
A Further Challenge to the Welfare State: Two … to the Welfare State: Two Paradoxes of Trust ......
32
Paper presented at the Conference on ‘Challenges to the Welfare State’ at the Minda de Gunzburg Center for European Studies, Harvard University, May 5, 2006 A Further Challenge to the Welfare State: Two Paradoxes of Trust. Peter Taylor-Gooby SSPSSR University of Kent CT2 7NY, UK [email protected] www.kent.ac.uk/scarr
Transcript of A Further Challenge to the Welfare State: Two … to the Welfare State: Two Paradoxes of Trust ......

Paper presented at the Conference on ‘Challenges to the Welfare State’ at the Minda de Gunzburg Center for European Studies, Harvard
University, May 5, 2006
A Further Challenge to the Welfare State:
Two Paradoxes of Trust. Peter Taylor-Gooby SSPSSR University of Kent CT2 7NY, UK [email protected] www.kent.ac.uk/scarr

2
The author is grateful to NatCen and to the ESRC Data Archive for providing the data discussed here. Abstract Recent work has reviewed challenges to the welfare state settlement from many
directions. The balance of judgement is that welfare states are not becoming obsolete
but rather are being restructured. The restructuring process includes spending
constraint, stress on labour market activation and the introduction of strict
performance management and new quasi-market systems. The rapid pace of change
raises the question of the long-term stability of the new settlement. One issue is the
impact of new policies on public trust in welfare state institutions.
Discussion of trust in public institutions across political science, psychology and
sociology indicates that a range of pressures are reducing the supply just as the
demand for public trust is increasing. Trust appears to be based on both rational
considerations (assessment of track-record in performance, transparency, availability
of information, regulation) and affective factors (shared values, belief that the trustee
has the trustor’s interests at heart). The New Public Management foregrounds
incentives that appeal to rational judgement, but ignores affective considerations. It
appears to succeed in improving service output in some areas. The risk is that a
process that delivers the goods in an objective sense may at the same time undermine
trust, by failing to address subjective factors. The issue is analysed using recent
attitude survey data in relation to health service reform in the UK, which furnishes an
excellent case-study of a broader direction of reform in European welfare states.

3
Challenges to the Welfare State:
Two Paradoxes of Trust Material and political challenges to the stability of welfare state settlements have been
extensively analysed. Topics covered include the impact of technological change and
shifts in trade on labour markets, of globalisation in currency markets on government
authority (McNamara, 1998), of post-industrialisation on growth rates (Iversen and
Wren, 1998), of demographic and household shifts on the need of services, of more
equal opportunities for women on the supply of unpaid care, of migration on public
attitudes (Alesina and Glaeser, 2004) and of all these factors on government policy
making and on patterns of new politics (Pierson, 2001) or responses to new social
risks (Bonoli, 2005) in different national contexts. At the risk of over-simplification,
the dominant theme in this work is that pressures are substantial but have not
undermined the welfare state. Instead they are leading to restructuring, with the pace
of change varying between countries (see Pierson 2001; Huber and Stephens, 2001;
Jessop, 2002; Scharpf and Schmidt, 2000; Taylor-Gooby, 2004).
One aspect of restructuring has been a renewed emphasis on policies that contribute to
both social and economic progress, expressed at the level of the EU (for example, in
the European Employment and Social Inclusion Strategies) and OECD (2005), and
also in the promotion of approaches like the Third Way or Neue Mitte, the
deregulation of areas of the labour market in Germany and attempts to do so in France,
the mobilisation of women workers, and a general commitment to activation. These
approaches bring European welfare policies closer to those often analysed as
‘productivist’ (Gough, 2001) in an East Asian context.
A second development has been cost containment, most notably in pension reforms
limiting future obligations in many countries from the early 1990s onwards. The
continuing pressure on provision in expensive service areas like health care and
education has led to spending control through cash-limited budgets, the assumption of
efficiency gains, tight performance management and the use of market or quasi-
market systems, which introduce competition as a spur to cost-efficiency (Saltman et

4
al, 1998). These developments form a central part of what has come to be known as
the New Public Management (Clarke et al., 2000).
The impact of the introduction of market and quasi-market systems within social
policy and the possibilities for fine-tuning such systems to achieve particular
outcomes for target groups has been extensively discussed (see Le Grand, 2003, ch. 5).
This paper considers a further aspect of the shift towards performance management,
involving close monitoring of success in achieving imposed targets, and towards the
introduction of the market in social policy: these policies well lead to greater cost-
efficiency and help welfare states to ‘deliver the goods’ under circumstances where all
the pressures tend towards ‘permanent austerity’ (Pierson, 2001, 456). However,
because they rest on principles other than those of the traditional welfare state
settlement, they may also damage the acceptability of welfare policies to citizens.
In the early 1970s, a number of writers suggested social changes might lead to a
‘legitimation crisis’ of the politico-economic settlement (Habermas 1976).
Difficulties were anticipated in maintaining the appropriate motivations among
citizens of an increasingly market-oriented society. In this paper we focus on an
appropriately downmarket analogue for the 2000s: material challenges may produce a
successful but market-oriented policy response that erodes public support, and in
particular institutional trust, a paradox of self-stultifying achievement.
The problem arises because trust in institutions contributes to their legitimacy. It is
only one factor: one may have a high level of trust in the health, education or postal
service, but be dissatisfied with the service because it does not serve the specific
interests of one’s own group or family; because it underperforms through lack of
funding; or because it is based on abhorrent principles, such as the use of child-labour;
or because it is manifestly unsustainable. Any of these factors might contribute to
making a welfare state settlement unstable. It is difficult to see, however, that a
public service that is not trusted by users can be seen as acceptable.
This paper falls into three parts: a discussion of trust in public institutions and of
recent developments in this field, pointing out the pressures which both enhance the
demand for trust and constrain the supply; a review of work in psychology and

5
sociology on the factors enhancing trust, stressing the common finding that trust
derives from both rational cognitive and non-rational affective factors; and an
examination of evidence on institutional trust and public satisfaction in relation to the
New Public Management in the UK NHS.
I Institutional Trust: Concepts and Developments
The term trust ranges across a large social science literature, in which Das and Teng
identify 28 definitions (2004, 96). Luhmann sums up the key points: trust is relevant
to managing uncertainty when something is at stake. ‘To show trust…is to behave as
though the future were certain … Trust is only involved when the trusting expectation
makes a difference to a decision’ (Luhmann, 1979, 10, 24; see also Rousseau et al,
1998, 395; compare Crasswell, 1993, 104; Sztompka, 1999, 25; Dasgupta, 1988, 51;
Robinson, 1964, 73-4; Gambetta 1988, 218). Our concern is with citizen trust in
institutions, particularly those that make up the welfare state and which are currently
undergoing reform, in contexts where misplaced trust will damage the citizen’s
interests and where the citizen as service-user faces uncertainty. The example of
health care in the UK, reviewed later, displays these features.
Institutional Trust: Towards Critical and Active Citizenship
Writers from various disciplines (political science, sociology and psychology) have
discussed the emergence of more active forms of citizenship in which trust is of
increasing importance. Almond and Verba's path-breaking analysis of the key aspects
of a successful civic culture identified two basic components: engagement and
deference (1963). More recent work in political science has investigated a possible
decline in support for major governmental institutions (Nye, Zelikow and King, 1997).
Norris concludes from a review drawing on the international attitude surveys (ISSP
and WVS) and national election studies that: ‘we have seen the growth of more
critical citizens who value democracy as an ideal, yet remain dissatisfied with the
performance of their political system …’ (1999, 269; see Held 2002, ch. 1; Marquand
and Crouch, 1995).

6
Many cultural sociologists arrive at similar positions by a different route. Received
authority is no longer available as a guide to everyday living (Tulloch and Lupton
2003; Lupton 1999; Giddens 1994; Lash et al, 1996; Bauman 2000). The kind of
‘organic solidarity’ which Durkheim saw as essential to resolve the problems
stemming from a continuing division of labour is in decline (Dahrendorf 1990;
Seligman, 2000, ch 1). One outcome is greater stress on the problem of achieving
social integration. Some commentators argue that new forms of citizen trust are
emerging. Giddens sees ‘active trust’ as replacing older traditions of trust. Citizens
become ‘clever’ – well-informed and confident in their capacity to criticise. In a
more unstable society, institutional trust rests on a continuing quest for grounds on
which trust might be based, leading, he suggests, to a more engaged and ‘dialogic’
democracy. ‘Active trust is the basis of self culture. It assumes not a clinging to
consensus, but the presence of dissent; it rests upon recognition … of the claim to a
‘life of one’s own’ in a cosmopolitan world.’ (Beck and Beck-Gernsheim 2002, 46).
Levi and Stoker summarise a comparable discussion of the role of ‘rational dissent’ in
participative democracies (2000, 484).
Work from a psychological perspective has tended to be more formally structured and
has not engaged centrally with citizenship. One theme has been the examination of
the circumstances under which lay publics are willing to accept expert and official
claims about matters which concern them, and the implications for institutional trust
(Weyman and Kelly, 1999, Petts, 1998; Renn and Levine, 1991, Slovic, 2000, Royal
Society 1997). Fruitful streams of work have discussed mental modelling and the
processes which account for the social amplification or attenuation of beliefs and
assumptions. There has been recent interest in the beliefs about institutions which
accompany institutional trust. Poortinga and Pidgeon conclude from a study of trust
in officials and institutions in relation to risky innovations such as nuclear power,
cloning or climate change, that critique is not the simple contradictory of citizen trust.
In fact ‘a high degree of general trust can also coexist with a relatively high level of
scepticism … best … described as critical trust’ (2003, 971; see DTI, 2005, Taylor-
Gooby, 2006).

7
These analyses support (from different directions) the view that changes are taking
place in democratic citizenship, and that one important aspect is that the public is less
likely to take on trust the virtue of government policies and the claims made by
authorities. Citizens challenge, test and assess for themselves the validity of
pronouncements and the quality of institutional provision. This is not so much an
endemic mistrust, a Hobbesian ‘war of every man against every man’, but an engaged,
quizzical, querulous and possibly more mature citizenship.
An analogous development is the increased attention paid by political scientists and
organisation theorists to the shifts within public and private sector organisations away
from bureaucratic and hierarchical management to more decentralised systems. The
driving force here has been the introduction of quasi-markets to promote greater
efficiency and responsiveness to service-users, typically within a framework in which
an authority sets targets and budgets and maintains quality control (Le Grand and
Bartlett, 1993; Scharpf 1999). The various agencies must establish new competitive
and co-operative relationships within a non-hierarchical structure. This is set in the
context of broader shifts. For sociologists, globalisation introduces further fluidity
and flexibility through increased contact with other cultures and the declining
authority of national traditions. For political scientists, the twin processes of
globalisation and of ‘hollowing-out’ of the state (Rhodes 1997; Jessop 2002) further
limit the predictability of systems and the authority of the nation state.
At the level of organisational practice the ‘phenomenal expansion of the risk industry
reflects a number of different but convergent pressures for change in organisational
practices for dealing with uncertainty. …. Risk has entered private and public sector
management thinking … as never before. …In both the public and private sectors,
risk management is part of a new style of organisational discipline and accountability’
(Power, 2004, 13). Rothstein and colleagues chart out the process by which systems
set up to regulate societal risks generate risks of failure for regulatory bodies which
leads to a feedback spiral of ever more intrusive regulation understood as the ‘risk
colonisation’ of government (Rothstein et al, 2006, 91). O’Neill links this trend to the
decline of respect for professionalism and for accredited expertise: ‘Perhaps the
culture of accountability that we are relentlessly building for ourselves actually
damages trust rather than supporting it’ (O’Neill 2002; see Rayner, 2004).

8
The outcome of these developments is a more general paradox of public trust: social
processes increase the demand for public trust; but related processes render public
trust in experts, official and institutions more equivocal.
The paradox of welfare state reform mentioned earlier rests on the collision between a
political economy of response to pressures and the social outcome of that response.
The above paradox deals with the social processes that damage trust. It is the
coincidence of these processes with the global politico-economic changes that brings
the two paradoxes together and implies further challenges to with current reforms.
There is widespread concern among policy-makers about declining institutional trust.
A number of writers refer to falling levels of trust in public institutions (O’Neil, 2002;
MORI, 2003; Neuberger, 2005). The Cabinet Office Strategy Unit report on Risk,
notes that ‘a very wide range of UK institutions have suffered from a significant drop
in trust over the past two decades’ (COSU, 2002, 3.26). It quotes evidence from
Henley Centre Surveys of attitudes to parliament and civil servants, the findings of the
World Values Survey and the work of Inglehart (1999, pp 88-120) and links the issue
to ‘parallel trends to declining deference’ (3.27). The OECD argues that ‘several
driving forces have led OECD countries to focus attention on strengthening their
relations with citizens, including … surveys showing declining confidence in key
public institutions’ (OECD, 2001).
In fact, the evidence discussed earlier suggests that institutional trust, as a component
of citizenship, may have become more discriminating rather than less vigorous.
Reform is not automatically distrusted, but must face the scrutiny of critical trust. The
paradoxes stated above direct attention to a serious and practical point: from the
policy-maker’s point of view, trust in government institutions, especially those
undergoing rapid reform, is both more necessary and more difficult to get. In relation
to some of the recent welfare state reforms, those involved may find the paradox
especially trying. Performance across a range of policy areas has improved markedly,
yet service-users are no more satisfied. This raises the question of what enhances and
what damages institutional trust.

9
II The Dual Basis of Trust
Social science perspectives on institutional trust as a way of managing uncertainty
may be roughly grouped into those where trust is based on reason and those where it
is based more on non-rational factors. The post-Enlightenment shift away from
traditionalism to modernity eroded reliance on such non-rational strategies as luck,
fate, the favour of the gods, commitment guaranteed by oath, attunement with cycles
of nature, and faith in a transcendental or temporal authority, and directed attention to
prediction through a range of techniques (probability theory, actuarial science,
epidemiology, demography, induction from previous applications of a technology,
micro-simulation, process modelling, and so on) coupled with the regulatory and legal
approaches available to a modern interventionist state. Recent developments are
bringing home the limitations of rational approaches and the value of non-rational
ones. The particular helpfulness of trust is that it bridges both these domains. The
relevance to discussion of policy is that the intellectual frameworks most influential in
current reforms stress rational, cognitive approaches, and this limits their capacity to
engage with the non-rational aspects of public trust and mistrust.
Rational Approaches to Trust
Rational approaches have at their core the idea that trust is based on the deliberative
consideration of evidence. Such approaches have dominated economics (Dasgupta
2002) and played an important role in psychology and sociology (Coleman 1995, 155,
Gambetta, 1998). Trust in institutions requires evidence of track-record (and
therefore confidence in the transparency of the agency and the quality of the
information made available) and an indication that past record is likely to be a good
guide to the future, for example, a system of regulation.
As O’Malley shows (2000), the development of legal frameworks which rewarded
appropriate trust and punished those who exploited others led to the expansion of
regulated private and then social insurance (Ewald, 1986; Dean, 1999). This was
reinforced by systems of indemnity and accreditation by trader’s associations and

10
others, and an emphasis on greater transparency, for example, Ebay’s posting of
transaction feedback (Ticoll and Tapscott, 2003). Some writers attribute the
economic success of Western countries (and in particular those countries in which
moral systems placed a high value on integrity) to social networks which facilitated
the production of public trust (Putnam, 1993; Fukuyama, 1996).
Transparency issues have played a central role in concerns about public trust in
science and technology, where risk communication has been a key theme (Pidgeon et
al 1992, Royal Society 1997). This has led to increasingly sophisticated analysis of
distortions and confusions in public understanding of expert pronouncements. One
practical outcome has been greater emphasis on the involvement of the public,
through exercises such as citizen’s juries, the ‘People’s Panel’ polling system
(established by the Labour government via MORI in 1998), the series of road-shows
on major policy issues and such set-pieces as the 2002-3 GM Nation? debate, or the
national debate on nuclear power presaged by Blair at the time of the 2005 Election
(Sourcewatch 2006) and the elaborate (and appropriate) Citizens’ Advisory Panel
exercise which led to the 2006 White Paper on Community Care, of which the key
feature is user consultation and involvement (DH, 2006, Annex 1).
Rational approaches have been important in relation to the UK quasi-market reforms.
A core concern has been to improve performance in relation to widely accepted and
salient measures of output. Detailed information on achievement against targets is
made available via the Treasury Public Spending Review website (http://www.hm-
treasury.gov.uk./spending_review/) and then publicised in the media.
Non-Rational Approaches to Trust
A separate stream of work, less influential in recent reforms, emphasizes the
importance of non-rational factors in trust. This work does not deny the significance
of rational deliberation, but argues that other factors operate alongside it, and are of
equal significance. Work by psychologists bridges the individualist methodology of
economists and the more collective focus of sociology by combining experimental
and survey methodologies and using conceptual frameworks that acknowledge the
significance of both individual cognitive and more socially-based affective elements.

11
Psychologists have emphasized the multi-dimensionality of trust. Hovland’s initial
studies distinguished two dimensions: competence and care, or trustworthiness
(Hovland et al, 1953). This has been refined by other researchers, typically using
principal components analysis techniques on responses to batteries of items in
questionnaires (for example, Renn and Levine, 1991; Metlay, 1999; Frewer et al,
1996; Poortinga and Pidgeon, 2003). Almost all the analyses produced distinguish the
capacity of the trustee to actually carry out the relevant task from the belief that she
shares the trustors values, is, as it were, on the trustor’s side. The background
assumption is that deliberation on track-record may be a reasonable guide to
competence, but trustworthiness – confidence that you are trusting someone who
actually takes your interests to heart - requires an extra-rational leap of faith supplied
by affect or cultural factors. This ‘leap of faith’ is necessary to address uncertainty,
where past record may not be a helpful guide.
Further work also focuses attention on the affective dimension of trust. Cvetovich
and Earle (1997) argue that most people find complex risk issues too difficult and
wearisome to analyze and resort to a general sense of sympathy with the institution
(or otherwise) rather than cognition. Similar points are made in the broader literature
on decision-making under uncertainty, which increasing emphasizes the contribution
of affective alongside deliberative factors often formalised in a ‘dual-process’ theory
(Finucane and Holup, 2006, 141; see Schwartz, 2000; Todd and Gigerenzer, 2003,
162; Slovic, 2000; Epstein, 1994).
The central argument is that both cognition and affect contribute to trust and mistrust.
This approach can be paralleled elsewhere in social science. Barbalet argues from a
sociological perspective that emotional factors play an important (he argues, leading)
role in many aspects of social behaviour (2002). His central point is that, although
rational procedures can help us evaluate risks, they do not apply to the circumstance
in which trust is most important, since these typically concern areas of uncertainty
where the capacity of reason to resolve the issue is limited. Under these
circumstances emotion makes an essential contribution to trust. He refers to Keynes’
oft-quoted passage about the drive to entrepreneurship under uncertainty: ‘most … of
our decisions … can only be taken as a result of animal spirits – of a spontaneous urge

12
to action rather than inaction, and not as the outcome of a weighted average of
quantitative benefits multiplied by quantitative probabilities’ (1936: 161).
Keynes is dealing with any future-oriented action under uncertainty. Trust refers to
the sub-group of actions involving reliance on another. More recent analysis of
economic decision-making draws attention to a similar role for emotions: ‘trust and
distrust are social emotions constituted within and between powerful organisations for
rationally coping with the unknown in decision processes, later ‘felt’ as emotions by
individuals or groups of them’ (Damasio 1996).
Pixley demonstrates on the basis of detailed interviews with chief executives and
directors of large corporations and financial institutions that emotional considerations
play a significant role in major financial decisions. This is typically defended on the
grounds of the uncertainty involved in moving in new directions: ‘trust and distrust
are the only way to project financial futures as certain’ (2004, 17). Other sociologists
have also placed considerable weight on the importance of emotional factors and
social relationships. Calnan and Rowe describe trust as ‘primarily consisting of a
cognitive element (grounded on rational and instrumental judgments) and an affective
dimension (grounded on relationships and affective bonds generated through
interaction, empathy and identification with others)’ (2005, 1). Page’s overview of
MORI attitude studies on UK health services shows that ‘there is a very strong
correlation between the extent to which patients feel they are treated with care and
respect and their overall perception of the hospital’ (Page, 2004). Anheier and
Kendall make similar points in the related field of voluntary organisations (2002, 354).
The affective and cognitive bases of trust have also been examined in political science,
which often distinguishes between the evaluation of programmes and responses to
particular political actors. The former are assessed in terms of self-interest, while the
latter often turn on affective issues - the perceived honesty of the politician or policy-
maker, the extent to which that person is in touch with citizens (Pattie and Johnston,
1998, Curtice and Seyd, 2003, 95; Marcus, 2002; Glaser and Salovey, 1999).
This discussion draws attention to the duality of trust in public provision. A
traditional model of government understood the state welfare sector as managed

13
thorough a combination of authority that was bureaucratic (in areas where discretion
was limited) and professional (where judgements were involved), and dealt with a
citizenry which largely accepted the effectiveness of these systems. Reason plays a
major role in their legitimacy, indeed the potential inhumanity of rational control has
been a major theme from Weber onwards. However, the dominant assumption has
been that both professionals and bureaucrats operated in the public interest and could
be trusted to do so. New developments in organisational theory from the 1970s
onwards, inspired by economic models and by public choice theory (Mueller, 1979;
Riker, 1986), pointed out that the behaviour of public sector bureaucrats and
professionals might be as much influenced by a self-regarding rationality as by an
ideal of public service (Niskanen, 1971; Barr, 1998, 92).
Interest in these theories in the UK context was driven by concern to achieve greater
cost-efficiency in the face of continuing pressures on the welfare state (Glennerster,
1997), by the dominance of anti-collectivist political ideologies (Bonoli and Powell,
2003) and by the attractiveness of incentive-based solutions to the problem of
directing ever more complex decentralised provider agencies (Dixit, 2002). In the
context of the NHS, the salience of principal/agent issues (Pratt and Zeckhauser, 1985;
Le Grand, 2003, 59-61) and of the opportunities for highly-regarded professionals to
engage in ‘shroud-waving’ have also been influential. A move to target-based
performance management and quasi-markets offered an attractive solution to the
problem of controlling service-providers, enhancing cost-efficiency and prioritising
responsiveness to service-users. Current reforms rely on rationality-driven solutions
to the problem of cost-constraint and improved output in a highly popular public
service where the majoritarian constitutional framework enables rapid reform.
III Trust in the UK NHS: a Case-Study
The previous Conservative administration introduced a series of quasi-market reforms
in the early 1990s. These constituted GP practices as budget-holders for a substantial
proportion of resources, allocated according to the number and status of patients for
whom they were responsible. GPs then provided treatment directly or purchased it

14
from NHS providers. This internal market was developed cautiously, since the
government was unwilling to provoke conflict with powerful and prestigious medical
interests (Klein, 1996). The incoming Labour government strengthened this policy as
a system of fund-holding by the Family Practitioner Committees responsible for GP
practices in a given area. They also decentralised the management of other NHS
agencies, so that hospitals or groups of hospitals and other services (ambulance,
domiciliary, specialist clinics and so on) became self-governing trusts, responsible for
managing their own budgets. This took place in the context of a new performance
management system which introduced ‘clear incentives to improve performance and
efficiency’, implemented in an increasingly stringent manner (DH, 1997, 3.12).
Agencies which met targets received resources, those which failed found their budgets
cut and their managers demoted. The play of market forces has more recently been
intensified by the introduction of new Independent Diagnostic and Treatment Centres
(IDTCs), run by NGOs or the private-for-profit sector, treating about 250,000 patients
a year by 2005. From 2006, the market logic will be taken further through the
introduction of a ‘Choose and Book’ system whereby those referred for non-
emergency treatment must be offered a choice of four clinics from across the range of
approved state or non-state providers, and the expansion of IDTCs (DH, 2005).
Two other developments are important. First, new institutions support performance
management and inform market actors. The Healthcare Commission provides an
inspection regime. League-table results for the performance of the various agencies
are published, Trusts are star-rated according to their success and progress towards
government targets published. The National Institute of Health and Clinical
Excellence, an expert body, assesses the cost-effectiveness of particular interventions
and advises on those which should be financed through the NHS, often against the
views of doctors and drug companies. Overall budgets are strictly controlled and
progress towards targets closely monitored. As a result a number of Trusts are
currently facing pressures to close facilities and sack staff to remain within budget.
Secondly, after an initial period during which the Labour government restricted
spending to the tight plans of the previous Conservative government to enhance its
credibility, health care spending has been sharply increased, from 5.4 to 7.0 per cent
of GDP between 1997/8 and 2004/5 (Treasury 2005, Table 3.4 – see Figure 1), in a

15
context of continuing restraint in other areas, financed partly by an unprecedented
earmarked one per cent extra on National Insurance contributions.
The impact of these reforms excites controversy. Critics (including the principal
adviser on the budget increases, Derek Wanless) argue that too much new money was
squandered on pay increases (Temko and Revill, 2006 1). Performance has
nevertheless arguably improved. The Kings Fund, often a critic of government,
concludes in a recent review: ‘Nevertheless, increased funding has bought more staff
and equipment, and together with tough targets in England, this has helped reduce
waiting times to an historic low’ (2005). The number waiting more than 13 weeks for
an outpatient appointment or six months for inpatient treatment have fallen by about
two-thirds in the four years since September 2001, and death rates for cancer and
heart disease continue to fall, although rather more slowly (Treasury, 2005b,
performance review website). An up to date study by Bevan and Hood reports that
the ‘the star rating system has improved reported performance on key targets’ (2006,
421).
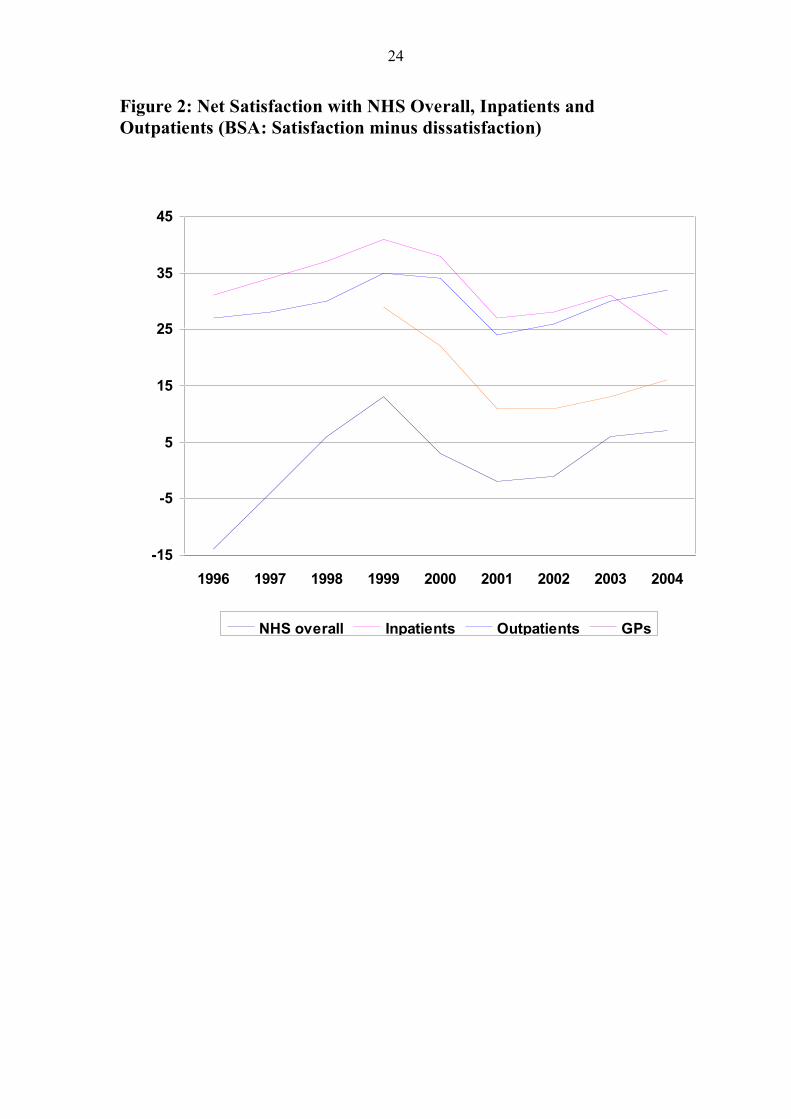
The experience of public response to the NHS reforms in the UK provides a good
opportunity to examine issues of public trust in state welfare institutions. Spending
has increased and performance in key areas improved. However, public satisfaction
with the services does not follow this pattern (Figure 2). There is a common pattern
across different areas of an initial sharp rise (probably a ‘honeymoon’ for the
incoming Labour government, associated with the NHS since its inception), followed
by a drop just at the time that performance management started to bite and then, as
spending starts to rise, by gradual improvement, which fails to reach the levels
attained earlier. Crucially, satisfaction with hospital services is disappointing: for
inpatients, the level is now falling, and, for outpatients, the rise appears to level off at
about the level reached under the previous government.
Attitude Survey Evidence
A substantial body of work on trust in health care exists, conveniently summarised in
a recent Nuffield-funded review (Rowe, 2004). The vast majority of the studies
reviewed (94.3 per cent) focus on patient-clinician relationships and 70 per cent were

16
carried out in the US or Canada. The review concludes: ‘Patient trust in clinicians
remains high although levels of public trust are lower.’ The one study that examines
patient-organisation relationships indicates falling public trust in the US in the late
1990s (Davies, 1999). The broader area of citizen perceptions of the health service as
an institution does not appear to be directly addressed.
In this analysis we use material from the British Social Attitudes survey1, a high-
quality annual UK survey, which included questions on trust in 2001, but contains
questions on satisfaction with components of the services and on a wide range of
perceptions of different aspects in most years. We argued earlier that trust is not
equivalent to satisfaction with a public service, but is a necessary component in it.
The Pearson correlation between measures of trust and of satisfaction from the 2001
survey is 0.17 (significant at the one per cent level), indicating the existing of a real
but not strikingly strong relationship. The attitude material is used here to:
- Investigate the development of public perceptions of the NHS from the 2001
and 2003 British Social Attitude surveys;
- Examine whether these perceptions can be organised into cognitive and
affective factors, as suggested by earlier discussion; and
- Consider their relationship to trust in and satisfaction with the service in the
context of such factors as demography and political party support.
The limitations of available data mean that it is not possible to address the impact on
public trust of perceptions of the most recent reforms, or to consider the development
of trust over time. However, the survey material demonstrates that factors other than
the output on which government policy focuses play an important role in generating
trust.
Trust and Satisfaction: 2001 and 2003
The 2001 survey included a battery of questions on trust in state and non-state
services. The question asked in the case of the NHS was: ‘Please tick a box to show
how much you trust NHS hospitals to spend their money wisely for the benefit of
their patients?’ The responses were: 12.1 per cent, ‘a great deal’, 46.6, ‘quite a bit’;

17
35.1, ‘not much’; and 6.1, ‘not at all’. While the balance of trust over mistrust was
positive at 18 per cent, it was substantially lower than in the case of private hospitals
(40 per cent), a pattern repeated in relation to state and non-state pensions and schools
(Taylor-Gooby, Hastie and Bromley, 2003). This confirms the disquiet evident in
policy debate at a more general level about relatively low levels of trust in state sector
provision.
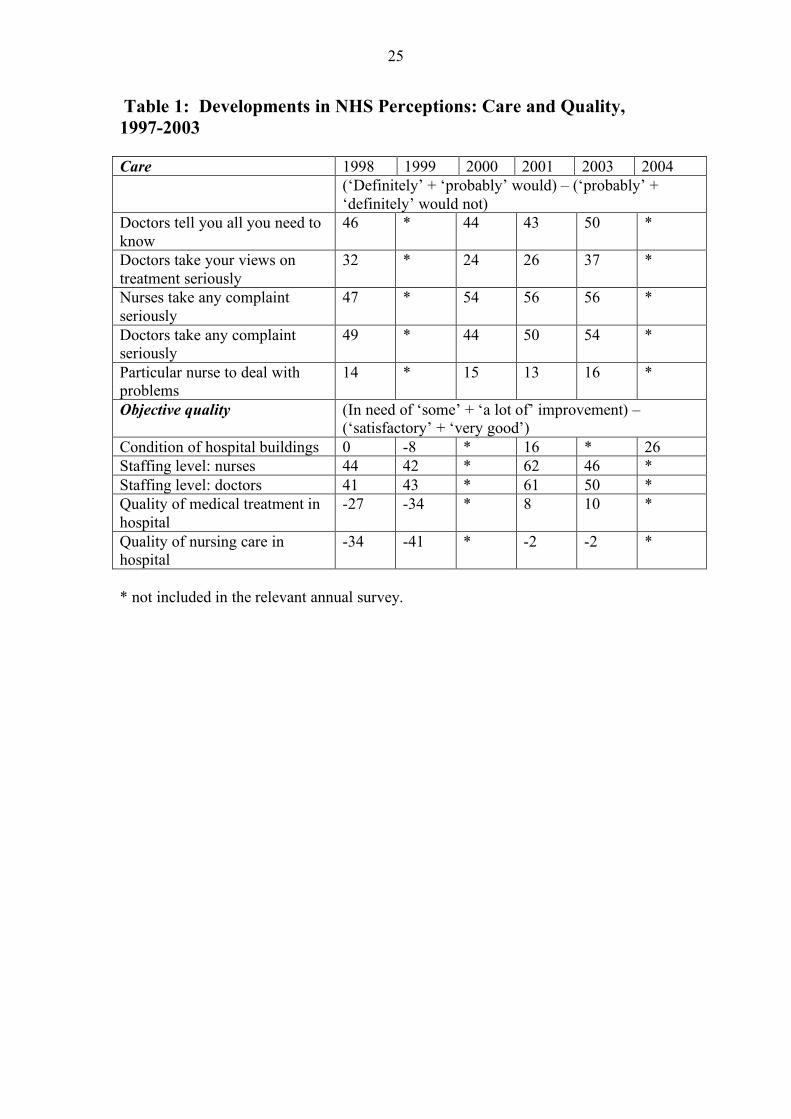
Batteries of questions on perceptions of the NHS provide evidence relevant to the
cognitive and affective bases of trust (Table 1). Questions on the perceived condition
of buildings, staffing levels and quality of care were hypothesized to correspond to the
more cognitive concerns. Questions on whether medical staff take complaints
seriously, keep patients fully informed and respond to their views on their treatment
concern the extent to which the system respects the patient as a person and correspond
to the affective issues. We hypothesize that the cognitive and affective concerns are
distinct and independent, but that both contribute to trust and satisfaction in the NHS.
Table 1 gives net attitude (the difference between positive and negative views) for
each variable. It should be noted that, for the first group, dealing with care issues,
higher scores reflect greater commitment. Conversely, higher scores imply a
perception of low quality provision for the second group, which deals with the
measures of objective quality,.
In relation to most aspects of care views are positive. Interestingly, there is
considerable concern about buildings and staffing levels but much less so about the
quality of provision. Perhaps the most striking feature of Table 1 is that concerns
about objective features of quality have grown much stronger over time and are
highest in relation to staffing levels. In relation to care, perceptions are generally
positive and have improved somewhat. The main problems with the NHS in relation
to service-user trust and satisfaction are likely to result from perceptions of the
objective standard of provision. The 2005 data is not yet available but early analysis
suggests that both trends have now halted. Concerns about care are growing
stronger.2

18
To investigate the structure of perceptions further, principal component analyses were
carried out on the datasets for 2001 and 2003. These generated two distinct factors
for each year, one corresponding to the more subjective issues of the extent to which
the service presents a caring face to users, and the other to the more objective,
cognitive issues of quality of service (Table 2). This indicates that the two aspects of
perceptions of the service discussed above are present and distinct in the public mind,
as the earlier discussion of trust suggests. We then examined the relation between
these factors and public trust and satisfaction with the service. Variables to represent
the two components were constructed by summing factor loadings, reversing the
scoring for the quality variable. The two indices were then recoded as dichotomous
variables and introduced as independent variables in logistic regression models in
which measures of overall trust and of satisfaction with the health service were the
dependent variables. The statistics given in Table 3 are odds ratios which indicate the
likelihood of someone with the relevant characteristic displaying trust or satisfaction
in the NHS compared with someone without it.
Previous work demonstrates that demographic and attitudinal factors relate to
satisfaction. Appleby and Alvarez-Rosete (2005, 132-3) show that political party
identification, age and income relate to satisfaction. Arguably, social class, education
level, newspaper readership and gender may also be relevant. The arguments of
Giddens and others reviewed earlier indicate that level of information and general
social self-confidence are important factors promoting the move away from deference
and towards critical trust. Gender (and of course age) relate to NHS use and may thus
enter. Variables representing these items were also included in the models to examine
how far the perception measures were independent from them. A full list of the
variables and their coding is given in Table 4.
The odds ratios in Table 3 indicates that the perception indices relate more strongly to
both trust and satisfaction than do the other variables. Many of the demographic and
ideological factors do not attain the five per cent significance level selected for
modelling. When they do enter, they do so in expected directions. Political party
support has the strongest showing, unsurprising since NHS reform is contentious.
The odds ratios for the care and quality indices change little when the other variables
are included, indicating that the role played by these factors does not reflect other

19
aspects of people’s social roles. The similarities between the indices for the two years
suggests that the pattern of a dual basis for satisfaction with and trust in the NHS is
not produced by short-run issues in public debate.
Differences in the contribution of the ‘care’ index (based on perceptions of how the
service treated the individual and the extent to which the service-user felt respected as
a person) and the ‘quality’ index (based on more objective perceptions of level and
quality of provision) are evident. The odds ratios for the care index are greater than
those for the quality index for trust, while the reverse is true for satisfaction. This
finding supports the view discussed earlier that trust is based both on perceptions of
care – of ‘having the service-users interests at heart’, and on perceived, objective,
cognitively-relevant factors, such as quality of provision These factors also enter into
satisfaction, but, following the political debate, the objective standards here play a
stronger role.
A further possibility is that these different aspects of perception might operate in
different ways for different demographic and ideological groups. Those on the
political left or working class people, who might feel less able to assert their interests,
might be more concerned, for example, about the extent to which the service presents
itself as caring. Alternatively, concerns about care and objective quality might be
more evenly spread across the population as the idea of the NHS as a universal
service implies. This is reinforced by the view discussed earlier, that the increased
concern with trust which focuses attention on these issues as separate factors, results
from general social changes and not from factors affecting specific groups. Table 5
presents logistic regression models which develop this idea, by regressing the
variables representing the care and quality indices on the range of demographic and
ideological variables listed in Table 4 for 2001 and 2003.
The most striking feature of the models presented is the low r squared statistics (0.04
or below), indicating weak linkage between the perceptions and the social groups.
There is some indication that older people are more inclined to higher trust and
satisfaction, as pervious work shows (Appleby and Alvarez-Rosete, 2004, 132;
Poortinga and Pidgeon 2003; Taylor-Gooby 2006). Positive views on quality seem to
be related in a general way to social class, indicated by routine manual working class

20
occupation, lack of educational qualifications and not reading a broadsheet newspaper.
In general, the models indicate that the perceptions of care and quality are shared
across most population groups, although there are some minor differences amongst
them. They are thus appropriately treated as independent variables. The perceptions
which form the basis of trust in the NHS are unlikely to be linked to the specific
interest of a particular social group.
The statistical analysis is hampered by the limitations on data. Trust questions were
asked only in 2001, the survey does not repeat the satisfaction questions in 2004 and
data for later years is not yet publicly available. The findings indicate a clear
distinction between perceptions of care and of objective quality, which both
contribute to trust in the service and to satisfaction with it in the way suggested by the
earlier theoretical discussion. These perceptions play a strong role in influencing trust
and satisfaction compared to the demographic and party politics variables.
Perceptions of care contribute more strongly to trust and perceptions of quality are
slightly more influential in relation to satisfaction. These perceptions appear broadly
spread through the population and not to be closely tied to any demographic or social
grouping or political allegiance, so that they can be seen to reflect aspects of public
discourse rather than interest. Views on the level of care in the NHS seem generally
positive and to be improving slightly, while those on quality of service to be
deteriorating, up to 2003, with an indication of a later reversal.
Conclusions
Welfare states are everywhere undergoing reform, for excellent reasons. The major
challenges to the sustainability of the traditional patterns of state provision from a
variety of directions - labour market, demographic and household shifts, post-
industrialism, globalisation, rising expectations, the declining authority of national
governments, the challenges posed by demands for greater equality by women,
migration and the new politics – require radical new approaches. One shift,
emphasized in policy debate at the EU level, is towards activation through measures
to encourage a greater mobilisation of the population into paid work and in some

21
cases to improve the value added by that labour. Another, of considerable
significance in the UK but also emerging in other European countries, is the shift
towards a New Public Management, involving the introduction of more rigorous
performance management and of quasi-markets into the state sector. Developments in
the UK NHS – an archetypal traditional state sector service from which improvements
in cost-efficiency are required in a context of ever-rising demand and a high degree of
politicisation of debate – provide a good opportunity to examine the implications of
these changes.
Sociological, psychological and political science research has identified a trend away
from deferential acceptance of authority and towards a more critical and sceptical
attitude to officials, experts, professionals and institutions in the state sector and
outside. Other streams of work in sociology, psychology and economics emphasize
the growth of uncertainty in social life just at the time when these established
authorities are called into question. It is often argued that trust, if it can be secured,
provides a valuable support for the pursuit of objectives that involve interaction with
others or with institutions under conditions where certainty is in short supply. Much
analysis suggests that trust is best thought of as derived from two analytically separate
bases: cognitive, deliberative, rational consideration of track-record, based on good
information, and a more affective acceptance that the trustee shares values and
interests with the trustor – reason and emotion.
Evidence from the 2001 and 2003 British Social Attitudes surveys, although limited
by short-comings in the data, indicates that both trust and satisfaction in the NHS in
recent years appear strongly influenced by perceptions that reflect these two
approaches, care playing a stronger role for trust and quality for satisfaction. Current
directions in reform, however, deploy rational incentives through rewards for meeting
targets and through quasi-markets, placing an exclusive stress on the first approach.
They have apparently been successful in raising standards in a number of areas. The
improvements in output are driven by an apparatus that inevitably and publicly
focuses the interests of providers upwards to those setting the targets for performance
management and to the incentives they experience as actors in a fine-tuned quasi-
market system. Service-users are more likely to experience the service as something
that may meet their needs, but does not have within its management a mechanism to

22
care for them as persons or reflect their concerns. The developments of the early
2000s were associated with perceptions of improvements in care, but, interestingly, a
deterioration in those for quality. The reforming NHS has managed to retain the care
component of trust and satisfaction, although both appear to be at a relatively low
level. Whether this will continue, and whether extra investment and further
improvement in output can retrieve the objective quality component remains to be
seen. The most recent attitude survey data suggests that this is not the case, and that
the more subjective aspect of satisfaction may now be in decline.
The policies necessary to preserve state welfare require developments that may
alienate service-users. One possibility is that citizens are likely to become less
trusting over time and that this may affect the long-term political sustainability of the
new welfare state settlement. It is frustrating for policy-makers to find that laborious
reforms that actually improve objective levels of provision do not gain the extra trust
or public satisfaction that such changes, achieved under very difficult circumstance,
might be thought to merit. It would be ironic if the processes that were anticipated to
render state welfare services sustainable in the face of current challenges resulted in a
destabilising of the system through an erosion of trust, caused by the same
mechanisms that improved the quality of output.

23
Figure 1: Public spending – selected services (% gdp)
0
3
6
9
12
15
18
1996 1997 1998 1999 2000 2001 2002 2003 2004
Health Education Social Protection
Health % state spend Edn % state spend
24
Figure 2: Net Satisfaction with NHS Overall, Inpatients and Outpatients (BSA: Satisfaction minus dissatisfaction)
-15
-5
5
15
25
35
45
1996 1997 1998 1999 2000 2001 2002 2003 2004
NHS overall Inpatients Outpatients GPs
25
Table 1: Developments in NHS Perceptions: Care and Quality, 1997-2003 Care 1998 1999 2000 2001 2003 2004 (‘Definitely’ + ‘probably’ would) – (‘probably’ +
‘definitely’ would not) Doctors tell you all you need to know
46 * 44 43 50 *
Doctors take your views on treatment seriously
32 * 24 26 37 *
Nurses take any complaint seriously
47 * 54 56 56 *
Doctors take any complaint seriously
49 * 44 50 54 *
Particular nurse to deal with problems
14 * 15 13 16 *
Objective quality (In need of ‘some’ + ‘a lot of’ improvement) – (‘satisfactory’ + ‘very good’)
Condition of hospital buildings 0 -8 * 16 * 26 Staffing level: nurses 44 42 * 62 46 * Staffing level: doctors 41 43 * 61 50 * Quality of medical treatment in hospital
-27 -34 * 8 10 *
Quality of nursing care in hospital
-34 -41 * -2 -2 *
* not included in the relevant annual survey.

26
Table 2: Factor Analysis of Perceptions of the NHS, BSA 2001 and 2003, Varimax rotation 2001 2003 Care Doctors tell you all you need to know
-.13 .71 -.08 .63
Doctors take your views on treatment seriously
-.08 .76 -.03 .67
Nurses take any complaint seriously
-.12 .74 -.05 .73
Doctors take any complaint seriously
-.12 .81 -.04 .74
Particular nurse to deal with problems
-.14 .52 -.02 .49
Quality Condition of hospital buildings*
.69 -.07 - -
Staffing level: nurses .84 -.05 .88 .02 Staffing level: doctors .85 -.07 .90 .02 Quality of medical treatment in hospital
.74 -.25 .88 -.13
Quality of nursing care in hospital
.70 -.26 .86 -.15
Eigenvalue 3.80 1.91 3.24 2.08 % total variance explained 38.00 19.09 36.03 23.09 N 1806 1848 * not included in 2003 survey.

27
Table 3: Logistic Regressions on Trust and Satisfaction (2001) and Satisfaction (2003): Odds ratios 2001 2003 Trust Satisfaction Satisfaction Care 2.27** 2.24** 2.40** 2.39** 2.22** 2.19** Quality 1.68** 1.68** 2.59** 2.72** 3.52** 3.62** 55 or older 1.67** 1.46** 35 or younger
1.46**
Professional/managerial
.80** .73**
Labour party support
1.62** 1.63**
Liberal party support
1.64**
Woman 1.27* Constant 1.22** 1.64** .54** .57** .35** .56** Nagelkerke r square
.10 .07 .15 .13 .19 .17
% correct predictions
62.1 62.5 60.5 67.5 57.7 57.4
Chi-squared
114.61** 82.17** 181.76** 152.06** 237.35** 253.13**
N 1526 1526 1574 1574 1547 1547 * significant at 5% level
** significant at 1% level

28
Table 4: Variables used in the regression (recoded for use in the dichotomous logistic model) Trust in the NHS (a great deal or quite a bit) 58.7% - Satisfaction with the NHS (very or quite satisfied) 39.2% 43.7% Care index (above the mean) 46.3% 41.0% Quality index (above the mean) 49.4% 44.0% Age: >54 33.1% 34.5% Age: <36 26.3% 29.2% Salariat: Professional/managerial 33.1% 29.7% Routine: Semi/unskilled working class 31.6% 28.9% Household income top quartile 19.8% 22.1% Household income bottom quartile 24.9% 25.2% Gender: woman 54.2% 53.3% Tabloid reader 37.7% 34.7% Broadsheet reader 11.9% 11.1% Education to degree level 15.7% 15.9% No educational qualifications 25.3% 24.7% Conservative voter 23.0% 25.2% Labour voter 44.7% 37.2% Liberal voter 12.9% 10.8%

29
Table 5: Logistic Regressions on Care and Quality Indices (2001 and 2003): Odds ratios 2001 2003 Care Quality Care Quality 55 or older 1.34** 1.44** 1.38** Professional/managerial 1.31* Routine working class 1.32* Conservative party support .79* Woman .75** Broadsheet newspaper reader .61** No educational qualifications 1.39* 1.58** Constant 1.107 .85** 1.33** .68** Nagelkerke r squared .01 .03 .01 .04 % correct predictions 53.7 50.6 59.3 55.6 Chi-squared 9.51** 35.81** 5.90* 50.77** N 1580 1580 1547 1547 * significant at 5% level
** significant at 1% level

30
References Alesina, A and Glaeser, E (2004), Fighting Poverty in the US and Europe, Oxford: Oxford University Press. Almond, G. and Verba, S. (1963) The Civic Culture, Princeton University Press. Appleby, J. and Alvarez-Rossete (2005) ‘Public responses to NHS reform’, Park A. et al. British Social Attitudes, Sage, London Barbalet, J, (2002) Emotions and Sociology. Blackwell Press, Oxford. Barr, N. (1998) The Economics of the Welfare State, Oxford University Press, Oxford. Bauman, Z. (2000) Liquid Modernity, Polity Press, Cambridge. Beck, U and Beck-Gernsheim, E (2002) Individualisation, Sage. Beck, U, Giddens, A, and Lash, S (1994) Reflexive Modernisation, Stanford University Press, Stanford. Bevan, G and Hood, C. (2006) ‘Have targets improved performance in the English NHS?’, BMJ, 332, 419-22. Blair, T. (1998) The Third Way, Fabian Society London. Bonoli, G. (2005) ‘The politics of the new social policies’, Policy and Politics, 33, 3, 431-49. Bonoli, G. and Powell, M. (eds. 2003), Social Democratic Party Policies in Contemporary Europe, London: Routledge Calnan, M. and Rowe, R. (2005) Trust relations in the NHS, SCARR Trust Conference, London, 12.12.05. Coleman, J. (1986) Individual Interests and Collective Action, Cambridge University Press. COSU (2002) Risk, Cabinet Office Strategy Unit, London. Crasswell, R. (1993) ‘On the uses of trust’, The Journal of Law and Economics, 36, 1, 487-500. Curtice, J. and Seyd, B. (2003) ‘Is there a crisis of political participation?’ in Park, A et al, (eds) British Social Attitudes, the 20th Report, Sage, London. Cvetkovich, G. and Earle, T. (1997) ‘Culture, cosmopolitanism and risk management’, Risk Analysis, 17, 1, 55. Dahrendorf, R (1990) Reflections on the Revolutions in Europe, Times Books, New York. Damasio, Antonio (1996). Descartes' Error, Macmillan. Das, T. and Teng, B. (2004) ‘The risk-based view of trust’ Journal of Business and Psychology, 19, 1, 85-116. Dasgupta , P. (1988) Trust as a commodity’ in Gambetta op cit. Dasgupta , P. (2002) ‘Social Capital and Economic Performance’ Dept of economics, University of Cambridge. Davies, H. (1999) ‘Falling public trust in health services’, Jnl Health Services Research Policy, 4, 4, 193-4. Dean, M. (1999) Governmentality, London: Thousand Oaks. DH (1997) The New NHS, cm 3807, HMSO, London. DH (2006) Our Health, Our Care, Our Say, Cm 6737, HMSO, London. Dixit, A. (2002) ‘ Incentives and organisations in the public sector’, Journal of Human Resources, vol 37, 696-727. DTI (2005) Science in Society: Findings from Qualitative and Quantitative Research, HMSO. Eiser, R., Miles, S. and Frewer, L. (2002) ‘Trust, perceived risk and attitudes towards food technologies’, Journal of Applied Social Psychology, 32, 11, 2423-34. Epstein, S (1994)‘Integration of the cognitive and the psychodynamic unconscious’ American Psychologist, 49, 709-24. Esping-Andersen, G (1996) Welfare States in Transition, Sage Ewald, F. (1986) L' État Providence, Paris: Grasset. Finucane, M. and Holup, J (2006) ‘Risk as value’, Journal of Risk Research, 9, 2, 141-64. Frewer, L. J., Howard, C., Hedderley, D. and Shepherd, R. (1996). ‘What determines trust in information about food-related risks?’ Risk Analysis, 16(4), 473-485. Fukuyama, F. (1996) Trust, Hamish Hamilton, London. Gambetta, D. (1988) Trust, Oxford University Press. Giddens, A (1994) Beyond Left and Right, Cambridge: Polity Press. Giddens, A. (1998) The Third Way, Polity Press, Cambridge. Glaser, J and Salovey, P (1998) ‘Affect in Electoral Politics’, Personality and Social Psychology Review, 2, 3, 156-72. Glennerster, H. (1997) Paying for Welfare, Prentice Hall, London.

31
Gough, I (2001) ‘Globalisation and welfare regimes: the East Asian case’ Global Social Policy, vol 1, no 2, 163-89. Habermas, J. (1976) Legitimation Crisis, Heineman, London. Held, D (2002) Democracy and the Global Order, Polity Press, Cambridge. Hobson-West, P (2004) ‘Understanding vaccination resistance’ Health, Risk and Society, 5, 3 273-83. Hovland, C., Janis, I. and Kelley, H. (1953) Communication and Persuasion, New Haven, Yale University Press. Huber, E and Stephens, J (2001) Development and Crisis of the Welfare State, Chicago University Press, Chicago. Inglehart, R. (1999) ‘Trust, Well-being and Democracy’, in Warren, M. ed Democracy and Trust CUP, Cambridge. Iversen, T. and Wren, A. (1998) ‘Equality, Employment and Budgetary Restraint’, World Politics, 50, 4, 507-46. Jessop, B (2002) The Future of the Capitalist State, Cambridge University Press, Cambridge. Keynes, J.M., (1936) The General Theory of Employment, Interest and Money, Macmillan, London. Kings Fund (2005) NHS Funding, Kings Fund, 1.4.05. Klein, R. (1996) ‘The NHS reforms revisited’, British Medical Journal, 313, 504-5. Le Grand, J and Bartlett, W (1993) Quasi-Markets and Social Policy, Macmillan, Basingstoke. Le Grand, J. (2003) Motivation, Choice and Public Policy, Oxford University Press, Oxford. Levi, M. and Stoker, L. (2000) ‘Political Trust and Trustworthiness’, Annual Review of Political Science 3, 475-507. Luhmann, N. (1979) Trust and Power, John Wiley, New York. Lupton, D. (1994): Risk London: Routledge and Kegan Paul. Marcus, G (2002) The Sentimental Citizen, Penn State University, Pennsylvania Marquand, D and Crouch, C (eds. 1995) Reinventing Collective Action, Blackwell, Oxford. McNamara, K. (1998) The Currency of Ideas, Cornell UP, Ithaca/London. Metlay, D. (1999). ‘Institutional trust and confidence’ in G. T. Cvetkovich, & R. E. Löfstedt (Eds.), Social Trust and the Management of Risk, London: Earthscan. MORI (2003) Trust in the Government Low, press release, 23.1.03, Market and Opinion Research International. Mueller, D. (1979) Public Choice, Cambridge University Press, Cambridge. Neuberger, J (2005) The Moral State We’re In, Harper Collins/IPPR, London. Niskanen, W. (1971) Bureaucracy and Representative Government, Aldine-Atherton, Chicago. Norris, P. (1999 ed) Critical Citizens, Oxford University Press. Nye, J., Zelikow, P. and King, D. (1997) Why People Don’t Trust Government, Harvard University Press, Harvard. O’Malley, P. (2000) ‘Uncertain subjects: risks, liberalism and contract’ Economy and Society 29, 4, 460-484. O’Neill, O. (2002) A Question of Trust (Reith Lectures), Cambridge, Cambridge University Press. OECD (2001) Citizens as Partners, OECD, Paris. OECD (2005) Extending Opportunities: How active social policy can benefit us all - Final Communiqué. Meeting of OECD Social Affairs Ministers Ostrom, E. and Walker, J. (editors, 2002) Trust and Reciprocity, Russell Sage Foundation Page, B. (2004) Understanding and Perception of the NHS, May, MORI. Park, A, (2002) ‘Technical details’ in Park A. et al. (2002) British Social Attitudes, 19th report, Sage, London. Petts, J. (1998) ‘Waste management and remediation services’, Journal of Risk Research, 1, 4, 307-21 Petts, J., Horlick-Jones, T. and Murdock, G. (2001) Social Amplification of Risk, Research report 329/01, Health and Safety Executive, London. Pidgeon, N., Hood, C., Jones, D., Turner, B. and Gibson, R. (1992) ‘Risk perception’ in Royal Society Group on Risk Assessment, Analysis, Perception and Management, Royal Society, London. Pidgeon, N., Kasperson, R. and Slovic, P. (2003) The Social Amplification of Risk, Cambridge University Press, Cambridge. Pierson, P (2001) The New Politics of the Welfare State, Oxford University press, Oxford. Pixley, J. (2004) Emotions in Finance, Cambridge University Press, Cambridge. Poortinga, W. and Pidgeon, N. (2003) ‘Exploring the dimensionality of trust in risk regulation’, Risk Analysis, 23, 5, 961-73. Power, M (2004) The Risk Management of Everything, Demos, 2004). Pratt, J., and R. Zeckhauser (1985). Principals and agents, Boston: Harvard Business School Press Putnam, R. (1993), Making Democracy Work, Princeton University Press.

32
R.Saltman, J.Figueras and C.Sakellarides (1998) Critical Challenges for Health Care Reform in Europe, WHO . Rayner, S (2004) ‘The novelty trap’ Industry and Higher Education, Dec. 349-55. Renn, O. and Levine, D. (1991) ‘Credibility and trust in risk communication’ in Kasperson, R. and Stallen, P.-J. (eds.) Communicating Risks to the Public, Kluwer, Dordrecht. Renn, O. and Levine, D. (1991) ‘Credibility and trust in risk communication’ in Kasperson, R. and Stallen, P.-J. (eds.) Communicating Risks to the Public, Kluwer, Dordrecht. Rhodes, R. (1997) Understanding Governance, Open University Press, Milton Keynes. Riker, W. (1986) Liberalism Against Populism, San Francisco: Freeman Robinson, J. (1964) Economic Philosophy, Penguin, Harmondsworth. Rothstein, H., Huber, M. and Gaskell, G. (2006) ‘A theory of risk colonization’, Economy and Society, 35, 1, 91-112. Rousseau, D., Sitkin, Sim B., Burt, Ronald S., Camerer, C. (1998), ‘A Cross-Discipline View Of Trust’, Academy of Management Review, 23, 3. Rowe R. (2004) Trust in Health Care: A review of the literature, Nuffield Foundation, London. Royal Society (1997) Science Policy and Risk, London. Scharpf, F (1999) Governing in Europe, Oxford University Press, Oxford. Scharpf. F, and Schmidt V. (2000, eds.), Welfare and Work in the Open Economy: Diverse Responses to Common Challenges, Oxford: University Press. Schwarz, N. 2000. ‘Emotion, Cognition, and Decision Making’ Cognition and Emotion, 14, 4, 433-440. Seligman, H. (2000) The problem of Trust, Princeton University Press, Princeton. Slovic, P, Finucane, M, Peters, E and MacGregor D (2004) ‘Risk as Analysis and Risk as Feelings’ Risk Analysis, 24, 2 Slovic, P. (2000) The Perception of Risk, Earthscan, London. Slovic, P. (2001) Smoking, Risk Perception and Policy. Sage, London. Sourcewatch (2006) ‘National debate on nuclear power, 2005-6’ (http://www.sourcewatch.org) consulted 9/1/06 Sztompka, P. (1998) Trust, Cambridge University Press, Cambridge. Taylor-Gooby, P. (2006) ‘New approaches to expert and institutional trust’, Jnl Risk Research, 9, 1, 79-95. Taylor-Gooby (2004) New Risks, New Welfare, Oxford University Press, Oxford. Taylor-Gooby, P., Hastie, C. and Bromley, C. (2003) 'Querulous Citizens’, Social Policy and Administration, vol 37 no 1, 1-20. Temko, N. and Revill, J., 2.4.06, ‘Brown’s Guru Rebukes NHS’ Observer newspaper. Ticoll, D. and Tapscott, D. (2003) The Naked Corporation, Simon and Schuster. Timmins, N. (2006) ‘NHS set to miss target on waiting times’ Financial Times 4.1.06 Todd, P., and Gigerenzer G. (2003) ‘Bounding rationality to the world’, Journal of Economic Psychology 24 (2003) 143–165. Treasury (2005) Public Expenditure Statistical Analysis 2005, Treasury web-site. Treasury (2005b) Public Services Targets and Performance, (http://www.hm-treasury.gov.uk/performance) consulted 9.01.06. Tulloch, J. and Lupton, D. (2003) Risk and Everyday Life, Sage, London. Weyman, A. and Kelly, C. (1999) Risk Perception and Communication: a review of the literature, Health and Safety Executive, research report, 248/99. 1 The British Social Attitudes survey is an annual attitude survey conducted since 1983 by the National Centre for Social Research with a large national stratified random sample and high professional standards. The 2001 survey generated a sample of 3287 with a response rate of 70 per cent. Further details are given in the technical report (Park et al, 2002, pp 231-46). The analysis discussed here refers to 1515 respondents, since it uses material from sections of the questionnaire directed to a random sub-sample of respondents. The 2003 survey sample was 4,432 with a response rate of 65 per cent. The analysis discussed refers to 1547 respondents (Park et al, 2004, p224). 2 Communication from NatCen


















