity towards the umbilicus;
mass may disappear• Sign - de – Dance, Right iliac fossa is empty Per rectal• Blood stained mucous• Apex of the intussusception may be felt• Intussusception may protrude from the anus
Investigations
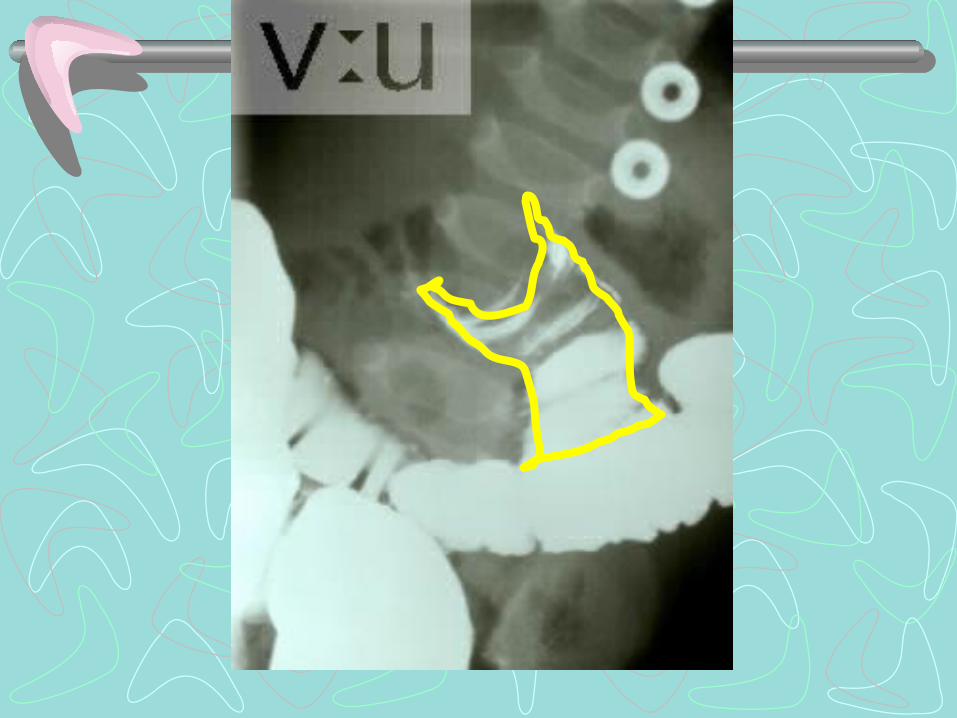
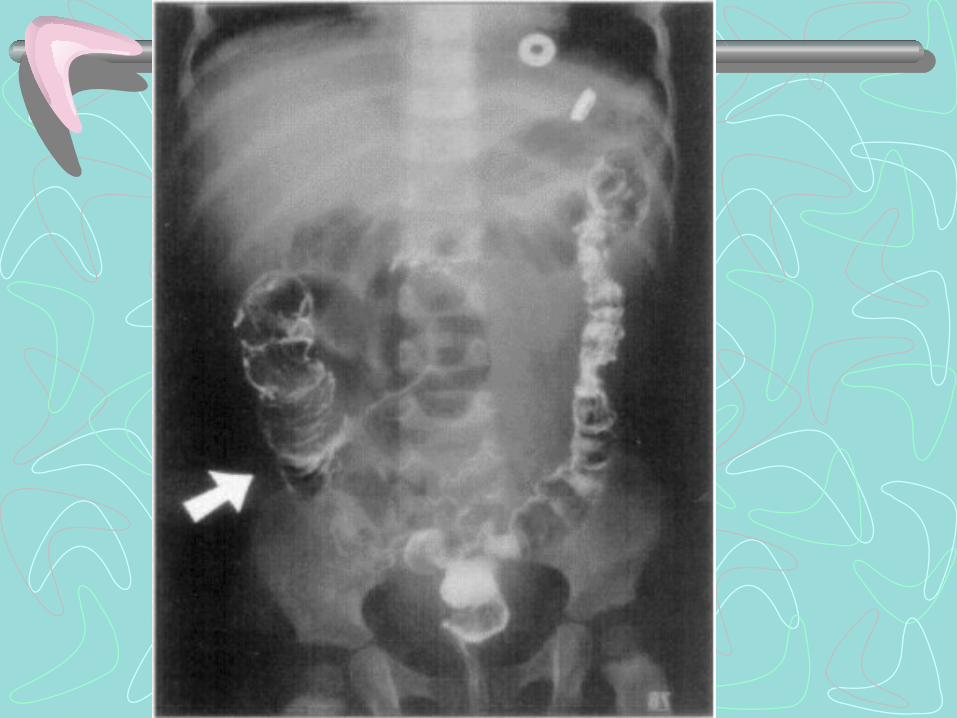
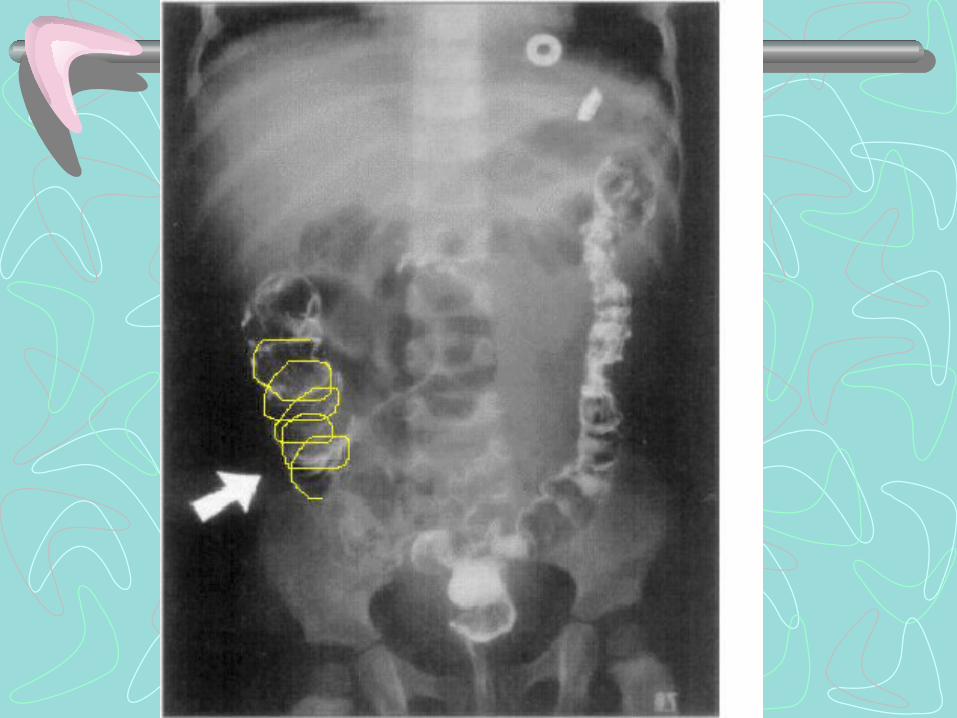
• Haemogram• Plain X ray abdomen• Barium enema -
Diagnostic and therapeutic
Pincer shaped filling defect
( Claw sign / meniscus sign / coiled
spring appearance)


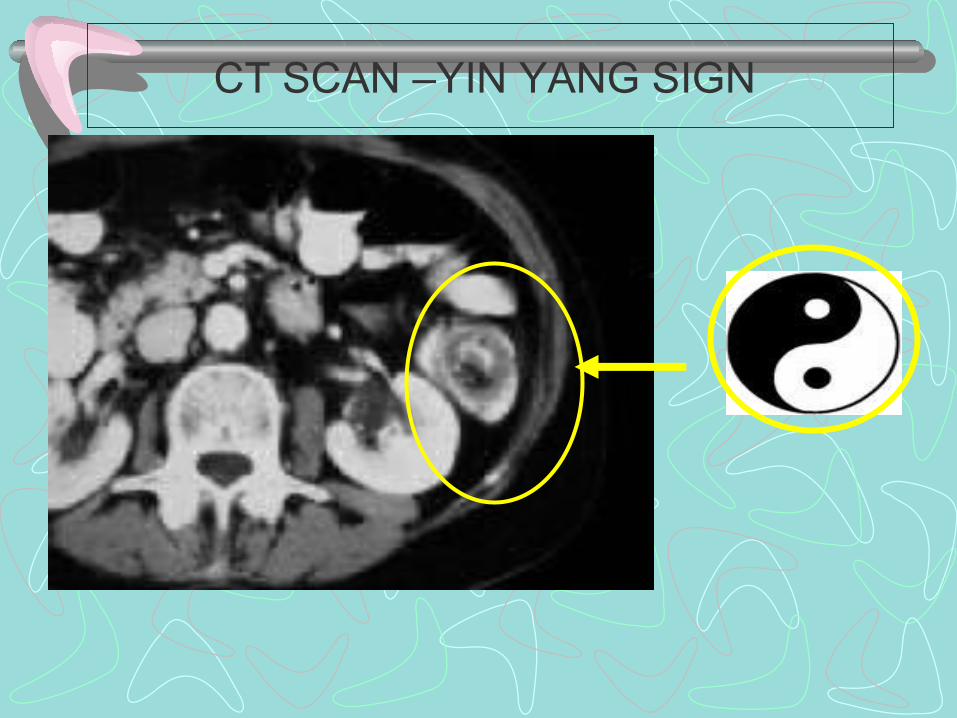
CT SCAN –YIN YANG SIGN
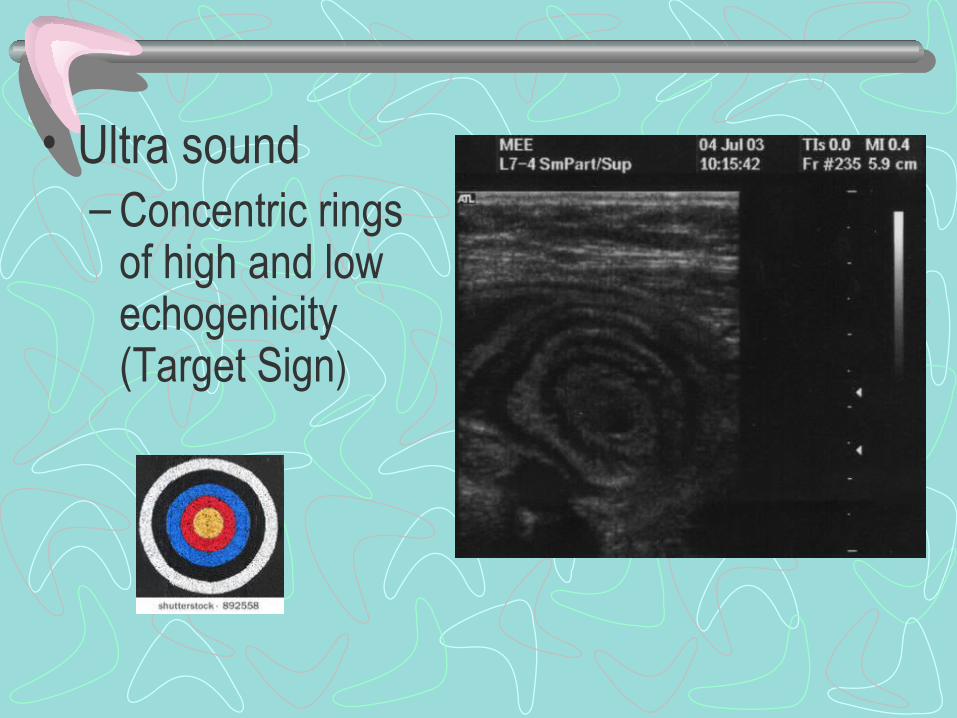
• Ultra sound– Concentric rings
of high and low echogenicity (Target Sign)
Treatment:• Nil per orally• IV fluids• Ryle’s tube aspiration• Electrolytes, Antibiotics
Hydrostatic reductionContraindicated in Presence of obstruction Peritonitis Gangrene Symptoms more than 48 hrs
• Hydrostatic reduction -–Selected cases –Barium enema – Infants –50% success

• Hydrostatic reduction -–Enema can at height –Push barium rapidly –Confirm with x-ray
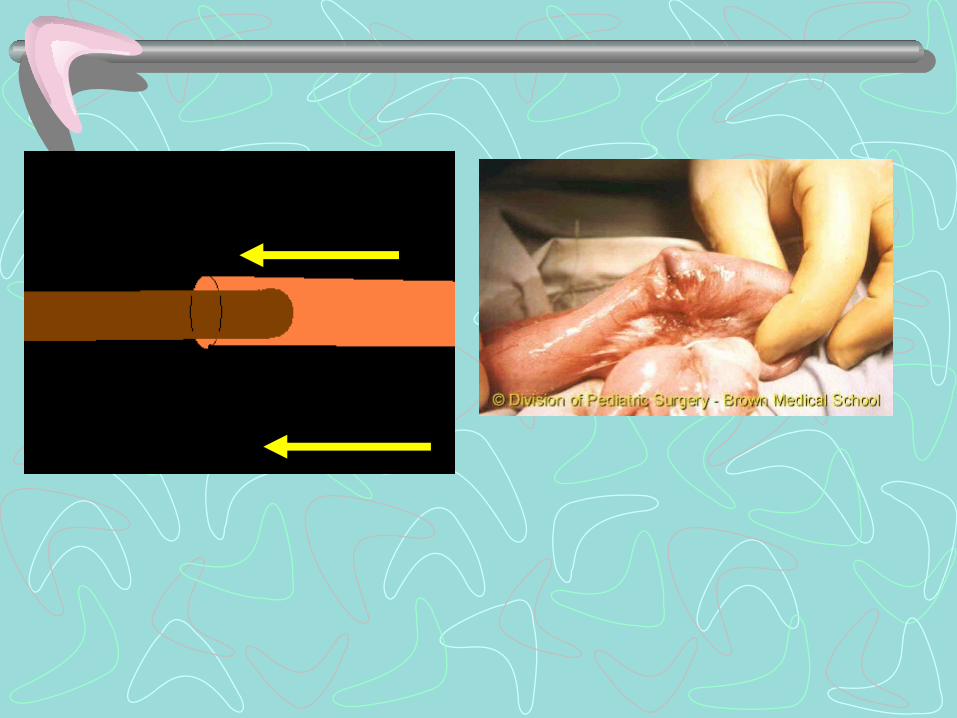
Surgical treatment• Laparotomy and reduction of intussusception• Reduction is done by squeezing the distal part proximally ( Do
not pull)• Last part of the intussusception is the most difficult part to
reduce• Free the adhesions between neck & distal bowel• Appedicectomy is done• If the intestine is gangrenous then resection and end to end
anastomosis is done

THANK YOU