A Pilot Study of Continuous Limited-Channel aEEG in Term Infants with Encephalopathy
8
Click here to load reader
-
Upload
russell-lawrence -
Category
Documents
-
view
221 -
download
3
Transcript of A Pilot Study of Continuous Limited-Channel aEEG in Term Infants with Encephalopathy

O(
Sfatr
Rs(sb
Cc
SpnRt
riAwAct
bso
a2
BEa
A Pilot Study of Continuous Limited-Channel aEEG in Term Infantswith Encephalopathy
RUSSELL LAWRENCE, MD, AMIT MATHUR, MD, SYLVIE NGUYEN THE TICH, MD, JOHN ZEMPEL, MD, PHD, AND TERRIE INDER, MD
bjective To evaluate the accuracy, feasibility, and impact of limited-channel amplitude integrated electroencephalogramaEEG) monitoring in encephalopathic infants.
tudy design Encephalopathic infants were placed on limited-channel aEEG with a software-based seizure event detectoror 72 hours. A 12-hour epoch of conventional EEG-video (cEEG) was simultaneously collected. Infants were randomlyssigned to monitoring that was blinded or visible to the clinical team. If a seizure detection event occurred in the visible group,he clinical team interpreted whether the event was a seizure, based on review of the limited-channel aEEG. EEG data wereeviewed independently offline.
esults In more than 68 hours per infant of limited-channel aEEG monitoring, 1116 seizures occurred (>90% clinicallyilent), with 615 detected by the seizure event detector (55%). Detection improved with increasing duration of seizures73% >30 seconds, 87% >60 seconds). Bedside physicians were able to accurately use this algorithm to differentiate trueeizures from false-positives. The visible group had a 52% reduction in seizure burden (P � .114) compared with thelinded group.
onclusions Monitoring for seizures with limited-channel aEEG can be accurately interpreted, compares favorably withEEG, and is associated with a trend toward reduced seizure burden. (J Pediatr 2009;154:835-41)
eizures are more prevalent during the neonatal period than at any other time in life, with an incidence of 1 to 3.5 per 1000live births.1,2 Term infants with seizures have very poor outcomes, with 20% dying in the neonatal period and survivorshaving a 28% to 35% risk for severe neurodevelopmental disability and 20% to 50% risk for epilepsy.3-7 This condition
oses additional challenges due to limitations in accurate clinical diagnosis. More than half of electrographic (EEG) seizures inewborn infants have no clinical correlate, and the majority of those with clinical correlates are missed at the bedside.8,9
ecognition of the presence and extent of seizure burden in these high-risk infants may be critical, as there is growing evidencehat seizures in the newborn may be harmful.10-13
Conventional EEG (cEEG) with greater than 10 electrodes and concurrent videoecording is the gold standard for the detection of seizures. However, cEEG is laborntensive to both set up and interpret, and the interpretation is rarely available in real time.s an alternative, many NICU centers have adopted amplitude integrated EEG (aEEG)ith the goal of identifying and more aggressively treating electrographic seizures.lthough some have questioned the accuracy of aEEG alone in detecting seizures,
ombining the unprocessed signal of limited-channel EEG to the aEEG has the potentialo detect close to 80% of seizures detected by cEEG.14-18
The aim of this study was to evaluate the feasibility and impact of continuousedside limited-channel aEEG monitoring in the NICU setting. Our hypothesis was thatuch monitoring could be accurately utilized by NICU clinicians and that the treatmentf EEG seizures using these devices would improve outcomes.
METHODSIn this prospective, randomized pilot trial, families of infants �36 weeks’ gestation
dmitted to St Louis Children’s Hospital between the dates of March 2007 to March008 who met any of the following criteria were approached: (1) Neonatal encephalopathy
E Base excessEG Electroencephalogram
cEEG Conventional electroencephalogramHIE Hypoxic ischemic encephalopathy
From the Department of Pediatrics (R.L.,A.M., J.Z., T.I.) and Department of Neurol-ogy (J.Z., T.I.), Washington University, StLouis, MO; and Service de Pediatrie (S.T.),University Hospital, Angers, France.
Cure Kids Foundation provided financialsupport of this project. The monitors wereprovided by BrainZ Instruments, Ltd, Auck-land, New Zealand, which had no role inany part of the study plan, data collection,processing, or interpretation of this data orthe preparation of this manuscript.
Submitted for publication Jul 3, 2008; lastrevision received Dec 30, 2008; acceptedJan 5, 2009.
Reprint requests: Dr Russell Lawrence, De-partment of Pediatrics, St Louis Children’sHospital, Washington University, One Chil-dren’s Place, St Louis, MO 63110. E-mail:[email protected].
0022-3476/$ - see front matter
Copyright © 2009 Mosby Inc. All rightsreserved.
EEG Amplitude-integrated electroencephalogram
10.1016/j.jpeds.2009.01.002835

(c(am
icWfwif
ssTBlilcfohEciumlewT1edulr7
ciNpeov
atwmgr
bcsEpsncapewscitwasrandu
icrtsstlreEtacgomwtboFwpiBa
S
8
defined by modified Sarnat I-III) including suspected oronfirmed clinical seizure event; (2) pH �7 or base excessBE) �12 by cord gas or within 1 hour of life; (3) Apgar �5t 5 minutes of life; and (4) severe clinical course requiringuscle relaxation for �4 hours.
Any infant suspected of having a congenital abnormal-ty of the central nervous system was excluded. The ethicsommittee at St Louis Children’s Hospital and the HRPO of
ashington University approved this study. Written in-ormed parental consent was obtained for all patients. Thereere no limitations for enrollment from the time of birth and
nfants could be either inborn or transported from an outsideacility.
Once enrolled, patients were randomly assigned byealed envelope into 1 of 2 different groups; either a blindedeizure group (blinded) or a monitored seizure group (visible).he infants were placed on limited-channel aEEG (BRM 3,rainZ Instruments, Auckland, New Zealand) for a goal of at
east 72 hours. Patients treated with hypothermia were mon-tored through rewarming. For the purposes of this study,imited-channel aEEG refers to the combined informationollected from both the unprocessed EEG signal collectedrom limited EEG channels (2 channels placed bilaterallyver the central-parietal regions of C3-P3 and C4-P4 usingydrogel electrodes) and the condensed-amplitude integratedEG (aEEG) processed from these 2 channels. Simultaneous
onventional EEG with video (cEEG) was collected, if clin-cally feasible, for up to 12 hours using a split lead set up,sually within the first 24 hours of limited-channel aEEGonitoring. Conventional EEG with video was done (Stel-
ate; Montreal, Quebec, Canada) with 17 standard gold disklectrodes using the 10-20 international system. Electrodesere placed at the following locations: FP1, FP2, F3, Fz, F4,7, C4, CZ, C3, T8, P7, P3, Pz, P4, P8, O1, O2, along withground electrode, 1 chin EMG electrode, bilateral eye
lectrodes, 1 respiratory electrode, and 1 standard electrocar-iographic electrode. The C3, P3, C4, P4 electrodes were alsosed for the limited-channel aEEG monitoring through spliteads with limited-channel aEEG and cEEG traces beingecorded simultaneously. Patients had MRI imaging betweenand 10 days of life if clinically stable.
In the blinded group, limited-channel EEG was re-orded but blinded to the clinical team with only the electrodempedance values visible to ensure adequate data collection.
urses annotated all care-giving activities such as feeding oratting on the monitor along with suspected clinical seizurevents. Blinded patients were treated for their seizures basednly on clinical observation and a 1-hour cEEG withoutideo as standard practice in our NICU.
In the visible group, data from the limited-channelEEG monitor was available for interpretation by the clinicaleam. Each limited-channel aEEG monitor was equippedith seizure detection software (RecogniZe, BrainZ Instru-ents, Ltd) to alert bedside caregivers to potential electro-
raphic seizures.19 This detector was tested previously with
etrospective cEEG data without video with favorable results (36 Lawrence et al
ut had not been evaluated prospectively with a limited-hannel aEEG device. When activated, the seizure detectionoftware placed a gold bar over the segment of suspectedEG seizure (Figure 1). Nurses were instructed to notify ahysician (fellow or attending level) if the seizure detectionoftware triggered a seizure detection event. In addition,urses were asked to mark all care events, feeds, and suspectedlinical seizure events by annotating on the limited-channelEEG monitor. When notified of a seizure detection event,hysicians evaluated the infant, the limited-channel unproc-ssed EEG signal, and the aEEG tracing and then decidedhether or not the seizure detection event was in fact a true
eizure event. These evaluations along with the subsequentlinical decision were documented at the bedside on standard-zed study recording sheets. Physicians received informalraining prior to and during the study on EEG interpretationith the limited-channel aEEG monitors. Clinical decisions
bout the timing and nature of pharmacological therapy foreizures were left to the discretion of the clinical team. Theoutine antiseizure medication regimen was phenobarbital asfirst-line treatment (up to 40 mg/kg), followed by fosphe-ytoin (20 mg phenytoin equivalents/kg) and then a benzo-iazepine (midazolam 0.1 mg/kg bolus followed by a contin-ous infusion).
Seizures were defined as EEG waveforms, which evolven frequency, amplitude, or morphology occurring in eithererebral hemisphere for �10 seconds. Seizure duration wasecorded in seconds, based on the limited-channel aEEG datao estimate the total seizure burden for a given patient (theummation of all the seizures in seconds). A cessation ineizure activity of �10 seconds qualified a subsequent epilep-ic event as a distinctly new seizure for both cEEG andimited-channel aEEG. Limited-channel aEEG data wereetrospectively and independently reviewed by both a blindedpileptologist and an unblinded experienced limited-channelEG reader. Any disputed seizures were resolved between the
wo readers. In the event that no agreement could be reached,third experienced reader was used to resolve the differences.
EEG data were interpreted by a separate blinded epileptolo-ist. Clinical data such as Apgar scores, length of time to fullral feeds, time to discharge, number and dose of antiseizureedications, and discharge medications were recorded. MRIsere read by a blinded reader who scored the images on injury
o the cortex, white matter, deep nuclear gray matter, andrainstem. Images were then assigned a global score based onverall degree of injury (1 � normal, 5 � severe global injury).or classification purposes, hypoxic ischemic encephalopathyas defined as 2 of the following 3 in the presence of a knownerinatal event (cord accidents, nonreassuring fetal heart trac-ngs, placental abruption, etc): evidence of acidosis (pH �7 orE �12), need for respiratory support shortly after birth, orn Apgar score at 5 minutes of �5.
tatistical AnalysisAll data processing was done on SPSS version 16.0
SPSS Inc, Chicago, Illinois). Comparisons between groups
The Journal of Pediatrics • June 2009

wtgdwmltit�
rfep1OtrdO(1hb
g5cm(
S
c1Eatstsfh(nsoda
L
Frscwrs
P
ere done using a standard t test for parametric data (gesta-ional age, birth weight, time monitoring). These results areiven as a mean with a standard deviation. Nonparametricata (seizure burden, age of recruitment, Apgar scores, etc)ere evaluated with the Mann Whitney U test and given as aedian value with a quartile range. For skewed data, such as
ength of hospital stay and number of days to full oral feeding,he data were analyzed by cross-tabulation for the number ofnfants lying within the upper quartile in each group using �2
esting. Statistical significance was determined at P values of.05.
RESULTSFifty-two patients were eligible for this study during the
ecruitment period and 44 of these patients were approachedor enrollment. Reasons for not approaching a family fornrollment included late notification of admission (n � 5),rimary physician wishes (n � 1), a critically ill mother (n �), and a patient with major scalp trauma at delivery (n � 1).f the 44 patients approached, 40 consented to participate in
he study; 26 of these patients (65%) were outborn and theest were born at the adjacent delivery hospital. The majoriagnosis was hypoxic-ischemic encephalopathy (28/40, 70%).ther diagnoses included cortical stroke (n � 5), meningitis
n � 4), congenital hydrocephalus with hypoxic injury (n �), intraparenchymal bleed with sepsis (n � 1), and brainstememorrhage (n � 1). No significant differences were present
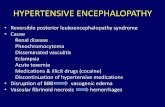
igure 1. Limited-channel aEEG screen displaying a patient with repeatedows show 10-second windows of unprocessed EEG tracing over the centraignal shows rhythmic discharges more pronounced over the right hemispheondensed amplitude integrated EEG (aEEG) background for the bilateralith both the upper and lower margin of the trace below 5 �V. The repeat
epeated seizure activity. The bar over both the raw signal (in real time) andoftware reporting events suspicious for seizure activity.
etween the visible and the blinded group with respect to t
ilot Study of Continuous Limited-Channel aEEG in Term Infants with E
estational age, birth weight, sex, race, age of enrollment,-minute Apgar score, percentage with hypoxic ischemic en-ephalopathy (HIE), percentage treated with hypothermia,ortality, and time monitored on limited-channel aEEG
Table I).
eizure AlgorithmOf the 40 infants, 25 had EEG seizures on limited-
hannel aEEG during the average of 68 hours (range, 3.5 to18) of limited-channel aEEG monitoring. There were 1116EG seizures retrospectively identified using limited-channel
EEG during the cumulative 2708 hours of recording. Ofhese 1116 events, 615 (55%) were detected in real time by theeizure detection software. The accuracy of the seizure detec-ion software improved with length of seizure with 73% ofeizures �30 seconds and 87% �60 seconds detected. Thealse-positive rate of seizure detection was 1 event every 11ours of monitoring resulting in a positive predictive valuePPV) of 73%, an overall false-positive rate of 26%, a false-egative rate of 45% (27% when looking at seizure �30econds), and a negative predictive value of 99%. In the subsetf patients with HIE (n � 28), the seizure detection softwareetected 79% of seizures �30 seconds with a PPV of 73% andfalse-positive rate of 1/11 hours.
imited-Channel EEG vs cEEGOf the 40 patients, 34 had simultaneous cEEG during
rographic seizures originating from the right hemisphere. The top twotal regions of the right and left hemispheres. This unprocessed EEGpicious for epileptic activity. The bottom 2 rows show the 3.5-hourpheres. This aEEG pattern is severely depressed over both hemispheresvations in the lower baseline (more pronounced on the right) representG background (at the corresponding time) represent the seizure detection
electl pariere sushemised ele
aEE
he limited-channel aEEG monitoring period, for an average
ncephalopathy 837

oiopdwwat8cdT6lwc(aesacrc
C
port1
nipdftwpc1tap(wc
ipcwwicmdcticssa
I
btavbTlddft
istgo
T
GBAMN5H
HMHS
Baaem
8
f 21 hours per patient (1 to 88 hours, 16 in blinded group, 18n monitored group). Reasons for not obtaining cEEG in thether 6 patients include clinical instability (n � 3), technicalroblems with the split leads (n � 2), and scalp trauma fromelivery (n � 1). In the 34 cEEG studies, 426 EEG seizuresere detected in 10 patients. Of these 426 seizures, 323 (76%)ere visible on the unprocessed EEG of the limited-channel
EEG. Of these 323 seizures, 171 (53%) were detected in realime by the seizure detection software (75% �30 seconds,8% �60 seconds). Just over 40% (171/426) of seizures oc-urring during cEEG monitoring were detected by the seizureetection software by the limited-channel aEEG monitor.his number increases to 57% for seizures �30 seconds and6% for seizures �60 seconds (seizure lengths based onimited-channel aEEG). In the subset of patients with HIEho had electrographic seizures on cEEG (n � 3), limited-
hannel aEEG compared more favorably, detecting 89%134/150) of the seizures seen on cEEG. On retrospectivenalysis of cEEG with video, �90% of the EEG seizurevents were clinically silent. Twelve events (3%) identified aseizures by retrospective expert review of limited-channelEEG monitoring were not characterized as seizures onEEG. By retrospective video analysis, these events wereelated to artifacts caused by patting or performing routineare without adequate nursing documentation.
linical FeasibilityIn 38 of 40 infants, the hydrogel electrodes were kept in
lace for the entire study period. In 2 patients, difficultyccurred, keeping the hydrogel electrodes in place and theecording was stopped early. The families’ preference was noto have their infant’s hair trimmed. In the visible group, 7 of
able I. Baseline characteristics
Blinded(n � 20)
Monitored(n � 20) P value
estation 38.5 � 1.7 wk 38.6 � 1.6 .775irth weight 3059 � 685 g 3289 � 890 g .365ge enrollment (h) 22 h (5-70) 20 h (6-52) .935ale gender 9 (45%) 13 (65%) .348on-Caucasian 9 (45%) 11 (55%) .916
-min Apgar 6 (4-7) 6 (3-9) .795ypoxic-ischemicEncphalopathy
13 (65%) 15 (70%) .496
ypothermia 6 (30%) 6 (30%) —ortality 2 (10%) 3 (15%) .643ours monitored 64 � 24 h/pt 72 � 22 h/pt .276eizures 13 (65%) 12 (60%) .752
irth weight and hours monitored are mean � SD. Apgar scores and age of recruitmentre medians with an interquartile range. P values were calculated by t test for gestationalge and birth weight (normal distribution) and by Mann-Whitney U test for gender,thnicity, age of enrollment, HIE, APGAR, mortality, and seizure incidence (nonpara-etric distribution).
2 (60%) infants with EEG seizures were accurately recog- i
38 Lawrence et al
ized and treated by the physicians. Of the remaining 5nfants in whom seizures were missed, 4 were due to failure ofhysician notification by the nursing staff when the seizureetection software was activated and 1 was missed due to aailure of the seizure detection software to detect a retrospec-ively identified EEG seizure. Only 1 of these 12 patientsith EEG seizures had recognized clinical correlates. The 5atients in whom seizures were missed were among the lowestumulative seizure burden of the 12 patients (between 35 and80 seconds, Figure 3; available at www.jpeds.com). Only 1 ofhe 20 patients (5%) in the visible group received inappropri-te antiseizure medication treatment secondary to misinter-retation of the limited-channel EEG data. Two patients10%) avoided treatment when clinically suspected seizuresere not treated with medication due to a lack of an EEG
orrelate on the limited-channel aEEG data.In the blinded group, 13 patients had EEG seizures
dentified in the limited-channel aEEG data, with only 3atients having clinical correlates. Of the 10 patients withlinically silent EEG seizures, 2 (with large seizure burden)ere detected on the 1-hour cEEG. Both of these patientsere placed on prolonged clinically indicated cEEG for mon-
toring and treatment of EEG seizures with neurologicalonsultation. The other 8 patients with EEG seizures re-ained blinded and were not treated with anticonvulsant
rugs. Of the 3 patients with initial clinical correlates, allontinued to have electrographic seizures with cessation ofheir clinical correlates after treatment with antiseizure med-cations. One of these 3 patients was also placed on prolongedlinical cEEG for monitoring and treatment of subclinicaleizures. Of the 7 patients in the blinded group withouteizures, 1 received treatment with antiseizure medications forclinical event that lacked a limited-channel aEEG correlate.
mpactTable II gives the short-term outcomes such as seizure
urden, antiseizure medication use, time to full oral feeding,ime to discharge, and MRI injury scores for both the visiblend the blinded group. Compared to the blinded group, theisible group had a 52% reduction in the overall seizureurden which was not found to be statistically significant.here was no significant difference in the number of antiepi-
eptic drugs or the number of antiepileptic drug boluses givenuring monitoring between the 2 groups. Figure 3 shows theistribution of seizure burden between the 2 groups. In in-ants with HIE, the reduction of seizure burden was similar tohe overall group (55% reduction).
In the 36 patients stable enough to undergo MRI exam-nation (18 in each group), qualitative scoring (1 � normal, 5 �evere global injury) in the visible group showed a trendoward decreased injury when compared with the blindedroup (median of 2 vs 3, P � .182). Other short-termutcome measures were similar between the 2 groups. Three
nfants in each group went home requiring either long-termThe Journal of Pediatrics • June 2009

npo(npb
mctwsrs
itcpbdbpp(onlo
ds
NaswsnnmstfirmcslTtvtTmi
5swgirsltbpstwicos
loirEEsl
T
SNSAIGD
F
D
AiPf
P
asogastric tube feeds or gastrostomy tube placement. Survivingatients in the visible group were less often discharged homen phenobarbital (4/17, 24%) than those in the blinded group8/18, 44%). Three of these patients in the blinded groupever displayed EEG seizures during monitoring and werelaced on phenobarbital for suspected clinical events eitherefore enrollment (n � 2) or during monitoring (n � 1).
DISCUSSIONLimited-channel aEEG is being increasingly used in
any NICU units for the monitoring and treatment of en-ephalopathic infants at risk for seizures. This study examineshe accuracy, feasibility, and impact of limited-channel aEEGhen used by bedside neonatologists. In addition, the current
tudy provides prospective data on the accuracy and utility ofeal-time seizure detection software (RecogniZe, BrainZ In-truments Ltd).
With limited-channel aEEG devices, the burden ofnterpretation and management shifts from the neurologist tohe bedside neonatologist. Thus, to demonstrate that limited-hannel aEEG devices are useful in patient management,hysicians not trained as specialists in electrophysiology muste able to accurately interpret the limited-channel aEEGata. The addition of software-based seizure detection helpsridge this gap. The overall seizure detection rate by therospective software-based seizure detector of 55% (false-ositive rate of 26%) improved as the seizure length increased73% �30 seconds, 87% �1 minute), leading to recognitionf infants with large seizure burdens. Furthermore, there waso evidence that the use of software based seizure detection
eads to overtreatment, supporting that this technology is not
able II. Short-term outcomes
Blindedseizuregroupn � 20
Monitoredseizuregroupn � 20
Pvalue
urviving to discharge 18 17 .223o. with seizures 13 12 .643
eizure burden/pt (s) 5352 � 11 880 2562 � 4237 .114ntiepileptic drugs/pt 0 (0-1) 0 (0-1) .783
ndividual boluses/pt 0 (0-1) 0 (0-1) .923lobal MRI injury (1-5) 3 (2-5) 2 (23) .110ischarge on
phenobarbital8/18 (44%) 4/17 (24%) .199
ull oral feeds�20 days (lower 75%) 14 13 .739�20 days (upper 25%) 4 4 N/Aays to discharge�21 days (lower 75%) 14 13 .739�21 days (upper 25%) 4 4 N/A
verage seizure burden is a mean � SD. Seizure burden, antiepileptic drug use,ndividual boluses, and global MRI injury are medians with an interquartile range.
values were calculated by using t test for comparison of means and Mann-Whitney Uor comparison of medians.
nly accurate, but safe. Only 1 of the 232 false-positive seizure p
ilot Study of Continuous Limited-Channel aEEG in Term Infants with E
etection events resulted in inappropriate administration of aingle dose of antiseizure medication (�1%).
None of the physicians or nurses on service in theICU were experienced at interpreting limited-channel
EEG data as such monitoring was utilized only for researchtudies. All received informal training at the bedside alongith daily reinforcement while their patient was part of the
tudy. In the majority of patients (7/12), physicians wereotified by the bedside staff and evaluated the limited-chan-el aEEG data correctly. In the instances of missed seizures,ost (4/5 patients) were not a result of a failed software-based
eizure detection or the physician’s inability to correctly in-erpret limited-channel aEEG data but rather a lack of noti-cation from the nursing staff. For this study, bedside nurseseceived minimal training on the limited-channel aEEGonitor focusing on sensor application, documentation of
are by annotation on the monitor, and recognition of theeizure event detector. This lack of focus on interpretationikely reduced their recognition of electrographic seizures.his issue seems easily remedied with additional training of
he nursing staff. Of the 12 patients with seizures in theisible group, the 5 in whom seizures were not recognized hadhe lowest total seizure burden (35 to 180 seconds, Figure 2).hus, all the patients with seizure burdens greater than 3inutes were appropriately identified and treated by the clin-
cal team.The seizure burden in the visible group was reduced by
2% when compared with the blinded group, who received atandard protocol of clinical observation and a 1-hour cEEGithout video. This was despite 3 patients in the blindedroup with large cumulative seizure burdens who were mon-tored continuously by cEEG for up to 4 days by clinicalecommendation from the neurology consultants. The lack oftatistical significance in the reduction of seizure burden wasikely due to either the small number of patients or reflectedhat a quantitatively large amount of the cumulative seizureurden in the blinded group came from a single patient. Thisatient was one of the few in the control group with a largeeizure burden who was not placed on prolonged cEEG. Therend toward decreasing seizure burden in the visible groupas despite any difference in the number of antiseizure med-
cation treatments given. Instead of increasing overall medi-ation use, limited-channel aEEG monitoring may decreaseverall seizure burden by leading to earlier, more targetedeizure treatment.
The long-term impact of decreased seizure burden onater outcomes remains unknown. It is notable that the extentf MRI injury was less in the visible group (trend only), butt is unclear if this is a reflection of the groups themselves oreflects a change due to the identification and treatment ofEG seizures. The hypothesis that aggressive treatment ofEG seizures may improve outcome has been previously
uggested but has been difficult to tease out from the under-ying injury causing the seizures.11,20,21
The present study has several limitations. First, this is a
ilot study designed to show feasibility and is not powered toncephalopathy 839

swwswaeeiand
EsissdscamlEcamEo
WfF
12s3ci4p5E6n7w8gn9E1a1w1er1Bs1E
Ftdlp
8
how differences in short- or long-term outcomes. Cliniciansere not given a specific protocol for treatment of seizures,hich led to variability in treatment strategies. Also, this
tudy recruited from a heterogeneous population of infantsith broad entry criteria. Patients with certain etiologies, such
s hypoxic-ischemic encephalopathy, may derive greater ben-fit from treatment of EEG seizures than those with othertiologies. Finally, while on limited-channel aEEG monitor-ng, all documentation of events such as clinical care, feeding,nd observation of clinical seizure events were dependent onursing annotation. Missing crucial documentation can makeata on retrospective analysis inaccurate.
Despite these limitations, monitoring and treatingEG seizures using limited-channel aEEG with real-time
oftware–based seizure detection is safe, accurate in thosenfants with seizure burden greater than 3 minutes, and fea-ible. Now we must ask the question, does treatment of EEGeizures with the goal of reducing seizure burden make aifference? In this cohort it is striking that 90% of EEGeizures lacked a clinical correlate even with retrospectiveEEG with video. Thus, clinical observation alone results ingross underestimation of true seizure burden coupled withany suspected clinical seizure events that lack a correlate on
imited-channel aEEG.8,9 Recognition and treatment ofEG seizures, however, may not be benign, as there are
ontinuing concerns regarding the effect of inducing neuro-poptosis in the immature brain with the use of antiseizureedications.16 To truly address if the reduction in cumulativeEG seizure burden, regardless of clinical correlate, improves
igure 2. Twelve patients in the monitored seizure group who had electroheir overall seizure burden. Black bars represent the 7 patients whose electretector software and properly interpreted and treated by the clinical neona
imited-channel EEG who were missed, either from failure of the seizure datients with seizure burden greater than 3 minutes were missed.
utcomes, a larger randomized, controlled study is required.1e
40 Lawrence et al
e thank the EEG technologists of St Louis Children’s Hospitalor their kind assistance (Barbara Smith, Sandra Boyd, Melanieitzgerald, Angela Johnson, and Nicole Moore).
REFERENCES. Volpe J, ed. Neurology of the Newborn. 4th edition. Philadelphia: Saunders; 2001.. Ronen GM, Penney S, Andrews W. The epidemiology of clinical neonataleizures in Newfoundland: a population-based study. J Pediatr 1999;134:71-5.. Tekgul H, Gauvreau K, Soul J, Murphy L, Robertson R, Stewart J, et al. Theurrent etiologic profile and neurodevelopmental outcome of seizures in term newbornnfants. Pediatrics 2006;117:1270-80.. Legido A CR, Berman PH. Neurologic outcome after electroencephalographicallyroven neonatal seizures. Pediatrics 1991;88:583-96.. Clancy RR, Legido A. Postnatal epilepsy after EEG-confirmed neonatal seizures.pilepsia 1991;32:69-76.. Pisani F, Cerminara C, Fusco C, Sisti L. Neonatal status epilepticus vs recurrenteonatal seizures: clinical findings and outcome. Neurology 2007;69:2177-85.. Ronen GM, Buckley D, Penney S, Streiner DL. Long-term prognosis in childrenith neonatal seizures: a population-based study. Neurology 2007;69:1816-22.. Murray DM, Boylan GB, Ali I, Ryan CA, Murphy BP, Connolly S. Defining theap between electrographic seizure burden, clinical expression, and staff recognition ofeonatal seizures. Arch Dis Child Fetal Neonatal Ed Epub 2007 Jul 11.. Bye AM, Flanagan D. Spatial and temporal characteristics of neonatal seizures.pilepsia 1995;36:1009-16.0. Holmes GL, Ben-Ari Y. Seizures in the developing brain: perhaps not so benignfter all. Neuron 1998;21:1231-34.1. McBride MC, Laroia N, Guillet R. Electrographic seizures in neonates correlateith poor neurodevelopmental outcome. Neurology 2000;55:506-13.2. Miller SP, Weiss J, Barnwell A, Ferriero DM, Latal-Hajnal B, Ferrer-Rogers A,t al. Seizure-associated brain injury in term newborns with perinatal asphyxia. Neu-ology 2002;58:542-8.3. Younkin DP, Delivoria-Papadopoulos M, Maris J, Donlon E, Clancy R, Chance. Cerebral metabolic effects of neonatal seizures measured with in vivo 31P NMR
pectroscopy. Ann Neurol 1986;20:513-9.4. Shellhaas RA, Clancy RR. Characterization of neonatal seizures by conventionalEG and single-channel EEG. Clin Neurophysiol 2007;118:2156-61.
ic seizures on retrospective analysis of the limited-channel EEG data andhic seizures on limited-channel EEG were detected by the seizurets. White bars represent the 5 patients who had electrographic seizures onr software (1), or by failure of nurses to notify the neonatologists (4). No
graphograp
tologisetecto
5. Shellhaas RA, Soaita AI, Clancy RR. Sensitivity of amplitude-integrated electro-ncephalography for neonatal seizure detection. Pediatrics 2007;120:770-7.
The Journal of Pediatrics • June 2009

1Ani1uN1c
1Sr2if2
P
6. Shah DK, Mackay MT, Lavery S, Watson S, Harvey AS, Zempel J, et al.ccuracy of bedside electroencephalographic monitoring in comparison with simulta-eous continuous conventional electroencephalography for seizure detection in term
nfants. Pediatrics 2008;121:1146-54.7. Rennie JM, Chorley G, Boylan GB, Pressler R, Nguyen Y, Hooper R. Non-expertse of the cerebral function monitor for neonatal seizure detection. Arch Dis Child Fetaleonatal Ed 2004;89:F37-40.
8. Freeman JM. Beware: the misuse of technology and the law of unintendedonsequences. Neurotherapeutics 2007;4:549-54.
nN
ilot Study of Continuous Limited-Channel aEEG in Term Infants with E
9. Navakatikyan MA, Colditz PB, Burke CJ, Inder TE, Richmond J, Williams CE.eizure detection algorithm for neonates based on wave-sequence analysis. Clin Neu-ophysiol 2006;117:1190-203.0. Hall RT, Hall FK, Daily DK. High-dose phenobarbital therapy in term newbornnfants with severe perinatal asphyxia: a randomized, prospective study with three-yearollow-up. J Pediatr 1998;132:345-8.1. Toet MC, Groenendaal F, Osredkar D, van Huffelen AC, de Vries LS. Postneo-
atal epilepsy following amplitude-integrated EEG-detected neonatal seizures. Pediatreurol 2005;32:241-7.50 Years Ago in The Journal of PediatricsINFANTILE AGRANULOCYTOSIS OF CONGENITAL ORIGIN
Blattner RJ. J Pediatr 1959;54:839-41.
In this 1959 report, Dr. Russell Blattner reviewed several cases of infantile agranulocytosis. They resembledKostmann’s 1956 description of 14 children from 9 families in an isolated Swedish population,1 and all died of infectionin infancy or early childhood. Kostmann inferred autosomal recessive inheritance and Blattner speculated on a metabolicdefect in sulfur-containing amino acids.
In the last 20 years, revolutionary advances have dramatically increased our understanding of the molecular basis ofsevere congenital neutropenia (SCN) and improved its prognosis but raised new questions about appropriate long-termmanagement. Recent studies have revealed the genes responsible for most forms of SCN.2 Homozygous mutations inHAX1, a gene encoding a mitochondrial protein, have been identified in several kindreds, including 3 from the originalreport, so “Kostmann syndrome” now refers specifically to autosomal recessive disease caused by HAX1 defects. MostSCN, and virtually all cyclic neutropenia cases, represent heterozygous, autosomal dominant mutations in the ELA2gene, which encodes neutrophil elastase.2 Although the exact pathophysiology remains unknown, differentiating myeloidcells show accelerated apoptosis, possibly because of initiation of an unfolded protein response.3
The advent of cytokine therapy has transformed this previously fatal disease of infancy into a chronic, oftenasymptomatic, disorder of children and adults. More than 90% of patients with SCN respond to granulocyte colony-stimulating factor (filgrastim) with increased neutrophil numbers and reduced infections. However, increasing numbersof patients with SCN receiving long-term granulocyte colony-stimulating factor therapy have developed of myelodys-plasia, often characterized by monosomy 7, progressing to myeloid leukemia.4 Hematopoietic stem cell transplantationis curative for SCN, but more difficult after onset of myelodysplasia or leukemia. Thus, physicians and families facedifficult choices about performing transplantation in patients with high risk but stable disease, or waiting for cytogeneticor hematologic signs of impending malignant transformation.
Peter E. Newburger, MDProfessor of Pediatrics
University of Massachusetts Medical SchoolWorcester, Massachusetts
10.1016/j.jpeds.2008.11.055
REFERENCES1. Kostmann R. Infantile genetic agranulocytosis; agranulocytosis infantilis hereditaria. Acta Paediatr 1956;45:1-78.2. Boxer LA, Newburger PE. A molecular classification of congenital neutropenia syndromes. Pediatr Blood Cancer 2007;49:609-14.3. Xia J, Link DC. Severe congenital neutropenia and the unfolded protein response. Curr Opin Hematol 2008;15:1-7.4. Rosenberg PS, Alter BP, Bolyard AA, Bonilla MA, Boxer LA, Cham B, et al. The incidence of leukemia and mortality from sepsis in patients with severe congenitalneutropenia receiving long-term G-CSF therapy. Blood 2006;107:4628-35.
ncephalopathy 841

Ft
8
igure 3. Cumulative seizure burdens in seconds for each patient with electrographic seizures on limited-channel aEEG (circles) are displayed for bothhe blinded group and the monitored group. Furthermore, the mean seizure burden for each entire group is also displayed (line).
41.e1 Lawrence et al The Journal of Pediatrics • June 2009