A Randomized Study Comparing Methylprednisolone Plus ......Research Laboratory test: orlowserum...
7
A Randomized Study Comparing Methylprednisolone Plus Chlorambucil Versus Methylprednisolone Plus Cyclophosphamide in Idiopathic Membranous Nephropathy CLAUDIO PONTICELLI,* PAOLO ALTIERI,t FRANCESCO SCOLARI, PATRIZIA PASSERINI,* DARIO ROCCATELLO, BRUNO CESANA,” PATRIZIA MELIS,t BRUNELLA VALZORIO, MAURO SASDELLI,1 SONIA PASQUALI,# CLAUDIO POZZI,** GIUSEPPE PICCOLI, ANTONIO LUPO,tt SIRO SEGAGNI, FRANCESCO ANTONUCCI,5 MAURO DUGO,111’ MARILENA MINARI,11 ALFIO SCALIA, LUCIANO PEDRINI,*** GABRIELE PISANO,ttt CLAUDIO GRASSI,t MARCO FARINA, and ROBERTO BELLAZZI’1111 *Dj,jsjone di Nefrologia e Dialisi IRCCS Ospedale Maggiore Milano; OspedaIe Brotzu Cagliari; Ospedale Regionale Spedali Civili Brescia; ‘Ospedale Giovanni Bosco Torino; ‘Laboratorio Epidemiologico IRCCS Ospedale Maggiore Milano; ‘Ospedale Civile Arezzo; #Ospedale Malpighi Bologna; **Ospedale Civile Lecco; “Ospedale Regionale Civile Maggiore Verona; Fondazione Clinica del Lavoro Pavia; Ospedale Provinciale Feltre; 1Ospedale Provinciale Castelfranco Veneto; tOspedale Regionale Parma; ##Ospedale Zonaie Uboldo Cernusco sul Naviglio; ***Ospedale Provinciale Civile Sondrio; Ospedale Provinciale Magenta; Ospedale Predabissi Melegnano; Ospedale Provinciale Maggiore Lodi; and hiOspedale Provinciale Civile Vigevano. Abstract. To assess whether chborarubucil or cycbophospha- mide may have a better therapeutic index in patients with idiopathic merubranous ncphropathy, we compared two regi- mens based on a 6-mo treatment, alternating every other month methylpnednisobone with chborambucib or mcthylprcdnisobone with cycbophosphamide. Patients with biopsy-proven membra- nous ncphropathy and with a ncphrotic syndrome were ran- domized to be given methylprednisobonc (1 g intravenously for 3 consecutive days followed by oral ructhylpnednisobone, 0.4 mg/kg per d for 27 d) alternated every other month either with chlonambucil (0.2 rug/kg per d for 30 d) or cycbophosphamide (2.5 mgfkg per d for 30 d). The whole treatment lasted 6 mo: 3 mo with corticosteroids and 3 mo with one cytotoxic drug. Among 87 patients followed for at beast 1 yr. 36 of 44 (82%; 95% confidence interval [CI], 67.3 to 91 .8%) assigned to methylprcdnisobone and chborambucib entered complete on par- tial remission of the ncphrotic syndrome, versus 40 of 43 (93%; 95% CI, 80.9 to 98.5%) assigned to mcthylpnednisobonc and cycbophosphamide (P = 0. 1 16). Of patients who attained remission of the ncphrotic syndrome, 1 1 of 36 in the chloram- bucib group (30.5%) and 10 of 40 in the cycbophosphamidc group (25%) had a relapse of the nephrotic syndrome between 6 and 30 mo. The reciprocal of plasma creatininc improved in the cohort groups followed for I yr for both treatment groups (P < 0.01) and remained unchanged when compared with basal values in the cohort groups followed for 2 and 3 yr. Six patients in the chborambucib group and two in the cycbophos- phamide group did not complete the treatment because of side effects. Four patients in the chlorambucil group but none in the cycbophosphamide group suffered from herpes zoster. One patient per group developed cancer. It is concluded that in ncphrotic patients with idiopathic merubranous nephropathy both treatments may be effective in favoring remission and in preserving renal function for at least 3 yr. (I Am Soc Nephrob 9: 444-450, 1998) There is now controlled evidence that a 6-mo course with methylprednisobonc and chbonambucil may favor remission of Received June 16, 1997. Accepted September 6. 1997. Correspondence to Dr. Claudio Ponticelli, Divisione di Nefrologia e Dialisi. Ospedale Maggiore Policlinico IRCCS, via Commenda 15. 20122 Milano, Italy. 1046-6673/0903-0444$03.00/0 Journal of the American Society of Nephrology Copyright 0 1998 by the American Society of Nephrology the nephrotic syndrome (1-3) and may significantly improve the 10-yr kidney survival rate in patients with idiopathic mem- branous nephropathy (4). Randomized (5) and nonrandomized (6,7) trials showed that this regimen can improve kidney func- tion and reduce protcinunia also in patients with established renal insufficiency. Only a few nephrobogists, however, arc familiar with chborarubucil; the majority have experience with cycbophosph- amidc. Although cycbophosphamide and chborambucil both have the capacity to contribute alkyl groups to biologically
Transcript of A Randomized Study Comparing Methylprednisolone Plus ......Research Laboratory test: orlowserum...
A Randomized Study Comparing Methylprednisolone Plus
Chlorambucil Versus Methylprednisolone Plus
Cyclophosphamide in Idiopathic Membranous Nephropathy
CLAUDIO PONTICELLI,* PAOLO ALTIERI,t FRANCESCO SCOLARI,�PATRIZIA PASSERINI,* DARIO ROCCATELLO,� BRUNO CESANA,”
PATRIZIA MELIS,t BRUNELLA VALZORIO,� MAURO SASDELLI,1
SONIA PASQUALI,# CLAUDIO POZZI,** GIUSEPPE PICCOLI,� ANTONIO LUPO,tt
SIRO SEGAGNI,� FRANCESCO ANTONUCCI,5� MAURO DUGO,111’
MARILENA MINARI,11 ALFIO SCALIA,� LUCIANO PEDRINI,***
GABRIELE PISANO,ttt CLAUDIO GRASSI,t� MARCO FARINA,� andROBERTO BELLAZZI�’1111*Dj�,jsjone di Nefrologia e Dialisi IRCCS Ospedale Maggiore Milano; �OspedaIe Brotzu Cagliari; �Ospedale
Regionale Spedali Civili Brescia; ‘�Ospedale Giovanni Bosco Torino; ‘Laboratorio Epidemiologico IRCCS
Ospedale Maggiore Milano; �‘Ospedale Civile Arezzo; #Ospedale Malpighi Bologna; **Ospedale Civile
Lecco; “Ospedale Regionale Civile Maggiore Verona; �Fondazione Clinica del Lavoro Pavia; �Ospedale
Provinciale Feltre; 1�Ospedale Provinciale Castelfranco Veneto; t��Ospedale Regionale Parma; ##Ospedale
Zonaie Uboldo Cernusco sul Naviglio; ***Ospedale Provinciale Civile Sondrio; �Ospedale Provinciale
Magenta; �Ospedale Predabissi Melegnano; �Ospedale Provinciale Maggiore Lodi; and hi�Ospedale
Provinciale Civile Vigevano.
Abstract. To assess whether chborarubucil or cycbophospha-
mide may have a better therapeutic index in patients with
idiopathic merubranous ncphropathy, we compared two regi-
mens based on a 6-mo treatment, alternating every other month
methylpnednisobone with chborambucib or mcthylprcdnisobone
with cycbophosphamide. Patients with biopsy-proven membra-
nous ncphropathy and with a ncphrotic syndrome were ran-
domized to be given methylprednisobonc (1 g intravenously for
3 consecutive days followed by oral ructhylpnednisobone, 0.4
mg/kg per d for 27 d) alternated every other month either with
chlonambucil (0.2 rug/kg per d for 30 d) or cycbophosphamide
(2.5 mgfkg per d for 30 d). The whole treatment lasted 6 mo:
3 mo with corticosteroids and 3 mo with one cytotoxic drug.
Among 87 patients followed for at beast 1 yr. 36 of 44 (82%;
95% confidence interval [CI], 67.3 to 91 .8%) assigned to
methylprcdnisobone and chborambucib entered complete on par-
tial remission of the ncphrotic syndrome, versus 40 of 43
(93%; 95% CI, 80.9 to 98.5%) assigned to mcthylpnednisobonc
and cycbophosphamide (P = 0. 1 16). Of patients who attained
remission of the ncphrotic syndrome, 1 1 of 36 in the chloram-
bucib group (30.5%) and 10 of 40 in the cycbophosphamidc
group (25%) had a relapse of the nephrotic syndrome between
6 and 30 mo. The reciprocal of plasma creatininc improved in
the cohort groups followed for I yr for both treatment groups
(P < 0.01) and remained unchanged when compared with
basal values in the cohort groups followed for 2 and 3 yr. Six
patients in the chborambucib group and two in the cycbophos-
phamide group did not complete the treatment because of side
effects. Four patients in the chlorambucil group but none in the
cycbophosphamide group suffered from herpes zoster. One
patient per group developed cancer. It is concluded that in
ncphrotic patients with idiopathic merubranous nephropathy
both treatments may be effective in favoring remission and in
preserving renal function for at least 3 yr. (I Am Soc Nephrob
9: 444-450, 1998)
There is now controlled evidence that a 6-mo course with
methylprednisobonc and chbonambucil may favor remission of
Received June 16, 1997. Accepted September 6. 1997.Correspondence to Dr. Claudio Ponticelli, Divisione di Nefrologia e Dialisi.
Ospedale Maggiore Policlinico IRCCS, via Commenda 15. 20122 Milano,
Italy.
1046-6673/0903-0444$03.00/0Journal of the American Society of Nephrology
Copyright 0 1998 by the American Society of Nephrology
the nephrotic syndrome (1-3) and may significantly improve
the 10-yr kidney survival rate in patients with idiopathic mem-
branous nephropathy (4). Randomized (5) and nonrandomized
(6,7) trials showed that this regimen can improve kidney func-
tion and reduce protcinunia also in patients with established
renal insufficiency.
Only a few nephrobogists, however, arc familiar with
chborarubucil; the majority have experience with cycbophosph-
amidc. Although cycbophosphamide and chborambucil both
have the capacity to contribute alkyl groups to biologically

Idiopathic Membranous Nephropathy 445
vital macromolecules such as DNA, there are differences be-
tween the two drugs in dosing, metabolism, pharmacokinetics,
and elimination. Thus, the results of treatment with either
chborambucil or cycbophospharuide might be different.
To evaluate whether these alkylating agents had similar
effects when alternated with corticosteroids in idiopathic mem-
branous nephropathy, we organized a multicenter, controlled
trial. Patients with biopsy-proven membranous nephropathy
and ncphrotic syndrome were randomly assigned to receive a
6-mo regimen with ructhylprednisobone alternated with
chborambucil or with the same doses of mcthylprednisobone
alternated with cycbophospharuide.
Materials and MethodsPatients
Patients of either sex. between the ages of 14 and 65 with a
biopsy-proven ruembranous nephropathy and a nephrotic syndrome
(defined as proteinuria exceeding 3.5 g/d and plasma albumin con-
centrations of <25 gIL), were considered for the study. The criteria
for exclusion were a plasma creatinine > I .7 mg per deciliter (150
�moLfL); previous treatments with corticosteroids, irumunosuppres-
sive drugs, or cycbosporine; a positive serum test for anti-DNA anti-
bodies (and antinuclear antibodies in many patients) or hepatitis B
antigen or hepatitis C virus antibodies; a positive Veneral Disease
Research Laboratory test: or low serum concentrations of the corn-
plement component C3 or C4. A clinical diagnosis of diabetes mel-
litus. malignancy. systemic lupus erythematosus, infections, or expo-
sure to drugs that could induce membranous nephropathy were also
criteria for exclusion.
Renal Histology
The pathologist at each study center examined each renal biopsy
specimen by light. immunofluorescence. and electron microscopy.
Gbomerular stages were classified according to the system of Ehren-
reich ci’ al. (8). Mesangial glornerular sclerosis and interstitial fibrosis
with tubular atrophy were classified as present or absent. No fob-
low-up biopsies were performed.
Study Design
This was an open-label multicenter study. The protocol was ap-
proved by the institutional review board of the coordinating center,
and each patient gave informed written consent. At the coordinating
center, patients were assigned consecutively to one of the two treat-
ruent regimens, according to a center-stratified random order. A
sample size of approximately 50 patients per group was necessary to
demonstrate a decrease of about 25% of response from a baseline of
80% with ruethylprednisobone plus chborambucil (2) at power of about
0.80 with a two-tailed test (alpha = 0.05). Patients were examined at
least every month during the first 6 ruo. every 2 mo until the end of
the first year, and every 3 to 6 ruo thereafter. At each visit, plasma
creatinine concentrations and 24-h urinary protein excretion rates
were measured, and the patient was questioned about symptoms and
possible side effects of therapy. Leukocyte, erythrocyte, and platelet
counts were measured every 7 to 10 d during administration of the
cytotoxic drug, and repeated at each visit.
In our previous experience with patients selected with the samecriteria, only one of 39 untreated patients had a spontaneous remission
of the nephrotic syndrome within 6 mo (4). Therefore, we preferred to
start early, without a run-in period, a potentially beneficial treatment
to prevent complications of the nephrotic syndrome. Patients assigned
to the chlorambucil group received three cycles of treatment with
methylprednisobone ( I g given intravenously on 3 consecutive days
and then 0.4 mg/kg body wt per d given orally for 27 d, in a single
morning dose), and each cycle was followed by 1 mo of treatment
with chborambucil (0.2 mg/kg per d, orally). Patients assigned to the
cyclophospharuide group received the same three cycles of methyl-
prednisobone, but chlorambucil was replaced by oral cycbophospha-
mide at a dose of 2.5 mg/kg body wt per d. If a patient’s leukocyte
count decreased below 5000 per cubic millimeter (5 X b0’�1L), the
dose of the cytotoxic agent was reduced by 50%. and it was discon-
tinued for the remainder of that cycle if the leukocyte count was less
than 3000 per cubic millimeter (3 X b0#{176}IL).The total duration of
treatment, therefore, was 6 mo for both groups; 3 ruo with the same
doses of methylprednisobone and 3 mo with either of the two cytotoxic
drugs. Steroids were completely stopped at the end of the study
period. The use of angiotensin-converting enzyme inhibitors was
discouraged but not prohibited. Hypolipemic drugs were permitted.
Clinical response was defined as a complete or partial remission.
Complete remission was defined as a reduction in the rate of urinary
protein excretion to �0.2 g/d for at least I wk. and partial remission
as a reduction in the rate of protein excretion to between 0.2 1 and 2
g/d for at least 1 wk, with a normal plasma creatinine concentration.
Relapse of the nephrotic syndrome was defined as an increase in
proteinuria to more than 3.5 g/d for at least I wk in patients who had
a remission. Stable worsening was defined as an increase in plasma
creatinine concentration of at least 50% over the baseline value.
Statistical Analyses
Cumulative probability of complete/partial remission, complete
remission alone, and thereafter of relapses was estimated according to
Kaplan and Meier (9). Because assumption of the hazard functions
proportionality cannot be considered fulfilled as suggested by the log
(-log) survival plots, survival curves have been shown for illustrative
purposes only; � tests have been performed on the cumulative
proportion of patients with complete or partial remission. A further
index of efficacy was obtained as the percentage of the remission time
(partial or complete) on the total follow-up for each patient. The two
treatments were then compared by the Wilcoxon rank sum test.
The reciprocal of the plasma creatinine and proteinuria values for
the two treatments were compared by mixed-factorial ANOVA for
repeated measurements (10), with treatment as a fixed, “between-
patient” factor at two levels and time as a fixed, “within-patient”
factor at 2 1 levels (every 6 mo). The Geisser-Greenhouse ( I I ) pro-
cedure for correction of the degrees of freedom for statistical signif-
icance of the within-patient terms was followed. In addition, a trend
analysis has been carried out by means of orthogonal polynomial
contrasts to assess the presence of a linear increasing/decreasing trend
(first degree), of an increasing and then decreasing (or vice versa)
trend (second degree). of an increasing-decreasing-increasing or de-
creasing-increasing-decreasing trend (third degree) of a mean fluctu-
ating pattern (degree higher than the third). Indeed, the shape of an
overall pattern could have therapeutic impact.
ResultsAmong 97 patients who satisfied the criteria for randomiza-
tion, two were wrongly randomized due to the presence of
underlying neoplasias (discovered, respectively, I wk and 2 mo
after randomization). Of the remaining 95 patients, 50 were
assigned to receive ructhylprednisobone and chlorarubucil,
whereas 45 were randomized to ruethylprednisobone and cy-
clophosphamide. However, two patients did not present at the
446 Journal of the American Society of Nephrobogy
follow-up visit and a 5 1 -yr-old woman died because of a
deep-vein thrombosis with acute renal failure and cardiac
shock 3 mo after the diagnosis of membranous nephropathy,
before treatment was started. There was no difference at pre-
sentation between the two groups in the main clinical, biobog-
ical, and histological features (Table I).
Four patients in the chborambucil group and one in the
cycbophosphamide group, who completed the treatment, did
not present at the follow-up visit and were considered lost to
follow-up after the sixth month. All of the other patients were
followed for at beast 1 yr (range, 12 to 78 mo). The median
period of follow-up was 36 mo (range, 12 to 78 mo) in the
chborambucil group and 42 mo (range, 12 to 72 mo) in the
cycbophosphamide group, with a very similar distribution.
Of the 87 patients followed for at least 1 yr. 76 (87.3%; 95%
CI, 78.5 to 93.5%) entered a complete (28 patients) or partial
remission (48 patients). The presence or absence of interstitial
fibrosis or mesangial sclerosis and the stage of gborucrubar
lesions at renal biopsy did not influence the likelihood nemis-
sion of ncphrotic syndrome. However, if one takes into account
the complete remission only this was significantly related to
the presence (8.7%; 95% CI, 10.7 to 28.0%) on absence
(40.6%; 95% CI, 28.5 to 53.6%) of mcsangial gbomenubar
sclerosis (P = 0.005). Of 44 patients assigned to methylpred-
nisobone and chlorarubucil, 36 (82%; 95% CI, 67.3 to 91.8%)
entered complete ( 12 patients) or partial remission (24 patients)
of protcinunia as a first event. Of the 43 patients given mcdi-
ylprednisobonc and cyclophosphamide, 40 (93%; 95% CI, 80.9
to 98.5%) entered complete (16 patients) or partial remission
(24 patients) as a first event. The difference between the two
groups was not significant (P = 0. 1 1 6). The curves of the
probability of a partial on a complete remission after treatment
were similar in the two study groups (Figure 1).
Eleven patients in the chborarubucib group and 10 in the
cycbophosphamide group had a relapse of the ncphrotic syn-
drome. All of the relapses occurred between the sixth and the
thirtieth month (Figure 2). Four patients were retreated. In the
chborambucil group, two patients were retreated with steroids
and chborambucil. One did not respond, and the other attained
partial remission. In the cycbophosphamidc group, one patient
was retreated with steroids and cycbophosphamide and had
complete remission. Another patient was treated with steroids
and chlorambucib and had partial remission. The median of the
percentage of time spent without nephrotic syndrome was 60%
of the whole period of observation for the entire study group,
without significant difference between the group given
chlorambucil (58.6%) and that given cycbophosphamide
(62.5%, P = 0.534). We considered separately patients with
complete follow-ups of 12, 24, and 36 mo, respectively, to
have more precise estimates on a greater number of patients for
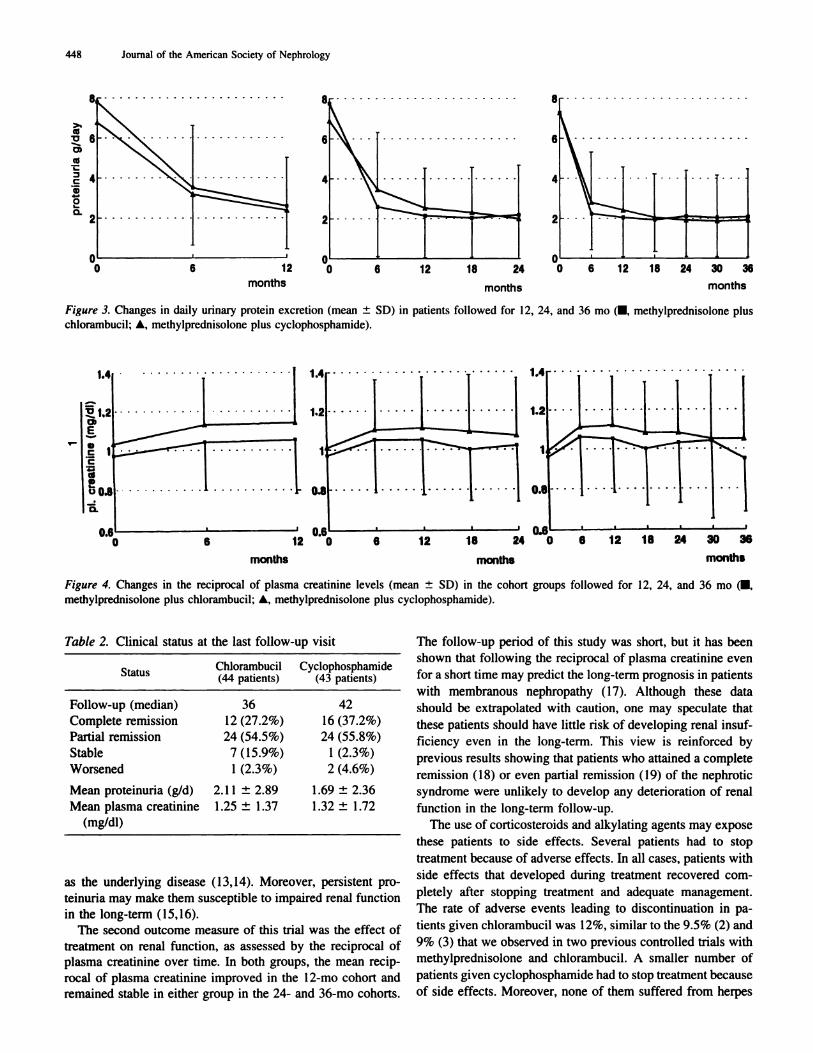
the I - and 2-yr analyses. For both of the treatment groups, there
was a significant decrease in proteinuria when compared with
the basal value for the patients with a complete follow-up of
12, 24, and 36 mo (P = 0.0001). Instead, differences between
the two treatment groups turned out not to be statistically
significant. After an early relevant decrease of protcinuria at 6
mo, there was a fluctuating pattern of approximately 2 g/d,
similar in the two treatment groups (Figure 3) as confirmed by
the significance (P < 0.0001) of the orthogonal polynomials
higher than the third degree.
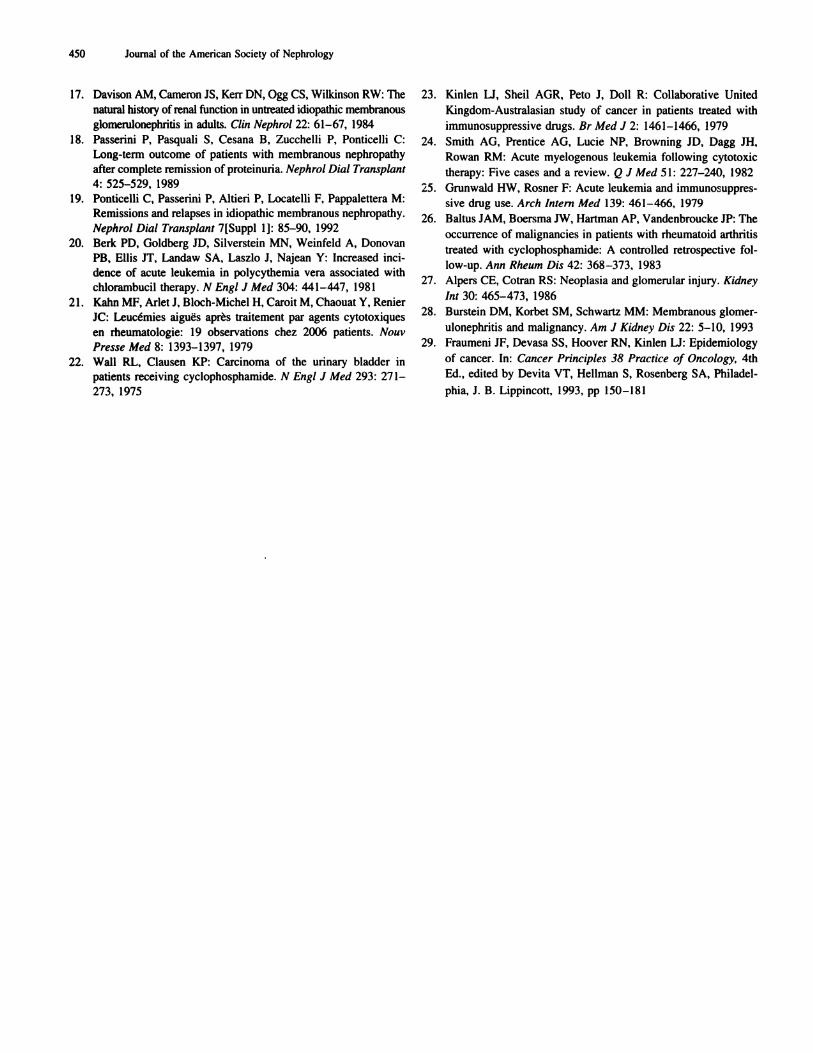
The reciprocal of plasma creatinine was significantly (at
least P < 0.0055) higher at 6 and 12 ruo for both treatment
Table 1. Characteristics of patients at the start of treatment with ructhylprcdnisolonc plus chborambucil on
ructhylprcdnisolonc plus cycbophospharuide”
CharacteristicMP + Chlorambucil
(�7 = 50)MP + Cyclophosphamide
(Ii = 45)
Age (median) 50 48
Range 18 to 65 17 to 55
Sex (MIF) 37/13 29/16
Plasma creatinine (mg/dl)” 1 .06 ± 0.27 1 .04 ± 0.27
Urinary protein excretion (g/d) 7.96 ± 5.19 6.85 ± 3.51
Hypertensive patients (ACE inhibitors) 15 (1) 14 (2)
Stage of gbomerular lesions at renal biopsy
lorIl 32 27
IIIorIV 18 18
Mesangial sclerosis
yes 14 12
no 36 33
Tububointerstitial lesions
yes 11 13
no 39 32
a Plus-minus values are means ± SD. Data for two patients (one per group) wrongly randomized are not included in this table. MP,methylprednisolone; ACE, angiotensin-converting enzyme.
h To convert values for creatinine to micromoles per liter, multiply by 88.4.

100
80
Partial + complete remiselon
0 6 12 18 24 30 36 42 48 54 60
months
Figure 1. Cumulative probability of obtaining partial or complete
remission of the nephrotic syndrome or complete remission alone as
a first event in patients given methylprednisobone plus chlorambucil
(- - -) and in patients given methylprednisolone plus cyclophospha-
mide (-). Data were calculated every 6 mo.
%
�
20 -
�o 6 12 18 24 30 36 42 48 54 60
Idiopathic Membranous Nephropathy 447
% at the sixth month because of leukopenia, which reversed
spontaneously. Two patients developed pneumonia after 5 and
3 mo of therapy, respectively. Both of them recovered but
continued without chlorambucil. One patient developed ane-
mia and thrombocytopenia with hypoplasia at the bone marrow
aspiration after I mo of chborambucib. He stopped treatment
with chborambucil and recovered. Another patient stopped
chborarubucil treatment because of nausea after a few days.
Two patients (4.5%) stopped treatment in the cycbophospha-
mide group, one because of nausea and vomiting after a few
days. The other patient stopped treatment after 2 ruo because of
a cerebral transient ischcmic attack. One patient per group
developed glucose intolerance during treatment, which re-
versed after completion of treatment. Four patients in the
chlorambucil group, but none in the cycbophosphamide group,
developed herpes zoster during treatment. In the long-term, a
40-yr-old woman treated with chlorambucib had irreversible
amenorrhea. In the chlorarubucil group, a man 58 yr old
developed a laryngeal carcinoma and underwent a laryngec-
tomy after 48 ruo. In the cyclophosphamide group, a 58-yr-old
man was recognized to have a prostatic carcinoma 66 mo after
randomization. Both patients are still alive after 1 2 and 6 mo,
respectively.
Figure 2. Cumulative probability of relapse of the nephrotic syndrome
after complete or partial remission in patients given methylpred-
nisolone plus chborambucil (- - -) and in patients given methylpred-
nisobone plus cyclophosphamide (-).
groups (without a statistically significant difference between
them) when compared with baseline, followed by a mild de-
crease to values similar to baseline, at least for patients fob-
bowed for 3 yr (Figure 4). One patient in the chborarubucil
group had worsening of renal function and had to be submitted
to regular dialysis after 42 mo of follow-up. Two patients in
the cycbophosphamide group worsened, and one of them had to
be submitted to regular dialysis after 36 mo of follow-up
(Table 2).
Six patients ( 12%) did not complete treatment in the
chborambucil group. Two of them did not receive chborambucil
DiscussionIn this study, a 6-mo course with methybprcdnisolonc and
chlorarubucil favored the remission of the ncphrotic syndrome
in patients with idiopathic ruembranous ncphnopathy. After
treatment, the mean proteinunia significantly decreased com-
pared with baseline at any time point considered. Eighty-two
percent of patients given mcthylprednisobonc and chborambucil
attained complete or partial remission of the ncphrotic syn-
droruc as a first event, a proportion similar to the 8 1 % (2) and
the 75% (3) found, respectively, in two previous different
controlled studies of Italian patients selected with the same
criteria and treated with methylprednisobone and chlonarubucil
for 6 mo. In the study presented here, some 30% of patients had
a relapse of the nephrotic syndrome, which occurred between
months the sixth and the thirtieth month.Similar results were observed in the group randomized to
ruethylprednisobone and cycbophosphamide. The mean de-
crease in protcinuria was similar to that seen in patients given
chborarubucil at any month cohort investigated. Ninety-three
percent of patients entered remission of the ncphrotic syn-
drome as a first event, and 24% had a relapse of the nephrotic
syndrome between the sixth and the twenty-fourth month.
However treated, patients spent 60% of the period of observa-
tion without nephrotic syndrome. The percentage of time in
remission was similar in the two study groups and was almost
the same as the 58% found in a previous trial with methyl-
prcdnisobonc and chborambucib (4). These data show that either
chborambucil or cycbophosphamide alternated with methyl-
prednisolone can result in a sustained remission of the ne-
phrotic syndrome in most patients. This result may have a
clinical impact if one considers that ncphrotic patients arc at a
greater risk of coronary heart disease (1 2) and thrombotic
events, particularly when they have membranous ncphnopathy
36
months months months
6 12 18 24 30
months months months
448 Journal of the American Society of Nephrology
>.(5
0)ci
:�Ca,0
0.
Figure 3. Changes in daily urinary protein excretion (mean ± SD) in patients followed for 12, 24, and 36 mo (�, methylprednisolone plus
chboranthucil; A, methylprednisobone plus cycbophospharuide).
Figure 4. Changes in the reciprocal of plasma creatinine levels (mean ± SD) in the cohort groups followed for 12, 24, and 36 mo (�,
methylprednisobone plus chlorambucil: A, methylprednisolone plus cyclophosphamide).
Table 2. Clinical status at the last follow-up visit
Status .Chborambucil(44 patients)
Cycbophosphamide(43 patients)
Follow-up (median) 36 42
Complete remission 12 (27.2%) 16 (37.2%)
Partial remission 24 (54.5%) 24 (55.8%)Stable 7 (15.9%) 1 (2.3%)
Worsened 1 (2.3%) 2 (4.6%)
Mean proteinunia (g/d) 2. 1 1 ± 2.89 1 .69 ± 2.36
Mean plasma creatinine 1 .25 ± 1 .37 1 .32 ± I .72
(mg/db)
as the underlying disease ( I 3, 14). Moreover, persistent pro-
teinunia may make them susceptible to impaired renal function
in the long-term ( 15,16).
The second outcome measure of this trial was the effect of
treatment on renal function, as assessed by the reciprocal of
plasma creatinine over time. In both groups, the mean recip-
rocal of plasma creatinine improved in the 12-mo cohort and
remained stable in either group in the 24- and 36-mo cohorts.
The follow-up period of this study was short, but it has been
shown that following the reciprocal of plasma creatinine even
for a short time may predict the long-term prognosis in patients
with membranous nephropathy ( 1 7). Although these data
should be extrapolated with caution, one may speculate that
these patients should have little risk of developing renal insuf-
ficiency even in the bong-term. This view is reinforced by
previous results showing that patients who attained a complete
remission (1 8) or even partial remission ( I 9) of the ncphrotic
syndrome were unlikely to develop any deterioration of renal
function in the long-term follow-up.
The use of corticosteroids and alkylating agents may expose
these patients to side effects. Several patients had to stop
treatment because of adverse effects. In all cases, patients with
side effects that developed during treatment recovered corn-
pletcly after stopping treatment and adequate management.
The rate of adverse events leading to discontinuation in pa-
ticnts given chborarubucib was 1 2%, similar to the 9.5% (2) and
9% (3) that we observed in two previous controlled trials with
methylprednisobone and chborarubucil. A smaller number of
patients given cycbophospharuide had to stop treatment because
of side effects. Moreover, none of them suffered from herpes

Idiopathic Membranous Nephropathy 449
zoster, which occurred in four patients given chborarubucil. The
main concern with the usc of cytotoxic drugs is the potential
risk of neoplasia in the long-term. Leukemia and, more rarely,
lyruphoma (20,2 1) arc the most frequent types of cancer that
develop in patients given chborambucil, whereas bladder can-
cen and lymphoreticular tumors (22,23) arc the most frequent
malignancies in patients treated with cycbophospharuide. None
of our patients suffered from any of these tumors. It is possible,
however, that alkylating agents may expose them to other
forms of neoplasia. In immunosuppressed patients, the hazard
of neoplasia is roughly related to the cumulative dose and to
the duration of cytotoxic therapy (24-26). Whether short-term
administration of an alkylating agent increases the risk of
cancer in patients with membranous ncphropathy is still un-
clear. The problem is further complicated by the fact that
membranous ncphropathy may be the first clue of an underly-
ing cancer (27,28). Even in this study, two patients were
recognized to have malignancy only after randomization. One
patient received steroids for only a few days, whereas the other
patient did not receive any treatment for ruerubranous nephrop-
athy. On the other hand, we observed one case of prostatic
cancer 5 yr after treatment in the group given chborarubucil and
one case of laryngeal cancer 4 yr after treatment in the group
given cyclophosphamide. To evaluate whether these cancers
represented a chance event or a complication of treatment, we
compared the cumulative risk of cancer in patients given meth-
ylprcdnisobone and chborambucil for 6 mo with that of a
general white population. To increase the number of patients at
risk (in addition to the patients of this study), 79 other patients
treated with steroids and chborambucil who participated to two
previous controlled trials in rucmbranous ncphropathy (3,4)
were considered. Therefore, we were able to collect informa-
tion about 662 patients/years treated with mcthylprcdnisobone
and chborambucil for 6 mo. In this population, we observed
three cases of cancer: one in the present study and two cases in
the two previous controlled studies. Thus, the cumulative risk
of developing cancer in our patients given mcthylprednisobonc
and chbonambucil was 4.53/1000 patients per year (95% CI,
0.935 to 1 3.24 1 ). This hazard is similar to that observed in a
general white population, being the average annual incidence
of primary cancer among white population (4.33/1000 for men
and 3.40/1000 for women) (29). We do not have controlled
data with the usc of cyclophospharuide other than those re-
ported in this trial, clearly too a small number of patients to
draw any conclusion.
In conclusion, this controlled trial confirms that the altenna-
tion of steroids and cytotoxic drugs for 6 mo favors remission
of the nephrotic syndrome and protects from renal dysfunction.
No significant difference could be observed between patients
given chborarubucil or cycbophosphamidc. On the basis of these
results, either of these cytotoxic drugs may be used in mem-
branous ncphnopathy whenever the clinician feels that a par-
ticular patient should be treated.
AcknowledgmentsWe are indebted to the following physicians who participated in
this study: G. Banfi (Ospedale Maggiore Milano), R. Maiorca (Uni-
versity of Brescia), D. Bizzarri (Ospedale Civile Arezzo), and P.
Zucchelli (Ospedale Malpighi Bologna). This work was supported in
part by a grant from Ospedabc Maggiore di Milano.
References1 . Ponticelli C, Zucchelli P, Imbasciati E, Cagnoli L, Pozzi C,
Passerini P, Grassi C, Liruido D, Pasquali S. Volpini T, Sasdelli
M, Locatelli F: Controlled trial of methylprednisolone and
chborarubucil in idiopathic membranous nephropathy. N EngI
J Med 310: 945-950, 1984
2. Ponticelbi C, Zucchelli P. Passerini P, Cagnoli L, Cesana B, Pozzi
C, Pasquali 5, Imbasciati E, Grassi C, Redaelli B, Sasdelli M,
Locatelbi F: A randomized trial of methylprednisolone and
chlorambucil in idiopathic membranous nephropathy. N Engl
J Med 320: 8-13, 1989
3. Ponticelbi C, Zucchelli P. Passerini P. Cesana B, and the Italian
Idiopathic Membranous Nephropathy Treatment Study Group:
Methylprednisolone plus chborambucil as compared with meth-
ylprednisolone alone for the treatment of idiopathic membranous
nephropathy. N Engl J Med 327: 599-603, 1992
4. Ponticelli C, Zucchelli P. Passerini P. Cesana B, Locatelli F,
Pasquali 5, Sasdelli M, Redaelli B, Grassi C, Pozzi C, Bizzarri D,
Banfi G: A 10-year follow-up of a randomized study with meth-
ylprcdnisobone and chlorambucil in membranous nephropathy.
Kidney bnt 48: 1600-1 604, 1995
5. Reichert U, Huysmans FTM, Assman K, Koene RAP, Wetzels
JFM: Preserving renal function in patients with membranousnephropathy: Daily oral chborambucil compared with intermit-
tent monthly pulses of cycbophosphamide. Ann bntern Med I 21:
328-333, 1994
6. Brunkhorst R, Wrenger E, Koch KM: Low-dose prednisobone/
chlorarubucib therapy in patients with severe membranous gb-
merubonephritis. Cli,z bnt’est 72: 277-280, 1994
7. Mathieson PW, Turner AN, Maidment CGH, Evans DI, Rees Al:
Prednisobone and chborambucil treatment in idiopathic membra-
nous nephropathy with deteriorating renal function. Lancet 2:
869-872, 1988
8. Ehrenreich T, Churg I: Pathology of ruerubranous nephropathy.
In: Pathology Annual, edited by Sommers SC, New York, Apple-
ton-Century-Crofts, I 986, pp 145-186
9. Kaplan EL, Meier P: Nonparametnic estimation from incomplete
observations. J Am Stat Assoc 53: 457-481, 1958
10. Kirk RE: Experimental Design: Procedures for the Behavioral
Sciences, 2nd Ed., Monterey, CA, Brooks-Cole, 1982, pp 489-
505
1 1 . Geisser 5, Greenhouse SW: An extension of Box’s results on the
use of the F distribution in multivariate analysis. Ann Math Stat
29: 885-891, 1958
I 2. Ordonez ID, Hiatt RA, Killebrew El, Fireman BH: The increasedrisk of coronary heart disease associated with nephrotic syn-
drorue. Kidney In! 44: 638-642, 1993
13. Bellomo R, Atkins RC: Membranous nephropathy and thrombo-embolism: Is prophylactic anticoagulation warranted? Nephron
63: 249-253, 1993
14. Sarasin FP, Schifferli IA: Prophylactic oral anticoagulation in
nephrotic patients with idiopathic ruembranous nephropathy.
Kidney but 45: 578 -585, 1994
15. Remuzzi G, Bertani T: Is glomerulosclerosis a consequence of
altered gbomerular permeability to macromolecules? Kidney bnt
38: 384-394, 1990
16. Burton C, Harris KPG: The role ofproteinuria in the progression
of chronic renal failure. Am J Kidney Dis 6: 765-77 1 , 1996
450 Journal of the American Society of Nephrology
17. Davison AM, Cameron IS, Kerr DN, Ogg CS, Wilkinson RW: The
natural history of renal function in untreated idiopathic membranousgbomembonephnitis in adults. Cli,i Nephrol 22: 61-67, 1984
18. Passenini P. Pasquali 5, Cesana B, Zucchelli P. Ponticelli C:
Long-term outcome of patients with membranous nephropathy
after complete remission of proteinuria. Nephrol Dial Transplant
4: 525-529, 1989
19. Ponticelli C, Passenini P. Altieri P. Locatelli F, Pappalettera M:Remissions and relapses in idiopathic membranous nephropathy.
Nephrol Dial Transplant 7[Suppl I]: 85-90, 1992
20. Berk PD, Goldberg ID, Silverstein MN, Weinfeld A, Donovan
PB, Ellis IT, Landaw SA, Laszbo I, Najean Y: Increased mci-dence of acute leukemia in polycythemia vera associated withchborambucil therapy. N EngI J Med 304: 441-447, 1981
2 1 . Kahn MF, Arlet I, Bboch-Michel H, Caroit M, Chaouat Y, Renier
IC: Leuc#{233}miesaigues apr#{232}straitement par agents cytotoxiques
en rheumatologie: I 9 observations chez 2006 patients. Nouv
Presse Med 8: 1393-1397, 1979
22. Wall RL, Clausen KP: Carcinoma of the urinary bladder inpatients receiving cycbophosphamide. N EngI J Med 293: 271-
273, 1975
23. Kinlen LI, Sheil AGR, Peto I, Doll R: Collaborative United
Kingdom-Australasian study of cancer in patients treated with
immunosuppressive drugs. Br Med J 2: 1461-1466, 1979
24. Smith AG, Prentice AG, Lucie NP, Browning ID, Dagg IH,
Rowan RM: Acute myelogenous leukemia following cytotoxic
therapy: Five cases and a review. Q J Med 5 1: 227-240, 1982
25. Grunwald HW, Rosner F: Acute leukemia and immunosuppres�
sive drug use. Arch Intern Med 139: 461-466. 1979
26. Baltus JAM, Boersrua 1W, Hartman AP, Vandenbroucke IP: The
occurrence of malignancies in patients with rheumatoid arthritis
treated with cycbophosphamide: A controlled retrospective fol-
low-up. Ann Rheum Dis 42: 368-373, 1983
27. Alpers CE, Cotran RS: Neoplasia and glomerular injury. Kidney
but 30: 465-473, 1986
28. Burstein DM, Korbet SM, Schwartz MM: Membranous gbomer-
ulonephnitis and malignancy. Am J Kidney Dis 22: 5-10, 1993
29. Fraurueni IF, Devasa 55, Hoover RN, Kinlen Li: Epidemiology
of cancer. In: L�ancer Principles 38 Practice of Oncology, 4th
Ed., edited by Devita VT, Hellman 5, Rosenberg SA, Philadel-
phia, I. B. Lippincott, 1993, pp 150-181