8. Progression in Chronic Kidney Disease

of 13
-
Upload
sudarmono-eddie -
Category
Documents
-
view
220 -
download
0
Transcript of 8. Progression in Chronic Kidney Disease
-
8/18/2019 8. Progression in Chronic Kidney Disease
1/13
Progression in Chronic Kidney DiseaseAllison A. Eddy
The pathogenic mechanisms that lead to chronic kidney disease (CKD) converge on a common
pathway that results in progressive interstitial fibrosis, peritubular capillary loss with hypoxia, and
destruction of functioning nephrons because of tubular atrophy. Interstitial recruitment of inflamma-tory leukocytes and myofibroblasts occurs early in kidneys destined to develop fibrosis. Circulating
monocytes are recruited by locally secreted chemoattractant molecules, facilitated by leukocyte
adhesion molecules. Functionally heterogeneous macrophages secrete many fibrosis-promoting
molecules, but under some circumstances they may also serve a protective scavenging role. Excessive
extracellular matrix production occurs primarily within interstitial myofibroblasts, a population of
cells that appears to have more than 1 origin, including the resident interstitial fibroblasts, transdif-
ferentiated tubular epithelial cells, and bone marrow–derived cells. Impaired activity of the endoge-
nous renal matrix-degrading proteases may enhance interstitial matrix accumulation, but the specific
pathways that are involved remain unclear. Tubules, inflammatory cells, and myofibroblasts synthe-
size the molecules that activate the fibrogenic cascades, the most important of which is transforming
growth factor (TGF-). TGF- may direct cells to assume a profibrotic phenotype or it may do so
indirectly after stimulating synthesis of other fibrogenic molecules such as connective tissue growth
factor and plasminogen activator inhibitor-1. Reduced levels of antifibrotic factors that are normally
produced in the kidney such as hepatocyte growth factor and bone morphogenic protein-7 may
accelerate fibrosis and its destructive consequences. Development of new therapeutic agents for CKDlooks promising, but several agents that target different components of the fibrogenic cascade will
almost certainly be necessary.
© 2005 by the National Kidney Foundation, Inc.
Index Words: Interstitial fibrosis; inflammation; chemokines; macrophages
A lthough patients develop chronic kid-ney disease (CKD) from any one of amultitude of primary disease processes, it isrecognized that several secondary factorscontribute to the rate of decline of kidneyfunction including hypertension, hyperlip-
idemia, proteinuria, mineral (eg, calcium,phosphate, urate) deposition, exposure tonephrotoxins, and perhaps chronic inflam-mation. Current medical therapy is based onthe goals of curing or controlling the pri-mary disease process, which is unfortu-nately not easily accomplished for manyrenal disorders and any secondary modify-ing factors. However, many patients firstcome to medical attention with a glomerularfiltration rate 60 mL/min/1.73 m2 (stage 3CKD),1 and for them the progression of kid-
ney disease is almost inevitable, althoughthe pace is highly variable. This reality un-derscores the pressing need for completelynew and innovative therapeutic strategies.The future looks encouraging for at least 2significant reasons. First, independent of theprimary diseases process and specific sec-ondary risk factors, the pathogenetic mech-anisms that cause progressive renal destruc-tion converge on a common pathway that is
characterized by progressive interstitial fi- brosis, peritubular capillary loss causing tu- bular hypoxia, and destruction of function-ing nephrons because of tubular atrophy.Thus, effective therapies are likely to be beneficial for most patients with CKD. Im-
portant scientific advances over the past de-cade have begun to elucidate the cellularand molecular pathways of renal destruc-tion and identified several obvious newtherapeutic candidates. It has also becomeclear that future therapy for CKD will com-prise a “cocktail” of agents analogous tocancer chemotherapy protocols because of both the complexity of the process and po-tential for adverse side effects should a sin-
From the Division of Nephrology, University of Washing-ton and Children’s Hospital and Regional Medical Center,Seattle, WA.
Supported by the National Institutes of Health grantsDK54500 and DK44757.
Address correspondence to Allison A. Eddy, MD, Chil-dren’s Hospital & Regional Medical Center, 4800 Sand PointWay NE, Division of Nephrology, Mail Stop M1-5, Seattle,WA 98105. E-mail: [email protected]
© 2005 by the National Kidney Foundation, Inc.1548-5595/05/1204-0004$30.00/0doi:10.1053/j.ackd.2005.07.011
Advances in Chronic Kidney Disease, Vol 12, No 4 (October), 2005: pp 353-365 353
-
8/18/2019 8. Progression in Chronic Kidney Disease
2/13
gle pathway be selected for therapeutic ab-lation. Second, many of the molecules thatare key perpetrators of CKD also play acentral role in other disease processes suchas cancer and cardiovascular disease. Byassociation with these broader “patient mar-kets,” the pharmaceutical industry will bemore enthusiastic about research and devel-
opment of new drugs that will eventually benefit CKD patients.
In the sections that follow, the key cellu-lar and molecular pathophysiological path-ways leading to CKD will be reviewed.
Viewed from afar, renal destruction is theconsequence of chronic inflammation andfibrogenesis. Close up, several cellular andmolecular events occur concurrently and forease of presentation, an analogy with a bat-tlefield is made (Fig 1). The strongest fight-ers are interstitial macrophages and (myo)-fibroblasts; the weapons are multiple, butthe most deadly is transforming growth fac-tor (TGF-). The key targets are interstitialcapillaries and tubules. The most seriousdamage ensues as a consequence of destruc-
tive fibrosis. The kidney does have somelimited intrinsic defense mechanisms (gen-eration of antifibrotic factors), but these arerelatively ineffective unless the battle
Fig 1. Cartoon depicts the key pathways involvedin the pathogenesis of chronic progressive kidneydisease.
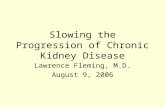
Fig 2. Interstitial macrophages are mediators of CKD. Typical of all CKDs, an interstitial infiltrate ofmacrophages develops in the experimental protein-overload proteinuria model. When renal MCP-1 isblocked by retrograde injection of a plasmid encoding a MCP-1 antagonist (7ND) into the renal vein, thenumber of interstitial macrophages is significantly reduced compared with control animals injected withnaked DNA and fibrosis severity (interstitial % area with Sirius-red stained collagen) is significantlyreduced. L, left kidney treated with 7ND; R, right kidney. (Reprinted with permission, Shimizu H,Maruyama S, Yuzawa Y, et al., Anti-monocyte chemoattractant protein-1 gene therapy attentuates renalinjury induced by protein-overload proteinuria, J Am Soc Nephrol, 14:1499-1502, Lippincott Williams &Wilkins.7).
354 Progression in CKD
-
8/18/2019 8. Progression in Chronic Kidney Disease
3/13
ceases. In primary glomerular disorders,podocyte loss, proteinuria, and extension of extracapillary lesions into the tubulointersti-tium are also involved directly as pathoge-netic mechanisms of CKD, as recently
reviewed by Kriz and LeHir.2
Interstitial Inflammation
A striking histological feature of CKD is thepresence of an interstitial infiltrate of inflam-matory mononuclear cells, both lymphocytesand macrophages. Macrophages, in particu-lar, appear to be a major participant in kidneyfibrosis (Fig 2). This has been established inseveral experiments that reduce the numberof interstitial macrophages. For example, ad-ministration of immunosuppressive drugssuch as corticosteroids or mycophenolatemofetil attenuates interstitial inflammationand fibrosis even in nonimmune models suchas polycystic kidney disease and 5/6 nephrec-tomy.3,4 Although a small population of resi-dent interstitial macrophages may proliferatein response to renal injury, most of the inflam-matory cells appear to be recruited from thecirculation. Inactivation of intrarenal path-ways that are involved in monocyte recruit-ment can reduce fibrosis. Examples includechemokines that recruit monocytes via inter-
actions with specific receptors, such as mono-cyte chemoattractant protein-1 (MCP-1) that binds to chemokine receptor 2 (CCR2) andregulated on activation normal T cell ex-pressed and secreted that binds to CCR1.MCP-1–deficient mice have significantly di-minished interstitial disease when they de-velop lupus or anti-glomerular basementmembrane (GBM) nephritis.5,6 Anti–MCP-1gene therapy reduces interstitial inflammationand fibrosis in rats with overload proteinuria(Fig 2).7 Mice treated with a CCR1 antagonist
or genetically engineered to lack CCR1 orCCR2 develop less interstitial inflammationand fibrosis after ureteral obstruction.8-10 Be-yond monocyte recruitment, chemokines suchas MCP-1 stimulate their target cells towardfibrosis-promoting activities.11 The ability of certain urinary proteins to activate nuclearfactor (NF)-– dependent inflammatorypathways and chemokine production by renaltubular epithelial cells is proposed as an im-
portant pathway that links proteinuria as arisk factor for CKD.12 Macrophage secretionof several products during acute renal injurylikely contributes to chronic interstitial in-flammation and fibrosis.13
Other pathways involved in monocyte re-cruitment during fibrogenic responses mayalso be amenable to therapeutic modulation.Adhesion molecules such as E and P selectins,intercellular adhesion molecules and vascularcell adhesion molecule activated on peritubu-lar capillary endothelial cells facilitate mono-nuclear cell recruitment.14-16 Renal tubularcells may be stimulated to express certainleukocyte adhesion molecules such as os-teopontin, intercellular adhesion molecule-1,and 11 integrin (VLA-1), but the extent towhich such tubular molecules promote renalfibrosis via inflammatory cell recruitmentrather than by their ability to activate othersignaling pathways involved in fibrosis is un-clear. Renal tubular cells may also expresstoll-like receptors that might promote renalinflammation.17,18 The complement cascade,long known to be a mediator of acute glomer-ular disease, may also induce tubular injuryand interstitial inflammation, especially inproteinuric disorders. The activated compo-nents C3a and C5a in particular are potentmacrophage chemoattractants. Soluble com-
plement receptors are effective blockers of complement activation. Treating MRL/lpr-lu-pus prone mice with soluble recombinantCrry (the mouse homologue of human com-plement receptor CR1) significantly reducesinterstitial inflammation and preserves kidneyfunction.19 Plasminogen activator inhibitor-1[PAI-1], discussed later, appears to have sig-nificant macrophage chemoattractant proper-ties that contribute to its potent fibrosis-pro-moting properties.20,21
Macrophages are functionally heteroge-
neous. During the phase of active fibrogen-esis, they are active participants. Macrophagesmay synthesize several molecules that con-tribute to the fibrogenic process, perhaps themost important of which are the fibrogenicgrowth factors, TGF- in particular. Other rel-evant macrophage products are matrix pro-teins, PAI-1, complement proteins, coagula-tion factors, bioactive lipids, reactive oxygenspecies, and endothelin.13 On the other hand,
355 Allison A. Eddy
-
8/18/2019 8. Progression in Chronic Kidney Disease
4/13
macrophage functional heterogeneity encom-passes several activities that may help to min-imize or even reverse fibrosis-associated tis-sue injury. Especially relevant is the role of macrophages as scavenger cells. When
chronic renal injury is induced in an environ-ment in which macrophages lack certain re-ceptors with scavenging properties, such asthe urokinase receptor (uPAR) or the angio-tensin II type 1 receptor, renal fibrosis is moresevere.22,23 The importance of the scavengingrole of macrophages has been clearly shownin an experimental model of reversible liverfibrosis where macrophage depletion duringthe recovery phase worsened residual fibrosiswhereas depletion during the earlier phase of fibrosis induction was protective.24 Whether Tcells play a pathogenetic role in progressiverenal fibrosis is less clear. In experimentalobstructive nephropathy, T-cell depletiondoes not appear to modify the degree of renalfibrosis.25
Interstitial Fibroblasts andMyofibroblasts
The normal interstitium is populated with asmall number of fibroblasts that are relativelyquiescent, but they may proliferate under cer-tain conditions. Beyond proliferation, these
cells may undergo a phenotypic transforma-tion and acquire fibrosis-promoting proper-ties. This phenotypic change can be recog-nized by the acquisition of smooth musclecell-type properties and de novo expression of alpha smooth muscle actin (SMA). SuchSMA-expressing cells, restricted to periarte-riolar regions in normal kidneys, densely pop-ulate the interstitium of chronically damagedkidneys. Platelet-derived growth factor(PDGF) and TGF- are 2 growth factors thatpromote fibroblast proliferation and/or trans-
formation into myofibroblasts.26,27
It seemsquite clear that these cells play an essentialrole in progressive kidney disease and are theprimary site of enhanced matrix synthesis.28
Understanding the pathobiology of intersti-tial myofibroblasts has become more complexwith the appreciation that resident interstitialfibroblasts are not the only precursor cells. Asmall subset may be bone marrow–derivedcells, and some may be cells that have mi-
grated into the interstitium from normalperivascular sites. An important additionalsource of origin is tubular epithelial cells thathave transdifferentiated into mesenchymalcells, likely in response to signals produced
locally within damaged kidneys.29,30
Afterthis process of epithelial-to-mesenchymaltransition (EMT), these cells (that have lostepithelial proteins like E-cadherin andcatenins and have begun to express mesen-chymal proteins such as vimentin and SMA)gain access to interstitial spaces after the dis-ruption of tubular basement membranes bylocally produced proteases such as some of the metalloproteinases. What remains unclearis whether interstitial myofibroblasts derivedfrom different sites serve distinct roles duringfibrogenesis. It is reasonable to speculate thatthere may be unique functions because thekinetics of their recruitment differs; EMT oc-curs later once initial kidney damage has de-veloped. Furthermore, studies using fibroblastspecific protein-1 (FSP-1) as a marker indicatethat most FSP-1–positive cells (includingthose derived by EMT) may not expressSMA, yet FSP-1–positive interstitial cellsplay a significant role in renal fibrosis as theirselective depletion attenuates fibrosis sever-ity.31,32
The importance of the EMT process in renal
fibrosis has recently been highlighted by stud-ies involving 2 different molecules that haveimpressive antifibrotic activities in experi-mental CKD models. The first is hepatocytegrowth factor (HGF), a multifunctional glyco-protein acting through its c-met receptor thatwas first identified because of its ability topromote liver regeneration. Inhibition of en-dogenous HGF has been shown to enhancerenal fibrosis, whereas recombinant HGF ther-apy has impressive renoprotective effects.33,34
HGF elicits several responses that serve to
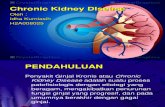
protect the kidney from chronic damage, in-cluding its ability to prevent EMT (Fig 3).Other effects are inhibition of fibroblast acti-vation, inhibition of TGF- production, sup-pression of renal inflammation, and enhancedMMP-dependent myofibroblast apoptosis.33,35
The second endogenous antifibrotic moleculeis bone morphogenic protein-7 (BMP-7), a mem- ber of the TGF- superfamily, first recognized asan important morphogen for the kidney when it
356 Progression in CKD
-
8/18/2019 8. Progression in Chronic Kidney Disease
5/13
was reported that BMP-7 null mice die in theperinatal period because of renal dysgenesis.36
Some normal tubular cells express BMP-7 andadministration of recombinant BMP-7 is benefi-cial in several experimental models. An impor-
tant renoprotective effect of BMP-7 is its abilityto preserve epithelial cell phenotype, not only by preventing tubular cell EMT during injury but perhaps even stimulating the conversion of myofibroblasts back to epithelium again (mes-enchymal-to-epithelial transition).27,37 BMP-7may elicit other effects that help to reduce fibro-sis including blockade of TGF-–dependent in-tracellular signaling and modulating interac-tions between inflammatory and residentkidney cells.38
Several other molecules have been reported
to elicit antifibrotic responses, but their pri-mary mechanism of action has not been com-pletely elucidated. Relaxin, a small peptidehormone first recognized for its role in preg-nancy, also has antifibrotic effects. Recombi-nant relaxin attenuates renal fibrosis, whereasrelaxin-1–deficient mice develop acceleratedCKD with aging.39,40 A novel effect of relaxinis its ability to enhance fibronectin degrada-tion through an ubiquitin-proteasome path-
way.41 Interferon gamma; interleukins (ILs) 7,11, and 15; and insulin-like growth factor areexamples of other molecules with the poten-tial to attenuate fibrotic responses.
The Weapons
Based on current evidence, there seems to belittle doubt that TGF- is the grand master of renal fibrosis. If TGF- could be ablated ther-apeutically, this might be the greatest advancein CKD intervention. Several clever strategieshave been used to illustrate the dominant roleof TGF- in short-term experimental modelsof fibrosis. TGF-–neutralizing antibodiesprevent diabetic nephropathy in mice and at-tenuate chronic nephropathy in rats.42,43
TGF- inactivation by administering solubleTGF- type II receptor or TGF- latency acti-vating peptide can effectively reduce fibro-sis.44,45 Mice with a deficiency of Smad3, a keyintracellular-signaling molecule involved inthe transcriptional activation of genes thatpromote fibrosis after TGF- binds to andactivates its cellular receptors, develop mark-edly attenuated renal fibrosis after ureteralobstruction.46 Converse studies have shownthat enhanced TGF- expression or signalingworsens renal fibrosis.47,48 But TGF- hasother biological functions that are cause for
concern should complete and chronic block-ade be the goal of antifibrotic therapy. Inparticular, TGF- has potent immunosuppres-sive properties. Genetic TGF- deficiency isincompatible with life in mice. Within a fewweeks of weaning, an unregulated inflamma-tory process causes a cardiopulmonarydeath.49 In rats with nephrotic syndrome, lowdoses of TGF-–neutralizing antibody areprotective, whereas disease severity appearsto be accentuated with high-dose therapy.50
Such toxicities are reminiscent of immunosup-
pressive protocols used in transplantation,where a fine line is drawn between rejectionprevention with long-term allograft survivaland serious complications because of infectionand malignancy as a consequence of compro-mised immunological surveillance.
Several important questions remain to beanswered about the role of TGF- in renalfibrosis. Furthermore, if TGF- is absolutelyessential for progressive CKD as is predicted,
Fig 3. Antifibrotic effects of HGF include inhibi-tion of epithelial-to-mesenchymal transition. Af-ter unilateral ureteral obstruction (UUO), a largenumber of myofibroblasts appear in the intersti-tium, as illustrated by SMA Western blotting (Aand B). Compared with vehicle-treated animals,interstitial myofibroblast density is significantlyreduced in the HGF-treated animals and is asso-ciated with less severe histological injury (C).Actin staining confirms that similar quantities ofprotein were loaded into each lane (A). In vitrostudies not shown demonstrate that HGF pre-vents TGF-–induced EMT. (Used with permis-sion from Am J Physiol Renal Physiol 384:F349-357, 2003.34)
357 Allison A. Eddy
-
8/18/2019 8. Progression in Chronic Kidney Disease
6/13
can blocking therapies be delivered specifi-cally to the kidney to minimize undesirablesystemic side-effects? Because several intra-cellular signaling pathways regulate cellularresponses to TGF-, it may be possible to
separate fibrogenic from immunosuppressiveeffects and to selectively target fibrosis-acti-vating pathways. Members of this pathwayinclude Smad 2 and Smad 3, whereas endog-enous pathways reported to block TGF-–dependent fibrosis signaling pathways mayinvolve Smad 7, Smurf, SnoN, or Ski.51 Ubiq-uitin-dependent degradation of the endoge-nous inhibitory Smad7 occurs after ureteralobstruction and Smad7 gene therapy attenu-ates fibrosis severity.4,8,52
Another important question is the extent towhich other molecules that have been as-cribed important fibrosis-promoting proper-ties do so directly or indirectly as TGF- ago-nists. Although experimental studies havereported important fibrogenic effects of endo-thelin 1, angiotensin II, PDGF, epidermalgrowth factor, basic fibroblast growth factor,tumor necrosis factor alpha, and IL-1, to namea few, each of these may stimulate TGF-production. Clinically, a significant degree of TGF- inhibition can be achieved with angio-tensin-converting enzyme (ACE) inhibitorand angiotensin II receptor (ARB) blocker
drugs. In vitro angiotensin II is a potentTGF- stimulant, and in experimental CKDstudies in animals, intrarenal levels of TGF-are significantly reduced by ACE and ARBtherapy.53 An observation that deserves fur-ther consideration as the debate between ACEversus ARB efficacy continues is the fact thatACE inhibition not only decreases angiotensinII but also increases bradykinin levels. It ap-pears that increases in bradykinin may beprotective as bradykinin receptor B2-deficientmice or mice treated with a bradykinin B2
receptor blocker develop more severe renalfibrosis after ureteral obstruction.54 Recentstudies provide evidence that aldosteronemay also have some direct fibrosis-promotingactivities.55
Activation of the TGF- fibrogenic signal-ing cascades elicits a multitude of pathoge-netic responses relevant to matrix accumula-tion. These include fibroblast proliferation(dose dependent) and activation, tubular epi-
thelial cell transdifferentiation, upregulated
expression of several integrin matrix adhesionmolecules, enhanced matrix synthesis, re-duced matrix turnover, and synthesis of addi-tional fibrosis-promoting molecules such asconnective tissue growth factor (CTGF) andPAI-1. TGF- is currently the only knownCTGF agonist. This cysteine-rich peptide wasfirst identified as a chemotactic and mitogenicfactor for fibroblasts. Its cellular effects aremediated by receptors that are distinct fromthe TGF- receptors. Both tubular and inter-stitial cells produce CTGF in chronically dam-
aged kidneys. CTGF antisense therapy di-rected to either interstitial or tubular cells iseffective in reducing the severity of renal fi- brosis.56,57
PAI-1, a glycoprotein that is not normallysynthesized in the kidney, is produced in sig-nificant quantities by tubules and interstitialcells of damaged kidneys. PAI-1 modulatescellular responses by interacting with uPARand its coreceptors, low-density lipoprotein
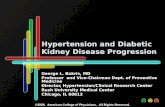
Fig 4. PAI-1 is an important profibrotic moleculein the kidney. In the experimental model of uni-lateral ureteral obstruction (UUO), PAI-1–nullmice develop less severe fibrosis (interstitial %area occupied by Sirius red stained collagen
fibrils), whereas mice genetically engineered tooverproduce PAI-1 develop worse fibrosis com-pared with wild-type mice. (Reprinted with per-mission Oda T, Jung YO, Kim H, et al: PAI-1deficiency attenuates the fibrogenic response toureteral obstruction. Kidney Int 30:587-596,2001, Blackwell Publishing, UK.20 Matsuo S,López-Guisa J, Cai X, et al: Multi-functionality ofPAI-1 in fibrogenesis: Evidence from obstructivenephropathy in PAI-1 over-expressing mice. Kid-ney Int 67:2221-2238, 2005, Blackwell Publish-ing, UK.59)
358 Progression in CKD
-
8/18/2019 8. Progression in Chronic Kidney Disease
7/13
receptor-associated protein, and integrins.58
In addition to its monocyte chemoattractantproperties, PAI-1 influences the migratory be-havior of many cells. In CKD, PAI-1 appearsto promote myofibroblast recruitment. PAI-1–
deficient mice develop less severe renal fibro-sis after ureteral obstruction while PAI-1 over-expressing mice develop worse fibrosis (Fig4).20,59 Other experimental observations thatestablish PAI-1 as an important mediator of progressive kidney disease include the protec-tive effects of a PAI-1 competitive inhibitor60
and associations between reduced PAI-1 lev-els and the renoprotective effects of angioten-sin II inhibition61 and enhanced PAI-1 accu-mulation and fibrosis severity in mice lackinguPAR, the receptor that mediates PAI-1 deg-radation.22 PAI-1 has a strong affinity for vi-tronectin, an extracellular matrix protein thataccumulates in the interstitium of chronicallydamaged kidneys. This interaction may con-tribute to the potent fibrogenic properties of PAI-1 because it provides a mechanism forconcentrating PAI-1 at sites of damage to thekidneys. Several other cytokines producedwithin the kidney in response to injury havethe potential to elicit fibrosis-promoting activ-ities. Depending on the nature of the primarykidney injury and early responses, it is likelythat cytokines in addition to TGF- play crit-
ical roles. Examples of other potentially pro-fibrotic cytokines include tumor necrosis fac-tor-, IL-1, IL-4, IL-5, IL-10, IL-13, PDGF-B,PDGF-C, and epidermal growth factor.
Interstitial Matrix Accumulation
The progressive accumulation of extracellularmatrix proteins within the renal interstitium isa dynamic process that changes not only byseverity but also by macromolecular compo-sition over time.62 The presence of interstitial
myofibroblasts appears to be essential for en-hanced matrix production, although intersti-tial inflammatory cells and tubular epitheliumalso contribute. The early phase of renal fibro-sis is typified by the production of a loosescaffold of matrix usually containing fibronec-tin and next fibrillar collagens. In the lung, anearly provisional fibrin precedes collagen ma-trix formation, but the extent to which fibrincontributes to renal interstitial fibrosis is not
clear. During this early phase, the matrix net-work is relatively unstable, susceptible toproteolytic degradation, and potentially re-versible.63 Several changes occur as fibrosisadvances. A variety of new matrix proteins
may be added such as glycoproteins (hyalu-ron, thrombospondin, vitronectin, secretedprotein acidic and rich in cysteine), proteogly-cans (decorin, biglycan, fibromodulin, aggre-can, versican, perlecan, heparan sulfateproteoglycan), and basement membrane pro-teins (laminin, type IV collagen). Significantlyincreased mRNA levels for several matrixproteins that are transcriptionally regulatedand the de novo appearance of novel intersti-tial matrix proteins highlight enhanced matrixsynthesis rates as important for interstitialmatrix expansion. As a result of chemicalmodifications, the interstitial matrix network becomes more rigid and protease-resistantwith time. Cross-linking is induced by en-zymes such as lysyl oxidase and tissue trans-glutaminase. Biochemical modifications mayoccur as a consequence of interactions withreactive oxygen species and advanced glyco-sylation end products to name a few. Severalrelevant molecules may become sequesteredthrough specific interactions with extracellu-lar matrix molecules such as PAI-1 binding tovitronectin, fibroblast growth factor binding
to proteoglycans, TGF- binding to decorin,PDGF, and vascular endothelial growth factor binding to secreted protein acidic and rich incysteine.
An important feature of the fibrogenic pro-cess that remains poorly understood is the ex-tent to which impaired endogenous turnoverpathways contribute to the net rate of matrixaccumulation and CKD progression. The nor-mal kidney is a rich source of proteases withmatrix-degrading properties including metallo-proteinases (especially MMP-2 and MMP-9),
serine proteinases (especially urokinase), andlysosomal cathepsins. Studies performed 25years ago in 2 experimental CKD models con-cluded that depressed collagenolytic activity,rather than enhanced collagen synthesis, wasthe predominant cause of renal fibrosis.64 Exis-tence of active matrix-degrading pathwayswithin normal kidneys is further supported byobservations from experimental studies show-ing that at least mild degrees of interstitial fibro-
359 Allison A. Eddy
-
8/18/2019 8. Progression in Chronic Kidney Disease
8/13
sis can reverse, as reported in acute tubularnecrosis, nephrotic syndrome remission or relief of ureteral obstruction.65-67 Furthermore, duringthe active phase of interstitial matrix accumula-tion, the kidney usually produces specific pro-
tease inhibitors that are not normally detected inthe kidney (eg, PAI-1 and the tissue inhibitors of metalloproteinases-1 [TIMP-1]), suggesting apotential mechanism for impaired matrix deg-radation during fibrogenesis.
However, identification of the specific pro-teases that might enhance matrix turnoverwithin the renal interstitium has proven chal-lenging. The MMPs are obvious candidates.Members of this large family of enzymes aregenerally secreted as latent zymogens thatrequire proteolytic activation and the pres-ence of divalent cations for protease activity.The type IV collagenases or gelatinases(MMP-2 and MMP-9) appear to be the mostabundant intrarenal MMPs. Yet definitivestudies have yet to be performed to establish if enhanced MMP activity can attenuate renalfibrosis. There may be important site-specificdifferences in the biological consequences of MMP activity. For example, MMP-2 can inter-act with mesangial cell receptors (likely 3or 5 integrins) to trigger responses thatpromote glomerular injury.68 When enhancedMMP-2 or MMP-9 activity occurs in the region
adjacent to tubular basement membranes, itpromotes basement membrane damage andfacilitates migration of transdifferentiated tu- bular cells into the interstitium.69,70 MMPsmay also be involved in the actual EMT pro-cess. MMP-2 has been shown to initiate renaltubular EMT71; MMP-7 (matrilysin) cleavesthe extracellular domain of E-cadherin, a cel-lular adhesion molecule whose loss is charac-teristic of the EMT process in tubular cells.72
Plasmin is a potent MMP activator; yet, invivo, when CKD is induced in mice with
genetic plasminogen deficiency, renal fibrosisis more severe.73,74 This may be partially be-cause of the fact that plasmin can activatelatent TGF-. Also surprising is the findingthat despite remarkably enhanced TIMP-1 ex-pression in kidneys damaged by ureteral ob-struction, genetic deficiency of TIMP-1 has noimpact on fibrosis severity.75 It is possible thatother metalloproteinase inhibitors (TIMP-2and TIMP-3) are able to compensate for the
absence of TIMP-1. Studies in mice lacking allthese inhibitors have yet to be performed toaddress this possibility.
What about renal serine proteinases? Tubu-lar cells are a rich source of urokinase (uPA)
but it is normally secreted apically into theurinary space. In addition to modest matrix-degrading activities, uPA also activates latentHGF, an important antifibrotic growth fac-tor.76 Therapeutic enhancement of uPA activ-ity is reported to attenuate pulmonary andhepatic fibrosis, but whether it plays a similarrole in CKD remains to be determined.77,78
Compared with uPA, levels of tissue-typeplasminogen activator are much lower in thetubulointerstitial compartment of the kidney.Studies of renal fibrosis in tissue-type plas-
minogen activator–deficient mice found thatfibrosis was less severe than in wild-typemice, an outcome that correlated with lowerMMP-9 activity, less tubular basement dam-age, and reduced EMT.70
Lysosomal cathepsins are also of interestfor their potential role in renal fibrosis, butfunctional studies have yet to be performed.The cathepsin B family is also involved in anapoptosis pathway, the inhibition of whichreduced fibrosis in a model of hepatic injury.79
At this juncture, it is evident that the intersti-
tial “scar” comprises a complex network of extracellular matrix molecules that are synthe-sized and secreted into the interstitial spaceand secondarily stabilized by a variety of bio-chemical modifications. Why endogenousproteases do not do a better job of limiting therate of matrix accumulation to prevent pro-gressive kidney destruction is currently un-clear. Possibilities include enzyme inactivity because of failed activation or the presence of inhibitors, expression within the wrong com-partment of the kidney (eg, tubular secretion
apically rather than basolaterally), or interac-tion with cellular receptors or other substrates(such as basement membranes) to elicit alter-native biological responses that dominateover their proteolytic actions on the interstitialmatrix. The functional role of several othermatrix-degrading proteases will need to becarefully investigated before the role of matrixturnover pathways in CKD is fully under-stood.
360 Progression in CKD
-
8/18/2019 8. Progression in Chronic Kidney Disease
9/13
Renal Fibrosis and CellularDestruction
As long as nephron units remain function-ally intact, interstitial fibrosis appears tohave little impact on glomerular filtrationrates. However, as chronic diseaseprogresses, the renal tubules atrophy pri-marily because of apoptosis (Fig 5).80,81
Even when glomeruli survive, the remain-ing atubular glomeruli will be nonfunc-tional. Ironically, during the inductionphase of renal fibrosis, renal tubules may beactive participants in the very process thatultimately causes their demise by producingproinflammatory mediators, reactive oxy-gen species, matrix proteins, proteases, anda myriad of other profibrotic molecules.
What remains unclear is which pathways
determine whether renal tubules are to re-generate, as is the typical outcome afterischemic-hypoxic injury of short duration,or undergo irreversible programmed celldeath. Tubular cell regeneration occurs pri-marily through proliferation of survivingtubular epithelial cells, although there isincreasing evidence that hematopoietic stem
cells also contribute to tubular regenera-tion.82-84 From a therapeutic perspective, thenotion that renal fibrosis is potentially re-versible is exciting, but the rate-limiting fac-tor that will determine if kidney functionwill also recover is the ability of the kidneyto restore or regenerate intact and functionalnephrons. The duration of hypoxic-ischemicinjury appears to be a critical determinant of the potential for renal recovery. A promi-
Fig 5. Peritubular capillary loss characterizesCKD. The interstitial capillary network becomesrarefied in CKD as shown by immunohistochem-ical staining for an endothelial cell protein. Inter-stitial capillary density correlates with the glo-merular filtration rate in studies of humankidney biopsies. (Reprinted with permission fromKang DH, Hughes J, Mazzali M, et al: Impairedangiogenesis in the remnant kidney model: II.Vascular endothelial growth factor administra-tion reduces renal fibrosis and stabilizes renalfunction. J Am Soc Nephrol 12:1448-1457, 2001,Lippincott Williams & Wilkins.88)
Fig 6. Tubular cell apoptosis and atrophy char-acterize CKD. Apoptotic tubular cells in a rem-nant kidney are identified by arrows. Ongoingapoptosis ultimately leads to tubular atrophy.In human kidney biopsy studies, tubular epi-thelial area correlates inversely with serum cre-atinine levels. (Reprinted with permission fromYang B, Johnson TS, Thomas GL, et al: Expres-sion of apoptosis-related genes and proteins inexperimental chronic renal scarring. J Am SocNephrol 12:275-288, 2001, Lippincott Williams& Wilkins.80 Mackensen-Haen S, Bohle A,Christensen J, Wehrmann M, Kendziorra H,Kokot F. The consequences for renal functionof widening of the interstitium and changes inthe tubular epithelium of the renal cortex and
outer medulla in various renal diseases. ClinNephrol 37:70-77, 1992, Dustri-Verlag Dr. KarlFeistle.93)
361 Allison A. Eddy
-
8/18/2019 8. Progression in Chronic Kidney Disease
10/13
nent peritubular capillary network normallydelivers oxygen to metabolically active tu- bules. Early in the course of injury to thekidneys, tubulointerstitial hypoperfusion isa response to locally produced vasocon-
stricting molecules.85
Anemia may be anindependent risk factor for end-stage renaldisease in humans.86 With more sustainedinjury, the interstitial capillaries physicallydisappear and, like the extent of tubularatrophy, the severity of peritubular capillaryloss evaluated histologically correlatesclosely with renal functional loss (Fig 6).87-89
A central unresolved question is why doperitubular capillaries not undergo an an-giogenic response to preserve oxygen deliv-ery? Furthermore, if angiogenic agents
could maintain interstitial capillary perfu-sion, would progressive CKD be arrested assuggested in animal studies using vascularendothelial growth factor intervention?88
Long before tubules die, hypoxia may pro-mote fibrosis. Several genes are activated inresponse to hypoxia via a process that in-volves the generation of hypoxia-inducibletranscription factors.90,91 In addition, oxi-dant stress triggers the release of reactiveoxygen species that have been implicated inseveral biological processes relevant to fi- brosis.
Summary
It is now known that several pathogeneticmechanisms converge on a final pathway of chronic progressive kidney disease due to in-terstitial inflammation, matrix protein accu-mulation, and nephron loss because of tubularcell apoptosis. Several molecular mediatorshave been identified and shown to play im-portant roles in this process. Future therapeu-
tic agents for CKD look promising, but the useof several agents that target different compo-nents of the pathogenetic cascade will almostcertainly be needed. It may also be possible toidentify patients at highest risk for CKD basedon genotype-dependent differences in the lev-els of expression and/or activity of key profi- brotic molecules and further to custom designtherapeutic protocols based on an individualpatient’s profibrotic genotype.92
Acknowledgments
The author would like to acknowledge the manyindividuals who performed the studies from herlaboratory that were cited.
References
1. National Kidney Foundation: K/DOQI clinical prac-tice guidelines for chronic kidney disease: Evaluation,classification and stratification. Am J Kidney Dis 39:S1-S266, 2002
2. Kriz W, LeHir M: Pathways to nephron loss startingfrom glomerular diseases-insights from animal mod-els. Kidney Int 67:404-419, 2005
3. Gattone VH II, Cowley BD Jr, Barash BD, et al: Meth-ylprednisolone retards the progression of inheritedpolycystic kidney disease in rodents. Am J Kidney Dis25:302-313, 1995
4. Romero F, Rodríguez-Iturbe B, Parra G, et al: Myco-phenolate mofetil prevents the progressive renal fail-
ure induced by 5/6 renal ablation in rats. Kidney Int55:945-955, 1999
5. Tesch GH, Maifert S, Schwarting A, et al: Monocytechemoattractant protein 1-dependent leukocytic infil-trates are responsible for autoimmune disease inMRL-Fas(lpr) mice. J Exp Med 190:1813-1824, 1999
6. Tesch GH, Schwarting A, Kinoshita K, et al: Monocytechemoattractant protein-1 promotes macrophage-me-diated tubular injury, but not glomerular injury, innephrotoxic serum nephritis. J Clin Invest 103:73-80,1999
7. Shimizu H, Maruyama S, Yuzawa Y, et al: Anti-monocyte chemoattractant protein-1 gene therapy at-tenuates renal injury induced by protein-overloadproteinuria. J Am Soc Nephrol 14:1496-1505, 2003
8. Anders HJ, Vielhauer V, Frink M, et al: A chemokinereceptor CCR-1 antagonist reduces renal fibrosis afterunilateral ureter ligation. J Clin Invest 109:251-259,2002
9. Eis V, Luckow B, Vielhauer V, et al: Chemokinereceptor CCR1 but not CCR5 mediates leukocyte re-cruitment and subsequent renal fibrosis after unilat-eral ureteral obstruction. J Am Soc Nephrol 15:337-347, 2004
10. Kitagawa K, Wada T, Furuichi K, et al: Blockade of CCR2 ameliorates progressive fibrosis in kidney.Am J Pathol 165:237-246, 2004
11. Schneider A, Panzer U, Zahner G, et al: Monocytechemoattractant protein-1 mediates collagen deposi-
tion in experimental glomerulonephritis by trans-forming growth factor-beta. Kidney Int 56:135-144,1999
12. Takase O, Hirahashi J, Takayanagi A, et al: Genetransfer of truncated IkappaBalpha prevents tubulo-interstitial injury. Kidney Int 63:501-513, 2003
13. Eddy AA: Proteinuria and interstitial injury. NephrolDial Transplant 19:277-281, 2004
14. Naruse T, Yuzawa Y, Akahori T, et al: P-selectin-dependent macrophage migration into the tubuloin-terstitium in unilateral ureteral obstruction. KidneyInt 62:94-105, 2002
362 Progression in CKD
-
8/18/2019 8. Progression in Chronic Kidney Disease
11/13
15. Janssen U, Ostendorf T, Gaertner S, et al: Improved
survival and amelioration of nephrotoxic nephritis in
intercellular adhesion molecule-1 knockout mice. J Am Soc Nephrol 9:1805-1814, 1998
16. Cook HT, Khan SB, Allen A, et al: Treatment with an
antibody to VLA-1 integrin reduces glomerular and
tubulointerstitial scarring in a rat model of crescenticglomerulonephritis. Am J Pathol 161:1265-1272, 2002
17. Tsuboi N, Yoshikai Y, Matsuo S, et al: Roles of toll-likereceptors in C-C chemokine production by renal tu-
bular epithelial cells. J Immunol 169:2026-33, 2002
18. Anders HJ, Banas B, Schlondorff D: Signaling danger:Toll-like receptors and their potential roles in kidney
disease. J Am Soc Nephrol 15:854-867, 2004
19. Bao L, Haas M, Kraus DM, et al: Administration of asoluble recombinant complement C3 inhibitor pro-
tects against renal disease in MRL/lpr mice. J Am SocNephrol 14:670-679, 2003
20. Oda T, Jung YO, Kim H, et al: PAI-1 deficiency
attenuates the fibrogenic response to ureteral obstruc-tion. Kidney Int 30:587-596, 2001
21. Degryse B, Neels JG, Czekay RP, et al: The lowdensity lipoprotein receptor-related protein is a mo-togenic receptor for plasminogen activator inhibi-
tor-1. J Biol Chem 279:22595-22604, 2004
22. Zhang G, Kim H, Cai X, et al: Urokinase receptordeficiency accelerates fibrosis in obstructive nephrop-
athy. J Am Soc Nephrol 14:1254-1271, 2003
23. Nishida M, Fujinaka H, Matsusaka T, et al: Absence of angiotensin II type 1 receptor in bone marrow-de-
rived cells is detrimental in the evolution of renal
fibrosis. J Clin Invest 110:1859-1868, 200224. Duffield JS, Forbes SJ, Constandinou CM, et al: Selec-
tive depletion of macrophages reveals distinct, oppos-
ing roles during liver injury and repair. J Clin Invest
115:56-65, 200525. Shappell SB, Gurpinar T, Lechago J, et al: Chronic
obstructive uropathy in severe combined immunode-ficient (SCID) mice: Lymphocyte infiltration is not
required for progressive tubulointerstitial injury. J Am Soc Nephrol 9:1008-1017, 1998
26. Tang WW, Ulich TR, Lacey DL, et al: Platelet-derived
growth factor-BB induces renal tubulointerstitialmyofibroblast formation and tubulointerstitial fibro-
sis. Am J Pathol 148:1169-1180, 1996
27. Zeisberg M, Hanai J, Sugimoto H, et al: BMP-7 coun-teracts TGF-beta1-induced epithelial-to-mesenchymal
transition and reverses chronic renal injury. Nat Med
9:964-968, 200328. Chai Q, Krag S, Chai S, et al: Localisation and pheno-
typical characterisation of collagen-producing cells inTGF-beta1-induced renal interstitial fibrosis. Histo-
chem Cell Biol 119:267-280, 2003
29. Kalluri R, Neilson EG: Epithelial-mesenchymal tran-sition and its implications for fibrosis. J Clin Invest
112:1776-1784, 200330. Liu Y: Epithelial to mesenchymal transition in renal
fibrogenesis: Pathologic significance, molecular mech-anism, and therapeutic intervention. J Am Soc Neph-
rol 15:1-12, 200431. Iwano M, Plieth D, Danoff TM, et al: Evidence that
fibroblasts derive from epithelium during tissue
fibrosis. J Clin Invest 110:341-350, 2002
32. Iwano M, Fischer A, Okada H, et al: Conditionalabatement of tissue fibrosis using nucleoside analogs
to selectively corrupt DNA replication in transgenic
fibroblasts. Mol Ther 3:149-159, 2001
33. Liu Y: Hepatocyte growth factor in kidney fibrosis:Therapeutic potential and mechanisms of action.
Am J Physiol Renal Physiol 287:F7-F16, 200434. Yang J, Liu Y: Delayed administration of hepatocyte
growth factor reduces renal fibrosis in obstructive
nephropathy. Am J Physiol Renal Physiol 284:F349-F357, 2003
35. Gong R, Rifai A, Tolbert EM, et al: Hepatocyte growth
factor ameliorates renal interstitial inflammation in ratremnant kidney by modulating tubular expression of
macrophage chemoattractant protein-1 and RANTES. J Am Soc Nephrol 15:2868-2881, 2004
36. Dudley AT, Lyons KM, Robertson EJ: A requirement
for bone morphogenetic protein-7 during develop-ment of the mammalian kidney and eye. Genes Dev
9:2795-2807, 199537. Zeisberg M, Shah AA, Kalluri R: Bone morphogenic
protein-7 induces mesenchymal to epithelial transi-
tion in adult renal fibroblasts and facilitates regener-
ation of injured kidney. J Biol Chem 280:8094-8100,2005
38. Zhang XL, Selbi W, de la Motte C, et al: Bone mor-
phogenic protein-7 inhibits monocyte-stimulatedTGF-beta1 generation in renal proximal tubular epi-
thelial cells. J Am Soc Nephrol 16:79-89, 2005
39. Garber SL, Mirochnik Y, Brecklin CS, et al: Relaxindecreases renal interstitial fibrosis and slows progres-
sion of renal disease. Kidney Int 59:876-882, 2001
40. Samuel CS, Zhao C, Bond CP, et al: Relaxin-1-defi-
cient mice develop an age-related progression of renalfibrosis. Kidney Int 65:2054-2064, 2004
41. McDonald GA, Sarkar P, Rennke H, et al: Relaxin
increases ubiquitin-dependent degradation of fi-
bronectin in vitro and ameliorates renal fibrosis invivo. Am J Physiol Renal Physiol 285:F59-F67, 2003
42. Ziyadeh FN, Hoffman BB, Han DC, et al: Long-term
prevention of renal insufficiency, excess matrix geneexpression, and glomerular mesangial matrix expan-
sion by treatment with monoclonal antitransforming
growth factor-beta antibody in db/db diabetic mice.Proc Natl Acad Sci U S A 97:8015-8020, 2000
43. Fukasawa H, Yamamoto T, Suzuki H, et al: Treatment
with anti-TGF-beta antibody ameliorates chronic pro-gressive nephritis by inhibiting Smad/TGF-beta sig-
naling. Kidney Int 65:63-74, 200444. Zhang Y, McCormick LL, Gilliam AC: Latency-asso-
ciated peptide prevents skin fibrosis in murine sclero-dermatous graft-versus-host disease, a model for hu-
man scleroderma. J Invest Dermatol 121:713-719, 2003
45. Zhou A, Ueno H, Shimomura M, et al: Blockade of TGF-beta action ameliorates renal dysfunction and
histologic progression in anti-GBM nephritis. KidneyInt 64:92-101, 2003
46. Sato M, Muragaki Y, Saika S, et al: Targeted disrup-tion of TGF-beta1/Smad3 signaling protects against
363 Allison A. Eddy
-
8/18/2019 8. Progression in Chronic Kidney Disease
12/13
renal tubulointerstitial fibrosis induced by unilateralureteral obstruction. J Clin Invest 112:1486-1494, 2003
47. Mozes MM, Bottinger EP, Jacot TA, et al: Renal ex-pression of fibrotic matrix proteins and of transform-ing growth factor-beta (TGF-beta) isoforms in TGF- beta transgenic mice. J Am Soc Nephrol 10:271-280,
199948. Lan HY, Mu W, Tomita N, et al: Inhibition of renalfibrosis by gene transfer of inducible Smad7 usingultrasound-microbubble system in rat UUO model. J Am Soc Nephrol 14:1535-1548, 2003
49. Kulkarni AB, Huh CG, Becker D, et al: Transforminggrowth factor beta 1 null mutation in mice causesexcessive inflammatory response and early death.Proc Natl Acad Sci U S A 90:770-774, 1993
50. Ma LJ, Jha S, Ling H, et al: Divergent effects of lowversus high dose anti-TGF-beta antibody in puromy-cin aminonucleoside nephropathy in rats. Kidney Int65:106-115, 2004
51. Yang J, Zhang X, Li Y, et al: Downregulation of Smadtranscriptional corepressors SnoN and Ski in the fi-
brotic kidney: An amplification mechanism for TGF- beta1 signaling. J Am Soc Nephrol 14:3167-3177, 2003
52. Fukasawa H, Yamamoto T, Togawa A, et al: Down-regulation of Smad7 expression by ubiquitin-depen-dent degradation contributes to renal fibrosis in ob-structive nephropathy in mice. Proc Natl Acad SciU S A 101:8687-8692, 2004
53. Zoja C, Corna D, Camozzi D, et al: How to fullyprotect the kidney in a severe model of progressivenephropathy: A multidrug approach. J Am Soc Neph-rol 13:2898-2908, 2002
54. Schanstra JP, Neau E, Drogoz P, et al: In vivo brady-kinin B2 receptor activation reduces renal fibrosis. J Clin Invest 110:371-379, 2002
55. Hollenberg NK: Aldosterone in the development and
progression of renal injury. Kidney Int 66:1-9, 200456. Yokoi H, Mukoyama M, Nagae T, et al: Reduction in
connective tissue growth factor by antisense treat-ment ameliorates renal tubulointerstitial fibrosis. J Am Soc Nephrol 15:1430-1440, 2004
57. Okada H, Kikuta T, Kobayashi T, et al: Connectivetissue growth factor expressed in tubular epitheliumplays a pivotal role in renal fibrogenesis. J Am SocNephrol 16:133-143, 2005
58. Eddy AA: Plasminogen activator inhibitor-1 and thekidney. Am J Physiol Renal Physiol 283:F209-F220,2002
59. Matsuo S, López-Guisa J, Cai X, et al: Multi-function-ality of PAI-1 in fibrogenesis: Evidence from obstruc-tive nephropathy in PAI-1 over-expressing mice. Kid-ney Int 67:2221-2238, 2005
60. Huang Y, Haraguchi M, Lawrence DA, et al: A mu-tant, noninhibitory plasminogen activator inhibitortype 1 decreases matrix accumulation in experimentalglomerulonephritis. J Clin Invest 112:379-388, 2003
61. Ma LJ, Nakamura S, Aldigier JC, et al: Regression of glomerulosclerosis with high-dose angiotensin inhibi-tion is linked to decreased plasminogen activatorinhibitor-1. J Am Soc Nephrol 16:966-976, 2005
62. Jernigan S, Eddy A: Experimental insights into themechanisms of tubulo-interstitial scarring, El Nahas
A, Harris K, Anderson S (eds): Mechanisms andClinical Management of Chronic Renal Failure. Ox-ford, UK, Oxford University Press, 2000
63. Eddy A: Can renal fibrosis be reversed? PediatrNephrol June 10, 2006 [Epub ahead of print]
64. González-Avila G, Vadillo-Ortega F, Pérez-Tamayo
R: Experimental diffuse interstitial renal fibrosis. A biochemical approach. Lab Invest 59:245-252, 198865. Forbes JM, Hewitson TD, Becker GJ, et al: Ischemic
acute renal failure: Long-term histology of cell andmatrix changes in the rat. Kidney Int 57:2375-2385,2000
66. Jones CL, Buch S, Post M, et al: Renal extracellularmatrix accumulation in acute puromycin amino-nucleoside nephrosis in rats. Am J Pathol 141:1381-1396, 1992
67. Koo JW, Kim Y, Rozen S, et al: Enalapril acceleratesremodeling of the renal interstitium after release of unilateral ureteral obstruction in rats. J Nephrol 16:203-209, 2003
68. Turck J, Pollock AS, Lee LK, et al: Matrix metallopro-
teinase 2 (gelatinase A) regulates glomerular mesan-gial cell proliferation and differentiation. J Biol Chem271:15074-15083, 1996
69. Cheng S, Pollock A, Olson J, et al: Transgenic renalproximal tubular cell expression of active matrix met-alloproteinase-2 drives epithelial-mesenchymal tran-sition and interstitial fibrosis. J Am Soc Nephrol:37A,2004 (abstr
70. Yang J, Shultz RW, Mars WM, et al: Disruption of tissue-type plasminogen activator gene in mice re-duces renal interstitial fibrosis in obstructive ne-phropathy. J Clin Invest 110:1525-1538, 2002
71. Cheng S, Lovett DH: Gelatinase A (MMP-2) is neces-sary and sufficient for renal tubular cell epithelial-mesenchymal transformation. Am J Pathol 162:1937-
1949, 200372. McGuire JK, Li Q, Parks WC: Matrilysin (matrix met-
alloproteinase-7) mediates E-cadherin ectodomainshedding in injured lung epithelium. Am J Pathol162:1831-1843, 2003
73. Edgtton KL, Gow RM, Kelly DJ, et al: Plasmin is notprotective in experimental renal interstitial fibrosis.Kidney Int 66:68-76, 2004
74. Zhang G, Collins S, Cai X, et al: Plasmin(ogen) pro-motes renal interstitial fibrosis by inducing epithelial-to-mesenchymal transition: Role of plasminogen acti-vate signals. J Am Soc Nephrol 15:36A, 2004 (abstr)
75. Kim H, Oda T, Lopez-Guisa J, et al: TIMP-1 deficiencydoes not attenuate interstitial fibrosis in obstructivenephropathy. J Am Soc Nephrol 12:736-748, 2001
76. Hattori N, Mizuno S, Yoshida Y, et al: The plasmin-ogen activation system reduces fibrosis in the lung bya hepatocyte growth factor-dependent mechanism.Am J Pathol 164:1091-1098, 2004
77. Sisson TH, Hattori N, Xu Y, et al: Treatment of bleo-mycin-induced pulmonary fibrosis by transfer of urokinase-type plasminogen activator genes. HumGene Ther 10:2315-2323, 1999
78. Salgado S, Garcia J, Vera J, et al: Liver cirrhosis isreverted by urokinase-type plasminogen activatorgene therapy. Mol Ther 2:545-551, 2000
364 Progression in CKD
-
8/18/2019 8. Progression in Chronic Kidney Disease
13/13
79. Canbay A, Guicciardi ME, Higuchi H, et al: CathepsinB inactivation attenuates hepatic injury and fibrosisduring cholestasis. J Clin Invest 112:152-159, 2003
80. Yang B, Johnson TS, Thomas GL, et al: Expression of apoptosis-related genes and proteins in experimentalchronic renal scarring. J Am Soc Nephrol 12:275-288,
200181. Truong LD, Choi YJ, Tsao CC, et al: Renal cell apo-ptosis in chronic obstructive uropathy: The roles of caspases. Kidney Int 60:924-934, 2001
82. Lin F, Cordes K, Li L, et al: Hematopoietic stem cellscontribute to the regeneration of renal tubules afterrenal ischemia-reperfusion injury in mice. J Am SocNephrol 14:1188-1199, 2003
83. Kale S, Karihaloo A, Clark PR, et al: Bone marrowstem cells contribute to repair of the ischemicallyinjured renal tubule. J Clin Invest 112:42-49, 2003
84. Morigi M, Imberti B, Zoja C, et al: Mesenchymal stemcells are renotropic, helping to repair the kidney andimprove function in acute renal failure. J Am SocNephrol 15:1794-1804, 2004
85. Manotham K, Tanaka T, Matsumoto M, et al: Evi-dence of tubular hypoxia in the early phase in theremnant kidney model. J Am Soc Nephrol 15:1277-1288, 2004
86. Keane WF, Brenner BM, de Zeeuw D, et al: The risk of developing end-stage renal disease in patients withtype 2 diabetes and nephropathy: the RENAALstudy. Kidney Int 63:1499-1507, 2003
87. Nangaku M: Mechanisms of tubulointerstitial injuryin the kidney: Final common pathways to end-stagerenal failure. Intern Med 43:9-17, 2004
88. Kang DH, Hughes J, Mazzali M, et al: Impaired an-giogenesis in the remnant kidney model: II. Vascularendothelial growth factor administration reduces re-
nal fibrosis and stabilizes renal function. J Am SocNephrol 12:1448-1457, 200189. Seron D, Alexopoulos E, Raftery MJ, et al: Number of
interstitial capillary cross-sections assessed by mono-clonal antibodies: Relation to interstitial damage.Nephrol Dial Transplant 5:889-893, 1990
90. Norman JT, Clark IM, Garcia PL: Hypoxia promotesfibrogenesis in human renal fibroblasts. Kidney Int58:2351-2366, 2000
91. Rosenberger C, Mandriota S, Jurgensen JS, et al: Ex-pression of hypoxia-inducible factor-1alpha and -2al-pha in hypoxic and ischemic rat kidneys. J Am SocNephrol 13:1721-1732, 2002
92. Henger A, Kretzler M, Doran P, et al: Gene expressionfingerprints in human tubulointerstitial inflammation
and fibrosis as prognostic markers of disease progres-sion. Kidney Int 65:904-917, 2004
93. Mackensen-Haen S, Bohle A, Christensen J, Wehr-mann M, Kendziorra H, Kokot F. The consequencesfor renal function of widening of the interstitium andchanges in the tubular epithelium of the renal cortexand outer medulla in various renal diseases. ClinNephrol 37:70-77, 1992
365 Allison A. Eddy