
Acute Respiratory Failure Yoon Jung Oh,M.D. Departments of Pulmonary and Critical Care Medicin Ajou...
24
Acute Respiratory Failure Yoon Jung Oh,M.D. Departments of Pulmonary and Critical Care Medic in Ajou University School of Medicine
-
date post
19-Dec-2015 -
Category
Documents
-
view
217 -
download
2
Transcript of Acute Respiratory Failure Yoon Jung Oh,M.D. Departments of Pulmonary and Critical Care Medicin Ajou...

Acute Respiratory Failure
Yoon Jung Oh,M.D.
Departments of Pulmonary and Critical Care MedicinAjou University School of Medicine

Hypoxemic respiratory failure PaO2 < 55 mmhg , FiO2 ≥ 0.6• Acute : develops in min to hr• Chronic : develops over several days or longer
Hypercapnic respiratory failure PaCO2 > 45 mmHg • Acute : develops in min to hr( pH < 7.3)• Chronic : develops over several days or longer
Hypercapnic and hypoxemic respiratory failure coexist.
Definition

Acute Respiratory Failure
PaCO2 < 45 mmHgType 1 respiratory failure
PaCO2 > 45 mmHgType II ventilatory failure
CXRCXR Black• acute pulmonary embolism• vascular obstruction• R-L shunt
WhiteDiffuse• ARDS• Pulmonay edema• Pulmonary fibrosisLocalized• Pneumonia• atelectasis
Black• COPD• Status asthmaticus• Alveolar hypoventilation• Drug overdose• Neuromuscular disease
WhiteDiffuse• ARDS• Pulmonary edema• Pulmonary fibrosisLocalized• Pneumonia + COPD• Drug overdose
ABGA

Ventilatorysupply
Ventilatorydemand
Ventilatory supply exceeds ventilatory demand.
Ventilatorysupply
Ventilatorydemand
Ventilatory supply equals ventilatory demand.
Ventilatorysupply
Ventilatorydemand
Ventilatory demand exceeds ventilatory supply.
A
B
C
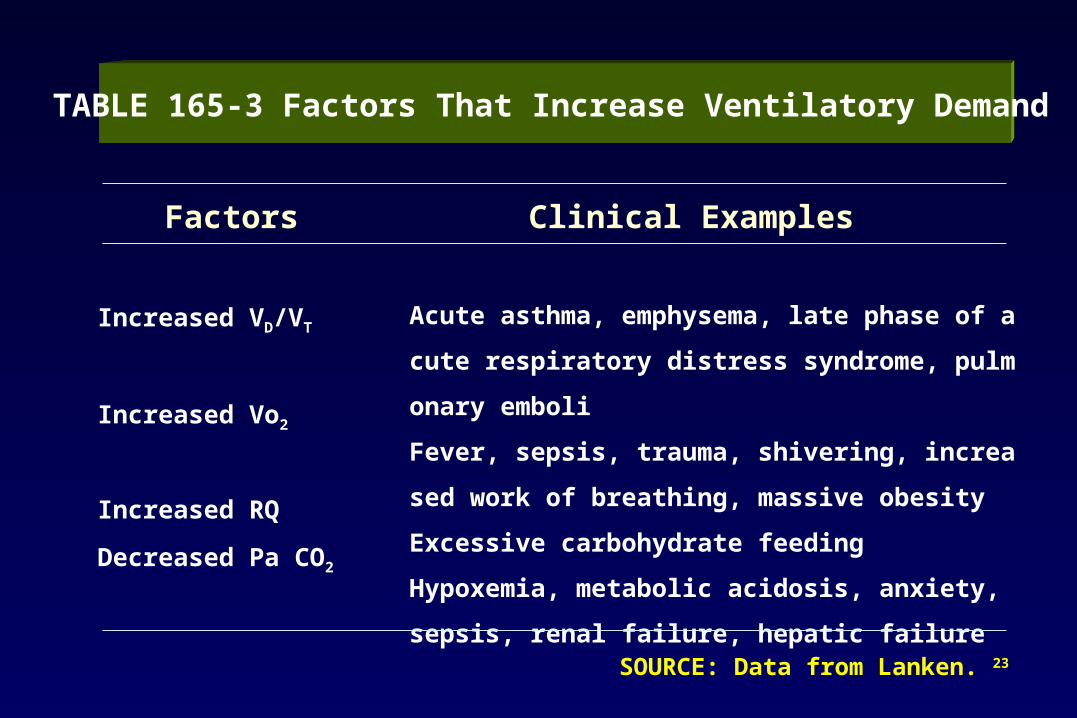
TABLE 165-3 Factors That Increase Ventilatory Demand
Factors Clinical Examples
Increased VD/VT
Increased Vo2
Increased RQ
Decreased Pa CO2
Acute asthma, emphysema, late phase of acute respirat
ory distress syndrome, pulmonary emboli
Fever, sepsis, trauma, shivering, increased work of brea
thing, massive obesity
Excessive carbohydrate feeding
Hypoxemia, metabolic acidosis, anxiety, sepsis, renal fa
ilure, hepatic failure
SOURCE: Data from Lanken. 23

TABLE 165-2 Factors That Diminish Ventilatory Supply
Factors Examples
Decreased respiratory muscle strength Muscle fatigue
Disuse atrophy
Malnutrition Electrolyte abnormalities Arterial blood gas abnormalities Fatty infiltration of diaphragm Unfavorable alteration in diaphragm length-tension relationshipIncreased muscle energy requirement or decreased substrate supply High elastic work of breathing High resistive work of breathing Reduced diaphragm perfusionDecreased motor neuron function Decreased phrenic nerve output
Decreased neuromuscular transmissionAbnormal respiratory mechanics Airflow limitation Loss of lung volume Other restrictive defects
Recovery from acute respiratory failure, high respiratory rates, increased Pdi/Pdimax,* increased inspiratory timeProlonged mechanical ventilation, following phrenic nerve injuryProtein-calorie starvationLow serum phosphate or potassium concentrationsLow pH, low PaO2, high PaCO2
ObesityFlattened domes of diaphragm caused by hyperinflation
Low lung or chest wall compliance, high respiratory rate Airway obstructionShock, anemia
Polyneuropathy, Guillain-Barré syndrome, phrenic nerve transection or injury, poliomyelitisMyasthenia gravis, use of paralyzing agents
Bronchospasm, upper-airway obstruction, excessive airway secretionsAfter lung resection, large pleural effusionPain-limited inspiration; tense abdominal distention due to ileus peritoneal dialysis fluid, or ascites

Hypoxemic Respiratory Failure
Alveolar hypoventilatio
n
Drug overdose Normal D(A-a)O2, PaCO2 > 40 mmHg
V/Q mismatching
COPD, asthma Corrected by oxygen
R-L shunt ARDS, pneumonia Not corrected by oxygen
Diffusion disturbance
Interstitial disease Same to V/Q mismatching
Low FiO2 High altitude Normal D(A-a)O2
Pathophysiology(1)

Hypercapnic Respiratory Failure
↓Alveolar ventilation Central-drug overdose,NM drug, flail chest, COPD, asthma
↑ Anatomic/physiologic dead space(Vd/Vt)
COPD, ARDS,bronchospasm
↑ CO2 production fever,sepsis,burn,infection,exercise, hyperalimentation
Pathophysiology(2)

Hx : 3 년전 bronchial asthma 진단받았으며 3 일전 URI 후 악화된 호흡곤란을 주소로 내원 . ABGA : pH 7.5 PaO2 50 mmHg, PaCO2 30 mmHg HCO3 22 mmol/L at room air O2 5 L/min PaO2 65 mmHg
P/E : RR 30/min, use of accessory muscle wheezing on whole lung field
CXR : hyperinflation
Case 1.1 F/30

Acute hypoxemic respiratory failure
due to acute exacerbation of asthma
Diagnosis 1.

병동에서 치료중 호흡곤란을 계속 호소함 .
ABGA : pH 7.4 PaO2 65 mmHg PaCO2 40 mmHg
O2 sat 92%
Case 1.2

Case 1.3
다음날 아침 , 밤새 호흡곤란으로 한숨도 자지 못했다하며
지속적인 호흡곤란을 호소함 .
ABGA : pH 7.35 PaO2 60mmHg PaCO2 50mmHg
O2sat 90%

Case 2. F/19
남자친구와 다툰 후 수면제 100 알을 복용후 응급실로 내원 .
ABGA : pH 7.25 PaO2 60mmHg PaCO2 70mmHg
HCO3 27 mmol/L O2sat 90%

Acute hypercapnic respiratory failure
due to drug overdose
Diagnosis 2
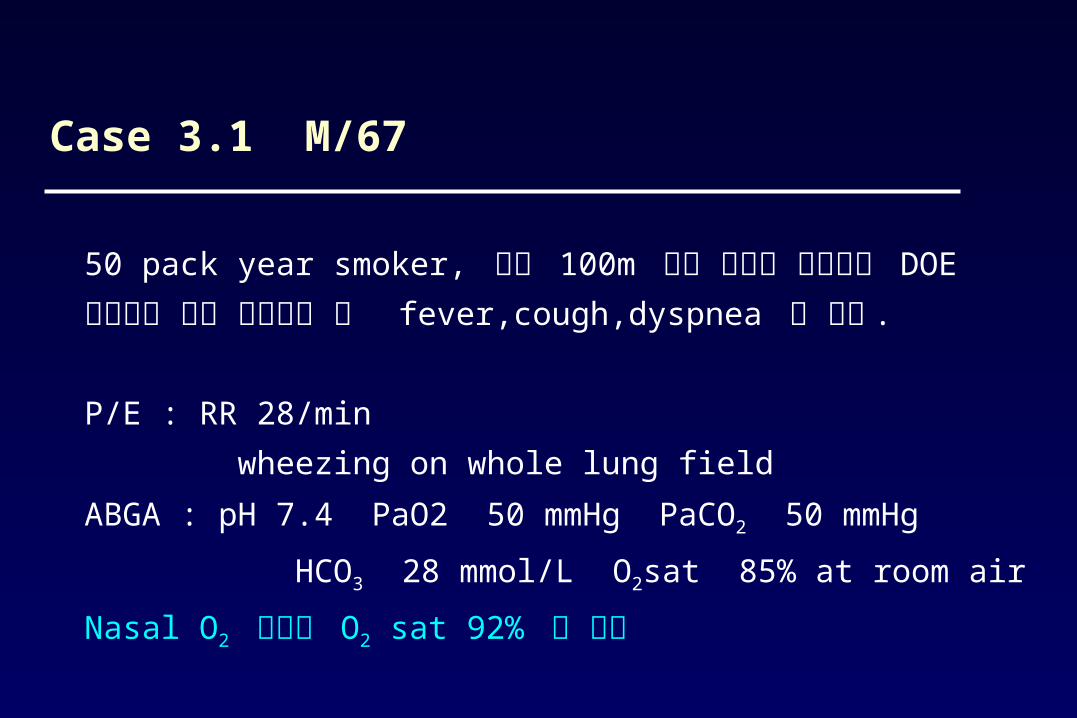
50 pack year smoker, 평소 100m 정도 걸으면 심해지는 DOE 있었으며 최근 감기앓은 후 fever,cough,dyspnea 로 내원 .
P/E : RR 28/min wheezing on whole lung field
ABGA : pH 7.4 PaO2 50 mmHg PaCO2 50 mmHg
HCO3 28 mmol/L O2sat 85% at room air
Nasal O2 투여후 O2 sat 92% 로 증가
Case 3.1 M/67

Chronic obstructive pulmonary disease ( Emphysema )
Diagnosis 3.1

응급실에서 산소를 투여한지 4 시간 후 , 환자가 헛소리를
하고 자꾸 자려고만 한다고 보호자가 호소함 .
ABGA : pH 7.2 PaO2 80 mmHg PCO2 90 mmHg
nasal O2 5L/min
Case 3.2

Acute hypercapnic respiratory failure
CO2 narcosis
Diagnosis 3.2

CNSEfferentsCNSEfferents
Effector Components
Perepheral Nerves
Perepheral Nerves
Repiratory m.Chest wall
Repiratory m.Chest wall
AirwayAlveoliAirwayAlveoli
AfferentIntegration
In CNS
AfferentIntegration
In CNS
Chemo-receptorsChemo-receptors
PaO2PaCO2PaO2
PaCO2VA, VEVA, VE

Failed respiratory component pH PaCO2 PaO2 P(A-a)O2 VE VA
Central nervous system ↓ ↑ ↓* NL or ↑# ↓ ↓
Peripheral nervous system or chest wall
↓ ↑ ↓* NL or ↑# ↓ ↓
Airways In acute asthma
Early phase(before respiratory failure)
↑ ↓ NL ↑ ↑ ↑
“Crossover point” NL NL NL or ↓
↑ ↑ NL
With respiratory muscle fatigue
↓ ↑ ↓ ↑ ↓$ ↓$
*PaO2 may decrease when pneumonia or atelectasis occurs as a complication#P(A-a)O2 widens when pnumonia or atelectasis occurs as a complication$VE declines when frank respiratory muscle failure occurs.

Failed respiratory component
pH PaCO2 PaO2 P(A-a)O2 VE VA
In COPD
Non-CO2 retainer ↓ NL or ↑& ↓ ↑ ↑ ↓
CO2 retainer
Basseline NL or ↓ ↑ ↓ ↑ NL or ↑ ↓
Flare ↓ ↑ ↑ ↓ ↓ ↑ NL or ↑Or ↓
↓
Alveoli
Before resp. m. fatigue ↑ ↓ ↓ ↓ ↑ ↑ ↑ ↑
After resp.m. fatigue ↓ ↑ ↓ ↓ ↑ ↑ ↓ ↓
&PaCO2 may increase during an exacerbation

• Correct hypoxemia/respiratory acidosis
• Patent upper airway
• Adequate ventilation
• Supplemental oxygen
Treatment of Acute Respiratory Failure

• Increase VA
• Bronchodilator
• Control of infection
• Oxygen therapy
Treatment of Respiratory Failure

To decrease VCO2
• Antipyretics
• Cooling blanket
• Decrease muscle activity
To increase VA
• Prevent airflow obstruction
• Respiratory training
• Intubation & mechanical ventilation
• Cautious administration of sedatives
Ventilatory Failure


















