9 Thrombosis

of 18
-
Upload
eslam-almassri -
Category
Documents
-
view
235 -
download
0
Transcript of 9 Thrombosis
-
8/3/2019 9 Thrombosis
1/18
Thrombosis
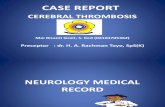
Pathogenesis There are three primary
influences on thrombus formation (called
Virchow's triad):
(1) endothelial injury
(2) stasis or turbulence of blood flow.
(3) blood hypercoagulability .
-
8/3/2019 9 Thrombosis
2/18
Virchow's triad
-
8/3/2019 9 Thrombosis
3/18
1 Endothelial Injury
This is a dominant cause of thrombosis asendothelial loss by itself lead to thrombosis.
It is particularly important for thrombus formationoccurring in the heart or in the arterial circulation,where the normally high flow rates might otherwisehamper clotting by preventing platelet adhesion ordiluting coagulation factors. Thus, thrombus formationwithin the cardiac chambers (e.g., after endocardialinjury due to myocardial infarction), over ulcerated
plaques in atherosclerotic arteries, or at sites oftraumatic or inflammatory vascular injury (vasculitis) islargely a function of endothelial injury
-
8/3/2019 9 Thrombosis
4/18
Thrombosis in Endothelial Injury 1
physical loss of endothelium leads to exposure ofsubendothelial ECM, adhesion of platelets,release of tissue factor, and local depletion of
PGI2 and plasminogen activators. dysfunctional endothelium may elaborate greater
amounts of procoagulant factors (e.g., plateletadhesion molecules, tissue factor, plasminogen
activator inhibitors) or may synthesize feweranticoagulant effectors (e.g., thrombomodulin,PGI2, t-PA).
-
8/3/2019 9 Thrombosis
5/18
Thrombosis in Endothelial Injury 2
Significant endothelial dysfunction (in the absence
of endothelial cell loss) may occur with
hypertension ._ turbulent flow over scarred valves ._ by
the action of bacterial endotoxins.
homocystinuria, hypercholesterolemia, radiation, or
products absorbed from cigarette smoke, may be sources
of endothelial dysfunction
-
8/3/2019 9 Thrombosis
6/18
Alterations in Normal Blood Flow 1
Turbulence contributes to arterial and cardiacthrombosis by causing endothelial injury ordysfunction, as well as by forming countercurrents andlocal pockets of stasis;
stasis is a major contributor to the development ofvenous thrombi. Normal blood flow is laminar, suchthat platelets flow centrally in the vessel lumen,separated from the endothelium by a slower movingclear zone of plasma. Stasis and turbulence therefore:
Disrupt laminar flow and bring platelets into contactwith the endotheliumPrevent dilution of activatedclotting factors resulting in local thrombosis andleukocyte adhesion.
-
8/3/2019 9 Thrombosis
7/18
Alterations in Normal Blood Flow 2
Turbulence and stasis contribute to thrombosis in severalclinical settings. Ulcerated atherosclerotic plaques not onlyexpose subendothelial ECM but also cause turbulence.Abnormal aortic and arterial dilations, called aneurysms,
create local stasis and consequently a fertile site forthrombosis .
Acute myocardial infarction results in focally noncontractilemyocardium; ventricular remodeling after more remoteinfarction can lead to aneurysm formation.
In both cases cardiac mural thrombi form more easilybecause of the local blood stasis Mitral valve stenosis (e.g.,after rheumatic heart disease) results in left atrial dilation .
-
8/3/2019 9 Thrombosis
8/18
Alterations in Normal Blood Flow 3
Hyperviscosity syndromes such as
polycythemia; increase resistance to flow cause
small vessel stasis .
sickle cell anemia with the deformed red cells
cause vascular occlusions, with the resultant stasis
also predisposing to thrombosis.
-
8/3/2019 9 Thrombosis
9/18
Hypercoagulability
alteration of the coagulation pathways that
predisposes to thrombosis .
It can be divided intoprimary(genetic) . inherited causes of
hypercoagulability, mutations in the factor V gene
and the prothrombin gene are the most common.
secondary(acquired) disorders : the pathogenesisofacquired thrombotic diatheses is frequently
multifactorial and is therefore more complicated.
-
8/3/2019 9 Thrombosis
10/18
secondary (acquired)
Hypercoagulability
oral contraceptive use
the hyperestrogenic state of pregnancy, probablyrelated to increased hepatic synthesis of coagulation
factors and reduced synthesis of antithrombin III. In disseminated cancers, release of procoagulant
tumor products predisposes to thrombosis.
advancing age has been attributed to increasing
platelet aggregation and reduced endothelial PGI2release.
Smoking and obesity promote hypercoagulability byunknown mechanisms.
-
8/3/2019 9 Thrombosis
11/18
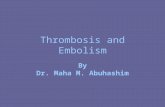
Hypercoagulability
-
8/3/2019 9 Thrombosis
12/18
Heparin-InducedThrombocytopenia
(HIT) syndrome
5% of the population
the HIT syndrome occurs when administration ofunfractionated heparin for therapeutic anticoagulationinduces autoantibodies to complexes of heparin and a
platelet membrane protein (platelet factor 4) . This antibody binds to similar complexes present on
platelet and endothelial surfaces, resulting in plateletactivation and endothelial cell injury, and a net
prothrombotic state. The occurrence ofHIT syndrome can
be reduced by using low-molecular-weight heparinpreparations that retain anticoagulant activity but do notinteract with platelets; these preparations have theadditional advantage of a prolonged serum half-life.
-
8/3/2019 9 Thrombosis
13/18
Morphology of thrombi
Thrombi can have grossly (and
microscopically) apparent laminations called
lines of Zahn; these represent pale platelet
and fibrin layers alternating with darker
erythrocyte-rich layers.
Antemortem thrombosis is distinguished
from the bland nonlaminated clots that occur
in the postmortem state.
-
8/3/2019 9 Thrombosis
14/18
Morphology and types of thrombi 1
Arterial thrombi are frequently occlusive and are produced by plateletand coagulation activation; friable meshwork of platelets, fibrin,erythrocytes, and degenerating leukocytes. Although arterial thrombi areusually superimposed on an atherosclerotic plaque, other vascular injury(vasculitis, trauma) can be involved
Venous
thrombosis (phlebothrombosis) occlusive, and the thrombus cancreate a long cast of the lumen; venous thrombosis is largely the result of
activation of the coagulation cascade, and platelets play a secondary role.Because these thrombi form in the sluggish venous circulation, they alsotend to contain more enmeshed erythrocytes and are therefore called red,or stasis, thrombi. The veins of the lower extremities are most commonlyaffected (90% of venous thromboses)
however, venous thrombi can occur in the upper extremities,periprostatic plexus, or ovarian and periuterine veins; under specialcircumstances they may be found in the dural sinuses, portal vein, orhepatic vein.
-
8/3/2019 9 Thrombosis
15/18
Morphology and types of thrombi 2
Postmortem clots : postmortem "thrombi" aregelatinous, with a dark red dependent portion wherered cells have settled by gravity, and a yellow "chickenfat cover, and they are usually not attached to the
underlying wall. In contrast, red thrombi are firmer andare focally attached, and sectioning reveals strands ofgray fibrin.
vegetations :Thrombi on heart valves. Bacterial orfungal blood-borne infections can cause valve damage,
subsequently leading to large thrombotic masses(infective endocarditis .Sterile vegetations can alsodevelop on noninfected valves in hypercoagulablestates, so-called nonbacterial thrombotic endocarditis
-
8/3/2019 9 Thrombosis
16/18
Fate of the Thrombus
Propagation. Thrombi accumulate additional plateletsand fibrin, eventually causing vessel obstruction.
Embolization. Thrombi dislodge or fragment and are
transported elsewhere in the vasculature. Dissolution. Thrombi are removed by fibrinolytic
activity.
Organization and recanalization. Thrombi induce
inflammation and fibrosis (organization). These caneventually recanalize (re-establishing some degree offlow), or they can be incorporated into a thickenedvessel wall.
-
8/3/2019 9 Thrombosis
17/18
Clinical Correlations: Venous versus
Arterial Thrombosis
Thrombi are significant because they cause obstructionof arteries andveins and are potential sources ofemboli.
Which effect is most important depends on the site of
thrombosis. Venous thrombi can cause congestion andedema in vascular beds distal to an obstruction, butthey are most worrisome for their capacity to embolizeto the lungs and cause death .
Conversely, while arterial thrombi can embolize andeven cause downstream tissue infarction their role invascular obstruction at critical sites (e.g., coronary andcerebral vessels) is much more significant clinically.
-
8/3/2019 9 Thrombosis
18/18
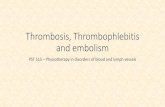
Venous Thrombosis
(Phlebothrombosis) Most venous thrombi occur in the superficial or deep veins of the
leg. Superficial venous thrombi usually occur in the saphenoussystem, particularly when there are varicosities.
Such superficial thrombi can cause local congestion, swelling, pain,and tenderness along the course of the involved vein, but they
rarely embolize. Nevertheless, the local edema and impairedvenous drainage do predispose the overlying skin to infections fromminor trauma and to the development ofvaricose ulcers. Deepthrombi in the larger leg veins at or above the knee joint (e.g.,popliteal, femoral, and iliac veins) are more serious because theymay embolize .
deep venous thromboses are entirely asymptomatic inapproximately 50% of patients and are recognized in retrospectonly after they have embolized.







![Thrombosis Class05[2]](https://static.fdocuments.in/doc/165x107/556b14a6d8b42ae47d8b5299/thrombosis-class052.jpg)