ALPINE SKIING - INJURY PROFILE, ACL INJURY RISK FACTORS ...
78
From DEPARTMENT OF MOLECULAR MEDICNE AND SURGERY Karolinska Institutet, Stockholm, Sweden ALPINE SKIING - INJURY PROFILE, ACL INJURY RISK FACTORS, AND PREVENTION Maria Westin Stockholm 2015
Transcript of ALPINE SKIING - INJURY PROFILE, ACL INJURY RISK FACTORS ...
From DEPARTMENT OF MOLECULAR MEDICNE AND
SURGERY
Karolinska Institutet, Stockholm, Sweden
ALPINE SKIING - INJURY PROFILE, ACL INJURY RISK FACTORS, AND
PREVENTION
Maria Westin
Stockholm 2015

All previously published papers were reproduced with permission from the publisher.
Cover page photo Nisses SportBild
Published by Karolinska Institutet.
Printed by E-print AB,2015
© Maria Westin, 2015
ISBN 978-91-7549-880-5
ALPINE SKIING- Injury profile, ACL injury risk factors, and prevention THESIS FOR DOCTORAL DEGREE (Ph.D.)
By
Maria Westin
Principal Supervisor:
Professor Suzanne Werner
Karolinska Institutet
Department of Molecular Medicine and Surgery
Stockholm Sports Trauma Research Center
Co-supervisor(s):
Professor Marie Alricsson
Mid Sweden University
Department of Health Sciences
Swedish Winter Sport Research Center
Associate Professor Björn Engström
Karolinska Institutet
Department of Molecular Medicine and Surgery
Stockholm Sports Trauma Research Center
Opponent:
Professor Emeritus
Arne Ekeland
University of Oslo
Martina Hansens Hospital
Examination Board:
Professor Sari Ponzer
Karolinska Institutet
Department of Clinical Science and Education
Division of Södersjukhuset
Professor Karin Henriksson-Larsén
The Swedish School of Sports and
Health Sciences
Professor Charlotte Häger
Umeå University
Department of Community Medicine and
Rehabilitation
Division of Physiotherapy

A contribution and thanks to, Johan, for infused me
with your passion for alpine skiing

ABSTRACT
Alpine skiing is a popular winter sport among children and adolescents. The combination of
great physical demands and ever-changing external conditions makes competitive alpine
skiing to one of our most complex sports. To reach the highest level of skiing skill, the skier
needs to take part in a long and carefully planned physical training in order to improve skiing
performance. This often starts when the skier enters a Swedish ski high school. Like other
sports, alpine skiing may unfortunately lead to injuries.
The main aim of the present thesis was to try to reduce ACL injuries in competitive alpine
skiers by the use of van Mechelen´s four steps model “Sequence of Prevention”. The first
step was to identify the magnitude of the injury problem in terms of injury incidence and
injury severity. The second step was to identify risk factors for ACL injuries. The third step
was to introduce ACL injury prevention strategies, and finally the fourth step was to evaluate
the prevention by repeating the first step.
The cohort of this thesis consisted of alpine ski students, attending ski high schools in
Sweden during at least one season between the seasons 2006/2007 and 2012/2013.
In a prospective five year study, injuries in 431 skiers (215 males, 216 females) were
recorded. Totally 312 injuries occurred in 193 skiers. The overall injury incidence was
1.7 injuries/1000 skiing hours or 3.11 injuries/100 months as a student at a ski high school.
In both male and female skiers most injuries occurred to the knee joint. ACL injuries
represented one third of these knee injuries.
ACL injury risk factors were studied. A family history, where either the skier´s father and/or
mother had had an ACL injury, increased the risk for this particular skier to sustain an ACL
injury. A number of other possible intrinsic and extrinsic risk factors for ACL injuries have
also been prospectively studied in 339 skiers (176 males, 163 females). During the study
period 25 skiers (11 males, 14 females) sustained a first time ACL injury. There was a higher
risk to sustain an ACL injury of the left knee than of the right knee, irrespective of gender.
The ACL injured skiers showed a greater side-to-side difference between legs according to
functional performance tests. The effect of an ACL injury prevention program was evaluated.
The prevention was conducted during a period of 21 months and included those skiers
(n=308) that were studying at a ski high school during the seasons 2011/2012 and 2012/2013.
Skiers, who attended a ski high school between the seasons 2006/2007 and 2010/2011 were
regarded as controls (n=456). The prevention program consisted of a video, and the goal was
to teach the skiers how to avoid getting into ACL injury risk situations while skiing. Since
there are the same demands on both legs in competitive alpine skiers a number of different
neuromuscular exercises as well indoors as outdoors on snow were implemented with the
purpose that the skier should carry out equally good performance on both legs. Twelve ACL
injuries occurred in the prevention group and 35 ACL injuries occurred in the control group.
The incident rate decreased with 0.22 (CI -0.44- 0.00) ACL injuries/ 100 month attending a
ski high school in favor of the intervention group.

The conclusion is that the prevention strategies reduced the ACL injuries with 45 %.
Although, not quite statistically significant, this result could be considered to be of clinical
importance on an individual level.
LIST OF SCIENTIFIC PAPERS
I. Westin M, Alricsson M, Werner S. Injury profile of competitive alpine
skiers: a five year cohort study. Knee Surg, Sports Traumatol, Arthrosc,
2012:20(6):1175-81
II. Westin M, Reeds- Lundqvist S, Werner S. The correlation between anterior
cruciate ligament injury in elite alpine skiers and their parents. Knee Surg,
Sports Traumatol, Arthrosc, 2014:April 13
III. Westin M, Harring M, Alricsson M, Engström B, Werner S. Risk factors for
anterior cruciate ligament injury in competitive alpine skiers. In manuscript
IV. Westin M, Harring M, Engström B, Alricsson M, Werner S. Prevention of
anterior cruciate ligament injuries in competitive alpine skiers. In manuscript
CONTENTS
SVENSK SAMMANFATTNING ................................................................................. 1 1
INTRODUCTION .......................................................................................................... 3 2
2.1 ALPINE SKIING .................................................................................................. 3
2.1.1 Competitive alpine skiing in Sweden ....................................................... 3
2.1.2 Profile of demands in competitive alpine skiers ...................................... 4
2.2 SPORTS INJURIES - EPIDEMIOLOGY ........................................................... 5
2.2.1 Sports injury definition ............................................................................. 5
2.2.2 Sports injury risk factors ........................................................................... 6
2.2.3 Sports injury prevention ............................................................................ 6
2.3 ANTERIOR CRUCIATE LIGAMENT INJURY ............................................... 6
2.3.1 Prevention of ACL injuries ....................................................................... 7
2.4 COMPETITIVE ALPINE SKIING - EPIDEMIOLOGY ................................... 7
2.4.1 ACL injury intrinsic risk factors in competitive alpine skiers ................. 8
2.4.2 ACL injury extrinsic risk factors in competitive alpine skiers ................ 8
2.4.3 ACL injury mechanisms in alpine skiing ................................................. 8
2.4.4 Injury prevention in alpine skiing ............................................................. 9
2.5 RATIONALE OF THE PRESENT THESIS ..................................................... 14
AIM OF THESIS .......................................................................................................... 15 3
MATERIAL AND METHODS ................................................................................... 17 4
4.1 STUDY DESIGNS .............................................................................................. 17
4.2 STUDY POPULATION ..................................................................................... 19
4.3 DATA COLLECTION ....................................................................................... 21
4.3.1 Questionnaires ......................................................................................... 21
4.3.2 Clinical examination (Study III) ............................................................. 22
4.3.3 Functional performance hop tests (Study III) ......................................... 24
4.3.4 Intervention - ACL injury prevention strategies (Study IV)................... 25
4.3.5 Injury definition and classification ......................................................... 26
4.4 STATISTICAL METHODS AND DATA ANALYSIS ................................... 27
4.4.1 Power analysis ......................................................................................... 28
4.5 ETHICAL APPROVAL ..................................................................................... 28
RESULTS ...................................................................................................................... 31 5
5.1 INJURY PROFILE BETWEEN THE SEASONS 2006/2007 AND
2010/2011 ............................................................................................................ 31
5.2 ACL INJURIES ................................................................................................... 33
5.2.1 ACL injury - Intrinsic risk factor ............................................................ 34
5.2.2 ACL injury - Familiar history as a risk factor ........................................ 37
5.2.3 ACL injury - Previous injury as a risk factor ......................................... 37
5.2.4 ACL injury - Extrinsic risk factors ......................................................... 37
5.3 PREVENTION OF ACL INJURIES.................................................................. 38
DISCUSSION ............................................................................................................... 41 6
6.1 INJURY PROFILE ............................................................................................. 41
6.2 ACL INJURIES ................................................................................................... 42
6.2.1 ACL injuries - Intrinsic risk factors in alpine skiing .............................. 42
6.2.2 ACL injuries - Extrinsic risk factors in alpine skiing............................. 44
6.3 PREVENTION OF ACL INJURIES .................................................................. 45
6.4 METHODOLOGICAL CONSIDERATIONS .................................................. 46
CONCLUSION ............................................................................................................. 49 7
FUTURE RESEARCH ................................................................................................. 51 8
ACKNOWLEDGEMENTS .......................................................................................... 53 9
REFERENCES .............................................................................................................. 57 10
LIST OF ABBREVIATIONS
ACL Anterior Cruciate Ligament
BIAD Boot Induced Anterior Drawer
CI Confidence Interval
DH Down Hill
FIS International Ski Federation
FIS ISS FIS Injury Surveillance System
GS Giant Slalom
ICC Intra Correlation Coefficient
IDB Injury Data Base
IR Injury Rate
IRD Injury Rate Differences
HR Hazard Ratio
Ns Non-Significant
OR Odds Ratio
OSICS Orchard Sports Injury Classification System
ROM Range of Motion
SIAS Spina Iliaca Anterior Superior
SD Standard Deviation
SG Super Giant Slalom
SL Slalom
SLAO Swedish Ski Lift Organization
STROBE Strengthening the Reporting of Observational studies in
Epidemiology
1
SVENSK SAMMANFATTNING 1
Alpin skidåkning är en av våra populäraste vinteridrotter bland barn och ungdomar.
Kombinationen av höga fysiska krav och ständigt varierande yttre förhållanden gör alpin
tävlingsskidåkning till en av våra mest komplexa idrotter. För att nå den högsta nivån inom
alpin idrott krävs en långsiktig och målinriktad träningsplanering. Majoriteten av skidåkarna
bygger sin professionella grund på något av våra alpina skidgymnasier. Liksom andra sporter,
kan alpin skidåkning tyvärr leda till skador.
Det övergripande syftet med denna avhandling var att försöka reducera antalet främre
korsbandsskador inom alpin skidsport med hjälp av van Mechelen's fyra steg modell
"Sequence of Prevention”. Det första steget innebar att kartlägga omfattningen av skador
avseende incidens och allvarlighetsgrad. Det andra steget innebar att identifiera både
individrelaterade och omgivningsrelaterade riskfaktorer för att drabbas av en främre
korsbandsskada. Det tredje steget innebar implementering av preventiva åtgärder mot
uppkomst av främre korsbandsskada och i det fjärde steget utvärderades preventionen genom
att upprepa det första steget.
Kohorten till föreliggande avhandling bestod av alpina skidgymnasister som studerade på
något av Sveriges alpina skidgymnasier under minst en säsong, mellan säsongerna 2006/2007
och 2012/2013.
I en prospektiv femårig studie omfattande 431 åkare (215 män, 216 kvinnor) registreras totalt
312 skador hos 193 åkare. Den totala skadeincidensen var 1,7 skador/1000
skidåkningstimmar eller 3,11 skador/100 månaders studier på ett skidgymnasium. Flest antal
skador inträffade i knäleden hos båda manliga och kvinnliga skidåkare och främre
korsbandsskador representerade en tredjedel av dessa knäskador.
Vidare har riskfaktorer för främre korsbandsskador studerats. En familjehereditet, där
skidåkaren antingen har en far och/eller mor med en främre korsbandsskada, ökade risken för
denna skidåkare att ådra sig en främre korsbandsskada.
En rad andra möjliga individrelaterade och omgivningsrelaterade riskfaktorer för främre
korsbandsskada har prospektivt studerats hos 339 skidåkare (176 män, 163 kvinnor). Under
studieperioden ådrog sig 25 åkare (11 män, 14 kvinnor) en främre korsbandsskada för första
gången. Resultatet visade att det var en högre risk att drabbas av en främre korsbandsskada i
vänster knä än i höger knä, oavsett kön. De skidåkare som drabbades av en främre
korsbandsskada uppvisade en större sidoskillnad mellan höger och vänster ben vid tre olika
funktionella hopptester. Preventiva strategier mot främre korsbandsskada genomfördes under
en period av 21 månader och inkluderade de skidåkare (n=308) som studerade på ett alpint
skidgymnasium under säsongerna 2011/2012 och 2012/2013. Skidåkare (n=456), som
studerade på ett alpint skidgymnasium mellan säsongerna 2006/2007 och 2010/2011 utgjorde
kontrollgrupp.
2
Målet med de preventiva strategierna var att medvetandegöra skidåkarna om en eventuell
prestationsskillnad mellan höger och vänster ben samt träna för att prestera mer liksidigt.
Alpin tävlingsskidåkning innebär att skidåkaren bör prestera lika bra svängar till höger som
till vänster. Efter att skidåkarna samt deras tränare utbildats i de preventiva strategierna mot
främre korsbandsskada uppmanades skidåkarna att regelbundet titta på en video. Videon
bestod av en informationsdel samt förslag på olika neuromuskulära övningar att genomföra
inomhus och skidövningar att utföra i samband med skidåkning. Tolv främre
korsbandsskador inträffade i preventionsgruppen och 35 främre korsbandsskador inträffade i
kontrollgruppen. Incidensen av främre korsbandsskador minskade med 0.22 främre
korsbandskador/ 100 månader på ett skidgymnasium i preventionsgruppen.
Konklusionen innebär att de preventiva strategierna reducerade incidensen med 45 % under
preventionsperioden. Statistisk signifikans kunde ej påvisas, men resultatet torde sannolikt
vara av klinisk betydelse på individnivå.
3
INTRODUCTION 2
2.1 ALPINE SKIING
In Sweden and worldwide alpine skiing has become one of the most popular sports for
children and adolescents. 56
Most individuals, irrespective of age, are skiing for recreational
purposes, though. Alpine ski racing has been an Olympic sport since 1936.Today ski racing is
organized in four competition disciplines, slalom (SL), giant slalom (GS), super giant slalom
(SG) and downhill (DH). There are also two different combination events Combined (C 2
runs of SL and 1 run of DH) or Super Combined (SC 1 run of SL and 1 run of SG or DH).
Races are held on natural slopes and each discipline has its own specific course and terrain
characteristics. The International Ski Federation (FIS) has regulated the specific competition
disciplines by course length, vertical drop from start to finish and course setting. 58
Slalom is the discipline with the shortest course and quickest turns. Course times are
approximately 60-90 seconds per run and the rule of the vertical drop is 140-220 meters.
Giant Slalom consists of a variety of short, medium and long turns. GS has fewer and
smoother turns than SL, and the minimum distance between the gates must be 10 meters.
The rule of the vertical drop is 250-450 meters.
Super Giant Slalom should consist of a variety of long and medium turns. The course is
longer than GS and the minimum distance between the gates must be 25 meters. The rule of
the vertical drop is 350-650 meters.
Downhill is the discipline with the smallest number of turns and the longest running time.
The shortest run time is 1 minute and the longest 2.5 minutes. The vertical drop varies
between 450 and 1100 meters.
SL and GS are suggested to be the most technical disciplines because of the different
technical difficulties regarding the courses, and SG and DH are the speed disciplines. 83
In
the technical events, each skier makes two runs on the same slope with different course
settings. The skier with the shortest combined time of the two runs wins the race. The speed
disciplines consist of only one single run down the course and the skier with the shortest time
wins the race.
The rules in the combined events are the same as in the individual disciplines. The winner of
the combined event is the skier with the shortest total time.
2.1.1 Competitive alpine skiing in Sweden
During the last decade competitive alpine skiing has increased among the younger
generation. 109
Today you can start to compete in alpine skiing from the age of 8 years (U8).
The competition system is age related and divided into two years age range. From the age of
15 the Swedish Championships are organized for youth athletes in all four disciplines. You
become a junior at the age of 17 years and a senior at the age of 22 years. From junior age,
the skier needs a license from FIS to participate in national and international competitions
and he/she is thereby ranked within the FIS ranking system with FIS points. The FIS points
are given in respective disciplines and based on the skier´s race results. Lower points provide
better ranking. 58
4
In Sweden, about 700 skiers hold a FIS-license and nearly 100% of these alpine skiers, aged
16-20 years, are studying at a Swedish ski high school. The skiers can study either three or
four years at a Swedish ski high school. To reach the highest level of competition, the FIS
World Cup (WC), the skier needs to take part in a long and carefully planned exercise
program, which often starts when they enter a Swedish ski high school. The skiers in Sweden,
who have reached the highest level, all have been successful nationally as juniors 109
Participation in the FIS WC is determined on the national quota of the skier’s national team
and the skier’s points.
2.1.2 Profile of demands in competitive alpine skiers
Competitive alpine skiing is one of our most complex sports, based on the combination of
great physical demands and ever-changing external conditions. Trying to determine the
skier’s level of performance is difficult, since the conditions are never the same. 109
Irrespective of discipline the skier must control the skis throughout the complete curve and
force must be applied with necessary kinesthetic sense and timing. To have good control and
balance during the different phases of the turn, the skier needs a good performance in several
physiological and psychological parameters.
Aerobe/Anaerobe capacity - For alpine skiers, the anaerobic energy processes dominate. 57
Distribution of the energetic systems is 45% aerobic, 55% anaerobic metabolism. 109
Despite
the high demand of anaerobic capacity an alpine skier need good values in aerobe capacity. 83
The reason for endurance training is to establish a high enough level to endure the mainly
static load of ski racing as well as the overall stress of a long season.
Leg muscle strength - The muscle strength requirements are complex. The external forces
arising when sliding down a hill change by turning and edging the skis. This force increase as
the speed and the edge angle increases. The highest loads arise during the eccentric phase.
The concentric phase is partially relieved and takes place directly after the initiation of the
turn. In many sports, the concentric muscle work is lower or the same as the eccentric work.
However, in alpine skiing the skier gets energy from the drop height, which is obtained when
you go down the hill. This leads to dominantly eccentric muscle actions and explains the
relatively high bone strength compared to in other sports. 109
In an EMG study Hintermeister et al. 54
suggested that the primary role of the quadriceps
muscle group was to maintain balance while the skier´s carves through the turn.
Core stability - Alpine skiing requires great forces. Therefore, in order to maintain a well-
balanced body position while skiing, the skiers need powerful and functional core stability. 109
Balance and coordination - Alpine skiing is characterized by the difficulties with the ski
snow contact. The vibrations, which arise in combination with increasing speeds, place high
demands on the skier’s coordination and balance. Therefore it should be included in the
training. 109
The purpose of coordination and balance training is to improve motor pattering
through neurologic adaptations.
The macro cycle for alpine skiers can be dived into three periods: 1. Preseason (May-July),
2. Sports specific period August-October) and 3. Competition season (November-April).
5
These macro periods are subdivided in mesoperiods and then further subdivided in micro
periods. 109
2.2 SPORTS INJURIES - EPIDEMIOLOGY
Swedish Civil Contingency Agency published 2010 a report based on the Swedish Injury
Database (IDB) that 280 000 injuries were related to sports and physical activity. This means
that almost half of all injuries that lead to a visit at an emergency hospital are related to some
form of physical activity 80
and alpine skiing was the third after soccer and ice hockey. To the
Swedish Ski Lift Organization (SLAO) 3177 cases were notified during the season
2013/2014 and one fourth of these injuries were located to the knee.110
The objective of epidemiological research is to try to prevent injuries. One of the first
suggested injury prevention models was described by van Mechelen 1992. 130
According to
van Mechelen the Sequence of Prevention consists of four steps. The first step is to try to
identify the magnitude of the injury problem by identifying the injury incidence and injury
severity specific for the studied sport. The second step means to identify the injury risk
factors. In the third step prevention strategies are introduced, and finally in the fourth step the
prevention is evaluated by repeating the first step. Finch 28
added another two steps, namely
to study barriers and trying to understand motivators before assessing the prevention in a real
world context. During the last decade several consensus statements regarding epidemiology
injury research for both team sports 36, 37
and individual sports 62, 95, 125
have been suggested.
In competitive alpine skiing Flörenäs et al. 32
suggested retrospective interviews with the as
well skiers as their coaches in order to get a complete injury surveillance.
2.2.1 Sports injury definition
It is well known that various injury definitions exist in the literature, and therefore it is
difficult to compare studies. In 1974 the National Athletic Injury/Illness Reporting Systems
(NAIRS) defined a sports injury as an injury which occurs as a result of participation in
sports, and limits the athletic participation for at least one day after onset. 68
The consensus
statement in football (soccer) 36
defined an injury as “any physical complaint sustained by a
player that results from a football match or football training, irrespective of need for medical
attention or time loss from football activities”. This definition has led to a somewhat similar
definition in other sports. 37, 62, 95, 125
The FIS Injury Surveillance definition means an injury
that occurred during training and competition and required attention by medical personnel. 32
A recurrent injury (re-injury) is defined as an injury of the same location and type, which
occurs after an athlete’s return to full participation from his/her previous injury. 36, 37, 62, 95
Injury incidence The incidence of injury is a key variable in the “Sequence of prevention” 130
Rothman 105
defines injury incidence to be the number of subjects developing problems
divided with the total time of exposure of a sport. Today the most common way of reporting
the injury incidence in sports medicine is the number of injury per 1000 exposure hours. 36
37
Injury classification Injury classification refers to the body localization and the damaged
structure or tissue. The most common classification system in sports medicine, worldwide is
the Orchard Sports Injury Classification System (OSICS). 36, 37, 62, 95
The OSICS system was
6
developed 1992 by Orchard and has been revised during the years and the latest version is
OSICS 10.1. 88
This injury surveillance system is a four character system for coding the body
localization (first letter) and the pathology of the injury (letters 2-4). 88
Injury severity The severity level of the injury is related to the injury definition. Van
Mechelen 129
described the severity of sports injuries with six closely related criteria. These
are the nature of the sport injury, the duration and nature of the treatment, sporting time lost,
working time lost, permanent damage and costs. In sports medicine, the severity is usually
reported as the time lost from participation in training or competition. The NAIRS system
discriminates between minor injuries (1-7 days), moderately serious injuries (8-21 days) and
serious injuries (>21 days). Recently, both team sports 36, 37
and individual sports 32, 62, 95, 125
distinguish between minor injuries (1-7 days), moderately serious injuries (8-28 days), severe
injuries (> 28 days- 6 months) and long-term or career-ending injuries (> 6 months).
2.2.2 Sports injury risk factors
The aetiology can be categorised by intrinsic (internal, person- related) and extrinsic
(external, environmental-related) risk factors. 69, 123, 130
The intrinsic risk factors are related to
the individual biological or psychosocial characteristics of a person such as age, gender, body
composition, previous injury, physical fitness and psychosocial stress. Extrinsic risk factors
are related to environmental variables such as type of sport, skill level, exposure, match or
training, rules, sports facilities (conditions of floor or surface, safety measures, lighting) and
equipment (tools, protective equipment, shoes, clothing). The risk factors have also in the
literature been categorized as environmental, anatomical, hormonal and neuromuscular. 40, 111,
112
2.2.3 Sports injury prevention
During the last decade the number of studies about injury prevention has increased. 74
The
prevention could be categorized into four different areas according to the mechanism of the
injuries. 74
1. Equipment, like protective devices. 2. Training, if the objective was to introduce
a neuromuscular adaption. 3. Regulations, if the prevention involved changes in the rules or
laws related to the sport/activity. 4 Education if the program was designed to improve
knowledge that would lead to a reduced injury risk/rate. A systematic review, the aim of
which was to evaluate specific interventions designed to reduce sports injuries showed that
most publications focused on protective equipment followed of by training. 74
The most
frequently studied sport was soccer and most of the neuromuscular training intervention
focused on lower extremity prevention. 74
Moreover, a systematic review, the objective of
which was to quantify the effectiveness of prevention programs in children and adolescents,
found good evidence that prevention programs could lead to a reduction of injury. 104
Preventions programs have been suggested to be based on the actual sport 28, 130
and its
specific injury mechanisms. 7
2.3 ANTERIOR CRUCIATE LIGAMENT INJURY
The anterior cruciate ligament (ACL) is an import ligament in the knee joint whose primary
aim is to restrain the tibia translation and secondarily the internal/external rotation and
7
varus/valgus motion. 137
Most ACL injuries occur in sports including pivoting movements 2, 5,
85 and are characterized as non-contact injuries.
102
Nordenvall et al. 85
reported an incidence rate of ACL injuries in Sweden to be between 78
and 81 injuries per 100 000 individuals and year. Females have six times greater risk for
sustaining a non-contact ACL injury than their male counterparts. 102
. In Sweden the most
common sports-related ACL injury was found in soccer, and the second most common one in
alpine skiing when it comes to females and the third most common one in males. 2 The
consequences of an ACL injury include both temporary and permanent disability resulting in
direct and indirect costs. This serious traumatic injury can lead to major problems for an ACL
injured individual in terms of knee joint instability and/or “giving way situations”. Still there
is no consensus for the best treatment, physiotherapy alone or reconstruction with subsequent
rehabilitation. 23, 35
In Sweden, the rehabilitation period after ACL reconstruction usually lasts
6-8 months.
Recently Smith et al. 111, 112
have published two literature reviews in terms of risk factors
associated with an ACL injury. They found decreased intracondylar femoral notch size,
decreased depth of the concavity of the medial tibia plateau, increased slope of the tibia
plateau, increased anterior-posterior knee laxity to be anatomical risk factors. In addition, a
prior reconstruction of the ACL and a family history of ACL injury were reported to be risk
factors.
2.3.1 Prevention of ACL injuries
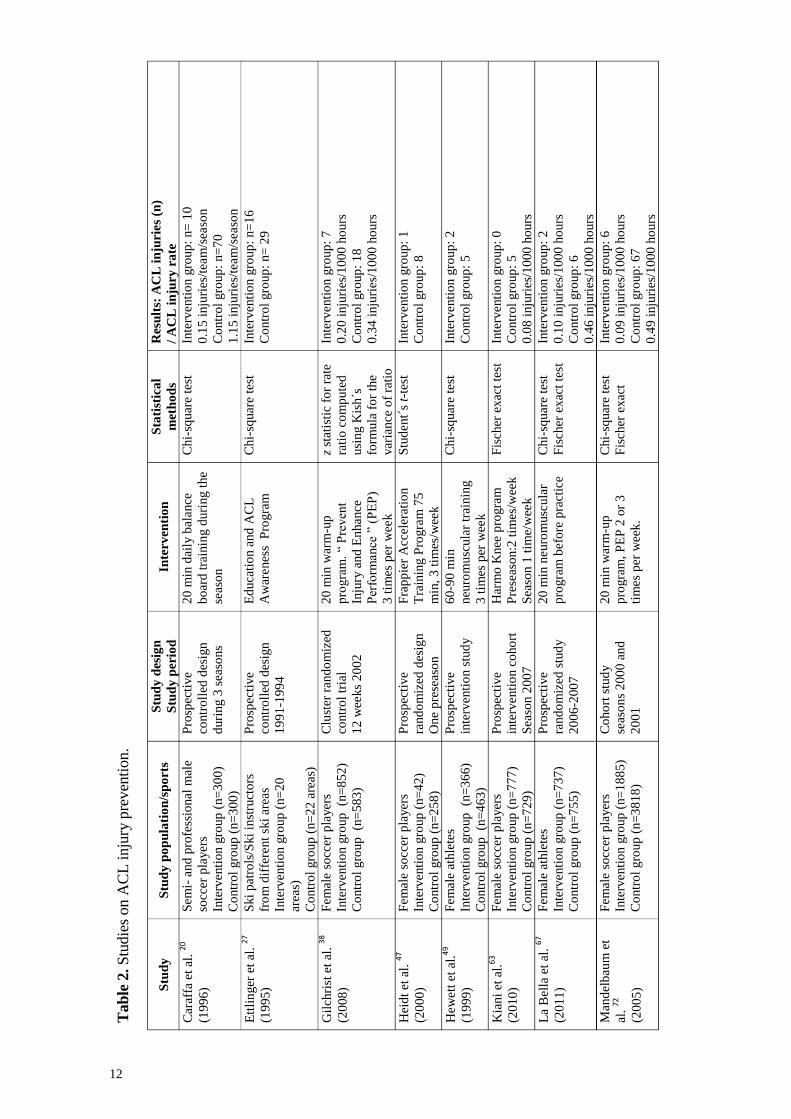
A number of prospective studies in terms of prevention of lower extremity injuries have been
performed. 90, 114, 131
There are fewer studies where ACL injuries are specified as the outcome
measure. An overview of these studies is presented in table 2. All but one out of 16 studies
included team sport athletes 27
and mostly soccer players. 20, 38, 47, 63, 72, 113, 117, 126
Only three of
these studies included male athletes. 20, 27, 86
After implementation of a prevention program no
reduction of the ACL injuries was shown in three of these investigations.94, 113, 117
The
prevention programs differ from each other with regards to type of exercises, length of the
program and duration of the intervention period. Caraffa et al. 20
and Söderman et al. 113
used
a stepwise balance board training during preseason and indoor season. Other authors but
Ettlinger et al. 27
included different exercises, for instance strength training, plyometric
training agility training and training for improving balance. 38, 47, 49, 63, 67, 72, 79, 86, 91, 93, 94, 117, 127
Hewett et al. 49
and Heidt et al. 47
conducted a prevention program during to the preseason
training, while other authors carried out their prevention programs both during preseason and
competitive season. 20, 27, 38, 63, 67, 72, 79, 86, 91, 93, 94, 113, 116, 127
Several authors have recommended
to include plyometric 52
, neuromuscular 40, 49
and core stability 138
in the ACL prevention
program.
2.4 COMPETITIVE ALPINE SKIING - EPIDEMIOLOGY
Some investigations about injury epidemiology in terms of competitive alpine skiers have
been carried out. Using a retrospective interview Flørenes et al. 31
performed an injury
surveillance of skiers that took part in the FIS World Cup during two winter seasons
2006/2007 and 2007/2008. Bere et al. 14
performed a follow up in FIS World Cup over six
seasons. Furthermore, three studies are available, two single event studies, the Olympic
8
Games 1994 24
and the Junior World Championship 1995 15
. Moreover, a retrospective Finish
study using a questionnaire 119
included competitive alpine skiers has been published. All
these studies reported that the knee joint was the most commonly injured body part with a
high number of ACL injuries.
2.4.1 ACL injury intrinsic risk factors in competitive alpine skiers
There is limited information about risk factors for sustaining an ACL injury in competitive
alpine skiers. The literature is also inconsistent about ACL injury incidence among gender.
Stevenson et al. 120
, Stenroos et al. 119
and Raschner et al. 101
reported a higher incidence of
ACL injuries in female than male alpine skiers, while other authors did not find any gender
difference 14, 31, 100
. Only one observational study has evaluated body composition and
physical fitness. 101
In this investigation the authors found core stability to be a critical factor
for ACL injuries in young alpine ski racers.
2.4.2 ACL injury extrinsic risk factors in competitive alpine skiers
In solely a few studies ACL injury extrinsic risk factors were evaluated in competitive alpine
skiing. From an interview study including 61 experts Spörri et al. 115
reported 25 “key” injury
risk factors to sustain an ACL injury. Ski equipment (boot, binding, plate) was ranked as
number one and changes in snow conditions as number two. The experts mean that icy
conditions on the slope probably could be safer than aggressive snow conditions, which are
consistent with the study by Bere et al. 13
Furthermore, Bere et al. 13
reported that technical
mistakes and inappropriate tactical choices might lead to injury situations and thereby
constituted the highest injury risk. Moreover, Bere et al. 14
and Flörenäs et al. 31
found that the
downhill race accounted for the highest number of ACL injuries. No correlation between
skiing performance/FIS point and injury risk has been found. 15
Spörri et al. 115
reported that
younger World Cup skiers, in particular female skiers, may not always be adequately
prepared for World Cup races.
2.4.3 ACL injury mechanisms in alpine skiing
Slip and catch has been described to be the most common ACL injury mechanism in
competitive alpine skiing. 12
This means that the skier´s outer ski catches the inside edge and
forces the knee joint into a combination of internal rotation and valgus (Figure 1). For
recreational alpine skiers the Phantom Foot mechanism has been described as the most
common ACL injury mechanism (Figure 2). 27, 81
This means that the skier is out of balance,
backwards with hips below the knee with the upper body generally facing the downhill ski.
The injury occurs when the inside edge of the downhill ski tail recurs the snow surface,
forcing the knee joint into a combination of internal rotation and valgus. Other ACL injury
mechanisms have been described in the literature. These are the Boot-Induced Anterior
Drawer (BIAD), 27
the valgus external rotation mechanism 60
and the dynamic snow plow. 66

9
2.4.4 Injury prevention in alpine skiing
In table 1 an overview of ski injury prevention studies is presented. Hitherto, publications of
injury prevention in alpine skiers have been focused on recreational skiers. Most of these
studies evaluate the effectiveness of using a helmet for injury prevention. One study,
Barschera et al. 9 did not find any effect of the use of a helmet. In contrast, five other
investigations were in agreement about that the use of a helmet reduces the risk for head
injuries. 42, 43, 70, 76, 121
Furthermore, Hagel et al. 42
could not show any relation between
behavior risk taking and the use of a helmet while skiing.
Two studies tried to improve the skier´s knowledge about how to avoid injuries and increase
skiing safety by watching a video. 27, 61
Ettlinger et al. 27
developed a specific awareness
training program, the aim of which was to improve the psychomotor skills and to develop an
awareness of possible events leading to an ACL injury during alpine skiing. The program was
divided into three parts, avoiding high risk behavior, recognizing potentially dangerous
situations and responding quickly and effectively whenever these conditions occurred. They
invited ski patrols and ski instructors from 25 ski areas in the USA to participate in this
education program. Twenty out of these 25 ski areas completed all training and reporting
requirements. The education program included a 19-minute video, a leader’s guide, a flip
chart for reviewing information and images covered in the video, a flip chart for recording
group responses to questions posed by the video and a workbook for each skier including the
video script. Furthermore, 40 skiers were extra trained in the awareness program. After the
intervention season a control group was consisted of 22 ski areas. The number of ACL injury
from the intervention season was compared with two previous seasons in both groups. The
result showed a decreased ACL injury rate in the intervention group with 62% during the
intervention season.
JØrgensen et al. 61
performed a randomized intervention study to test the effect of an
instructional ski video, which was shown for recreational skiers traveling by bus to the Alps.
The skiers (n= 763) were divided into two groups, depending on whether the video had or not
had been viewed during the bus transport to the Alps. The video was shown during the
outward journey and focused on information about skiing safety including, self-test of release
binding, skiing behavior and the ten golden rules for skiers. During the return journey the
skiers answered a questionnaire regarding skiing behavior and number of injuries that had
happened during the week. The result showed a 30% reduction of injuries in the intervention
Figure 1. Common mechanism of ACL
injury among competitive alpine skiers. Slip and catch mechanism.
Figure 2. Common mechanism of ACL injury
among recreational skiers. a. Phantom Foot, b.
BIAD, c.Valgus-external rotation

10
group compared with the control group and the risk of sustaining a knee injury was lower if
the bindings had been tested and adjusted.
To the best of our knowledge only one research group has evaluated prevention strategies
regarding skiing environment. 16
This study was performed at two Norwegian ski areas
during a five year period. They studied the effect of trail design and grooming hours of the
slopes regarding the rate and severity of injuries. Both the injury rate and injury severity
decreased after improvement of the slopes (widening slopes, new slopes for beginners, better
grooming, repairing roughness.

11
Tab
le 1
. S
tudie
s on i
nju
ry p
reven
tion i
n a
lpin
e sk
iing.
Stu
dy
S
tud
y d
esig
n
Stu
dy
per
iod
S
tud
y p
op
ula
tio
n
Pri
ma
ry o
utc
om
e
Sta
tist
ica
l m
eth
od
s R
esu
lts
Bas
cher
a et
al.
9
(20
15
)
Ret
rosp
ecti
ve
coho
rt
stud
y
20
00
-201
0
Skie
rs w
ith t
rau
mat
ic b
rain
inju
ries
(n=
24
5)
Tra
um
atic
bra
in i
nju
ries
eval
uate
d w
ith G
lasg
ow
com
a sc
ale
Mult
iple
reg
ress
ion
anal
ysi
s
Hel
met
use
did
no
t re
duce
the
risk
of
sever
e tr
aum
atic
bra
in i
nju
ries
.
OR
1.2
3 (
0.5
2-2
.92
)
Ber
gst
rØm
& E
kel
and
. 16
(20
04
)
Pro
spec
tive
surv
ey
19
90
-199
6
Inju
red
skie
rs a
nd
sno
wb
oar
der
s
(n=
14
10
)
Inju
ries
eval
uat
ed b
y
Inju
ry s
ever
ity s
core
of
1-7
5.
Stu
dent´
s t-
test
,
Pea
rso
n´s
co
rrel
atio
n,
Mult
iple
lin
ear
regre
ssio
n.
The
inci
den
t ra
te d
ecre
ased
aft
er
imp
rovem
ent
of
the
slo
pes
.
Incr
ease
d i
nju
ry r
ate
duri
ng t
he
yea
rs
gro
om
ing h
ours
wer
e re
duce
d (
r2=0
.99
).
Ett
lin
ger
et
al.
27
(19
95
)
Inte
rventi
on s
tud
y
(AC
L A
war
enes
s
Pro
gra
m)
19
91
-199
4
Ski
pat
rols
/Ski
inst
ruct
ors
fro
m
dif
fere
nt
ski
area
s
Inte
rventi
on g
roup
(n=
20
)
Co
ntr
ol
gro
up
(n=
22
)
Ser
ious
knee
sp
rain
s
(Gra
de
III
knee
sp
rain
s
and
gra
de
II a
nd
III
AC
L
spra
ins)
Chi-
squar
e te
st
The
nu
mb
er o
f se
rio
us
knee
sp
rain
s
dec
reas
ed 6
2%
am
on
g t
he
trai
ned
ski
pat
rols
co
mp
ared
wit
h t
he
con
tro
ls.
Hag
el e
t al
. 4
2
(20
05
a)
Cas
e-c
ontr
ol
20
01
-200
2
32
95
inju
red
skie
rs w
itho
ut
hea
d f
ace
or
nec
k i
nju
ry.
1.
Inju
ry s
ever
ity
2.
Hig
h e
ner
gy c
rash
circ
um
stance
s
Hel
met
use
C
ond
itio
nal
logis
tic
regre
ssio
n
No
dif
fere
nce
s b
etw
een n
on h
elm
et u
sers
and
hel
met
use
rs r
egar
din
g b
ehav
ior
risk
.
Hag
el e
t al
. 4
3
(20
05
b)
Mat
ched
cas
e-c
ontr
ol
20
01
-200
2
Hea
d,
nec
k o
r fa
ce i
nju
red
skie
rs (
n=
10
82
)
32
95
skie
rs w
ith o
ther
inju
res
Hel
met
use
C
ond
itio
nal
logis
tic
regre
ssio
n
Hel
met
use
led
to
29
% r
educe
d r
isk o
f
hea
d i
nju
ries
(O
R 0
.71
.)
JØrg
ense
n e
t al
. 61
(19
98
)
Inte
rventi
on s
tud
y
(Inju
ry s
afety
vid
eo)
1 w
eek
Skie
rs t
ravel
ed b
y b
us
to t
he
Alp
s
Inte
rventi
on g
roup
(n=
24
3)
Co
ntr
ol
gro
up
(n=
52
0)
A s
ki
inju
ry w
as
def
ined
as a
ph
ysi
cal
dis
abil
ity,
that
bo
ther
ed t
he
skie
rs
for
> 2
4 h
ours
Chi-
squar
e te
st,
Fis
cher
´s e
xac
t te
st
A s
afe
ty i
nst
ruct
ional
sk
i vid
eo
sig
nif
icantl
y r
educe
d t
he
risk
of
inju
ry i
n
the
inte
rventi
on g
roup
.
Mac
nab
et
al.
70
(20
08
)
Cas
e-
contr
ol
19
98
-199
9
Skie
r/sn
ow
bo
ard
ers
>1
3 y
ears
(n=
70
)
Unin
jure
d s
kie
rs a
s co
ntr
ols
(Est
imat
ed b
y o
bse
rvat
ions)
Hel
met
use
C
hi-
sq
uar
e te
st
Mat
el-H
aenzs
el
test
Hig
her
ris
k o
f hea
d i
nju
ries
fo
r b
oth
skie
rs (
RR
1.7
4)
and
sno
wb
oard
ers
(R
R
1.8
2)
that
do
no
t use
hel
met
.
Muel
ler
et a
l. 76
(2
008
)
Cas
e-
contr
ol
20
00
-200
5
Hea
d,
nec
k o
r fa
ce i
nju
red
skie
rs/s
no
wb
oar
der
s (n
=3
70
1),
17
674
skie
rs w
ith o
ther
inju
ries
Hel
met
use
M
ult
iple
lo
gis
tic
regre
ssio
n
Hel
met
use
red
uce
d t
he
risk
fo
r hea
d
inju
ries
(O
R 0
.85
).
Sulh
eim
et
al.
121
(20
06
)
Cas
e-
contr
ol
20
02
Inju
red
skie
rs/s
no
wb
oar
der
s
(n=
32
77
), u
nin
jure
d s
kie
rs
as c
ontr
ols
(n=
29
92
)
Hel
met
use
M
ult
ivar
ite
logis
tic
regre
ssio
n
Hel
met
use
red
uce
d t
he
risk
of
hea
d
inju
ries
(O
R 0
.40
)
12
Tab
le 2
. S
tudie
s on A
CL
inju
ry p
reven
tion.
Stu
dy
S
tud
y p
op
ula
tio
n/s
po
rts
Stu
dy
des
ign
Stu
dy
per
iod
In
terv
enti
on
S
tati
stic
al
met
ho
ds
Res
ult
s: A
CL
in
juri
es
(n)
/ A
CL
in
jury
ra
te
Car
affa
et
al.
20
(19
96
)
Sem
i- a
nd
pro
fess
ional
mal
e
socc
er p
layer
s
Inte
rventi
on g
roup
(n=
30
0)
Co
ntr
ol
gro
up
(n=
30
0)
Pro
spec
tive
contr
oll
ed d
esig
n
duri
ng 3
sea
son
s
20
min
dai
ly b
alance
bo
ard
tra
inin
g d
uri
ng t
he
seas
on
Chi-
squar
e te
st
Inte
rventi
on g
roup
: n=
10
0.1
5 i
nju
ries
/tea
m/s
easo
n
Co
ntr
ol
gro
up
: n=
70
1.1
5 i
nju
ries
/tea
m/s
easo
n
Ett
lin
ger
et
al.
27
(19
95
)
Ski
pat
rols
/Ski
inst
ruct
ors
fro
m d
iffe
rent
ski
area
s
Inte
rventi
on g
roup
(n=
20
area
s)
Co
ntr
ol
gro
up
(n=
22
are
as)
Pro
spec
tive
contr
oll
ed d
esig
n
19
91
-199
4
Ed
uca
tio
n a
nd
AC
L
Aw
arenes
s P
rogra
m
Chi-
squar
e te
st
Inte
rventi
on g
roup
: n=
16
Co
ntr
ol
gro
up
: n=
29
Gil
chri
st e
t al
. 38
(20
08
)
Fem
ale
socc
er p
layer
s
Inte
rventi
on g
roup
(n
=8
52
)
Co
ntr
ol
gro
up
(n
=5
83
)
Clu
ster
ran
do
miz
ed
contr
ol
tria
l
12
wee
ks
20
02
20
min
war
m-u
p
pro
gra
m.
“ P
reven
t
Inju
ry a
nd
En
hance
Per
form
ance
” (
PE
P)
3 t
imes
per
wee
k
z st
atis
tic
for
rate
rati
o c
om
pu
ted
usi
ng K
ish
´s
form
ula
fo
r th
e
var
iance
of
rati
o
Inte
rventi
on g
roup
: 7
0.2
0 i
nju
ries
/10
00
ho
urs
Co
ntr
ol
gro
up
: 1
8
0.3
4 i
nju
ries
/10
00
ho
urs
Hei
dt
et a
l. 47
(20
00
)
Fem
ale
socc
er p
layer
s
Inte
rventi
on g
roup
(n=
42
)
Co
ntr
ol
gro
up
(n=
25
8)
Pro
spec
tive
rand
om
ized
des
ign
One
pre
seas
on
Fra
pp
ier
Acc
eler
atio
n
Tra
inin
g P
rogra
m 7
5
min
, 3
tim
es/w
eek
Stu
dent´
s t-
test
Inte
rventi
on g
roup
: 1
Co
ntr
ol
gro
up
: 8
Hew
ett
et
al.49
(19
99
)
Fem
ale
athle
tes
Inte
rventi
on g
roup
(n
=3
66
)
Co
ntr
ol
gro
up
(n
=4
63
)
Pro
spec
tive
inte
rventi
on s
tud
y
60
-90
min
neu
rom
usc
ula
r tr
ainin
g
3 t
imes
per
wee
k
Chi-
squar
e te
st
Inte
rventi
on g
roup
: 2
Co
ntr
ol
gro
up
: 5
Kia
ni
et a
l.6
3
(20
10
)
Fem
ale
socc
er p
layer
s
Inte
rventi
on g
roup
(n=
77
7)
Co
ntr
ol
gro
up
(n=
72
9)
Pro
spec
tive
inte
rventi
on c
oho
rt
Sea
son 2
00
7
Har
mo
Knee
pro
gra
m
Pre
seas
on:2
tim
es/w
eek
Sea
son 1
tim
e/w
eek
Fis
cher
exac
t te
st
Inte
rventi
on g
roup
: 0
Co
ntr
ol
gro
up
: 5
0.0
8 i
nju
ries
/10
00
ho
urs
La
Bel
la e
t al
. 67
(20
11
)
Fem
ale
athle
tes
Inte
rventi
on g
roup
(n=
73
7)
Co
ntr
ol
gro
up
(n=
75
5)
Pro
spec
tive
rand
om
ized
stu
dy
20
06
-200
7
20
min
neuro
musc
ula
r
pro
gra
m b
efo
re p
ract
ice
Chi-
squar
e te
st
Fis
cher
exac
t te
st
Inte
rventi
on g
roup
: 2
0.1
0 i
nju
ries
/10
00
ho
urs
Co
ntr
ol
gro
up
: 6
0.4
6 i
nju
ries
/10
00
ho
urs
Man
del
bau
m e
t
al.
72
(20
05
)
Fem
ale
socc
er p
layer
s
Inte
rventi
on g
roup
(n=
18
85
)
Co
ntr
ol
gro
up
(n=
38
18
)
Co
ho
rt s
tud
y
seas
on
s 2
00
0 a
nd
20
01
20
min
war
m-u
p
pro
gra
m,
PE
P 2
or
3
tim
es
per
wee
k.
Chi-
squar
e te
st
Fis
cher
exac
t
Inte
rventi
on g
roup
: 6
0.0
9 i
nju
ries
/10
00
ho
urs
Co
ntr
ol
gro
up
: 6
7
0.4
9 i
nju
ries
/10
00
ho
urs

13
Myk
leb
ust
et
al.79
( 2
002
)
Fem
ale
han
db
all
pla
yer
s
Inte
rventi
on g
roup
s:
Sea
son o
ne
(n=
85
5)
Sea
son t
wo
(n=
85
0)
Co
ntr
ol
gro
up
(n=
94
2)
Pro
spec
tive
inte
rventi
on s
tud
y
19
99
-200
1
15
min
neuro
musc
ula
r
pro
gra
m3
tim
es a
wee
k
duri
ng a
5-t
o 7
-wee
k
trai
nin
g p
erio
d,
and
then
once
/wee
k d
uri
ng t
he
seas
on
Chi-
squar
e te
st
Fis
cher
exac
t te
st
Wal
d´s
tes
t
Inte
rventi
on s
easo
n 1
: 2
3
0.1
3 i
nju
ries
/10
00
ho
urs
Inte
rventi
on s
easo
n 2
: 1
7
0.0
9 i
nju
ries
/10
00
ho
urs
Co
ntr
ol
gro
up
: 2
9
0.1
4 i
nju
ries
/ 1
000
h
Ols
en e
t al
. 86
(2
005
)
Han
db
all
pla
yer
s
Inte
rventi
on g
roup
(n=
95
8)
Co
ntr
ol
gro
up
(n=
87
9)
Pro
spec
tive
rand
om
ized
stu
dy
15
-20
min
war
m-u
p
neu
rom
usc
ula
r p
rogra
m
Init
iall
y 1
5 t
imes
and
ther
eaft
er 1
tim
e/w
eek
Co
x
regre
ssio
n
Wal
d t
est
Inte
rventi
on g
roup
: 3
0.0
3 i
nju
ries
/10
00
ho
urs
Co
ntr
ol
gro
up
: 1
0
0.1
1 i
nju
ries
/10
00
ho
urs
Pas
anen
et
al.
91
(20
08
)
Fem
ale
flo
orb
all
pla
yer
s
Inte
rventi
on g
roup
(n=
25
6)
Co
ntr
ol
gro
up
(n=
20
1)
Pro
spec
tive
rand
om
ized
des
ign
Duri
ng s
easo
n 2
00
5-
20
06
20
-30
min
war
m-u
p
neu
rom
usc
ula
r p
rogra
m
Pre
seas
on:
2-3
tim
es/w
eek
Co
mp
etit
ive
seaso
n:
1 t
ime/
wee
k
One
way a
nal
ysi
s
of
var
iance
,
Po
isso
n
regre
ssio
n m
od
el
Inte
rventi
on g
roup
: 6
0.1
9 i
nju
ries
/10
00
ho
urs
Co
ntr
ol
gro
up
: 4
0.1
6 i
nju
ries
/10
00
ho
urs
Pet
erse
n e
t al
. 93
(20
05
)
Fem
ale
han
db
all
pla
yer
s
Inte
rventi
on g
roup
(n=
13
4)
Co
ntr
ol
gro
up
(n=
14
2)
Pro
spec
tive
case
-
contr
ol
stud
y
One
seaso
n
10
min
neuro
musc
ula
r
pro
gra
m
Pre
seas
on:
3 t
imes
/wee
k
duri
ng 8
wee
ks
Sea
son:
1 t
ime/
wee
k
Fis
cher
´s e
xac
t
test
Inte
rventi
on g
roup
: 1
0.0
4 i
nju
ries
/10
00
ho
urs
Co
ntr
ol
gro
up
: 5
0.2
1 i
nju
ries
/10
00
ho
urs
Pfe
iffe
r et
at.
94
(20
06
)
Fem
ale
athle
tes
in b
asket
,
vo
lleyb
all
and
so
ccer
Inte
rventi
on g
roup
(n=
57
7)
Co
ntr
ol
gro
up
(n=
86
2)
Pro
spec
tive
coho
rt
stud
y
Tw
o s
easo
ns
Knee
Lig
am
ent
Inju
ry
Pre
ven
tio
n (
KL
IP)
2 t
imes
/wee
k
Lo
gis
tic
regre
ssio
n
Inte
rventi
on g
roup
: 3
0.1
7 i
nju
ries
/10
00
ho
urs
Co
ntr
ol
gro
up
: 3
0.0
8 i
nju
ries
/10
00
ho
urs
Ste
ffen e
t al
. 11
6
(20
08
)
Fem
ale
socc
er p
layer
s
Inte
rventi
on g
roup
(n=
10
73
)
Co
ntr
ol
gro
up
(n=
94
7)
Pro
spec
tive
rand
om
ized
stu
dy
The
seas
on 2
00
5,
8 m
onth
s
“ F
IFA
11
”
15
min
pro
gra
m,
Init
iall
y 1
5 t
imes
ther
eaft
er 1
tim
e/w
eek
One
way a
nal
ysi
s
of
var
iance
,
Chi-
squar
e te
st
Inte
rventi
on g
roup
: 4
0.0
6 i
nju
ries
/10
00
ho
urs
Co
ntr
ol
gro
up
: 5
0.0
8 i
nju
ries
/10
00
ho
urs
Sö
der
man e
t al
. 11
3
(20
00
)
Fem
ale
socc
er p
layer
s
Inte
rventi
on g
roup
(n=
62
)
Co
ntr
ol
gro
up
(n=
78
)
Pro
spec
tive
rand
om
ized
stu
dy
Bal
ance
bo
ard
tra
inin
g
Init
iall
y 1
0-1
5 m
in a
t 3
0
sess
ions
ther
eaft
er 3
tim
es/w
eek
duri
ng t
he
seas
on
Kap
lain
-Mei
er
surv
ival
anal
ysi
s,
the
log r
ank t
est
Inte
rventi
on g
roup
: 4
0.4
9 i
nju
ries
/10
00
ho
urs
Co
ntr
ol
gro
up
: 1
0.1
1 i
nju
ries
/10
00
ho
urs
Wal
dén
et
al.
126
(20
12
)
Fem
ale
socc
er p
layer
s
Inte
rventi
on g
roup
(n=
24
79
)
Co
ntr
ol
gro
up
(n=
20
85
)
Clu
ster
ran
do
miz
ed
contr
ol
tri
al
7 m
onth
s, 2
00
9
15
min
neuro
musc
ula
r
war
m-u
p p
rogra
m.
2 t
imes
/ w
eek d
uri
ng
the
who
le s
easo
n.
Ab
solu
te r
ate
red
uct
ion
Co
x R
egre
ssio
n
Inte
rventi
on g
roup
: 7
0.0
5 i
nju
ries
/ 1
000
ho
urs
Co
ntr
ol
gro
up
: 1
4
0.1
1 i
nju
ries
/10
00
ho
urs
14
2.5 RATIONALE OF THE PRESENT THESIS
For competitive alpine skiers an injury is common. Hitherto, all epidemiological studies have
reported ACL injuries to be the single most common injury in competitive alpine skiers 14, 24,
31 In Sweden, nearly all Swedish alpine skiers aged 16-20 years who try to reach the national
team attend a ski high school. For the individual skier, an ACL injury has consequences, not
only for time lost from skiing but also an increased risk for sustaining a new knee injury 44, 77,
92, 136and long-term decreased knee function with a reduced activity level
5 as well as an
increased risk of early onset of knee osteoarthritis. 8, 84
Not infrequently this injury leads to
that the young skier has to end his (or her) skiing career. 103
The total economic burden of these injuries is not easily quantified, as indirect long-term
costs likely overshadow the more readily quantifiable direct costs. From cost effectiveness
analysis Swart el al. 122
found that an implementation of neuromuscular programs is more
cost effective than screening methods to identify high risk athletes.
However, in order to prevent this serious knee injury the literature recommends that ACL
injury prevention programs should be developed for each sport and the intervention must be
based on the sport specific ACL mechanism and sport specific intrinsic as well as extrinsic
injury risk factors. 7, 28, 75, 130
Moreover, the literature prefers prospective observational studies
when planning and implementing a prevention program. 6, 29
Furthermore, there is a considerable lack of data in terms of competitive alpine skiing in
general. Consequently, it is of interest to evaluate whether an ACL injury prevention program
specifically developed based on known risk factors and thereby tailored for competitive
alpine skiers could lead to a reduction of ACL injuries in alpine skiing.
15
AIM OF THESIS 3
The main aim of the present thesis was to try to reduce the number of ACL injuries in
adolescent competitive alpine skiers by a specifically developed prevention program based on
van Mechelen´s “Sequence of Prevention”. 130
The specific aims were:
Study I: To prospectively follow and study injury incidence, injury location, type of injury as
well as injury severity in alpine ski students at the Swedish ski high schools, and additionally
to study possible gender differences.
Study II: To investigate a possible relationship between the prevalence of ACL injuries in
alpine ski students at the Swedish ski high schools and ACL injuries in their parents.
Study III: To identify potential intrinsic and extrinsic risk factors for ACL injuries in alpine
ski students at the Swedish ski high schools.
Study IV: To evaluate whether a specific prevention program could reduce the incidence of
ACL injuries in alpine ski students at the Swedish ski high schools.

16
17
MATERIAL AND METHODS 4
The present thesis has been based on van Mechelen´s ”Sequence of Prevention”. 130
Several
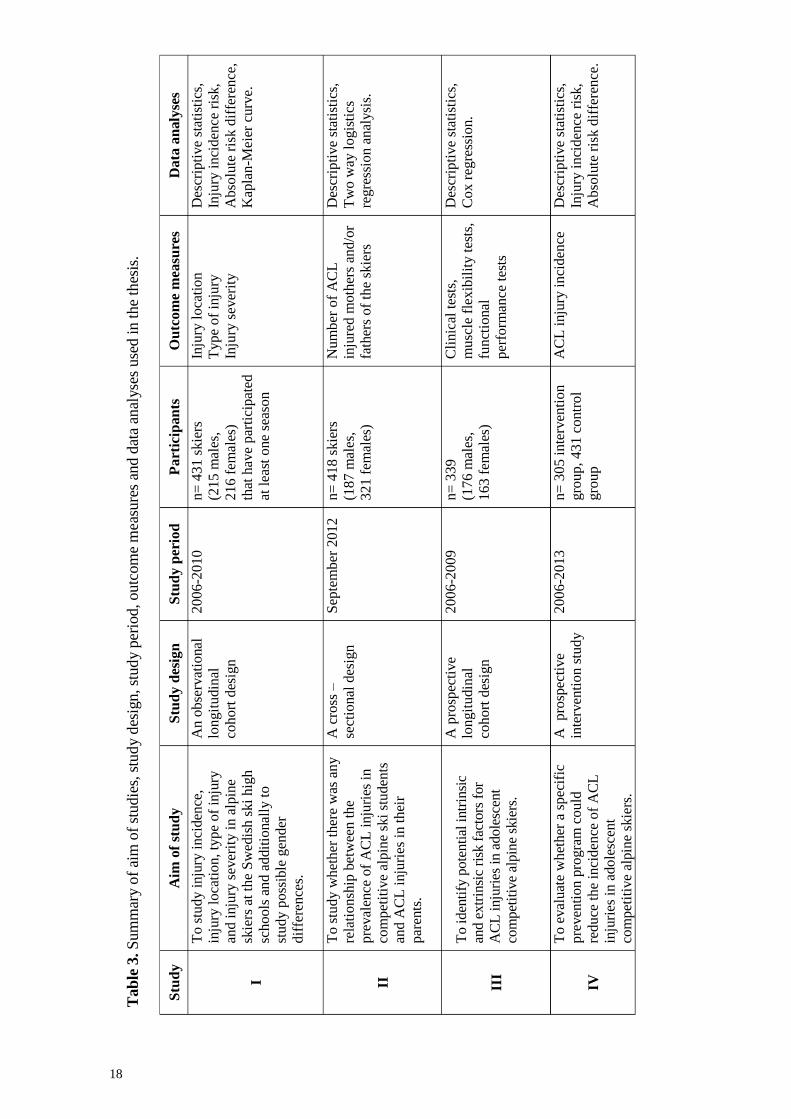
outcome measures have been used in the four studies included in the thesis (Table 3). A short
summary of the study outlines are presented below, followed by a more detailed description
in tables and text regarding population, evaluation methods and testing procedure as well as
data analysis. Data collection started in August 2006 and was ended in May 2013. The
project was preceded by a pilot study during the ski season 2005/2006 133
. The STROBE
guidelines for reporting of observational epidemiological studies have been applied in the
present thesis. 135
4.1 STUDY DESIGNS
Study I
An observational longitudinal cohort design was used to identify an injury profile of
competitive alpine ski students regarding injury location, type of injury and injury incidence.
Four hundred and thirty-one skiers (215 males and 216 females) were prospectively followed
at least one season during their study time at a ski high school. The study period started in
August 2006 and ended in June 2010.
Study II
A cross–sectional design was used to evaluate a possible relationship between the prevalence
of ACL injuries in competitive alpine ski students and their parents. In September 2012 all
alpine ski students (n= 593), who have studied at a Swedish ski high school during 2006 and
2012 were invited to answer a questionnaire whether they and/or one or both parents had
suffered an ACL injury.
Study III
A prospective cohort design was used to identify possible intrinsic and extrinsic risk factors
for ACL injuries in competitive alpine ski students. A cohort of 339 alpine ski students went
through a clinical examination and 25 of them sustained a first time ACL injury during the
season following the clinical examination. The study was carried out during the seasons
2006/2007 and 2009/2010.
Study IV
A prospective intervention study was used to investigate whether a specific prevention
program tailored for alpine ski students at a Swedish ski high school could reduce the number
of ACL injuries in this cohort. In September 2011 a specific prevention program was
implemented at the ski high schools. The prevention program was focused on each skier´s
awareness to perform different exercises equally well on the right as on the left lower
extremity. The intervention group consisted of 305 alpine ski students that attended the ski
high schools during the seasons 2011/2012 and 2012/2013. The control group (n=431)
consisted of those alpine ski students that attended the ski high schools during five seasons
(2006/2007 - 2010/2011).
18
Tab
le 3
. S
um
mar
y o
f ai
m o
f st
udie
s, s
tud
y d
esig
n, st
ud
y p
erio
d, outc
om
e m
easu
res
and d
ata
anal
yse
s use
d i
n t
he
thes
is.
Stu
dy
Aim
of
stu
dy
Stu
dy d
esig
n
Stu
dy p
erio
d
Part
icip
an
ts
Ou
tco
me
mea
sure
s D
ata
an
aly
ses
I
To
stu
dy i
nju
ry i
nci
den
ce,
inju
ry l
oca
tio
n, ty
pe
of
inju
ry
and
inju
ry s
ever
ity i
n a
lpin
e
skie
rs a
t th
e S
wed
ish
ski
hig
h
sch
ools
an
d a
ddit
ional
ly t
o
stu
dy p
oss
ible
gen
der
dif
fere
nce
s.
An o
bse
rvat
ional
longit
udin
al
cohort
des
ign
2006
-2010
n=
431 s
kie
rs
(215 m
ales
,
216 f
emal
es)
that
hav
e p
arti
cip
ated
at l
east
one
seas
on
Inju
ry l
oca
tio
n
Typ
e o
f in
jury
Inju
ry s
ever
ity
Des
crip
tive
stat
isti
cs,
Inju
ry i
nci
den
ce r
isk,
Ab
solu
te r
isk d
iffe
ren
ce,
Kap
lan
-Mei
er c
urv
e.
II
To
stu
dy w
het
her
ther
e w
as a
ny
rela
tio
nsh
ip b
etw
een
th
e
pre
val
ence
of
AC
L i
nju
ries
in
com
pet
itiv
e al
pin
e sk
i st
uden
ts
and
AC
L i
nju
ries
in
th
eir
par
ents
.
A c
ross
–
sect
ional
des
ign
Sep
tem
ber
2012
n=
418 s
kie
rs
(187 m
ales
,
321 f
emal
es)
Nu
mb
er o
f A
CL
inju
red
mo
ther
s an
d/o
r
fath
ers
of
the
skie
rs
Des
crip
tive
stat
isti
cs,
Tw
o w
ay l
ogis
tics
regre
ssio
n a
nal
ysi
s.
III
To i
den
tify
pote
nti
al i
ntr
insi
c
and e
xtr
insi
c ri
sk f
acto
rs f
or
AC
L i
nju
ries
in a
dole
scen
t
com
pet
itiv
e al
pin
e sk
iers
.
A p
rosp
ecti
ve
longit
udin
al
coh
ort
des
ign
2006
-2009
n=
339
(176 m
ales
,
16
3 f
emal
es)
Cli
nic
al t
ests
,
mu
scle
fle
xib
ilit
y t
ests
,
funct
ional
per
form
ance
tes
ts
Des
crip
tive
stat
isti
cs,
Co
x r
egre
ssio
n.
IV
To
eval
uat
e w
het
her
a s
pec
ific
pre
ven
tio
n p
rogra
m c
ou
ld
red
uce
th
e in
cid
ence
of
AC
L
inju
ries
in
ado
lesc
ent
com
pet
itiv
e al
pin
e sk
iers
.
A
pro
spec
tive
inte
rven
tion s
tudy
2006
-2013
n=
305 i
nte
rven
tio
n
gro
up,
431 c
ontr
ol
gro
up
AC
L i
nju
ry i
nci
den
ce
Des
crip
tive
stat
isti
cs,
Inju
ry i
nci
den
ce r
isk,
Ab
solu
te r
isk d
iffe
ren
ce.
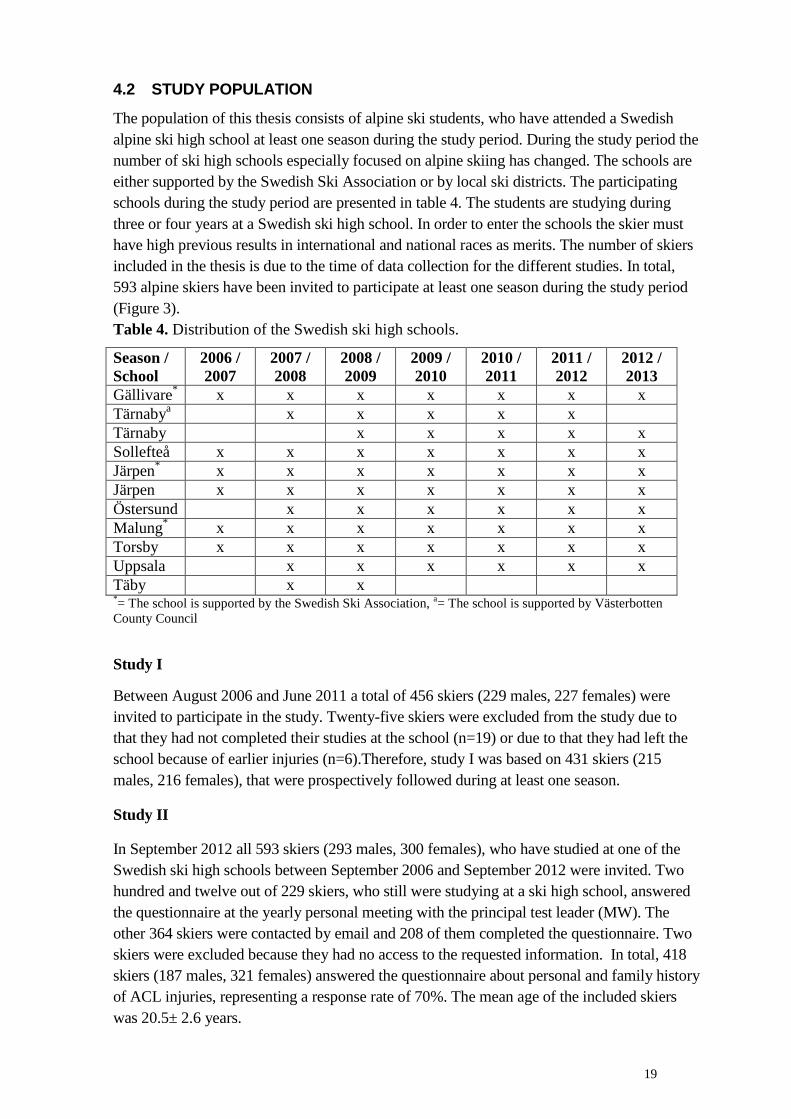
19
4.2 STUDY POPULATION
The population of this thesis consists of alpine ski students, who have attended a Swedish
alpine ski high school at least one season during the study period. During the study period the
number of ski high schools especially focused on alpine skiing has changed. The schools are
either supported by the Swedish Ski Association or by local ski districts. The participating
schools during the study period are presented in table 4. The students are studying during
three or four years at a Swedish ski high school. In order to enter the schools the skier must
have high previous results in international and national races as merits. The number of skiers
included in the thesis is due to the time of data collection for the different studies. In total,
593 alpine skiers have been invited to participate at least one season during the study period
(Figure 3).
Table 4. Distribution of the Swedish ski high schools.
Season /
School
2006 /
2007
2007 /
2008
2008 /
2009
2009 /
2010
2010 /
2011
2011 /
2012
2012 /
2013
Gällivare*
x x x x x x x
Tärnabya
x x x x x
Tärnaby x x x x x
Sollefteå x x x x x x x
Järpen*
x x x x x x x
Järpen x x x x x x x
Östersund x x x x x x
Malung*
x x x x x x x
Torsby x x x x x x x
Uppsala x x x x x x
Täby x x *= The school is supported by the Swedish Ski Association,
a= The school is supported by Västerbotten
County Council
Study I
Between August 2006 and June 2011 a total of 456 skiers (229 males, 227 females) were
invited to participate in the study. Twenty-five skiers were excluded from the study due to
that they had not completed their studies at the school (n=19) or due to that they had left the
school because of earlier injuries (n=6).Therefore, study I was based on 431 skiers (215
males, 216 females), that were prospectively followed during at least one season.
Study II
In September 2012 all 593 skiers (293 males, 300 females), who have studied at one of the
Swedish ski high schools between September 2006 and September 2012 were invited. Two
hundred and twelve out of 229 skiers, who still were studying at a ski high school, answered
the questionnaire at the yearly personal meeting with the principal test leader (MW). The
other 364 skiers were contacted by email and 208 of them completed the questionnaire. Two
skiers were excluded because they had no access to the requested information. In total, 418
skiers (187 males, 321 females) answered the questionnaire about personal and family history
of ACL injuries, representing a response rate of 70%. The mean age of the included skiers
was 20.5± 2.6 years.

20
Figure 3. Flow chart of the skiers in the thesis
Study III
Alpine ski students attending a Swedish ski high school between September 2006 and May
2010 were invited to participate in this study. Totally 384 skiers (191 males and 193 females)
accepted to participate. Forty-six skiers were excluded from the study, since they did not
complete a full year at the school (n=17) or entered the study with a previous ACL injury
(n=28, 4 males and 24 females). Consequently, the study was based on 339 skiers (176 males
and 163 females) without an earlier ACL injury.
Study IV
In study IV 308 skiers belonged to an intervention group and 456 skiers to a control group.
The control group consisted of all available skiers studying at a ski high school between the
seasons 2006/2007 and 2010/2011. The intervention group consisted of the skiers attending a
school during two seasons, 2011/2012 and 2012/2013. Two ski seasons or 21 months
attending a ski high school were the maximal time of exposure for each skier. A total of 28
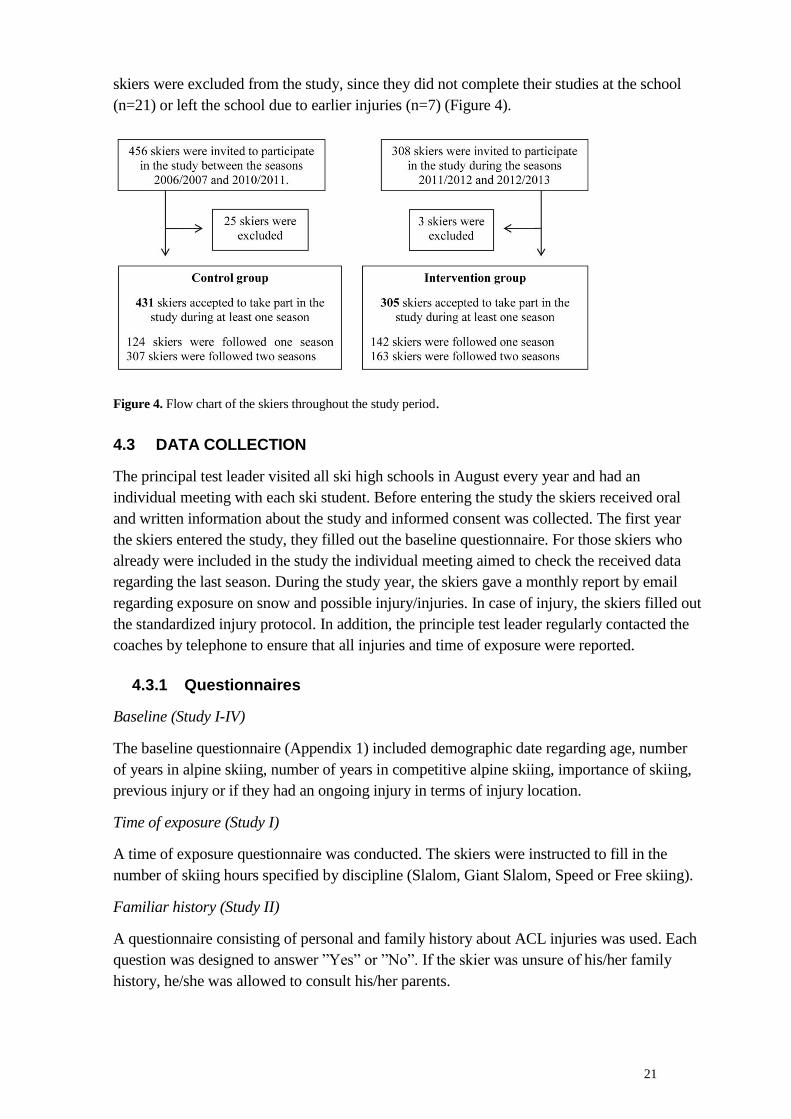
21
skiers were excluded from the study, since they did not complete their studies at the school
(n=21) or left the school due to earlier injuries (n=7) (Figure 4).
Figure 4. Flow chart of the skiers throughout the study period.
4.3 DATA COLLECTION
The principal test leader visited all ski high schools in August every year and had an
individual meeting with each ski student. Before entering the study the skiers received oral
and written information about the study and informed consent was collected. The first year
the skiers entered the study, they filled out the baseline questionnaire. For those skiers who
already were included in the study the individual meeting aimed to check the received data
regarding the last season. During the study year, the skiers gave a monthly report by email
regarding exposure on snow and possible injury/injuries. In case of injury, the skiers filled out
the standardized injury protocol. In addition, the principle test leader regularly contacted the
coaches by telephone to ensure that all injuries and time of exposure were reported.
4.3.1 Questionnaires
Baseline (Study I-IV)
The baseline questionnaire (Appendix 1) included demographic date regarding age, number
of years in alpine skiing, number of years in competitive alpine skiing, importance of skiing,
previous injury or if they had an ongoing injury in terms of injury location.
Time of exposure (Study I)
A time of exposure questionnaire was conducted. The skiers were instructed to fill in the
number of skiing hours specified by discipline (Slalom, Giant Slalom, Speed or Free skiing).
Familiar history (Study II)
A questionnaire consisting of personal and family history about ACL injuries was used. Each
question was designed to answer ”Yes” or ”No”. If the skier was unsure of his/her family
history, he/she was allowed to consult his/her parents.
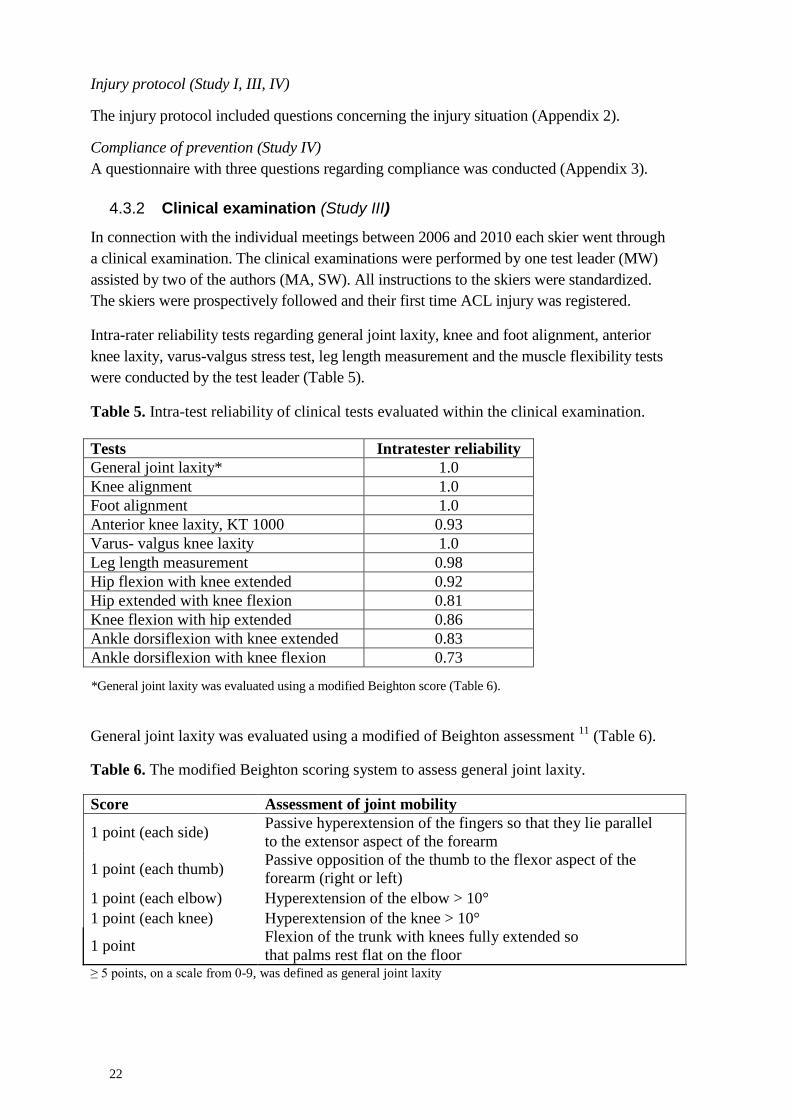
22
Injury protocol (Study I, III, IV)
The injury protocol included questions concerning the injury situation (Appendix 2).
Compliance of prevention (Study IV)
A questionnaire with three questions regarding compliance was conducted (Appendix 3).
4.3.2 Clinical examination (Study III)
In connection with the individual meetings between 2006 and 2010 each skier went through
a clinical examination. The clinical examinations were performed by one test leader (MW)
assisted by two of the authors (MA, SW). All instructions to the skiers were standardized.
The skiers were prospectively followed and their first time ACL injury was registered.
Intra-rater reliability tests regarding general joint laxity, knee and foot alignment, anterior
knee laxity, varus-valgus stress test, leg length measurement and the muscle flexibility tests
were conducted by the test leader (Table 5).
Table 5. Intra-test reliability of clinical tests evaluated within the clinical examination.
Tests Intratester reliability
General joint laxity* 1.0
Knee alignment 1.0
Foot alignment 1.0
Anterior knee laxity, KT 1000 0.93
Varus- valgus knee laxity 1.0
Leg length measurement 0.98
Hip flexion with knee extended 0.92
Hip extended with knee flexion 0.81
Knee flexion with hip extended 0.86
Ankle dorsiflexion with knee extended 0.83
Ankle dorsiflexion with knee flexion 0.73
*General joint laxity was evaluated using a modified Beighton score (Table 6).
General joint laxity was evaluated using a modified of Beighton assessment 11
(Table 6).
Table 6. The modified Beighton scoring system to assess general joint laxity.
Score Assessment of joint mobility
1 point (each side) Passive hyperextension of the fingers so that they lie parallel
to the extensor aspect of the forearm
1 point (each thumb) Passive opposition of the thumb to the flexor aspect of the
forearm (right or left)
1 point (each elbow) Hyperextension of the elbow > 10°
1 point (each knee) Hyperextension of the knee > 10°
1 point Flexion of the trunk with knees fully extended so
that palms rest flat on the floor ≥ 5 points, on a scale from 0-9, was defined as general joint laxity

23
Anatomical alignment of the knee and foot was determined in a standing position. The
relationship between the knee joint and calcaneus was estimated as either varus, normal or
valgus. 71
Leg length discrepancy was measured with the skier lying on a bench in supine position. The
distance from the spina iliaca anterior superior (SIAS) to the medial malleolus of the ankle
was measured with a measure tape. A side-to-side discrepancy of ≥2 cm was considered as
asymmetry. 10
Valgus-varus stress test of the knee joint was assessed in 30° of knee flexion. The skier was
lying on a bench in supine position. The test leader stressed the knee in valgus and varus and
assessed the movement as positive or negative. 55
Anterior knee laxity was measured with KT-1000 (MED metric Corp., San Diego CA,
USA). The test was performed in 30° of knee flexion with the skier in supine position using a
foot support to prevent external tibia rotation of both legs. The joint line was marked, the
arms were placed along the side of the body and the skier was instructed to stay relaxed from
a muscular point of view. Prior to each measurement the KT-1000 was calibrated. The
measurements were performed three times on each leg. The highest value of the different
measurements (30lb and manual max) was recorded in mm. A side-to-side difference of
≥ 3 mm was defined as an increased knee laxity 22
(Figure 5).
Figure x. Anterior knee laxity.
Ankle dorsiflexion was measured using a goniometer. The measurements were performed
with the knee joint in both extension and flexion. The skier was standing with one leg in front
of the other leg. With the rear leg in full knee extension and the heel maintained against the
floor while loading the flexed front leg, ankle dorsiflexion of the rear leg was measured.
With the rear leg in knee flexion and the heel maintained against the floor while loading the
flexed front leg, ankle dorsiflexion of the rear leg was measured. One trial of each leg was
performed and the result was given in degrees 25
(Figure 6).
Hip flexion with knee extended according to Ekstrand et al. 25
was performed in order to
measure muscle length of the hamstring muscles. The skier was measured in supine position
with a flexometer (“Myrin”, Follo A/S, Norway) applied to the basis of the patella. The pelvis
and the contralateral leg were manually fixed. The skier´s test leg was passively raised with
Figure 5. Anterior knee laxity
measured with KT 1000. Figure 6. Ankle dorsiflexion measured
using a goniometer
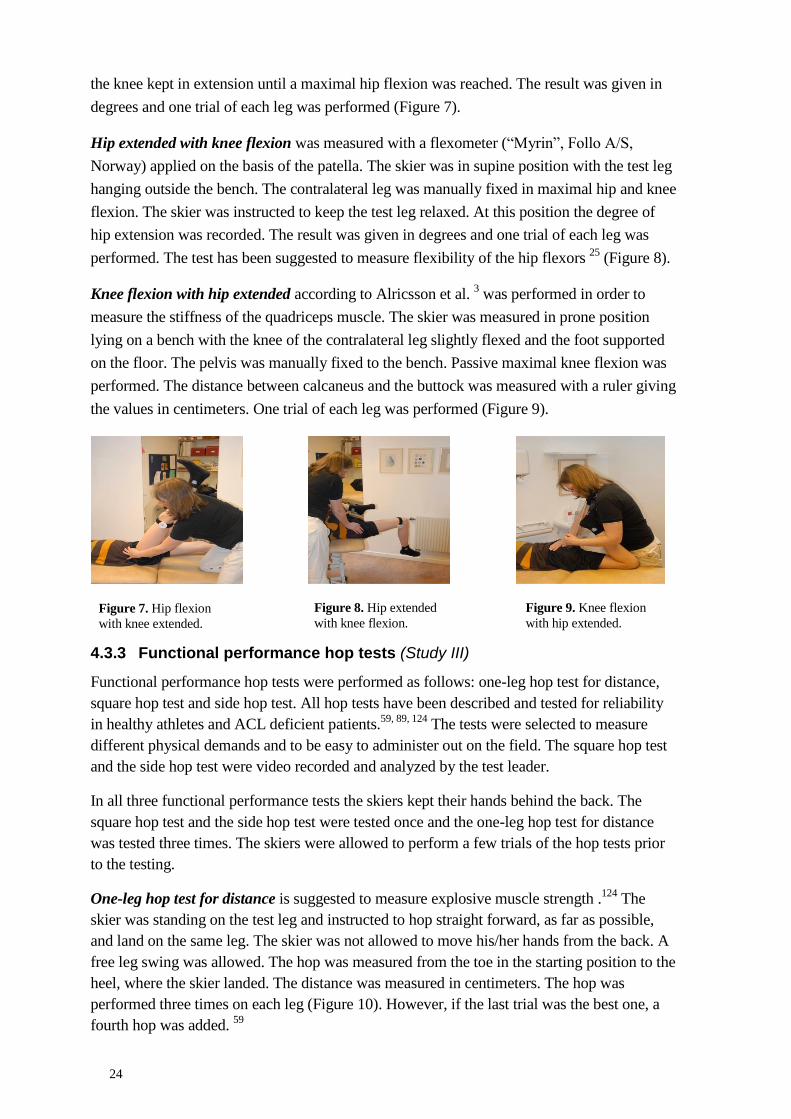
24
the knee kept in extension until a maximal hip flexion was reached. The result was given in
degrees and one trial of each leg was performed (Figure 7).
Hip extended with knee flexion was measured with a flexometer (“Myrin”, Follo A/S,
Norway) applied on the basis of the patella. The skier was in supine position with the test leg
hanging outside the bench. The contralateral leg was manually fixed in maximal hip and knee
flexion. The skier was instructed to keep the test leg relaxed. At this position the degree of
hip extension was recorded. The result was given in degrees and one trial of each leg was
performed. The test has been suggested to measure flexibility of the hip flexors 25
(Figure 8).
Knee flexion with hip extended according to Alricsson et al. 3 was performed in order to
measure the stiffness of the quadriceps muscle. The skier was measured in prone position
lying on a bench with the knee of the contralateral leg slightly flexed and the foot supported
on the floor. The pelvis was manually fixed to the bench. Passive maximal knee flexion was
performed. The distance between calcaneus and the buttock was measured with a ruler giving
the values in centimeters. One trial of each leg was performed (Figure 9).
4.3.3 Functional performance hop tests (Study III)
Functional performance hop tests were performed as follows: one-leg hop test for distance,
square hop test and side hop test. All hop tests have been described and tested for reliability
in healthy athletes and ACL deficient patients.59, 89, 124
The tests were selected to measure
different physical demands and to be easy to administer out on the field. The square hop test
and the side hop test were video recorded and analyzed by the test leader.
In all three functional performance tests the skiers kept their hands behind the back. The
square hop test and the side hop test were tested once and the one-leg hop test for distance
was tested three times. The skiers were allowed to perform a few trials of the hop tests prior
to the testing.
One-leg hop test for distance is suggested to measure explosive muscle strength .124
The
skier was standing on the test leg and instructed to hop straight forward, as far as possible,
and land on the same leg. The skier was not allowed to move his/her hands from the back. A
free leg swing was allowed. The hop was measured from the toe in the starting position to the
heel, where the skier landed. The distance was measured in centimeters. The hop was
performed three times on each leg (Figure 10). However, if the last trial was the best one, a
fourth hop was added. 59
Figure 7. Hip flexion
with knee extended.
Figure 8. Hip extended
with knee flexion.
Figure 9. Knee flexion
with hip extended.
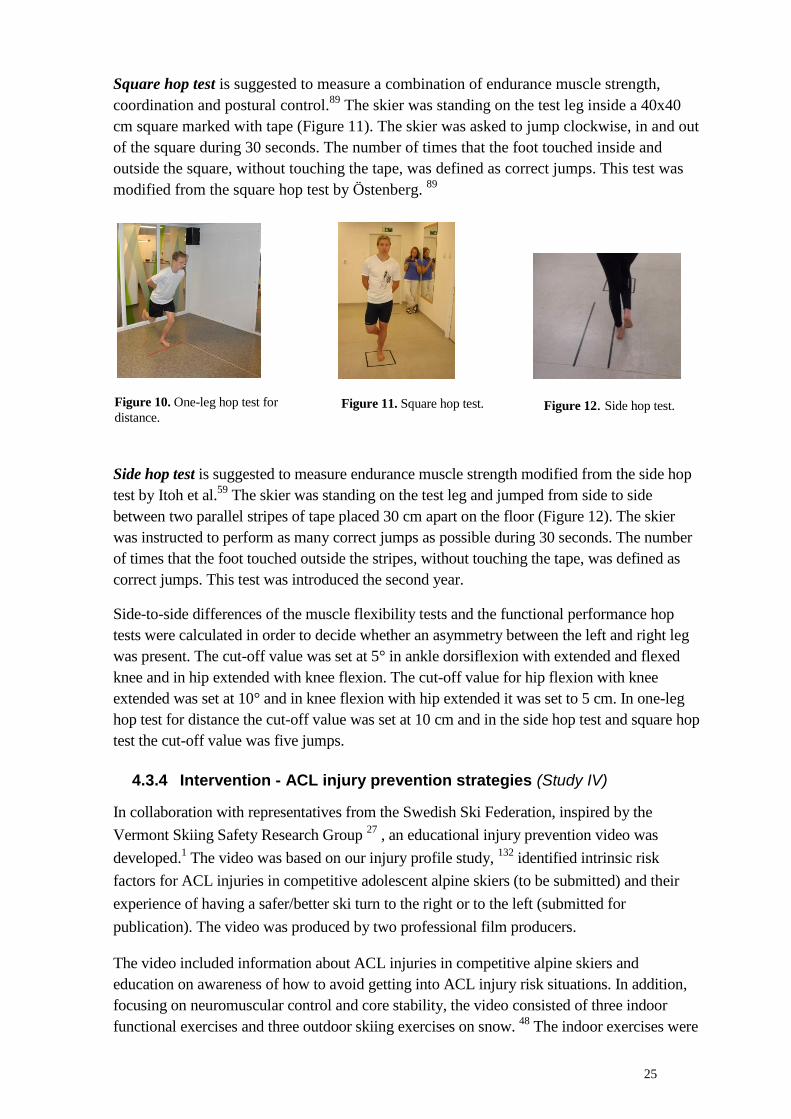
25
Square hop test is suggested to measure a combination of endurance muscle strength,
coordination and postural control.89
The skier was standing on the test leg inside a 40x40
cm square marked with tape (Figure 11). The skier was asked to jump clockwise, in and out
of the square during 30 seconds. The number of times that the foot touched inside and
outside the square, without touching the tape, was defined as correct jumps. This test was
modified from the square hop test by Östenberg. 89
Side hop test is suggested to measure endurance muscle strength modified from the side hop
test by Itoh et al.59
The skier was standing on the test leg and jumped from side to side
between two parallel stripes of tape placed 30 cm apart on the floor (Figure 12). The skier
was instructed to perform as many correct jumps as possible during 30 seconds. The number
of times that the foot touched outside the stripes, without touching the tape, was defined as
correct jumps. This test was introduced the second year.
Side-to-side differences of the muscle flexibility tests and the functional performance hop
tests were calculated in order to decide whether an asymmetry between the left and right leg
was present. The cut-off value was set at 5° in ankle dorsiflexion with extended and flexed
knee and in hip extended with knee flexion. The cut-off value for hip flexion with knee
extended was set at 10° and in knee flexion with hip extended it was set to 5 cm. In one-leg
hop test for distance the cut-off value was set at 10 cm and in the side hop test and square hop
test the cut-off value was five jumps.
4.3.4 Intervention - ACL injury prevention strategies (Study IV)
In collaboration with representatives from the Swedish Ski Federation, inspired by the
Vermont Skiing Safety Research Group 27
, an educational injury prevention video was
developed.1 The video was based on our injury profile study,
132 identified intrinsic risk
factors for ACL injuries in competitive adolescent alpine skiers (to be submitted) and their
experience of having a safer/better ski turn to the right or to the left (submitted for
publication). The video was produced by two professional film producers.
The video included information about ACL injuries in competitive alpine skiers and
education on awareness of how to avoid getting into ACL injury risk situations. In addition,
focusing on neuromuscular control and core stability, the video consisted of three indoor
functional exercises and three outdoor skiing exercises on snow. 48
The indoor exercises were
Figure 11. Square hop test. Figure 12. Side hop test. Figure 10. One-leg hop test for
distance.
26
one-leg hop test for distance, 59
square hop test 89
and single leg squat. 57
The outdoor
exercises were suggested by the Swedish Ski Federation, the shuffle, the back and forth, and
turns with lifted inner ski. The videotape demonstrated how to perform each exercises with
proper technique and the skiers were instructed to be aware of whether they were able to
perform the exercises equally well on both legs as well as equally well ski turns to the left as
to the right.
First year
The prevention program was introduced in September 2011 and all ski coaches were taught
how to implement the preventive strategies. The video has been used as a support in order to
educate the ski students about ACL injury prevention. They were instructed to watch the
movie every third week between September and November (preseason) and once each month
between December and April (competition season).The education included information about
identified risk factors for ACL injuries in alpine skiing and the importance of stimulating the
skiers to perform the suggested exercises. The coaches were informed about the fact that left
leg was more often injured and that the exercises should be performed equally good on both
legs.
Second year
Prior to the second year the principal test leader educated the new ski students and reminded
the other ski students about the prevention strategies by visiting every ski high school at
preseason.
During the entire study period the principal test leader had monthly contacts with as well
the ski students as their coaches. The reason for these contacts was to ensure data injury
collection and information about how the skiers complied with the suggested exercises.
Compliance to the training was collected using a questionnaire.
At the end of the second year all coaches were re-invited to a meeting in order to secure
that all ACL injuries had been recorded and reported to the principal test leader.
4.3.5 Injury definition and classification
Injury definitions
In the present investigation an injury was defined as an injury that occurred during training or
competition, which made it impossible for the skier to participate fully in skiing or physical
training for at least one training session or competition.36
A previous injury was defined as an injury that the skier had sustained earlier and from which
he/she had fully recovered and been allowed to return to skiing before enrolled in the study.
An ongoing injury was defined as an injury from which the skier was still suffering and for
whom active rehabilitation was ongoing.
A first time ACL injury was defined as the first time a total ACL injury occurred.
27
Injury classification
Definitions of injury location and type of injury were based on the Orchard Sports Injury
Classification System (OSICS). 87
Injuries to the spine included injuries of the neck, thorax
and lumbar spine. Trunk injuries included injuries of the chest and abdomen. All reported
ACL injuries in the present thesis were total ACL ruptures, diagnosed by experienced sports
orthopedic surgeons.
The classification of the injuries was based on the time-loss definition: minimal injury 1-3
days, mild injury 4-7 days, moderate injury 8-28 days, and severe injury ≥ 28 days. 36
4.4 STATISTICAL METHODS AND DATA ANALYSIS
The Statistica, StatSoft®, Scandinavia AB, for personal computer was used for statistical
analysis in all papers except for study II where the Statistical Package for the Social Sciences,
SPSS 20.0 was used. The quantitative data are presented as mean and standard deviation or
median and range. Categorical data are presented as frequencies, portions and percentage in
all studies. The statistical significant level was set at 0.05. The statistical methods and data
analyses used are presented in detail below.
Study I
To compare males and females, the Chi 2 test was used for categorical variables and t-test for
continuous variables. Injury incidence rate (IRR) was calculated as the number of injuries per
1000 hours exposure for skiing and as the number of injuries per 100 months attended a ski
high school and were presented for males and females with 95% Confidence Interval (CI) for
different injury locations. The absolute risk, incidence rate difference (IRD), between males
and females for different localization was calculated with 95% CI. P-values for the
comparisons were also presented. Poisson distribution and test-based methods were used to
construct the confidence intervals.108
Kaplan-Meier survival curves were calculated for time
to the first injury development in groups, skiers with an ongoing injury and skiers without
injury at the start of the study and also in groups of skiers that sustained one injury, two
injuries, three injuries and four injuries during the study period. In comparisons between the
two groups, the non-parametric log-rank test was used.
Study II
An ACL injury in the skier and in one of his/her parents were coded as "Yes" or "No".
Furthermore, a variable, "ACL injury of either parent" was encoded in the same way, "Yes"
or "No". If either parent or both parents had an ACL injury the code was "Yes". For
categorical data the Chi-2 test was used to study possible group differences. The level of
significance was set at p <0.05. Two logistic regression analyses with multivariate method
were performed to control for gender, where male skiers were coded to 1 and female skiers to
2. In the first step the independent variables were gender and an ACL injured father or an
ACL injured mother. The dependent variable was an ACL injury in an alpine skier. The
second step was an ACL injured father or an ACL injured mother with the variable "ACL
injury of either parent." The results are presented as Odds Ratio (OR) with 95 % (CI)
28
Study III
Differences in continuous variables between the study groups were analyzed using Student´s
t test. For categorical variables the Chi-2 test was used.
Extrinsic risk factors are presented with cross tables and frequencies and percentages.
The exposure data were calculated as the total number of months attending a ski high school
and the injury rates (IR) were reported as the total number of ACL injuries per 100 months
attending a ski high school. The prevalence of ACL injury was calculated as the number of
ACL injuries divided by the total number of skiers. To investigate intrinsic risk factors the
values of the latest clinical examination before ACL injury were used, and for the uninjured
skiers the values of the latest clinical examination during their participation in the project
were used. A Cox proportional Hazard regression model was used to identify intrinsic risk
factors for ACL injuries. The time to the first injury was considered important because of the
risk that clinical tests may change after injury. Only the first time ACL injuries were included
in the analysis. Univariate analyses were performed, entering each variable separately into the
Cox regression model. Variables with a p-value <0.05 in the Cox model were illustrated with
Kaplan-Meier curves. The results were reported as Hazard ratios (HR) with 95% (CI). The
intra-reliability coefficients were calculated using the method by Bland and Altman. 17
Study IV
ACL injury prevalence was calculated as the number of ACL injuries divided by the total
number of skiers. Time of exposure was calculated as the total number of months that a skier
was attending a ski high school and the ACL injury incidence (IR) was reported as the total
number of ACL injuries per 100 months that a skier was attending a ski high school. A 95%
confidence interval was estimated. The absolute rate reduction of the intervention was
calculated as absolute incidence rate differences [IRD= IR (intervention group) - IR (control
group)] with 95% (CI).105
The time to the occurrence of an ACL injury between the groups
was calculated and presented with the Kaplan-Meier survival curve.
4.4.1 Power analysis
Prior to the study a power analysis was made based on the number of ACL injuries. The
power analysis was estimated to detect 25 ACL injuries during an observation period of five
years, significance level was set to 0.05 and the statistical power was 80%. The study needed
136 skiers in each group in order to detect the estimated effect with an effect size of 0.35.
4.5 ETHICAL APPROVAL
All studies in the present thesis were approved by the Regional Ethics Committee in
Stockholm, Sweden.
Dnr 2006/833-31/1 (Study I, III, IV and unpublished data)
Dnr: 2012/1280-32 (Study II)

29
Prior to entering the studies all skiers and their coaches were given both oral and written
information about the studies. Participation was voluntary and all skiers and coaches agreed
to participate in this thesis.

31
RESULTS 5
The thesis is based on a project included 593 alpine skiers´ attending a ski high schools. The
baseline ski related factors are presented in table 7.
Table 7. Demographic data of the skiers at the time when they entered the study.
Skiers related factors Male skiers (n=293) Female skiers (n=300)
Age 16.5 ±0.9 16.4±0.8
Skiing experience (year) 10.1±1.93 10.3±1.89
Competitive experience
(year) 7.7±2.16 7.7±2.19
FIS-point SL 102±62.5 98±80.1
FIS-point GS 128±126.7 114±104.9
Previous injury 172 (59%) 193 (64%)
Ongoing injury 49 (17%) 81 (27%)
Three hundred and sixty-five out of 593 skiers (172 males, 193 females) reported a previous
injury when they entered the study. The lower extremity (hip, groin, knee, lower leg, foot,
heel, and toe) accounted for 71% of all injuries.
One hundred and thirty out of 593 skiers reported ongoing injuries when they entered the
study. Fifty-two skiers (40%) reported injuries to the knee, and 42 skiers (32%) injuries to
other locations of the lower extremity.
5.1 INJURY PROFILE BETWEEN THE SEASONS 2006/2007 AND 2010/2011
Injuries and injury incidence
One hundred and ninety-three skiers (91 males, 102 females) sustained a total of 312 injuries
during the five year period that the skiers were prospectively followed. Two hundred and
sixty-five injuries (85%) occurred during skiing and 47 injuries (15%) occurred during
physical training. There was a total incidence rate for males and females of 1.7 injuries/1000
skiing hours (95% CI 1.51–1.88) or 3.11 injuries/100 months of studies at a ski high school
(95% CI 2.77–3.46). The incidence rate for males was 1.62 injuries/1000 ski hours (95% CI
1.36–1.88) or 2.97 injuries/100 months of studies at a ski high school (95% CI 2.50–3.45)
and for females 1.77 injuries/1000 skiing hours (95% CI 1.50–2.04) or 3.25 injuries/100
months of studies at a ski high school (95% CI 2.75–3.75). The highest number of
injuries/1000 skiing hours was found in the knee joint for both male and female skiers (Table
9).
No significant gender differences were found when it comes to the number of reported
injuries. The risk of sustaining a new injury increased the sooner the first time injury occurred
(p=0.001). No significant difference was found in this aspect between those skiers who had
an ongoing injury and those who were not injured when entering the study.
The absolute risk for being injured showed that males have a higher risk than females to
sustain injuries to the hand/finger/thumb (p= 0.01) (Table 9).
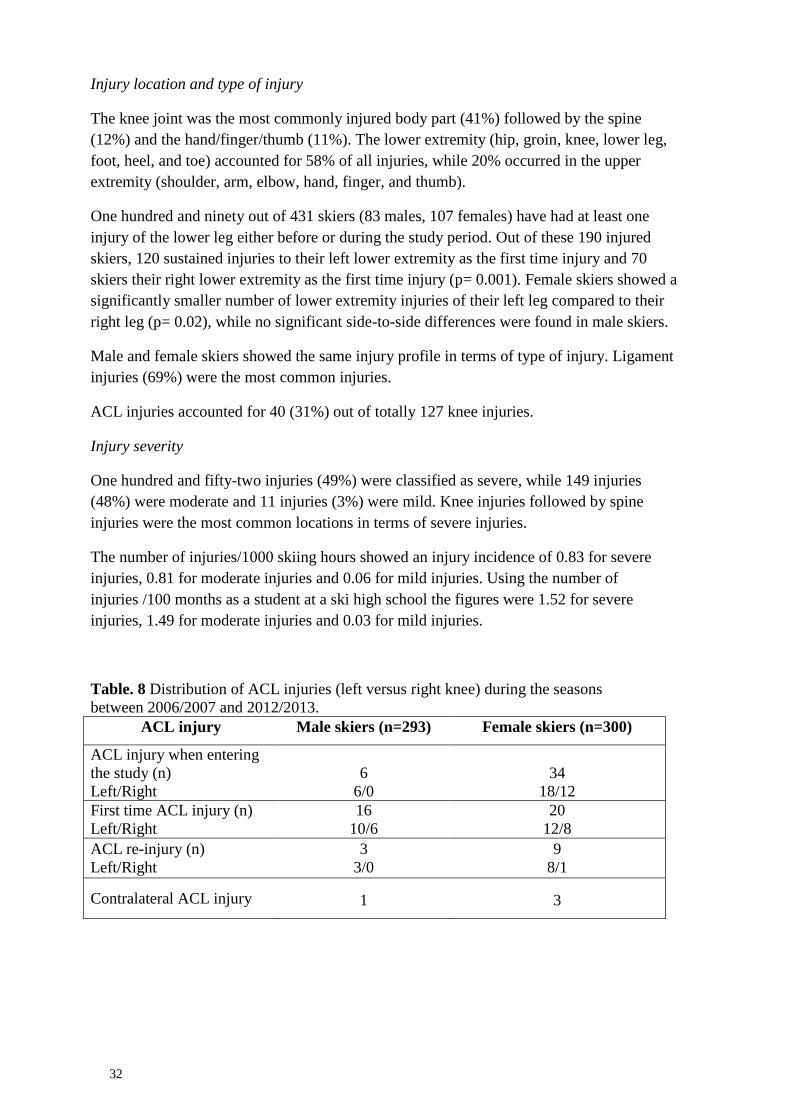
32
Injury location and type of injury
The knee joint was the most commonly injured body part (41%) followed by the spine
(12%) and the hand/finger/thumb (11%). The lower extremity (hip, groin, knee, lower leg,
foot, heel, and toe) accounted for 58% of all injuries, while 20% occurred in the upper
extremity (shoulder, arm, elbow, hand, finger, and thumb).
One hundred and ninety out of 431 skiers (83 males, 107 females) have had at least one
injury of the lower leg either before or during the study period. Out of these 190 injured
skiers, 120 sustained injuries to their left lower extremity as the first time injury and 70
skiers their right lower extremity as the first time injury (p= 0.001). Female skiers showed a
significantly smaller number of lower extremity injuries of their left leg compared to their
right leg (p= 0.02), while no significant side-to-side differences were found in male skiers.
Male and female skiers showed the same injury profile in terms of type of injury. Ligament
injuries (69%) were the most common injuries.
ACL injuries accounted for 40 (31%) out of totally 127 knee injuries.
Injury severity
One hundred and fifty-two injuries (49%) were classified as severe, while 149 injuries
(48%) were moderate and 11 injuries (3%) were mild. Knee injuries followed by spine
injuries were the most common locations in terms of severe injuries.
The number of injuries/1000 skiing hours showed an injury incidence of 0.83 for severe
injuries, 0.81 for moderate injuries and 0.06 for mild injuries. Using the number of
injuries /100 months as a student at a ski high school the figures were 1.52 for severe
injuries, 1.49 for moderate injuries and 0.03 for mild injuries.
Table. 8 Distribution of ACL injuries (left versus right knee) during the seasons
between 2006/2007 and 2012/2013. ACL injury Male skiers (n=293) Female skiers (n=300)
ACL injury when entering
the study (n)
Left/Right
6
6/0
34
18/12
First time ACL injury (n)
Left/Right
16
10/6
20
12/8
ACL re-injury (n)
Left/Right
3
3/0
9
8/1
Contralateral ACL injury 1 3
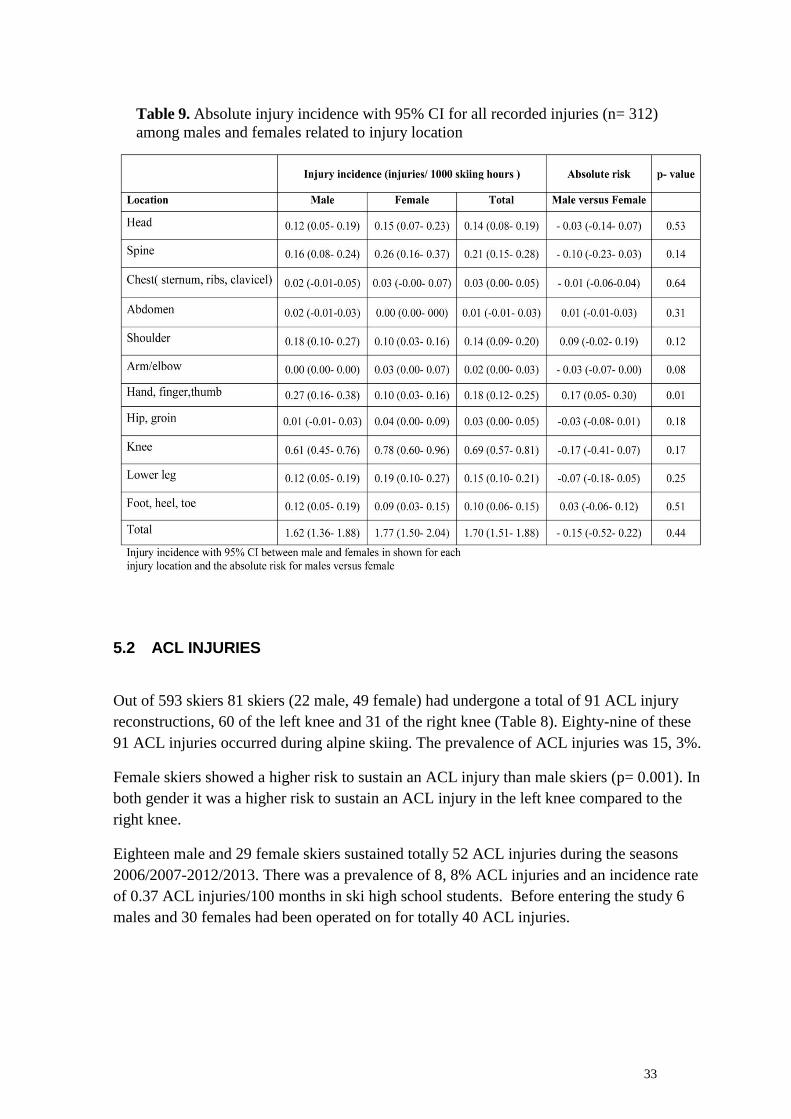
33
5.2 ACL INJURIES
Out of 593 skiers 81 skiers (22 male, 49 female) had undergone a total of 91 ACL injury
reconstructions, 60 of the left knee and 31 of the right knee (Table 8). Eighty-nine of these
91 ACL injuries occurred during alpine skiing. The prevalence of ACL injuries was 15, 3%.
Female skiers showed a higher risk to sustain an ACL injury than male skiers (p= 0.001). In
both gender it was a higher risk to sustain an ACL injury in the left knee compared to the
right knee.
Eighteen male and 29 female skiers sustained totally 52 ACL injuries during the seasons
2006/2007-2012/2013. There was a prevalence of 8, 8% ACL injuries and an incidence rate
of 0.37 ACL injuries/100 months in ski high school students. Before entering the study 6
males and 30 females had been operated on for totally 40 ACL injuries.
Table 9. Absolute injury incidence with 95% CI for all recorded injuries (n= 312)
among males and females related to injury location

34
5.2.1 ACL injury - Intrinsic risk factor
Clinical examination
There were no significant differences between skiers, who sustained a first time ACL injury
and skiers who did not with respect to age, BMI, skiing experience and previous injuries.
Anthropometric data, muscle flexibility tests and functional performance hop tests are
presented in tables10 and 11, respectively. The ranges and standard deviations were smaller
in all measured variables in ACL injured skiers compared to those without an ACL injury
when it comes to muscle flexibility tests and functional performance hop tests. A Cox
proportional Hazard regression model was used to identify intrinsic risk factors for ACL
injuries (Table 12).
The ACL injured group showed an increased side-to-side difference in the one leg hop test
for distance (Table 10). When judging the skier´s side-to-side performance, equally
good/unequally good performance between legs in terms of the functional hop tests, the ACL
injured group showed a higher percentage of unequal side-to-side difference than the group
without an ACL injury (Table 10).
Table 10. Functional performance hop tests.
Group differences were analysed with Chi-2 test and Student’s t test.
Functional performance hop tests
ACL injured
skiers
(n=25)
Skiers without
an ACL injury
(n=314)
One-leg hop test for distance (cm)
Left leg a
158 (119-198) 157 (104-235)
Right leg a
150 (105-191) 156 (102-227)
≥ 10 cm side-to-side diff.b
9 (36%) 72 (23%)
Square hop test (number of correct hops)
Left leg a
76 (63-90) 74 (52-108)
Right leg a
76 (56-86) 75 (50-104)
> 5 side-to-side diff.b
15 (60%) 136 (43%)
Side hop test (number of correct hops) *
Left leg a
66 (49-73) 61 (31-81)
Right leg a
63 (51-74) 62 (33-82)
> 5 side-to-side diff.b
10 (63%) 132 (50%)
a Median and range b
Number and percentage
* ACL injured skiers (n=16), skiers without an ACL injury (n=265)
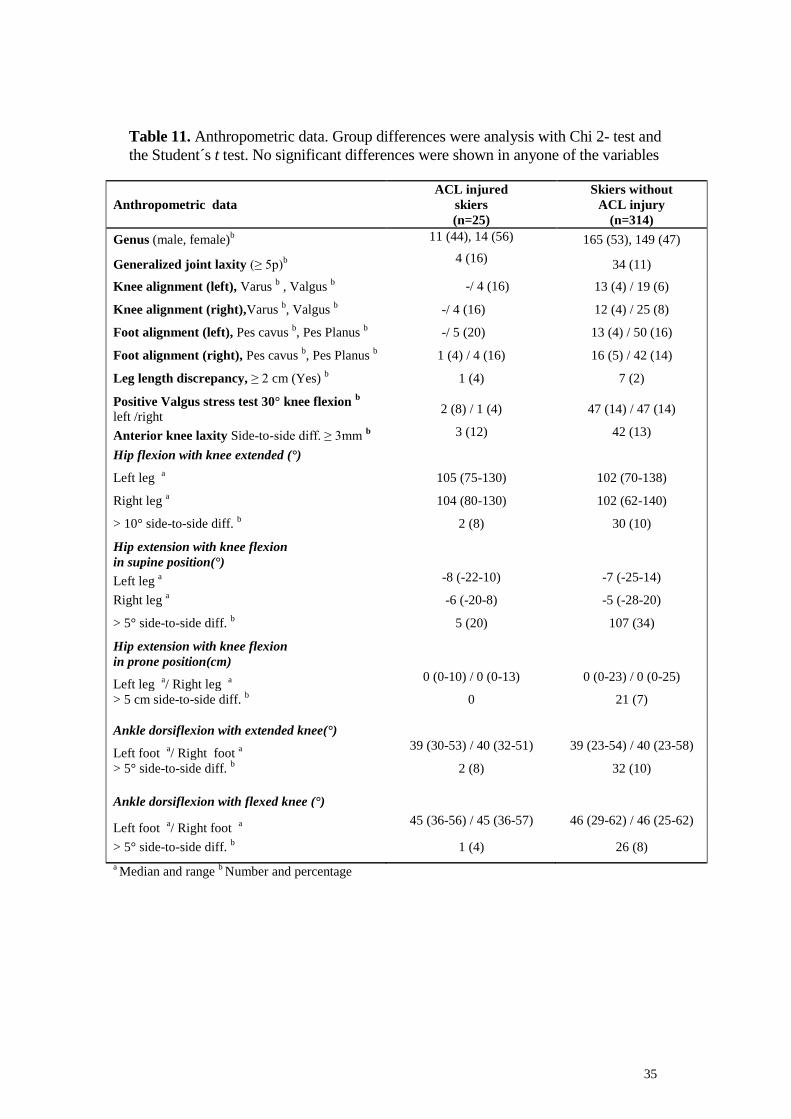
35
Anthropometric data
ACL injured
skiers
(n=25)
Skiers without
ACL injury
(n=314)
Genus (male, female)b 11 (44), 14 (56) 165 (53), 149 (47)
Generalized joint laxity (≥ 5p)b 4 (16)
34 (11)
Knee alignment (left), Varus b , Valgus
b -/ 4 (16) 13 (4) / 19 (6)
Knee alignment (right),Varus b, Valgus
b -/ 4 (16) 12 (4) / 25 (8)
Foot alignment (left), Pes cavus b, Pes Planus
b -/ 5 (20) 13 (4) / 50 (16)
Foot alignment (right), Pes cavus b, Pes Planus
b 1 (4) / 4 (16) 16 (5) / 42 (14)
Leg length discrepancy, ≥ 2 cm (Yes) b
1 (4) 7 (2)
Positive Valgus stress test 30° knee flexion b
left /right 2 (8) / 1 (4) 47 (14) / 47 (14)
Anterior knee laxity Side-to-side diff. ≥ 3mm b 3 (12) 42 (13)
Hip flexion with knee extended (°)
Left leg a 105 (75-130) 102 (70-138)
Right leg a
104 (80-130) 102 (62-140)
> 10° side-to-side diff. b
2 (8) 30 (10)
Hip extension with knee flexion
in supine position(°)
Left leg a -8 (-22-10) -7 (-25-14)
Right leg a -6 (-20-8) -5 (-28-20)
> 5° side-to-side diff. b
5 (20) 107 (34)
Hip extension with knee flexion
in prone position(cm)
Left leg a/ Right leg
a
0 (0-10) / 0 (0-13) 0 (0-23) / 0 (0-25)
> 5 cm side-to-side diff. b
0 21 (7)
Ankle dorsiflexion with extended knee(°)
Left foot a/ Right foot
a
39 (30-53) / 40 (32-51) 39 (23-54) / 40 (23-58)
> 5° side-to-side diff. b
2 (8) 32 (10)
Ankle dorsiflexion with flexed knee (°)
Left foot a/ Right foot
a
45 (36-56) / 45 (36-57) 46 (29-62) / 46 (25-62)
> 5° side-to-side diff. b
1 (4) 26 (8)
a Median and range
b Number and percentage
Table 11. Anthropometric data. Group differences were analysis with Chi 2- test and
the Student´s t test. No significant differences were shown in anyone of the variables
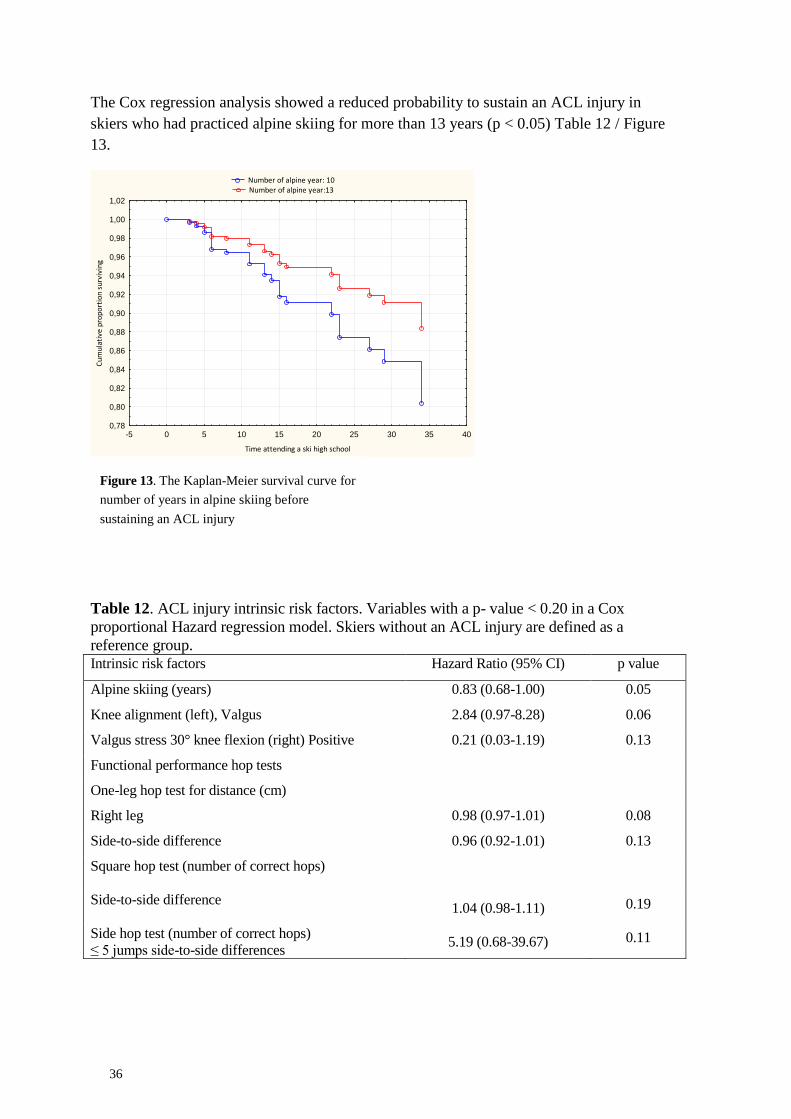
36
The Cox regression analysis showed a reduced probability to sustain an ACL injury in
skiers who had practiced alpine skiing for more than 13 years (p < 0.05) Table 12 / Figure
13.
Number of alpine year: 10 Number of alpine year:13
-5 0 5 10 15 20 25 30 35 40
Time attending a ski high school
0,78
0,80
0,82
0,84
0,86
0,88
0,90
0,92
0,94
0,96
0,98
1,00
1,02
Cu
mu
lati
ve p
rop
ort
ion
su
rviv
ing
Table 12. ACL injury intrinsic risk factors. Variables with a p- value < 0.20 in a Cox
proportional Hazard regression model. Skiers without an ACL injury are defined as a
reference group. Intrinsic risk factors Hazard Ratio (95% CI) p value
Alpine skiing (years) 0.83 (0.68-1.00) 0.05
Knee alignment (left), Valgus 2.84 (0.97-8.28) 0.06
Valgus stress 30° knee flexion (right) Positive 0.21 (0.03-1.19) 0.13
Functional performance hop tests
One-leg hop test for distance (cm)
Right leg 0.98 (0.97-1.01) 0.08
Side-to-side difference 0.96 (0.92-1.01) 0.13
Square hop test (number of correct hops)
Side-to-side difference
1.04 (0.98-1.11) 0.19
Side hop test (number of correct hops)
≤ 5 jumps side-to-side differences 5.19 (0.68-39.67) 0.11
Figure 13. The Kaplan-Meier survival curve for
number of years in alpine skiing before
sustaining an ACL injury

37
5.2.2 ACL injury - Familiar history as a risk factor
Sixty-five out of 418 skiers, who answered a question about familiar history of ACL injuries,
had suffered at least one ACL injury. Among their parents, 51 fathers and 35 mothers had
sustained an ACL injury. In ACL injured skiers there was a significantly higher proportion of
parents that have sustained an ACL injury when compared to skiers without an ACL injury
(p= 0.04).
The results showed an OR of 1.95 to suffer an ACL injury if you have a parent who has had
an ACL injury compared to if none of the skier´s parents have had an ACL injury.
There was no significant difference between male and female skiers about their familial
relationship.
5.2.3 ACL injury - Previous injury as a risk factor
During the study period 52 ACL injuries occurred. Out of these, 23 skiers reported that they
have had an earlier injury in the same knee. A total rupture of the ACL was the most common
previous injury (n=12) followed by other ligament injuries located to the knee joint (n=6).
Three skiers had an earlier injury in the meniscus, one had a bone bruise, and one suffered
from patellar tendinopathy.
5.2.4 ACL injury - Extrinsic risk factors
A total of 52 ACL injuries occurred between September 2006 and May 2013. Fifty ACL
injuries occurred during alpine skiing and two during indoor training. Twenty ACL injuries
(40%) occurred during the skier´s third year at a ski high school and 15 (20%) during their
second year (Figure 14). The majority of the ACL injuries occurred in March followed by
November and December (Figure 15).
Thirty-two out of the 52 ACL injuries (62%) occurred during training. Twenty-six ACL
injuries (52%) occurred in giant slalom, 12 (24%) in slalom and nine (18%) in speed
disciplines. Eighty-three percent of the ACL injuries occurred in prepared slopes.
The snow conditions were aggressive when 25 skiers (50%) tore their ACL and icy when
eight skiers (16%) tore their ACL, loose when seven skiers (13%) tore their ACL and wet
First year
Second Year
Third year
Forth year
02468
101214
Jan
uar
y
Feb
ruar
y
Mar
ch
Ap
ril
May
Sep
tem
be
r
Oct
ob
er
No
vem
be
r
De
cem
ber
Figure 14. Distribution of ACL injuries each
year at a ski high school
Figure 15. Monthly distribution of the
occurrence of ACL injuries
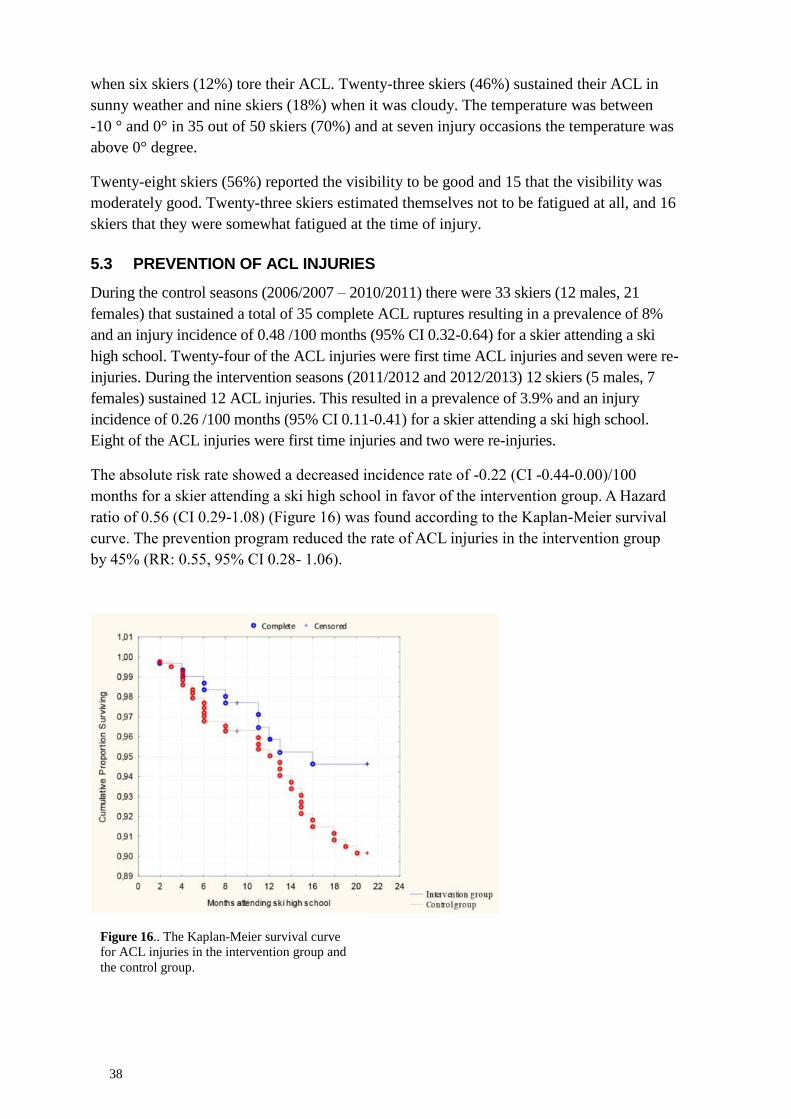
38
when six skiers (12%) tore their ACL. Twenty-three skiers (46%) sustained their ACL in
sunny weather and nine skiers (18%) when it was cloudy. The temperature was between
-10 ° and 0° in 35 out of 50 skiers (70%) and at seven injury occasions the temperature was
above 0° degree.
Twenty-eight skiers (56%) reported the visibility to be good and 15 that the visibility was
moderately good. Twenty-three skiers estimated themselves not to be fatigued at all, and 16
skiers that they were somewhat fatigued at the time of injury.
5.3 PREVENTION OF ACL INJURIES
During the control seasons (2006/2007 – 2010/2011) there were 33 skiers (12 males, 21
females) that sustained a total of 35 complete ACL ruptures resulting in a prevalence of 8%
and an injury incidence of 0.48 /100 months (95% CI 0.32-0.64) for a skier attending a ski
high school. Twenty-four of the ACL injuries were first time ACL injuries and seven were re-
injuries. During the intervention seasons (2011/2012 and 2012/2013) 12 skiers (5 males, 7
females) sustained 12 ACL injuries. This resulted in a prevalence of 3.9% and an injury
incidence of 0.26 /100 months (95% CI 0.11-0.41) for a skier attending a ski high school.
Eight of the ACL injuries were first time injuries and two were re-injuries.
The absolute risk rate showed a decreased incidence rate of -0.22 (CI -0.44-0.00)/100
months for a skier attending a ski high school in favor of the intervention group. A Hazard
ratio of 0.56 (CI 0.29-1.08) (Figure 16) was found according to the Kaplan-Meier survival
curve. The prevention program reduced the rate of ACL injuries in the intervention group
by 45% (RR: 0.55, 95% CI 0.28- 1.06).
Figure 16.. The Kaplan-Meier survival curve
for ACL injuries in the intervention group and
the control group.

39
Compliance with the prevention program
The alpine skiers have regularly watched the video 1-10 times.
Ninety-four skiers (42%) answered the questionnaire about their compliance.
Three out of these 94 skiers injured their ACL during the intervention period.
Question: How many times have you watched the video?
75% answered "1-5 times".
Question: How much of your training has been focused on equilaterality?
62% answered “it is a part of each physical training occasion” and 20% answered "never".
Question: Have you used the suggested exercises from the video to find out whether you can
perform equally well with the left as the right leg?
41% answered "yes 1-10 times/month" and 36% answered "never".
40
41
DISCUSSION 6
The overall aim of this thesis was to try to reduce ACL injuries in competitive alpine skiers
by a specific prevention program based on van Mechelen´s "Sequence of Prevention".130
All studies involve alpine ski students at the Swedish ski high schools between August
2006 and May 2013.
The first investigation is a five year prospective cohort study presenting the injury profile in
terms of injury incidence, injury location, type of injury as well as injury severity among
ski high school students. The aim in the second investigation was to study whether there
was any relationship between the prevalence of ACL injuries in competitive alpine ski
students and ACL injuries in their parents. In the third investigation we tried to identify
potential intrinsic and extrinsic risk factors for ACL injuries in competitive alpine ski
students. Finally, in the fourth investigation a specific prevention program was
implemented in order to try to reduce the incidence of ACL injuries in adolescent
competitive alpine skiers.
Competitive alpine skiing is one of our most complex sports, depending on the combination
of great physical demands and ever-changing external conditions.
6.1 INJURY PROFILE
The result from the injury profile showed that close to 50% of the skiers attending a
Swedish ski high school sustained at least one injury during their study period at the
schools. This is alarming because almost all Swedish competitive alpine skiers in this age
group have studied at a Swedish ski high school. The highest number of severe injuries in
both genders was found in the knee joint and most of these were a ligament injury which is in
accordance with earlier publications on alpine skiing at competitive level. 14, 15, 24, 31
No
gender differences were found regarding the injury profile, which is in contrast to the
publication from FIS ISS system. 14, 31
To our knowledge only a few studies on competitive alpine skiing have been published, 14, 15,
24, 31 which makes comparisons in terms of competitive injury profile difficult. The study
design and the injury definition therefore differ between the present investigation and studies
by other authors. In the present study all injuries that occurred during both training and
competition, which made it possible for the skier to fully participate in skiing or physical
training, were recorded including training off-snow over the entire year. In the studies by
Bere et al. 14
, Bergstrøm et al. 15
, Ekeland et al. 24
and Flørenes et al. 31
, injury recording was
performed during skiing and solely for a part of the year or during a single-event and the
injury was defined as an injury that required the skiers to be transported or treated by a
medical team. One reason for the study design of the present investigation was to find a total
picture of the injury profile in young elite alpine skiers. Alpine skiing on elite level is
complex requiring a variety of physical demands. This means that not only injuries during
skiing but also during physical training were of great importance. A further reason was due to
that a previous injury might be a risk factor for a new injury. 44, 77
About two thirds of the
injuries in the present investigation were joint and ligament injuries. These results are in
42
agreement with the literature when it comes to both recreational and competitive skiers. 14, 31,
64, 107, 118
6.2 ACL INJURIES
In this study population the prevalence of ACL injury was 15,3%, which is in accordance
with the epidemiological study from one ski high school in Austria 101
but lower than what
Pujol et al.100
reported from a French cohort study on competitive alpine skiers. The literature
is inconsistent when it comes to gender differences regarding the incidence of ACL injury in
competitive alpine skiers. Pujol et al. 100
and Bere et al. 14
did not find any gender differences,
while Raschner et al. 101
and Stevenson et al. 120
reported a twofold increased risk for females
compared with males to sustain an ACL injury, which is similar to the findings of the present
study. A reason for these variations in the literature might depend on differences in terms of
the study populations used. Both Bere et al. 14
, Pujol et al. 100
and Stevenson et al. 120
studied
adult alpine skiers, while Raschner et al. 101
studied alpine skiers aged between 14 and 19
years. Several studies showed similar results that ACL injuries occur in a younger age in
female athletes than in their male counterparts.2, 85, 128
An important finding was a significantly higher risk for an elite alpine skier to sustain an
ACL injury in the left knee compared to the right knee, which is in concert with Stevenson et
al. 120
and inconsistent with Pujol et al. 100
The requirement for an alpine skier is to perform ski turns equally well to the left as to the
right. This means that the skier needs the same physical requirements for the left and right
half of the body. A possible explanation for the finding in the present study can of course be
that the skiers really had a side-to-side difference and/or a dominant leg, which may influence
the risk of getting injured. Ford et al. 34
reported a greater difference in the side-to-side knee
valgus motion on the dominant side in uninjured females, but not in uninjured males. Leg
dominance has been discussed as a potential risk factor for sustaining an ACL injury. 19, 73, 82,
106 In recreational skiers Ruedl et al.
106 reported a twofold risk to injure the dominant knee,
while other authors did not find the dominant knee to be a risk factor.19, 73, 82
However,
Negrete et al. 82
and Brophy et al. 19
found a trend that females had a higher incidence of
injuries to their left knee, which was not found in males.
6.2.1 ACL injuries - Intrinsic risk factors in alpine skiing
Most injuries occurred in the left knee, and it seems like the side-to-side difference when
performing the functional tests may play a role of importance.
Furthermore, those who reported a higher number of active years in alpine skiing showed a
reduced risk of sustaining an ACL injury. A possible explanation could be that the skiers had
a longer period of experiences and therefor more prepared for the performance.
In the present investigation an increased ACL injury risk was found in skiers who performed
shorter jumps than those who performed longer ones in the one leg hop test for distance. This
hop test is suggested to measure explosive muscle strength, reported to be a characteristic
factor of demands in alpine skiing. 57
Moreover, when performing the one leg hop test for
distance a side-to-side difference of 10 centimeter was indicated to be a predictor for ACL
injury in the present study. Gustavsson et al. 41
concluded that the one leg hop test for
43
distance can discriminate between the injured and uninjured leg in patients with ACL injury.
Furthermore, Haitzet al. 45
studied normal values for the one leg hop test for distance as well
as for the square hop test, and they did not find a side-to-side leg difference. In view of the
published normative data the choice of cut off in the present study, 10 cm of side difference is
not too small in order to determine a real side difference.
The side hop test alone and the square hop test alone were not found to be significant
predictors of ACL injury. However, unequal performance when comparing the left and right
side regarding the hop tests seems to be predictive for ACL injury in this group of skiers.
These tests require a more complex movement pattern represented by as well endurance
muscle strength as neuromuscular/postural control. 59, 89
In these two hop tests the number of
correct jumps is counted irrespective of the quality of the performance of the tests. According
to Hewett et al. 51
the knee angle at landing after a jump is important and increased hip
adduction and knee valgus have been identified as risk factors for sustaining an ACL injury.
The results of the present study indicate that skiers with an increased knee valgus alignment
were somewhat more prone to injury than those with a normal knee alignment. When
analyzing the performance of the hop tests with respect to alignment and to side-to-side
differences valuable information might be found and lead to possibilities for predicting injury
risk. The hop tests used in the present study indicated a side-to-side difference to be a
predictor for ACL injury. Hewett et al. 48
highlighted the importance of taking the side-to-
side difference of the lower extremity into account when it comes to imbalance of
neuromuscular control, muscle strength and muscle flexibility. This may probably be of
importance in an equilateral sport like alpine skiing, where the same physical demands are
put on both legs. Both decreased 18
and increased 134
muscle flexibility have been discussed
as injury risk factors. However, to the best of our knowledge there are no reported normal
values of muscle flexibility. In contrast to an increased valgus alignment a positive valgus
stress test seems to decrease the risk for sustaining an ACL injury. An explanation could be
that a clinical test differs from a functional performance test. It could be hypothesized that
tests for neuromuscular control are more important from a functional point of view than a
clinical stability test of the knee joint. By analyzing the hop tests with respect to alignment
this might give us an indication of injury risk. Another reason could be that a positive valgus
stress test means that the knee is lax in medio-lateral direction and could thereby help the
skier to perform an increased range of motion before an injury occurs. However, a higher
percent of the ACL injured skiers than those without ACL injury presented with a side-to-
side difference in all three functional performance tests.
The present study showed that an alpine ski student at a ski high school is almost twice more
likely to sustain an ACL injury if he (or she) has a parent with an ACL injury when compared
to ski students without a family history of ACL injury. This is in accordance with earlier
publications. 33, 46, 50, 78
This is the first study including a homogenous group, recruited as a
cohort from the same sport, This is in contrast to other studies that have included different
sports. 33, 46
50, 78
A study by Anderson et al. 4 is the only study where no relationship was
found between family history and ACL injury. However, a problem when comparing these
studies is that the definition of the family member is unclear. Harner et al. 46
included family
members, while Hewett et al. 50
found a familiar risk when they studied sisters in one family.
Myer et al. 78
used the definition of first degree relative but did not define what they mean by
44
that, while Flynn et al. 33
define the first degree relative as someone whom they shared 50%
of their genetic make-up with.
A series of publications 96-99
relating genetic factors have shown that genetic factors
predispose subjects to an ACL injury, but one of these studies 98
on female soccer players did
not show any generalization to males or other populations. The results of the present study
showed a higher tendency to suffer an ACL injury if the skier has a mother who has had an
ACL injury than if he/she has a father with a previous ACL injury. However, this result was
not statistically significant, which may depend on too few cases.
The cohort, adolescent competitive alpine skiers, belongs to a group of athletes that are
exposed to high risk of ACL injuries. The data collection in the present study was performed
through a questionnaire, and is in agreement with methods used in earlier studies. 33, 46
When it comes to injury occurrence the impact of heredity and environmental factors is an
ongoing discussion without a definitive answer. However, it is important to take every
possible opportunity to identify risk factors for suffering an ACL injury in competitive alpine
skiers. Knowing that a skier with a family history of ACL injury, defined in this study as
having a parent that has sustained an ACL injury, means that he/she is twice as likely to
suffer a knee injury. However, this information is not easy to communicate to their children
and may not have any impact on their behavior, as it would be unethical not to allow
children/adolescent to ski because he/she has a parent who has had an ACL injury. On the
other hand it would be unethical not to recognize this knowledge. The first step may be to ask
questions about familial relationships regarding ACL injuries in order to identify the
adolescents at increased injury risk. It is suggested that individuals with a possible
predisposition for an ACL injury should be especially careful and observe safety precautions
of external risk factors for not exposing themselves to unnecessary risk situations. From a
clinical point of view a further suggestion could be to introduce and highlight preventive
strategies for the risk to sustain a severe knee injury.
In contrast to earlier studies on ACL injury risk factors 44, 65, 92
previous lower extremity
injuries were not found to be a significant risk factor in the present investigation. However, in
the present study ski students with an ACL injury prior to the start of the study were excluded
leaving only other previous injuries to the lower extremities than ACL injury as potential risk
factors. When including the skiers with an ACL injury, lower extremity injuries were found
to be a significant risk factor consistent with the literature (unpublished data). From the injury
profile we found no differences, regarding time to the first injury between those skiers that
had an ongoing injury and those that were uninjured at the start of the study. When the skiers,
which sustained one injury, two, three or four injuries were divided it was found that the
sooner the first injury occurred, the risk of sustaining another injury increased. It is likely,
although not evidence based, that this finding underlines the importance of a proper
rehabilitation and to be fully recovered before returning to skiing after an injury.
6.2.2 ACL injuries - Extrinsic risk factors in alpine skiing
In only a few studies evaluation of extrinsic risk factors in competitive alpine skiing has been
performed. From an interview study including 61 expert stakeholders Spörri et al. 115
reported
25 key injury risk factors. Ski equipment (boot, binding, plate) was ranked as number one and
45
physical aspects were ranked as number four and suggested to be more investigated.
Furthermore, the experts believed that the icy conditions would be safer than aggressive snow
conditions, which is consistent with the present study as well as with Bere et al. 13
An
interesting finding was that most ACL injuries occurred during the skiers´ second and third
study year. A reason for this could be stress related, because most of the skiers who have
reached the highest level in alpine skiing also have been successful as juniors. 109
In the present investigation the majority of the ACL injuries occurred during training. This
may be due to that the slopes were not as well prepared as they usually are during
competition. A larger effort to achieve a safe course is likely to be an injury prevention factor.
The technical disciplines giant slalom and slalom account for 38 out of the 52 ACL injuries.
This is in accordance with Gilgien et al. 39
but in contrast to earlier studies 14, 31
, where
downhill race accounted for the highest number of injuries. In the present study no
calculations of ACL injuries between the different ski disciplines were carried out, which
may explain the contradictory results. However, it is assumed that the volumes of training
and competition are similar between the different Swedish ski high schools and the different
disciplines. Another possible explanation may be change of rules. During this study period
only small changes of rules have occurred and this therefore probably does not influence the
occurrence of injury in the different disciplines.
6.3 PREVENTION OF ACL INJURIES
The principal finding in study IV was that a prevention program reduced the overall rate of
ACL injuries by 45% in alpine ski students attending a Swedish ski high school.
To the best of our knowledge the present investigation is the first one in adolescent alpine
skiers at competitive level. Out of previous studies evaluating ACL injury prevention only
one studied alpine skiers, 27
but in recreational skiers. Ettlinger et al. 27
reported a decreased
ACL injury rate as a result of a special educational program in order to avoid ACL injury risk
situations, like how to fall when off balance and how to stop after a fall. In accordance with
Ettlinger et al. 27
the authors of the present study have tried to teach both the ski coaches and
the skiers to be aware of possible ACL injury risk situations. Awareness of certain risk
situations may help to reduce the skier´s technical mistakes and thereby preventing an ACL
injury. 13
The difference between recreational skiers and competitive skiers is due to that a recreational
skier can choose his/her own course, while a competitive skier is skiing in an already
prepared course. Few studies on injury prevention in alpine skiing exist and most of them
include recreational skiers and are studies on the use of helmet. 9, 42, 43, 70, 76, 121
Alpine skiing is an equilateral sport meaning that the same physical demands are put on both
legs. Unpublished data have shown that ACL injured alpine skiers had an increased side-to-
side difference when performing the one leg hop test for distance compared to uninjured
skiers. The side-to-side difference may at least to some extent explain why the skiers´ left
knee was more often injured than their right knee. A recent publication about normative data
when performing hop tests showed various results in terms of the best leg (left or right) for
hop performance. 53
When it comes to the one leg counter movement jump, hop performance
of the dominant leg was superior to the non-dominant leg.53
Contrary, in the one leg stability
46
test the performance of the non-dominant leg was superior to that of the dominant leg. 53
Alpine skiing is a multifactorial sport including a number of different physiological demands
on the skier. 57
Therefore, the goal of the prevention program in the present investigation was
to perform different types of exercises, indoors as well as outdoors on snow, with focus on
how to perform equally well on the left and right leg. In female athletes it has been reported
that those with a side-to-side asymmetry in terms of muscle strength are at a greater risk of
injury than athletes without this asymmetry. 51
Whether this goes for male athletes, as well is,
however, not known. Moreover, Hewett et al. 48
have pointed out the importance of a good
neuromuscular balance between the quadriceps and hamstring muscles, the dominant and
non-dominant leg and a good postural control in order to prevent ACL injuries. These aspects
are probably of potential interest especially in an equilateral sport like alpine skiing. Likewise
found Raschner at al.101
pore core stability to be a critical factor for ACL injury in
competitive skiers attending a boarding school.
The somewhat sparse compliance to the suggested exercises may not explain the reduced
number of ACL injuries in the intervention group. An explanation of the low compliance
among the skiers might be that they did not understand that neuromuscular exercises to reach
the same performance of both legs were suggested in order to prevent ACL injuries. Finch et
al. 30
concluded that a prevention program must be carried out regularly and be integrated
with the normal sport specific training. This is what has been taken into account in the present
investigation. Unfortunately, the sample of the study group was somewhat small in order to
do group analyzes of high compliance and low compliance, which could be of interest in
future studies. This means that other factors might have been more important. From a
psychological point of view the close contact between the principal test leader and the
coaches and their alpine skiers throughout the entire study period might have played a more
prominent role.
Sport performance is synonymous with success in the sport. The optimal prevention program
should be designed not only to prevent injury, but also to increase performance. Combined
performance and prevention training could be instituted with a higher potential for coach and
athlete adherence. Moreover, it should be kept in mind that a sports-related injury may have
several causes, and all injuries can not be prevented. The However, it is likely to believe that
the use of sports injury prevention strategies may reduce the number of injuries and/or injury
severity.
6.4 METHODOLOGICAL CONSIDERATIONS
Despite the large prospective cohort design of the present thesis, there are a few limitations to
take into account while interpreting our results.
Time of exposure is an overall methodological consideration. Most studies report time of
exposure in hours during practice and game or competition.36
In alpine skiing the number of
runs also has been suggested.31
Since the slopes vary in length and a run may vary in time the
use of runs as time of exposure might be misleading. In the present thesis the number of
months that a skier attended a ski high school was chosen to represent time of exposure. The
reason for this choice was that all schools have approximately the same schedule with respect
to practice, competition and ski camps.

47
Study I: A study limitation is that injury location and not the specific injury diagnosis, except
for ACL injury, was reported. Mild injuries that did not need to be treated by a physician
could thus not be diagnosed. Only ACL injuries were properly diagnosed by sports
orthopedic surgeons.
Study II: The questionnaire used in this study was not tested for reliability and validity,
which is another limitation of the study. A further study limitation is lack of access to the
injury records regarding the ACL injuries of those parents that had had an ACL injury.
Moreover, this also led to lack of information about whether the ACL injuries of the skiers´
parents were sports-related or not, and if this was the case, in what sport.
Study III: The clinical tests and functional performance tests were not completed in a
laboratory due to very different geographical locations of the ski high schools. To be able to
include all Swedish ski high schools, the tests had to be performed at each specific ski high
school. The reliability of these tests has been published earlier and to minimize possible
measurement errors the present study used one test leader (MW) with good intratest-retest
reliability. However, the complex interaction between different types of variables makes the
study design of injury risk factors somewhat complicated. Finch 28
as well as Bahr and Holm6
have recommended prospective cohort studies with multivariate statistical approaches in
order to detect injury risk factors within the area of sports medicine. Twenty to 50 injury
cases are suggested for a moderate to strong association, and the choice of the participants
should be representative for the actual sport. Dallinga et al.21
have recommended to use a
prospective design in different age groups, which is similar to the present study including
almost all Swedish competitive alpine skiers in the age group 16-20 years. Despite, the large
sample size of the present investigation the occurrence of ACL injuries did not allow a
multivariate regression analysis or separate analysis of injury risk factors with respect to
gender. Such an analysis might have shown different injury risk factors for male and female
skiers, since physical performance and muscle flexibility may vary between genders.
Study IV: The use of historic controls might be seen as a study limitation. The reason for
using historic controls was twofold, though. The alpine ski students from the different ski
high schools are regularly meeting each other at both national and international ski camps and
ski competitions. Consequently, it was impossible to randomize some of the skiers to one
intervention group and others to a control group without the risk of a crossover effect.
Furthermore, due to the limited number of alpine ski students in Sweden, the use of historic
controls was the way of being able to perform a controlled prevention study of this type.
More alpine ski students and/or a higher number of studied ski seasons could possibly have
been more appropriate. However, it should be pointed out that the present study was based on
a cohort consisting of all Swedish alpine ski students including more than 200 students per
year. In addition, the students are solely studying three or four years at a Swedish ski high
school. Subsequently, to increase the number of skiers and/or ski seasons could result in some
logistical problems.
The present thesis was thus based on four studies with observational design including a
homogenous cohort of adolescent competitive alpine skiers. The main strength of the thesis is
the prospective design with a large sample size, as has been recommended in order to
minimize recall bias. 6, 28, 130
Another strength when using the prospective cohort design is

48
that you are able to calculate the absolute risk. The absolute risk, associated with exposure, is
of greater interest than the relative risk. It provides the researcher with information to make it
possible to evaluate the overall risk of being injured at different levels and across sports by
using the absolute injury rate.

49
CONCLUSION 7
The injury incidence rate in competitive alpine skiing was found to be 1.7
injuries/1000 skiing hours or 3.11 injuries/100 months´ attending a ski high school.
No gender difference in terms of injury incidence was shown.
Nearly 50% of alpine ski students sustained at least one injury during their study
years at a Swedish ski high school. The highest number of injuries was located in
the knee joint for both male and female skiers, and ligament injuries were the most
common ones.
Almost half of the injuries were considered to be severe, while most other injuries
were classified as moderate.
An alpine ski student is almost twice more likely to sustain an ACL injury
if he (or she) has a parent that has had an ACL injury when compared to
an alpine ski student without a family history of ACL injury.
One third of the knee injuries were represented by ACL injuries. Female skiers
showed a higher risk to sustain an ACL injury compared to male skiers. Two thirds
of the ACL injuries occurred in the left knee.
Of the studied potential risk factors, no one was identified as an ACL injury risk
factor. A side-to-side difference of functional performance hop tests was found in
those skiers that sustained an ACL injury.
Skiers with a higher number of active years in alpine skiing had a reduced risk of
sustaining an ACL injury.
The majority of the ACL injuries occurred when the skiers´ studied their third year
at a ski high school, and most injuries occurred in March. More than half of the
injuries occurred during training and most often in the technical disciplines. The
snow conditions were aggressive and icy in two thirds of the injury occasions. The
weather was sunny in almost half of the injury occasions.
The prevention program showed a 45% reduction of the ACL injury incidence rate
during the intervention period in comparison with the control period.

51
FUTURE RESEARCH 8
Future studies on competitive alpine skiing are warranted. A number of publications
regarding recreational skiers exist, while there is a lack of studies on competitive alpine
skiers.
The results from the present thesis revealed a large number of injuries in adolescent
competitive alpine skiers, especially ACL injuries. This indicates the need for future research
within this field.
More advanced laboratory evaluation instruments could improve identification of alpine
skiers at risk for an ACL injury while skiing. Competitive alpine skiing puts high demands
on thigh muscle strength. Therefore, adding isokinetic measurements of knee extensors and
knee flexors to physical performance tests might further improve identification of skiers at
risk for ACL injuries. Furthermore, the counter movement jump may be a suitable hop test
since it has been suggested to be associated with sporting results in at least male but not
female competitive alpine skiers. 26
To the best of our knowledge no study about ACL
injury risk factors comparing male and female skiers has been performed. This is a further
subject of potential interest because of gender differences during growth and maturation.
Another area of study within alpine skiing could be to control the skier´s adjustments of
bindings during the season. This has been suggested by Spörri et al. 115
, who found the ski-
binding-plate-boot to be the number one key risk factor for ACL injuries.
Moreover, it would be interesting to add the suggested two further steps in the TRIPP
model by Finch 28
The goal of a possible fifth step in injury prevention would be to study
the context regarding the athletes´ and their coaches´ barriers. Finally, in a sixth step, to
evaluate injury preventive strategies in a larger real context such as implementing the
prevention program to younger skiers. Based on these steps our research group recently has
conducted an interview of alpine ski coaches using a qualitative approach in order to
capture the experiences from the coaches’ perspective. Hopefully, that study may provide
us with information on how to increase the compliance of preventive strategies among
alpine skiers, before implementing the prevention program in a real world context.

53
ACKNOWLEDGEMENTS 9
I have really enjoyed the time to be a PhD student. It has been nearly 20% of my lifetime!
I would like to thank a number of people for having supported me during this fantastic
research process. I would, especially like to thank the following persons without whom this
thesis could never have been performed:
Suzanne Werner, my main supervisor: Thank you, for encouraging me to become a PhD
student and for always believing in me. In addition, thank you for being a marvellous tutor,
you have been the best English teacher I have ever had. You have magic critical eyes!
Thanks, also for all your help and for introducing me to all your research friends. You took
me into the fascinating scientific world!
Marie Alricss on, my co-supervisor: Thanks, for your patience and for accompanying me
when travelling around to the ski high schools, and for your “nothing is impossible”
enthusiasm.
Björn Engström, my co-supervisor: Thanks, for your support by fruitful discussions about
how skiing technique could be related to different orthopedic injuries.
Björn Lison-Almqvist, my mentor: Thanks, for your support and for generously sharing your
expertise of the specific physical demands in alpine skiing, and in combination with the
skiing technique.
Ejnar Eriksson: Thank you, for all superior support and for introducing me to your research
friends. Your enthusiasm, knowledge and life experiences in ACL injuries and alpine skiing
have been a great inspiration!
Marita Harringe, my co-author: Thanks, for sharing your experience and critical view in
research for evidence based medicine, and for sharing thoughts about life challenges. I am
looking forward to our next projects.
Robert J (Bob) Johnson: Thanks, for your mentorship and contribution with your knowledge
about ACL injury prevention in alpine skiing, and for understanding my “Swenglish”.
Sara Anderson: Thanks, for all support from the start to the end of this project! Thanks, for
all valuable discussions and tangible help with developing the prevention program, both in
Swedish and English.
All alpine ski students and coaches at the Swedish ski high schools whom I have met during
the project. Thanks, for all fruitful and constructive discussions during these years, and for
generously sharing your experiences with me.
Gunilla Bokvist, Marie-Louise Broomé, Birgitta Nordahl, Annelie Norlén, Louise Levin,
Sandra Reed, Maria Sjöberg and Cecilia Ålander: Thanks, for taking part in this alpine
project in different ways. Your collaboration with me has been a real pleasure!
Magnus Forssblad, head of Capio Artro Clinic: Thanks a lot, for giving me access to be a
part of the Artro Clinic during these years.
54
All former and present colleagues at Capio Artro Clinic: Thanks, for all stimulated
“meetings” covering small clinical questions to deeper fruitful discussions. I will miss these
meetings!
Former and present members of the research group at the Stockholm Sports Trauma Research
Center, especially Anna Eliason, Kerstin Sunding and Ulrika Tranaeus: Thanks, for many
fruitful discussions about “how to be a PhD student”, and all good advice and stimulating
discussions about research questions.
Lina Johansson: Thanks, for your inspiration and energy to be a part of the next alpine
project.
Henrik Gustafsson: Thanks, for fruitful cooperation and interesting discussions contributing
with deep knowledge in the field of sports psychology.
To all my colleagues at Hela Kroppen Fysioterapi AB: Thanks, a lot for all appreciation from
the beginning of my PhD work, and during the whole research trip. Now, we will take a
further step!
Malin Åman, my colleague and really good friend, throughout the years: Thanks, for all
fruitful discussions about science and for sharing thoughts about everything in life.
Åsa Svedmark: Thanks, for always being there!
Elisabet Berg, Thanks, for great statistical help during the years and for your patience with
me!
Gunnar Edman, Thanks, for giving me reasonable statistical advice.
Swedish Ski Association, Education: Thanks, for constructive discussions.
Kjell Ruder: Thanks, for all support, especially all your help when recording the video on
ACL injury prevention.
All skiing friends, “skiing parents” and skiing coaches around Sweden: Thanks, for all
constructive feedback and grateful stimulating support during this project.
All my wonderful friends and colleagues outside work: Thanks, for sincere interest in my
project, and for providing opportunities to talk about everything but research.
My sisters and their families: Thanks, for always believing in me and supporting me
whenever needed.
Family in law: Thanks, for all your support and interest in my PhD process.
Last, but certainly not least: I am very thankful to my beloved husband, Johan and our lovely
sons Carl, Adam and David for always having supported and encouraged me go through this
journey, to become a PhD….especially during the last months. I could never have done this
without you! You are the best ever!
55
Thanks, to the Swedish National Centre for Research in Sports and to the Stockholm County
Council for economic support that made this PhD thesis possible.
The work of this thesis was also supported by the Swedish Winter Sport Research Centre,
Sophiahemmets Foundation and the Swedish Association of Physiotherapists.

57
REFERENCES 10
1. Serious knee injury prevention. http://youtu.be/wtYxMJ_ij1g.
2. Swedish ACL register- Annual Report www.aclregister.nu. Accessed 20140420,
2014.
3. Alricsson M WS. Reliability tests of joint motion and muscle flexibility of the hip.
Nordisk Fysioterapi. 2002;6:119- 124.
4. Anderson AF, Lipscomb AB, Liudahl KJ, Addlestone RB. Analysis of the
intercondylar notch by computed tomography. Am J Sports Med. 1987;15(6):547-552.
5. Ardern CL, Taylor NF, Feller JA, Webster KE. Return-to-sport outcomes at 2 to 7
years after anterior cruciate ligament reconstruction surgery. Am J Sports Med.
2012;40(1):41-48.
6. Bahr R, Holme I. Risk factors for sports injuries--a methodological approach. Br J
Sports Med. 2003;37(5):384-392.
7. Bahr R, Krosshaug T. Understanding injury mechanisms: a key component of
preventing injuries in sport. Br J Sports Med. 2005;39(6):324-329.
8. Barenius B, Ponzer S, Shalabi A, Bujak R, Norlen L, Eriksson K. Increased risk of
osteoarthritis after anterior cruciate ligament reconstruction: a 14-year follow-up
study of a randomized controlled trial. Am J Sports Med. 2014;42(5):1049-1057.
9. Baschera D, Hasler RM, Taugwalder D, Exadaktylos A, Raabe A. Association
between Head Injury and Helmet Use in Alpine Skiers: Cohort Study from a Swiss
Level I Trauma Center. J Neurotrauma. 2015;32(8):557-562.
10. Beattie P, Isaacson K, Riddle DL, Rothstein JM. Validity of derived measurements of
leg-length differences obtained by use of a tape measure. Phys Ther. 1990;70(3):150-
157.
11. Beighton P, Solomon L, Soskolne CL. Articular mobility in an African population.
Ann Rheum Dis. 1973;32(5):413-418.
12. Bere T, Florenes TW, Krosshaug T, et al. Mechanisms of anterior cruciate ligament
injury in World Cup alpine skiing: a systematic video analysis of 20 cases. Am J
Sports Med. 2011;39(7):1421-1429.
13. Bere T, Florenes TW, Krosshaug T, Nordsletten L, Bahr R. Events leading to anterior
cruciate ligament injury in World Cup Alpine Skiing: a systematic video analysis of
20 cases. Br J Sports Med. 2011;45(16):1294-1302.
14. Bere T, Florenes TW, Nordsletten L, Bahr R. Sex differences in the risk of injury in
World Cup alpine skiers: a 6-year cohort study. Br J Sports Med. 2014;48(1):36-40.
15. Bergstrom KA, Bergstrom A, Ekeland A. Organisation of safety measures in an
Alpine World Junior Championship. Br J Sports Med. 2001;35(5):321-324.
16. Bergstrom KA, Ekeland A. Effect of trail design and grooming on the incidence of
injuries at alpine ski areas. Br J Sports Med. 2004;38(3):264-268.
17. Bland JM, Altman DG. Measurement error. BMJ. 1996;312(7047):1654.
58
18. Boden BP, Dean GS, Feagin JA, Jr., Garrett WE, Jr. Mechanisms of anterior cruciate
ligament injury. Orthopedics. 2000;23(6):573-578.
19. Brophy R, Silvers HJ, Gonzales T, Mandelbaum BR. Gender influences: the role of
leg dominance in ACL injury among soccer players. Br J Sports Med.
2010;44(10):694-697.
20. Caraffa A, Cerulli G, Projetti M, Aisa G, Rizzo A. Prevention of anterior cruciate
ligament injuries in soccer. A prospective controlled study of proprioceptive training.
Knee Surg Sports Traumatol Arthrosc. 1996;4(1):19-21.
21. Dallinga JM, Benjaminse A, Lemmink KA. Which screening tools can predict injury
to the lower extremities in team sports?: a systematic review. Sports Med.
2012;42(9):791-815.
22. Daniel DM, Malcom LL, Losse G, Stone ML, Sachs R, Burks R. Instrumented
measurement of anterior laxity of the knee. J Bone Joint Surg Am. 1985;67(5):720-
726.
23. Delince P, Ghafil D. Anterior cruciate ligament tears: conservative or surgical
treatment? A critical review of the literature. Knee Surg Sports Traumatol Arthrosc.
2012;20(1):48-61.
24. Ekeland A, Dimmen S, Lystad H, Aune AK. Completion rates and injuries in alpine
races during the 1994 Olympic Winter Games. Scand J Med Sci Sports.
1996;6(5):287-290.
25. Ekstrand J, Wiktorsson M, Oberg B, Gillquist J. Lower extremity goniometric
measurements: a study to determine their reliability. Arch Phys Med Rehabil.
1982;63(4):171-175.
26. Emeterio CA, Gonzalez-Badillo JJ. The physical and anthropometric profiles of
adolescent alpine skiers and their relationship with sporting rank. J Strength Cond
Res. 2010;24(4):1007-1012.
27. Ettlinger CF, Johnson RJ, Shealy JE. A method to help reduce the risk of serious knee
sprains incurred in alpine skiing. Am J Sports Med. 1995;23(5):531-537.
28. Finch C. A new framework for research leading to sports injury prevention. J Sci Med
Sport. 2006;9(1-2):3-9; discussion 10.
29. Finch CF, Ullah S, McIntosh AS. Combining epidemiology and biomechanics in
sports injury prevention research: a new approach for selecting suitable controls.
Sports Med. 2011;41(1):59-72.
30. Finch CF, White P, Twomey D, Ullah S. Implementing an exercise-training
programme to prevent lower-limb injuries: considerations for the development of a
randomised controlled trial intervention delivery plan. Br J Sports Med.
2011;45(10):791-796.
31. Florenes TW, Bere T, Nordsletten L, Heir S, Bahr R. Injuries among male and female
World Cup alpine skiers. Br J Sports Med. 2009;43(13):973-978.
32. Florenes TW, Nordsletten L, Heir S, Bahr R. Recording injuries among World Cup
skiers and snowboarders: a methodological study. Scand J Med Sci Sports.
2011;21(2):196-205.
59
33. Flynn RK, Pedersen CL, Birmingham TB, Kirkley A, Jackowski D, Fowler PJ. The
familial predisposition toward tearing the anterior cruciate ligament: a case control
study. Am J Sports Med. 2005;33(1):23-28.
34. Ford KR, Myer GD, Hewett TE. Valgus knee motion during landing in high school
female and male basketball players. Med Sci Sports Exerc. 2003;35(10):1745-1750.
35. Frobell RB, Roos HP, Roos EM, Roemer FW, Ranstam J, Lohmander LS. Treatment
for acute anterior cruciate ligament tear: five year outcome of randomised trial. BMJ.
2013;346:f232.
36. Fuller CW, Ekstrand J, Junge A, et al. Consensus statement on injury definitions and
data collection procedures in studies of football (soccer) injuries. Scand J Med Sci
Sports. 2006;16(2):83-92.
37. Fuller CW, Molloy MG, Bagate C, et al. Consensus statement on injury definitions
and data collection procedures for studies of injuries in rugby union. Clin J Sport
Med. 2007;17(3):177-181.
38. Gilchrist J, Mandelbaum BR, Melancon H, et al. A randomized controlled trial to
prevent noncontact anterior cruciate ligament injury in female collegiate soccer
players. Am J Sports Med. 2008;36(8):1476-1483.
39. Gilgien M, Crivelli P, Sporri J, Kroll J, Muller E. Characterization of course and
terrain and their effect on skier speed in world cup alpine ski racing. PLoS One.
2015;10(3):e0118119.
40. Griffin LY, Albohm MJ, Arendt EA, et al. Understanding and preventing noncontact
anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, January
2005. Am J Sports Med. 2006;34(9):1512-1532.
41. Gustavsson A, Neeter C, Thomee P, et al. A test battery for evaluating hop
performance in patients with an ACL injury and patients who have undergone ACL
reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006;14(8):778-788.
42. Hagel B, Pless IB, Goulet C, Platt R, Robitaille Y. The effect of helmet use on injury
severity and crash circumstances in skiers and snowboarders. Accid Anal Prev.
2005;37(1):103-108.
43. Hagel BE, Pless IB, Goulet C, Platt RW, Robitaille Y. Effectiveness of helmets in
skiers and snowboarders: case-control and case crossover study. BMJ.
2005;330(7486):281.
44. Hagglund M, Walden M, Ekstrand J. Previous injury as a risk factor for injury in elite
football: a prospective study over two consecutive seasons. Br J Sports Med.
2006;40(9):767-772.
45. Haitz K, Shultz R, Hodgins M, Matheson GO. Test-retest and interrater reliability of
the functional lower extremity evaluation. J Orthop Sports Phys Ther.
2014;44(12):947-954.
46. Harner CD, Paulos LE, Greenwald AE, Rosenberg TD, Cooley VC. Detailed analysis
of patients with bilateral anterior cruciate ligament injuries. Am J Sports Med.
1994;22(1):37-43.
47. Heidt RS, Jr., Sweeterman LM, Carlonas RL, Traub JA, Tekulve FX. Avoidance of
soccer injuries with preseason conditioning. Am J Sports Med. 2000;28(5):659-662.
60
48. Hewett TE, Ford KR, Hoogenboom BJ, Myer GD. Understanding and preventing acl
injuries: current biomechanical and epidemiologic considerations - update 2010. N
Am J Sports Phys Ther. 2010;5(4):234-251.
49. Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular
training on the incidence of knee injury in female athletes. A prospective study. Am J
Sports Med. 1999;27(6):699-706.
50. Hewett TE, Lynch TR, Myer GD, Ford KR, Gwin RC, Heidt RS, Jr. Multiple risk
factors related to familial predisposition to anterior cruciate ligament injury: fraternal
twin sisters with anterior cruciate ligament ruptures. Br J Sports Med.
2010;44(12):848-855.
51. Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular
control and valgus loading of the knee predict anterior cruciate ligament injury risk in
female athletes: a prospective study. Am J Sports Med. 2005;33(4):492-501.
52. Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes.
Decreased impact forces and increased hamstring torques. Am J Sports Med.
1996;24(6):765-773.
53. Hildebrandt C, Muller L, Zisch B, Huber R, Fink C, Raschner C. Functional
assessments for decision-making regarding return to sports following ACL
reconstruction. Part I: development of a new test battery. Knee Surg Sports Traumatol
Arthrosc. 2015.
54. Hintermeister RA, O'Connor DD, Dillman CJ, Suplizio CL, Lange GW, Steadman
JR. Muscle activity in slalom and giant slalom skiing. Med Sci Sports Exerc.
1995;27(3):315-322.
55. Hughston JC, Andrews JR, Cross MJ, Moschi A. Classification of knee ligament
instabilities. Part I. The medial compartment and cruciate ligaments. J Bone Joint
Surg Am. 1976;58(2):159-172.
56. Hunter RE. Skiing injuries. Am J Sports Med. 1999;27(3):381-389.
57. Hydren JR, Volek JS, Maresh CM, Comstock BA, Kraemer WJ. Review of Strength
and Conditioning for Alpine Ski Racing. Strength and Conditioning Journal.
2013;35(1):10-28.
58. InternationalSkiFederation. The Interantional Ski Competition Rules. http://www.fis-
ski.com/mm/Document/documentlibrary/AlpineSkiing/03/29/54/ICR_clean_12082014
_Neutral.pdf. Accessed 20150420, 2014.
59. Itoh H, Kurosaka M, Yoshiya S, Ichihashi N, Mizuno K. Evaluation of functional
deficits determined by four different hop tests in patients with anterior cruciate
ligament deficiency. Knee Surg Sports Traumatol Arthrosc. 1998;6(4):241-245.
60. Jarvinen M, Natri A, Laurila S, Kannus P. Mechanisms of anterior cruciate ligament
ruptures in skiing. Knee Surg Sports Traumatol Arthrosc. 1994;2(4):224-228.
61. Jlrgensen U, Fredensborg T, Haraszuk JP, Crone KL. Reduction of injuries in
downhill skiing by use of an instructional ski-video: a prospective randomised
intervention study. Knee Surg Sports Traumatol Arthrosc. 1998;6(3):194-200.
62. Junge A, Engebretsen L, Alonso JM, et al. Injury surveillance in multi-sport events:
the International Olympic Committee approach. Br J Sports Med. 2008;42(6):413-
421.
61
63. Kiani A, Hellquist E, Ahlqvist K, Gedeborg R, Michaelsson K, Byberg L. Prevention
of soccer-related knee injuries in teenaged girls. Arch Intern Med. 2010;170(1):43-49.
64. Kim S, Endres NK, Johnson RJ, Ettlinger CF, Shealy JE. Snowboarding injuries:
trends over time and comparisons with alpine skiing injuries. Am J Sports Med.
2012;40(4):770-776.
65. Kramer LC, Denegar CR, Buckley WE, Hertel J. Factors associated with anterior
cruciate ligament injury: history in female athletes. J Sports Med Phys Fitness.
2007;47(4):446-454.
66. Krosshaug T, Andersen TE, Olsen OE, Myklebust G, Bahr R. Research approaches to
describe the mechanisms of injuries in sport: limitations and possibilities. Br J Sports
Med. 2005;39(6):330-339.
67. LaBella CR, Huxford MR, Grissom J, Kim KY, Peng J, Christoffel KK. Effect of
neuromuscular warm-up on injuries in female soccer and basketball athletes in urban
public high schools: cluster randomized controlled trial. Arch Pediatr Adolesc Med.
2011;165(11):1033-1040.
68. Levy IM. Formulation and sense of the NAIRS athletic injury surveillance system.
Am J Sports Med. 1988;16 Suppl 1:S132-133.
69. Lysens RJ, de Weerdt W, Nieuwboer A. Factors associated with injury proneness.
Sports Med. 1991;12(5):281-289.
70. Macnab AJ, Smith T, Gagnon FA, Macnab M. Effect of helmet wear on the incidence
of head/face and cervical spine injuries in young skiers and snowboarders. Inj Prev.
2002;8(4):324-327.
71. Magee D. Orthopedic Physical assessment. Philadelphia, USA: W.B.Saunders
Company; 1992.
72. Mandelbaum BR, Silvers HJ, Watanabe DS, et al. Effectiveness of a neuromuscular
and proprioceptive training program in preventing anterior cruciate ligament injuries
in female athletes: 2-year follow-up. Am J Sports Med. 2005;33(7):1003-1010.
73. Matava MJ, Freehill AK, Grutzner S, Shannon W. Limb dominance as a potential
etiologic factor in noncontact anterior cruciate ligament tears. J Knee Surg.
2002;15(1):11-16.
74. McBain K, Shrier I, Shultz R, et al. Prevention of sport injury II: a systematic review
of clinical science research. Br J Sports Med. 2012;46(3):174-179.
75. Meeuwisse WH, Tyreman H, Hagel B, Emery C. A dynamic model of etiology in
sport injury: the recursive nature of risk and causation. Clin J Sport Med.
2007;17(3):215-219.
76. Mueller BA, Cummings P, Rivara FP, Brooks MA, Terasaki RD. Injuries of the head,
face, and neck in relation to ski helmet use. Epidemiology. 2008;19(2):270-276.
77. Murphy DF, Connolly DA, Beynnon BD. Risk factors for lower extremity injury: a
review of the literature. Br J Sports Med. 2003;37(1):13-29.
78. Myer GD, Heidt RS, Waits C, et al. Sex comparison of familial predisposition to
anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc. 2014.
79. Myklebust G, Engebretsen L, Braekken IH, Skjolberg A, Olsen OE, Bahr R.
Prevention of anterior cruciate ligament injuries in female team handball players: a
62
prospective intervention study over three seasons. Clin J Sport Med. 2003;13(2):71-
78.
80. MyndighetenförsamhällsskyddochberedskapStatensfolkhälsoinstitut. Fysisk aktivitet
och skador. www.msb.se/RibData/Filer/pdf/25550.pdf. Accessed 20150420, 2015.
81. Natri A, Beynnon BD, Ettlinger CF, Johnson RJ, Shealy JE. Alpine ski bindings and
injuries. Current findings. Sports Med. 1999;28(1):35-48.
82. Negrete RJ, Schick EA, Cooper JP. Lower-limb dominance as a possible etiologic
factor in noncontact anterior cruciate ligament tears. J Strength Cond Res.
2007;21(1):270-273.
83. Neumayr G, Hoertnagl H, Pfister R, Koller A, Eibl G, Raas E. Physical and
physiological factors associated with success in professional alpine skiing. Int J
Sports Med. 2003;24(8):571-575.
84. Nordenvall R, Bahmanyar S, Adami J, Mattila VM, Fellander-Tsai L. Cruciate
ligament reconstruction and risk of knee osteoarthritis: the association between
cruciate ligament injury and post-traumatic osteoarthritis. a population based
nationwide study in Sweden, 1987-2009. PLoS One. 2014;9(8):e104681.
85. Nordenvall R, Bahmanyar S, Adami J, Stenros C, Wredmark T, Fellander-Tsai L. A
population-based nationwide study of cruciate ligament injury in Sweden, 2001-2009:
incidence, treatment, and sex differences. Am J Sports Med. 2012;40(8):1808-1813.
86. Olsen OE, Myklebust G, Engebretsen L, Holme I, Bahr R. Exercises to prevent lower
limb injuries in youth sports: cluster randomised controlled trial. BMJ.
2005;330(7489):449.
87. Orchard J. Orchard sports injury classification systems. In: Bloomfield J FP, Fitch K.,
ed. Science and medicine in sports. 2nd ed. Blackwell: Carlton; 1995:277-293.
88. Orchard J, Rae K, Brooks J, et al. Revision, uptake and coding issues related to the
open access Orchard Sports Injury Classification System (OSICS) versions 8, 9 and
10.1. Open Access J Sports Med. 2010;1:207-214.
89. Ostenberg A, Roos E, Ekdahl C, Roos H. Isokinetic knee extensor strength and
functional performance in healthy female soccer players. Scand J Med Sci Sports.
1998;8(5 Pt 1):257-264.
90. Owoeye OB, Akinbo SR, Tella BA, Olawale OA. Efficacy of the FIFA 11+ Warm-
Up Programme in Male Youth Football: A Cluster Randomised Controlled Trial. J
Sports Sci Med. 2014;13(2):321-328.
91. Pasanen K, Parkkari J, Pasanen M, et al. Neuromuscular training and the risk of leg
injuries in female floorball players: cluster randomised controlled study. BMJ.
2008;337:a295.
92. Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of contralateral
and ipsilateral anterior cruciate ligament (ACL) injury after primary ACL
reconstruction and return to sport. Clin J Sport Med. 2012;22(2):116-121.
93. Petersen W, Braun C, Bock W, et al. A controlled prospective case control study of a
prevention training program in female team handball players: the German experience.
Arch Orthop Trauma Surg. 2005;125(9):614-621.
63
94. Pfeiffer RP, Shea KG, Roberts D, Grandstrand S, Bond L. Lack of effect of a knee
ligament injury prevention program on the incidence of noncontact anterior cruciate
ligament injury. J Bone Joint Surg Am. 2006;88(8):1769-1774.
95. Pluim BM, Fuller CW, Batt ME, et al. Consensus statement on epidemiological
studies of medical conditions in tennis, April 2009. Clin J Sport Med.
2009;19(6):445-450.
96. Posthumus M, Collins M, van der Merwe L, et al. Matrix metalloproteinase genes on
chromosome 11q22 and the risk of anterior cruciate ligament (ACL) rupture. Scand J
Med Sci Sports. 2012;22(4):523-533.
97. Posthumus M, September AV, Keegan M, et al. Genetic risk factors for anterior
cruciate ligament ruptures: COL1A1 gene variant. Br J Sports Med. 2009;43(5):352-
356.
98. Posthumus M, September AV, O'Cuinneagain D, van der Merwe W, Schwellnus MP,
Collins M. The COL5A1 gene is associated with increased risk of anterior cruciate
ligament ruptures in female participants. Am J Sports Med. 2009;37(11):2234-2240.
99. Posthumus M, September AV, O'Cuinneagain D, van der Merwe W, Schwellnus MP,
Collins M. The association between the COL12A1 gene and anterior cruciate
ligament ruptures. Br J Sports Med. 2010;44(16):1160-1165.
100. Pujol N, Blanchi MP, Chambat P. The incidence of anterior cruciate ligament injuries
among competitive Alpine skiers: a 25-year investigation. Am J Sports Med.
2007;35(7):1070-1074.
101. Raschner C, Platzer HP, Patterson C, Werner I, Huber R, Hildebrandt C. The
relationship between ACL injuries and physical fitness in young competitive ski
racers: a 10-year longitudinal study. Br J Sports Med. 2012;46(15):1065-1071.
102. Renstrom P, Ljungqvist A, Arendt E, et al. Non-contact ACL injuries in female
athletes: an International Olympic Committee current concepts statement. Br J Sports
Med. 2008;42(6):394-412.
103. Ristolainen L, Kettunen JA, Kujala UM, Heinonen A. Sport injuries as the main cause
of sport career termination among Finnish top-level athletes. European Journal of
Sport Science. 2012;12(3):274-282.
104. Rossler R, Donath L, Verhagen E, Junge A, Schweizer T, Faude O. Exercise-based
injury prevention in child and adolescent sport: a systematic review and meta-
analysis. Sports Med. 2014;44(12):1733-1748.
105. Rothman J, K. Epidemiology- An introduction. New York: Oxford; 2002.
106. Ruedl G, Webhofer M, Helle K, et al. Leg dominance is a risk factor for noncontact
anterior cruciate ligament injuries in female recreational skiers. Am J Sports Med.
2012;40(6):1269-1273.
107. Rust DA, Gilmore CJ, Treme G. Injury Patterns at a Large Western United States Ski
Resort With and Without Snowboarders: The Taos Experience. Am J Sports Med.
2013.
108. Sahai H, Khurshid A. Formulae and tables for the determination of sample sizes and
power in clinical trials for testing differences in proportions for the two-sample
design: a review. Stat Med. 1996;15(1):1-21.

64
109. SkiTeamSweden. Kravanlys. 2011,
http://www.skidor.com/ImageVaultFiles/id_96766/cf_104/Kravanalys_110525_Bjo-
rn.PDF.
110. SLAO. Snörapporten. 2014;No. 20150420,
www.//slao.se/Userfiles/Branschrapport_2014_webb_sidor.pdf.
111. Smith HC, Vacek P, Johnson RJ, et al. Risk factors for anterior cruciate ligament
injury: a review of the literature-part 2: hormonal, genetic, cognitive function,
previous injury, and extrinsic risk factors. Sports Health. 2012;4(2):155-161.
112. Smith HC, Vacek P, Johnson RJ, et al. Risk factors for anterior cruciate ligament
injury: a review of the literature - part 1: neuromuscular and anatomic risk. Sports
Health. 2012;4(1):69-78.
113. Soderman K, Werner S, Pietila T, Engstrom B, Alfredson H. Balance board training:
prevention of traumatic injuries of the lower extremities in female soccer players? A
prospective randomized intervention study. Knee Surg Sports Traumatol Arthrosc.
2000;8(6):356-363.
114. Soligard T, Myklebust G, Steffen K, et al. Comprehensive warm-up programme to
prevent injuries in young female footballers: cluster randomised controlled trial. BMJ.
2008;337:a2469.
115. Sporri J, Kroll J, Amesberger G, Blake OM, Muller E. Perceived key injury risk
factors in World Cup alpine ski racing--an explorative qualitative study with expert
stakeholders. Br J Sports Med. 2012;46(15):1059-1064.
116. Steffen K, Emery CA, Romiti M, et al. High adherence to a neuromuscular injury
prevention programme (FIFA 11+) improves functional balance and reduces injury
risk in Canadian youth female football players: a cluster randomised trial. Br J Sports
Med. 2013;47(12):794-802.
117. Steffen K, Myklebust G, Olsen OE, Holme I, Bahr R. Preventing injuries in female
youth football--a cluster-randomized controlled trial. Scand J Med Sci Sports.
2008;18(5):605-614.
118. Stenroos A, Handolin L. Incidence of Recreational Alpine Skiing and Snowboarding
Injuries: six years experience in the largest ski resort in Finland. Scand J Surg. 2014.
119. Stenroos AJ, Handolin LE. Alpine skiing injuries in Finland - a two-year retrospective
study based on a questionnaire among Ski racers. BMC Sports Sci Med Rehabil.
2014;6(1):9.
120. Stevenson H, Webster J, Johnson R, Beynnon B. Gender differences in knee injury
epidemiology among competitive alpine ski racers. Iowa Orthop J. 1998;18:64-66.
121. Sulheim S, Holme I, Ekeland A, Bahr R. Helmet use and risk of head injuries in
alpine skiers and snowboarders. JAMA. 2006;295(8):919-924.
122. Swart E, Redler L, Fabricant PD, Mandelbaum BR, Ahmad CS, Wang YC.
Prevention and screening programs for anterior cruciate ligament injuries in young
athletes: a cost-effectiveness analysis. J Bone Joint Surg Am. 2014;96(9):705-711.
123. Taimela S, Kujala UM, Osterman K. Intrinsic risk factors and athletic injuries. Sports
Med. 1990;9(4):205-215.
65
124. Tegner Y, Lysholm J, Lysholm M, Gillquist J. A performance test to monitor
rehabilitation and evaluate anterior cruciate ligament injuries. Am J Sports Med.
1986;14(2):156-159.
125. Timpka T, Alonso JM, Jacobsson J, et al. Injury and illness definitions and data
collection procedures for use in epidemiological studies in Athletics (track and field):
consensus statement. Br J Sports Med. 2014;48(7):483-490.
126. Walden M, Atroshi I, Magnusson H, Wagner P, Hagglund M. Prevention of acute
knee injuries in adolescent female football players: cluster randomised controlled
trial. BMJ. 2012;344:e3042.
127. Walden M, Hagglund M, Magnusson H, Ekstrand J. Anterior cruciate ligament injury
in elite football: a prospective three-cohort study. Knee Surg Sports Traumatol
Arthrosc. 2011;19(1):11-19.
128. Walden M, Hagglund M, Werner J, Ekstrand J. The epidemiology of anterior cruciate
ligament injury in football (soccer): a review of the literature from a gender-related
perspective. Knee Surg Sports Traumatol Arthrosc. 2011;19(1):3-10.
129. van Mechelen W. The severity of sports injuries. Sports Med. 1997;24(3):176-180.
130. van Mechelen W, Hlobil H, Kemper HC. Incidence, severity, aetiology and
prevention of sports injuries. A review of concepts. Sports Med. 1992;14(2):82-99.
131. Wedderkopp N, Kaltoft M, Lundgaard B, Rosendahl M, Froberg K. Prevention of
injuries in young female players in European team handball. A prospective
intervention study. Scand J Med Sci Sports. 1999;9(1):41-47.
132. Westin M, Alricsson M, Werner S. Injury profile of competitive alpine skiers: a five-
year cohort study. Knee Surg Sports Traumatol Arthrosc. 2012;20(6):1175-1181.
133. Westin M., Alricsson M., Werner S. ACL injured and non- injured top level alpine
skiers - a descriptive comparative study on possible intrinsic and extrinsic risk factors.
Karolinska Institutet: Department of Molecular medicine and Surgery; 2007:Master
project
134. Witvrouw E, Danneels L, Asselman P, D'Have T, Cambier D. Muscle flexibility as a
risk factor for developing muscle injuries in male professional soccer players. A
prospective study. Am J Sports Med. 2003;31(1):41-46.
135. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP.
Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)
statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806-
808.
136. Wright RW, Magnussen RA, Dunn WR, Spindler KP. Ipsilateral graft and
contralateral ACL rupture at five years or more following ACL reconstruction: a
systematic review. J Bone Joint Surg Am. 2011;93(12):1159-1165.
137. Zantop T, Petersen W, Sekiya JK, Musahl V, Fu FH. Anterior cruciate ligament
anatomy and function relating to anatomical reconstruction. Knee Surg Sports
Traumatol Arthrosc. 2006;14(10):982-992.
138. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. Deficits in
neuromuscular control of the trunk predict knee injury risk: a prospective
biomechanical-epidemiologic study. Am J Sports Med. 2007;35(7):1123-1130.

66