Acute Respiratory Failure Lecture 2014-2015 (5!1!14) FINAL
60
Acute Respiratory Failure Matthew Karulf, MD Pulmonary & Critical Care Medicine Michigan State University College of Human Medicine Spectrum Health Medical Group
-
Upload
rentedmule00 -
Category
Documents
-
view
19 -
download
1
description
Acute Respiratory Failure Lecture 2014-2015 (5!1!14) FINAL
Transcript of Acute Respiratory Failure Lecture 2014-2015 (5!1!14) FINAL
Acute Respiratory Failure
Matthew Karulf, MD Pulmonary & Critical Care Medicine
Michigan State University College of Human Medicine
Spectrum Health Medical Group
Hypoxemic Respiratory Failure Type I Respiratory Failure
• Definition
– Impairment of respiratory function characterized by the presence of hypoxemia as diagnosed by a reduced partial pressure of oxygen in arterial blood.
– PaO2 <= 60 mmHg
• Acute vs. Chronic
– Acute hypoxemia occurs over period of hours to days.
– Chronic hypoxemia occurs over a period of weeks to months.
Murray & Nadel’s Textbook of Respiratory Medicine (5th ed.)

PaO2 <= 60 is chosen because below this Hgb saturation falls rapidly.
Murray & Nadel’s Textbook of Respiratory Medicine (5th ed.)

Anatomic Differential
Murray & Nadel’s Textbook of Respiratory Medicine (5th ed.)

(A-a) gradient
• Normal (A-a) gradient increases with age.
= Approx 10-20 (depending on age of patient)
• Alveolar gas equation 100 = 0.21 X [760 – 47] – [40/0.8] = 150 - 50
• (A-a) gradient = PAO2 – PaO2
• Differential of a Normal (A-a) gradient
– Normal – Pure Hypoventilation – Low FIO2

Common Causes with an abnormal (A-a) gradient
• Cardiogenic pulmonary edema
• Pneumonia
• Sepsis
• Aspiration
• Trauma
• Multiple transfusions
– TRALI/TACO

Case #1
• 48 yo woman complains of 3 days of dyspnea, cough, fevers, malaise and left-sided pleuritic chest pain.
• Vital Signs
– Temp 39.2 Celsius HR 95 BP 100/60 RR 35
– Room Air O2 saturation 82%
• What is your differential diagnosis for this patient?

Differential Diagnosis
• Pneumonia
• Pericarditis
• Influenza
• Infective Endocarditis with septic emboli
• Empyema
• Venous Thromboembolic Disease

What are your initial diagnostic and therapeutic steps?

HPI
• Symptoms began 3 days prior with cough, fevers and malaise.
• Progressively worsening
• No hemoptysis
• No syncope, trauma
• No significant past medical or surgical history
• Works as a grade school teacher without recent sick contacts aside from students with colds.
• Non-smoker, No EtOH or illicit drug use

• What risk factors identify a patient who may have multidrug resistant pathogens?
Initial Evaluation
• ABC’s!
• Supplemental Oxygen is placed
– O2 saturation improves to 90% on NRBM
• Physical Exam
– Appears in acute distress
– Lung auscultation reveals rhonchi over left base
• IV access, fluid challenge, labs and CXR


Interpret the following labs
• Na 136 Cl 100 BUN 30 • K 3.8 HCO3 18 Cr 1.4
• WBC 4.2 (36% Bands) • Lactate 2.7
• Room Air ABG
– 7.36/28/47 • PAO2 = 0.21 x [760 – 47] – [28/0.8] = 115
= 150 - 35
• (A-a) gradient = PAO2 – PaO2 = 115 – 47 = 68 – Normal (A-a) gradient for this patient = 2.5 + (0.21 * Age) = 13

Case #1 Working Diagnosis
• Previously healthy 48 yo woman with
– Community Acquired Pneumonia
– Severe Sepsis
– Acute Respiratory Failure with Hypoxemia
– Acute Kidney Injury
– Lactic Acidosis
– Elevated Anion Gap Metabolic Acidosis
– Respiratory Alkalosis

• Why is this patient hypoxemic?
• Why does pneumonia cause hypoxemia?

Five Mechanisms of Hypoxemic Respiratory Failure
• Normal (A-a) gradient
– Decreased Inspired Oxygen Pressure
– Hypoventilation
• Abnormal (A-a) gradient
– Impaired Diffusion
– Right-to-Left Shunt
– Ventilation-Perfusion Mismatch

Five Mechanisms of Hypoxemic Respiratory Failure
• Decreased Inspired Oxygen Pressure
– Reduction in FIO2 (suffocation)
– Altitude

Murray & Nadel’s Textbook of Respiratory Medicine (5th ed.)

Five Mechanisms of Hypoxemic Respiratory Failure
• Decreased Inspired Oxygen Pressure
• Hypoventilation
– As alveolar CO2 increases Alveolar O2 decreases
– Opioid Overdose • Will see a normal (A-a) gradient

Murray & Nadel’s Textbook of Respiratory Medicine (5th ed.)

Five Mechanisms of Hypoxemic Respiratory Failure
• Decreased Inspired Oxygen Pressure
• Hypoventilation
• Impaired Diffusion
– Unlikely to be sole cause of respiratory failure
– Often coexists with other mechanisms
– Pulmonary Edema • Cardiogenic
• Non-Cardiogenic

Significant reserve overcomes many diffusion impairments
Murray & Nadel’s Textbook of Respiratory Medicine (5th ed.)

Five Mechanisms of Hypoxemic Respiratory Failure
• Decreased Inspired Oxygen Pressure
• Hypoventilation
• Impaired Diffusion
• Right-to-Left Shunt
– Intrapulmonary • Atelectasis or Consolidation with loss of hypoxic vasoconstriction
• Pulmonary arteriovenous malformation
– Intracardiac • ASD with eisenmeinger’s physiology

Five Mechanisms of Hypoxemic Respiratory Failure
• Decreased Inspired Oxygen Pressure
• Hypoventilation
• Impaired Diffusion
• Right-to-Left Shunt
• Ventilation-Perfusion Mismatch
– A Small V/Q mismatch is normal and explains the normal (A-a) gradient.
– Pulmonary Embolus

The two most common mechanisms of acute hypoxemic respiratory failure.
Murray & Nadel’s Textbook of Respiratory Medicine (5th ed.)

Clinical Approach
Murray & Nadel’s Textbook of Respiratory Medicine (5th ed.)
Case #1 Working Diagnosis
• Previously healthy 48 yo woman with
– Community Acquired Pneumonia
– Severe Sepsis
– Acute Respiratory Failure with Hypoxemia
– Acute Kidney Injury
– Lactic Acidosis
– Elevated Anion Gap Metabolic Acidosis
– Respiratory Alkalosis

Case #1(cont.)
• Pt. remains distressed, complaining of dyspnea, despite the non-rebreather mask. – Temp 39.2 Celsius HR 112 BP 100/60 RR 38
– 90% Non-Rebreather Mask
• What additional management steps should be implemented now? – Intubation
– Empiric antibiotics for CAP in the ICU
– Early Sepsis Resuscitation
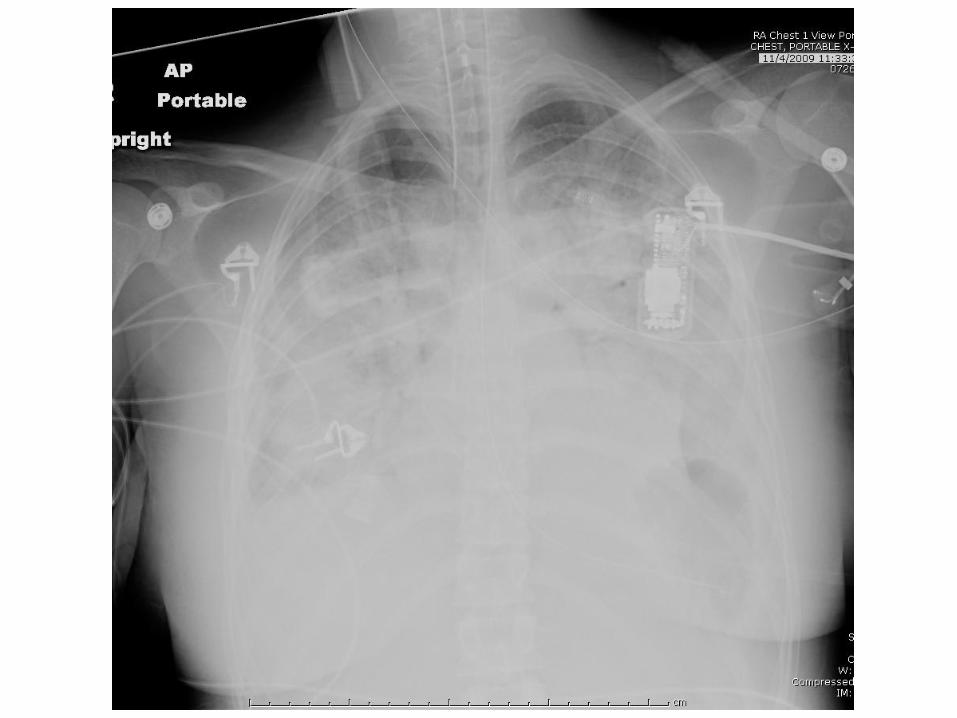
What clinical syndrome of respiratory failure does this patient have?
• Acute Respiratory Distress Syndrome (ARDS)
• Berlin Criteria 2012
• Acute onset (within 7 days of insult)
• PaO2/FiO2 < 300 (with a minimum PEEP of 5) – Mild 200-300
– Moderate 100-200
– Severe <100
• Bilateral opacities consistent with pulmonary edema (on either CXR or CT)
• Not fully explained by cardiac failure or volume overload

When should mechanical ventilation be initiated?
When hypoxemic or hypercapneic respiratory failure cannot be treated by less aggressive
methods.
Non-Invasive Positive Pressure Ventilation (NIPPV) or Invasive.

What is the mechanical ventilation strategy in ARDS?
Low Tidal Volume Ventilation.
(6ml/kg PBW)
• 861 patients w/ ALI randomized – 4-6ml/kg PBW vs. 12ml/kg PBW
– Goal Pplat <30 cm H2O
• Main Outcomes – Mortality

The Acute Respiratory Distress Syndrome Network. N Engl J Med 2000;342:1301-1308

• What information is needed in order to determine the appropriate tidal volume?
– Gender and Height
– Not the measured weight!
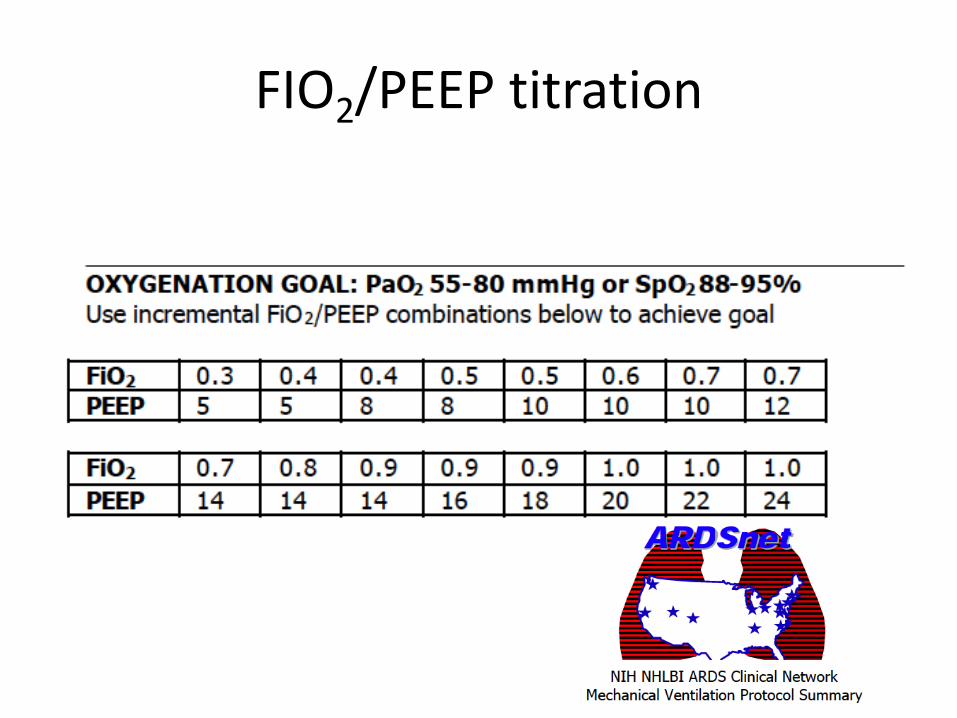
FIO2/PEEP titration

• Why do patients with ARDS benefit from a low tidal volume and PEEP strategy?
• Limits ventilator associated lung injury.
• Decreases biomechanical factors contributing to multisystem organ failure and death.

Slutsky AS, Ranieri VM. N Engl J Med 2013;369:2126-2136.

Slutsky AS, Ranieri VM. N Engl J Med 2013;369:2126-2136.

Protective Ventilation
Malhotra A. N Engl J Med 2007;357:1113-1120

Lung Protective Ventilation
Slutsky AS, Ranieri VM. N Engl J Med 2013;369:2126-2136.
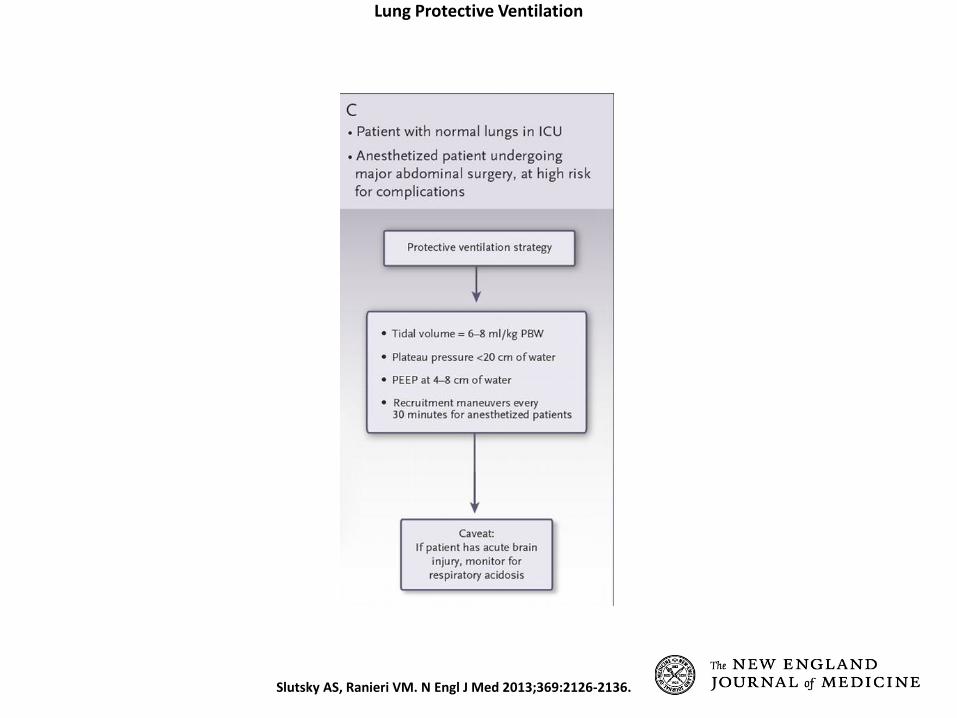
Lung Protective Ventilation
Slutsky AS, Ranieri VM. N Engl J Med 2013;369:2126-2136.

Case #2
• 68 yo man presents with 5 days of progressive dyspnea and increased cough productive of purulent sputum.
• Vital Signs
– Temp 37.9 Celsius HR 95 BP 100/60 RR 35
– Room Air O2 saturation 82%
• What is your differential diagnosis?

Differential Diagnosis
• Acute Exacerbation of Chronic Bronchitis
• Pneumonia
• Venous Thromboembolic Disease
• Acute Myocardial Infarction

HPI (cont.)
• History of COPD, FEV1 47% predicted.
• Ongoing 50 pack year history of Tobacco Abuse.
• Two “pneumonias” in the past year treated with prednisone and azithromycin.
Objective Findings
• Oxygen saturation improves to 89% on 3L
• Appears distressed, speaks in 4 word sentences.
• Intercostal retractions, pursed lip breathing
• Lung auscultation reveals diffuse expiratory wheezes.
ABG on 3L 7.24/80/78 Na 139 Cl 99 BUN 25 K 3.8 HCO3 34 Cr 1.2


• What is your patient suffering from?
• Acute on Chronic Hypercarbic Respiratory Failure
• Acute Exacerbation of Chronic Bronchitis

Acute Hypercarbic Respiratory Failure
• PaCO2 is elevated.
• Total minute ventilation is the sum of alveolar ventilation
and dead space ventilation.
• A decrease in total minute ventilation or an increase in dead space ventilation can reduce alveolar ventilation.
• Any decrease in or increase in with constant results in increased PaCO2.
= CO2 production
= Alveolar ventilation

Acute Hypercarbic Respiratory Failure
• The absolute PaCO2 level is not diagnostic.
– Many conditions result in chronic hypercapnia.
• “Acute” implies that PaCO2 rises faster than the kidneys are able to retain bicarbonate, resulting in acute respiratory acidosis.
• The diagnosis requires an arterial blood gas!

Physiologic mechanisms of acute ventilatory failure
Murray & Nadel’s Textbook of Respiratory Medicine (5th ed.)
Won’t Breathe Can’t Breathe

Reduced Ventilatory Drive “Won’t Breathe”
• Pharmacologic disruption – Drug overdose
• Consider reversal agents (naloxone for opioids and flumazenil for benzodiazepines)
• Acquired Defect – Stroke
– Neoplasm
– Obesity-Hypoventilation syndrome
• Myxedema

Inadequate Ventilation despite effort “Can’t Breathe”
• Neuromuscular weakness – Cervical spinal cord injury – Myasthenia gravis (Monitor Vital Capacity)
• Restrictive Chest Wall disease – Kyphoscoliosis
• Airway Obstruction – Upper – foreign body, vocal cord paralysis – Lower – COPD, Status Asthmaticus
• Increased Dead-space ventilation – High V/Q – COPD (Emphysema) – Generalized pulmonary hypoperfusion – shock
• Increased CO2 production (unable to compensate) – Fever, sepsis, burns, trauma, seizures

Case #2 (cont.)
• What is your next step in the management of your patient with an acute exacerbation of COPD?
– ABC’s
– Bronchodilators
– Systemic Glucocorticoids
– Antibiotics
– NiPPV
Noninvasive Mechanical Ventilation
• Invasive mechanical ventilation for COPD (i.e. Intubation) exacerbations is associated with high morbidity and mortality.
• Noninvasive Positive Pressure Ventilation (NIPPV – e.g. BiPAP or CPAP) reduces intubation rates and in-hospital mortality for COPD exacerbations
• Plant et al. Lancet, 2000.
– NIPPV vs. standard therapy
– reduced intubation rates (15% vs. 27%, P = .02)
– Reduced mortality (10% vs. 20%, P = .05)

What are the indications for NIPPV?
• Hypoxemic respiratory failure
– Cardiogenic pulmonary edema
– Immunocompromised patients
• Hypercapnic respiratory failure
– Acute exacerbation of COPD
– Acute Asthma exacerbation

What are the contraindications to NIPPV?
• Uncooperative patient
• Inability to protect airway
• High risk for aspiration
• Cardiac or respiratory arrest
• Hemodynamic instability
• Myocardial ischemia
• Facial trauma, surgery, burns
Is post-extubation NIPPV beneficial in preventing reintubation?
• NIPPV for patients who develop respiratory distress within 48 hours of extubation may not prevent reintubation and may be harmful.
• Preemptive use of NIPPV (extubating to BiPAP) may prevent reintubation.
• Review on Liberation from mechanical ventilation: – McConville JF, Kress JP. N Engl J Med 2012;367:2233-2239
.