Acl Injury and It's Management
133
ACL Injury and it¶s MANAGEMENT Chair person:DR.A.K.Mannur Speaker:Dr.Dorai 03-11-2007
-
Upload
sunil-kumar-pd -
Category
Documents
-
view
225 -
download
0
Transcript of Acl Injury and It's Management

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 1/133
ACL Injury and it¶s
MANAGEMENT
Chair person:DR.A.K.Mannur Speaker:Dr.Dorai03-11-2007

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 2/133
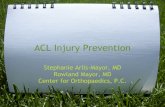
AnatomyMarshall, and Al
Monajem described
the anterior cruciateligament as a two-bundle ligament,consisting of a smallanteromedial and alarger posterolateralbundle.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 3/133
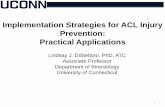
ACL originates from the posterior part of the medial surface of the lateral femoralcondyle within the condylar notch wellposterior to the longitudinal axis of thefemoral shaft.
It inserts on the tibial plateau , medial to
the insertion of the anterior horn of thelateral meniscus in a depressed areaanterolateral to the anterior tibial spine.
The tibial attachment site is larger andmore secure than the femoral site.
The ligament is 31 to 35 mm in length and31.3 mm2 in cross section.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 4/133
The primary blood supply to the ligament is fromthe middle geniculate artery.
Additional supply comes from the retropatellar fat pad via the inferior medial and lateralgeniculate arteries.
This source plays a more important role whenthe ligament is injured.
The posterior articular nerve , a branch of thetibial nerve innervates the acl

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 5/133
The ACL functions
to prevent prevent anterior anterior displacement of displacement of the tibia on thethe tibia on thefemur.femur.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 6/133
BiomechanicsThe ACL is the primaryrestraint to anterior tibial displacement.
According tobiomechanical tests byNoyes et al., it accountsfor approximately 85%of the resistance to theanterior drawer testwhen the knee is at 90degrees flexion andneutral rotation.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 7/133
S elective sectioning of the ACL has shown that
the anteromedial bandis tight in flexion,providing the primaryrestraint, whereas theposterolateral bulkyportion of this ligament
is tight in extension .The posterolateralbundle provides theprincipal resistance for hyperextension.The normal ACL hasbeen shown to carryloads throughout theentire range of flexionand extension of theknee.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 8/133
KNEE B IOMECHANICS OF ACL&PCL

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 9/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 10/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 11/133
H IS TORY AND P H YS ICALEXAMINATIONThe classic history of an anterior cruciateligament injury begins with a non contact
deceleration, jumping, or cutting action .Obviously, other mechanisms of injury includeexternal forces applied to the knee.The patient often describes the knee as having
been hyper extended or popping out of joint andthen reducing. A pop is frequently heard or felt.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 12/133
The patient usually has fallen to theground and is not immediately able to getup.
Within a few hours, the knee swells, andaspiration of the joint revealshaemarthrosis. In this scenario, the
likelihood of an anterior cruciate ligamentinjury is greater than 70%.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 13/133
Knee ligaments often are injured in athleticactivities, such as American football.Skiing, ice hockey, gymnastics, tennis andother sports
Motor vehicle accidents ,Ligament disruption can occur without a
fall or direct contact when sudden, severeloading or tension is placed on theligaments, such as when a running athleteplants a foot to suddenly decelerate orchange directions .
ETIOLOGY

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 14/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 15/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 16/133
The unhappy triad of O'DonoghueWhen abduction, flexion, and internal rotationof the femur on the tibia occur, the medialsupporting structures³ the tibial collateral
ligament and the medial capsular ligament ³ are the initial structures injured. If the forceis of sufficient magnitude, the anterior cruciate ligament also can be torn. Themedial meniscus may be trapped between thecondyles of the femur and the tibia, and itmay be torn at its periphery as the medialstructures tear, thus producing ´the unhappytriadµ of O'Donoghue.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 17/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 18/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 19/133
The Lachman test has a sensitivity of 95%.The pivot shift test requires a relaxed patient andan intact medial collateral ligament.When positive, this test reproduces the
pathological motion in an anterior cruciateligament-deficient knee and is easier to elicit in achronic anterior cruciate ligament disruption or inan anesthetized patient with an acute anterior
cruciate ligament injury.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 20/133
Lachman TestThe Lachman test can be useful if the knee isswollen and painful . The patient is placedsupine on the examining table with theinvolved extremity to the examiner's side .The involved extremity is positioned in slightexternal rotation and the knee between fullextension and 15 degrees of flexion; thefemur is stabilized with one hand, and firmpressure is applied to the posterior aspect of the proximal tibia, which is lifted forward inan attempt to translate it anteriorly.
The position of the examiner's hands isimportant in doing the test properly.
P H YS ICAL EXAMINATION

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 21/133
One hand should firmly stabilize the
femur while the other grips the proximal tibiain such a manner that the thumb lies onthe anteromedial joint margin.When an anteriorly directed lifting force
is applied by the palm and the fingers,anterior translation of the tibia inrelation to the femur can be palpated bythe thumb.
Anterior translation of the tibiaassociated with a soft or a mushy endpoint indicates a positive test.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 22/133
Anterior drawer testP H YS ICAL EXAMINATION

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 23/133
Anterior drawer test
W ith the patient supine on the examining table, thehip is flexed to 45 degrees and the knee to 90degrees, with the foot placed on the table top. Thedorsum of the patient's foot is sat on to stabilize it,and both hands are placed behind the knee to feelfor relaxation of the hamstring muscles .The proximal part of the leg then is gently and
repeatedly pulled and pushed anteriorly andposteriorly, noting the movement of the tibia on thefemur.
P H YS ICAL EXAMINATION

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 24/133
The test is done in three positionsof rotation, initially with the tibiain neutral rotation and then in 30
degrees of external rotation.Internal rotation to 30 degrees
may tighten the posterior cruciate enough to obliterate anotherwise positive anterior drawer test .

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 25/133
The degree of displacement in eachposition of rotation is recorded andcompared with the normal knee. Ananterior drawer sign 6 to 8 mm greater than that of the opposite knee indicates atorn anterior cruciate ligament.However, before applying anterior drawer stress, the examiner must make sure that
the tibia is not sagging posteriorly as aresult of laxity of the posterior cruciateligament.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 26/133
Any tendency of one tibial plateau to rotateabnormally should be noted as the test iscarried out.In an acutely painful knee it may not be
possible to carry out the anterior drawer testin the conventional 90-degree flexed position.Small degrees of anterior translation of thetibia on the femur may be detected better inthe relatively extended position, in which the
´doorstopµ effect of the posterior horn of themenisci is negated .

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 27/133
Anterior drawer sign

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 28/133
Lachman Test
P H YS ICAL EXAMINATION

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 29/133
When viewed from the lateral
aspect, a silhouette of the inferior pole of the patella, patellar tendon,and proximal tibia shows slightconcavity. With disruption of theanterior cruciate ligament, anterior translation of the tibia obliteratesthe patellar tendon slope.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 30/133
Roentgenographic studies
Plain roentgenograms often arenormal; however, a tibial
eminence fracture indicates anavulsion of the tibial attachment of the anterior cruciate ligament.The Segond fracture , or avulsionfracture of the lateral capsule , ispathognomonic of an anterior cruciate ligament tear

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 31/133
Recent studies have
implicated gender andfemoral intercondylar notch width as factorscontributing to injury of the anterior cruciate
ligament. Numerousinvestigators havereported that athletessustaining non contactanterior cruciate ligamenttears have statisticallysignificant intercondylar notch stenosis.
Notch width index

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 32/133
Souryal and Freemanformulated the notchwidth index, which isthe ratio of the widthof the intercondylar notch to the width of the distal femur at thelevel of the poplitealgroove measured ona tunnel viewroentgenogram of theknee

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 33/133
. The normal intercondylar notch ratio was0.231 ± 0.044. The intercondylar notchwidth index for men was larger than thatfor women

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 34/133
Magnetic resonance imagingshowing bone bruise after anterior cruciate ligament tear.
MRI is the most helpfuldiagnosticroentgenographictechnique.
The reported accuracyfor detecting tears of theanterior cruciateligament has rangedfrom 70% to 100%.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 35/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 36/133
TREATMENT
The treatment options available includenonoperative management,repair of the anterior cruciate ligament,
either isolated or with augmentation,and reconstruction with either autograft or
allograft tissues or synthetics.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 37/133
Nonoperative treatment is a viable optionfor sedentary occupations, low athleticdemands, or who were older than 30 yearsand a patient who is willing to makelifestyle changes and avoid the activities
that cause recurrent instability.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 38/133
If a nonoperative approach is chosen, it shouldinclude an aggressive rehabilitation program and
counseling about activity level.The use of a functional knee brace iscontroversial and has not been shown to reducethe incidence of reinjury significantly if a patientreturns to high-level sports.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 39/133
C onservative treatment involves the re-
education of the quadriceps and hamstring
muscles. Emphasis should be placed on
the hamstrings as they can restrict theamount of anterior tibial translation on the
femur.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 40/133
O perative treatment
ACL reconstruction is done traditionally usingeither an intra-articular reconstruction, an extra-
articular reconstruction, or a combination of both.Isolated extra-articular reconstruction may be
useful in the skeletally immature, when there isconcern about damage to the growing physis. Inisolation, extra-articular reconstruction is proneto failure within3 to 5 years.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 41/133
O perative treatment
Primary intra-articular repair often fails unless there isclear evidence of bony avulsion from either the femoralor tibial attachments, where this can be reapposed.In the majority of cases a reconstructive technique isrequired and a bone-patellar-tendon-bone or hamstringgraft is the most frequently used method of reconstruction. These grafts may be used in conjunctionwith an extra-articular tenodesis (MacIntosh typetwo)augment stability.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 42/133
Continued ««««..Those patients requiring reconstruction wereyounger and had a higher preinjury activity leveland a stronger desire to stay at that levelThree factors known at the time of the initialexamination that correlated with the need for surgery:younger age ,preinjury hours of sports participation,andamount of anterior instability as measured by
the KT-1000 arthrometer.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 43/133
Primary repair of the anterior cruciate ligament is
no longer preferred but reconstruction severalweeks after the acute injury is preferred .
Acute repair is appropriate when a bonyavulsion occurs with the anterior cruciateligament attached. The avulsed bone fragmentoften can be replaced and fixed with sutures or passed through transosseous drill holes or screws placed through the fragment into thebed. Anterior cruciate ligament avulsions usuallyoccur from the tibial insertion.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 44/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 45/133
Intraarticular Reconstruction .The advances made in arthroscopy haveled to the development of arthroscopictechniques for anterior cruciate ligamentreconstruction.Increased understanding of technicalissues of graft selection, placement,tensioning, and fixation, as well aspostoperative rehabilitation, led todramatically improved results comparedwith previous intraarticular reconstructions.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 46/133
These same principles can be applied toopen intraarticular reconstruction of the
anterior cruciate ligament through a smallarthrotomy incision, which preservesattachment of the vastus medialis obliquusmuscle to the patella, or through thepatellar tendon defect when the centralthird is used as a graft source.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 47/133
G raft S election.
Autograft tissue is used most commonly,but allografts and synthetics also are
available . Autografts have the advantages of low riskof adverse inflammatory reaction andvirtually no risk of disease transmission.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 48/133
Continued ««««..
As a biological graft, it undergoesrevascularization and recollagenization,but initially a 50% loss of graft strengthoccurs after implantation.Therefore it is desirable to begin with a
graft stronger than the tissue to bereplaced.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 49/133
The most common currentgraft choices arebone-patellar tendon-bone
graftquadrupled hamstring
tendon graft
andQuadriceps tendon graft

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 50/133
The bone-patellar tendon-bone graftusually is an 8- to 11-mm wide graft takenfrom the central third of the patellar tendon, with its adjacent patella and tibial
bone blocks.This graft's attractive features include its
high ultimate tensile load (approximately2300 N), its stiffness (approximately620N/mm), and the possibility for rigidfixation with its attached bony ends

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 51/133
The use of the hamstring tendon graft and
quadriceps tendon graft has increased inrecent years because of their relativelylow donor site morbidity.This quadriceps graft has become analternative replacement graft, especiallyfor revision anterior cruciate ligamentsurgeries and for knees with multiple
ligament injuries.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 52/133
G raft Placement.The preferred location has been isometricplacement of the graft that limits changes ingraft length and tension during knee flexionand extension, which possibly may lead to
overstretching or failure of the graft. Although both the tibial and femoralattachment sites are important, errors in thefemoral site are more critical because of the
closer proximity to the center of axis of kneemotion.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 53/133
A femoral tunnel that is too anterior willresult in lengthening of the intraarticular
distance between tunnels with kneeflexion.Posterior placement of the femoral tunnelproduces a graft that is taut in extensionbut loosens with flexion. This locationproduces an acceptable result.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 54/133
Currently, most surgeons advocate placing
the graft at the posterior portion of theanterior cruciate ligament tibial insertionsite near the posterolateral bundle positionfor best reproduction of the function of the
intact anterior cruciate ligament.This location also decreases graftimpingement against the roof of theintercondylar notch with knee extensionthat can occur with anterior placement.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 55/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 56/133
A bony ridge (³resident's ridge´) anterior tothe femoral attachment of the anterior cruciate ligament should be removed, if present, since it impairs the proper
identification of the femoral attachmentsite and also hinders the proper placementof the over-the-top guides used for drillingthe femoral tunnel.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 57/133
G raft Tension.
The application of tension to the graft atthe time of initial fixation can significantlyalter joint kinematics and in situ forces inthe graft during knee motion.Theoretically, the desired tension in thegraft should be sufficient to obliterate theinstability (Lachman test). Too muchtension may ³capture´ the joint, resulting indifficulty in regaining motion, or it may leadto articular degeneration from altered jointkinematics.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 58/133
Less tension was required for a bone-patellar tendon-bone graft than asemitendinosus graft because the tendonportion of the former was shorter andstiffer.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 59/133
Initial graft tension remains controversial,as the in situ forces in the anterior cruciateligament during daily activities areunknown.
In addition, the significance of theviscoelastic behavior of the anterior cruciate ligament replacement grafts hasnot been entirely characterized.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 60/133
G raft Fixation.
Fixation of replacementgrafts can be
classified intodirect andindirect method .

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 61/133
Direct fixation devices include interferencescrews, staples, washers, and crosspins.Indirect fixation devices include polyester
tape-titanium button and suture-post.
Interference screw fixation is the mostpopular fixation method for bone-patellar tendon-bone grafts

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 62/133
complications of the interference
screw fixation(1) inadvertent graftadvancement can
occur unless constanttension is applied tothe bone plug as thescrew is inserted.
Appropriate graft fixation byinterference screw ( left) andinappropriate graft advancement byscrew (right).

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 63/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 64/133
(3) the screw threadcan lacerate the
tendon if the tip of thescrew protrudesbeyond the end of thebone plug Proper relationship of
interference screw to bonegraft ( left) and improper advancement of screw leadingto potential tendon injury( right) .

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 65/133
ACL Reconstruction Using Bone-Patellar Tendon-Bone G raft
Modified Clancy t e chn ique . A, S ingle sk in in c i s ion . B, A n t eromedial and la t eral in c i s ion s .

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 66/133
A, Release of graft with
patellar and tibial tuberositybony attachments. B,Removal of segment of tibial tuberosity.
G raft freed from tibialtuberosity .

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 67/133
A, Free, nonvascularized, bone-tendon-bone graft:patellar bone is 5 mm thick, 10 mm wide, and 2 to 3 cm
long and is connected to 10-mm wide full-thicknesspatellar tendon attached topiece of tibial tuberosity 8 mm thick, 10 mm wide, and 2to 3 cm long. B, S utures are placed through holes inbony portions of graft.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 68/133
Intercondylar notch can be exploredthrough defect in patellar tendon createdby harvesting of graft.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 69/133
S mall curet marks femoral anatomical attachmentsite.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 70/133
Correct positioning of pilot holes for right knee(A) and left knee (B) .

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 71/133
Exit site for femoral tunnel 3 to 4 cmproximal to lateral femoral epicondyle.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 72/133
Incorrect ( top) and correct ( bottom) positioning of graft.Bone plug should not be too far into tunnel to avoid wear on tendinous part of graft.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 73/133
Reconstruction Using H amstringTendons.
The use of H amstring tendon graft for ACL reconstructions has increased inpopularity.Initially, the semitendinosus tendonand gracilis tendon were used together as two single strands. Their initialcombined strength according to Noyes'research exceeded that of the anterior cruciate ligament.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 74/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 75/133
More recently surgeons have chosen
to fold the semitendinosus andgracilis tendons upon themselves,creating four strands and theoretically
doubling the strength of the graftconstruct.Others have chosen to use only the
semitendinosus tendon and folding iton itself to create either three or four strands.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 76/133
Anterior Cruciate Ligament ReconstructionUsing H amstrings (with Proximal Release of H amstrings )
Anterior cruciate ligament reconstruction with hamstrings .
.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 77/133
Two-screw fixation of hamstring graft in tibial tunnel

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 78/133
Currently, extraarticular procedures are usedprimarily in conjunction with an intraarticular reconstruction when severe anterior instability isdue to injury or late stretching of the secondary
stabilizing capsular structures or the lateral sideof the knee.Extraarticular techniques described are those of MacIntosh, Losee, and Andrews (iliotibial bandtenodesis and bicepsplasty).
E xtra articular procedures

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 79/133
MacIntosh technique of lateralreconstruction using strip of iliotibial band
Dissect a 1.5-cm wide strip of iliotibial band from its midportion
beginning approximately16 cm from its distal insertionand turn it down to itsattachment at the Gerdytubercle.
Pass this strip of iliotibial bandto the posterolateral corner of the knee through a tunnel deepto the lateral collateral ligament

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 80/133
Losee modification of MacIntosh technique of lateral
reconstruction using iliotibial band. A, Fascial strip (18cmlong × 1.5 cm wide) of iliotibial tract attached to Gerdytubercle. B , Imbrication through lateral head of gastrocnemius plus posterolateral corner. C, Rerouting of fascial strip deep to fibular collateral ligament, reattachingit to Gerdy tubercle.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 81/133
H old the iliotibial tractagainst the distal femur bysutures passed through the
track and through two parallelholes in the distal femur andtied to each other on themedial side of the femur,
beneath the vastus medialis .
Andrews ³minireconstruction´ technique

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 82/133
By fixing the tract to the distal femur, aligament is created that closely approximates
the biomechanical function of the anterior cruciate ligament, extending from the distalfemur to the G erdy tubercle and preventinganterolateral subluxation of the lateral tibial
plateau on the lateral femoral condyle .

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 83/133
A, Two points on lateral femoral condylecorresponding to major femoral intraarticular attachments of anterior cruciate ligament.B, Posterior band tight in extension.C, Anterior band tight in flexion.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 84/133
AFTERTREATMENT.
At 5 days after surgery the wound is inspectedand the cast changed. The cast is removed at 6weeks.Not to rigidly immobilize the knee in flexion for
several weeks because of the deterioration of the articular cartilage surfaces associated withthe absence of motion, especially in thepatellofemoral joint.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 85/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 86/133
Complications of Anterior CruciateLigament S urgery
Complications of anterior cruciate ligamentsurgery can be caused by preoperative,
intraoperative, and postoperative factors.Preoperative factors include appropriate
timing of surgery, adequate preoperative
conditioning and strengthening, and graftand fixation choices.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 87/133
Intraoperative complications includepatellar fracture, inadequate graft length,
mismatch between the bone plug andtunnel sizes, graft fracture, suturelaceration, violation of the posterior femoral cortex, and incorrect femoral or tibial tunnel placement.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 88/133
The most common postoperativecomplications are motion (primarily
extension) deficits and persistent anterior knee pain. Anterior knee pain probably is the mostcommon and most persistent complicationafter anterior cruciate ligamentreconstruction.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 89/133
Motion loss after anterior cruciateligament reconstruction can result from
preoperative, intraoperative, or postoperative factors. Preoperativeeffusion, limited range of motion, and
concomitant knee ligament injuries makepoor postoperative motion more likely.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 90/133
Intraoperative factors associated withmotion deficits most often are incorrecttunnel position and inadequatenotchplasty, which can result in over tightening or impingement of the graft,leading to loss of extension.Postoperative factors include prolongedimmobilization and inadequate or inappropriate rehabilitation.
S ynthetic Materials for Ligament

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 91/133
S ynthetic Materials for LigamentReconstruction.
Artificial ligaments (Gore-Tex ligament, theStryker Dacron ligament, and Leeds-Keioprostheses) offer a number of theoretical
advantages compared with reconstruction usingautogenous tissues: no autogenous tissues aresacrificed, and the increased morbidityassociated with the harvest of autogenoustissues is avoided.
If autogenous tissues have been used in afailed reconstruction or if they are unacceptable,

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 92/133
the use of a readily available synthetic device isappealing.
Artificial ligaments generally permit a simpler and easier reconstructive technique, frequentlyarthroscopic, and they allow a more rapidrehabilitation because they do not become weak
during tissue revascularization andreorganization.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 93/133
Artificial ligaments function in one of threeways:(1) as a prosthetic ligament; that is, theprosthesis is implanted as a permanentreplacement for the normal ligament;(2) as a stent temporarily protecting or
augmenting an autogenous graft; or (3) as a scaffold providing support for andstimulating the in growth of collagentissue.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 94/133
S ynthetic Augmentation for Anterior Cruciate
Ligament Repair or Reconstruction. ( Kennedy)
The Ligament Augmentation Device(LAD), developed with the 3M Co., is a
braided, polypropylene, synthetic ribbonthat is inserted along with the biologicalgraft tissue in the form of a compositebiological-synthetic graft.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 95/133
The purpose of the synthetic augmentationdevice was to enhance the initial graft strength,to allow for immediate proper intraoperativetensioning of the graft, and to provide for moresecure fixation of the graft.The LAD has been used in conjunction with theMarshall-Macintosh technique, the iliotibial band,and the hamstring tendons, as well as withpatellar bone-tendon-bone grafts and allografts.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 96/133
Allograft Ligament Replacement
The ideal ligament replacement should bereadily available; it should be of sufficient lengthand diameter; it should have biomechanicalproperties similar to the ligament it replaces; itshould not disturb normal structures; and itshould retain or develop a vascular supply. Although autogenous tissues currently are themost commonly used grafts for reconstruction of the cruciate ligament,

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 97/133
these transfers sacrifice a normalmusculotendinous structure in an alreadydeficient knee, adding to the functionaldisturbance. Extensive surgical exposure, longtourniquet times, and prolonged rehabilitationare other disadvantages of these techniques.collagen allografts appear capable of fulfillingmany of the requirements for an ideal ligamentsubstitute,

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 98/133
Autografts and allografts bothgo throughfour stages after transplantation: necrosis,
revascularization, cellular proliferation, andremodeling. After incorporation, however, neither autograft norallograft tendons have beendemonstrated to return to their originalstrength.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 99/133
Most reports show 30% to 40% ultimateload strengths. B ecause of this consistent
reductionin strength, use of grafts or combination of grafts that begin with morethan 100% of anterior cruciate ligamentstrength, which should result insufficientstrength after incorporation.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 100/133
Allografts can be sterilized either by sterileprocurement with careful donor screening or bysecondary sterilization with gaseous ethyleneoxide or gamma irradiation.The major concern in using allografttransplantation for ligament reconstructionremains the possibility of diseasetransmission,especially of hepatitis or acquiredimmune deficiency syndrome (AIDS).
h b l f

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 101/133
Rehabilitation after Anterior Cruciate LigamentReconstruction
The goal of rehabilitation after anterior cruciateligament surgery is to restore normal jointmotion and strength while protecting theligament graft. Appropriate rehabilitation iscrucial to the success of anterior cruciateligament reconstruction. Some stress to the graft
is desirable for healing and remodeling butshould not be excessive and disruptive.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 102/133
Intensive rehabilitation can help prevent earlyarthrofibrosis and restore strength and functionearlier. Perhaps the most important step is theearly restoration of full extension.Knee immobilization in a fully extended brace isstarted immediately after surgery to prevent
development of a flexion contracture.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 103/133
After isolated anterior cruciate ligamentreconstruction, partial weight-bearing withcrutches is allowed immediately. A straight legbrace is worn to support the weakenedquadriceps. Certain types of concurrentmeniscal repairs or articular cartilageprocedures may dictate a different weight-
bearing status. Usually crutches arediscontinued by 3 to 4 weeks postoperatively.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 104/133
Arthroscopy
Though arthroscopic Reconstruction of ACL is the present trend,
if the surgeon is not well versed with thearthroscope, open ACL reconstructionsurgery results are much better than
arthroscopic ACL reconstruction

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 105/133
Advantages
-The arthroscopically aided approach has the advantagesof smaller skin and capsular incisions,
less extensor mechanism trauma,Improved viewing of the intercondylar notch for placement of the tunnel and attachment sites,less postoperative pain,
fewer adhesions,
earlier motion, andeasier rehabilitation.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 106/133
The selection of grafts depends on thesurgeon's preference and the tissues
available. Among the autogenous tissues currentlyavailable, the most commonly used arecentral one third patellar tendon,
quadrupled hamstrings, and lesscommonly quadriceps tendon grafts.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 107/133
Techniques
Graft harvesting vertical skin incisionfrom inferior pole of patella to 1 cm medial
to tibial tubercle. Skin flap raised andpatellar tendon (central) of 1 cm width israised with two vertical incision frompatella to tibial tubercle. The bone plugs of
27mm length is removed with oscillatingsaw.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 108/133
Preparation of graft
Excess of soft tissue is removed from graftand diameter of bone plug is trimmed to
10mm and checked with templets. Theplug from the tibial tubercle is prepared for placement in the femoral tunnel. Holes aredrilled in graft to permit passage of no5
non-absorbable sutures to use later topass and tension the graft.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 109/133
Notch plasty-
A second suprapatellar inflow is used toimprove visualization. The remnant of ACL
are removed using intra-articular punchand then saver.Notch plasty is begun by removing about6mm of antero-lateral wall of notch using
burr. It is important to identify and removethe resident ridge.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 110/133
Drilling the tibial tunnel
A drill guide is set at 55* as more posterior tunnel preferred to prevent the
impingement.The tip is inserted through the medialportal and correct position is confermed.
The guide pin is inserted and tunnel isdrilled.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 111/133
Femoral Tunnel Preparation
With the knee flexed approximately 90 degrees, confirmthe previously chosen femoral pilot hole with an Arthrex7-mm offset femoral guide passed through the tibial
tunnel. The starting point is at the 11-o'clock position onthe right knee (1 o'clock on the left knee) approximately8 mm lateral to the posteriorcruciate ligament.
Advance a long guide wire through the guide to thechosen physiometric point on the posterolateral portion
of the femoral condyle.Pass a 10-mm endoscopic reamer over the previouslyplaced wire and ream.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 112/133
Graft Passage
Use the eyelet guide wire to pass the patellar bone plug guide suture up through
the femoral tunnel and then out through thelateral thigh. When the graft is about halfway intothe femoral tunnel, pass a flexible guide wirethrough either the medial portal place the wire
anterior to the graft and, with the wire parallel tothe graft, advance both up into the tibial tunnel.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 113/133
Graft Fixation
Place an 8-mm cannula with a cannulated screw withnoncutting threads through the medial portal or centralpatellar portal.
Tension the graft with about 8 to 10 pounds of pull. Over tensioning of the graft can cause failure because of jointcapture or graft necrosis. Secure the graft with an 8-mmscrew if the bone plug-to-tunnel gap is less than 2 mm;use a 9-mm screw if the gap is 3 mm or more. If the gap
is more than 5 mm, add a cancellous screw and washer post 1.5 cm distal to the tibial tunnel.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 114/133
Rehabilitation

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 115/133
Posterior drawer test
The posterior drawer test is done with the patientsupine and the knee flexed to 90 degrees;the foot is secured to the table by sitting on it. A posterior force is applied on the proximal tibia,which is opposite but similar to the force appliedin the anterior drawer test.Posterior movement of the tibia on the femur
demonstrates posterior instability whencompared with the normal tibia.
I i i diffi l i h h

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 116/133
It is sometimes difficult to interpret whether the tibia is abnormally moving too far
anteriorly or too far posteriorly.Careful attention to the neutral position or
unstressed reduction point preventsmisinterpretation.
B oth knees are placed in the position toperform a posterior drawer test, and a thumbis placed on each anteromedial joint line.Loss of the normal 1-cm anterior step-off of
the medial tibial plateau with respect to themedial femoral condyle indicates a tornposterior cruciate ligament .

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 117/133
As with the anterior drawer test, any
abnormal rotation of the tibial condylesis noted as the posterior drawer istested.To further evaluate stability, the
Posterior force applied to tibia andnormal patellar tendon slope.
Obliteration of patellar tendon slopewith disruption of anterior cruciateligament as forceful anterior translationof tibia takes place.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 118/133
Posterior Cruciate

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 119/133
Posterior Cruciate
LigamentImpact onanterior tibia.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 120/133
PCL Tear

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 121/133
The arteries supplying the joint

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 122/133
are the highest genicular (anastomotica magna), abranch of the femoral,the genicular branches of thepopliteal, the recurrent branchesof the anterior tibial, and the
descendingbranch from the lateral femoralcircumflex of the profundafemoris.20
The nerves are derived fromthe obturator, femoral, tibial, andcommon peroneal.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 123/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 124/133
ACL AND PCL

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 125/133
Two important intra-articular ligamentsthat provide static support to the kneeare the anterior (ACL) and posterior (PCL) cruciate ligaments.
Although the ligaments are intra-articular they are not contained withinthe joint capsule of the knee.The ACL extends from the anterior area
between the condyles of the tibia in aposterior and lateral direction to aposterior area on the medial surface of the lateral condyle of the femur.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 126/133
The PCL runs from a posterior depressionbetween the condyles of the tibia in ananterior and medial direction to the lateralside of the medial femoral condyle.The PCL functions to preventposterior translation of the tibiaon the femur.Additionally both the ACL and PCL serve toreduce rotation of the femur on the tibia. The
ligaments are tense in all positions, butincrease their tension in the extremes of flexion and extension
PCL

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 127/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 128/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 129/133
Intraarticular reconstruction procedures was

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 130/133
pdiscouraging because of the frequentpostoperative stiffness and persistent avulsionlaxity.Extra-articular procedures were developed toobviate these problems. These proceduresgenerally create a restraining band on the lateral
side of the knee, extending from the lateralfemoral epicondyle to the Gerdy tubercle in aline parallel with the anterior cruciate ligament.They avoid the problem of a lack of blood supplyto the intraarticular reconstructions. Most lateral
extraarticular procedures use the iliotibial bandor tract connecting the lateral femoral epicondyleto the Gerdy tubercle.
Reconstruction for Anterior

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 131/133
Reconstruction for Anterior
Cruciate Ligament Insufficiency ACL reconstruction is done traditionally usingeither an intra-articular reconstruction, an extra-articular reconstruction, or a combination of both.Isolated extra-articular reconstruction may be
useful in the skeletally immature, when there isconcern about damage to the growing physis.
In isolation, extra-articular reconstruction isprone to failure within3 to 5 years.

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 132/133

8/7/2019 Acl Injury and It's Management
http://slidepdf.com/reader/full/acl-injury-and-its-management 133/133