Adaptive Treatment Strategies in the Addictions: Current Examples and Future Directions James R....
44
Adaptive Treatment Strategies in the Addictions: Current Examples and Future Directions James R. McKay, Ph.D. Professor of Psychology in Psychiatry University of Pennsylvania CTN Meeting 3.22.07
-
Upload
marsha-ryan -
Category
Documents
-
view
215 -
download
1
Transcript of Adaptive Treatment Strategies in the Addictions: Current Examples and Future Directions James R....

Adaptive Treatment Strategies in the Addictions:
Current Examples and Future Directions
James R. McKay, Ph.D.
Professor of Psychology in Psychiatry
University of Pennsylvania
CTN Meeting
3.22.07

Overview of Presentation
• Major problems in providing addiction treatment and how we’ve tried to address them
• Adaptive treatment models and how they are developed
• Examples of adaptive treatment in specialty care• Examples of adaptive treatment in other treatment
settings• Challenges in designing and implementing
adaptive treatment protocols

Problems in Addiction Treatment
• High rates of dropout and continued alcohol and drug use– In community-based programs– In research protocols
• Even with evidence-based treatments, considerable response heterogeneity

Attempts to Address Nonresponse?
• Improve existing treatments
• Develop new treatments
• Tailoring, or “matching” treatments to subgroups of patients
Results???

Still left with variable response…..
• Even when treatment delivery is standardized and high adherence to manual is achieved, some patients do well and others do not.
• Very hard to predict who will do well in a particular treatment
• Some patients do well at first, but then deteriorate• Nonresponse often blamed on the patient, but that
is likely not the whole story.

Another Possible Approach?
Adaptive Treatment

In Adaptive Treatment Protocols…
• Treatment is tailored or modified on the basis of measures of response (e.g., symptoms, status, or functioning) obtained at regular intervals during treatment
• Goal is to deliver the treatment that is most effective for a particular patient at a particular time.
• Rules for changing treatment are clearly operationalized and described…..
“If……..Then”• Temporal issues important– when has sufficient time
elapsed to indicate “non-response”?

How Do You Put Together an Adaptive Protocol?

Experimental Design for Developing Adaptive Protocols
• Use randomization to develop optimal adaptive treatment strategies– Example: What to do with early non-responders?
• Switch treatment?• Augment treatment?
• Determine the set of decision rules and interventions that produce the highest percentage of responders
THEN…….
• Compare the optimal adaptive protocol to TAU or other treatments in standard RCT

The alternative approach….
• Devise adaptive protocol on the basis of:– Expert clinical judgment– Feedback from patients– Prior research findings– Face validity
• Compare that adaptive protocol to TAU or other treatment in standard RCT
• Pros and Cons: Faster than experimental approach, but protocol may be flawed

Examples of Adaptive Protocols from Addiction Specialty Care

Recovery Management Checkups
• Protocol developed by Dennis, Scott et al.– Interview patients every quarter for 2 years– If patient reports any of the following……
• Use of alcohol or drugs on > 2 weeks
• Being drunk or high all day on any days
• Alcohol/drug use led to not meeting responsibilities
• Alcohol/drug use caused other problems
• Withdrawal symptoms
….. ….Patient transferred to linkage manager

RMC
• Linkage Manager provides the following:– Personalized feedback– Explore possibility of returning to treatment– Address barriers to returning to treatment– Schedule an intake assessment– Reminder cards, transportation, and escort to
intake appointment

Results: RMC vs. TAU
• Time to return to treatment 376 vs. 600 days (p< .05)
• Total days of treatment 62 vs. 40 days (p< .05)
• In need of treatment at 24 months 43% vs. 56% (p< .01)
• In need of treatment in at least 5 quarters 23% vs. 32% (p< .05)
Dennis et al. (2003) Evaluation and Program Planning, 26, 339-352

Adaptive Methadone Treatment
• Brooner & Kidorf (2002) protocol– Methadone patients start in low intensity
psychosocial condition– Missed session or dirty/missing urine leads to
increases in psychosocial counseling– Providing additional contingencies for
participation further improves outcomes• More/less convenient dosing times• Methdone taper and possible discharge

Penn Telephone Continuing Care Study
• Patients: – 359 graduates of 4-week IOP programs– Cocaine (75%) and/or alcohol (75%) dependent
• Continuing care treatment conditions (12 weeks):– Standard group counseling (STND) – Individualized relapse prevention (RP) – brief telephone-based counseling (TEL)
McKay et al., 2004, Journal of Consulting and Clinical Psychology

Continuing Care Conditions
• Telephone Monitoring and Counseling
– Weeks 1-4, patients make a 15 minute call and attend a “transition” group (1x/week @)
– Weeks 5-12, patients have telephone contact only (1x/week)
– During calls, patients report results of self-monitoring and progress toward 1-2 goals, and plan goals for next week
– Patients use a workbook that structures intervention for each week.
– Total minutes of contact with therapist 50% of minutes in other conditions

Total Abstinence Rates
0
10
20
30
40
50
60
70
80
3 6 9 12 15 18 21 24
Month
% A
bstin
ent STND
RP
TEL
Tx Main EffectTEL > STND p< .05
McKay et al., 2005, Archives of General Psychiatry

Adaptive Treatment Strategy:
Using Progress in Initial Phase of Treatment to Select Optimal
Continuing Care Models

7-Item Composite Risk Indicator
• Failure to achieve key goals while in IOP:– Any alcohol use in prior 30 days– Any cocaine use in prior 30 days– Attendance at < 12 self-help meetings in prior 30 days– Social support < median for the sample– Does not have goal of absolute abstinence– Self-efficacy < 80%
• Current dependence on both alcohol and cocaine
(each item: yes=1, no=0)
McKay et al., 2005, Addiction, Archives of General Psychiatry

0
20
40
60
80
100
120
Nu
mb
er o
f P
arti
cip
ants
0 1 2 3 4 5 6 7Composite Risk Indicator Score
Distribution of Scores on the Composite Risk Indicator
Mean score= 2.50

TEL vs. STND contrast X Risk Index Score: p < .05

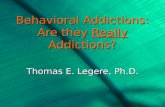
Figure #1 Predicted Aggregated and Compressed Log "Bad" Costs Model: FGRBadcostlog = Txcond Sequence FGRBLBadcostlog Program
Txcond*FGRBLBadcostlog
0
2
4
6
8
10
0 2 4 6 8 10
Baseline "Bad" Costs (log)
3-m
onth
Fol
low
-up
"Bad
" C
osts
(log
)
STD RP (Not Significant) TR
Most favorable baseline level
Most favorable interventions
Crossover point STD vs. TR: "Bad" costs $830
(6.72 on log scale)
Least favorable baseline level
≥ $830; 27% (N = 98)
< $830; 73% (N = 261)

Extended Telephone-Based Adaptive Protocol for the Management of Cocaine
Dependence

Design
• Patients: Cocaine dependent IOP participants recruited after achieving early engagement
• Treatment conditions:– Treatment as usual (TAU)
– TAU plus adaptive protocol (24 mo.)
– TAU plus adaptive protocol (24 mo.), plus incentives for participation and cocaine-free urines (12 mo)
• Outcomes assessed over 24 months

The Telephone Calls
• Frequency: weekly at first, titrated to bimonthly• Each call starts with a brief “risk assessment” that assesses
negative and positive factors and yields overall risk score (low, moderate, high)
• Similar protocol to prior study for telephone counseling: 1. Provide feedback on risk level 2. Review progress/goals from last call3. Identify upcoming high-risk situations 4. Select target for remainder of call5. Brief problem-solving regarding target concern(s)6. Set goal(s) for interval before next call7. Suggest change in level of care if warranted

Adaptive Protocol
• Increases in services triggered when risk reaches moderate level– First: increase frequency of phone calls– Second: bring patient in for 1-2 face-to-face
evaluation and motivational interviewing (MI) sessions
– Third: provide 8 CBT relapse prevention sessions
– Fourth: refer back to IOP

Examples of Adaptive Protocols from Non-Specialty Addiction
Care

Adaptive Primary Care Protocols for Heavy Drinkers
• Kristenson et al. (1983, 2003)– Patients randomized to visits with a nurse (every
month) and physician (every 3 months), vs. TAU
– Both provided for up to 4 years
– GGT levels monitored, and treatment/drinking goals modified on basis of scores
– Results: fewer sick days, fewer hospital days, lower mortality over 6 and 16 years than TAU

Adaptive Continuing Care Naltrexone Protocol
• O’Malley et al. (2003) study of NTX treatment comparing primary care (PC) and specialty care (CBT) approaches
• First, pts given NTX and randomized to PC or CBT for 10 weeks
• Responders (57%) further randomized:– PC plus extended NTX vs. placebo (24 wks)
– CBT plus extended NTX vs. placebo (24 wks)

Alcohol Use Results and Interpretations
• Findings:– Initiation phase: PC=CBT– Extended PC phase: NTX > placebo– Extended CBT phase: NTX= placebo
• Resulting treatment algorithm– If patient responds to PC and NTX in first 10 weeks,
continue both for at least 24 more weeks– If patient responds to CBT and NTX in first 10 weeks,
continue CBT but stop NTX
• Note: no guidance regarding nonresponders

Adaptive Naltrexone Study(David Oslin, PI)
• Experimental design to determine optimal algorithms for naltrexone responders and nonresponders
• All patients begin with 8 week trial of open label naltrexone, plus weekly medication management session
• During the 8 week trial, patients self-select into Responder and Non-responder groups
• First randomization: Different definitions of “non-response”– More than 1 heavy drinking day– More than 4 heavy drinking days

Adaptive Naltrexone, cont.
Second Randomization
• Nonresponders:– Add CBI and drop NAL (i.e., “switch”)– Add CBI and continue NAL (i.e., augment”)
• Responders: – NAL script plus no further care– NAL script plus telephone disease management

Adaptive Intervention Strategies Embedded in Oslin Trial
Adaptive intervention
Definition of nonresponder
Decision rules for responders
Decision rules for nonresponders
1 > 1 heavy drinking day Stay with NTX alone NTX with CBI
2 > 1 heavy drinking day Stay with NTX alone Change to CBI alone
3 > 1 heavy drinking day NTX with TDM NTX with CBI
4 > 1 heavy drinking day NTX with TDM Change to CBI alone
5 > 4 heavy drinking day Stay with NTX alone NTX with CBI
6 > 4 heavy drinking day Stay with NTX alone Change to CBI alone
7 > 4 heavy drinking day NTX with TDM NTX with CBI
8 > 4 heavy drinking day NTX with TDM Change to CBI alone

Comparing Definitions of Response
Adaptive intervention
Definition of nonresponder
Decision rules for responders
Decision rules for nonresponders
1 > 1 heavy drinking day Stay with NTX alone NTX with CBI
2 > 1 heavy drinking day Stay with NTX alone Change to CBI alone
3 > 1 heavy drinking day NTX with TDM NTX with CBI
4 > 1 heavy drinking day NTX with TDM Change to CBI alone
5 > 4 heavy drinking day Stay with NTX alone NTX with CBI
6 > 4 heavy drinking day Stay with NTX alone Change to CBI alone
7 > 4 heavy drinking day NTX with TDM NTX with CBI
8 > 4 heavy drinking day NTX with TDM Change to CBI alone

Comparing Augment vs. Switch for NonResponders
Adaptive intervention
Definition of nonresponder
Decision rules for responders
Decision rules for nonresponders
1 > 1 heavy drinking day Stay with NTX alone NTX with CBI
2 > 1 heavy drinking day Stay with NTX alone Change to CBI alone
3 > 1 heavy drinking day NTX with TDM NTX with CBI
4 > 1 heavy drinking day NTX with TDM Change to CBI alone
5 > 4 heavy drinking day Stay with NTX alone NTX with CBI
6 > 4 heavy drinking day Stay with NTX alone Change to CBI alone
7 > 4 heavy drinking day NTX with TDM NTX with CBI
8 > 4 heavy drinking day NTX with TDM Change to CBI alone

Summary of Possible Adaptations
• Non-responders– Step up (e.g., OP to IOP or residential)
– Lateral move (e.g., CBT to TSF)
– Modality change (e.g., CBT to medication)
– Step down (e.g., IOP to telephone monitoring)
• Responders– Reduce frequency of intervention (e.g., IOP to OP)
– Change to lower burden intervention (e.g., OP to periodic check-ups, or e-treatment)

Adaptive Treatment and the CTN:
Difficult Problems………….. But Big Opportunitiesand Potential Benefits

Challenges in Adaptive TreatmentClinical• Keeping patients engaged, especially when
deterioration occurs• Increasing compliance with adaptive changes,
especially “step ups” • Identifying alternative treatments for non-
responders– Lack of a variety of effective medications– Are different types of “talk” therapy really different
enough? – How important is patient preference/choice?

Challenges, cont.Research• Incorporating choice in algorithms
– Comparing heterogeneous condition to other interventions
• Sequential randomization designs– Randomizing patients 2+ times– Analytic issues (first decision)
• Power– Primary vs. secondary comparisons– New methods under development

Focus of Efforts in Treatment Development
• Emphasis in field has been on improving efficacy and adherence to manuals, and coming up with more cost-effective approaches.
• Shift emphasis to making participation more attractive to the patients to improve retention:– Greater weight to patient choice– at intake, and for
non-responders– Use of more convenient forms of care whenever
possible– Incentives for participation?

Possible Research Designs
• Adaptive strategies to address early dropout– Test providing a menu of treatment options vs. efforts
to re-engage in standard care
“So you don’t like IOP. How about…….?”
• Adaptive medication algorithms– Start with promising med– augment with or switch to
additional medication for nonresponders

Research Designs, cont.
• Adaptive studies that combine behavioral and pharmacological interventions:– Start with medication and low intensity behavioral
treatment, step up to more intensive treatment if no response
– Offer non-responders sequential package that first involves switching meds, but then includes augmentation with stepped up behavioral treatment if response still not achieved.

Acknowledgments
• Colleagues:– NIDA CTN algorithms group– Dave Oslin, Kevin Lynch, Tom TenHave– Susan Murphy, Linda Collins
• Grant support:– NIDA: K02-DA00361, R01-DA14059, R01-
DA20623 – NIAAA: R01AA14850