
Arcadia Plani-a: Acheron Fossae and Erebus Montes Workshop ...

Strategy & Action PlanStrategy & Action Plan
for Nursing & Midwifery
for Nursing & Midwifery
Acute Hospital Services
HSE Mid-Western Area
2005 - 2008

AcknowledgementsOn behalf of the Regional Steering Group for theStrategic Development of Nursing and Midwifery inthe Acute Hospital Services, I wish to acknowledgethe contribution of a number of people in thecreation of this strategy:-
• I would like to acknowledge the invaluable inputof the views of nurses and midwives asexpressed in the report of ‘The Explorative Studyinto the Expansion of Nursing and MidwiferyProfessional Roles in response to the EuropeanWorking Time Directive’ (Peelo-Kilroe, MWHB,2003).
• I wish to thank Mary Harris, Management andTraining Consultant, Change ManagementTraining, Limerick, who provided facilitation formeetings of the group.
• Appreciation is also expressed to Cora Lunn,Assistant Project Officer for the Development ofPost-Graduate Education, Nursing and MidwiferyPlanning and Development Unit, who providedconsistent support for and invaluable input tothe strategy.
• Thanks too to the consumer panels who gave oftheir time, and the facilitators of the sessions,Anne Buckley, Health Promotion Hospital Co-Ordinator, Mid-Western Regional Hospital, Ennisand Cathleen Ryan, CNM 3, Oncology Services,Mid-Western Regional Hospital, Limerick.
• I would also like to thank Dr. Kathleen MacLellan, Head of Professional Development,National Council for the ProfessionalDevelopment of Nursing and Midwifery, for heradvice on the development of this strategy andfor reviewing the document.
• Finally, I would like to thank John O Brien,Hospital Network Manager, for his support forthe development of the strategy.
Marie CaseyRegional Professional Development OfficerHSE Mid-Western Area

ContentsForeword
2 by Nora Irwin O’Rourke3 by John O’Brien
4 Section 15 1.0 Introduction5 1.1 Steering Group5 1.2 Methodology5 1.3 Implementation and Timeframe
6 Section 2Vision StatementStrategic Themes and Action Plan
20 Section 321 3.0 The Policy Context21 3.1 National Policy Drivers24 3.2 Nursing and Midwifery in Ireland
32 Section 433 4.1 Clinical Governance36 4.2 Leadership39 4.3 Professional Development of Nursing and Midwifery43 4.4 Fundamental Nursing Care44 4.5 Learning and Development48 4.6 Improving Working Lives
52 Section 553 5.1 Costing53 5.2 Implementation and Communication of the Strategy
54 Appendix 155 Feedback from Consumer Panel
Consultation
56 References
Strategy & Action Plan for N
ursing & M
idwifery
1

It is with great pleasure that I introduce thisStrategy and Action Plan for Nursing and Midwiferyin the Acute Hospitals Network, HSE Mid-WesternArea.
This strategy is timely now that we are five monthsinto the Health Service Reform Programme. TheAcute Hospital Networks are evolving and work isprogressing on collaborative working with allhospitals involved.
The strategy reflects the principles of the NationalHealth Strategy - Quality and Fairness: A HealthSystem for you (2001) and the Strategy for AcuteHospital Services, MWHB (2001).The strategy was informed by a literature review ofnational health and nursing and midwifery policydrivers and consultation with 38 focus groups ofnursing and midwifery staff in the acute hospitals inthis region.
This strategy will facilitate nursing and midwiferystaff across the six acute hospitals to work togetherwith a shared vision to take forward thedevelopment of nursing and midwifery practice.The strategy outlines plans to increase nurses’ andmidwives’ capabilities to provide responsive andneeds-driven services along the patient journey.The strategic themes - Clinical Governance,Leadership, Professional Development of Nursingand Midwifery, Fundamental Nursing Care,Learning and Development and Improving WorkingLives - will facilitate nurses and midwives inmeeting their potential in their professional andlegal responsibilities within the Scope of Nursingand Midwifery Practice Framework.Especially important is nurses and midwives focuson the traditional values of fundamental caring.This is relevant now as nurses and midwivesexpand their roles.
The document also acknowledges that nurses andmidwives are part of a much wider multi-disciplinary team incorporating clinical and non-clinical colleagues and it is only through a patient-centred team approach that the strategy will beachieved.
I am aware of the collaborative effort that has beenput into the creation of this comprehensivedocument and I would like to acknowledge thework of all Directors and Assistant Directors ofNursing and others involved in developing thisstrategy. I would also like to acknowledge the workof Marie Casey, Professional Development Officer, inleading this initiative.
I affirm my support to all involved in achieving theobjectives outlined in the action plan, which willensure that nurses and midwives have theopportunity to develop personally andprofessionally in order to provide high standards ofnursing and midwifery care.
Nora Irwin O’RourkeDirector, Nursing and Midwifery Planning andDevelopment UnitHSE Mid-Western Area
Foreword by Nora Irwin O’Rourke
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
2

The Strategy and Action Plan for Nursing andMidwifery in the Acute Hospitals Network HSE Mid-Western Area is a further addition to the strategicapproach to care group management and themanagement of functional supports in the Network.
The National Health Strategy - Quality and Fairness,the Networks Strategy for Acute Hospital Servicesand the Action Plan for People Managementprovide the basis for the plan. The documentemerged following widespread consultation withkey stakeholders and an extensive review ofrelevant literature.
The purpose of the document is to provide acohesive vision and approach to the developmentof nursing and midwifery across the Acute HospitalsNetwork in the HSE Mid-Western Area relying onkey themes of Leadership, Clinical Governance,Professional Development and Learning. Thetraditional caring role of the profession is alsorecognised as a keystone in future professionaldevelopment.
The ever increasing reliance on multidisciplinaryapproaches to caring and the key role of nursingand midwifery in that regard, recognising thecentrality of the patient, is the key to successfulimplementation.
I would like to thank all concerned with theformulation and production of the Strategyparticularly the Steering Group and those in thenursing profession generally and specifically thestaff in the Nursing and Midwifery Planning andDevelopment Unit led by Ms. Nora Irwin O’Rourkeand the project leader of this initiative, Ms. MarieCasey.
John O’BrienHospital Network ManagerHSE Mid-Western Area
Strategy & Action Plan for N
ursing & M
idwifery
3
Forewordby John O’Brien

Introduction
and Methodology

1.0 INTRODUCTIONThe emerging reform programme represents the biggest change process ever undertaken in the state. Nursesand midwives recognise the need to engage actively in the Health Service Reform Programme (HSRP, 2004)and lead the professional development of nursing and midwifery based on healthcare objectives.
This document is a strategy for nursing and midwifery in the Acute Hospital Services in the HSE Mid-WesternArea. The strategy provides a shared vision and framework to develop nursing and midwifery practice acrossthe region in order to respond and further contribute to the changing needs of patients in acute hospitals. Itsdevelopment commenced in 2004.
This strategy is built upon the aims of the Health Strategy (2001) and the Strategy for Acute Hospital Services,Mid-Western Region (2002) and the Health Service Reform Programme (2004).
1.2 METHODOLOGYThe strategy was informed by a literature review of national health and nursing and midwifery policy driversand documents.
Feedback from consultation with 38 focus groups of nursing and midwifery staff in the acute hospitals in thisregion (Peelo-Kilroe, 2003) was utilised in drafting the strategy.
Two consumer panels within the region were consulted regarding their views on important aspects of nursingfrom their perspective. Feedback from the consultation is presented in Appendix 1.
1.3 IMPLEMENTATION AND TIMEFRAME
The timeframe of the strategy is three years. Responsibility for the development and implementation ofthis Strategy lies with Directors and Assistant Directors of Nursing and Midwifery. The Steering Grouprecognise that nurses and midwives belong to a wider interdisciplinary team and that it is only throughcollaborative working with clinical and non-clinical colleagues that the strategy will be achieved. Nursingand midwifery managers recognise the value of working as a network and sharing developments.Ongoing evaluation of the strategy will occur on a six-monthly basis.The Strategy for Nursing and Midwifery was approved by the Hospital Network Manager in May 2005.
Strategy & Action Plan for N
ursing & M
idwifery
5
1.1 STEERING GROUPIn order to develop the strategy a steering group was set up in June, 2004. The Steering Group met over aperiod of six months. The Steering Group has a membership inclusive of the six acute hospitals in theMid-Western Area:-
THE MID-WESTERN REGIONAL HOSPITAL, LIMERICKTHE MID-WESTERN REGIONAL ORTHOPAEDIC HOSPITAL, CROOM, LIMERICKTHE MID-WESTERN REGIONAL MATERNITY HOSPITAL, ENNIS ROAD, LIMERICKTHE MID-WESTERN REGIONAL HOSPITAL, ENNIS, CO. CLARETHE MID-WESTERN REGIONAL HOSPITAL, NENAGH, CO. TIPPERARYST. JOHN’S HOSPITAL, LIMERICK

Vision and Action Plan

Vision StatementIt is our vision that the nursing and midwifery profession will be leaders in influencing the
delivery of quality, person inclusive nursing and midwifery acute services in the HSE Mid-
Western Region.
Care will be evidence-based, holistic, responsive to change and will reflect demographic
needs.
Nurses and midwives will be enabled to meet their potential in their professional and legal
responsibilities within the Scope of Nursing and Midwifery Practice Framework.
The vision is underpinned by the core values of mutual respect, dignity and justice in
collaboration with all stakeholders.
Key Themes
1) CLINICAL GOVERNANCE
2) LEADERSHIP
3) PROFESSIONAL DEVELOPMENT OF NURSING AND MIDWIFERY
4) FUNDAMENTAL NURSING CARE
5) LEARNING AND DEVELOPMENT
6) IMPROVING WORKING LIVES
Nursing and Midwifery workforce planning is an integral component of each of the above.
Strategy & Action Plan for N
ursing & M
idwifery
7

Theme 1: Clinical GovernanceTo support the provision of high quality patient care, we will have a Nursing andMidwifery foundation to underpin the use of a clinical governance framework
• Collaborate with other disciplines to develop a clinical governance framework for acuteservices regionally
• Develop an implementation plan for rolling out the framework across the region
• Standardise nursing and midwifery job descriptions across the region in the acute services
• Staff will have the appropriate information to help them understand their roles andresponsibilities within clinical governance
• Collaborate with patients and carers to ensure that they are at the center of our serviceprovision
• Develop the skills and knowledge of the nursing and midwifery workforce to ensurecompetence to deliver a high quality, measurable care
• Ensure that our practice is underpinned by evidence, research and audit
Specific plans for Clinical GovernanceObjective Completion Lead Critical Success
Date Responsibility Factor/s
1.1Influence the development of a clinical January 2006 DONS of the Inter-disciplinarygovernance model which underpins the pillars region and partnershipof governance within the Acute Hospital Strategy workingfor the HSE Mid-Western Region
1.2Clinical Governance awareness sessions will be December 2006 MCprovided to Nursing and Midwifery staff in allacute hospitals in the region.
1.3To develop a booklet / leaflet on clinical July 2005 JSM / MOBgovernance for all staff
1.4Accreditation process to continue, including Ongoing All managers Cooperation ofAn Bord Altranais recommendations to develop MWRHs multi-disciplinarysystematic documentation teams in
collaboration withthe AccreditationManager
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
8

Objective Completion Lead Critical SuccessDate Responsibility Factor/s
1.5Audit: Develop Nursing Forum for systematic December 2005 Nursing Managementprocesses of MWRH
1.6Staff who have an audit role will attend clinical May 2005 DONS/ADONs This applies audit training. especially to CNSs/
CMSs & ANPs/AMPs
1.7That the patient will be included as a partner in Ongoing All nurses andplanning their care, either independently or with midwivesthe help of family and significant others.
1.8Development and implementation of clinical care Ongoing Multi-disciplinary Cooperation ofpathways to improve the patient experience working multi-disciplinary
team
1.9Each hospital will conduct focus groups on key December 2006 All DONs andaspects of service delivery with patients. ADONs
1.10Develop a regional committee for the October 2005 GK Nominations by development of Clinical Policies and Procedures DONs across thei.e. one committee where all clinical policies regioncome through and are signed off.
1.11Work with the Research Officer to promote nursing As soon as Research NMPDU & Wholetimeand midwifery research across the network. Officer is appointed DONs/ADONs equivalent
1.12Have a speaker on Clinical Governance at the April 2005 NMPDUNMPDU conference in April 2005.
1.13Produce a newsletter on Governance to be May 2006 MOBdisseminated to all staff at three monthly intervals
1.14Clinical supervision process in place for ADONs, December 2005 DONS, ADONsCNM3s, and CNM2s in MWRH, Dooradoyle, and MCMaternity, Nenagh, St Johns and RegionalOrthopaedic Hospital, Croom by the end of 2005
1.15Develop a guideline for the implementation of December 2005 DONs, ADONsclinical supervision in acute sites. and MC
1.16Clinical supervision rolled out to all sites December 2007 DONs/ADONs
1.17Develop standarised job descriptions for all Collaborationgrades of nursing and midwifery, identifying with keycore competencies for each role (except for Group stakeholdersANP/AMP and CNS/CMS) KC
- Health Care Assistant September 2005 NK- Staff Nurse / Midwife January 2006 GK
MCMOD
- Clinical Nurse / Midwife Manager One March 2006- Clinical Nurse / Midwife Manager Two September 2006
Group 2- Clinical Nurse / Midwife Manager Three September 2005 BM / JSM
PCCL
- Assistant Director of Nursing / Midwifery December 2005 MFCH
- Director of Nursing /Midwifery June 2006
Strategy & Action Plan for N
ursing & M
idwifery
9

Theme 2: LeadershipIn order to engage effectively with other professions and disciplines, Nurses andMidwives will be confident in their roles as clinical leaders and to achieve this wewill:
• Create an awareness of the leadership role of all nurses and midwives
• Promote and expand nursing and midwifery led services and practice in the interests ofpatients
• Implement nursing and midwifery Advanced Nurse/Midwife Practitioner posts
• Collaborate with interdisciplinary teams to optimize the contribution of all members of theworkforce to meet the needs of the patient
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
10

Specific plans for LeadershipObjective Completion Lead Critical Success
Date Responsibility Factor/s
2.1 Deliver six LEO programmes to management staff December 2005 MC & LPK Availabilityfrom all six sites by the end of December 2005 of trainers
2.2Deliver leadership awareness sessions to staff at December 2005 Allall levels on each site by the end of December 2005 DONs/ADONs
2.3 Release of ProjectFour sites developed for the establishment of December 2005 DONs /ADONs Persons to prepare ANP/AMP roles and MC sites and Inter-
disciplinarycollaboration
2.4Midwifery led discharges in place by June 2005 June 2005 ADONs @ MWRMHMidwifery led admissions in place by December 2005 December 2005 ADONs @ MWRMH
2.5Ensure that leadership and management See job description ADON/DON expectation are clearly defined within job section in clinical groups workingdescriptions and person specifications governance section on job descriptions
2.6 Funding for postsFour ANPs/AMPs in post by December 2006 December 2006 DONs and ADONs through the service
from prepared sites planning process
2.7 Release of ProjectFurther site development for ANP/AMP by December 2006 DONs and ADONs Persons to prepareDecember 2006 sites
2.8Six LEO programmes run for staff and managers December 2006 MC & LPK As abovefrom all sites by the end of December 2006
2.9 Collaboration of theNurse-led Warfrin Clinic in Ennis by December 2006 December 2006 DON/ADON from multi-disciplinary
MWRH Ennis team
2.10Introduce D.O.M.I.N.O. community-based December 2006 ADONs @ MWRMHmidwifery service by 2006.
2.11Deliver leadership awareness sessions on December 2006 All DONsall sites by December 2006 and ADONs
2.12ANP/AMP posts in place in Ennis and Nenagh December 2008 DONs Ennis andby the end of 2008 Nenagh
2.13Six LEO programmes delivered during 2007 December 2007 MC & LPK A/A
Strategy & Action Plan for N
ursing & M
idwifery
11

Theme 3: Professional Development of Nursing and Midwifery
Nurses and midwives will be enabled to reach their potential in their professionaland legal responsibilities within the Scope of Nursing and Midwifery PracticeFramework in order to respond to patient need
• Develop methods for the practical application of job descriptions to the person’s role
• Identify the support structures that need to be in place to enable staff to develop and fulfilltheir roles in meeting the needs of the service users
• A competency-based approach is adopted to facilitate role development
• Share developments and innovations throughout the network
• Ensure our education and training provision serves the future needs of the service and theindividual nurse / midwife
Specific plans for Professional Developmentof Nursing and Midwifery
Objective Completion Lead Critical Successdate Responsibility Factor/s
3.1To develop a competency based document June 2006 MC and alloutlining the competencies required to work in Divisional Nurseeach clinical area / Midwife Managers
in each acutehospital
3.2Support the development of clinical practice All DONs/ADONs/ Collaboration withwithin the acute Nursing and Midwifery services supported by key partners throughas identified in the report ‘An Explorative Study NMPDU, CNE, the partnershipinto the Expansion of Nursing and Midwifery and processProfessional Roles’, (Lorna Peelo-Kilroe, June 2003). NPDU, MWRH- Cannulation Multi-disciplinary- Phlebotomy developed protocols/- Administration of first dose of intravenous policies (e.g. Drugs
antibiotic and Therapeutics)- Catheterisation Ongoing
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
12

Objective Completion Lead Critical Successdate Responsibility Factor/s
- Insertion of fine bore NG tubes- Defibrillation Resuscitation Dept.- and other roles considered appropriate (NPDU, MWRH)
3.3Produce a report that identifies what resources January 2006 All DONs/ADONswould be required to implement identified services.
3.4Identify areas where CNS / CMS and ANP /AMP Ongoing DONs/ADONs Utilisation ofposts are required and secure funding through Director of National Councilthe service planning process N.M.P.D.U. criteria
3.5Prioritise admission to training programmes for Ongoing All Nurse /clinical areas whose need is greatest Midwife
managers
3.6Funded protected time for Ward Managers June 2007 All DON/ADON Wholetimespecifically related to staff development including via the Service Equivalentpreceptorship, mentorship and competency Planningidentification and development. processDedicated Senior HR post additional to anddedicated to Nursing Management.
3.7On-going commitment to the development of 2005 Phase 1 N.M.P.D.U.Post Graduate programmes for nurses 2006 Phase 2 ULand midwives CNE
DONs
3.8Provide workshops to enable nurses and midwives to January 2006 N.M.P.D.U.explore the concept of delegation and increase CNEqualified nurses’ and midwives’ knowledge of ADONs/DONsaccountability in relation to delegation andsupervision of health care assistants.
3.9Clinical Supervision pilot sites to be evaluated September 2005 MC
DONs/ADONs
3.10Ensure that Personal Professional Portfolio January 2005 MCdocuments are available to all staff locally
3.11Annual Orthopedic Conference Ongoing KC
3.12Annual NMPDU Conference Yearly NMPDU
Strategy & Action Plan for N
ursing & M
idwifery
13

Theme 4: Fundamental Nursing CareThe essentials of care are acknowledged by all nurses and midwives as thecornerstone of their clinical practice
• Ensure that fundamental care is valued by all nurses and midwives, by use of a framework
• Ensure evidence based practice underpins all quality nursing and midwifery care
• Ensure all qualified nurses and midwives deliver high standards of care and act as rolemodels
• The contributions of health care support workers will be supported by nurses and midwives
• Adopt a tool for evaluating the appropriate skill mix which will allow optimum care to bedelivered safely
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
14

Specific plans for Fundamental Nursing CareObjective Completion Lead Critical Success
Date Responsibility Factor/s
4.1 - Adopt the Essence of Care as a benchmarking KH Support from
framework for best practice in nursing care Corporate and develop a strategy for implementing it Management across the region. N.M.P.D.U.
Funding to- Begin process implement the
by October 2005 framework.and then publish Time implications fortimeframe staff to facilitate it.
Administration staffto support it.Practice DevelopmentCo-ordinator to leadthe initiative.
4.2Midwifery led postnatal discharge of low risk women June 2005 NK & MQ
4.3Midwifery led admissions of low risk women December 2005 NK & MQ
4.4FETAC Level 2 Courses for Health Care Assistants Ongoing CNE continues to be rolled out.
4.5Develop a register of Care Plans and Integrated November 2005 GK Information suppliedCare Pathway documents that are in use in all by ADONs/DONs hospitals in the region across the service
4.6Pursue the implementation of a staff: patient December 2006 GK & NK Funding anddependency evaluation tool support from
CorporateManagement
Introduce hard copy user-friendly tool in MWRH October 2005 GK Support of pilot areas DONs/ADONs
Strategy & Action Plan for N
ursing & M
idwifery
15

Theme 5: Learning and DevelopmentNurses and midwives will be enabled to develop in order to respond to patientneed through education, training and practice development
• Nurses and midwives will be supported to take responsibility for their own developmentthrough Personal Development Planning (PDP)
• Develop a method of aggregating outcomes of PDP’s into the organisational training anddevelopment plan
• Collaborate with internal and external agencies involved in education provision to maximiselearning and development of staff appropriate to changing health care requirements
• Evaluate, review and develop learning and education to ensure consistency andtransferability of skills and qualifications
• Develop a standard to ensure that all learning opportunities are maximised for theorganisation and the individual
• Support the development of nurses / midwives towards achieving the required competenciesby providing appropriate development opportunities
• Ensure that learning and development is aligned with service need
Specific plans for Learning and DevelopmentObjective Completion Lead Critical Success
Date Responsibility Factor/s
5.1Individual nurses and midwives, supported Ongoing All / ADOMsby their line managers, will continue to take / ADONsresponsibility for their own professionaldevelopment in line with the demands oftheir clinical roles
5.2To encourage staff to participate in the December 2005 All / ADOMs HR Department &PDP process by increasing their awareness / ADONs Corporate Learningthrough information sessions. & Development (CLAD)
and ADONs / DONs / ADOMs support
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
16

Objective Completion Lead Critical Success Date Responsibility Factor/s
5.370 CNSs provided with information on January 2005 ADONs / MC Support of CLADutilising the PDP process
5.4Each site will have at least one person December 2005 All DONs and ADONs Support of trained as a PDP facilitator by the end of from each site Corporate &December 2005 Learning &
Development Department
5.5Support and grow the culture of learning, supervision Ongoing NPDUs, CPCs Effectiveand competency assessment for undergraduate student DONs/ADONs partnershipnurses/midwives by supporting nurses and midwives with HEIsto undertake Teaching and Assessing and Competency and staffAssessment of student practice. support onClinical Learning Environment audits annually Annually NPDUs, CPCs clinical sitesin partnership with HEI (UL)
5.6Direct entry to midwifery training September 2006 Mid-Western
Regional MaternityHospital and Tutors
5.7Masters in Midwifery education to be September 2005 NMPDU &available for staff in the region MWRMH
5.8Develop a standard for identifying, February 2006 CL & MC Support of CLAD &planning, implementing and evaluating Centre for Nurseeducation and training for all nurses and Educationmidwives within acute hospital services.
5.9Provision of in-service onsite training and Ongoing All sites - DONs,development for staff using a variety of methods, ADONs and allincluding E-Learning, Study Clubs, Journal Clubs, nurse managementAction Learning and Learning Laboritories. to organize.
5.10To secure funding for Practice Development January 2006 All sites - DONs, WholetimeFacilitators who would lead and innovate ADONs Equivalentpractice through the service planning process.
5.11Work with the CNE to ensure that the FETAC CNEProgramme is meeting service need and is Ongoing DONs/ADONssupported by adequate mentors
Strategy & Action Plan for N
ursing & M
idwifery
17

Theme 6: Improving Working LivesThere would be an ethos of mutual respect, equity, dignity and justice within theorganisation
• Develop an awareness of what respect, dignity and justice will mean in peoples workinglives
• Nurse and Midwives are valued by the organisation
• The organisation will support Nurses and Midwives in carrying out their professional rolesand responsibilities
Specific plans for Improving Working LivesObjective Completion Lead Critical Success
Date Responsibility Factor/s
6.1Ensure that all Staff are provided with onsite Ongoing HR DepartmentAwareness Sessions with regard to D.O.H.& C. and ADONs /publications in relation to dignity, equity DONs.and are enabled to attend.
6.2Ensure management practices are in line with the Ongoing HR All Nurse & Midwife Grievance Procedure and Dignity at Work included managers attendin People Management – The Legal Framework. the programme
6.3Ensure that Clinical Supervision continues to be Phase 1 MCrolled out from A.D.O.N.’s – to all CNM2’s and June 2005 DONs / ADONsCNM1’s. This incorporates reflective analysis, CNE values staff through listening and support, andpromotes mutual respect and dignity.
6.4Review of absence and sickness policy with a December 2006 DONs / ADONsview to reducing the absence and sickness level,ensuring that the policies are in line with theHSEA document, ‘People Management – TheLegal Framework’.
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
18

Objective Completion Lead Critical SuccessDate Responsibility Factor/s
Nursing and Midwifery Workforce Planning
6.5.1• Work with the Resource Officer to raise the Ongoing ADONs / DONs Integrated
profile of nursing and midwifery as a career With Resource workforcechoice among school leavers, mature persons Officer in planningand support workers through the career collaborationframework with HR and
Recruitment Officers
6.5.2• Each hospital will plan the Nursing and
Midwifery workforce requirement utilisingthe service planning process, PPARS and theAnnual Nursing and Midwifery Turnover Report
6.5.3• Work with the Resource Officer to develop
opportunities for mature students and supportworkers to enter nurse and midwifery training
6.5.4• Recruit and retain nurses of the highest
standard using a competency framework
6.5.5• Ensure that all nurses and midwives attend
a comprehensive induction programme andare aware of mandatory training requirements
6.5.6• Utilise evidence from exit interviews
6.5.7• Plan and monitor demand forecasting for
qualified nurses and midwives incollaboration with the Resource Officer,including the implications of the transitionto a graduate profession
6.5.8• Provide opportunities to encourage nurses
and midwives to re-enter the workforcethrough providing return to practice courses
6.5.9• Continue to run overseas orientation courses
twice a year
6.6Develop an awareness strategy on the values and June 2007 All Nurses /dignity of nurses in support of their roles as patient Midwifery Staffadvocates.
Strategy & Action Plan for N
ursing & M
idwifery
19

Literature Review

3.1.1
Quality and Fairness: A Health Systemfor YouThe Health Strategy isparticularly relevant to thedevelopment of nursing andmidwifery services, whichcomprise the largest groupof staff in the health service.Nurses and midwives facethe challenge of embracingnew methods of caredelivery that will provide aquality service that is truly people-centred – anapproach that underpins the current HealthStrategy (National Council, 2003a).
This strategy is underpinned by the principles putforward to support the vision of the HealthStrategy: Quality and Fairness:-• Equity and fairness• A people-centred service• Quality of care• Clear accountability.
Framework for reform of acute hospitalsThe Health Strategy: Quality and Fairness (2001)identified six major frameworks for change. Reformof the acute hospital system was one of theframeworks.It stated that• Co-operation between hospitals needs to be re-
inforced so that a fully integrated system isachieved.
• Minor injury units will be established in A & EDepartments
• Chest pain clinics, respiratory clinics will be usedto fast track patients as appropriate
• Advanced Nurse Practitioners (ANPs) will be
appointed in acute hospitals. ANPs diagnose andtreat certain groups of patients independentlywithin protocols agreed with the interdisciplinaryteam.
• Chronic disease management protocols topromote integrated care planning and supportself-management of chronic disease will bedeveloped.
Framework for Developing HumanResourcesThe Framework for Developing Human Resources(Quality and Fairness, 2001)An objective of the framework for developinghuman resources is to develop and explicitly valuestaff at all levels of the health system, which in turnwill benefit service users.• Best practice in recruitment and retention will be
promoted. This includes initiatives such asflexible working and training, arrangements foratypical working hours and specific family-friendly approaches will be aimed at meeting theneeds of health service workers and theirfamilies as well as efficiency of the service.
• Greater inter-disciplinary working betweenprofessions will be promoted to facilitateintegrated and holistic care.
• Creation of a detailed Action Plan for PeopleManagement in the Health Services (APPM) tobe developed jointly between management,trades unions and partnership structures. TheAPPM was launched in 2002. The plan addressesseven important themes identified in Quality andFairness.
3.1.2
Health Service ReformProgramme (2003)One of the six frameworks for change in the healthstrategy is organisational reform. The reformprogramme incorporates recommendations of two
Strategy & Action Plan for N
ursing & M
idwifery
21
3.0 THE POLICY CONTEXTCurrent health policy has informed the development of the strategy with respect to theirimplications for the development of nursing and midwifery care.
3.1 NATIONAL POLICY DRIVERS

reports, the Commission on Financial Managementand Control Systems in the Health Service (BrennanReport) and the Audit of Structures and Functions inthe Health System (Prospectus Report) (Departmentof Health and Children, June 2003).
The Health Services Executivewas established on 1stJanuary, 2005. This body ischarged with managing thehealth service as a singlenational entity and isaccountable to the DOH&C.The three tenets of theHealth Service Executive areto provide:-• Better quality services to patients, clients and
service users• Better working conditions for staff• Better value for money for the tax payer
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
22
National Hospitals OfficeA key element of the Reform Programme isthe establishment of a National HospitalsOffice (NHO), a Primary, Community andContinuing Care Directorate (PCCC) and aNational Shared Services Centre (NSSC)within the Health Service Executive (DOH&C,2004).
The NHO is responsible for ensuring hospitalservices are integrated with the wider healthsystem. The NHO will be responsible forensuring acute sector delivery on nationalhealth strategies (e.g. Cancer, Cardiovascular,etc).
The re-organisation of the acute hospitals willbring all 52 statutory and non-statutory acutehospitals into a single unified structure. Therewill be significant emphasis on integration ofhospital services with primary, communityand continuing care (PCCC) focusing on theneeds of individuals, their families andcommunities at local level. The NHO will beresponsible for ensuring that each hospitalnetwork provides an integrated service (HSRP,2004).
The six acute hospitals in the Mid-West Areawill be managed as a regional network.
10 Hospital Network Managers
Assistant Directorof Quality, Risk and
Customer Care
Assistant Directorof
Planning
Assistant Directorof Contracts andUtilisation Review
Assistant Directorof
Ambulance Services
DirectorNHO
NHO STRUCTURE
Health Service Executive, 2004
Group 1
Waterford Regional
St. Lukeʼs GH Kilkenny
Wexford General
South Tipperary GH
Group 2
CUH
Erinville
St. Maryʼs Ortho.
Mallow
Tralee
Bantry
Mercy
S. Infirmary
Group 3
Lourdes Drogheda
Louth County
Cavan General
Monaghan General
Our Ladyʼs Navan
Group 4
Sligo General
Letterkenny General
Group 5
Galway University
Merlin Park
Mayo General
Roscommon County
Portiuncula
Group 7
LimerickReg.LimerickMat.CroomOrtho.EnnisHosp.NenaghHosp.St. JohnʼsLimerick
Group 8
St. Vincentʼs
St. Michaelʼs
Columcilleʼs
Holles Street
Hume Street
St. Lukeʼs
Eye & Ear
Group 9
St. Jamesʼ
Tallaght
Naas
Coombe
Crumlin
Group 10
Mater Hosp.
Beaumont
JCMH
Rotunda
Cappagh
Temple St.
Group 6
Mullingar General
Tullamore General
Portlaoise General

Report of theNational Task Forceon Medical StaffingThe National Task Forceon Medical Staffing wasestablished in February2002 by the Minister forHealth and Children.Its purpose was to fulfilthree key requirements:-
1. To devise an implementation plan for reducingsubstantially the average working hours ofnon-consultant hospital doctors (NCHDs) tomeet the requirements of the EuropeanWorking Time Directive (EWTD)
2. To plan for the implementation of a consultant-provided service, and
3. To address the medical education and trainingneeds associated with the EWTD and the moveto a consultant-provided service.
The task force examined two regions, the EastCoast Area Health Board and the Mid-WesternHealth Board regions and focused on acute hospitalcare.
Key messages included:• The priority must be to provide a safe, high
quality service to all patients at all times.• In the two pilot regions studied, acute hospital
services should be delivered by an integratedregional network of hospitals which should be asself-sufficient as possible, currently servingpopulations of about 350,000. Each hospital inthe network should form part of a closelyintegrated system of regional and national carefor patients, in which primary care, othercommunity care services and continuing care arefully linked. A small number of more specialistservices should continue to be provided on asupra-regional or national basis.
• Health professionals should work as part of amulti-disciplinary team.
Implications of the Task Force’s workfor the development of Nursing andMidwifery.A group chaired by the Chief Nursing Officer of theDepartment of Health and Children considered theimplications of the Task Force’s work for thedevelopment of nursing and midwifery. Findingswere published in two reports:-
• The Challenge for Nursing and Midwifery:A Discussion Paper (DOH&C, 2003)
• An Explorative Study into the expansion ofNursing and Midwifery Professional Roles inresponse to the European Working Time Directive(MWHB, Peelo-Kilroe, 2003).
Where nurses and midwives expand their roles, thiswould be within a framework of nursing/midwiferycare. The fundamental aspects of nursing/midwiferymust be retained and role expansion must centrearound patient/client needs (National Council,2003a).
The findings of the two reports are presented laterin the section on Professional Development.
Strategy & Action Plan for N
ursing & M
idwifery
23
3.1.3
Strategy for Acute Hospital Services,MWHB, 2001The Acute Care Strategy recommends that thesix hospitals in the Mid-Western region shouldfunction as a region wide service network.Principles on which to base services identifiedwere:• Patient centred services, which
are accessible to the populationof the region without compro-mising safety, quality and clinicalstandards
• Clinical practice and care basedon the most up to date evidence
• Co-operation and clinical net-working between hospitals tomaximise outcomes, particularly wherespecialist or complex inputs are required
• Co-operation in planning and care provisionwith primary, community and non-acutesystems
• A service underpinned by Quality, RiskManagement, Clinical Governance, Audit, stafftraining, education and development and con-tinuous assessment, evaluation and review.
FINDINGS3.2.1
The Report of the Commission onNursing, published in 1998, put forward a framework for thefurther development of nursing and midwifery,emphasising that nursing and midwifery wereamong the cornerstones of the Irish health service.
National Council for the ProfessionalDevelopment of Nursing and MidwiferyThe Commission on Nursing recommended theestablishment of a National Council for theProfessional Development of Nursing andMidwifery (National Council) to give guidance anddirection in relation to the development ofspecialist nursing and midwifery posts and post-registration educational programmes offered tonurses and midwives.
The National Council for the ProfessionalDevelopment of Nursing and Midwifery ‘exists topromote and develop the professional roles ofnurses and midwives in order to ensure the deliveryof quality nursing and midwifery care topatients/client in a changing healthcareenvironment’ (National Council Mission Statement).
3.2.2
Clinical career pathwayThe creation of meaningful and rewarding clinicalcareer pathways was one of the most importantrecommendations to emerge from the Commissionon Nursing (National Council, 2001).
With the establishment of the National Council forthe Professional Development of Nursing andMidwifery in 1999, the clinical career pathway forthe general nurse (from Staff Nurse/Midwife toClinical Nurse/Midwife Specialist to AdvancedNurse/Midwife Practitioner) was formalised.
3.2.3
Generalist nursesGeneralist nurses provide the majority of care andincreasingly work in specialist areas and / orexpand their roles. They comprise the largest groupof health service workers and as such have greatpotential to further contribute to population health,achieve the goals of the national health strategyand to support the implementation of the healthservice reform programme.
The National Council for the ProfessionalDevelopment of Nursing and Midwifery (2003a)advocates a competency-based approach to the
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
24
3.2 Nursing and Midwifery in Ireland:
KEY NURSING AND MIDWIFERYPOLICY STATEMENTS
Report of the Commission on Nursing, 1998.Effective Utilisation of the Professional Skillsof Nurses and Midwives, 2001.Agenda for the Professional Development ofNursing and Midwifery, National Council, 2003The Challenge for Nursing and Midwifery:Discussion Paper, DOH&C, 2003.Explorative Study into the Expansion of Nursingand Midwifery Professional Roles in response tothe European Working Time Directive, (Peelo-Kilroe, N.M.P.D.U., Mid-Western region, (2003).

professional development of generalist nurses,which allows for the development andenhancement of roles.
Role expansion, not extension, needs to occur tosupport holistic approaches to care management(National Council, 2003a).
In the consultative process for the Agenda for theFuture Development of Nursing and Midwifery(2003a), a recurring theme was the need for actionin developing, supporting and valuing the role ofthe generalist nurse and a need to give particularattention to medical and surgical nurses. Generalnurses identified that they wanted continuingprofessional development (CPD) which enhancedtheir clinical skills.
Novice to ExpertStudies have demonstrated that nurses move alonga continuum from advanced beginner, competent,proficient to expert (King and Clarke, 2002: Loganand Boss, 1993; cited in Agenda for the ProfessionalDevelopment for Nursing and Midwifery, 2003a).
Generalist nurses should be supported to developskills and gain experience, so that they can progressfrom novice to expert in their area of practice, andhave opportunities for CNS/CMS and ANP/AMP roletransition (National Council, 2003a). Clinical /professional supervision facilitates this process.
Competency DevelopmentThe identification of core competencies for a clinicalarea and orientation to an area involves thedevelopment of these competencies by use ofmentorship, portfolios and competencydevelopment (National Council, 2003a). In addition,it was suggested that CPD for generalist nursesshould include management development training(National Council, 2003a).
The National Council for the ProfessionalDevelopment of Nursing and Midwifery published areport in 2004 which reviews the activities of staffnurses and staff midwives in relation to continuingprofessional development.
The Scope of Practice for Nursingand MidwiferyIn the Review of Scope of Practice for Nursing(An Bord Altranais, 2000) the views of nurses and
midwives were sought ontheir current role and scopeof practice. As part of thestudy, nurses and midwivesdescribed nursing as aservice with caring asits core function. Thefocus of general nursing wasdescribed as patient-centred care facilitatedthrough a locally interpreted model of nursingto aid clinical decision-making.
The Review of Scope of Practice for Nursing (AnBord Altranais, 2000) also identified non-nursingduties as clerical, portering and general work thatdetracted from what was seen as ‘core caring’nursing functions.
The report of the working group on the EffectiveUtilisation of Professional Skills of Nurses andMidwives (DOH&C, 2001) stated that ‘there is nosubstitution for the skilled expertise of the qualifiednurse who must remain central to the assessment,planning, implementation and evaluation ofpatient-care and to the supervision and delegationof all activities related to patient-care.
The changes in population, and the health needs ofthe nation have all challenged general nursing. Thepopulation of Ireland continues to increase, thebirth rate is rising, life expectancy increasing, olderpeople will form a larger portion of the totalpopulation and migration will result in a multi-ethnic and culturally diverse client base.
Skill mix The nursing profession needs to examine skill mix,measure levels of patient dependency and reviewclinical skills and competencies in order to respondto the changing demographic and epidemiologicalpicture (National Council, 2003a).
Strategy & Action Plan for N
ursing & M
idwifery
25

Framework for MidwiferyMidwifery practice is underpinned by values thatguide the way in which midwives deliver care (AnBord Altranais, 2001). The focus of midwiferypractice is pregnant women and their families anddelivery of woman-centred maternity services.Midwives in Ireland have a role to play inmaintaining the normality of pregnancy and birthand promoting the philosophy that pregnancy andbirth are normal physiological events within thewider context of women’s lives (National Council,Agenda for Professional Development, 2003a).Midwives need to recognise and overcome thebarriers to providing women with alternatives tomedicalised care, i.e. lack of acknowledgement ofthe role of the midwife within private insuranceschemes, maternity services policies not informedby evidence-based research or by bodies such asthe World Health Organisation, lack of collaborationamong professionals in the maternity services andfailure to recognise midwives as professionalscapable of and responsible for the safe andeffective care of healthy pregnant women (NationalCouncil, Agenda for Professional Development,2003a).
In order to sustain and build on the existing modelsand potential of maternity care, midwives mustwork in partnership with women, and with otherrelevant professionals, to help ensure a qualityservice and a wider choice of care options forwomen and their families throughout the country.The community role of the midwife needs to beenhanced and more midwife-led antenatal clinicsdeveloped. Midwives should be involved in policyformulation, service review and planning.
The Health Strategy (DOH&C, 2001) recommendedthe increased involvement of midwives in themanagement and delivery of maternity services.
Professional and practice development of midwiferyrequires effective management and leadership. Theroles of midwives and midwife managers need tobe clarified and levels of authority established(National Council, Agenda for ProfessionalDevelopment, 2003a).
The National Council has funded the post ofMidwifery Practice Development Co-ordinator forthe Mid-Western Area. The Practice DevelopmentCo-ordinator took up the post in October, 2004.
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
26
3.2.4
Student Nurses / Midwives andNewly-QualifiedNurses There is a need to support and develop nursing/ midwifery staff in a clinical area to whichstudent nurses and midwives are assigned. It isimportant that staff in these clinical areas areaware of the needs of students and aresupported in ensuring that students obtain abeneficial educational outcome from theirclinical placement (Commission on Nursing,1998).
Student nurses / midwives need a supportiveenvironment for academic skills to betransferred to direct patient-care.
These types of learning and supportopportunities are also believed to contribute toretaining nurses within the profession, assist-ing students to make the challenging transitionfrom the academic to the clinical setting(Canadian Nursing Advisory Committee, 2003).
Newly-qualified nurses / midwives needsupport also in the form of preceptorship tomake the transition from student to staff nurse/ midwife.

3.2.5
Clinical Nurse and Midwife Specialists The Commission on Nursing(1998) recognised thatpromotional opportunitiesshould be open to nursesand midwives wishing toremain in clinical practiceand accordingly recommend-ed a clinical career pathwayleading from registration toclinical specialisation and toadvanced practice. The development of this careerpathway serves to develop clinical nursing andmidwifery expertise in the interests of holism andexcellence in patient/client care (National Council,2004).
The definition of clinical nurse/midwife specialist asoutlined by the National Council is as follows:
The CNS/CMS is in a key position to contribute tothe successful implementation of the health servicereforms (National Council, 2004c). CNSs/CMSs willsupport the implementation of national healthpolicy, in particular the national health strategyQuality and Fairness: A Health System for You(DOH&C, 2001) and the Report of the NationalTask Force on Medical Staffing (DOH&C, 2003).The Report of the National Task Force on MedicalStaffing concludes that the CNS/CMS role is alreadywell defined and is in keeping with the Task Force’sconcept of utilising the skills of professionals tobest effect.
CNSs/CMSs have an important role in providingspecialist knowledge and skills; but they needongoing support from their managers and medicalcolleagues and they require real opportunities toparticipate in continuing professional development(National Council, 2004c).
Role Resource Packfor CNSs/CMSsA Role Resource Pack forCNSs/CMSs was developedby the SEHB in 2003 (fundedby the National Council).This pack is available to allCNSs/CMSs nationally.
Strategy & Action Plan for N
ursing & M
idwifery
27
A nurse or midwife specialist in clinical practicehas undertaken formal recognised post-regis-tration education relevant to his/her area ofspecialist practice at higher diploma level. Suchformal education is underpinned by extensiveexperience and clinical expertise in therelevant clinical area (National Council, 2004c).
THE FIVE CORE CONCEPTS INHERENT INTHE ROLE OF CLINICAL NURSE/MIDWIFESPECIALIST AS DETERMINED BY THENATIONAL COUNCIL ARE:
• CLINICAL FOCUS• PATIENT ADVOCATE• EDUCATION AND TRAINING• AUDIT AND RESEARCH• CONSULTANT
Marlo Kearney (MediSense),Dr. Ned Barrett (PrincipalClinical Biochemist), Pat Barron (DiabetesClinical Nurse Specialist),Nurse Ann Quinn and SarahFitzpatrick (Diabetes ClinicalNurse Specialist) examiningthe new point-of-careglucose testing system.

Following application by nurse and midwifemanagers in this region, the National Councilprovided funding for management developmentprogrammes for 75 CNSs/CMSs within this region.The programme was further supported bypresentations to CNSs/CMSs and nurse and midwifemanagers by Ms. Jenny Hogan, ProfessionalDevelopment Officer, National Council and Ms. JoanGallagher who led the project on the developmentof the role resource pack.
Evaluation of the role of CNSs/CMSsAn evaluation of theeffectiveness of the rolewas carried out in 2003(National Council, 2004c).Findings indicated that thereis overwhelming support forthe effectiveness of the roleof clinical nurse/midwifespecialist.
Patients’ responses were predominantly and warmlypositive when asked to comment on how the role ofthe CNS/CMS affected their care. They saw theCNS/CMS as a true professional and an expert inthe clinical field. The key role of the CNS/CMS wasperceived as that of a translator and an educator.Patients also had the perception that the CNS/CMSacted as a conduit through which all of theirhealthcare was organised, for example the diabeticCNS/CMS not only managed the diabetes aspect ofcare but co-ordinated other aspects of patient care.
All patients had had excellent experience of andreaction to the role. They agreed that the CNS/CMSco-ordinated their healthcare pathway. The feelingof confidence that the CNS/CMS inspired ‘rubbedoff’ on them and gave them a feeling of overallconfidence in their treatment and the decisionsabout their care options.
Development of the role of AuditThe research findings indicated that audit andresearch are the least well developed aspects of thecore concepts of the CNS/CMS role. The reportrecommends that the audit role of the CNS/CMS bemade more explicit when job descriptions are beingprepared and managerial feedback to the CNS/CMSshould include discussion around audit techniques.The report recommended investment in thedevelopment of audit skills. This will support clinical
governance and is in line with the Strategy forAcute Hospital Services, Mid-Western Region(2001).
Geographic distribution CNSs/CMSs roles are evolving and will continue todo so as the demand for specialisation continuesapace. Increased specialisation can be seen as apositive factor that will enhance the alreadyimportant role that nursing and midwifery plays inthe delivery of quality healthcare (National Council,2004c).
The establishment of a database of CNSs/CMSs bythe National Council facilitates examination of thegeographical distribution of CNS/CMS roles. Thenational average of CNS/CMS per head ofpopulation per health board is one per 2,584. TheMid-Western area figure is one CNS/CMS per 2,518(National Council, 2004c).
The database highlights the fact that the majority ofCNS posts in paediatrics are based in the ERHAregion. The report recommends that servicesexplore whether parents and children require localaccess to specialist services. Areas identified in the‘Agenda for the Professional Development ofNursing and Midwifery’ include such areas as painmanagement, neonatology and health promotion.
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
28

The report also recommends that otheropportunities for specialist practice be explored,e.g. areas such as critical care. A CNS role in criticalcare could support patients following transfer fromITU to general wards. Such a CNS could provide aconsultative role, lead and undertake audit, be aneducator and carry her or his own caseload(National Council, 2004c).This must occur as part of need assessment in theservice planning process (National Council, 2004c).For example, large numbers of respiratory patientsin A&E, may dictate the need for a CNS/CMS in thisarea. If a service deems that a specialist post isnecessary it is the responsibility of the localmanager to use the service planning process toseek funding and work closely with the Nursing andMidwifery Planning and Development Unitregarding the parameters of the role. One meetingper year should be dedicated to this purpose(National Council, 2004c).
3.2.6
Advanced Nurse and Midwife Practitioners(ANP/AMP)The development andenhancement of nursingand midwifery roles hasbeen recognised as anongoing and vitalcomponent of healthservice reform (DOH&C,2003) and implementationof the health strategy(DOH&C, 2001).
The development of ANP/AMP roles and services ispart of the strategic development of the overallhealth service and needs to take place in thecontext of contemporary health and social policy,the requirements of population health and theservice planning process (National Council, 2004a).
Core concepts of the ANP/AMP roleThe role combines clinical responsibilities,education, research and leadership. Advancednursing and midwifery practice is carried out byautonomous, experienced practitioners who arecompetent, accountable and responsible for theirown practice. They are highly experienced in clinical
practice and are educated to masters degree level(or higher) (National Council for the ProfessionalDevelopment of Nursing and Midwifery, 2004a).
The role offers nurses and midwives the opportunityto practice clinically at a very senior level whileproviding clinical leadership and carrying outresearch within their specialist areas of practice.Clinical leadership is about driving serviceimprovement and the effective management ofteams to provide excellence in patient care (ScottishExecutive, 2004b).
Process for establishment of ANP/AMPThe process for the establishment of an ANP/AMPservice comprises two important parts. Firstly, theservice applies to have the post approved as anANP/AMP post (Part 1. job description and sitepreparation approval). Secondly, the nurse/midwifeapplies to be accredited as an ANP/AMP to theapproved post (Part 2. individual accreditation).
Establishment of ANP/AMP in the HSEMid-Western AreaThe National Council have provided funding for sitepreparation for advanced practitioners in fourclinical areas in this region. The clinical areas are:• Bereavement and Loss• Colposcopy• Oncology• Minor Injuries, Accident and Emergency
3.2.7
Integration of Health Care Assistants intothe HealthcareEnvironment The Report of the Commission on Nursing (DOH&C,1998) identified the concerns of many nurses andmidwives at the number of non-nursing ormidwifery tasks which they were required toperform. The Commission recommended that agroup be established to ‘examine opportunities forthe increased use of care assistants and other non-nursing personnel in the performance of other non-nursing tasks (paragraph 7.63). A working groupwas established to examine the ‘effective utilisationof the professional skills of nurses and midwives’,which issued its report in May, 2001. The report of
Strategy & Action Plan for N
ursing & M
idwifery
29

the working group Effective Utilisation ofProfessional Skills of Nurses and Midwives(DOH&C, 2001) recommended that the gradeof Health Care Assistant/Maternity Health CareAssistant be introduced as a member of thehealthcare team to assist and support thenursing and midwifery function (DOH&C, 2001).
The collective views of nurses and midwives ‘is thata supervised health care assistant allows registerednurses and midwives to focus upon what they areeducated to do’ and ‘allows the registerednurse/midwife the flexibility to engage in roledevelopment through expansion associated withbecoming more expert, competent, reflectivepractitioners, developing skills to meet patients’needs (DOH&C, 2001).
When defining the role of nurses and midwives andexpanding the scope of practice, it is the registerednurse/midwife who is responsible for the delivery ofcare. The appropriate delegation to the non-professional healthcare worker should be based onthe complexity of the patient’s healthcare needs(DOH&C, 2003).
Rushforth et. Al. (1999) have cautioned that nursingmust be closely and proactively involved in ongoingdecisions about the boundaries of practice ofhealthcare assistants, carefully considering theappropriateness of each role they undertake interms of its impact on care delivery.
Recommendations of the Report on the Effective Utilisationof Professional Skills of Nurses andMidwives included:• That the nursing/ midwifery
function remains thepreserve of nurses andmidwives.
• That health care assistants engage in both direct patient care and indirect care activitiesfollowing delegation by andunder the supervision of aregistered nurse or midwife.
• That registered nurses/midwives befacilitated to explore the concept ofdelegation at local level and developappropriate guidelines.
• That a National Council for VocationalAwards (NCVA) level 2 qualification be thepreparation required for employment as ahealth care assistant.
• That registered nurses/midwives receivetraining to understand the principles ofNCVA assessment; appreciate the role ofthe health care assistant as related toNCVA criteria; and increase the qualifiednurses’/midwives’ knowledge andawareness of accountability in relationto delegation of supervision of health careassistants
Effective team communication appears as thekernel to successful utilisation of the healthcare assistant (DOH&C, 2001).
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
30

In Ireland, a national pilotprogramme to train HCAswas completed in May 2002,in conjunction with the FurtherEducation Training Awards Council (FETAC).The University of Ulster evaluated the programme.(DOH&C, 2003).
Career ladderA career ladder and opportunities to developcareers within nursing and midwifery are opento HCAs.
FETAC Programme in HSE Mid-WesternAreaFETAC Level 2 programmes are offered through theCentre for Nurse Education.In this region, nurses and midwives in acuteservices identified the need for qualified HealthCare Assistants (HCAs) who would operate underthe supervision and delegation of nurses andmidwives and would be accountable for their ownactions in accordance with the recommendations
of the Commission on Nursing (Peelo-Kilroe, 2003).Nurses and midwives are already involvedin supervising trainee HCAs undertaking theprogramme. There is a resource implication inenabling nurses and midwives to train, assess,delegate and supervise increasing numbers ofHCAs (as well as pre-registration student nurses).
3.2.8 Strategic ResponseBased on these policy initiatives, the Regional Steering Group identified sixstrategic themes as key to the future development of nursing and midwiferyservices in the region.
• CLINICAL GOVERNANCE
• LEADERSHIP
• PROFESSIONAL DEVELOPMENT OF NURSING AND MIDWIFERY
• FUNDAMENTAL NURSING CARE
• LEARNING AND DEVELOPMENT
• IMPROVING WORKING LIVES
Nursing and Midwifery workforce planning is an integral component of eachof the above.
Strategy & Action Plan for N
ursing & M
idwifery
31

Strategic Themes

Strategy & Action Plan for N
ursing & M
idwifery
33
Evidence-based clinical guidelines andprotocolsEvidence-based clinical guidelines and protocols area key feature of clinical effectiveness. Developingprotocols and guidelines collaboratively will enablenew practitioners to understand how these can helpto ensure consistent, high quality clinical standards,while allowing nurses and midwives to exerciseclinical judgement in response to the patient path-way (Scottish Executive Health Department, 2004)
Professional AccountabilityUnderpinning clinical governance is professionalself-regulation (PSR). Professional self-registrationis about exercising professional accountabilitythrough using professional knowledge, judgementand skill to apply professional standards in practice(UKCC, 1999). Practice must therefore be com-petent, up to date and based on the best availableevidence. This requires nurses and midwives tocontinuously develop their practice throughout theircareers, through lifelong learning. Effective clinicalgovernance will strengthen accountability forindividuals, teams and organisations.
The Scope of Professional Practice and the Code ofProfessional Conduct set out clearly and succinctlythe acceptable boundaries of practice. Nurses andmidwives have a responsibility to ensure theyunderstand issues of professional accountabilityas they relate to their clinical function. It is theresponsibility of each individual nurse and midwifeto understand their responsibility, accountabilityand scope of practice (An Bord Altranais, 2000).
4.1 CLINICAL GOVERNANCE
4.1.0 IntroductionOne of the four guiding principles of thehealth strategy is high performance, whichrelates to quality of care, continuousimprovement and accountability.
The Prospectus Report (2003) stated thatconsideration of accountability and perfor-mance measurement in the healthcarecontext has to take account of the clinicaldimensions of care. A strong role is envisagedfor the Health Information and QualityAuthority in reviewing the performance of thehealth service overall in order to ensure thatquality of care is promoted throughout thesystem.
Clinical governance is a framework for thequality assurance of clinical performance.Clinical governance is a ‘whole-system’process and includes all disciplines –including nurses and midwives – involvedin patient care (Prospectus Report, 2003).
Clinical governance may be defined as ‘aframework through which organisations areaccountable for continually improving thequality of their services and safegaurdinghigh standards of care by creating anenvironment in which excellence in clinicalcare will flourish (Scally and Donaldson,1998).
4.1.2
FindingsDeveloping robust clinical governance systemssuch as risk management, clinical audit andbenchmarking, accountability, research andeffectiveness and clinical guideline development,will create an environment in which roledevelopment and innovation that is focused onthe patient experience can flourish (ScottishExecutive, 2004).

34
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
Organisational culture to supportaccountabilityTo truly practice in an accountable manner, nursesand midwives need to work within organisationsthat recognise the importance of accountableprofessional practice and support its development.They need to play an active role not only indelivering services, but also in planning them. Theyneed to work within a culture in which they areencouraged to learn from their mistakes rather thanbeing punished for them, and to focus on quality bybuilding on examples of good practice (ScottishExecutive Health Department, 2004).However, clinical governance is much more thanjust setting up structures and systems. It isfundamentally about fostering an open culturethat celebrates what is done well and learns frommistakes, moving away from a culture of blame(Jones, 2001).
Involving patientsClinical governance is also about developingpartnerships with patients, involving them indecisions about their care. Nurses and midwivesneed to be involved in consulting patients, to findout what is important to them in terms of quality ofcare, as this may be different to what is considered
important by staff. By consulting patients, nursescan also obtain valuable feedback on the service,in terms of what works and what needs to change(Jones, 2001).
Components of a framework forclinical governance: • Implementation of evidence-based clinical
practice• Development of clinical leadership skills• Clarity of roles and responsibilities • Continuing professional development of
staff• Ensuring staff competencies for the
services and procedures they provide• Clinical audit• Risk management• Implementation of lessons learned from
complaints, incidents • Involvement of patients in all aspects of
their care• Patient feedback, and audit to ensure the
findings are being implemented (ScottishExecutive, 2003).

Strategy & Action Plan for N
ursing & M
idwifery
35
and midwives to develop skills in literaturesearching and in critical appraisal, as poorquality research is an unreliable basis fromwhich to change practice.
The Commission on Nursing (1998) attachedparticular importance to the development ofnursing and midwifery research at every level.The Research Strategy for Nursing andMidwifery in Ireland was launched in 2003 bythe Minister for Health and Children (DOH&C,2003). The strategy provides a blueprint for theexpansion of research activities and outlines21 recommendations in the area of national,institutional and professional commitments.
The National Council have grantedfunding in this region for a ResearchOfficer for a 3-year period to fosternursing and midwifery research. TheResearch Officer will facilitate thedevelopment of research awarenessamong nurses and midwives through:-
• supporting nurses and midwives incarrying out studies in order tostrengthen capacity for undertakingresearch and to encourage inter-disciplinary research.
• developing the use of evidence bynurses and midwives
CNSs/CMSs will lead the utilisation of evidencebased practice within their service, and set andmonitor standards through clinical audit.
The role of advanced practitioners will makean important contribution by instigating andleading research projects which examine clinicalnursing and midwifery issues (Commission onNursing, 1998).
Access to informationNurses and midwives in the focus groups in thisregion (Peelo-Kilroe, 2003) identified access toup-to-date best practice guidelines, electroniclibraries and evidence-based practice resourcesas a requirement to delivering high-quality care.
4.1.3 Strategic responseNurses and midwives are already engagedin many elements of clinical governance. Forexample, nurses and midwives in this regionhave developed guide-lines and are activelyengaged in the currenthealth service accredit-ation process for acutehospitals. Nurses arebecoming involved alsoin clinical audit, inparticular clinical nurse/midwife specialists.
Clinical/Professional SupervisionThe nature of Nursing and Midwifery practicemeans that support and supervision forpractitioners is essential. Clinical supervision hasemerged as an effective and acceptable meansof enhancing support for staff developmentthrough encouraging reflective practice,openness and accountability (Scottish ExecutiveHealth Department, 2001).
The National Council recommends thatstructures for the development of clinicalsupervision of nurses and midwives should bedeveloped where they do not exist (NationalCouncil, 2003a).
ResearchA key to quality nursing or midwifery practiceand professional development is research andunderpins the health strategy’s goal of effectivecare. Evidence-based practice requires nurses

4.2.2
FindingsEmpowering leadershipThe strategic planning and professional leadershipof nursing and midwifery means that senior nursingand midwifery management cannot be involved inthe minutiae of the day to day management ofnurses and midwives (such as rostering). Theinvolvement of senior nursing and midwiferymanagement in detailed management issues wouldalso undermine all levels of nursing and midwiferymanagement.
As the Health Service is delivered by professionalswho are knowledge workers, old autocratic styles ofmanagement cannot work. ‘Command and control’styles of management or leadership have negativeimpacts on a highly educated, committed work-force. A more enlightened and participative style ofmanagement, with an emphasis on delegation andempowerment of staff, needs to be fostered andsupported (DOH&C, 2003). This is echoed in theAction Plan for People Management (2002),which states that ‘A management style based onparticipation rather than the exercise of authority,and which encourages andpromotes transfor-mational change,must prevail in thehealth system.’
Leadership at all levels of nursing andmidwiferyClinical nurse and midwife managers areacknowledged clinical leaders, ensuring highstandards of clinical care and developing evidence-based care. Clinical nurse/midwife managers haveto deliver both a leadership and a management rolein their jobs. Leadership is about transformationalchange, while management is about operationalprocesses (Scottish Executive Health Department,2004b). Leaders influence and inspire staff to giveof their best in the service of others and of thehealth service as a whole.
Developing new roles and changing practicerequires leaders to have a clear vision and awillingness to take risks (Scottish Executive, 2003;DOH&C, 2003d).
Leadership does not necessarily have to equatewith clinical or management seniority, however. It iscertainly true that nurses and midwives in seniorclinical and management positions should showleadership qualities and act as role models for theirstaff. But nurses and midwives at all levels canacquire and develop leadership skills and applythem with great effect in their practice (ScottishExecutive, 2001). Leaders issue from a number ofplaces in the system and play as divergent a role astheir places in the system require (Porter –O’Grady,1999). Staff nurses and midwives at the bedside24 hours a-day, seven days a week are on the frontlines and have a distinct power to influencesustainable outcomes and productivity. They are, infact, at the first level of decision-making. Nursesdecide appropriate times to call a physician, chooseapplicable care plans and pertinent interventions(Valentine, 2002). This issue was raised in severaldifferent focus groups carried out in this region(Peelo-Kilroe, 2003). Some participants said thatdecisions relating to the patients assigned to theircare are often made by ward managers. To motivateleadership from the bottom up, managers can‘develop staff self-direction rather than givingdirection’ (Porter-O’Grady, 1999).
This is endorsed by the Action Plan for PeopleManagement, (DOH&C/HSEA, 2002) which states
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
36
4.2 LEADERSHIP
4.2.1
IntroductionLeadership at managerial and clinical levelsis essential to safeguard clinical standards ofcare. Senior nursing and midwiferymanagement has a crucial role in providingprofessional leadership to nurses andmidwives (Commission on Nursing, 1998).The Commission recommended that seniornursing and midwifery management shouldfocus to a greater extent on strategicplanning and quality assurance.

that staff at all levels will be empowered bydevolving decision-making responsibility to thelowest feasible level.
EmpowermentLeaders empower staffand empowerment is a keyrequirement for innovationin practice (Nurses’ andMidwives’ Understandingand Experience ofEmpowerment in Ireland,DOH&C, 2003b).
Attridge (1996) (cited in DOH&C, 2003b), fromher research carried out with a sample of nursesworking in British Columbia, defined power as ‘theability to have control over my work situation suchthat I can successfully bring about more effectivepatient care or other work-related activity’.
A number of factors were identified in the literatureas influencing the presence, absence, or level ofempowerment. These include conditions relatingto management, organisations, interpersonalrelationships, personal characteristics andprofessional issues. In this sense, these conditionsare both external (resources, information and
support, (Kanter, 1979) and internal honesty,flexibility and personal responsibility, (Kuokkanenand Leino-Kilpi, 2001), (cited in DOH&C, 2003b).The empowered nurse or midwife will consequentlyact in particular ways, making decisions, solvingproblems, daring to say and act.
Empowerment has a reciprocal nature - empowerednurses will empower patients, empoweredmanagers will empower nurses (DOH&C, 2003b).
Factors that influence empowerment:Factors that lead to a potential lowering of self-efficacy (from Conger and Kanungo, 1988, cited inDOH&C, 2003b).
Strategy & Action Plan for N
ursing & M
idwifery
37
ORGANISATIONAL
• Competitive pressures
• Impersonal bureaucratic climate
• Highly centralised organisational resources
• Poor communications
SUPERVISORY STYLE
• Authoritarian (high control)
• Negativism (emphasis on failures)
• Lack of reason for actions
REWARD SYSTEMS
• Lack of competence-based rewards
• Lack of motivation-based rewards
JOB DESIGN
• Lack of role clarity
• Lack of training and technical support
• Unrealistic goals
• Lack of appropriate authority/discretion
• Limited participation in decisions that havea direct impact on job performance
• Lack of appropriate/necessary resources
• Lack of network-forming opportunities
• High rule structure
• Lack of meaningful goals/tasks
• Limited contact with senior management

According to Conger and Kanungo (1988)leadership and / or supervision practices that areidentified as empowering include:-• Expressing confidence in staff accompanied by
high performance expectations• Fostering opportunities for staff to participate in
decision making• Providing autonomy from bureaucratic constraint• Setting inspirational and / or meaningful goalsRodwell (1996, cited in DOH&C, 2003b) describeswhat she considers to be related concepts,
antecedents and consequences of empowerment.The related concepts she includes are autonomy,responsibility, accountability, power, choice,advocacy, motivation and authority.The antecedents of empowerment identified aremutual trust and respect, education and support,and participation and commitment.As consequences of empowerment, Rodwell (1996)includes positive self-esteem, ability to set andreach goals, a sense of control over life and changeprocesses and a sense of hope for the future.
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
38
4.2.3
Strategic ResponseInvestment in leadership skills training is aninvestment in developing quality nursing &midwifery services and should be made availableto all nurses & midwives.Strenghtening nursingleadership is one of thestrategic themes and afocus of this strategy isto develop leadershipand accountability andsupport through all levelsof nursing and midwifery.
Actions to takeleadership forward include:• Leading an Empowered
Organisation (LEO):The LEO Programmeis widely recognisedin the United Kingdomand the United Statesof America for itsquality and relevancein the developmentof nurse and midwifemanagers. It has been
offered internationally for over fifteen years.The LEO Programme has been evaluated bythe Office for Health Management (2001).A successful application was made by theNursing and Midwifery Planning andDevelopment Unit to the National Councilfor funding to train two LEO facilitators forthe Mid-Western region. Five programmeshave already been delivered within the regionon an intradisciplinary basis.
Diane Miller, Nora Irwin O’Rourke and Sandy Tinson at the NMPDU Conference in 2004. Diane is the author of thecurrent version of the Leading an Empowered Organisation(LEO) Programme.

Strategy & Action Plan for N
ursing & M
idwifery
39
4.3
PROFESSIONAL DEVELOPMENT OF NURSING AND MIDWIFERY
Key Policy and Strategic Influences on New Nursing Role DevelopmentReport of the Commission on Nursing, 1998.Review of Scope of Practice for Nursing and Midwifery: Final Report,2000.The Code of Professional Conduct for each Nurse and Midwife, 2000.Quality and Fairness – A Health Strategy for You, 2001.Agenda for the Professional Development of Nursing and Midwifery, National Council, 2003The Challenge for Nursing and Midwifery: Discussion Paper, DOH&C, 2003.Explorative Study into the Expansion of Nursing and Midwifery Professional Roles in response to theEuropean Working Time Directive, N.M.P.D.U., Mid-Western region, 2003.Report of the Task Force on Medical Staffing, 2003.
4.3.1
IntroductionDelivery of the objectives of the HealthStrategy: Quality and Fairness- A HealthSystem for You, and of the Health ServiceReform Programme is dependant on theavailability of a range of core competencieswithin clinical practice, management andeducation.
Focus on interdisciplinary patientcareThe way in which nursing practice isdeveloped must have the interests and needsof patients, carers and wider communities atits core, and the need to work collaborativelywith other professionals (Scottish Executive,2003a). For example, in the research for theAgenda for the Professional Development ofNurses and Midwives (National Council,2003), nurses described a role for the CNSwhich could reshape the way in whichsurgical care is provided. The CNS could runa nurse-led pre-admission clinic, provide in-patient care and support a nurse-led follow-up outpatient clinic. Links could be madedirectly from the surgical ward to thecommunity thereby making the transfer fromsecondary to primary care seamless.
4.3.2
FindingsThe Commission on Nursing (1998) establishedthe clinical pathway for professional developmentin nursing. This encapsulated expanding roles forgeneralist nurses and midwives, the establishmentof clinical nurse/midwife specialist and advancednurse/midwife practitioner posts.
Identified competenciesThe focus is on utilising all the competencies ofall clinical nurses and midwives.Core competencies have been established forclinical nurse/midwife specialists and advancednurse/midwife practitioners.
The Office for HealthManagement has identifiedcompetencies required forfrontline, middle and seniornurse managers (OHM,2004).
The Scope of Nursingand MidwiferyPractice FrameworkThe Scope of Nursing and Midwifery PracticeFramework (An Bord Altranais, 2000) providesa framework for role development andexpansion in nursing and midwifery.
The scope of nursing and midwifery practicein Ireland is ‘the range of roles, functions,responsibilities and activities, which a registerednurse/midwife is educated, competent, and has theauthority to perform’ (An Bord Altranais, 2000a). Theframework was developed following considerationof national and international developments innursing practice and its aim is to support nurses inthe expansion of their scope of practice.
In determining his/her scope of practice, the nurseor midwife must make a judgement as to whether
he/she is competent to carry out aparticular role or function. Nurses mustcomply with the Code of ProfessionalConduct (An Bord Altranais, 2000b)and be aware of their own account-ability for their practice (DOH&C,2003d).
Role expansion versus role extensionDevelopment of roles will be underpinned by theaim of reducing fragmentation of patient care,fitting within the legal and ethical and regulatoryframework of the Scope of Professional Practice toensure patient safety is maintained.
Role expansion involves becoming morecompetent, reflective, autonomous practitioners anddeveloping expertise and skills to meet patients’nursing needs (An Bord Altranais, 1999).
The extended role is defined as one thatinvolves tasks borrowed from other professions;these tasks are used by the nurse at the discretionand convenience of others and may involvetraining, supervision and certification by otherprofessions (National Council, 2003a).Therefore, developing roles must be underpinnedby role expansion rather than role extension.The negative effect of fragmented patient care onthe quality of care was identified by Menzies in herseminal research (Menzies, 1977). This led to anover emphasis on mechanical tasks and a reducedemphasis on psychosocial aspects of nursing care.
The Legal FrameworkNurses and midwives who develop their role toinclude roles/tasks currently undertaken by otherhealthcare professionals must be aware of the legalboundaries, and that they have sufficient trainingand preparation to ensure that they can performthe role to the required standard (DOH, UK, 2004;
National Council, 2003a). Within the legal frame-work they will be judged by two legal standards:• The rule of law which requires a nurse or
midwife to act within the law• The rule of negligence which requires a nurse
or midwife who takes on roles/tasks currentlyundertaken by another healthcare professionalto perform that role or task to the same stand-ard. Nurses are expected to have undertakensufficient training and preparation to ensure thatthey are competent to perform the role to therequired standard (Scottish Executive HealthDepartment, 2003a).
Vicarious Liability: When a nurse is employed bya hospital, the organisation has vicarious liabilityfor the nurse’s actions. This is in addition to thenurse’s own professional accountability to An BordAltranais. It is important that any role developmentor new role is reflected in the job description, sothat it is clear that the employer is aware that thenurse is taking on the new role.
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
40

Regional Requirements for RoleDevelopment - Mid-Western AreaA significant amount of exploratory and consul-tative work was undertaken in the Acute HospitalServices by the Nursing and Midwifery Planningand Development Unit, in the Mid-Western Area,led by Lorna Peelo-Kilroe (2003). The method usedinvolved focus group interviews with all grades ofnursing and midwifery personnel in the acutehospitals. These included staff nurses / midwives,clinical nurse / midwife managers 1, 2 & 3, clinicalnurse/ midwife specialists, and Assistant Directorsand Directors of Nursing. Thirty eight groups wereheld involving 226 participants. The informationobtained from focus groups with nurses andmidwives in acute hospital services contributed tothe nursing and midwifery section of the Report ofthe National Task Force on Medical Staffing (2003).
Participants of all grades welcomed the opportunityto explore professional development. Theyidentified many areas where role developmentwould be beneficial in delivering a seamless serviceto patients (Peelo-Kilroe, 2003).
Nurses and midwives appreciated the need to workin partnership with patients, their relatives andother carers in collaboration with others asmembers of the multi-disciplinary team.
Nurses and midwives identified a number of keyareas in their practice which could be expanded:• Pre-assessment clinics• Minor injury clinics• Nurse-led respiratory clinics• Nurse-led admission and discharge protocols• CNS and ANP roles in Mental Health Services
Requirements for role developmentidentified in the national andinternational literature.Role development should be driven by thenursing and midwifery profession, responsive tothe changing health care needs of patients andservices (National Council, 2003a).
Competence, and theacceptance of individualaccountability, is key torole expansion (NationalCouncil, 2003a).Competence is defined asthe ability of the registerednurse/midwife to practicesafely and effectively, ful-filling his/her professionalresponsibility within his/her scope of practice(An Bord Altranais, 2000a). Safe and effectivepractice is based on valid and reliable evidence.
Education is central to role development andunderpinned by local competency-basedframeworks
Role development must occur in a planned andcoordinated way and the acquisition of skills andqualifications will require a lead in time (Reportof the National Task Force, 2003).
Nurses and midwives expanding their rolesneed time to become confident in these roles,and hospital systems need to adapt andembrace such role changes (National Council,2003a)
Adequate resources must be put in place by theorganisation to ensure these aspects of patientcare are still performed to a high standard(DOH&C, 2003 Hanly).
Robust resource and finance planning should beincorporated into role development policy toensure sustainability (Scottish Executive HealthDepartment, 2003a).
Role development should be evidence basedand build the body of nursing knowledge, beinformed by needs assessment andsubstantiated by an evaluation of effectivenessand benefit to patients (Scottish ExecutiveHealth Department, 2003a). Also, roledevelopment should be evaluated and thefindings widely disseminated.
Effective leadership, communication, partnership,educational and professional development,competence and clinical guidelines wereidentified as key success factors in developmentof roles and responsibilities (DOH&C, 2003d).
Strategy & Action Plan for N
ursing & M
idwifery
41

• Midwifery-led clinics, early transfer schemes• Community Mental Health Liaison Officers• Administration of the first dose of intravenous
antibiotics• Intravenous cannulation, venepuncture, male
catheterisation,• Ordering of routine blood tests according to
agreed protocols (Peelo-Kilroe, 2003).
Critical success factors for roledevelopment identified in focus groupswere:• Professional Development opportunities • Competency based education and training for all
role development• Development of guidelines and protocols• Clinical supervision• Adequate support services, such as, clerical,
portering and pharmacy support• Information Technology Infrastructure• Partnership with all stakeholders and
multidisciplinary team working • Role development must include autonomy and
decision making (Peelo-Kilroe, 2003).
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
42
4.3.3
Strategic Response Nurses in the Mid-West Area have alreadydeveloped roles to improve patient services.• Peripheral Cannulation• Venepuncture• Administration of Chemotherapy• Administration of first dose of antibiotics• Midwife-led discharge• Nurse-led haematology clinics• Nurse-led needs based assessment clinic for
joint replacement surgery
Clinical care pathways are in use in ENT andare being developed in orthopaedics,haematology and medicine.
Nurse PrescribingThe Nursing andMidwifery PrescribingProject is examining theimplications of involvingnurses and midwives inthe prescription andadministration ofmedicinal products.This project started in September, 2001, and is ajoint project managed by the National Counciland An Bord Altranais. The steering committeeof the project is multidisciplinary comprising
representatives from nursing, midwifery,medicine, pharmacy, education, health boardmanagement and the public.
Sixteen sites were selected representing adiversity of practice settings across communityand acute care sectors. The pilot site in the Mid-West region is the Coronary Care Unit, MWRH,Dooradoyle.
Locally developed medication protocols arebeing used to supply medication to theindividual patient/client, implementing a modelof collaborative prescribing. The interdisciplinarynature of collaborative prescribing requires thecommitment of both medical practitioners intheir role as clinical mentors and pharmacists.
As part of the evaluation of this study, patientsreceiving care as per the medication protocolswill be asked to comment on their satisfactionwith the information that the participatingnurse/midwife has provided on their conditionand the medicines needed to treat it.
The Review of Nurses and Midwives in thePrescribing and Administration of MedicinalProducts will conclude in the spring of 2005and will be published in a comprehensive FinalReport.

Strategy & Action Plan for N
ursing & M
idwifery
43
4.4.2
FindingsPractice development should happen throughexpansion of role rather than just taking on tasks(National Council, 2003a). Expansion of practiceinvolves a broader holistic process, both in relationto patient/client needs and the individual nurse(National Council, 2003a).
There needs to be consideration of how bestgeneral nurses and midwives can assess, plan,implement and evaluate general nursing care. Therewill need to be an integrated approach with thecare provided by the interdisciplinary team, whilebeing able to maintain the unique contribution ofthe general nurse (National Council, 2003a).
In order to develop roles, nurses must be clearabout the value of current roles, core competenciesof all nurses and the value of the generalist(Scottish Executive Health Department, 2003a).
Castledine (1998) is emphatic in his belief that it isfrom the generalist domain that all nursing practiceevolves, making it the fundamental basis of allnursing care. This could be interpreted in the Irish
context that, for general nurses, generalist practiceforms the basis of care (National Council, 2003a).
Essence of CareThe Essence of Care programme, launched by theDepartment of Health in England (2001), provides atool to help practitioners take a patient-focused andstructured approach to sharing and comparingpractice. It enables health care personnel to workwith patients to identify best practice and todevelop action plans to improve care.
The nine benchmarks of care are:-1. COMMUNICATION2. PERSONAL AND ORAL HYGIENE3. FOOD AND NUTRITION4. PRESSURE ULCERS5. PRIVACY AND DIGNITY6. RECORD KEEPING7. CONTINENCE AND BLADDER AND BOWEL CARE8. SAFETY OF CLIENTS WITH MENTAL HEALTH
NEEDS IN ACUTE MENTAL HEALTH ANDGENERAL HOSPITAL SETTINGS
9. PRINCIPLES OF SELF-CARE
Essence of Care fits into clinical governancethrough the components of :-• Consultation and patient involvement• Clinical risk management• Clinical audit• Use of information about the patients’ and or
carers’ experience• Staffing and staff management• Education, training and continuing personal and
professional development• Strategic capacity
4.4 FUNDAMENTALNURSING CARE
4.4.1
IntroductionCaring is at the core of nursing and must becentral to role development. In light ofexpanding roles, it will be important toensure that the fundamental aspects ofgeneral nursing and midwifery care areretained and that fragmentation of nursingroles is avoided.
There is a widespread concern in the nursingprofession that the expansion of nursing roleswill erode the capacity of nurses to providebasic nursing care which are core to the artof nursing.
4.4.3
Strategic ResponseThe Essence of Care programme wasidentified by the Steering Group as being ameans of ensuring that fundamental care isprotected.

Values underpinning nursing/midwiferypractice decisions and practicedevelopment in this StrategyThe Service delivered to patients/clients is focusedon the values identified in the Scope of Nursingand Midwifery Framework (2000). This documentidentifies that nursing practice decisions must bebased on the patient’s/client’s best interests main-taining the highest standards of quality; respect forthe uniqueness and dignity of each patient/client;a therapeutic relationship empowering patients/clients based on trust, compassion and support;advocacy on behalf of patient/clients and on behalfof nursing and management structures withinwhich care is delivered, nursing practice based onbest available evidence and practice based on TheCode of Professional Conduct for each Nurse andMidwife, (2000).
4.5.2
FindingsContinuing Professional Development(CPD)The Report on the Commission on Nursing (1998)recognised the ‘absolute importance of continuingeducation to the quality of services offered topatients and the development and growth ofprofessional nursing and midwifery’.
The Health Strategy (DOH&C, 2001) alsoemphasised the need to provide the financial andpractical supports necessary for training anddeveloping people in the health system:-
‘in addition to the commitments to trainingand development of new staff, health service
employers will demonstrate a commitment tocontinuous learning by facilitating existingstaff to undertake programmes that enhancethe quality of patient care and contribute totheir own career development.’
Action Plan for People ManagementThis concept is endorsed by the Action Plan forPeople Management (APPM, 2002) -
THEME 5: ‘Investing in training, development andeducation to ensure that all staff have theknowledge, skills and attitudes required to deliver aquality health service.’
ACTION 5.2 states that ‘Delivery of the objectivesoutlined in Quality and Fairness will be dependenton the availability and development of a range ofcore competencies’.
In the future, clinical governance will provide anoverall framework for a coherent approach tocontinuing professional development (CPD), whichensures that priority is given to addressing learningneeds linked to specific service quality issues(National Council, 2003a). A framework for asystematic approach to identifying learning needs,the ‘Learning and Development Needs AnalysisToolkit’ was developed bythe Office for HealthManagement in 2002.This includes assessmentof individual and ward/unit/department needs. The aimof a systematic approachis to align the existingtraining funds with localservice objectives.
Continuing Professional Development(CPD) ActivitiesAn important principle of CPD is that it includesmuch more than going on courses. There is growingemphasis on work based learning as the outcomesfor CPD become increasingly focused on skills,competencies and behaviours (DOH, UK, 2004).
4.5
LEARNING AND DEVELOPMENT
4.5.1
IntroductionIntegrated human resource developmentinvolves developing a competent workforcethat delivers evidence-based effective carethrough the acquisition of skills andknowledge (Munro et al, 2004).
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
44

Work based learning includes, e.g., learning fromthe results of clinical audit and putting in placeservice improvements based on audit; andreflecting on practice and experiential learning.
Work based learning should focus on findingsolutions to common and important problems.It should be based on real life situations. Workbased learning can involve a wide range ofactivities, as identified in Action 5.3 of theAPPM (2002).
These include:-
• COACHING ON THE JOB
• MENTORING
• JOB ROTATION
• LEARNING SETS
• WORK BASED PROJECTS
EvaluationThe National Council (2003a) advocates amore rigorous approach to evaluation of CPDprogrammes. Evaluation needs to consider theimpact on patient care, as well as how theprogramme was perceived by participants.The National Council (2003a) also recommendsthat consideration should be given to the culturaldiversity of the workforce in planning educationalprogrammes.
Ongoing learning and development of the nursingand midwifery workforce absorbs a large amount
of resources both in terms of finance and locumreplacement and therefore it is necessary to ensurethat the investment results in the requiredoutcomes and that the education ultimatelyimpacts on patient care.
4.5.3
Strategic ResponseWho is responsible for CPD?CPD should be a partnership between the individualand the organisation. Responsibility lies withindividual nurses and midwives to take measuresto develop and maintain the competence to deliversafe, competent and evidence-based nursing/midwifery care to patients/clients (An BordAltranais, 2002).
All involved in CPD, Clinical Nurse/MidwifeManagers, Assistant Directors and Directors ofNursing, Nurse Practice Development Co-ordinators,Nursing and Midwifery Planning and DevelopmentUnit and the staff of the Centre for NurseEducation, should make sure that CPD is alignedwith ward/department needs (National Council,2003a).
The Centre for Nurse Education (CNE)The Centre for Nurse Education provides astructured framework for in-service and continuingeducation within the geographical remit of thecentres. The Centre for Nurse Education will becomea centre of excellence in the pursuit of practice-based inter- and multidisciplinary education in the
Staff at the Regional Orthopaedic Conference, 2004.
Strategy & Action Plan for N
ursing & M
idwifery
45

health service, thus contributing to the continueddevelopment of effective and equitable health andsocial care in accordance with national policy(National Council, 2003).The CNE also provides education for health careassistants.
Local access to PostgraduateDiploma/MSc programmes Action 5.4 of the Action Plan for PeopleManagement states that in order to meet theworkforce planning and skills needs of the healthservice, significantly better integration witheducation and training authorities is required(APPM, 2002). The development of strategicalliances and joint working arrangements with thirdlevel institutions and professional colleges will be akey feature of the service (MWHB, 2001). Post-registration education provision should be flexible,and developed in modular frameworks wherepossible, to facilitate transferability, transparencyand credit accumulation (National Council, 2003a;National Qualifications Authority of Ireland, 2003).The difficulty in gaining accreditation for priorlearning (APEL) was mentioned frequently in theconsultation process with Irish nurses and midwives(National Council, 2003a).
The Nursing and Midwifery Planning andDevelopment Unit, HSE Mid-Western Area and the
Department of Nursing and Midwifery, University ofLimerick are collaborating to develop and deliverPostgraduate Diploma/MSc programmes inspecialist practice. The following programmes havebeen developed:-
• Graduate Diploma / M. Sc. Nursing (PsychosocialInterventions in Mental Health Care).
• Graduate Diploma / M. Sc. Nursing (IntellectualDisability Studies)
• Graduate Diploma / M. Sc. Nursing(Rehabilitation of the Older Person)
• Graduate Diploma / M. Sc. in Midwifery Studies.
Professional / Clinical supervisionA crucial element of work based CPD is the abilityto reflect on and learn from relevant experiences,including adverse events (CPD, NHS, 1999).
Professional / Clinical supervision is also a meansof integrating new knowledge acquired in CPD intopractice. The National Council for the ProfessionalDevelopment of Nursing and Midwifery has fundedtraining for 96 nurse managers to undertakesupervisor and supervisee training.This includes the development of professionalsupervision guidelines and evaluation of theprogramme.
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
46
Back row, left to right: Pat McLoughlin, Deputy Chief Executive, HSE and Director of National Hospitals Office; Cora Lunn, AssistantProject Manager, Post-Graduate Education; Geraldine Cunningham, Acting Director, RCN, London, and Paschal Moynihan, Director ofOlder Persons Services, HSE Mid-Western area.Front row, left to right: Geraldine Regan, Director of Nursing, Our Lady’s Hospital for Sick Children, Crumlin; Paula Stanley, Care & CaseManagement Co-ordinator, East Clare Community Care; Nora Irwin O‘Rourke, Director, NMPDU and Dr. Joanna Bennett, WorkforceDevelopment Manager, Sainsbury Centre for Mental Health, at the NMPDU Conference, April 2005.

Personal Development Plans (PDPs) A process for individual development -Personal Development Plans (PDPs) - is also included in the Officefor Health Managementtoolkit. A PersonalDevelopment Plan is aform of self-managedlearning that is ownedby the individual andenables a strategicapproach to identifyinglearning and develop-ment goals.
The principles which might underpin personaldevelopment planning were outlined by RobinDouglas in an article for the Office for HealthManagement (OHM: Issue 3, May 1998) p 126
These included:
• An acceptance of personal responsibility forone’s own learning;
• A recognition that self knowledge is crucial toeffective development;
• An understanding of the many formal andinformal opportunities that may be taken toimprove knowledge and skills;
• A belief that action-based learning canprovide the means to embed substantiveknowledge and give a chance to apply ideasto practice;
• The understanding that the process oflearning is not a simple change fromincompetence to full capability, but containsmany challenges in both intellect andemotion that must be met along the way;
• An acceptance that, although theresponsibility for planning and implementinga personal development plan is likely to be anindividual process, work with others will becrucial in achieving any development goals.
Personal Professional PortfoliosA portfolio is an organised collection ofdocuments chronicling an individual’s career:these accumulated documents may then be
drawn upon when applying for jobs or courses orin order to demonstrate learning (NationalCouncil, 2003b).
The National Council for the ProfessionalDevelopment of Nursing and Midwiferypublished guidelines for portfolio developmentfor nurses and midwives (National Council,2003b). Based on these, a Professional Portfoliowas developed by the Nursing and MidwiferyPlanning and DevelopmentUnit and is available viathe Unit. The portfolioprovides a framework for individual nurses andmidwives to documenttheir continuingeducation anddevelopment.
The portfolio can be used to record:
• Competency development
• Formal and informal learning
• Reflective practice and clinical supervision
• Achievements e.g. poster presentations
• Employment history
• Plans for future development
Line managers should play a key role inencouraging and supporting nurses andmidwives to engage in PDP and the use ofportfolios (National Council, 2004b).
Intra- and Interdisciplinary CPDThe Health Strategy emphasises the need forintegrated healthcare provision and for initia-tives that promote relationships between health-care professionals (National Council, 2003a)
There is an increased incidence of intra-disciplinary education in the region, e.g.,professional supervision and managementdevelopment programmes. There is alsoincreased level of interdisciplinary education,e.g. healthcare management in third leveleducation sector and also at in-service e.g.,basic and advanced cardiac life support.
Strategy & Action Plan for N
ursing & M
idwifery
47

4.6.2
FindingsThe Health Strategy (DOH&C, 2001) in itsframework for developing human resources,identified as a key objective to develop andexplicitly value staff at all levels of the healthsystem. A working environment where people feelvalued, recognised and safe is important to theimprovement of morale and the retention of staff.This in turn benefits service users.
ChallengesThe Health Strategy identified serious challengesfacing staff and managers in the health system atthe moment including skills shortages, difficulties inrecruiting and retaining qualified staff, stressfulworking conditions, high turnover rates, poormorale, and complex industrial relations.Factors impacting on the demand for nursesinclude:• An aging workforce that will retire in large
numbers during the next decade• An aging population predicted to require
increased nursing and other health care• A shortage of nurses• The non-graduation of nurses in 2005
The Final Report of Nurses’ andMidwives’ Understanding andExperiences of Empowerment (2003b)found that many nurses working within the Irishhealth system feel invisible and undervalued withinthe current structures. There were some strong
4.6
IMPROVING WORKING LIVES
4.6.1
Introduction High standards of care, innovation, flexibilityand enthuasism for change can only thrive inan environment in which people’s efforts,commitment, professionalism and expertiseare valued (Scottish Executive, 2001).
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
48

comments made in one focus group discussionregarding nurses and midwives leaving theprofession as a result of not being respected.Many examples were given relating to nurses andmidwives in practice not having a voice in relationto patient care. The Report of the Commission(1998) also highlighted nurses and midwivesfeeling of not being involved in policy and strategicdirection and having a voice in the running ofhealth care organisations.
Increasing demandsFactors such as increased average acuity resultingfrom reduced beds and shorter length of stay andthe introduction of new technologies and treat-ments have had significant impact on nursingpractice requirements, demanding increased skills,autonomy, and ability to work with multidisciplinaryteams.
Systems to determine staffing levelsThe Commission on Nursing (1998) recommendedthat the Department of Health and Children, healthservice providers and nursing organisationsexamine the development of appropriate systemsto determine nurse staffing levels (paragraph 7.63).A working group was established in January, 2004to make recommendations.
Objective assessment of care needs, providing theopportunity for Clinical Nurse / Midwife Managersto measure patient dependency data, is a keyelement of the information required to ensure aneffective nursing skill mix.
Linked with staffing levels, almost all of theparticipants of focus groups in the empowermentstudy felt that having an increased workload wassingularly disempowering (DOH&C, 2003b).
Framework for Human ResourcesTwo key strands were addressed in the Frameworkfor Human Resources in the Health Strategy: Qualityand Fairness (DOH&C, 2001):• Ensuring a qualified, competent
workforce to meet the changing demands ofthe people: It is vital to plan effectively atnational and local level so as to recruit, retainand develop a workforce with the capacity andskills to meet service needs.
• Becoming an employer of choice:Many factors, other than financial rewards,
draw workers to join and remain with aparticular employer. These include:- best practice employment policies and
procedures- positive strategies for improving the work
environment and the quality of working life- a positive and participative style of
management which makes for a stimulatingwork environment
- a culture that emphasises the value ofcontinuous learning and improvement in theskills and experience of everyone working inthe system
- greater flexibility in times of work /attendance patterns.
To achieve the above, initiatives were undertakenby the Department of Health and Children.• Implement the Final
Report of the Studyof the Nursing andMidwifery Resource(DOH&C, 2002).
• Introduce degree-leveleducation for nursing in2002
• Build on existing stepsincluding recent intro-duction of flexible workingarrangements; payment of fees to nursesand midwives undertaking part-time post-registration degrees and courses in specialisedareas of clinical practice
• Provide flexible return to nursing and midwiferycourses for nurses wishing to rejoin theworkforce
• Develop further clinical specialist and advancedpractitioner posts in nursing and midwiferywithin the framework of the National Council forthe Professional Development of Nursing andMidwifery
Action Plan for People ManagementThe Action Plan for People Management(DOH&C/HSEA, 2002) is a key component in thedelivery of the framework for Human Resourcesoutlined in Quality and Fairness. At the strategiclevel, human resource management must becomean integral part of the service planning process.At the operational level, the Action Plan tacklesissues which negatively impact on workingrelations.
Strategy & Action Plan for N
ursing & M
idwifery
49

One of the seven key elements that the APPMaddresses is the quality of working life.
Support and ConsultationThe Customer Service Action Plan (DOH&C, 2003-2004) recognises staff as internal customers.A principle of quality customer service is to ensurethat staff are properly supported and consultedwith regard to service delivery issues.
Action Plan: Towards Workforce PlanningThe Nursing and Midwifery Resource Final Reportof the Steering Group, Towards Workforce Planning(2002) suggested action plan for retentionidentified the following factors:
3. ORGANISATIONAL SUPPORT
• Career pathway and professionaldevelopment
• Quality of working life and environment
4. STAFFING
• Staffing ratio, skill mix and workloadmeasurement
• Health care assistant and other supportstaff
• Flexibility in rostering
The report identified a comprehensive approach toworkforce planning and made recommendationswith 118 attributable actions
Providing Educational OpportunitiesOpportunities for continuing education and trainingare an important quality of care issue but it is alsoa quality of work life issue: nurses want to have theskill to provide competent care and also meet theirown needs for professional satisfaction (CanadianNursing Advisory Committee, 2003). It is essentialto ensure that there are mechanisms and resourcesto provide them with the competencies they needto do their job. Nurses and midwives in differentfocus groups in the Mid-Western region frequentlyidentified transparency in education budgets withinan equitable system for allocating study leave asimportant (Peelo-Kilroe, 2003).
1. PROFESSIONAL NURSING AND MIDWIFERY PRACTICE
• Induction and orientation• Support for quality professional nursing
practice• Involvement in decision-making, autonomy
and empowerment
2. MANAGEMENT
• Value, respect and acknowledgement ofstaff
• Participative style of management• Communication• Team building
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
50

Strategy & Action Plan for N
ursing & M
idwifery
51
4.6.3
Strategic ResponseIntegrated Workforce Planning in theHSE Mid-Western AreaThe Health Strategy (2001) recommended thatintegrated workforce planning be introduced ina way that:-• Aligns workforce planning with the service
planning process• Promotes the use of skill mix • Ensures that training places match the
demand for specific skills in the health sector
A Resource Officer is employed in the Nursingand Midwifery Planning and Development Unit,HSE Mid-West area, to collaborate andcommunicate with stakeholders at regional andnational level to ensure that the recommen-dations of the report Towards WorkforcePlanning are acted upon, and also to play akey role in driving the process of integratedworkforce planning in the future.
Priorities include:• Completion of the Nursing and Midwifery
Minimum Dataset• Planning workforce needs in light of the non-
graduation of nurses in 2005 • Development of a recruitment and retention
strategy for nursing and midwifery• Education for nurse managers on workforce
planning and the service planning process• Provision of current workforce profiles that
will assist in future forecasting of numbers,skills and qualifications required to meetservice need
• Ongoing monitoring of turnover in nursingand midwifery
• Promotion of nursing as a career• Development of a healthcare assistants’
training programme• Further development of Return to
Nursing/Midwifery programmes
The mean annual turnover rate of nurses inIreland peaked in 1999 to 12% (DOH&C, 2002).The turnover for the Mid-Western Region in2003 was 7.4%.
DiversityDiversity has become a reality withinorganisations (Office for Health Management,2002). The APPM (DOH&C/HSEA, 2002) statesthat equal opportunities and accommodatingdiversity in the workplace recognises the talentsand skills of all staff and provides access toemployment and promotion to the widestpossible pool of employees and potentialemployees. Equal opportunities and diversityis about creating a culture that seeks, respects,values and harnesses difference.
In the Mid-West Region, ‘People Management -The Legal Framework program (HSEA, 2004)is being facilitated by in-house trainers,co-ordinated by the Corporate Learning andDevelopment Manager. This programme providesthe knowledge to enable line managers tounderstand and operate key human resourcepolicies and procedures to enhance employeeperformance, motivation and commitment andthus contribute to high quality care. It coversthe areas of grievance, discipline, employeewell being, equal opportunities/ accommodatingdiversity, dignity at work, recruitment andselection, and statutory leave entitlements.
Our aim is to have a stable workforce in order toensure continuity and safety of care, retain staffin which we have invested and avoid additionalcosts and risks involved in employing agencystaff.

Implementation
and Communication

In response to application from Directors andAssistant Directors in collaboration with theProfessional Development Officer, Nursing andMidwifery Planning and Development Unit in thisregion, The National Council for the ProfessionalDevelopment of Nursing and Midwifery havefunded the following:• Two ‘LEO’ facilitators (Leading an Empowered
Organisation) have been trained. This enablesthe in-house delivery of LEO Programmes withinthe region.
• Funding has been granted for Phase 1 of theestablishment of Advanced Nurse/MidwifePractitioner posts. This involves the developmentof job descriptions and development ofcollaborative protocols.
• Funding was secured for training for Nurse/Midwife managers in Professional/ClinicalSupervision on a pilot basis. This commenced in2004 for 24 supervisors and 72 supervisees.
• Funding has also been granted for the post ofResearch Officer for a period of three years.
• The Council has part funded the Nursing andMidwifery Planning and Development UnitConference and the Regional OrthopaedicConference.
• Two Project Officers for the development of Post-graduate Nursing and Midwifery education, inassociation with the University of Limerick.
The Department of Health and Children hasprovided funding for a Level 2 FETAC Programmefor Health Care Assistants.The National Council / An Bord Altranais is fundingthe Nurse Prescribing Project.Funding of Advanced Nurse / Midwife Practitionerposts will be through the service planning process.The development of clinical practice will beresourced through the service planning process.Personal Professional Portfolios have beendeveloped and made available to nurses andmidwives regionally and nationally by the Nursingand Midwifery Planning and Development Unit.Currently, the portfolio is priced at €20.
5.1 COSTING
Lead responsibility and suggested timelines were identified for actions required to implement the strategy.
The strategy will be communicated to all nurses and midwives in the region through establishedcommunication networks, existing newsletters and via the intranet. Copies will be available for staff andfor inclusion in recruitment packs.
Implementation of the action plan will depend on collaboration, interdisciplinary working and partnership.
While the strategy is intended to provide a plan for the next three years it will be reviewed quarterly toensure it remains relevant to changes in service need and will be amended in the light of emergingregional and national priorities. Yearly action plans will be monitored on a bi-annual basis.
The strategic aims will be used to guide service planning.
5.2 IMPLEMENTATION AND COMMUNICATION OF THE STRATEGY
Magnus Conteh, Project Manager, Post-Graduate Education,Joan Somers Meaney, Director of Nursing, Mid-WesternRegional Hospital, Ennis and P.J. Cleary, Director of Nursing,Mid-Western Regional Hospital, Nenagh, at the NMPDUConference, 2005.
Strategy & Action Plan for N
ursing & M
idwifery
53


The key areas of feedback on the documentfrom the group were:
1. That continuing care after the first few days ofacute care could be improved by appropriateinformation, disease specific education andadvice about self-care (e.g. medication
management) post discharge.2. Professionals with specialist knowledge are
required. This includes education aboutmedication and self-care. The groupemphasised the importance of increasedunderstanding of their disease (i.e. COPD).
3. The importance of having a voice in one’s owncare plan; and involvement of carers.
4. The importance of fundamental care e.g.,handwashing, ‘the nurse giving hands on careat the bedside’, the importance of privacy, etc.
5. The importance of specialist nurses developingin all areas of practice in order to ensure thatnursing care is based on up-to-date evidenceand is of high quality.
The group discussed elements of the Acute Nursingand Midwifery Strategy.
The key areas of feedback on the documentfrom the group were:
1. The need for nursing and midwifery staff toconcentrate on the fundamental aspects ofcare.
2. The importance of appropriate education andtraining for staff being in place to support thedelivery of patient care.
3. Ensuring that the change to Degree Level
Nursing Education offers adequate ClinicalExperience time.
4. That the continuity of patient care and servicesis assured.
5. There was support for more nursing andmidwifery led services, for example by ClinicalNurse Specialist and Advanced NursePractitioners.
6. Information about new positions, e.g. ANP,should be communicated to the public.
7. Ensuring that there was adequate numbersof Nurses and Midwives through goodRecruitment and Retention strategies.
8. That there is a need for more resources e.g.increasing nursing and midwifery pay to ensurethat staff remain within the profession.
9. There was an acknowledgement thatimplementing the strategy would take time andthat it would not happen overnight.
10. That implementing the strategy would beabout changing some of the culture that existswithin the current system.
Strategy & Action Plan for N
ursing & M
idwifery
55
Focus Group Feedback from the Consumer Panel ONCOLOGY SERVICES
Focus Group Feedback from the Consumer Panel RESPIRATORY MEDICINE
Date: 11th of February 2005Venue: Social Service Centre, Henry Street
Limerick.Topic: Acute Nursing and Midwifery StrategyPresent: Cathleen Ryan, Mid-Western Regional
Hospital, Cora Lunn, NMPDU.
Date: 16th of February 2005Venue: School of Nursing, Mid-Western
Regional Hospital, Ennis.Topic: Acute Nursing and Midwifery StrategyPresent: Anne Buckley, Health Promotion
Hospital Co-ordinator, Marie Casey,NMPDU.


Advisory Committee on Health HumanResources (2000) The Nursing Strategy forCanada. Health Canada: Ontario.
An Bord Altranais (2000a) Review of Scope ofPractice for Nursing and Midwifery: FinalReport. Dublin: An Bord Altranais.
An Bord Altranais (2000b) The Code ofProfessional Conduct for each Nurse andMidwife. Dublin: An Bord Altranais.
An Bord Altranais (2000c) Requirements andStandards for Nurse Education Programmes.Dublin: An Bord Altranais.
Attridge, C.B. (1996) Analysis of powerlessnessin nursing work. Canadian Journal of NursingAdministration. 36-57, May-June.
Benefield, L.E., Clifford, J., Cos, S., Hagenow,N.R., Hastings, C. and Kobs, A. (2000) Nursingleaders predict top trends for 2000. NursingManagement. 31(1), 21-23.
Canadian Nursing Advisory Committee (2003) A Report on the Nursing Strategy for Canada.Advisory Committee Health Delivery and HumanResources: Ontario
Conger, J.A. and Kanungo, R.N. (1988) Theempowerment process: integrating theory andpractice. Academy of Management Review.13(3): 471-482.
Continuing Professional Development: Qualityin The New NHS (1999) NHS Executive,Department of Health, London.
Department of Health (2003) Developing keyroles for nurses and midwives: A guide formanagers. Department of Health: London.
Department of Health (2004) Learning forDelivery: Making connections between postqualification learning/continuing professionaldevelopment and service planning. UK: Learningand Personal Development Division.
Department of Health and Children (2004)Health Service Reform Programme: Phase 1.The Composite Report. DOH&C: Dublin.
Department of Health and Children (2003)The Health Service Reform Programme Dublin:The Stationery Office.
Department of Health and Children (2003 -2004) Customer Service Action Plan. Dublin:The Stationery Office.
Department of Health and Children (2003a) AResearch Strategy for Nursing and Midwifery inIreland, Final Report. Dublin: The StationeryOffice.
Department of Health and Children (2003b)Nurses’ and Midwives’ Understanding andExperiences of Empowerment in Ireland: TheFinal Report. Dublin: The Stationery Office.
Department of Health and Children (2003c) The Challenge for Nursing and Midwifery: ADiscussion Paper. Dublin: The Stationery Office.
Department of Health and Children (2003d)Report of the National Taskforce on MedicalStaffing. Dublin: The Stationery Office.
Department of Health and Children (2003e)Audit of Structures and Functions in the HealthSystem, Prospectus. Dublin: The Stationery Office.
Department of Health & Children (2003f)Evaluation of the Irish Pilot Programme for theEducation of Health Care Assistants, NursingPolicy Division, Dublin: The Stationery Office.
Department of Health and Children/HealthService Employer’s Agency (2002) Action Planfor People Management in the Health Services.Dublin: The Stationery Office.
Department of Health and Children (2002) TheNursing and Midwifery Resource: Final Report ofthe Steering Group – Towards WorkforcePlanning, Nursing Policy Division. Dublin: TheStationery Office.
Strategy & Action Plan for N
ursing & M
idwifery
57

Department of Health and Children (2001)Quality and Fairness: A Health System for You.Dublin: The Stationery Office.
Department of Health and Children (2001)Effective Utilisation of Professional Skills ofNurses and Midwives. Dublin: The StationeryOffice.
Department of Health and Children (1998)Report of the Commission of Nursing – ABlueprint for the Future. Dublin: The StationeryOffice.
Dublin Academic Teaching Hospitals (2001) SkillMix Group Report. Dublin: Dublin AcademicTeaching Hospitals.
Jones, J. (2001) Exploring nurses’ experiencesof clinical governance. Journal of ClinicalExcellence. 2(4): 243-248.
Kanter, R.M. (1979, 2nd Ed. 1993) Men andWomen of the Corporation. New York: BasicBooks. Cited in
Kuokkanen, L. and Leino-Kilpi, H. (2001) Thequalities of an empowered nurse and the factorsinvolved. Journal of Nursing Management. 9:273-280.
Menzies, I. (1977) The Functioning of SocialSystems as a Defence Against Anxiety. TheTavistock Institute of Human Relationships.
Mid-Western Health Board (2001) Strategy forAcute Hospital Services. Mid-Western HealthBoard.
Munro, K., Cook, F., Crawford, A. and Kilbride, L.(2004) Developing and Accrediting a ContinuingProfessional Development Framework. NursingStandard. 19 (8), 40-44.
National Council for the ProfessionalDevelopment of Nursing and Midwifery (2004a)Framework for the Establishment of AdvancedNurse Practitioner and Advanced MidwifePractitioner Posts. 2nd Ed.Dublin: National Council for the ProfessionalDevelopment of Nursing and Midwifery
National Council for the ProfessionalDevelopment of Nursing and Midwifery(2004b) Report on the Continuing ProfessionalDevelopment of Staff Nurses and Staff Midwives.Dublin: National Council for the ProfessionalDevelopment of Nursing and Midwifery
National Council for the ProfessionalDevelopment of Nursing and Midwifery(2004c) An Evaluation of the Effectiveness ofthe Role of the Clinical Nurse/MidwifeSpecialist.Dublin: National Council for the ProfessionalDevelopment of Nursing and Midwifery
National Council for the ProfessionalDevelopment of Nursing and Midwifery (2003a)Agenda for the Future ProfessionalDevelopment of Nursing and Midwifery.Dublin: National Council for the ProfessionalDevelopment of Nursing and Midwifery
National Council for the ProfessionalDevelopment of Nursing and Midwifery (2003b)Guidelines for Portfolio Development for Nursesand Midwives.Dublin: National Council for the ProfessionalDevelopment of Nursing and Midwifery
National Council for the ProfessionalDevelopment of Nursing and Midwifery (2001)Clinical Nurse / Midwife Specialists –Intermediate Pathway.Dublin: National Council for the ProfessionalDevelopment of Nursing and Midwifery
National Qualification Authority of Ireland(2003) The National Framework ofQualifications: A framework for thedevelopment, recognition and award ofqualifications in Ireland, National QualificationsAuthority of Ireland, Dublin.http:/www.nqai.ie/publications
Nursing and Midwifery Planning andDevelopment Unit, Mid-Western Region (2003)An Explorative Study into the Expansion ofNursing and Midwifery Professional Roles inresponse to the European Working TimeDirective.
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
58

Office for Health Management (2004)Management Competency User Pack: For Nurseand Midwife Managers. OHM: Dublin.
Office for Health Management (2003) Reporton an Evaluation Study of the Leading anEmpowered Organisation Programme (LEO)for Clinical Nurse Managers.OHM: Dublin.
Office for Health Management (2003) Dialogueon Implementing Reform – Communication &Consultation Programme. OHM: Dublin.
Porter-O’Grady, T. (1999) Quantum Leadership:New Roles for a New Age. Journal of NursingAdministration. 29(10): 37-42.
Rodwell, C. M. (1996) An analysis of the conceptof empowerment. Journal of Advanced Nursing.23: 305-313
Rushforth, H. and Glasper, E.A. (1999)Implications of nursing role expansion forprofessional practice. British Journal of Nursing.8(22): 1507 – 1513.
Scally, G. and Donaldson, L.J. (1998) Clinicalgovernance and the drive for qualityimprovement in the new NHS in England.British Medical Journal, 4 July, 61-65.
Scottish Executive Health Department(2004a) Framework for Developing NursingRoles (Consultation). Edinburgh: The StationeryOffice.
Scottish Executive Health Department (2004b)Leadership Development Framework: ForDiscussion. Edinburgh: The Stationery Office.
Scottish Executive Health Department (2003a)New Nursing Roles: Deciding the future forScotland. Consensus Statement. Edinburgh:The Stationery Office.
Scottish Executive Health Department (2003b)Safe and Effective Care: Generic ClinicalGovernance Standards. Edinburgh: TheStationery Office.
Scottish Executive Health Department (2001)Caring for Scotland: The Strategy for Nursingand Midwifery in Scotland. Edinburgh: TheStationery Office.
Valentine, S.O. (2002) Nursing Leadership andthe New Nurse. Charlotte: University of NorthCarolina.
Strategy & Action Plan for N
ursing & M
idwifery
59

60
Stra
tegy
& A
ctio
n Pl
an fo
r Nur
sing
& M
idw
ifery
Mid-Western RegionalMaternity Hospital Limerick
Mid-Western RegionalHospital Limerick
Mid-Western RegionalHospital Ennis
Mid-Western RegionalOrthopaedic Hospital
St. John’s HospitalLimerick
Mid-Western RegionalHospital Nenagh
Regional Steering Group for the Strategic Development of Nursing and Midwifery in the Acute Hospital Services

Regional Steering Group for the Strategic Development of Nursing and Midwifery in the Acute Hospital Services
Kay Hogan Director of Nursing St. John’s Hospital Limerick
Mary Carey Assistant Director of Nursing St. John’s Hospital Limerick
Kay Chawke Assistant Director of Nursing Mid-Western Regional Orthopaedic Hospital
Joan Broderick Assistant Director of Nursing Mid-Western Regional Orthopaedic Hospital
Joan Somers Meaney Director of Nursing Mid-Western Regional Hospital Ennis
Barbara Madigan Assistant Director of Nursing Mid-Western Regional Hospital Ennis
Maura Fitzgerald Deputy Director of Nursing Mid-Western Regional Hospitals
Joan Quinn-Chaplin Assistant Director of Nursing Mid-Western Regional Hospital Limerick
Brenda Egan Assistant Director of Nursing Mid-Western Regional Hospital Limerick
Gerardine Kennedy Nurse Practice Development Mid-Western Regional Hospitals LimerickCo-ordinator
Peig Harnett Assistant Director of Nursing Mid-Western Regional Hospital Limerick
Mary O Brien Assistant Director of Nursing Mid-Western Regional Hospital Limerick
Catherine Hand Assistant Director of Nursing Mid-Western Regional Hospital Limerick
Maura Cahill Assistant Director of Nursing Mid-Western Regional Hospital Ennis
Patrick Cleary Director of Nursing Mid-Western Regional Hospital Nenagh
Mary O Donoghue Assistant Director of Nursing Mid-Western Regional Hospital Nenagh
Margaret Quigley Assistant Director of Midwifery Mid-Western Regional Maternity Hospital Limerick
Noreen Keane Assistant Director of Midwifery Mid-Western Regional Maternity Hospital Limerick
Cora Lunn Project Officer for the Nursing and Midwifery Planning and Development of Development UnitPost-Graduate Education
James Costelloe Clinical Nurse Manager 3 Mid-Western Regional Hospital Ennis
Marie Casey Regional Professional Nursing and Midwifery Planning and Development Officer Development Unit
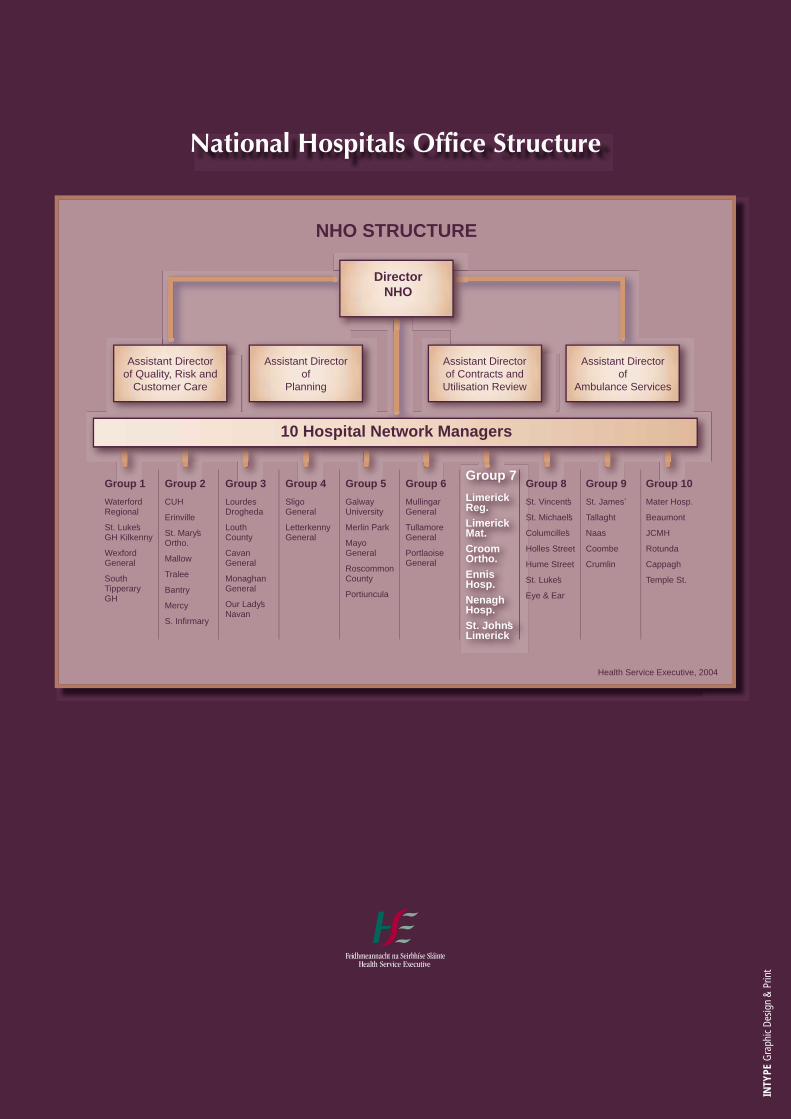
National Hospitals Office Structure
10 Hospital Network Managers
Assistant Directorof Quality, Risk and
Customer Care
Assistant Directorof
Planning
Assistant Directorof Contracts andUtilisation Review
Assistant Directorof
Ambulance Services
DirectorNHO
NHO STRUCTURE
Health Service Executive, 2004
Group 1
Waterford Regional
St. Lukeʼs GH Kilkenny
Wexford General
South Tipperary GH
Group 2
CUH
Erinville
St. Maryʼs Ortho.
Mallow
Tralee
Bantry
Mercy
S. Infirmary
Group 3
Lourdes Drogheda
Louth County
Cavan General
Monaghan General
Our Ladyʼs Navan
Group 4
Sligo General
Letterkenny General
Group 5
Galway University
Merlin Park
Mayo General
Roscommon County
Portiuncula
Group 7
LimerickReg.LimerickMat.CroomOrtho.EnnisHosp.NenaghHosp.St. JohnʼsLimerick
Group 8
St. Vincentʼs
St. Michaelʼs
Columcilleʼs
Holles Street
Hume Street
St. Lukeʼs
Eye & Ear
Group 9
St. Jamesʼ
Tallaght
Naas
Coombe
Crumlin
Group 10
Mater Hosp.
Beaumont
JCMH
Rotunda
Cappagh
Temple St.
Group 6
Mullingar General
Tullamore General
Portlaoise General
Strategy & Action Plan
for Nursing & Midwifery
INTY
PEG
raph
ic D
esig
n &
Prin
t













![emlakkulisi.com...Netcad 5.0 GIS for Windows - Proje ÇiZ Düzenle Görüntü PARSELASYON PLANI-2. [PARSELASYON PLANI- Araçlar 2. NCZ] Raster Netmap Hesap 398230.361](https://static.fdocuments.in/doc/165x107/5e63ecff478f5f4ca612c9cc/-netcad-50-gis-for-windows-proje-iz-dzenle-grnt-parselasyon-plani-2.jpg)




