A place principle for vertigo - MM3 Admin · A place principle for vertigo Richard R. Gacek*...
10
A place principle for vertigo Richard R. Gacek * Department of Otolaryngology, Head and Neck Surgery, University of Massachusetts Medical School, Worcester, MA 01655, USA Received 16 March 2007; accepted 13 April 2007 Available online 24 October 2007 Abstract Objective: To provide a road map of the vestibular labyrinth and its innervation leading to a place principle for different forms of vertigo. Method: The literature describing the anatomy and physiology of the vestibular system was reviewed. Results: Different forms of vertigo may be determined by the type of sense organ, type of ganglion cell and location in the vestibular nerve. Conclusion: Partial lesions (viral) of the vestibular ganglion are manifested as various forms of vertigo. # 2007 Elsevier Ireland Ltd. All rights reserved. Keywords: Vertigo; Vestibular nerve; Pathology Contents 1. Introduction ................................................................................ 1 2. Sense organ................................................................................. 2 3. Ganglion cells ............................................................................... 4 4. Hair cells .................................................................................. 5 5. Hair cell polarization .......................................................................... 5 6. Efferent vestibular system ....................................................................... 8 7. A place principle for vertigo ..................................................................... 9 8. Conclusion ................................................................................ 10 References ................................................................................ 10 1. Introduction Sensory systems must be highly organized to function effectively. The special senses are especially well developed. This organization exists at the periphery and is duplicated with ascent of the system centrally. The auditory system provides an excellent example of a place principle for hearing. The reception of frequencies in orderly fashion from low at the apex of the cochlea to high at the base is determined by the physical characteristics of the cochlear partition. Components in the cochlear duct (basilar membrane, spiral ligament, support cells in the organ of Corti) determine the place for maximal displacement of this partition by a given traveling wave induced by an auditory stimulus. This orderly transmission of frequencies is preserved over the primary auditory neuron, and multiple central neurons to the cortex for proper integration of auditory messages. Vision and olfaction have a similar precise organization to their neural systems. Sufficient morphologic, physiologic and clinical evi- dence has accumulated in the past few decades to indicate an organization in the vestibular system that may account for different forms of vertigo depending on the location of pathology in the vestibular nerve. The evidence supporting such a ‘‘place principle for vertigo’’ will be reviewed in this www.elsevier.com/locate/anl Auris Nasus Larynx 35 (2008) 1–10 * Tel.: +1 508 856 4162; fax: +1 508 856 6703. E-mail address: [email protected]. 0385-8146/$ – see front matter # 2007 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.anl.2007.04.002
Transcript of A place principle for vertigo - MM3 Admin · A place principle for vertigo Richard R. Gacek*...

www.elsevier.com/locate/anl
Auris Nasus Larynx 35 (2008) 1–10
A place principle for vertigo
Richard R. Gacek *
Department of Otolaryngology, Head and Neck Surgery, University of Massachusetts Medical School,
Worcester, MA 01655, USA
Received 16 March 2007; accepted 13 April 2007
Available online 24 October 2007
Abstract
Objective: To provide a road map of the vestibular labyrinth and its innervation leading to a place principle for different forms of vertigo.
Method: The literature describing the anatomy and physiology of the vestibular system was reviewed.
Results: Different forms of vertigo may be determined by the type of sense organ, type of ganglion cell and location in the vestibular nerve.
Conclusion: Partial lesions (viral) of the vestibular ganglion are manifested as various forms of vertigo.
# 2007 Elsevier Ireland Ltd. All rights reserved.
Keywords: Vertigo; Vestibular nerve; Pathology
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
2. Sense organ. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
3. Ganglion cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
4. Hair cells . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
5. Hair cell polarization . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
6. Efferent vestibular system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
7. A place principle for vertigo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
8. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
1. Introduction
Sensory systems must be highly organized to function
effectively. The special senses are especially well developed.
This organization exists at the periphery and is duplicated
with ascent of the system centrally. The auditory system
provides an excellent example of a place principle for
hearing. The reception of frequencies in orderly fashion
from low at the apex of the cochlea to high at the base is
determined by the physical characteristics of the cochlear
partition. Components in the cochlear duct (basilar
* Tel.: +1 508 856 4162; fax: +1 508 856 6703.
E-mail address: [email protected].
0385-8146/$ – see front matter # 2007 Elsevier Ireland Ltd. All rights reserved
doi:10.1016/j.anl.2007.04.002
membrane, spiral ligament, support cells in the organ of
Corti) determine the place for maximal displacement of this
partition by a given traveling wave induced by an auditory
stimulus. This orderly transmission of frequencies is
preserved over the primary auditory neuron, and multiple
central neurons to the cortex for proper integration of
auditory messages. Vision and olfaction have a similar
precise organization to their neural systems.
Sufficient morphologic, physiologic and clinical evi-
dence has accumulated in the past few decades to indicate an
organization in the vestibular system that may account for
different forms of vertigo depending on the location of
pathology in the vestibular nerve. The evidence supporting
such a ‘‘place principle for vertigo’’ will be reviewed in this
.

R.R. Gacek / Auris Nasus Larynx 35 (2008) 1–102
Fig. 1. Section through the vestibular ganglion and nerve from a patient
with vestibular neuronitis. Arrows point to the numerous bundles of
degenerated axons resulting from degenerated groups of ganglion cells.
Fig. 2. Light microscope photomicrograph of the utricular macula demon-
strates the otoconial blanket (arrow head) resting on the neurosensory
epithelium (arrow). N: utricular nerve.
report. Such a principle might aid our clinical approach to
the evaluation and treatment of vertigo in patients, with
recurrent vertigo. The recurrent vestibulopathies are now
known to be caused by discrete vestibular ganglion cell
lesions, likely viral induced. A significant body of
histopathologic evidence has demonstrated that viral lesions
are limited to discrete clusters of degenerating neurons in the
vestibular ganglion in vestibular neuronitis, Meniere’s
disease and benign paroxysmal positional vertigo (Fig. 1)
[1–3]. This pattern of ganglion cell loss is typical of a viral
neuropathy (4) caused by re-activation of a latent
neurotropic virus (e.g. Zoster) [4]. Because the description
of dizziness by patients may vary (i.e. vertigo, unsteadiness,
positional vertigo), attempts have been made to classify
vestibular disorders according to the nature of the imbalance
symptom. An example of such a knowledge based system is
that of Mira et al. [5]. This system used vertigo and dizziness
to divide a long list of clinical pathologies encountered by
the otologist or neurologist.
The organization of the peripheral vestibular system is
determined largely by two anatomical features. These are:
(1) type of sense organ. (2) Type of ganglion cell.
Fig. 3. Photomicrograph of crista ampullaris and its cupula. Note that the
cupula is attached to the ampullary roof.
2. Sense organ
Of the two types of vestibular sense organs, the otolith
organs are probably the most important in a gravity dependent
environment. They are the oldest phylogenetically with the
canal system making a presence as more mobility (swimming,
walking, running) was acquired. Since the otolith organs
feature a covering membrane containing high specific gravity
(2.71) calcium carbonate particles (otoconia) resting on the
ciliary bundles of the hair cells in the sensory epithelium, they
are in a constant state of stimulation (Fig. 2). The canal
system, on the other hand, is activated by transitory increases
in angular acceleration or deceleration of the fluid (endo-
lymph) within the membranous canal. Such inertial changes
deform the cupular partition of the ampullary enlargement in
the canal resulting in deflection of the ciliary bundles of hair
cells in the sensory epithelium (Fig. 3) [6].
R.R. Gacek / Auris Nasus Larynx 35 (2008) 1–10 3
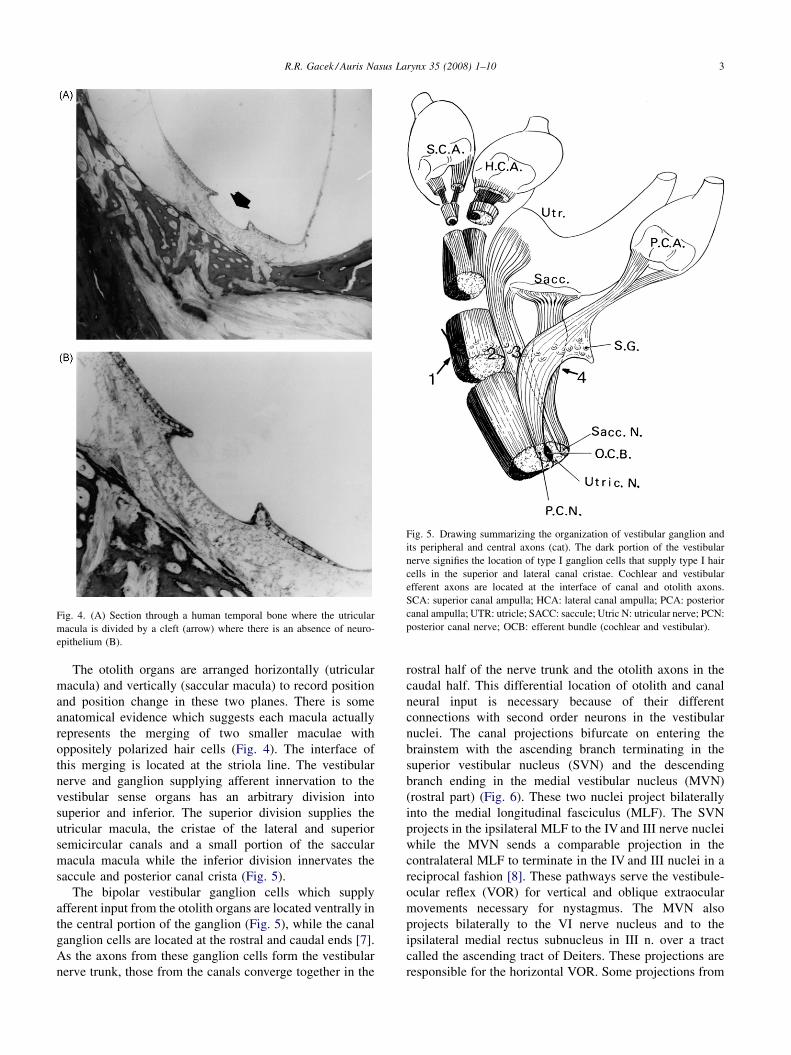
Fig. 4. (A) Section through a human temporal bone where the utricular
macula is divided by a cleft (arrow) where there is an absence of neuro-
epithelium (B).
Fig. 5. Drawing summarizing the organization of vestibular ganglion and
its peripheral and central axons (cat). The dark portion of the vestibular
nerve signifies the location of type I ganglion cells that supply type I hair
cells in the superior and lateral canal cristae. Cochlear and vestibular
efferent axons are located at the interface of canal and otolith axons.
SCA: superior canal ampulla; HCA: lateral canal ampulla; PCA: posterior
canal ampulla; UTR: utricle; SACC: saccule; Utric N: utricular nerve; PCN:
posterior canal nerve; OCB: efferent bundle (cochlear and vestibular).
The otolith organs are arranged horizontally (utricular
macula) and vertically (saccular macula) to record position
and position change in these two planes. There is some
anatomical evidence which suggests each macula actually
represents the merging of two smaller maculae with
oppositely polarized hair cells (Fig. 4). The interface of
this merging is located at the striola line. The vestibular
nerve and ganglion supplying afferent innervation to the
vestibular sense organs has an arbitrary division into
superior and inferior. The superior division supplies the
utricular macula, the cristae of the lateral and superior
semicircular canals and a small portion of the saccular
macula macula while the inferior division innervates the
saccule and posterior canal crista (Fig. 5).
The bipolar vestibular ganglion cells which supply
afferent input from the otolith organs are located ventrally in
the central portion of the ganglion (Fig. 5), while the canal
ganglion cells are located at the rostral and caudal ends [7].
As the axons from these ganglion cells form the vestibular
nerve trunk, those from the canals converge together in the
rostral half of the nerve trunk and the otolith axons in the
caudal half. This differential location of otolith and canal
neural input is necessary because of their different
connections with second order neurons in the vestibular
nuclei. The canal projections bifurcate on entering the
brainstem with the ascending branch terminating in the
superior vestibular nucleus (SVN) and the descending
branch ending in the medial vestibular nucleus (MVN)
(rostral part) (Fig. 6). These two nuclei project bilaterally
into the medial longitudinal fasciculus (MLF). The SVN
projects in the ipsilateral MLF to the IV and III nerve nuclei
while the MVN sends a comparable projection in the
contralateral MLF to terminate in the IV and III nuclei in a
reciprocal fashion [8]. These pathways serve the vestibule-
ocular reflex (VOR) for vertical and oblique extraocular
movements necessary for nystagmus. The MVN also
projects bilaterally to the VI nerve nucleus and to the
ipsilateral medial rectus subnucleus in III n. over a tract
called the ascending tract of Deiters. These projections are
responsible for the horizontal VOR. Some projections from
R.R. Gacek / Auris Nasus Larynx 35 (2008) 1–104
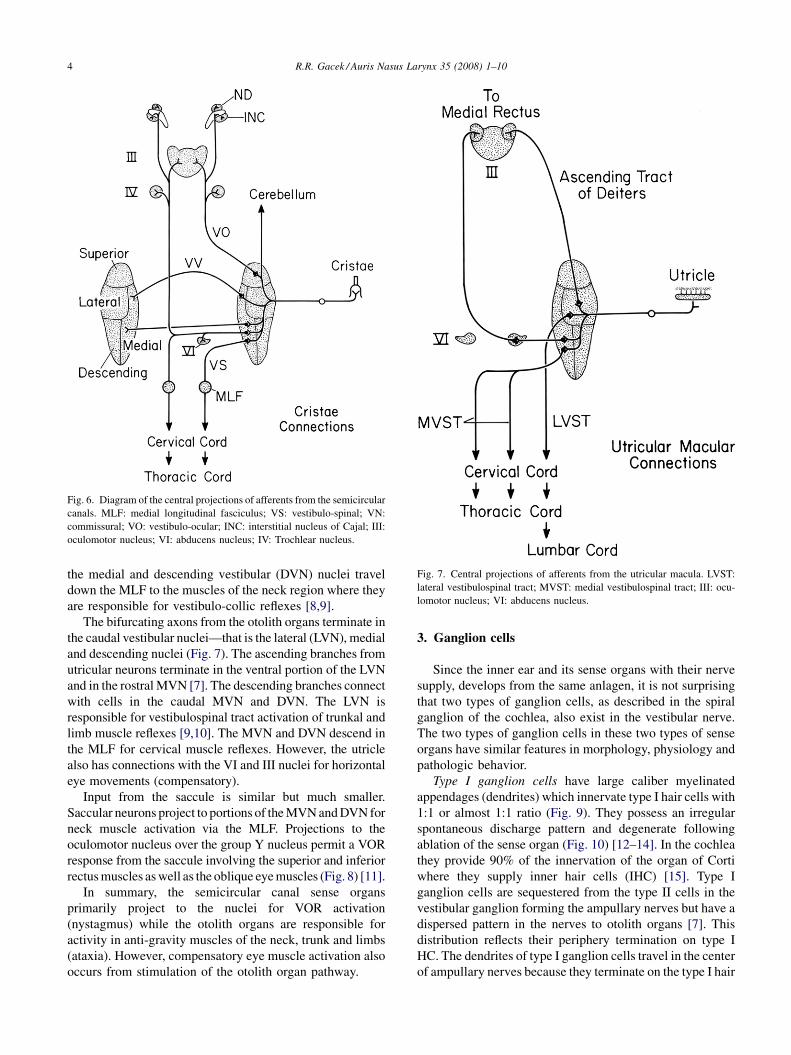
Fig. 6. Diagram of the central projections of afferents from the semicircular
canals. MLF: medial longitudinal fasciculus; VS: vestibulo-spinal; VN:
commissural; VO: vestibulo-ocular; INC: interstitial nucleus of Cajal; III:
oculomotor nucleus; VI: abducens nucleus; IV: Trochlear nucleus.
Fig. 7. Central projections of afferents from the utricular macula. LVST:
lateral vestibulospinal tract; MVST: medial vestibulospinal tract; III: ocu-
lomotor nucleus; VI: abducens nucleus.
the medial and descending vestibular (DVN) nuclei travel
down the MLF to the muscles of the neck region where they
are responsible for vestibulo-collic reflexes [8,9].
The bifurcating axons from the otolith organs terminate in
the caudal vestibular nuclei—that is the lateral (LVN), medial
and descending nuclei (Fig. 7). The ascending branches from
utricular neurons terminate in the ventral portion of the LVN
and in the rostral MVN [7]. The descending branches connect
with cells in the caudal MVN and DVN. The LVN is
responsible for vestibulospinal tract activation of trunkal and
limb muscle reflexes [9,10]. The MVN and DVN descend in
the MLF for cervical muscle reflexes. However, the utricle
also has connections with the VI and III nuclei for horizontal
eye movements (compensatory).
Input from the saccule is similar but much smaller.
Saccular neurons project to portions of the MVN and DVN for
neck muscle activation via the MLF. Projections to the
oculomotor nucleus over the group Y nucleus permit a VOR
response from the saccule involving the superior and inferior
rectus muscles as well as the oblique eye muscles (Fig. 8) [11].
In summary, the semicircular canal sense organs
primarily project to the nuclei for VOR activation
(nystagmus) while the otolith organs are responsible for
activity in anti-gravity muscles of the neck, trunk and limbs
(ataxia). However, compensatory eye muscle activation also
occurs from stimulation of the otolith organ pathway.
3. Ganglion cells
Since the inner ear and its sense organs with their nerve
supply, develops from the same anlagen, it is not surprising
that two types of ganglion cells, as described in the spiral
ganglion of the cochlea, also exist in the vestibular nerve.
The two types of ganglion cells in these two types of sense
organs have similar features in morphology, physiology and
pathologic behavior.
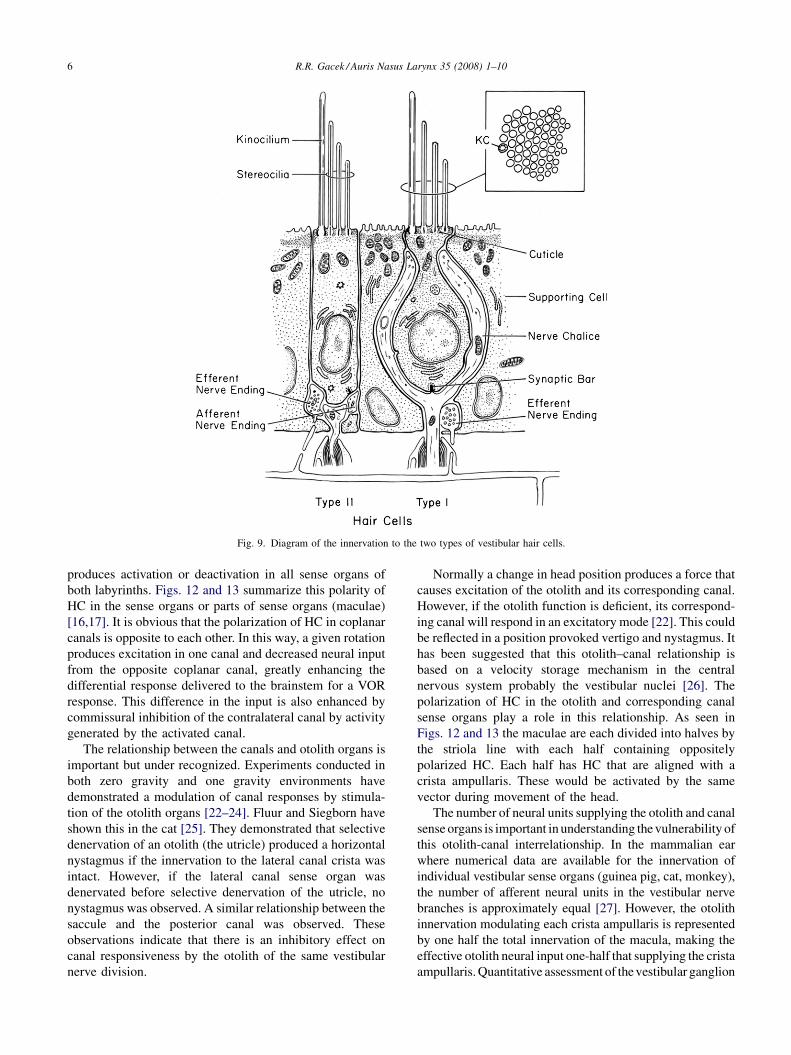
Type I ganglion cells have large caliber myelinated
appendages (dendrites) which innervate type I hair cells with
1:1 or almost 1:1 ratio (Fig. 9). They possess an irregular
spontaneous discharge pattern and degenerate following
ablation of the sense organ (Fig. 10) [12–14]. In the cochlea
they provide 90% of the innervation of the organ of Corti
where they supply inner hair cells (IHC) [15]. Type I
ganglion cells are sequestered from the type II cells in the
vestibular ganglion forming the ampullary nerves but have a
dispersed pattern in the nerves to otolith organs [7]. This
distribution reflects their periphery termination on type I
HC. The dendrites of type I ganglion cells travel in the center
of ampullary nerves because they terminate on the type I hair

R.R. Gacek / Auris Nasus Larynx 35 (2008) 1–10 5
Fig. 8. Central projections from the saccular macula. IFC: infracerebellar
nucleus; Y: group Y nucleus; LVST: lateral vestibulospinal tract; MVST:
medial vestibulospinal tract; MLF: medial longitudinal fasciculus; III:
oculomotor nucleus.
cells which are concentrated at the crest of the crista
ampullaris [16,17]. These hair cells are positioned to be most
sensitive to cupular displacement.
The central projection of type I ganglion cells is to
vestibulo-ocular neurons in the SVN and MVN via axo-
somatic synapses (Fig. 11) [18]. Thus the type I hair cell –
type I ganglion cell – vestibulo-ocular neuron in the
vestibular nuclei (SVN, MVN) is responsible for the VOR
responses associated with stimulation or degeneration of the
cristae ampullaris. In the otolith system these type I ganglion
cells project to large multipolar neurons of the vestibulosp-
inal tracts as well as to vestibulo-ocular neurons in the
caudal vestibular nuclei.
Type II ganglion cells have small caliber myelinated
dendrites which, innervate type II hair cells in a diffuse
manner [16,17] (i.e. many HC supplied by a single fiber)
(Fig. 9), and demonstrate a regular spontaneous discharge
pattern [12,13,19]. They do not degenerate after end organ
ablation (Fig. 10) [18]. The type II hair cells located along
the slopes of the crista ampullaris are not in a position to
optimally respond to cupular displacement but may have a
supporting role in end organ sensitivity by virtue of their rich
efferent innervation.
Because the lateral canal sense organ is a recent
phylogenetic development, making an appearance in
amphibians (frog), the type I and II ganglion cell populations
are separated in the superior division ganglion [7,20]. The
type I ganglion cells are concentrated at the most rostral end
of the ganglion while type II cells occupy the caudal region
of the superior division ganglion (Fig. 5). The dendrites of
type II ganglion cells envelop those of type I ganglion cells
as the ampullary nerves are formed. This separate location of
type I and II ganglion cells in the superior vestibular division
has been confirmed in the monkey and human vestibular
nerve [20] and provides an opportunity for a differential
functional response from injury to either of these two types
of neurons.
4. Hair cells
The two types of hair cells (HC) in the vestibular organs
are somewhat similar to the inner (HC) and outer hair (OHC)
cells in the organ of corti. The type I HC in the vestibular
organs (i.e. crista) are innervated by type I vestibular
ganglion cells with the same irregular spontaneous electrical
activity as the type I spiral ganglion cells which innervate the
IHC in the organ of corti [15,16]. In both systems they are
responsible for the major afferent input to the brain for
balance and hearing.
The type II vestibular hair cells may play an enhancing
role in the sensitivity of balance organs similar to the role
that OHC impose on the IHC and auditory sensitivity. The
contractile properties of OHC allow a change in the cochlear
amplifier effect in the organ of corti [21]. This contractile
function of the OHC is under efferent neural control and
serves to enhance the sensitivity of auditory neurons (type I).
5. Hair cell polarization
In addition to the different functionalities of two types of
HC (with their innervation) in the vestibular system, an
important feature of vestibular hair cells is their alignment
within an individual sense organ and the relationship of this
orientation to that of other sense organs in the labyrinth
[16,17]. This is referred to as the ‘‘polarization of hair cells’’
in the labyrinth.
In contrast to cochlear hair cells vestibular HC have a
ciliary bundle comprised of 70–100+ stereocilia and one
longer Kinocilium [16,17]. This Kinocilium is located at the
end of the ciliary bundle where the longest sterocilia are
located. The significance of this arrangement is that when
the cilia are deflected toward the kinocilium there is
depolarization of the HC and an increase in the afferent
neural unit activity while deflection away from the
kinocilium results in hyper-polarization and a decrease in
neural activity [16]. This has great functional significance
and accounts for the different responses obtained by testing
individual canals by warm and cool caloric stimulation.
An equally important consideration, however, is the
relationship of this polarity of HC between the five sense
organs of the labyrinth. Any movement of the body and head
R.R. Gacek / Auris Nasus Larynx 35 (2008) 1–106
Fig. 9. Diagram of the innervation to the two types of vestibular hair cells.
produces activation or deactivation in all sense organs of
both labyrinths. Figs. 12 and 13 summarize this polarity of
HC in the sense organs or parts of sense organs (maculae)
[16,17]. It is obvious that the polarization of HC in coplanar
canals is opposite to each other. In this way, a given rotation
produces excitation in one canal and decreased neural input
from the opposite coplanar canal, greatly enhancing the
differential response delivered to the brainstem for a VOR
response. This difference in the input is also enhanced by
commissural inhibition of the contralateral canal by activity
generated by the activated canal.
The relationship between the canals and otolith organs is
important but under recognized. Experiments conducted in
both zero gravity and one gravity environments have
demonstrated a modulation of canal responses by stimula-
tion of the otolith organs [22–24]. Fluur and Siegborn have
shown this in the cat [25]. They demonstrated that selective
denervation of an otolith (the utricle) produced a horizontal
nystagmus if the innervation to the lateral canal crista was
intact. However, if the lateral canal sense organ was
denervated before selective denervation of the utricle, no
nystagmus was observed. A similar relationship between the
saccule and the posterior canal was observed. These
observations indicate that there is an inhibitory effect on
canal responsiveness by the otolith of the same vestibular
nerve division.
Normally a change in head position produces a force that
causes excitation of the otolith and its corresponding canal.
However, if the otolith function is deficient, its correspond-
ing canal will respond in an excitatory mode [22]. This could
be reflected in a position provoked vertigo and nystagmus. It
has been suggested that this otolith–canal relationship is
based on a velocity storage mechanism in the central
nervous system probably the vestibular nuclei [26]. The
polarization of HC in the otolith and corresponding canal
sense organs play a role in this relationship. As seen in
Figs. 12 and 13 the maculae are each divided into halves by
the striola line with each half containing oppositely
polarized HC. Each half has HC that are aligned with a
crista ampullaris. These would be activated by the same
vector during movement of the head.
The number of neural units supplying the otolith and canal
sense organs is important in understanding the vulnerability of
this otolith-canal interrelationship. In the mammalian ear
where numerical data are available for the innervation of
individual vestibular sense organs (guinea pig, cat, monkey),
the number of afferent neural units in the vestibular nerve
branches is approximately equal [27]. However, the otolith
innervation modulating each crista ampullaris is represented
by one half the total innervation of the macula, making the
effective otolith neural input one-half that supplying the crista
ampullaris. Quantitative assessment of the vestibular ganglion

R.R. Gacek / Auris Nasus Larynx 35 (2008) 1–10 7
Fig. 10. Photomicrograph of the rostral part of the superior division axons
in the cat. (A) Normal vestibular nerve demonstrates the high concentration
of large diameter axons (type I ganglion cells). (B) Six months after
labyrinthectomy the large axons have degenerated.
Fig. 11. Diagram of the central projections of types I and II hair cells and
ganglion cells in the cristae.
Fig. 12. View of the human vestibular nerve branches and sense organs
demonstrating the polarization of hair cells in the cristae and utricular
macula supplied by the superior division. F: facial nerve; V: vestibular
nerve; S: saccular macula; U: utricular macula; PC: posterior canal crista;
LC: lateral canal crista; SC: superior canal crista.
of TB from patients with BPPV have shown a greater than
50% loss of ganglion cells in both vestibular divisions [28]. A
loss of this magnitude in afferent units already a fraction of
those to the crista ampullaris is likely to cause a disruption in
the otolith-canal relationship resulting in BPPV.
This neuropathologic explanation may account for the
various categories of BPPV. Posterior canal BPPV is by far
the most common possibly because the saccular nerve is the
smallest in all species studied [27]. Thus it represents the
greatest mismatch between otolith and canal innervation and
most likely to lose its inhibitory effect on posterior canal
Fig. 13. Posterior view of the specimen in Fig 12 shows the polarization of
hair cells in the saccular macula and posterior canal crista (PC).

R.R. Gacek / Auris Nasus Larynx 35 (2008) 1–108
excitation. Lateral canal and anterior canal BPPV are less
commonly recognized because of a smaller mismatch
between otolith and canal innervation.
Fig. 15. Transverse section of the vestibular (V) and cochlear (C) nerves in
the cat shows the efferent labyrinthine pathway (arrow) in the center of the
vestibular nerve. Acetylcholinesterase preparation. F: facial nerve.
6. Efferent vestibular system
The final form of vestibular injury which may present as
dysequilibrium relates to the efferent vestibular pathway.
The vestibular efferent pathway originates bilaterally in the
MVN just lateral to the abducens nucleus [29]. Axons of
these neurons [30] merge with and travel with the efferent
cochlear pathway (olivo-cochlear pathway) in the vestibular
nerve as it exits the brainstem (Fig. 14) [31]. This common
efferent bundle is clearly demonstrated by the high aceteyl
cholinesterase activity which suggests acetycholine as its
neurotransmitter agent (Fig. 15) [32]. This efferent bundle
passes through the saccular portion of the vestibular
ganglion and, therefore, may be affected (loss of function)
by inflammatory lesions in this area (Fig. 16). Individual
efferent axons ramify as they travel in a dispersed
arrangement to the sense organs (Fig. 17). This branching
pattern permits a rich efferent termination on HC in the sense
organ neuroepithelium.
Although an inhibitory effect is associated with stimula-
tion of the vestibular efferent pathway [33–35], the function
of this neural system in balance has not been demonstrated.
However, certain established facts on efferent systems
permit speculation on the role that the efferent system may
play in balance.
Fig. 14. Diagram of the efferent vestibular pathway (solid lines); stippled area =
vestibular nucleus; DCN: dorsal ventral cochlear nuclei; VCN: ventral cochlear
superior olivary nucleus; LSO: lateral superior olivary nucleus.
The role of the efferent cochlear pathway has been shown
to be one of modifying the physical characteristics of the
sense organ to enhance sensitivity for stimulation of the
primary auditory unit. By activating the contractile potential
of the OHC to lengthen or shorten thus adjusting the reticular
lamina and the tectorial membrane to sharpen the tuning
curves for the primary auditory units (IHC and type I spiral
ganglion cells) [21]. Otoacoustic emissions (OAE) gener-
ated by this ‘‘cochlear amplifier’’ [36] have been shown to be
efferent cochlear pathway. LVN: lateral vestibular nucleus; MVN: medial
nuclei; VII: genu of facial nerve; VI: abducens nucleus; ASO: accessory

R.R. Gacek / Auris Nasus Larynx 35 (2008) 1–10 9
Fig. 16. This section through the same specimen as Fig. 15 shows the
efferent cochlear pathway (OC) leaves the saccular nerve while vestibular
efferents have entered the vestibular nerve branches.
inhibited by the activity of the crossed (efferent) olivo-
cochlear pathway.
Efferent vestibular activity in lower forms (fish) has been
shown to be increased before vigorous movement (swim-
ming) which would over stimulate the organ of balance
(lateral line) [37–39]. Presumably this efferent activation is
intended to reduce (prevent) self-stimulation by the animals
activity.
This a role is compatible with the numerous demonstra-
tions of inhibition of afferent neural transmission following
stimulation of the vestibular efferent system [33,34]. Such a
system may play a role in preventing auto stimulation of
vestibular sense organs during physical activity.
A suggested corollary in the vestibular system would be
for the efferent pathway to prevent auto-stimulation of sense
organs by mechanically changing the sensitivity of the sense
Fig. 17. The vestibular efferent axons (arrows) are spread throughout the
afferent fibers before reaching the sense organ epithelium.
organs by altering the covering membrane (cupula,
otoconial blanket) during vigorous physical activity. The
clinical syndrome that could result from dysfunction of the
efferent vestibular system might be motion sickness. A
particularly efficient efferent system would be a requirement
for a gymnast or figure skater.
7. A place principle for vertigo
This anatomical organization (supported by physiologi-
cal correlates) provides a basis for attributing various forms
of vertigo to pathology in discrete part of the vestibular
ganglion. There is increasing pathologic evidence that the
recurrent vestibulopathies (ventricular neuronitis, Meniere’s
disease, benign paroxysmal positional vertigo) are caused by
discrete ganglion injury (degeneration) from reactivation of
neurotropic viruses (herpes virinae family) [1–3]. The
severity and form of dysequilibrium described by such
patients will depend on the location and number of
vestibular ganglion cells injured by virus [40]. The location
of sites in the vestibular ganglion responsible for different
forms of vertigo are represented by the numbers 1–5 in
Fig. 5.
1. L
esions in the most rostral part of the vestibular ganglion(type I GC) are responsible for episodes of rotatory
vertigo. A strong VOR disturbance (nystagmus) signals
this form of vertigo.
2. I
f the ganglion cell lesion is located immediately caudalto this rostral pole of the superior division type II GC are
affected. Unsteadiness, especially on head movement,
will be experienced because these type II GC project to
commissural pathways.
3. D
egeneration of ganglion cells in ventral parts of boththe superior (utricle) and inferior (saccule) divisions of
the vestibular ganglion, causes loss of function in the
vestibulospinal tract to neck, trunk and limb muscles.
Frequently these are described by patients as ‘‘drop’’
attacks. Ataxia may be a lingering form of this form of
dysequilibrium.
4. T
he most common form of vertigo encountered inpractice is position induced. Short duration episodes of a
rotatory vertigo which is fatiquable have been described
since Barany [41]. Both Barany [41] and Citron and
Hallpike [42] felt this was an otolith disorder but the
nystagmus response observed in this syndrome prevented
acceptance of an otolith cause. Hallpike’s description of
utricular degeneration [42] in the TB of BPPV was not
enough to neutralize the predominant support of a canal
etiology. Although the clinical response is a rotatory form
of vertigo, the uninhibited response is caused by loss of
the inhibitory role of the otolith organs.
5. L
esions in the saccular portion of the vestibular ganglion(inferior vestibular) may secondarily interrupt the
efferent pathways to the cochlear and vestibular sense

R.R. Gacek / Auris Nasus Larynx 35 (2008) 1–1010
organs. Clinically, the loss of this control may be
perceived as tinnitus and mot’on sickness.
8. Conclusion
This review is an attempt to provide a guide to
pathologies involving portions of the peripheral vestibular
pathway. It is unusual that only a specific location of
pathology will be present in a given patient. More often, a
mixture of locations will be present. However, the goal here
is to establish a map or framework to guide the evaluation
and management of patients with recurrent vestibulopathy.
References
[1] Gacek RR. The pathology of facial and vestibular neuronitis. Am J
Otolaryngol 1999;20:202–10.
[2] Gacek RR, Gacek MR. Meniere’s disease as a manifestation of
vestibular ganglionitis. Am J Otolaryngol 2001;22:241–50.
[3] Gacek RR, Gacek M. The three faces of vestibular ganglionitis. Ann
Otol Rhinol Laryngol 2002;111:103–14.
[4] Denny-Brown D, Adams RD, Fitzgerald PJ. Pathologic features of
herpes zoster: a note on geniculate herpes. Arch Neurol Psychiatry
1944;51:216–31.
[5] Mira E, Schmid R, Zanocco P, Buizza A, Magenes G, Maufrin M. A
computer-based consultation system for the classification and diag-
nosis of dizziness.. In: Pirodda E, editor. Clinical Testing of the
Vestibular System Adv Oto-Rhino-Laryng, vol. 42. Basel: Karger;
1988. p. 77–80.
[6] McLaren JW, Hillman DE. Displacement of the semicircular canal
cupula during sinusoidal rotation. Neurosci Abstr 1977;3:544.
[7] Gacek RR. The course and central termination of first order neurons
supplying vestibular end organs in the cat. Acta Otolaryngol
1969;253(Suppl):1–66.
[8] Gacek RR. Anatomical demonstration of the vestibulo-ocular projec-
tions in the cat. Acta Otolaryngol 1971;293(Suppl):1–63.
[9] Brodal A. Anatomy of the vestibular nuclei and their connections. In:
Kornhuber HH, editor. Handbook of Sensory Physiology Vestibular
System, vol. VI. New York: Springer-Verlag; 1974. p. 239–352.
[10] Pompeiano I, Brodal A. The origin of vestibulo-spinal fibers in the cat.
An experimental-anatomical study, with comments on the descending
medial longitudinal fasciculus. Arch Ital Biol 1957;95:166–95.
[11] Gacek R. Location of trochlear vestibulo-ocular neurons in the cat.
Exp Neurol 1979;66:692–706.
[12] Fernandez C, Goldberg JM. Physiology of peripheral neurons inner-
vating semicircular canals of the squirrel monkey. II. Response to
sinusoidal stimulation and dynamics of peripheral vestibular system. J
Neurophysiol 1971;34:661–75.
[13] Goldberg JM, Fernandez C. Physiology of peripheral neurons inner-
vating semicircular canals of the squirrel monkey. I. Resting discharge
and response to constant angular accelerations. J Neurophysiol
1971;34:635–60.
[14] Schunknecht HF. Behavior of the vestibular nerve following labyr-
inthectomy. Ann Otol Rhinol Laryngol Suppl 1997;91:16–32.
[15] Spoendlin HH. The innervation of the cochlear receptor. In: Moller
AR, editor. Basic Mechanisms in Hearing. New York: Academic
Press; 1973. p. 185–234.
[16] Spoendlin HH. The ultrastructure of the vestibular sense organ. In:
Wolfson RJ, editor. The Vestibular System and its Diseases. Phila-
delphia: University of Pennsylvania Press; 1966. p. 39–68.
[17] Lindeman HH. Studies on the morphology of the sensory regions of
the vestibular apparatus. Ergeb Anat Entw Gesch 1970;42:1–113.
[18] Gacek RR, Schoonmaker J. Morphologic changes in the vestibular
nerves and nuclei after labyrinthectomy in the cat: a case for the
neurotrophin hypothesis in vestibular compensation. Acta Otolaryngol
(Stockh) 1997;1(17):244–9.
[19] Walsh BT, Miller JB, Gacek RR, Kiang NYS. Spontaneous activity in
the eighth cranial nerve of the cat. Int J Neurosci 1972;3:221–36.
[20] Honrubia V, Kuruvilla A, Mamikunian D, Eichel J. Morphological
aspects of the vestibular nerve of the squirrel monkey. Laryngoscope
1987;97:228–38.
[21] Brownell WE. Outer hair cell electromotility and otoacoustic emis-
sions. Ear Hear 1990;11:82–92.
[22] Benson A. Modification of the response to angular accelerations by
linear accelerations. In: Kornhuber H, editor. Handbook of sensory
physiology Part 2, vol. 6. Berlin: Springer Verlag; 1974. p. 281–320.
[23] Clarke AH, Scherer H. Calorictesting of the vestibular function during
orbital flight Adv Oto-Rhino-Laryng, vol. 41. Basel: Karger; 1988. p.
31–5.
[24] Clement G, Berthoz A. Vestibulo-ocular reflex and optokinetic nys-
tagmus in microgravity Adv Oto-Rhino-Laryng, vol. 42. Basal: Kar-
ger; 1988. p. 1–4.
[25] Fluur E, Siegborn J. The otolith organs and the nystagmus problem.
Acta Otolaryngol (Stockh) 1973;76:438–42.
[26] Curthoys IS, Markham CH. Convergence of labyrinthine influences on
units in the vestibular nuclei of the cat. I. Natural stimulation. Brain
Res 1971;35:469–90.
[27] Gacek R, Rasmussen G. Fiber analysis of the statoacoustic nerve of
guinea pig, cat and monkey. Anat Rec 1961;139:455–63.
[28] Gacek RR. Pathology of benign paroxysmal positional vertigo revis-
ited. Ann Otol Rhinol Laryngol 2003;112:574–82.
[29] Gacek R, Lyon M. The localization of vestibular efferent neurons in the
kitten using horseradish peroxidase. Acta Otolaryngol 1974;77:92–101.
[30] Gacek R. Efferent component of the vetibularnerve. In: Rasmussen
GL, Windle WF, editors. Neural mechanisms of the auditory and
vestibular systems. Springfield, Ill: Charles C. Thomas; 1960.
[31] Rasmussen GL. The olivary peduncle and other fiber projections of the
superior olivary complex. J Comp Neurol 1946;84:141–220.
[32] Gacek RR, Nomura Y, Balogh K. Acetylcholinesterase activity in the
efferent fibers of the stato-acoustic nerve. Acta Otolaryngol 1965;59:
541–53.
[33] Sala O. The efferent vestibular system. Electrophysiol Res Acta
Otolaryngol 1965;197(Suppl.):1–34.
[34] Schmidt RS. Frog labyrinthine efferent impulses. Acta Otolaryngol
1965;56:51–64.
[35] Gribenski A, Caston J. Tonic influence of the efferent vestibular
system on the spontaneous afferent activity from semicircular canals
in the frog. Exp Brain Res 1976;26:275–83.
[36] Kemp DT. Stimulated acoustic emissions from within the human
auditory system. J Acoust Soc Am 1978;64:1386–91.
[37] Russell IJ, Robert BL. Inhibition of spontaneous lateral line activity by
efferent nerve stimulation. J Exp Biol 1972;57:77–82.
[38] Flock A, Russell IJ. The post-synaptic action of efferent fibers in the
lateral line organ of the burbot lota lota. J Physiol 1973;235:591–605.
[39] Flock A, Russell IJ. Inhibition by efferent nerve fibers: action on hair
cells and afferent synaptic transmission in the lateral line canal organ
of the burbot lota lota. J Physiol 1976;257:45–62.
[40] Meier JL, Straus SE. Comparative biology of latent varicella-zoster
virus and herpes simplex virus infections. J Infect Dis 1992;166(Sup-
ple):S13–23.
[41] Barany R. Diagnose von Krankheit sercheinangen im Bereiche des
Otolithen apparatus. Acta Otolaryngol (Stockh) 1921;2:434–7.
[42] Citron L, Hallpike CS. Observations upon the mechanism of positional
nystagmus of the so-called ‘‘benign paroxysmal positional type’’. J
Laryngol Otol 1956;70:253–9.