Post-infectious glomerulonephritis presenting as acute renal failure ...

Acute GlomerulonephritisMOHD ZAMIR GHOUSE
060100848
FAKULTAS KEDOKTERANUNIVERSITAS SUMATERA UTARA
2010

Introduction


• The glomerular filtration barrier (blood-urine) has 3 special layers:1. Endothelial cells2. Glomerular basement membrane3. Podocytes

• Diseases that injure the glomeruli are called glomerular diseases.
• Lab analysis often shows persons with glomerular disease to have:1. Proteinuria2. Hematuria

Definition• AGN is a disease characterized by sudden appearance of:
1. Edema2. Hematuria3. Proteinuria4. Hypertension 5. Oliguria
• This is due to the immunologic response which triggers inflammation and proliferation of glomerular tissue that results in damage to the glomerular layers.
Nephritic syndrome

Incidence
• Most cases occur in patients aged 2-12 years
• Only 10% of cases occur in patients older than 40 years
• Less than 5% of cases occur in patients younger than 2 years
old.
• Male to female ratio 2:1
• In children, most common is post infectious AGN, the majority
of which is post streptococcal AGN.

Etiology • Include post infectious, renal and systemic etiologies.
Post infectious
• Bacterial • Virus • Fungal • Parasitic
Renal
• MPGN• IgA nephropathy• Idiopathic rapidly
progressive GN
Systemic
• Vasculitis • Collagen vascular
disease (eg. SLE)• Polyarthritis
nodosa• Henoch-Schonlein
Purpura• Goodpasture
syndrome• Drug induced (eg.
Gold, penicillamine)

Pathophysiology • A streptococcal “nephritogenic” neuraminidase may alter
hosts’ IgG.• These causes IgG/anti-IgG immune complexes to be formed
and deposits in the glomeruli which causes damage to the glomeruli tissue.
• In patients with moderate-severe AGN, reduction in GFR causes expansion of the ECF which is responsible for edema, hypertension, anemia, circulatory congestion and encephalopathy.

Clinical manifestation
• Edema (appx. 85% of cases)
• Gross hematuria (30% of cases) cardinal signs
• Hypertension
• Oliguria
• Shortness of breath or dyspnea on exertion 2 ͦ� ͦ ͦpulmonary
edema.
• Pallor


Laboratory studies• APSGN remains a clinical
diagnosis and diagnosis of exclusion.
• Several lab studies may suggest either post infectious, renal or systemic causes of GN
• Results of the following tests may suggest other possible DDx.
FBC UFEME
BUSE
ASOT/anti-DNase B
C3,C4 levels
LFT
PT/APTT
Throat/skin swab
Urine C&S
USG

Differential diagnosis
• Other post infectious AGN
• IgA Nephropathy (Berger disease)
• Membranoproliferative glomerulonephritis (MPGN)
• Chronic Glomerulonephritis
• Vasculitis

Management • Management is aimed to:
1. Eradicate source of infection by a course of antibiotics
2. Control hypertension with anti hypertensive drugs (if severe)
3. Control fluid intake or the usage of diuretics to minimize edema and fluid overload
4. Restriction of high salt and protein diet in acute phase.
• Antibiotics Penicillin 25-50mg/kg/d PO tds for
10 days Erythromycin 30-50mg/kg/d PO
tds for 10 days
• Anti hypertensive Labetalol 0.5-2mg/kg/hr. IV Nitroprusside 0.5-2mcg/kg/hr. IV
• Diuretics Furosemide 1-3mg/kg/d PO bd
Prognosis
• Ultimate prognosis of PSGN largely depends on the severity of
the initial insult
• Complete recovery occurs in >95% of patients within 5 years.
• Prognosis is worst if there is:
1. Heavy proteinuria
2. Severe hypertension
3. Significant elevations of creatinine levels
• About 1-3% of patients progress to chronic renal failure.

Case report
MOHD ZAMIR GHOUSE060100848

Personal identification
DOA : 24th November 2010
• Name : Loh Win Son • DOB : 4th August 2004• Age : 6 years old• Sex : Male• Race : Chinese• Address: Kuala Perlis• Source of referral : Pediatric clinic
• Chief complaint : dark colored urine one day prior to admission

History of presenting illness• Patient was apparently well
until one day before admission at night when he noticed his urine dark in color.
• His mother also said she saw the urine and describes it as being tea colored. She said that it was the first time she noticed it.
• Patient went to KK the next morning and urinalysis was done and noted to have +3 proteinuria and hematuria with granular casts. Was then referred to HTF.
However there was no:• Body swelling • Loin pain• Pain upon urination • Abdominal pain• Headache • Dark/pale colored stool• Sore throat• History of recent skin infection
or trauma
Mother said that patient looks pale andwith decreased urine output.

Associated symptoms• 3 days before onset of dark colored urine patient had fever
with cough and runny nose.Fever : - low grade continuous throughout day, temperature
wasn’t documented. Fever subsided after given syrup paracetamol obtained from clinic.
Cough : - productive whitish sputum worsens at night and in cold weathers, also exaggerated when patient drinks
cold water. Was given cough syrup.+ difficulty in breathing without any chest tightness occasionally.Currently not eating well because he vomits each time taking food since his illness.No other significant findings in system review.

Past Medical History
Illness
• Patient has recurrent episodes of cough whenever exposed to cold weather or cold beverages
• Had an episode of difficulty in breathing last year, was given neb salbutamol at casualty. No admission and no similar attack since.
Past admissions
• First admission
Allergies
• Patient will cough and have runny nose when exposed to cold weather.
• No other known food or drug allergies
Surgical history
• No past surgical history

Birth history
•Age of conception was at 26 years old•Was compliant to doctors advices and follows routine follow up during pregnancy•No significant illness during pregnancy
Antenatal history
•Born term at 38th week gestation•Spontaneous vaginal delivery •Birth weight of 2.9kg•No complications during birth•Baby was also perfectly well
Birth history

Immunization and feeding history
• Immunization is currently complete and up to date, however no confirmation could be done as she did not bring the immunization card.
• He is currently on normal adult diet. Not eating well since illness.

Developmental history
• No history of developmental delay.
• Currently in kindergarten and always will be among the top 3
students in class.
• Socially active and communicates well with his surroundings

Family history

Social history• Patient is 6 year old with 2 younger brothers• He is active, cheerful and friendly. Often plays with his
Gameboy or with his brothers.• They all live with their parents in a house located in Kuala
Perlis• Father of patient owns a plaster ceiling shop while mother is a
housewife.• They are both financially stable• Mother is taking full care of her kids at home• No recent travel to endemically diseased areas

General examination• He was generally alert and conscious, playing with his toys and
brothers.• He looks nutritionally well with no signs of distress or gross
deformity.• His hydration status was good with moist mucous membrane
and intact skin turgor.• There was mild pitting edema noted on both lower limbs up to
one third of tibia• No jaundice, cyanosis or pallor

Vital signs• Level of consciousness : Alert• Pulse rate : 144x/min with good volume
and regular • Respiratory rate : 30x/min• Blood Pressure : 112/70mmHg• Temperature : 36.4 Celsius• Weight : 28.3kg plotted at 75th centile• Height : 115cm plotted at 50th centile

Physical examination
Head
• Throat was injected• Nasal discharge• No other abnormal findings
Neck
• No abnormal findings
Respiratory
• On auscultation breath sound was vesicular with fine crepitation on both lungs
• No other abnormal findings

Cardiovascular
• No abnormal findings
Abdomen
• Slightly distended with no visible veins or protruding umbilicus• On palpation was soft and non tender• No abnormal findings
Genitalia
• No scrotal swelling• No other abnormal findings
Summary • My patient Loh Win Son, a 6 year old Chinese boy from Kuala
Perlis who came with his mother to the paediatric clinic HTF on 24th November 2010 with the chief complaint of dark coloured urine for one day prior to admission. Upon urine examination there was + haematuria and + proteinuria. On examination there was no raised BP, throat was injected, mild pitting oedema noted up to 1/3 of tibia, lungs with fine crepitation. There was no other abnormal findings.
• Symptoms are correlated with recent history of respiratory tract infection and not associated with history of trauma.

Diagnosis
Provisional diagnosis
• Acute glomerulonephritis TRO other causes of hematuria
• Underlying bronchial asthma exb. URTI
Differential diagnosis
• Nephrotic syndrome• IgA nephropathy• Membranoproliferative
glomerulonephritis

Investigations • 24th November 2010
Full Blood Count• WBC 11.0 x10^9/L• RBC 6.0 x10^6/L
(high)• Hb 14.0 g/dL• Ht 41.0 %• MCV 70.4 fl (low)• MCH 23.5 pg (low)• MCHC 33.4 g/dL• PLT 395 x10^3/uL• Neutrophils 6.83 x10^3/uL• Lymphocytes 2.53 x10^3/uL• Monocytes 1.32 x10^3/uL
(high)• Eosinophils 0.22 x10^3/uL• Basophils 0.00 x10^3/uL
Urine FEME
• Urine glucose NORMAL• Bilirubin NEGATIVE• Ketone +3• Specific gravity 1.038• Blood +3• Urine pH 6.5• Protein +3• Urobilinogen 3.2• Nitrite NEGATIVE• Leucocytes NEGATIVE• Color Red• Turbidity Slightly cloudy• Microscopic >2250 Rbc with
granular casts
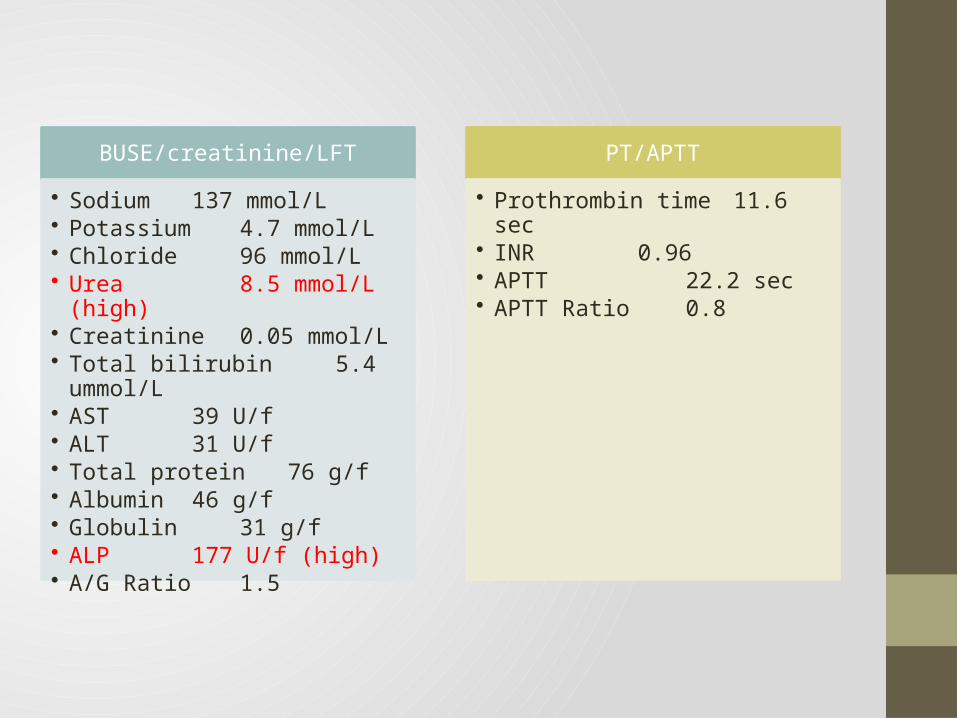
BUSE/creatinine/LFT
• Sodium 137 mmol/L• Potassium 4.7 mmol/L• Chloride 96 mmol/L• Urea 8.5 mmol/L
(high)• Creatinine 0.05 mmol/L• Total bilirubin 5.4 ummol/L• AST 39 U/f• ALT 31 U/f• Total protein 76 g/f• Albumin 46 g/f• Globulin 31 g/f• ALP 177 U/f (high)• A/G Ratio 1.5
PT/APTT
• Prothrombin time 11.6 sec• INR 0.96• APTT 22.2
sec• APTT Ratio 0.8
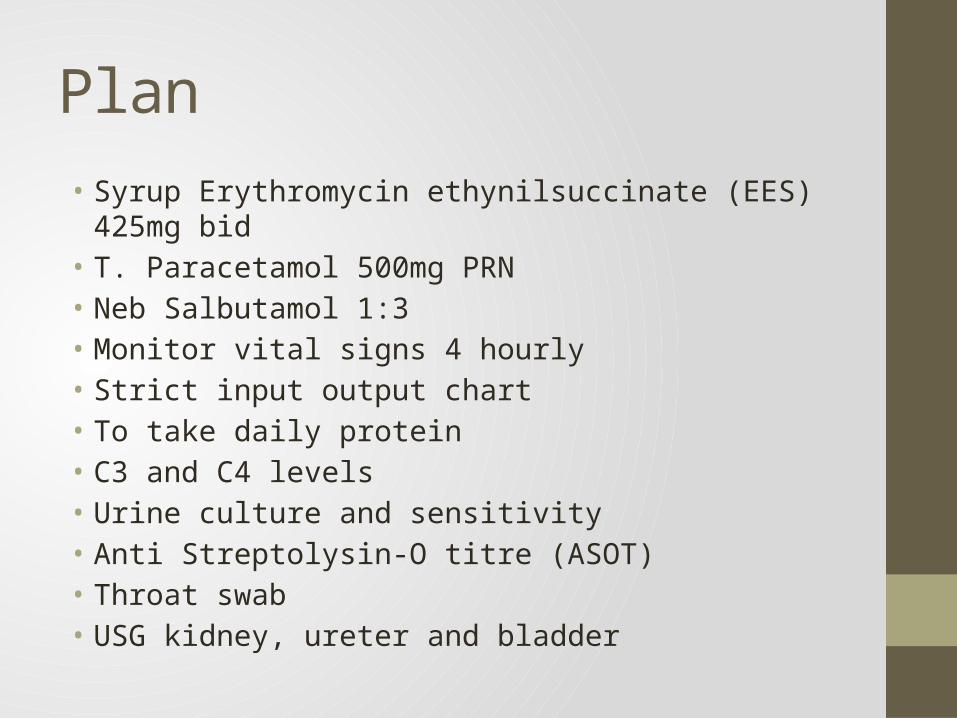
Plan• Syrup Erythromycin ethynilsuccinate (EES) 425mg bid• T. Paracetamol 500mg PRN• Neb Salbutamol 1:3• Monitor vital signs 4 hourly• Strict input output chart• To take daily protein• C3 and C4 levels• Urine culture and sensitivity• Anti Streptolysin-O titre (ASOT)• Throat swab• USG kidney, ureter and bladder

Follow up• 25th November 2010 (day one)
Subjective
• Comfortable and active
• Tolerating orally well
• Hydration status good
• No signs of oedema
• Currently no fever• Cough has reduced
since yesterday• No runny nose• No vomiting and
diarrhoea• No pain and
headache
Objective
• Alert and conscious
• HR : 120x/min• RR : 43x/min• SpO2 : 96% under
room air• Temperature : 37
Celsius• BP : 110/84mmHg• Weight : 27.3kg• Lungs with
occasional rhonchi and crepitation
• Heart : Dual rhythm no murmur
• Abdomen : Soft & non tender
Analysis
• AGN tro other cause of haematuria with URTI
Plan
• For 24hr protein analysis
• Monitor vital signs 4 hourly
• To review urine culture and ultrasound results
• To review ASOT results
• Continue syrup EES 435 bid (day 2)
• Give neb Salbutamol 4 hourly

• 26th November 2010 (day two)
Subjective
• Comfortable and active
• Started to eat normally
• Tolerating orally well• Hydration status
good• No more fever, cough
and runny nose• No vomiting and
diarrhoea• No pain and
headache• No signs of oedema• No longer pallor
according to mother
Objective
• Alert and conscious• HR : 118x/min• RR : 28x/min• SpO2 : 96% under
room air• Temperature : 37
Celsius• BP : 114/70mmHg• Weight : 28kg• Lungs clear• Heart : Dual rhythm
no murmur• Abdomen : soft and
non tender
Analysis
• AGN tro other cause of haematuria, URTI has resolved
Plan
• To discharge today• Review C3, C4, ANA,
RF and throat swab results on TCA (one week)
• To inform mother collect urine from Sunday and send to lab on Monday (24hrs protein)
• Continue syrup EES (D3) for 5 days
• Syrup Salbutamol 3mg tds
Urine FEME was done again noted to have :Ketone +2Blood +3Protein +3Rbc 900

I/O Monitoring Input output monitoring on first day of admission• Input : 500ml• Output : 295ml• Balance : +205ml
Urine output ≈ 0.43cc/kg/hr.
Input output monitoring on second day of admission• Input : 950mls• Output : 580mls• Balance : +370
Urine output ≈ 0.86cc/kg/hr.
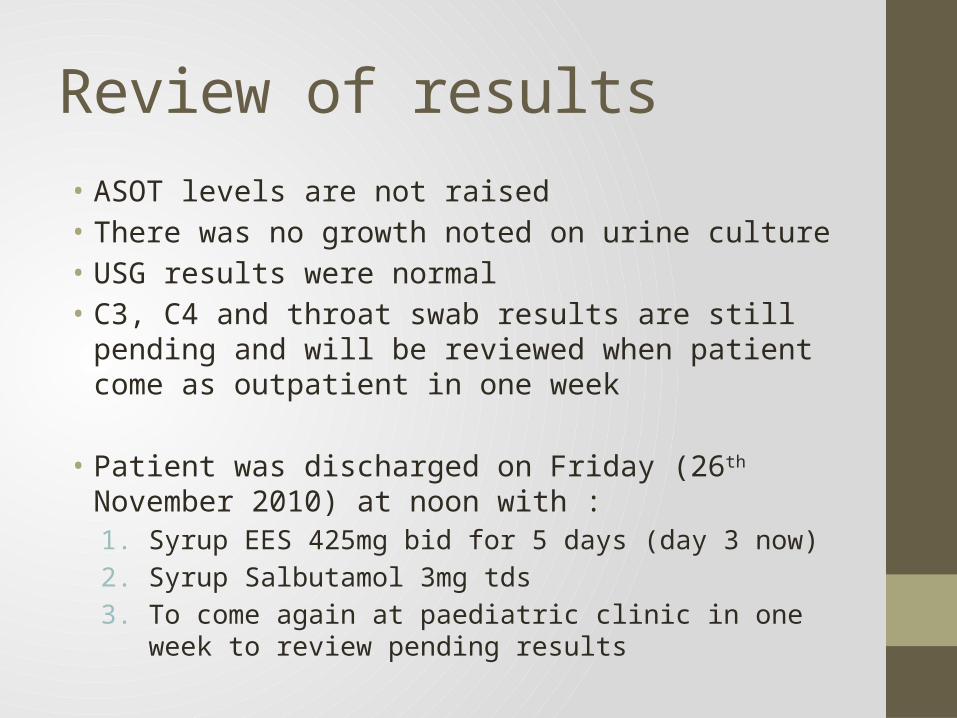
Review of results• ASOT levels are not raised• There was no growth noted on urine culture• USG results were normal• C3, C4 and throat swab results are still pending and will be
reviewed when patient come as outpatient in one week
• Patient was discharged on Friday (26th November 2010) at noon with :1. Syrup EES 425mg bid for 5 days (day 3 now)2. Syrup Salbutamol 3mg tds3. To come again at paediatric clinic in one week to review
pending results
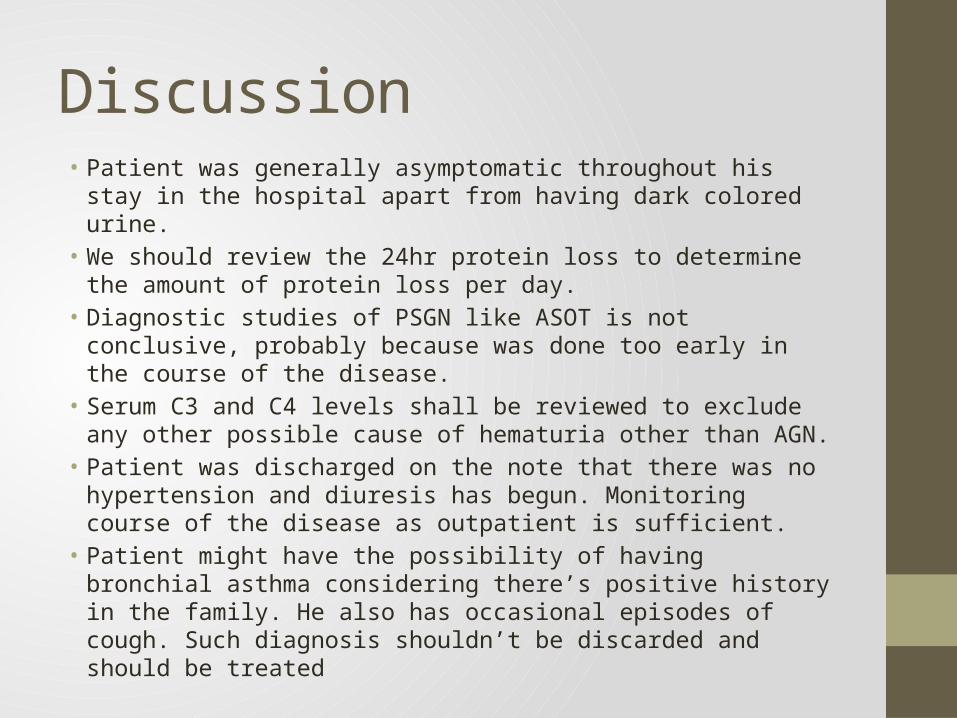
Discussion • Patient was generally asymptomatic throughout his stay in the
hospital apart from having dark colored urine.• We should review the 24hr protein loss to determine the
amount of protein loss per day.• Diagnostic studies of PSGN like ASOT is not conclusive, probably
because was done too early in the course of the disease.• Serum C3 and C4 levels shall be reviewed to exclude any other
possible cause of hematuria other than AGN.• Patient was discharged on the note that there was no
hypertension and diuresis has begun. Monitoring course of the disease as outpatient is sufficient.
• Patient might have the possibility of having bronchial asthma considering there’s positive history in the family. He also has occasional episodes of cough. Such diagnosis shouldn’t be discarded and should be treated
References 1. Behrman RE, Kliegman RM, Jenson HB. Nelson Textbook of Paediatrics: 19th Edition: Chapter
503.1, Post-streptococcal Acute Glomerulonephritis.
2. Brouhard BH, Travis LB. Acute postinfectionus glomerulonephritis. In: Edelman CM, ed. Pediatric Kidney Disease. 1992:1169-221.
3. Tom lissauer, Graham Clayden. Illustrated Textbook of Paediatrics: 3rd Edition: Chapter 18, Kidney and urinary tract disorders. 2007:307-320.
4. Travis LB, Dodge WF, Beathard GA, et al. Acute glomerulonephritis in children. A review of the natural history with emphasis on prognosis. Clin Nephrol. 1973;1(3):169-81
5. Oda T, Yamakami K, Omasu F, et al. Glomerular plasmin-like activity in relation to nephritis-associated plasmin receptor in acute poststreptococcal glomerulonephritis. J Am Soc Nephrol.2005;16(1):247-54
6. Herman A, Kappler JW, Marrack P, Pullen AM. Superantigens: mechanism of T-cell stimulation and role in immune responses. Annu Rev Immunol. 1991;9:745-72
7. Haycock GB. The treatment of glomerulonephritis in children. Pediatr Nephrol. 1988;2(2):247-55
8. Vander, Sherman, Luciano. Human physiology, the mechanism of body function. McGraw Hill. Chapter 16: Basic principles of renal physiology.1994:515-517.
9. Sharon Taylor, Andrew Raffles. Diagnosis in color paediatrics. Mosby-Wolfe. Chapter 6: Kidney and Urinary tract.1997: 173-185.