
Adaptive Radiotherapy: Merging Principle Into Clinical Practice
5
Adaptive Radiotherapy: Merging Principle Into Clinical Practice R adiotherapy plays an important role in cancer manage- ment. Continued improvement of the therapy, however, is seriously impeded by the inherent variability in the indi- vidual’s treatment. Treatment variation during the course of radiotherapy can be classified as the dosimetric variation in organs of interest induced by daily patient setup error, radi- ation beam placement error, and physiological and morpho- logical changes of patient anatomical position, shape, and volume, as well as the biological variation caused by cell phenotypic changes. These variations are all patient-specific, spatial, and temporal events, and most of them depend on the radiation dose. Therefore, they cannot be properly managed using conventional treatment techniques with pretreatment imaging and planning alone. Adaptive radiotherapy has been introduced as a feedback control strategy to include patient-specific treatment varia- tion explicitly in the control of treatment planning and deliv- ering during the treatment course. 1 It is possible to cope with, or even take advantage of treatment variation in the individ- ualized treatment optimization. The potential of adaptive ra- diotherapy extends far beyond the increase of radiation dose delivery accuracy. It could also improve radiotherapy efficacy after patient-specific biological changes are incorporated in the adaptive optimal control process. To date, most clinical applications of adaptive radiotherapy have been limited to target position correction alone, and the extensive feedback information obtained during the treatment course has not been fully used in treatment optimization. Principle of Adaptive Radiotherapy The principle of adaptive radiotherapy originates from infor- matics and modern control theory, and focuses on including feedback knowledge of patient-specific anatomical or biolog- ical variations observed frequently during the radiotherapy course in the individual treatment plan and dose delivery optimization. The major impediment to applying feedback control theory in radiotherapy is the unpredictable event of instant variation. In addition to managing the instantaneous appearance of treatment variation, adaptive radiotherapy fo- cuses more on assessing treatment dose, characterizing pa- tient-specific variation process, and then including the pre- dicted treatment dose distribution in organs of interest and the variation characteristics in treatment control through adaptive planning optimization to determine the best plan or control for treatment delivery. 2 The most effective and reli- able control mechanism in radiotherapy should be the mod- ification of radiation dose distribution through the adjust- ments of radiation beam aperture, direction, and intensity, instead of directly adjusting patient/organ position. Clinical implementation of adaptive radiotherapy could vary with respect to different considerations and clinical goals. However, a complete implementation should include 4 key components, which are (1) treatment dose assessment, (2) treatment variation identification/evaluation, (3) treat- ment modification decisions, and (4) adaptive treatment modification. The typical adaptive control system, Model Identification Adaptive Control (MIAC) System or Self-tun- ing Regulator (STR), 3 can be adopted to integrate these 4 sub-processes into a feedback loop for adaptive radiotherapy. Clinical activity of adaptive radiotherapy in this system is a proactive approach, achieving the best possible treatment of the individual, instead of maintaining the existed treatment plan. Figure 1 shows a flow chart of the MIAC-based adaptive treatment system. In this system, the patient-specific treat- ment variation is constantly observed and modeled using a random process. The corresponding characteristics of the random process are regularly estimated and updated using the new observations, and then used to evaluate the total treatment dose as well as the potential treatment effects, such as dose-volume of organs of interest, tumor control, and nor- mal organ toxicity. These evaluations are then keyed in the predesigned decision rules or control laws for treatment modification decisions. Depending on the cause of the vari- ation and the clinical goals, the adaptive treatment modifica- tion can be as simple as a treatment position correction ac- complished by adjusting patient position or beam aperture, or as complex as a 4D adaptive inverse replanning accom- Volume 20, Number 2 April 2010 79 1053-4296/10/$-see front matter © 2010 Elsevier Inc. All rights reserved. doi:10.1016/j.semradonc.2009.11.001
Transcript of Adaptive Radiotherapy: Merging Principle Into Clinical Practice
Rivroalvpsrui
cteouddatatib
PATmficoci
Volume 20, Number 2 April 2010
1d
Adaptive Radiotherapy:
Merging Principle Into Clinical Practiceactdtacaimi
vgk(mmIisCptp
tmrrttampmatc
adiotherapy plays an important role in cancer manage-ment. Continued improvement of the therapy, however,
s seriously impeded by the inherent variability in the indi-idual’s treatment. Treatment variation during the course ofadiotherapy can be classified as the dosimetric variation inrgans of interest induced by daily patient setup error, radi-tion beam placement error, and physiological and morpho-ogical changes of patient anatomical position, shape, andolume, as well as the biological variation caused by cellhenotypic changes. These variations are all patient-specific,patial, and temporal events, and most of them depend on theadiation dose. Therefore, they cannot be properly managedsing conventional treatment techniques with pretreatment
maging and planning alone.Adaptive radiotherapy has been introduced as a feedback
ontrol strategy to include patient-specific treatment varia-ion explicitly in the control of treatment planning and deliv-ring during the treatment course.1 It is possible to cope with,r even take advantage of treatment variation in the individ-alized treatment optimization. The potential of adaptive ra-iotherapy extends far beyond the increase of radiation doseelivery accuracy. It could also improve radiotherapy efficacyfter patient-specific biological changes are incorporated inhe adaptive optimal control process. To date, most clinicalpplications of adaptive radiotherapy have been limited toarget position correction alone, and the extensive feedbacknformation obtained during the treatment course has noteen fully used in treatment optimization.
rinciple ofdaptive Radiotherapy
he principle of adaptive radiotherapy originates from infor-atics and modern control theory, and focuses on including
eedback knowledge of patient-specific anatomical or biolog-cal variations observed frequently during the radiotherapyourse in the individual treatment plan and dose deliveryptimization. The major impediment to applying feedbackontrol theory in radiotherapy is the unpredictable event of
nstant variation. In addition to managing the instantaneous o053-4296/10/$-see front matter © 2010 Elsevier Inc. All rights reserved.oi:10.1016/j.semradonc.2009.11.001
ppearance of treatment variation, adaptive radiotherapy fo-uses more on assessing treatment dose, characterizing pa-ient-specific variation process, and then including the pre-icted treatment dose distribution in organs of interest andhe variation characteristics in treatment control throughdaptive planning optimization to determine the best plan orontrol for treatment delivery.2 The most effective and reli-ble control mechanism in radiotherapy should be the mod-fication of radiation dose distribution through the adjust-
ents of radiation beam aperture, direction, and intensity,nstead of directly adjusting patient/organ position.
Clinical implementation of adaptive radiotherapy couldary with respect to different considerations and clinicaloals. However, a complete implementation should include 4ey components, which are (1) treatment dose assessment,2) treatment variation identification/evaluation, (3) treat-ent modification decisions, and (4) adaptive treatmentodification. The typical adaptive control system, Model
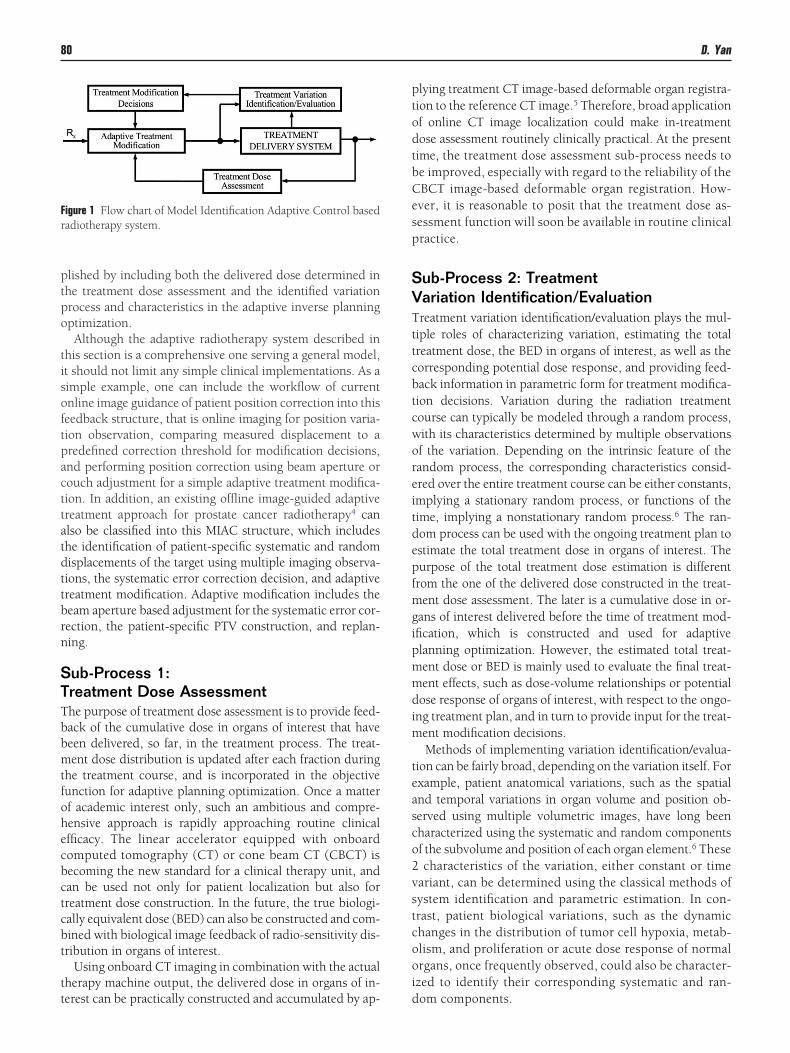
dentification Adaptive Control (MIAC) System or Self-tun-ng Regulator (STR),3 can be adopted to integrate these 4ub-processes into a feedback loop for adaptive radiotherapy.linical activity of adaptive radiotherapy in this system is aroactive approach, achieving the best possible treatment ofhe individual, instead of maintaining the existed treatmentlan.Figure 1 shows a flow chart of the MIAC-based adaptive
reatment system. In this system, the patient-specific treat-ent variation is constantly observed and modeled using a
andom process. The corresponding characteristics of theandom process are regularly estimated and updated usinghe new observations, and then used to evaluate the totalreatment dose as well as the potential treatment effects, suchs dose-volume of organs of interest, tumor control, and nor-al organ toxicity. These evaluations are then keyed in theredesigned decision rules or control laws for treatmentodification decisions. Depending on the cause of the vari-
tion and the clinical goals, the adaptive treatment modifica-ion can be as simple as a treatment position correction ac-omplished by adjusting patient position or beam aperture,
r as complex as a 4D adaptive inverse replanning accom-79
ptpo
tisoftpacttatdttbrn
STTbbmtfohecbctcbt
tt
ptodtbCesp
SVTttcbtcworeitdepfmgipmmdim
teasco2vstcooi
Fr
80 D. Yan
lished by including both the delivered dose determined inhe treatment dose assessment and the identified variationrocess and characteristics in the adaptive inverse planningptimization.Although the adaptive radiotherapy system described in
his section is a comprehensive one serving a general model,t should not limit any simple clinical implementations. As aimple example, one can include the workflow of currentnline image guidance of patient position correction into thiseedback structure, that is online imaging for position varia-ion observation, comparing measured displacement to aredefined correction threshold for modification decisions,nd performing position correction using beam aperture orouch adjustment for a simple adaptive treatment modifica-ion. In addition, an existing offline image-guided adaptivereatment approach for prostate cancer radiotherapy4 canlso be classified into this MIAC structure, which includeshe identification of patient-specific systematic and randomisplacements of the target using multiple imaging observa-ions, the systematic error correction decision, and adaptivereatment modification. Adaptive modification includes theeam aperture based adjustment for the systematic error cor-ection, the patient-specific PTV construction, and replan-ing.
ub-Process 1:reatment Dose Assessmenthe purpose of treatment dose assessment is to provide feed-ack of the cumulative dose in organs of interest that haveeen delivered, so far, in the treatment process. The treat-ent dose distribution is updated after each fraction during
he treatment course, and is incorporated in the objectiveunction for adaptive planning optimization. Once a matterf academic interest only, such an ambitious and compre-ensive approach is rapidly approaching routine clinicalfficacy. The linear accelerator equipped with onboardomputed tomography (CT) or cone beam CT (CBCT) isecoming the new standard for a clinical therapy unit, andan be used not only for patient localization but also forreatment dose construction. In the future, the true biologi-ally equivalent dose (BED) can also be constructed and com-ined with biological image feedback of radio-sensitivity dis-ribution in organs of interest.
Using onboard CT imaging in combination with the actualherapy machine output, the delivered dose in organs of in-
igure 1 Flow chart of Model Identification Adaptive Control basedadiotherapy system.
erest can be practically constructed and accumulated by ap- d
lying treatment CT image-based deformable organ registra-ion to the reference CT image.5 Therefore, broad applicationf online CT image localization could make in-treatmentose assessment routinely clinically practical. At the presentime, the treatment dose assessment sub-process needs toe improved, especially with regard to the reliability of theBCT image-based deformable organ registration. How-ver, it is reasonable to posit that the treatment dose as-essment function will soon be available in routine clinicalractice.
ub-Process 2: Treatmentariation Identification/Evaluationreatment variation identification/evaluation plays the mul-
iple roles of characterizing variation, estimating the totalreatment dose, the BED in organs of interest, as well as theorresponding potential dose response, and providing feed-ack information in parametric form for treatment modifica-ion decisions. Variation during the radiation treatmentourse can typically be modeled through a random process,ith its characteristics determined by multiple observationsf the variation. Depending on the intrinsic feature of theandom process, the corresponding characteristics consid-red over the entire treatment course can be either constants,mplying a stationary random process, or functions of theime, implying a nonstationary random process.6 The ran-om process can be used with the ongoing treatment plan tostimate the total treatment dose in organs of interest. Theurpose of the total treatment dose estimation is differentrom the one of the delivered dose constructed in the treat-ent dose assessment. The later is a cumulative dose in or-
ans of interest delivered before the time of treatment mod-fication, which is constructed and used for adaptivelanning optimization. However, the estimated total treat-ent dose or BED is mainly used to evaluate the final treat-ent effects, such as dose-volume relationships or potentialose response of organs of interest, with respect to the ongo-
ng treatment plan, and in turn to provide input for the treat-ent modification decisions.Methods of implementing variation identification/evalua-
ion can be fairly broad, depending on the variation itself. Forxample, patient anatomical variations, such as the spatialnd temporal variations in organ volume and position ob-erved using multiple volumetric images, have long beenharacterized using the systematic and random componentsf the subvolume and position of each organ element.6 Thesecharacteristics of the variation, either constant or time
ariant, can be determined using the classical methods ofystem identification and parametric estimation. In con-rast, patient biological variations, such as the dynamichanges in the distribution of tumor cell hypoxia, metab-lism, and proliferation or acute dose response of normalrgans, once frequently observed, could also be character-zed to identify their corresponding systematic and ran-
om components.
STTsttcttemnuvitcmpmtttFupstscc
SAAlbaoimimcct
iiia(fittt
ip
ptpsbtashmgtsabsmm
trtamfssttaosbpCsa
niititttrbsc
CT
Adaptive radiotherapy 81
ub-Process 3:reatment Modification Decisionsreatment modification decisions contain a set of prede-igned decision rules or control laws. Each of them is a func-ion mapping between an input value and output action ofreatment modification decisions. The typical output actionan be treatment position correction, beam aperture correc-ion, new PTV, or a plan modification. The decision rules areriggered by the outputs of treatment variation identification/valuation, and used to determine whether the ongoing treat-ent needs to be modified and what type of modificationeeds to take place. A modification decision can be activatedsing a detected variation, a variation characteristic, a dose-olume parameter, or potential dose response in an organ ofnterest determined using the ongoing treatment plan in thereatment variation identification/evaluation. Proactively, itan also be activated using the potential improvement of aodified plan. In a complete MIAC process, potential im-rovement of a modified plan can be evaluated on the basis ofodeled random process in treatment variation identifica-
ion/evaluation as shown as an inner loop of the adaptivereatment modification, the treatment variation identifica-ion/evaluation, and the treatment modification decision inig. 1. In practice, a cutoff value or threshold is commonlysed to switch on a treatment modification, which can beredetermined by performing sensitivity or perturbationtudies with respect to the specific treatment plan. In addi-ion, a set of PTVs or treatment plans predesigned with re-pect to different values of a specific variation characteristican also be used as a predesigned control law in the modifi-ation decisions.
ub-Process 4:daptive Treatment Modificationdaptive treatment modification can be performed either on-
ine or offline, and the modification method can be fairlyroad, including patient position correction, beam aperturedjustment, margin modification for target or critical normalrgans, or dose distribution reoptimization through beamntensity modulation. Among them, the most sophisticated
ethodology for adaptive treatment modification is adaptivenverse planning optimization,7 which has been, thus far,
ostly applied to manage organ geometrical variation. But, itan be applied to manage other treatment variations, such ashanges in hypoxic, metabolic, and proliferating distribu-ions in tumor as well.
The major difference between conventional and adaptivenverse planning is in the dose construction in organs ofnterest. In the former, the dose distribution in organs ofnterest is calculated using a single 3D CT image. In contrast,daptive inverse planning includes both the delivered doseor BED) in organs of interest before the time of plan modi-cation and the random process of organ geometrical varia-ion (or biological variation) for the remaining treatment inhe total treatment dose (or BED) construction.8 Because of
he inclusion of temporal information of the random process wn the adaptive inverse planning, it is also called 4D inverselanning or probability-based inverse planning.Two approaches of 4D adaptive inverse planning can be
roposed fundamentally with respect to different assump-ions of organ displacement detection and beam control ca-abilities. If patient organ position at any time can be in-tantly detected and immediately tracked using the radiationeam, then inverse planning can be performed with respecto the organ geometry at each time instant, and the beamperture can be designed to synchronize with the target po-ition of the time instant. At the present time, this techniqueas been proposed to manage low frequency or intertreat-ent organ volume/position variation, such as online image-
uided replanning for prostate cancer treatment.9 In theracking of high frequency or intratreatment organ motion,uch as patient respiratory-induced target motion, computernd moving phantom simulations, thus far, are constrainedy the assumption of motion reproducibility.10 Indeed, theuccess of real time tracking of respiratory-induced targetotion is fully dependent on the reproducibility of the organotion and the controllability of radiation beam.The other 4D adaptive inverse planning technique7 uses
he frequency information of organ variation or motion,ather than its instantaneous appearance, obtained from mul-iple 3D or 4D volumetric images in the dose construction,nd thus the objective function and the constraints for opti-ization. By directly including organ variation or motion
requency/probability density function (PDF) in dose con-truction, inverse planning can optimize machine deliveryuch that a greater dose is assigned to the area where thearget appears with a high frequency, while avoiding dose tohe area where the normal organ appears more frequently. Inddition, by including the previously delivered dose in thebjective of inverse planning, the modified plan can compen-ate for the unexpected hot or cold spots of dose that haveeen so far delivered in organs of interest. Adaptive inverselanning for different treatment sites has been explored.8,11
urrent studies of 4D inverse planning on lung cancer12 havehown that the optimization results are comparable to thosechieved by the idealized 4D tracking technique.
Adaptive plan modification with 4D adaptive inverse plan-ing is one of the ultimate goals for adaptive treatment mod-
fication. However, it should not be the limitation for clinicalmplementation of adaptive techniques. Different studies onhe effects of adaptive replanning have been performed dur-ng the last decade, and demonstrate clear benefit on thereatment.13-16 Adaptive modifications, such as patient posi-ion correction, beam aperture, or target margin modifica-ions based on multiple treatment observations, as well aseplanning using single but the most recent CT image, haveeen routinely applied in some clinics for different treatmentites and will be discussed extensively in the following arti-les.
linical Practicehe principle of adaptive radiotherapy is fairly intuitive and
ell understood. However, clinical implementation of this
titfiacccoa
goacsicrocsf
avwuBoamrvmt
omsDrggnd
cUfraitc
v
trbmftcntssio
btttotpapuii
anatdapitaf
apdsttatbtrttc
82 D. Yan
echnique is complex, requiring a fundamental shift of thenfrastructure of the radiotherapy process from the conven-ional open-loop planning/treatment process to a closed-loopeedback control process. In the following articles, pioneer-ng efforts in clinical implementation of adaptive radiother-py based on patient anatomical imaging feedback are dis-ussed, with application to radiotherapy of head-and-neckancer, lung cancer, liver cancer, bladder cancer, cervical can-er, and prostate cancer. In addition, the potential applicationf biological imaging feedback for adaptive radiotherapy islso included.
Dose response–related organ deformation and volume re-ression are the most significant variations during the coursef head-and-neck treatment. Pierre Castadot and colleaguesccomplished a comprehensive review on head-and-neckancer adaptive radiotherapy. In summary, patient’s dailyetup variation causes limited dose variation in the organs ofnterest. However, radiotherapy induces major volumetrichanges in target and organs at risk during the treatment,esulting in a significant increase of treatment dose in normalrgans. Therefore, adaptive replanning during the treatmentourse becomes essential, although the optimal adaptivetrategy still needs to be defined because of the extra burdenor staff and associated cost.
Clinical implementation of lung cancer adaptive radiother-py needs to address multiple issues on intertreatment setupariation, intratreatment respiratory induced variation, asell as dose response–induced tumor regression, organ vol-me, and position variations. Jan-Jakob Sonke and Joseelderbos give a detail overview of the evolution and devel-pment of adaptive management for lung cancer radiother-py. In their article, different approaches of adaptive manage-ent for inter- and intratreatment variation, as well as dose
esponse–induced organ variation, are systematically over-iewed. It is clear from their report that adaptive manage-ent of lung cancer radiotherapy is essential and an impor-
ant clinical implementation for lung cancer radiotherapy.Liver cancer radiotherapy faces a similar challenge as the
ne in lung cancer radiotherapy. Respiratory-induced organotion causes significant inter- and intratreatment target po-
ition variation. In their overview, Kristy Brock and Lauraawson outline the existing methodologies in image-guided
adiotherapy for liver cancer, including patient-specific mar-in construction, 4D adaptive inverse planning, breath hold,ating, and tracking. Clinical applicability of these tech-iques, as well as patient selection and workflow, are alsoiscussed.One of the major challenges in the success of bladder can-
er radiotherapy is inherent intratreatment bladder motion.sing onboard CBCT imaging, different adaptive strategies
or either whole or partial bladder cancer radiotherapy areeviewed by Floris Pos and Peter Remeijer in their article ofdaptive management of bladder cancer radiotherapy. Clin-cal implementation of these strategies showed clear reduc-ion in treatment volume or radiation dose given to normalritical organs, thus justifying additional dose escalation.
Physiological and radiation dose induced morphologic
ariations of tumor and normal organs are significant duringhe course of cervical cancer radiotherapy and thus adaptiveadiotherapy has great potential. However, integrating bothrachy and external beam radiotherapy in the adaptive treat-ent process is challenging. Kari Tanderup et al provide a
ull overview of currently proposed techniques and simula-ion studies. On the basis of preliminary results from currentlinical implementation of adaptive radiotherapy, this tech-ique can most likely produce significant improvement inreatment outcome. Clinical implementation also faces con-iderable uncertainties, at the present time, the limitation ofoft-tissue contrast in CT image. Using multiple MR imagingn the adaptive process for cervical cancer is, therefore, rec-mmended.Adaptive management of prostate cancer radiotherapy has
een the earliest clinical implementation of adaptive radio-herapy. In their article, the Beaumont group provides theechnique and experiences of their early clinical implemen-ation of offline adaptive radiotherapy to manage patient/rgan position and volume variation during prostate cancerreatment. They also provide an overview of the recent pro-osals for online and offline CBCT image-guided adaptivepproaches for prostate cancer radiotherapy. From their re-ort, clinical outcome on tumor control and GI/GU toxicitysing the offline adaptive technique have demonstrated clear
mprovement in prostate cancer radiotherapy with convinc-ng evidence of the benefits of adaptive radiotherapy.
Clinical application of biological image feedback anddaptive radiotherapy is in its early stage, but represents theext frontier of adaptive control of radiotherapy. Aste Soviknd colleagues provide a wide-range overview on the spatial/emporal variation of tumor and normal organ bio-functionuring the radiotherapy course. They also provide an outlinend description on the bio-image feedback and adaptivelanning modification strategies. Simulation results in lim-
ted examples have shown that significant improvement inherapeutic ratio could be achieved by performing frequentlydaptive inverse planning modification based on bio-imagingeedback.
Adaptive radiotherapy is a growing area in clinical researchnd development. Different adaptive techniques to includeatient-specific variations online or offline in planning andelivering modifications are discussed extensively in this is-ue of Seminars in Radiation Oncology. The actual and poten-ial improvements in clinical treatment outcome reported inhe articles are extremely encouraging and greatly promotedaptive radiotherapy. Although there are extra burdens inhe clinical application of adaptive radiotherapy and theseurdens are impediments to the clinical implementation ofhis technique, the rapid improvement in onboard volumet-ic imaging, 4D adaptive treatment planning, and deliveryechnology will progressively diminish these burdens. Adap-ive radiotherapy will eventually become the standard in thelinical practice of image-guided radiotherapy.
Di Yan, DSc, FAAPM
Guest Editor
R
1
1
1
1
1
1
1
Adaptive radiotherapy 83
eferences1. Yan D, Vicini F, Wong J, et al: Adaptive radiation therapy. Phys Med
Biol 42:123-132, 19972. Yan D: Image-guided/adaptive radiotherapy in new technologies in
radiation oncology, in Schlegel W, Bortfeld T, Grosu AL (eds): MedicalRadiology-Radiation Oncology. Springer, Germany, 2005, pp 321-336
3. Astrom KJ, Wittenmark B: Adaptive Control, Second edition. Addison-Wesley, USA, 1995
4. Yan D, Lockman D, Brabbins D, et al: An off-line strategy for construct-ing a patient-specific planning target volume for image guided adaptiveradiotherapy of prostate cancer. Int J Radiat Oncol Biol Phys 48:289-302, 2000
5. Yan D, Jaffray D, Wong J: A model to accumulate fractionated dose in adeforming organ. Int J Radiat Oncol Biol Phys 44:665-675, 1999
6. Yan D, Lockman D: Organ/patient geometric variation in external beamradiotherapy and its effect. Med Phys 28:593-602, 2001
7. Lof J, Lind K, Brahme A: An adaptive control algorithm for optimizationof intensity modulated radiotherapy considering uncertainties in beamprofiles, patient setup and internal organ motion. Phys Med Biol 43:1605-1628, 1998
8. Birkner M, Yan D, Alber M, et al: Adapting inverse planning to patientand organ geometrical variation: Algorithm and implementation. MedPhys 30:2822-2831, 2003
9. Ghilezan M, Yan D, Liang J, et al: Online image-guided IMRT for
prostate cancer: How much improvement can we expect? A theoreticalassessment of clinical benefits and potential for dose escalation byimproving precision and accuracy of radiation delivery. Int J RadiatOncol Biol Phys 60:1602-1610, 2004
0. Keall PJ, Joshi S, Vedam SS, et al: Four-dimensional radiotherapy plan-ning for DMLC-based respiratory motion tracking. Med Phys 32:942-951, 2005
1. Trofimov A, Rietzel A, Lu HM, et al: Temporo-spatial IMRT optimiza-tion: Concepts, implementation and initial results. Phys Med Biol 50:2779-2798, 2005
2. Zhang P, Hugo G, Yan D: A planning study comparison of real-timetarget tracking and 4D inverse planning for managing patient respira-tory motion. Int J Radiat Oncol Biol Phys 72:1221-1227, 2008
3. Martinez A, Yan D, Brabbins D, et al: Improvement in dose escalationusing the process of adaptive radiotherapy combined with 3D-confor-mal or intensity modulated beams for prostate cancer. Int J RadiatOncol Biol Phys 50:1226-1234, 2001
4. Harsolia A, Hugo G, Kestin L, et al: Dosimetric advantages of four-dimensional (4D) adaptive image-guided radiotherapy (IGRT) for lungtumors using online cone-beam CT. Int J Radiat Oncol Biol Phys 70:582-589, 2008
5. Pötter R, Dimopoulos J, Georg P, et al: Clinical impact of MRI assisteddose volume adaptation and dose escalation in brachytherapy of locallyadvanced cervix cancer. Radiother Oncol 83:148-155, 2007
6. Hansen EK, Bucci MK, Quivey JM, et al: Repeat CT imaging and re-planning during the course of IMRT for head-and-neck cancer. Int J
Radiat Oncol Biol Phys 64:355-362, 2006

















