ABCs in EIDs: Preparing for Emerging Infectious Diseases
59
Your Step by Step Guide in Preparing for Emerging Infectious Diseases Arthur Dessi E. Roman MD MTM FPCP FPSMID PHICS 21 st Annual Convention Crowne Plaza Galleria Manila, 28 May 2015 EIDs @ gonnabedess # WhatNow @PHICS2015 @ gonnabedess ‘s in by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
-
Upload
arthur-dessi-roman -
Category
Health & Medicine
-
view
200 -
download
1
Transcript of ABCs in EIDs: Preparing for Emerging Infectious Diseases
Your Step by Step Guide in Preparing for Emerging Infectious Diseases
Arthur Dessi E. Roman MD MTM FPCP FPSMIDPHICS 21st Annual Convention
Crowne Plaza Galleria Manila, 28 May 2015
EIDs
@gonnabedess #WhatNow@PHICS2015 @gonnabedess
‘s in
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
2RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Why is PH concerned about the threat of EIDs?
According to NSO, as of April 2014:
•
worldwide
• ~53.3 % in Middle East (majority are in KSA)
• China is nearby
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
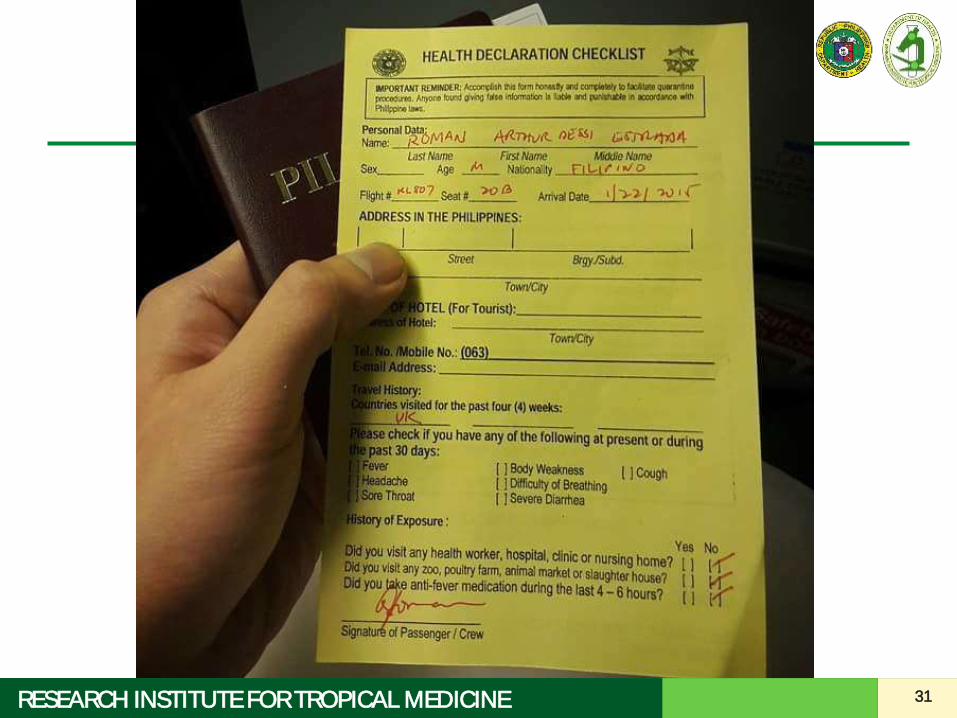
With emerging diseases at the forefront, should travel
history be placed in the general data?
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
4RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Objectives
• To discuss general guidelines in preparing for EIDs in your institution
• To elaborate on the roles of hospitals/frontliners in case detection, reporting, and controlling the spread of EIDs
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
5RESEARCH INSTITUTE FOR TROPICAL MEDICINE
EIDs are evolving
Interim guidelines change as new information becomes available.
Keep yourself updated!
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
7RESEARCH INSTITUTE FOR TROPICAL MEDICINE
www.ritm.gov.ph
8RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Patient care Safety of HCW
9RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Definitions
“Emerging" infectious diseases
Infectious diseases whose incidence in humans has increased in the past 2 decades or threatens to
increase in the near future which respect no national boundaries
http://wwwnc.cdc.gov/eid/page/background-goals
10RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Definitions
Re-emerging Infectious Diseases
Old infections re-emerging as a result of antimicrobial resistance in known agents or breakdowns in public
health measures/ infrastructures, e.g. diphtheria, pertussis, measles, Chikungunya

11RESEARCH INSTITUTE FOR TROPICAL MEDICINE
12RESEARCH INSTITUTE FOR TROPICAL MEDICINE
European Centre for Disease Prevention and Control. Communicable disease threats report, Week 21, 17-23 May 2015. Accessed on 23 May 2015 from http://www.ecdc.europa.eu/en/publications/Publications/ communicable-disease-threats-report-23-may-2015.pdf
MERS-CoV Case Count as of 23 May 2015
• Total no. of confirmed cases: 1,152
• Total no. of deaths: 471 deaths
• Crude case fatality rate: 40.9%
13RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Where did MERS-CoV come from?
• MERS CoV found in camels from Egypt, Qatar, and Saudi Arabia
• Camels from Jordan, Oman, Qatar, Saudi Arabia and the UAE (even from Egypt, Kenya, Nigeria and other African araes) have shown high rates of antibodies against MERS-CoV
Evidence for Camel-to-Human Transmission of MERS Coronavirus. New England Journal of Medicine, 2014. 371(14): p. 1359-1360.Alagaili, A.N., et al., Middle East respiratory syndrome coronavirus infection in dromedary camels in Saudi Arabia. mBio, 2014. 5(2): p. e00884-14.
14RESEARCH INSTITUTE FOR TROPICAL MEDICINE
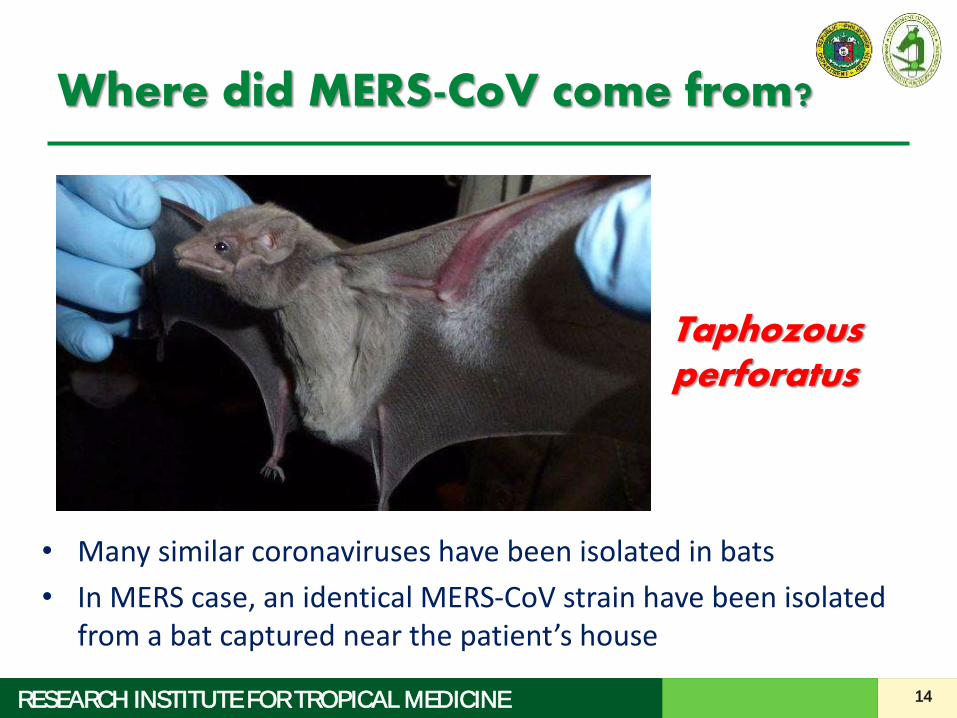
Where did MERS-CoV come from?
• Many similar coronaviruses have been isolated in bats
• In MERS case, an identical MERS-CoV strain have been isolated from a bat captured near the patient’s house
Taphozousperforatus
15RESEARCH INSTITUTE FOR TROPICAL MEDICINE
How did it transfer from camels to humans?
• Still not clear.
• Droplet contact?
– high viral loads in nasal swab samples from camels
– Fecal samples
– conjunctival swabs
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
16RESEARCH INSTITUTE FOR TROPICAL MEDICINE
How did it transfer from camels to humans?
• A recent study published by Azhar EI et al. reported the isolation of the virus in an air sample collected in a camel barn involved in a possible camel-to-human outbreak, warranting further investigations for the possible airborne transmission of MERS-CoV
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
17RESEARCH INSTITUTE FOR TROPICAL MEDICINE
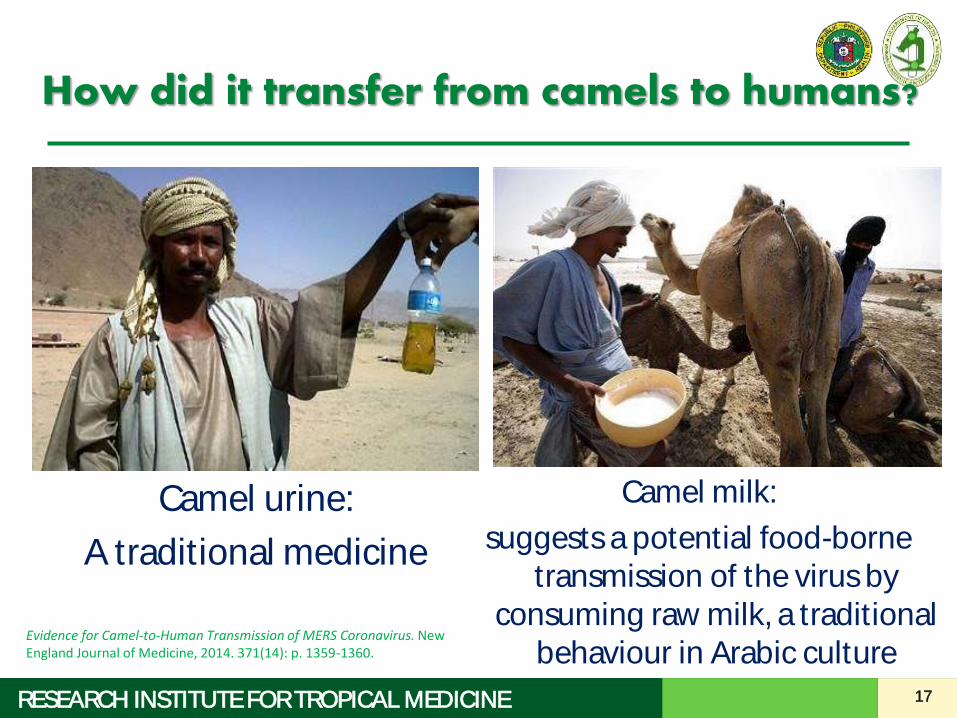
How did it transfer from camels to humans?
Camel urine:
A traditional medicine
Camel milk:
suggests a potential food-borne transmission of the virus by
consuming raw milk, a traditional behaviour in Arabic culture
Evidence for Camel-to-Human Transmission of MERS Coronavirus. New England Journal of Medicine, 2014. 371(14): p. 1359-1360.
How infectious is MERS?
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
19RESEARCH INSTITUTE FOR TROPICAL MEDICINE
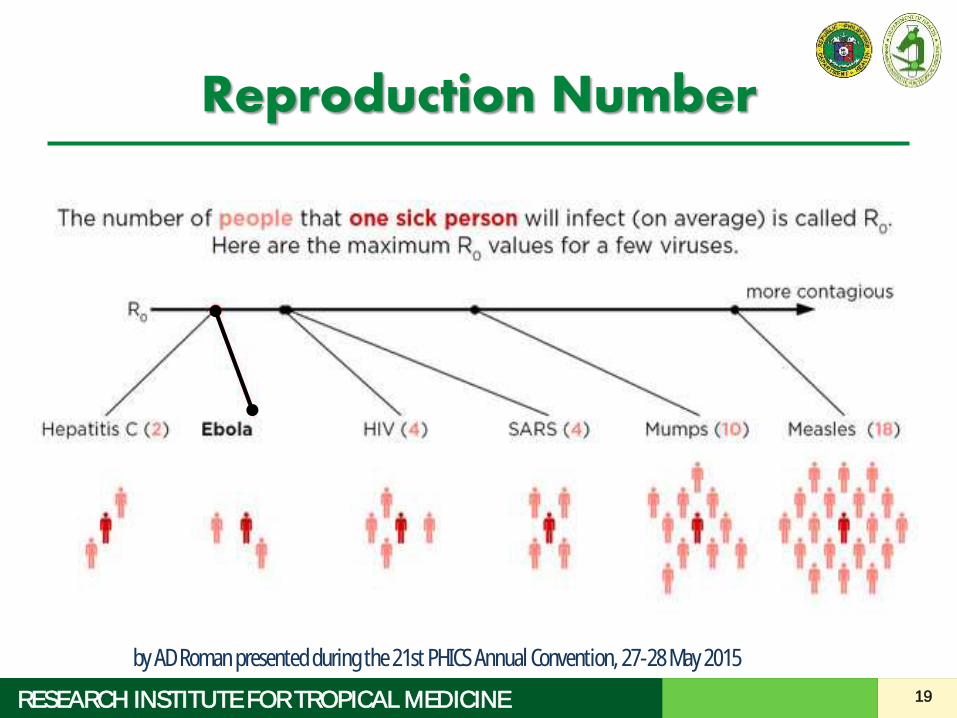
Reproduction Number
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
20RESEARCH INSTITUTE FOR TROPICAL MEDICINE
MERS: Reproduction number
MERS R0 = 0.60 to 0.69
suggests that MERS-CoV does not yet have pandemic potential
No ongoing spreading of MERS-CoV in the community
Romulus Breban, Julien Riou, Arnaud Fontanet: Interhuman transmissibility of Middle East respiratory syndrome coronavirus: estimation of pandemic risk. The Lancet, 05 July 2013
21RESEARCH INSTITUTE FOR TROPICAL MEDICINE
MERS: Transmission
• human-to-human transmission occurs via, close contact
– caring for or living with an infected person
– healthcare workers taking care of MERS patients
• All reported cases have been linked to countries in and near the Arabian Peninsula.
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
22RESEARCH INSTITUTE FOR TROPICAL MEDICINE
MERS-CoV
• It is not always possible to identify patients with MERS-CoV early because some have mild or unusual symptoms
– It is important that health-care workers apply standard precautions consistently with all patients regardless of their diagnosis in all work practices all the time
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
23RESEARCH INSTITUTE FOR TROPICAL MEDICINE
MERS-CoV
• Droplet precautions should be added to the standard precautions when providing care to all patients with symptoms of acute respiratory infection
• Contact precautions and eye protection should be added when caring for probable or confirmed cases of MERS-CoV infection
• Airborne precautions should be applied when performing aerosol generating procedures
24RESEARCH INSTITUTE FOR TROPICAL MEDICINE
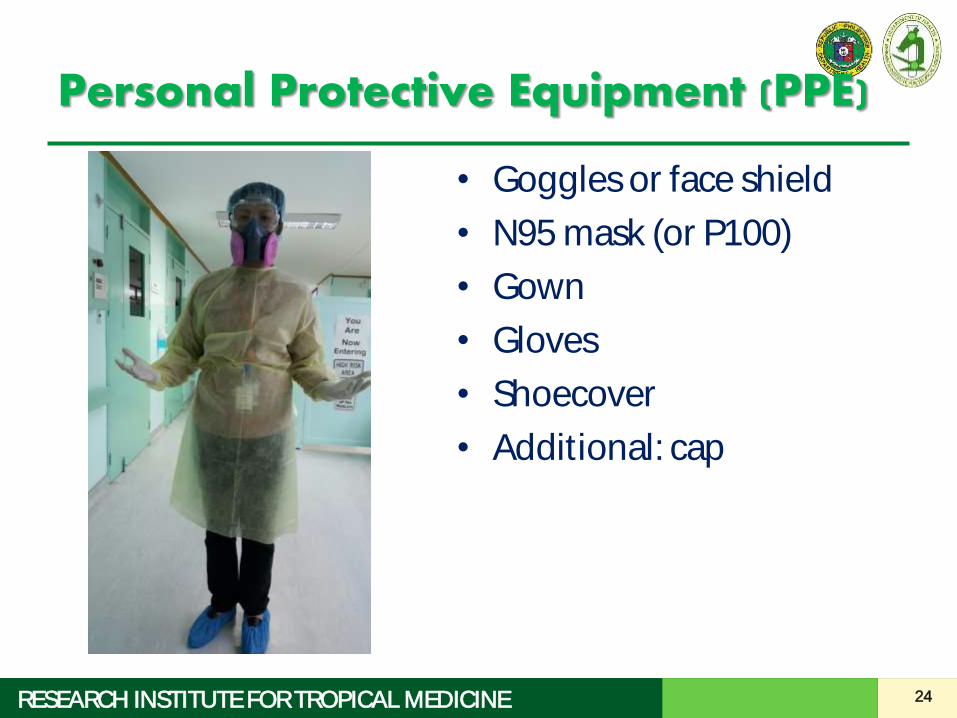
Personal Protective Equipment (PPE)
• Goggles or face shield
• N95 mask (or P100)
• Gown
• Gloves
• Shoecover
• Additional: cap
Spot Quiz
What is the is the single most important action to stop
spreading infection and disease?
A. Wearing a mask
B. Taking daily Vitamin C
C. Handwashing
D. Taking antibiotics
26RESEARCH INSTITUTE FOR TROPICAL MEDICINE
General Guidelines in the Preparation and Management of EIDs
1. Operationalize your response.2. Designate a team in charge of EIDs.3. Designate areas in your institution for:
– Screening and triage– Isolation of suspect cases
4. Apply standard precautions for all patients.5. Understand the basics of transmission-based
precautions.6. Decide on the extent of your patient
involvement and prepare accordingly.
27RESEARCH INSTITUTE FOR TROPICAL MEDICINE
General Guidelines in the Preparation and Management of EIDs
1. Operationalize your response.2. Decide on the extent of your patient
involvement and prepare accordingly.3. Designate a team in charge of EIDs.4. Designate areas in your institution for:
– Screening and triage– Isolation of suspect cases
5. Apply standard precautions for all patients.6. Understand the basics of transmission-based
precautions.
• Align with national preparedness plan.• Determine response based on current situation.oNo reported case locally, one reported cases, all
referral hospital full, overflow of cases in the community
• Determine how the regular hospital operations will be affected by admitting EID cases.
28RESEARCH INSTITUTE FOR TROPICAL MEDICINE
General Guidelines in the Preparation and Management of EIDs
1. Operationalize your response.2. Decide on the extent of your patient
involvement and prepare accordingly.3. Designate a team in charge of EIDs.4. Designate areas in your institution for:
– Screening and triage– Isolation of suspect cases
5. Apply standard precautions for all patients.6. Understand the basics of transmission-based
precautions.
• Assess your capacity as a hospital in terms of:o Manpower and skillso Space, equipment, facilityo Hospital operationo Need of the communityo Availability and proximity of other institutions
who will admit EIDs
29RESEARCH INSTITUTE FOR TROPICAL MEDICINE
General Guidelines in the Preparation and Management of EIDs
1. Operationalize your response.2. Decide on the extent of your patient
involvement and prepare accordingly.3. Designate a team in charge of EIDs.4. Designate areas in your institution for:
– Screening and triage– Isolation of suspect cases
5. Apply standard precautions for all patients.6. Understand the basics of transmission-based
precautions.
• Formulate and train your ICC• Attend trainings• Seek the help of experts (IDS, ICN Nurses, PHICS)
30RESEARCH INSTITUTE FOR TROPICAL MEDICINE
General Guidelines in the Preparation and Management of EIDs
1. Operationalize your response.2. Decide on the extent of your patient
involvement and prepare accordingly.3. Designate a team in charge of EIDs.4. Designate areas in your institution for:
– Screening and triage– Isolation of suspect cases
5. Apply standard precautions for all patients.6. Understand the basics of transmission-based
precautions.
31RESEARCH INSTITUTE FOR TROPICAL MEDICINE
32RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Screening and Triage
Screening
To quickly identify people with a travel history to affected countries
Triage
To determine if these persons have significant contact and if they have symptoms
Goal
To promptly isolate suspects if symptomatic or provide home advice as necessary
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
33RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Screening and Triage
A stepwise process of screening based on travel history followed by triage is more manageable in most
institutions than a combined screening and triage process.
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015

34RESEARCH INSTITUTE FOR TROPICAL MEDICINE
35RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Isolation/Holding Area
• This is the area where patients wait while
transfer to the referral hospital is being
coordinated.
• Provide surgical masks to the patients and as
much as possible minimize contact with them
unless deemed necessary
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
36RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Isolation/Holding Area
• The holding area should be:
– Near triage area for quick transfer
– Distant from other crowded areas1
– Well ventilated / adequate ventilation and room
air exchange (negative pressure or
independent air-conditioning unit and exhaust
or open windows)1,2
– Own sink and toilet facilities2
– Have adequate sunlight1
– Known to everyone in the facility11Clinical Management of Patients with Viral Haemorrhagic Fever: A pocket Guide for the Front-line Health Worker
13 April 2014. . World Health Organization 20142Interim Clinical Guidelines on Severe Acute Respiratory Syndrome (SARS) for Health Facilities in the Philippines
Department of Health. Technical Working Group on SARS Clinical Guidelines, July 25, 2003
What if we don’t have a negative pressure room?
• Properly labeled and identified, easily recognizable by visitors and hospital personnel
• Good ventilation• Entering HCWs should wear appropriate PPE
by AD Roman presented during the 21st PHICS Annual Convention, 27-28
38RESEARCH INSTITUTE FOR TROPICAL MEDICINE
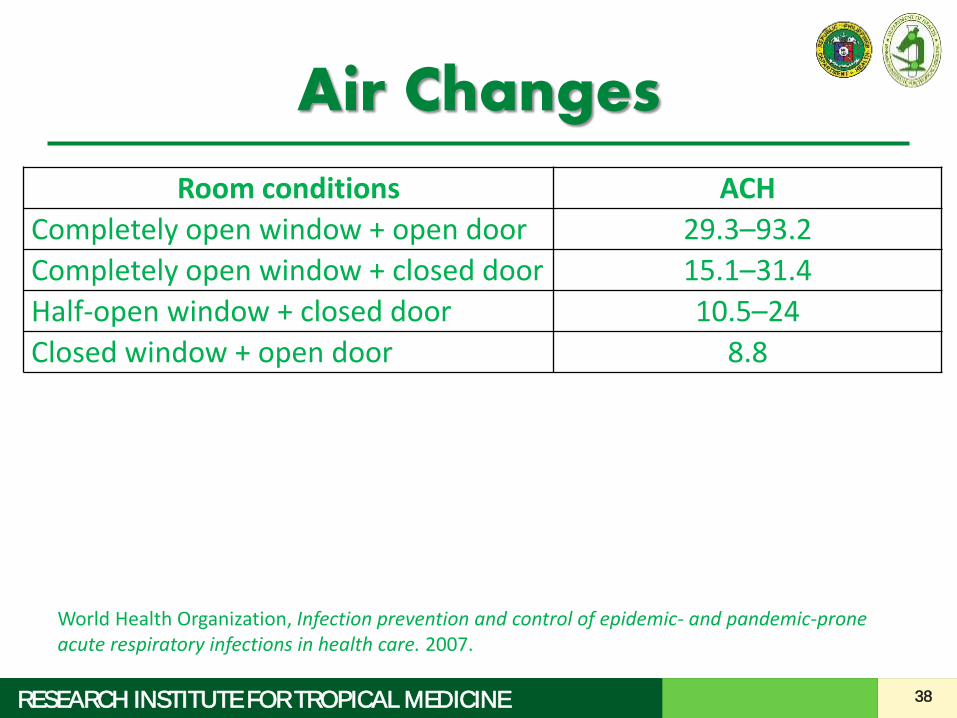
Air Changes
Room conditions ACH
Completely open window + open door 29.3–93.2
Completely open window + closed door 15.1–31.4
Half-open window + closed door 10.5–24
Closed window + open door 8.8
World Health Organization, Infection prevention and control of epidemic- and pandemic-prone acute respiratory infections in health care. 2007.
39RESEARCH INSTITUTE FOR TROPICAL MEDICINE
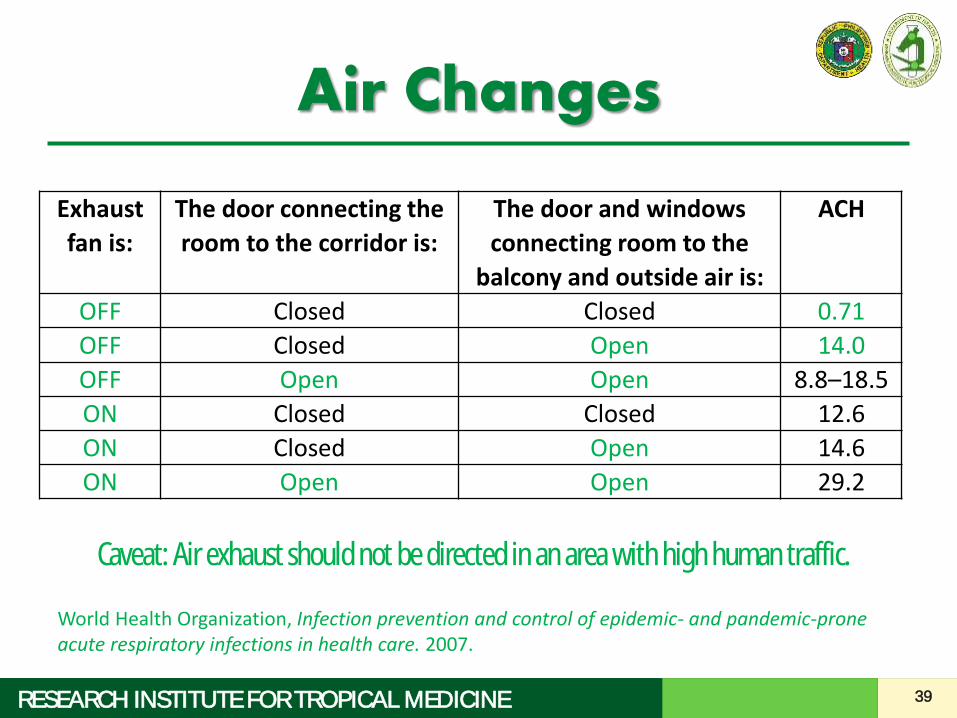
Air Changes
Exhaust
fan is:
The door connecting the
room to the corridor is:
The door and windows
connecting room to the
balcony and outside air is:
ACH
OFF Closed Closed 0.71
OFF Closed Open 14.0
OFF Open Open 8.8–18.5
ON Closed Closed 12.6
ON Closed Open 14.6
ON Open Open 29.2
World Health Organization, Infection prevention and control of epidemic- and pandemic-prone acute respiratory infections in health care. 2007.
Caveat: Air exhaust should not be directed in an area with high human traffic.
40RESEARCH INSTITUTE FOR TROPICAL MEDICINE
General Guidelines in the Preparation and Management of EIDs
1. Operationalize your response.2. Decide on the extent of your patient
involvement and prepare accordingly.3. Designate a team in charge of EIDs.4. Designate areas in your institution for:
– Screening and triage– Isolation of suspect cases
5. Apply standard precautions for all patients.6. Understand the basics of transmission-based
precautions.
41RESEARCH INSTITUTE FOR TROPICAL MEDICINE
General Guidelines in the Preparation and Management of EIDs
1. Operationalize your response.2. Decide on the extent of your patient
involvement and prepare accordingly.3. Designate a team in charge of EIDs.4. Designate areas in your institution for:
– Screening and triage– Isolation of suspect cases
5. Apply standard precautions for all patients.6. Understand the basics of transmission-based
precautions.

Airborne precautions for...
by AD Roman presented during the 21st PHICS Annual Convention, 27-28
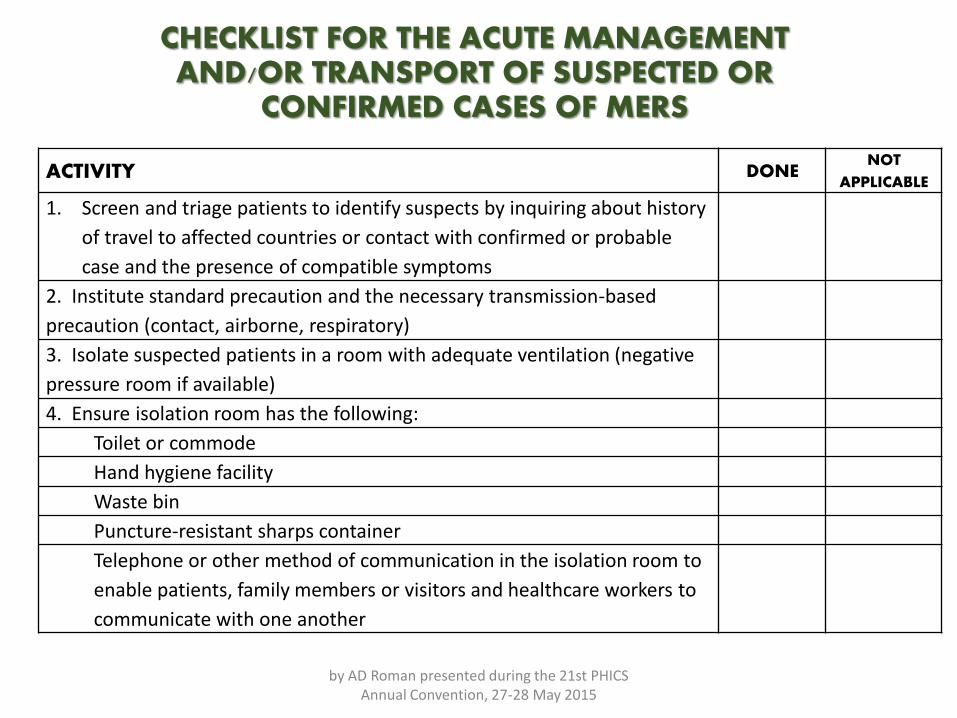
CHECKLIST FOR THE ACUTE MANAGEMENT AND/OR TRANSPORT OF SUSPECTED OR
CONFIRMED CASES OF MERS
ACTIVITY DONENOT
APPLICABLE
1. Screen and triage patients to identify suspects by inquiring about history
of travel to affected countries or contact with confirmed or probable
case and the presence of compatible symptoms
2. Institute standard precaution and the necessary transmission-based
precaution (contact, airborne, respiratory)
3. Isolate suspected patients in a room with adequate ventilation (negative
pressure room if available)
4. Ensure isolation room has the following:
Toilet or commode
Hand hygiene facility
Waste bin
Puncture-resistant sharps container
Telephone or other method of communication in the isolation room to
enable patients, family members or visitors and healthcare workers to
communicate with one another
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
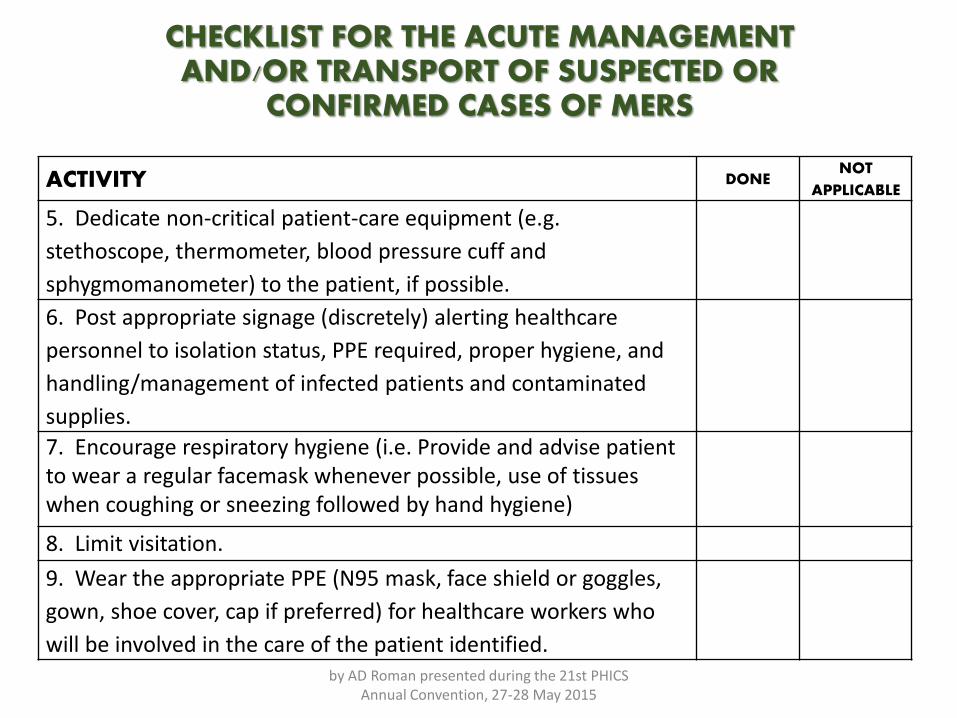
CHECKLIST FOR THE ACUTE MANAGEMENT AND/OR TRANSPORT OF SUSPECTED OR
CONFIRMED CASES OF MERS
ACTIVITY DONENOT
APPLICABLE
5. Dedicate non-critical patient-care equipment (e.g.
stethoscope, thermometer, blood pressure cuff and
sphygmomanometer) to the patient, if possible.
6. Post appropriate signage (discretely) alerting healthcare
personnel to isolation status, PPE required, proper hygiene, and
handling/management of infected patients and contaminated
supplies.
7. Encourage respiratory hygiene (i.e. Provide and advise patient to wear a regular facemask whenever possible, use of tissues when coughing or sneezing followed by hand hygiene)
8. Limit visitation.
9. Wear the appropriate PPE (N95 mask, face shield or goggles,
gown, shoe cover, cap if preferred) for healthcare workers who
will be involved in the care of the patient identified.by AD Roman presented during the 21st PHICS
Annual Convention, 27-28 May 2015
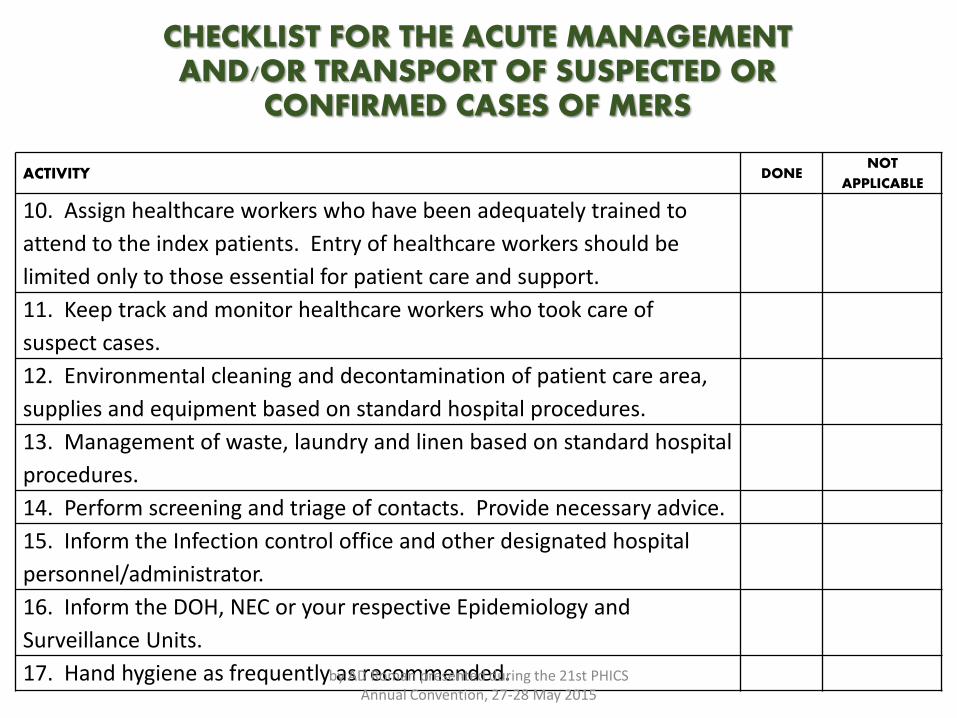
CHECKLIST FOR THE ACUTE MANAGEMENT AND/OR TRANSPORT OF SUSPECTED OR
CONFIRMED CASES OF MERS
ACTIVITY DONENOT
APPLICABLE
10. Assign healthcare workers who have been adequately trained to
attend to the index patients. Entry of healthcare workers should be
limited only to those essential for patient care and support.
11. Keep track and monitor healthcare workers who took care of
suspect cases.
12. Environmental cleaning and decontamination of patient care area,
supplies and equipment based on standard hospital procedures.
13. Management of waste, laundry and linen based on standard hospital
procedures.
14. Perform screening and triage of contacts. Provide necessary advice.
15. Inform the Infection control office and other designated hospital
personnel/administrator.
16. Inform the DOH, NEC or your respective Epidemiology and
Surveillance Units.
17. Hand hygiene as frequently as recommended.by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
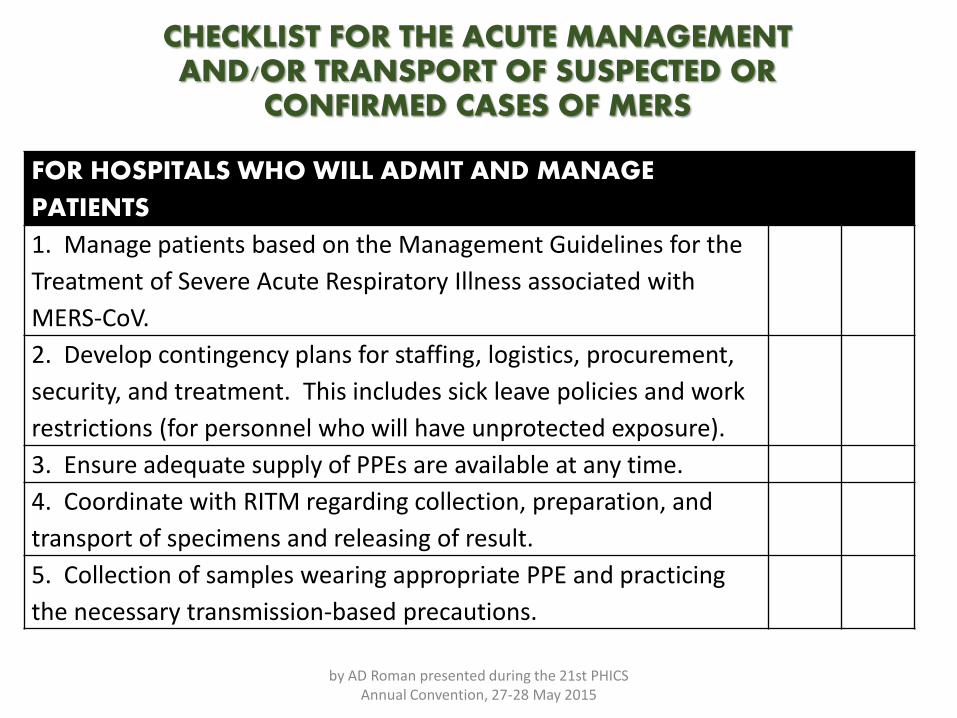
CHECKLIST FOR THE ACUTE MANAGEMENT AND/OR TRANSPORT OF SUSPECTED OR
CONFIRMED CASES OF MERS
FOR HOSPITALS WHO WILL ADMIT AND MANAGE
PATIENTS
1. Manage patients based on the Management Guidelines for the
Treatment of Severe Acute Respiratory Illness associated with
MERS-CoV.
2. Develop contingency plans for staffing, logistics, procurement,
security, and treatment. This includes sick leave policies and work
restrictions (for personnel who will have unprotected exposure).
3. Ensure adequate supply of PPEs are available at any time.
4. Coordinate with RITM regarding collection, preparation, and
transport of specimens and releasing of result.
5. Collection of samples wearing appropriate PPE and practicing
the necessary transmission-based precautions.
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
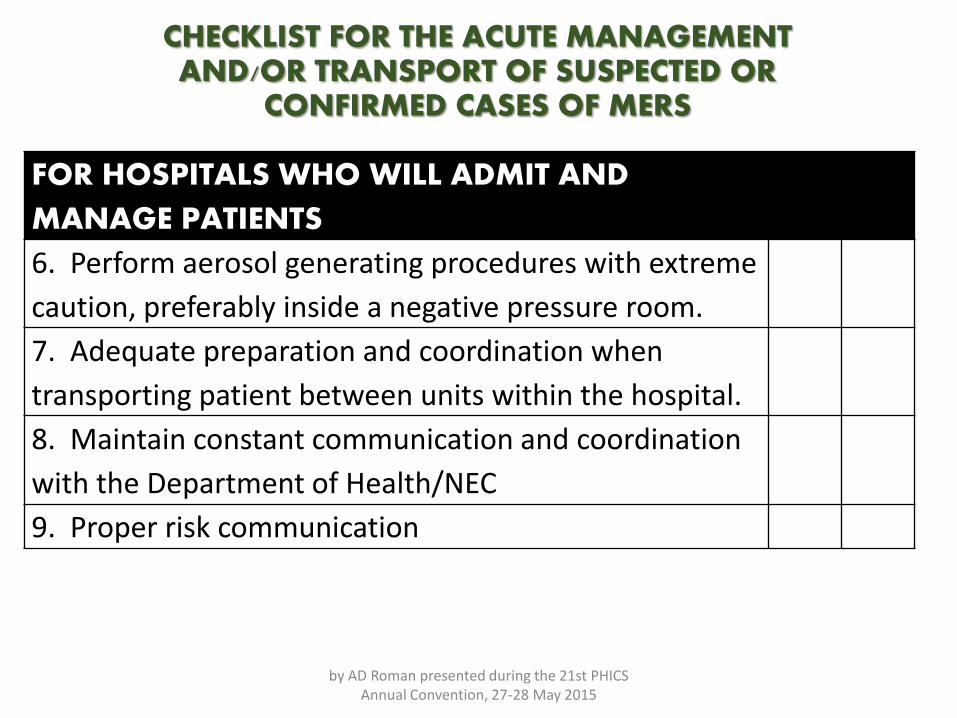
CHECKLIST FOR THE ACUTE MANAGEMENT AND/OR TRANSPORT OF SUSPECTED OR
CONFIRMED CASES OF MERS
FOR HOSPITALS WHO WILL ADMIT AND
MANAGE PATIENTS
6. Perform aerosol generating procedures with extreme
caution, preferably inside a negative pressure room.
7. Adequate preparation and coordination when
transporting patient between units within the hospital.
8. Maintain constant communication and coordination
with the Department of Health/NEC
9. Proper risk communication
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
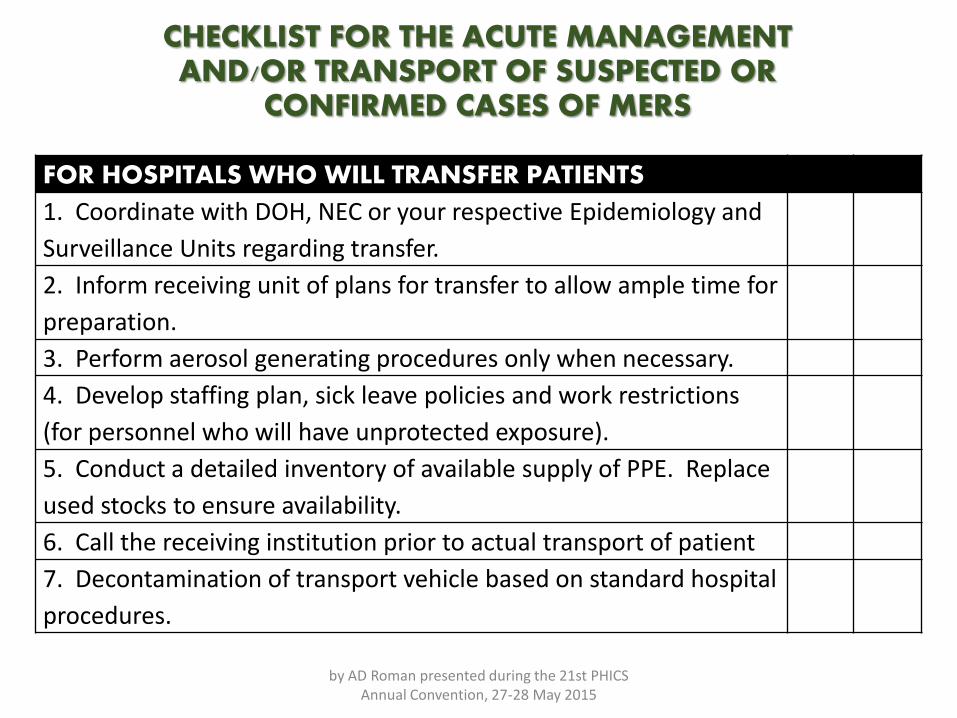
CHECKLIST FOR THE ACUTE MANAGEMENT AND/OR TRANSPORT OF SUSPECTED OR
CONFIRMED CASES OF MERS
FOR HOSPITALS WHO WILL TRANSFER PATIENTS
1. Coordinate with DOH, NEC or your respective Epidemiology and
Surveillance Units regarding transfer.
2. Inform receiving unit of plans for transfer to allow ample time for
preparation.
3. Perform aerosol generating procedures only when necessary.
4. Develop staffing plan, sick leave policies and work restrictions
(for personnel who will have unprotected exposure).
5. Conduct a detailed inventory of available supply of PPE. Replace
used stocks to ensure availability.
6. Call the receiving institution prior to actual transport of patient
7. Decontamination of transport vehicle based on standard hospital
procedures.
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
49RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Transport
• Use portable devices (e.g. portable x-ray, ultrasound) as much as possible.
• Decontaminate infected surfaces afterwards.
• Transport and move patients only when necessary.
• Ask patients to wear surgical masks (if they can tolerate) when going out of the isolation room to contain secretions.
50RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Transport
• Ensure that health-care workers who are transporting patients wear appropriate PPE and perform hand hygiene afterwards.
• Prior to transport and arrival, notify the receiving unit of the patient's diagnosis and precautions that will be required.

51RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Transport: Ebola

52RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Transport: Ebola

53RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Transport: Ebola

54RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Transport: Ebola

55RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Transport: Ebola
56RESEARCH INSTITUTE FOR TROPICAL MEDICINE
Contact numbers
• NEC 711-1001/711-1002
• RITM Hotline 664-6568 (24 hrs)
• RITM Surveillance Unit 994-1887 (24 hrs)
EIDs are here and they are here to stay.
Efficient screening and triage is important:To prevent entry and spread in the country
For prompt isolation and management
In the management of EIDs, balance between patient care & healthcare worker
safety should be achieved
Summary
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015
Infection control strategies play a major role in the control of EIDs. This will depend on
transmission-based precautions and application of standard precautions on all patients.
Institution should be ready to handle specific issues that may arise in the course of
management in EIDs via a multidisciplinary approach.
Do not be caught off guard.
Summary
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015

ありがとう (JP) Thank you (En)Arigatou
by AD Roman presented during the 21st PHICS Annual Convention, 27-28 May 2015