Abdominal trauma
30
6/5//2010 MBChB V Lecture Abdominal Abdominal Trauma Trauma Prof. J. A. Adwok Prof. J. A. Adwok MBChB, MMED (Surg.), FICS, MBChB, MMED (Surg.), FICS, FCS(ECSA), FRCS FCS(ECSA), FRCS Dept. of Surgery, U.o.N Dept. of Surgery, U.o.N
-
Upload
avid-listener -
Category
Documents
-
view
70 -
download
5
Transcript of Abdominal trauma

6/5//2010 MBChB V Lecture
Abdominal Abdominal TraumaTraumaProf. J. A. Adwok Prof. J. A. Adwok
MBChB, MMED (Surg.), FICS, MBChB, MMED (Surg.), FICS, FCS(ECSA), FRCSFCS(ECSA), FRCS
Dept. of Surgery, U.o.NDept. of Surgery, U.o.N

Abdominal TraumaAbdominal Trauma• Frequent cause of preventable deathFrequent cause of preventable death• Peritoneal signs often masked by:Peritoneal signs often masked by:
– Pain from associated extra-abdominal Pain from associated extra-abdominal traumatrauma
– Head injuryHead injury– IntoxicantsIntoxicants
• Significant deceleration injury or a Significant deceleration injury or a penetrating torso wound penetrating torso wound

Abdominal RegionsAbdominal Regions
Peritoneal cavity:Peritoneal cavity:–Upper abdomenUpper abdomen
–Lower abdomenLower abdomen
Retroperitoneal spaceRetroperitoneal space PelvisPelvis


Mechanism of Abdominal Mechanism of Abdominal TraumaTrauma
BluntBluntPenetratingPenetrating
Geographical Geographical location and location and demographics demographics affect pattern of affect pattern of injuryinjurySocioeconomic Socioeconomic environment environment influences influences prevalence and prevalence and ratioratio

Muzzle Velocity of GunsMuzzle Velocity of Guns Low velocityLow velocity
<1200ft./Sec.(<366m/sec.)<1200ft./Sec.(<366m/sec.) Hand gunsHand guns
Medium velocityMedium velocity >1200-2000ft./Sec.(366-609m/sec)>1200-2000ft./Sec.(366-609m/sec)
High velocityHigh velocity >2000ft./Sec.(>609m/sec.)>2000ft./Sec.(>609m/sec.) Military, assault and high-power hunting Military, assault and high-power hunting
riflesrifles Usually automatic and semiautomatic Usually automatic and semiautomatic
weaponsweapons

Blunt Trauma•Direct impact•Compression injury•Shearing forces

Blunt Trauma-Blunt Trauma-AssessmentAssessment HistoryHistory Physical examination:Physical examination:
Inspection: Evidence of injuryInspection: Evidence of injury Palpation: GuardingPalpation: Guarding Auscultation: Bowel soundsAuscultation: Bowel sounds Percussion: TendernessPercussion: Tenderness

Blunt Trauma--Blunt Trauma--AssessmentAssessment
Nasogastric tubeNasogastric tubeAspiration minimizationAspiration minimizationUpper GIT bleedingUpper GIT bleeding
Caution : facial injuriesCaution : facial injuries

Blunt Trauma—Pelvic Blunt Trauma—Pelvic AssessmentAssessment Penile:Penile: Scrotum:Scrotum: Vaginal:Vaginal:
Rectal:Rectal:
Gross bloodGross blood HaematomaHaematoma Gross blood, Gross blood,
fracture fragmentsfracture fragments Sphincter tone, Sphincter tone,
prostate position, prostate position, fracture fragments fracture fragments and gross bloodand gross blood

Pelvic--AssessmentPelvic--AssessmentTransurethral CatheterTransurethral Catheter
Rectal/genital exam firstRectal/genital exam first Decompress bladder, monitor urinary Decompress bladder, monitor urinary
outputoutput Diagnostic: haematuriaDiagnostic: haematuria Caution: pelvic fracturesCaution: pelvic fractures Contraindicated: suspected urethral Contraindicated: suspected urethral
injuryinjury

Blunt Trauma--AssessmentBlunt Trauma--Assessment• Positive exam---Positive exam---• Negative exam--Negative exam--
• Negative exam--Negative exam--
Re-evaluate !Re-evaluate !
SignificantSignificant Does not Does not
preclude injurypreclude injury May become May become
positive with timepositive with time

AssessmentAssessmentBlood SamplingBlood Sampling
Group and crossmatchGroup and crossmatch TbcTbc Pregnancy test Pregnancy test AmylaseAmylase Alcohol/drug levelsAlcohol/drug levels

AssessmentAssessmentScreening RadiographsScreening Radiographs
Based on patient Based on patient status/mechanism of status/mechanism of injuryinjury
Free air/extraluminal airFree air/extraluminal airLoss of psoas shadowLoss of psoas shadowAssociated bony injuryAssociated bony injury


Special Diagnostic Special Diagnostic StudiesStudies Done for multiply injured Done for multiply injured
patient i f abdominal exam patient i f abdominal exam is :is :– EquivocalEquivocal– UnreliableUnreliable– ImpracticalImpractical
Do not delay treatment or Do not delay treatment or transporttransport

Diagnostic Peritoneal LavageDiagnostic Peritoneal Lavage
Operative procedureOperative procedure Performed by surgeonPerformed by surgeon Perform early if hypotensivePerform early if hypotensive 98% sensitive for 98% sensitive for
intraperitonealintraperitoneal bleedingbleeding

Computed Tomographic Computed Tomographic ScansScans Stable patients onlyStable patients onlyContrastContrast Include lower thorax and Include lower thorax and
pelvispelvis





Indications for Indications for LaparotomyLaparotomy
Low BP + Abdominal injuryLow BP + Abdominal injury
Extraluminal airExtraluminal air
Injured diaphragmInjured diaphragm
Intraperitoneal injury (+DPL or Intraperitoneal injury (+DPL or +CT)+CT)
Peritoneal signsPeritoneal signs

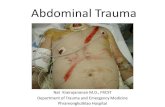
Grade III Injury to Spleen


SummarySummary Two major types of Two major types of abdominal trauma abdominal trauma occur: Penetrating and occur: Penetrating and blunt.blunt.
In either case, early In either case, early evaluation by a surgeon evaluation by a surgeon is essentialis essential

Penetrating traumaPenetrating trauma A surgeon must evaluate all A surgeon must evaluate all
penetrating injuries of the penetrating injuries of the abdomen.abdomen.
Penetrating trauma to flanks, Penetrating trauma to flanks, buttocks, and lower chest may buttocks, and lower chest may produce intra-abdominal injuries produce intra-abdominal injuries as well as should be regarded as well as should be regarded with a high degree of suspicion.with a high degree of suspicion.

Blunt TraumaBlunt Trauma Blunt Trauma : Intra-abdominal Blunt Trauma : Intra-abdominal
visceral damage must strongly visceral damage must strongly be suspected following blunt be suspected following blunt trauma to the abdomen, trauma to the abdomen, especially because evidence is especially because evidence is frequently subtle and misleading.frequently subtle and misleading.
Diagnosis of such injuries is Diagnosis of such injuries is often difficult, and an aggressive often difficult, and an aggressive approach is mandatoryapproach is mandatory

Blunt Trauma Multiple injuries are common, and
common signs and symptoms guide diagnosis.
If the above are absent or obscured by other injuries, special techniques must be applied.
Peritoneal lavage is a valuable diagnostic tool. A specific organ injury diagnosis is not necessary- only the finding of an acute abdominal injury.

ManagementManagement Re-establish vital function and Re-establish vital function and
optimizing oxygenation and tissue optimizing oxygenation and tissue perfusion.perfusion.
Delineating injury mechanism.Delineating injury mechanism. Maintaining a high index of suspicion Maintaining a high index of suspicion
related to occult vascular and related to occult vascular and retroperitoneal injuries.retroperitoneal injuries.
Repeating a meticulous physical Repeating a meticulous physical examination, assessing for changesexamination, assessing for changes
Selecting adjunctive diagnostic Selecting adjunctive diagnostic maneuvers as needed, performed with maneuvers as needed, performed with a minimal loss of t imea minimal loss of t ime ..