A Combined Branched Stent Grafting Technique to Reconstruct Total Aortic Arch in the Treatment of...
3
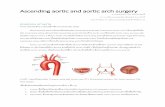
A Combined Branched Stent Grafting Technique to Reconstruct Total Aortic Arch in the Treatment of Stanford A Aortic Dissection Zhong-Ya Yan, MD, Yun-Hua Shen, MD, Qing-chun Zhang, MD, Zheng-Yan Zhu, MD, Hong Lei, MD, Guang-Cun Cheng, MD, Zhong Lu, MD, Yu Yan, MD, and Luan Wang, MD Department of Cardiac Surgery, AnHui Provincial Hospital, Anhui Medical University, Hefei, Anhui, China Traditional total arch replacement technology and artifi- cial blood vessels are designed for patients with Stanford A aortic dissection who have 3 branches (brachiocephalic trunk, left common carotid artery, and left subclavian artery) arising from the arch of the aorta. However, if there is anatomical variation of the aortic arch branches, the operation will be very difficult. The number of primary branches of the aortic arch can be reduced to 1 or 2 or increased to 4 to 6. Also, anastomoses of the graft to the left subclavian artery and descending aorta are usually very difficult because of the deep surgical field. Moreover, once bleeding occurs after the anasto- moses, hemostasis in the deep field is difficult. Therefore, we applied a “combined branched” stent grafting tech- nique for total arch reconstruction to reduce such problems. (Ann Thorac Surg 2013;96:1888–90) Ó 2013 by The Society of Thoracic Surgeons I n traditional total arch replacement for Stanford A aortic dissection, anastomoses of the graft to the left subclavian artery and descending aorta are often very difficult. Once bleeding occurs after the anastomoses, hemostasis in the deep field is difficult. Moreover, manipulations of the arch and anastomoses are more difficult when there is anatomical variation of aortic arch branches. The number of primary branches of the aortic arch can be reduced to 1 or 2 or increased to 4 to 6 [1, 2]. To reduce such problems, we applied a “combined branched” stent grafting technique to reconstruct total aortic arch in the treatment of Stanford A aortic dissec- tion. With open placement of our single-branched stent graft and branched stent grafts into the open descending aorta and arch vessels, we avoided the distal anastomosis at the descending aorta. Using this technique, total arch replacement may become easier, safer, and more widely used for Stanford A aortic dissection. Technique Stent Graft The single-branched stent graft (Yuhengjia Science and Technology Co Ltd, Beijing,China) (Fig 1A) consists of a conventional straight aortic stent graft and a sidearm stent graft. The conventional straight aortic stent graft was 130 to 170 mm long and 26 to 32 mm in diameter. It consisted of a zigzag self-expandable nitinol stent and a high-porosity woven polyester graft. The sidearm stent graft was 23 to 32 mm long and 12 to 18 mm in diameter, and it consisted of a self-expanding nitinol stent and polyester graft. The stent graft that was implanted into the arch vessel stump was 20 to 30 mm long and 12 to 18 mm in diameter (Fig 1B); it consisted of a self-expanding nitinol stent and polyester graft (Yuhengjia Science and Technology Co Ltd, Beijing, China). Operative Technique The ascending aorta and arch were approached through a median sternotomy. Cardiopulmonary bypass was established by 2 venous cannulas through the right atrium and femoral arterial cannulation. Myocardial protection was achieved by multiple administrations of histidine-tryptophan-ketoglutarate solution. During core cooling, the innominate and left common carotid arteries were dissociated and exposed as much as possible. The ascending aorta was clamped at the base of the innominate artery (Fig 2A). Proximal manipulations such as aortic valve repair and sinus of Valsalva reconstruction were performed. The transected proximal stump of the ascending aorta was reconstructed with a polyester tube graft (Fig 2B). When core cooling to a 16 C rectal temperature was achieved, selective antegrade cerebral perfusion through the right subclavian artery was established, and perfusion to the lower body was discontinued. Through the transverse incision, the main graft of the single-branched stent graft was inserted into the true lumen of the arch and descending aorta, and the sidearm graft was positioned in the left subclavian artery (Fig 2C). Once both sections of the main graft and sidearm graft were properly positioned, the restraining strings were Accepted for publication April 15, 2013. Address correspondence to Dr Yan, Department of Cardiac Surgery, AnHui Provincial Hospital, Anhui Medical University, Hefei, Anhui, 230001, China; e-mail: [email protected]. Ó 2013 by The Society of Thoracic Surgeons 0003-4975/$36.00 Published by Elsevier Inc http://dx.doi.org/10.1016/j.athoracsur.2013.04.112 FEATURE ARTICLES
Transcript of A Combined Branched Stent Grafting Technique to Reconstruct Total Aortic Arch in the Treatment of...

FEATUREARTIC
LES
A Combined Branched Stent Grafting Technique toReconstruct Total Aortic Arch in the Treatment ofStanford A Aortic DissectionZhong-Ya Yan, MD, Yun-Hua Shen, MD, Qing-chun Zhang, MD, Zheng-Yan Zhu, MD,HongLei,MD,Guang-CunCheng,MD,ZhongLu,MD,YuYan,MD, andLuanWang,MDDepartment of Cardiac Surgery, AnHui Provincial Hospital, Anhui Medical University, Hefei, Anhui, China
Traditional total arch replacement technology and artifi-cial blood vessels are designed for patients with StanfordA aortic dissection who have 3 branches (brachiocephalictrunk, left common carotid artery, and left subclavianartery) arising from the arch of the aorta. However, ifthere is anatomical variation of the aortic arch branches,the operation will be very difficult. The number ofprimary branches of the aortic arch can be reduced to 1or 2 or increased to 4 to 6. Also, anastomoses of the
Accepted for publication April 15, 2013.
Address correspondence to Dr Yan, Department of Cardiac Surgery,AnHui Provincial Hospital, Anhui Medical University, Hefei, Anhui,230001, China; e-mail: [email protected].
� 2013 by The Society of Thoracic SurgeonsPublished by Elsevier Inc
graft to the left subclavian artery and descending aortaare usually very difficult because of the deep surgicalfield. Moreover, once bleeding occurs after the anasto-moses, hemostasis in the deep field is difficult. Therefore,we applied a “combined branched” stent grafting tech-nique for total arch reconstruction to reduce suchproblems.
(Ann Thorac Surg 2013;96:1888–90)� 2013 by The Society of Thoracic Surgeons
n traditional total arch replacement for Stanford A
Iaortic dissection, anastomoses of the graft to the leftsubclavian artery and descending aorta are often verydifficult. Once bleeding occurs after the anastomoses,hemostasis in the deep field is difficult. Moreover,manipulations of the arch and anastomoses are moredifficult when there is anatomical variation of aortic archbranches. The number of primary branches of the aorticarch can be reduced to 1 or 2 or increased to 4 to 6 [1, 2].To reduce such problems, we applied a “combinedbranched” stent grafting technique to reconstruct totalaortic arch in the treatment of Stanford A aortic dissec-tion. With open placement of our single-branched stentgraft and branched stent grafts into the open descendingaorta and arch vessels, we avoided the distal anastomosisat the descending aorta. Using this technique, total archreplacement may become easier, safer, and more widelyused for Stanford A aortic dissection.Technique
Stent GraftThe single-branched stent graft (Yuhengjia Science andTechnology Co Ltd, Beijing,China) (Fig 1A) consists ofa conventional straight aortic stent graft and a sidearmstent graft. The conventional straight aortic stent graftwas 130 to 170 mm long and 26 to 32 mm in diameter. Itconsisted of a zigzag self-expandable nitinol stent anda high-porosity woven polyester graft. The sidearm stent
graft was 23 to 32 mm long and 12 to 18 mm in diameter,and it consisted of a self-expanding nitinol stent andpolyester graft.The stent graft that was implanted into the arch vessel
stump was 20 to 30 mm long and 12 to 18 mm in diameter(Fig 1B); it consisted of a self-expanding nitinol stent andpolyester graft (Yuhengjia Science and Technology CoLtd, Beijing, China).
Operative TechniqueThe ascending aorta and arch were approached througha median sternotomy. Cardiopulmonary bypass wasestablished by 2 venous cannulas through the rightatrium and femoral arterial cannulation. Myocardialprotection was achieved by multiple administrationsof histidine-tryptophan-ketoglutarate solution. Duringcore cooling, the innominate and left common carotidarteries were dissociated and exposed as much aspossible. The ascending aorta was clamped at thebase of the innominate artery (Fig 2A). Proximalmanipulations such as aortic valve repair and sinus ofValsalva reconstruction were performed. The transectedproximal stump of the ascending aorta wasreconstructed with a polyester tube graft (Fig 2B).When core cooling to a 16�C rectal temperature wasachieved, selective antegrade cerebral perfusionthrough the right subclavian artery was established,and perfusion to the lower body was discontinued.Through the transverse incision, the main graft of thesingle-branched stent graft was inserted into the truelumen of the arch and descending aorta, and the sidearmgraft was positioned in the left subclavian artery (Fig 2C).Once both sections of the main graft and sidearm graftwere properly positioned, the restraining strings were
0003-4975/$36.00http://dx.doi.org/10.1016/j.athoracsur.2013.04.112

Fig 1. Stent grafts. (A) Single-branched stentgraft. (B) Small stent grafts.
1889Ann Thorac Surg HOW TO DO IT YAN ET AL2013;96:1888–90 BRANCHED STENT GRAFT FOR ARCH RECONSTRUCTION
withdrawn. After having measured the diameter anddistance of the other 2 arch vessels, 2 branched stentgrafts (10% to 20% bigger than the diameters of thearch vessels) were inserted into the true lumen of theother arch vessels (Fig 2D). Two holes with diametersof 12 to 18 mm were then made at the correspondingposition of the main body of the single-branchedstent graft. The 2 branched stent grafts were
anastomosed to the 2 holes in an end-to-side fashionwith 4-0 polypropylene suture (Fig 2E). In this way,a combined branched stent graft was made. Finally, thedistal end of the polyester tube graft was anastomosedto the proximal end of the combined branched stentgraft in an end-to-end fashion (Fig 2F). The air wascarefully flushed from the combined branched stentgraft when blood flow from the femoral and right
Fig 2. Schematic diagram of the operation.(A) Ascending aorta was transected at thebase of the innominate artery. (B) Thetransected proximal stump of ascending aortawas reconstructed with polyester tube graft.(C) The single-branched stent graft wasinserted and deployed into open descendingaorta and left subclavian artery. (D) Twobranched stent grafts were inserted into thetrue lumen of the other 2 arch vessels. (E) The2 branched stent grafts were anastomosed tothe single-branched stent graft in an end-to-side fashion. (F) Finally, the distal end of thepolyester tube graft and the proximal end ofthe combined branched stent graft wereanastomosed in an end-to-end fashion.
FEATUREARTIC
LES

1890 HOW TO DO IT YAN ET AL Ann Thorac SurgBRANCHED STENT GRAFT FOR ARCH RECONSTRUCTION 2013;96:1888–90
FEATUREARTIC
LES
subclavian arteries was restored. Antegrade systemicperfusion from the branch was then started, and thepatient was rewarmed.
Comment
From August 2010 to September 2012, the combinedbranched stent graft placement technique was used in 10consecutive patients in our department (6 men and 4women; mean age, 46.4 � 10.01 years; range, 32-61 years).All patients were classified as having Stanford A aorticdissection. Placement of the single-branched stent graft and2 branched stent grafts into the true lumen of the proximaldescending aorta, arch, and 3 arch vessels was technicallysuccessful in all 10 patients. The mean cardiopulmonarybypass time was 173.90 � 9.31 minutes, aortic cross-clamptime was 89.80 � 7.04 minutes, and selective cerebralperfusion and lower body arrest time was 43.90 � 6.35minutes. No patient required a reopening of the chest tocorrect excessive postprocedural bleeding. Postoperativehoarseness did not occur. Therewere no late deaths or needfor reoperation. All patients were given prospective follow-up by means of aortic computed tomographic angiographybefore discharge and 3months after the operation. The first
Fig 3. Postoperative computed tomographic scan showing that allstent grafts were fully open, and there was no space or blood flowsurrounding the stent grafts.
postoperative aortic computed tomographic angiogram(Fig 3)showed that all stent grafts were fully open and notkinked and that there was no space or blood flowsurrounding the single-branched stent grafts and 2branched stent grafts. All patients resumed normal lives.With open placement of our single-branched stent graft
and small stent grafts, and with the anastomosis of the 2small stent grafts to a single-branched stent graft in an end-to-side fashion, we avoided anastomoses of the archvessels and distal anastomosis at the descending aorta.Weperformed the distal aortic anastomosis at the proximalarch at the base of the innominate artery, which provideda better surgical view, and the anastomosis and hemostasiswere much easier to perform than with traditional totalarch replacement. Placement of the single-branched stentgraft in the descending aorta and the left subclavian arterywas easily completed in 1 to 2 minutes. During thisprocedure, the distal arch and proximal descending aortadid not require dissection, incision, and suturing. In thisstudy, the mean cardiopulmonary bypass time, aorticcross-clamp time, and selective cerebral perfusion andlower body arrest time were lower than in the study ofSakamoto and colleagues [3] who finished the total aorticarch replacement using the 4-branched prosthetic graft(204 � 53 minutes, 136 � 43 minutes, and 83 � 14minutes, respectively).The diameters of the aortic arch and arch vessels and
the distances between 2 neighboring arch vessels aredifferent in each patient. The proper size of each stentgraft is key to quick clot formation and shrinkage of thefalse lumen and also for preventing new intimal traumaowing to the continuous compression of the oversizedstent graft on the dissected and fragile intimal wall [4]. Inthe procedure, the diameters of the single-branched stentgraft and small stents graft should be 10% to 20% biggerthan the diameters of the aortic arch and arch vessels.Moreover, the location of the holes made in the single-branched stent graft anastomosed to the correspondingsmall stent grafts should be suitable; this could avoidstent migration, distortion, and endoleak.In conclusion, open combined branched stent graft
placement is a feasible technique. With this technique,total arch replacement may become easier, safer, andmore widely used for Stanford A aortic dissection.However, rigorous long-term evaluation and furtherextensive clinical trials are necessary.
References
1. Piyavisetpat N, Thaksinawisut P, Tumkosit M. Aortic archbranches’ variations detected on chest CT. Asian Biomed2011;5:817–23.
2. Nayak SR, Pai MM, Prabhu LV, D’Costa S, Shetty P.Anatomical organization of aortic arch variations in the India:embryological basis and review. J Vasc Bras 2006;5:95–100.
3. Sakamoto S, Matsubara J, Nagayoshi Y, et al. Clinical resultsof aortic arch replacement using a four branched prostheticgraft. J Cardiovasc Surg (Torino) 2003;44:751–5.
4. Chen LW, Dai XF, Yang GF, Zhang GC, Cao H, Wang QM.Open-branched stent graft placement makes total archreplacement easier for acute type a aortic dissection. AnnThorac Surg 2010;89:1688–90.