ACLS Arrhythmias and Treatment Modalities
33
ACLS Arrhythmias and Treatment Modalities Presented by CMR CPR (a division of CMR Medical Supply, LLC) An American Heart Association Affiliated Training Site
Transcript of ACLS Arrhythmias and Treatment Modalities

ACLS Arrhythmias and Treatment Modalities
Presented by CMR CPR (a division of CMR Medical Supply, LLC)
An American Heart Association Affiliated Training Site

DISCLAIMER
• The following information is provided by the American Heart Association.
• Monies collected do not represent income for the American Heart
Association. • Please review and study your American
Heart Association ACLS Manual before attempting to complete the AHA ACLS
Course.

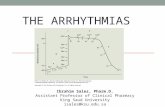
QRS Complex
P wave indicates Atrial depolarization. QRS complex indicates Ventricular depolarization
T wave indicates re-polarization

Normal Sinus Rhythm

1st Degree Heart Block
• Usually benign, very common
• Not treatable in ACLS
• Progressively gets worse over time
• Not actually a block- just a delay in conduction
• PRI- >20 (4 small boxes)
• Normally regular

2nd Degree Heart Block, type 1 aka “Wenckebach”
• Usually Irregular
• Not treatable in ACLS
• PRI- Long, long, longer, DROP- must be a Wenckebach!

2nd Degree, Type 2 Heart Block
• Blocked P waves/dropped QRS Complexes
• Usually 1 or 2 additional P waves
• This is getting worse…

3rd Degree Heart Block (Complete Heart Block)
• Malignant
• Usually Bradycardic, Irregular
• Won’t take long…NEED TO TREAT!
• P waves regular, not associated w/ QRS complexes

Supra Ventricular Tachycardia (SVT)
• Firing somewhere above the Ventricles
• Treatable over 150 BPM per ACLS
• Regular and FAST!

Ventricular Tachycardia (V- tach with or w/o Pulses)
• Extremely dangerous arrhythmia
• Patient wont last long
• Wide and Bizarre pattern, but regular
• Shock-able rhythm (if no pulse present)

Torsades de Pointes
• Translates to: “Twisted of the Spikes”
• Described as Polymorphic Tachycardia
• May degenerate to V-Fib if persistent
• Caused by HYPOkalemia/HYPOmagnasemia

Ventricular Fibrillation (V-Fib)
• Won’t have a pulse
• Fine or coarse
• Shock-able rhythm
• Patient is in CARDIAC ARREST at this point

Pulseless Electrical Activity (PEA)
• ANY rhythm can be PEA as long as it doesn’t have a PULSE!
• YOU MUST CHECK A PULSE WITH EVERY RHYTHM- In a Cardiac Arrest!

Asystole (Flat line)
• Heart not producing ANY electrical activity
• NON-Shock-able Rhythm
• Patient is DEAD

Acute M.I. (Leads 2,3 & aVF)

ACLS DRUGS
Atropine
• Derived from the Nightshade Plant (deadly)
• Dilates pupils, increases heart rate
• Used to treat symptomatic bradycardia
• No longer used for PEA
DOSE: 0.5 mg with a maximum of 3.0 mg

ACLS DRUGS
Adenosine
• Inhibits neurotransmitters
• “Resets” heart
• Asystole for 3-5 seconds
• Causes a transient heart block in the AV node
• Used to treat Asymptomatic SVT over 150bpm
• NOT for wide complex IRREGULAR V -Tach
DOSE: 6.0 mg then 12.0 mg

ACLS DRUGS
Amiodarone Bolus
• Anti-arrythmic
• Works on the Atria and the Ventricles
DOSE: 300 mg then 150 mg. MAX: 450 mg

ACLS DRUGS Epinephrine (Bolus)
• Hormone naturally occurring in the body
• Affects the Sympathetic Nervous System
• Constricts blood vessels, increases peripheral resistance
• Increases Heart Rate (Inotropic effects and Chronotropic effects) (electricity and rate)
DOSE: 1.0 mg NO MAX DOSE!

ACLS DRUGS Vasopressin
• Anti-diuretic hormone
• Retains water in the body and constricts blood vessels
• May be used in cardiac arrest in place of 1st or second dose of epinephrine
• Half life is 10-20 minutes
DOSE: 40 units

ACLS DRUGS
Dopamine
• Second-line drug for symptomatic bradycardia when atropine is not effective
• Used for cardiogenic shock in the absence of hypovolemia
Dose: 2-10 micrograms/kg/min infusion

ACLS DRUGS
Epinephrine (Infusion)
• Second-line drug for symptomatic bradycardia when atropine is not effective. Choose EPI or Dopamine
Dose: 2-10 micrograms/kg/min infusion

ACLS DRUGS
Magnesium Sulfate
• For the treatment of Torsades with pulses present
Dose: 1-2 Grams

H’s and T’s
• Hypovolemia
• Hypoxia
• Hydrogen Ions (acidosis)
• Hyper/Hypo kalemia
• Hypothermia
• Toxins
• Tamponade (cardiac)
• Tension Pneumothorax
• Thrombosis (coronary)

Circular Algorithm

Treatment Modalities per ACLS
• V-FIB or (V-TACH w/o pulses) are the only shock-able rhythms.
• Start at 360J, and continue at 360J* (With a MONO-phasic Defibrillator)
• High Quality CPR
• EPI or (Vasopressin, 1st or 2nd dose)
• Amiodarone- 300mg, then 150mg (450mg MAX)

SVT
• Treatable at 150 BPM
• Use Valsalva Maneuver First (Think BLS)
• Stable= Drugs. Adenosine 6mg, 12mg, done
• Unstable= Electricity. Synchronized Cardioversion. (sedate first) 100 J,200J, 300J 360J* (discussed in class)
• MAKE SURE YOU PUSH SYNCH BUTTON!
• Be careful w/ rapid A fib- throw a clot…BAD

V-TACH w/PULSES (Regular)
• Dangerous arrhythmia- PT. wont last long
• Valsalva maneuver first (Think BLS)
• Stable= Use Adenosine
• Unstable= Electricity (Monophasic)
• 100J,200J, 300J 360J
• Try to sedate first. Don’t delay treatment.
• PT. will usually be UNSTABLE!

V-Tach (Irregular, Torsades)
• Dangerous arrhythmia- PT. wont last long
• Valsalva maneuver first (Think BLS)
• Stable= Adenosine- not indicated.
• Magnesium Sulfate
• Electricity. 100J,200J, 300J 360J (Monophasic)

Bradycardias
• Less than 60 BPM
• Stable= DO NOT TREAT- watch patient
• Unstable= (1) Atropine (2) Dopamine or EPI Drip (3)Pacing…

Pacing
• Apply D-Fib Pads on Pt
• Set Pacer at 80 bpm
• Increase mA until 1 pacer spike precedes QRS
• Check Femoral Artery for pulse that matches monitor
• If is doesn’t, increase mA until it does

PEA (Pulsless Electrical Activity)
• A rhythm that appears on a monitor to have a pulse, but does not when the pulse is checked
• High quality CPR
• Epinephrine, 1.0 mg
• NON- SHOCKABLE!

Complete Heart Block (3rd degree)
• The use of Atropine is not indicated
• Transcutaneous pacing
• Fluids
• Oxygen
• Cardiology consult