
607 Delivery of Monthly Patient Radiation Exposure Report Cards to Endoscopists Significantly...
1
total costs for the whole initial treatment, including hospitalization, were not different between the two stent types (plastic €4,120 vs. SEMS €4,592; pZ0.29). Total costs for all endoscopic procedures, initial placement and reinterventions, were lower for plastic stents vs. SEMS (2,434 vs. €2,078; pZ0.04), whereas total costs for hospitalization were slightly higher in de plastic stent group (€5,336 vs. €4,536; pZ0.23). As a result, total costs per patient were not significantly different between plastic stents and SEMS (7,320 vs. €6,932, pZ0.61). In patients with a short survival (% 3 months), total costs per patient were also not different between plastic stents and SEMS (€6,796 vs. €6,538; pZ0.81). No differences in costs were found between pcSEMS and uSEMS placement. Conclusion: Although initial costs of stent place- ment are higher for SEMS than for plastic stents, total costs are not different be- tween both stent types, also in patients with a short survival (% 3 months). Since the clinical outcome for SEMS is favorable and total costs are not different, SEMS placement is recommended for palliation in all patients with CBD obstruction. 607 Delivery of Monthly Patient Radiation Exposure Report Cards to Endoscopists Significantly Reduces Patient Radiation Exposure During ERCP: a Prospective Quality Improvement Study Nirav C. Thosani*, Shai Friedland, Ann M. Chen, Shivangi Kothari, Rajan Kochar, Charles Liao, Subhas Banerjee Gastroenterology & Hepatology, Stanford University, Stanford, CA Background: Patients exposure to radiation during ERCP may increase their lifetime risk of developing cancer. In prior studies we demonstrated that low volume en- doscopists (LVE) exposed patients to significantly higher amounts of radiation compared to high volume endoscopists (HVE) and that educating endoscopists in fluoroscopy best practices significantly reduced patient radiation exposure during ERCP for both LVE and HVE. Aim: To prospectively evaluate the impact of monthly radiation exposure report cards to endoscopists, on radiation exposure to patients during ERCP. Methods: All endoscopists performing ERCP at a tertiary care center received individualized monthly Patient Radiation Exposure Report Cards high- lighting radiation parameters including Fluoroscopy Time, Effective Radiation Dose and Dose Area Product (DAP) for their procedures, along with patient radiation exposure data for the best performing endoscopist (anonymous) as a comparator. The report card reinforced education on fluoroscopy best practices to minimize patient radiation exposure, including minimizing fluoroscopy time, image collima- tion, use of lower magnification images, reducing frame rates & spot films. Radiation parameters were prospectively collected over a 3 month period for 2 HVE and 7 LVE (endoscopists performing !200 ERCPs/yr) and compared with data on ERCPs per- formed by the same endoscopists over a 12-month period prior to the educational program, obtained from a prospectively maintained database. Results: Radiation data on 811 ERCPs was analyzed: Pre-education (nZ331), Post-education (nZ252), Lag period (nZ232) was compared with that of 92 patients undergoing ERCP following delivery of a monthly report card (Table 1). Overall, monthly report cards resulted in significant decline in median DAP and median Effective Radiation Dose for both HVE and LVE. A significant decline in Fluoroscopy Time was noted for HVE, while a trend towards lower Fluoroscopy Time was noted for LVE. Significant increases were noted in the use of collimation and in the proportion of lower magnification images for both HVE and LVE. Compared to the lag period before delivery of report cards, reduction in median DAP was greater for HVE (37%), compared to LVE (21%) (Figure 1). HVE performed significantly better than LVE for all radiation parameters after receiving the report card. None of the endoscopists reported any compromise in their ability to interpret and perform ERCP despite incorporating fluoroscopy best practices. Conclusion: 1. Delivery of a monthly Radiation Exposure Report Card significantly reduces patient radiation exposure during ERCP. 2. All endoscopists (HVE & LVE) benefited from a monthly report card highlighting their radiation utilization, allowing for significant reductions in patient radiation exposure, without compromising their ability to perform & interpret ERCP. Table 1. Radiation Exposure parameters Pre and Post education, during the Lag period and following a Monthly Report Card Parameter Pre Education Post Education Lag Period Monthly Report Card p value (Trend) Overall Fluoroscopy Time (minutes) 5.6 3.3 3.05 1.95 !0.001 Total Effective Dose (mGy)(Median) 80.1 51.9 50.42 31.85 !0.001 Dose Area Product (DAP) (Gycm 2 ) 9.6 6.19 3.02 2.99 !0.001 No. of images/procedure 6 5 4 4 !0.001 Collimation of any image (%) 16% 80% 77% 90% !0.001 % of images that are low magnification 10% 19% 34% 72% !0.001 Low Volume Endoscopist ( !200ERCP/Year) Fluoroscopy Time (minutes) 4 3.75 3.5 2.2 0.395 Total Effective Dose (mGy) 98.3 46.89 60.92 41.1 0.012 Dose Area Product (DAP)(Gycm 2 ) 13.98 7.21 7.95 6.25 !0.001 Parameter Pre Education Post Education Lag Period Monthly Report Card p value (Trend) No. of images/procedure 6 4 5 5 0.154 Collimation of any image (%) 22% 54% 54% 71% !0.001 % of images that are low magnification 42% 56% 40% 49% 0.991 High Volume Endoscopist (O200ERCP/Year) Fluoroscopy Time (minutes) 6 3.3 2.6 1.9 !0.001 Total Effective Dose (mGy) 74.13 53.14 48.22 31.51 !0.001 Dose Area Product (DAP)(Gycm ^ 2) 8.8 5.71 4.35 2.75 !0.001 No. of images/procedure 6 5 4 4 !0.001 Collimation of any image (%) 10% 85% 84% 95% !0.001 % of images that are low magnification 1% 14% 32% 79% !0.001 608 A Nationwide Quality Registry - Endoscopist-Related Predictors of Procedural Outcome in ERCP Vivian E. Ekkelenkamp* 1 , Frank Ter Borg 2 , Pieter Ter Borg 3 , Marco J. Bruno 1 , Marcel Groenen 4 , Robert a. De Man 1 , Erik Rauws 5 , Antonie J. P. Van Tilburg 6 , Arjun D. Koch 1 1 Department of Gastroenterology and Hepatology, Erasmus University Medical Center, Rotterdam, Netherlands; 2 Department of Gastroenterology and Hepatology, Deventer Hospital, Deventer, Netherlands; 3 Department of Gastroenterology and Hepatology, Ikazia Hospital, Rotterdam, Netherlands; 4 Department of Gastroenterology and Hepatology, Rijnstate Hospital, Arnhem, Netherlands; 5 Department of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, Netherlands; 6 Department of Gastroenterology and Hepatology, Sint Franciscus Gasthuis, Rotterdam, Netherlands Introduction: The interest in quality of outcome of ERCPs is increasing. However, real-life data on procedural outcome and quality of ERCP are sparse. The Rotter- dam Assessment Form for ERCP (RAF-E) is an easy-to-use web-based ERCP registry tool. The aim of this study was to evaluate ERCPs in the Netherlands and to relate endoscopist-dependent factors to procedural outcome. Methods: All ERCP-per- forming endoscopists in the Netherlands were invited to participate and were enabled to register their ERCPs over a one-year period using the RAF-E. The primary outcome was procedural success. The a priori difficulty level of the procedure was classified according to Schutz’s grade. Baseline characteristics of the endoscopist, for instance previous experience, were recorded at entry. Difficulty degree level 1 procedures with the intention to perform complete stone extraction or stent placement in patients with native papillary anatomy were included in this analysis to compare procedural outcome. This type of ERCP was chosen because it is consid- ered to be one of the routine indications to perform ERCPs and carried out by all AB158 GASTROINTESTINAL ENDOSCOPY Volume 79, No. 5S : 2014 www.giejournal.org Abstracts
Transcript of 607 Delivery of Monthly Patient Radiation Exposure Report Cards to Endoscopists Significantly...
Abstracts
total costs for the whole initial treatment, including hospitalization, were notdifferent between the two stent types (plastic €4,120 vs. SEMS €4,592; pZ0.29). Totalcosts for all endoscopic procedures, initial placement and reinterventions, werelower for plastic stents vs. SEMS (2,434 vs. €2,078; pZ0.04), whereas total costs forhospitalization were slightly higher in de plastic stent group (€5,336 vs. €4,536;pZ0.23). As a result, total costs per patient were not significantly different betweenplastic stents and SEMS (7,320 vs. €6,932, pZ0.61). In patients with a short survival(% 3 months), total costs per patient were also not different between plastic stentsand SEMS (€6,796 vs. €6,538; pZ0.81). No differences in costs were found betweenpcSEMS and uSEMS placement. Conclusion: Although initial costs of stent place-ment are higher for SEMS than for plastic stents, total costs are not different be-tween both stent types, also in patients with a short survival (% 3 months). Since theclinical outcome for SEMS is favorable and total costs are not different, SEMSplacement is recommended for palliation in all patients with CBD obstruction.
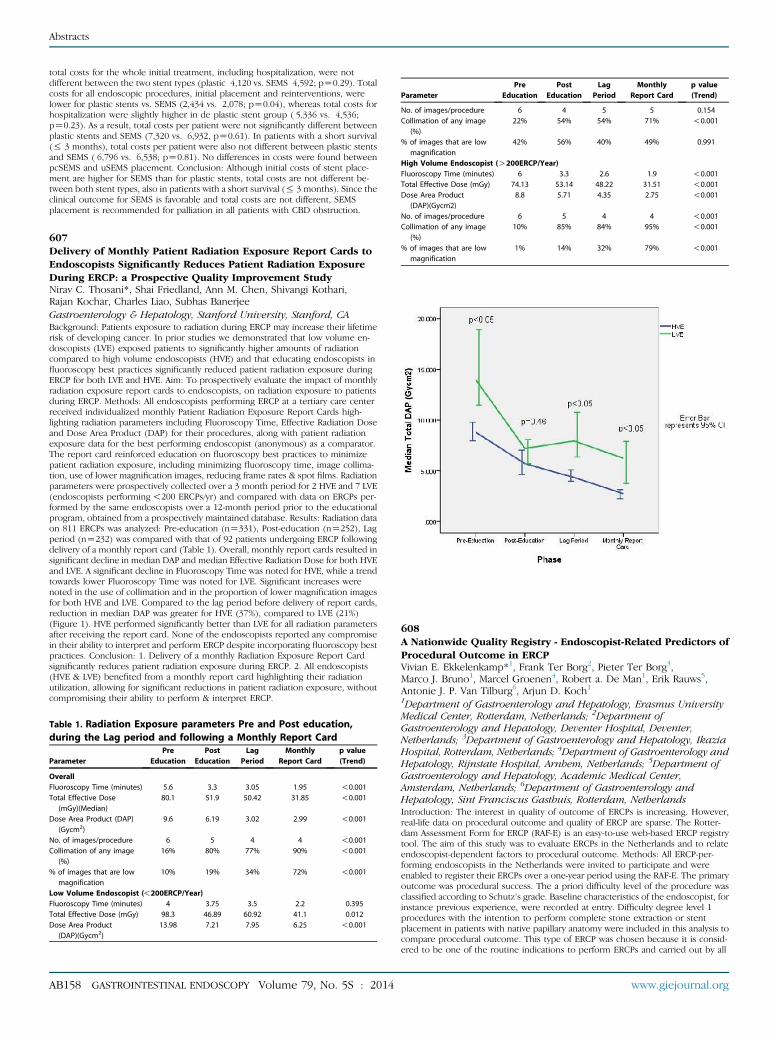
607Delivery of Monthly Patient Radiation Exposure Report Cards toEndoscopists Significantly Reduces Patient Radiation ExposureDuring ERCP: a Prospective Quality Improvement StudyNirav C. Thosani*, Shai Friedland, Ann M. Chen, Shivangi Kothari,Rajan Kochar, Charles Liao, Subhas BanerjeeGastroenterology & Hepatology, Stanford University, Stanford, CABackground: Patients exposure to radiation during ERCP may increase their lifetimerisk of developing cancer. In prior studies we demonstrated that low volume en-doscopists (LVE) exposed patients to significantly higher amounts of radiationcompared to high volume endoscopists (HVE) and that educating endoscopists influoroscopy best practices significantly reduced patient radiation exposure duringERCP for both LVE and HVE. Aim: To prospectively evaluate the impact of monthlyradiation exposure report cards to endoscopists, on radiation exposure to patientsduring ERCP. Methods: All endoscopists performing ERCP at a tertiary care centerreceived individualized monthly Patient Radiation Exposure Report Cards high-lighting radiation parameters including Fluoroscopy Time, Effective Radiation Doseand Dose Area Product (DAP) for their procedures, along with patient radiationexposure data for the best performing endoscopist (anonymous) as a comparator.The report card reinforced education on fluoroscopy best practices to minimizepatient radiation exposure, including minimizing fluoroscopy time, image collima-tion, use of lower magnification images, reducing frame rates & spot films. Radiationparameters were prospectively collected over a 3 month period for 2 HVE and 7 LVE(endoscopists performing!200 ERCPs/yr) and compared with data on ERCPs per-formed by the same endoscopists over a 12-month period prior to the educationalprogram, obtained from a prospectively maintained database. Results: Radiation dataon 811 ERCPs was analyzed: Pre-education (nZ331), Post-education (nZ252), Lagperiod (nZ232) was compared with that of 92 patients undergoing ERCP followingdelivery of a monthly report card (Table 1). Overall, monthly report cards resulted insignificant decline in median DAP and median Effective Radiation Dose for both HVEand LVE. A significant decline in Fluoroscopy Time was noted for HVE, while a trendtowards lower Fluoroscopy Time was noted for LVE. Significant increases werenoted in the use of collimation and in the proportion of lower magnification imagesfor both HVE and LVE. Compared to the lag period before delivery of report cards,reduction in median DAP was greater for HVE (37%), compared to LVE (21%)(Figure 1). HVE performed significantly better than LVE for all radiation parametersafter receiving the report card. None of the endoscopists reported any compromisein their ability to interpret and perform ERCP despite incorporating fluoroscopy bestpractices. Conclusion: 1. Delivery of a monthly Radiation Exposure Report Cardsignificantly reduces patient radiation exposure during ERCP. 2. All endoscopists(HVE & LVE) benefited from a monthly report card highlighting their radiationutilization, allowing for significant reductions in patient radiation exposure, withoutcompromising their ability to perform & interpret ERCP.
Table 1. Radiation Exposure parameters Pre and Post education,during the Lag period and following a Monthly Report Card
Parameter
AB158 GASTROINT
PreEducation
ESTINAL E
PostEducation
NDOSCO
LagPeriod
PY Vo
MonthlyReport Card
lume 79, No
p value(Trend)
Overall
Fluoroscopy Time (minutes) 5.6 3.3 3.05 1.95 !0.001 Total Effective Dose(mGy)(Median)
80.1 51.9 50.42 31.85 !0.001Dose Area Product (DAP)(Gycm2)
9.6
6.19 3.02 2.99 !0.001No. of images/procedure
6 5 4 4 !0.001 Collimation of any image(%)
16% 80% 77% 90% !0.001% of images that are lowmagnification
10%
19% 34% 72% !0.001Low Volume Endoscopist (!200ERCP/Year)
Fluoroscopy Time (minutes) 4 3.75 3.5 2.2 0.395 Total Effective Dose (mGy) 98.3 46.89 60.92 41.1 0.012 Dose Area Product(DAP)(Gycm2)
13.98 7.21 7.95 6.25 !0.001. 5S : 2014
Parameter
PreEducation
PostEducation
LagPeriod
MonthlyReport Card
www.giejo
p value(Trend)
No. of images/procedure
6 4 5 5 0.154 Collimation of any image(%)
22% 54% 54% 71% !0.001% of images that are lowmagnification
42%
56% 40% 49% 0.991High Volume Endoscopist (O200ERCP/Year)
Fluoroscopy Time (minutes) 6 3.3 2.6 1.9 !0.001 Total Effective Dose (mGy) 74.13 53.14 48.22 31.51 !0.001 Dose Area Product(DAP)(Gycm̂2)
8.8 5.71 4.35 2.75 !0.001No. of images/procedure
6 5 4 4 !0.001 Collimation of any image(%)
10% 85% 84% 95% !0.001% of images that are lowmagnification
1%
14% 32% 79% !0.001608A Nationwide Quality Registry - Endoscopist-Related Predictors ofProcedural Outcome in ERCPVivian E. Ekkelenkamp*1, Frank Ter Borg2, Pieter Ter Borg3,Marco J. Bruno1, Marcel Groenen4, Robert a. De Man1, Erik Rauws5,Antonie J. P. Van Tilburg6, Arjun D. Koch11Department of Gastroenterology and Hepatology, Erasmus UniversityMedical Center, Rotterdam, Netherlands; 2Department ofGastroenterology and Hepatology, Deventer Hospital, Deventer,Netherlands; 3Department of Gastroenterology and Hepatology, IkaziaHospital, Rotterdam, Netherlands; 4Department of Gastroenterology andHepatology, Rijnstate Hospital, Arnhem, Netherlands; 5Department ofGastroenterology and Hepatology, Academic Medical Center,Amsterdam, Netherlands; 6Department of Gastroenterology andHepatology, Sint Franciscus Gasthuis, Rotterdam, NetherlandsIntroduction: The interest in quality of outcome of ERCPs is increasing. However,real-life data on procedural outcome and quality of ERCP are sparse. The Rotter-dam Assessment Form for ERCP (RAF-E) is an easy-to-use web-based ERCP registrytool. The aim of this study was to evaluate ERCPs in the Netherlands and to relateendoscopist-dependent factors to procedural outcome. Methods: All ERCP-per-forming endoscopists in the Netherlands were invited to participate and wereenabled to register their ERCPs over a one-year period using the RAF-E. The primaryoutcome was procedural success. The a priori difficulty level of the procedure wasclassified according to Schutz’s grade. Baseline characteristics of the endoscopist, forinstance previous experience, were recorded at entry. Difficulty degree level 1procedures with the intention to perform complete stone extraction or stentplacement in patients with native papillary anatomy were included in this analysis tocompare procedural outcome. This type of ERCP was chosen because it is consid-ered to be one of the routine indications to perform ERCPs and carried out by all
urnal.org


















