4th National Health Care Quality Improvement...
26
4 th National Health Care Quality Improvement Conference 29-31 August 2017 Kampala Serena Conference Centre Kampala, Uganda Theme: Transforming Health Care through Leadership, Innovation, and Accountability Conference Report
Transcript of 4th National Health Care Quality Improvement...

4th National Health Care Quality Improvement Conference
29-31 August 2017 Kampala Serena Conference Centre
Kampala, Uganda
Theme: Transforming Health Care through Leadership, Innovation, and Accountability
Conference Report

1 | P a g e
Acknowledgments Our great appreciation goes to the main conference funder the United States
Agency for International Development (USAID) through the USAID Applying
Science to Strengthen and Improve Systems (ASSIST) Project, JICA, CDC, and
Makerere University School of Public health- Monitoring and Evaluation
Technical Support (METS) Programme. We also acknowledge all other
implementing partners who contributed financial and organisational support
that led to the success of the symposium.
We extend our gratitude to the keynote speakers; Dr. M. Rashad Massoud, Prof.
Gerald Kagambirwe Karyeija, and Dr. Eleuter Roki Samky, presenters, session
chairs and moderators. We would also like to acknowledge the important
contributions of all the conference participants from Uganda and around the
world who attended and used this conference as a platform to share their
experiences, and lessons learned in improving quality of care through
leadership, innovation, and accountability.
We wish to convey our sincere gratitude to all the conference rapporteurs who
captured and recorded all presentations and discussions over the 3 days. These
are: Amanda Ottosson, Leah Goldmann, Matovu Nicholas, Maria Martinez,
Grace Biyinzika, Tony Muwonge, and Lucy Hartshorn.

2 | P a g e
Executive Summary The Ministry of Health (MOH) has long prioritised assuring and improving
quality of care for all people in Uganda. In an effort to continuously improve
quality of service delivery and health outcomes across the country, the Ministry
of Health wanted to develop a platform for all practitioners, implementers,
academics, policy makers and beyond to discuss improvement.
In order to provide this platform to share best practices, successes, and
challenges in working to improve quality across Uganda, the Ministry of Health
established the Annual Health Care Quality Improvement Conference. This
annual conference aims to bring together frontline health workers, policy
makers, academics, researchers, and implementers to come together on an
annual basis to discuss achievements to date and the way forward.
Over 450 participants came together at the 4th Annual Health Care Quality
Improvement Conference on 29-31 August 2017 at the Kampala Serena
Conference Centre to discuss lessons learned and best practices under the
theme of “Transforming Health Care through Leadership, Innovation, and
Accountability”. 49 oral and 55 poster presentations were shared and discussed
at length during the conference.
This report outlines the key takeaways and examples from key note speeches,
oral and poster presentations, and discussions over the three days of the 4th
Annual Health Care Quality Improvement Conference. It showcases the key
takeaways and outstanding examples under the thematic areas of leadership,
innovation, and accountability.

3 | P a g e
Abbreviations 5S Sort, set, shine, standardise, sustain
ASSIST Applying Science to Strengthen and Improve Systems
CDC Centers for Disease Control and Prevention
CQI Continuous Quality Improvement
DHO District Health Officer
DOTS Directly observed treatment – short term
EMTCT Elimination of Mother to Child Transmission
IPTp2 Intermittent Preventative Treatment of Malaria in Pregnancy
JICA Japan International Cooperation Agency
METS Monitoring Evaluation and Technical Support Program
mHealth Mobile health
MOH Ministry of Health
MPDSR Maternal and Perinatal Deaths Surveillance and Response
PEPFAR President’s Emergency Plan for AIDS Relief
QAID Quality Assurance and Inspection Department
TB Tuberculosis
UMI Uganda Management Institute
UNICEF United Nations Children’s Fund
URC University Research Co., LLC
URLN Uganda Regional Learning Network
USAID United States Agency for International Development
VHT Village Health Team
VMMC Voluntary medical male circumcision
WHO World Health Organisation

4 | P a g e
Table of Contents Acknowledgments ........................................................................................................................ 1
Executive Summary ..................................................................................................................... 2
Abbreviations ................................................................................................................................. 3
Introduction .................................................................................................................................... 5
Institutionalising quality improvement .......................................................................... 5
The 4th Annual Health Care Quality Improvement Conference ................................. 8
Key takeaways ................................................................................................................................ 8
Leadership ................................................................................................................................ 10
Innovation ................................................................................................................................. 12
Technology .......................................................................................................................... 12
Community engagement ............................................................................................... 12
Low-cost solutions ........................................................................................................... 13
Accountability ......................................................................................................................... 14
Conclusion ..................................................................................................................................... 16
Way forward ............................................................................................................................ 17
Annex I: List of conference organisers.............................................................................. 19
Annex II: Conference programme .......................... Error! Bookmark not defined.
Annex III: Evaluation results .................................................................................................... 0

5 | P a g e
Introduction The 4th Annual National Health Care Quality Improvement Conference took
place at the Kampala Serena Conference Centre on 29-31 August 2017. Over
450 participants came together discuss lessons learned and best practices
under the theme of “Transforming Health Care through Leadership, Innovation,
and Accountability”. This report outlines the key takeaways, highlighting some
outstanding examples across Uganda, captured from the 49 oral presentations
and 55 poster presentations over the three days of the 4th Annual Health Care
Quality Improvement Conference, specifically focusing on leadership,
innovation, and accountability.
Institutionalising quality improvement The Ministry of Health (MOH) has long prioritised assuring and improving
quality of care for all people in Uganda. Since 1994, the MOH have worked hard
to ensure there are formal structures in the health care system to assure,
improve, and foster quality of care in all health facilities across the country. In
1994, the Ministry of Health established the Quality Assurance Programme to
support quality health service delivery in our decentralised system. Although
the programme made great strides in forming a quality assurance committee,
wide-scale training of district health teams and district leaders in quality
assurance management, and developed manuals and guidelines for health
workers, it was soon determined in 1998 that more resources were necessary
to improve quality of care. This led the MOH to turn the Quality Assurance
Programme into the now existing Quality Assurance and Inspection
Department (QAID).
Since the establishment of QAID, the MOH has made achievements in improving
the capacity of health workers to assure and continuously improve quality and
improve service coverage quality of care and improved health outcomes.
In an effort to continuously improve quality of service delivery and health
outcomes across the country, the MOH conducted a situation analysis in 2010
to identify gaps and challenges to address. The MOH identified the need to
better institutionalise quality improvement in health service delivery, integrate
quality improvement interventions in all programmatic areas, streamline and
guide efforts among partners and health facilities, as well as set clear national
standards, recommended tools and approaches. This led to the development of

6 | P a g e
the first Health Sector Quality Improvement Framework & Strategic Plan
2010/11-2014/15. The goal of this plan was to provide a common framework
for all public and private health institutions, partners, and stakeholders to
coordinate, plan, mobilise resources, implement, monitor and evaluate quality
improvement initiatives in Uganda.
Last year, the MOH again rigorously evaluated the implementation of the Health
Sector Quality Improvement Framework & Strategic Plan 2010/11-2014/15.
The evaluator found that over the period of 2010 to 2015, there were many
achievements in the area of quality. As the first quality improvement
framework for the country, it provided clear guidance to government, partners,
health facilities and others working on quality interventions in their area.
Furthermore, a National Quality Improvement Coordination Committee and
Regional, District, and Facility Quality Improvement Committees, with
designated quality focal persons were established across Uganda. This assisted
in institutionalising continuous quality improvement and accountability for
quality in a decentralised manner. In strengthening the formal infrastructure
for quality improvement and assurance, the MOH has been able to have greater
participation and motivation among health workers and partners to improve
quality in their facility of operation. Using recommendations of this evaluation,
the MOH/QAID revised the Quality Improvement Framework and Strategic
Plan in line with the Health Sector Development Plan 2015/16 – 2019/20.
Objectives 3 is to strengthen the
framework for documentation,
reporting and sharing quality
improvement knowledge.
In order to provide a platform to
share best practices, successes, and
challenges across Uganda, the
Ministry of Health established the
Annual Health Care Quality
Improvement Conference. This
conference invites frontline health
workers, policy makers, academics,
researchers, and implementers to
Box 1: Significant improvements
The recent Uganda Demographics and Health Survey
(2016) report we have registered significant
progress in last five years (2011-2016) on the key
health sector performance indicators:
Total Fertility rate reduced from 6.2 to 5.4
Infant Mortality Rate (IMR) has reduce from
54 to 43 per 1000 live births.
Under 5 mortality reduced from 90 to 64 per 1000 live births
Mothers delivering in health facilities increased from 57% to 73%
Maternal Mortality Ratio (MMR) has reduced
from 438 to 368 per 100,000 live births.

7 | P a g e
come together on an annual basis to discuss achievements to date and the way
forward.
Last year, the conference hosted approximately 500 national and international
presenters, participants, keynote speakers, and distinguished guests. The 3rd
Annual Conference also served as the platform to launch the Second Quality
Improvement Framework and Strategic Plan (2015/16-2019/20). The plan
was disseminated to all districts and is currently being implemented in 70% of
the districts with support from partners. The Plan emphasizes implementation
of 5S (sort, set, shine, standardise, sustain) as a foundation for Continuous
Quality Improvement (CQI).
This year, the 4th Annual Conference had over 450 national and international
presenters, participants, keynote speakers, and distinguished guests. The 4th
Annual Health Care Quality Improvement Conference had the theme of
“Transforming Health Care through Leadership, Innovation, and Accountability”.
The MOH worked hard to bring together international experts and key
stakeholders from all levels of our health system to discuss best practices,
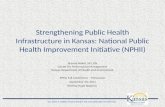
Figure 1- Hon. Minister of Health, Dr. Jane Ruth Aceng (third from left), launching the Service Standards and Service Delivery Standards at the 4th National Health Care Quality Improvement Conference. (Photo: Bryan Tumusiime, URC)

8 | P a g e
lessons learned, and way forward in strengthening and improving the health
system governance structures, supply chains, information systems, financing,
human resources, infrastructure, service delivery, and patient safety.
It also hosted the launch of two key documents, the Service Standards and
Service Delivery Standards and Maternal and Perinatal Death Surveillance and
Response (MPDSR), and a new and improved Ministry of Health online
knowledge management platform.
The 4th Annual Health Care Quality Improvement Conference The 4th Annual Health Care Quality Improvement Conference brought together
all of the main sets of health actors, citizens, clients, providers (public and
private), educational institutions, and pharmaceutical companies, Honourable
Members of Parliament, and MOH officials present.
The objectives of the conference were to:
Share experiences, challenges, and opportunities and tested solutions in
implementation of QI in health care in Uganda and other countries;
Provide feedback to stakeholders;
Provide an opportunity for peer learning on qi among health workers and
other stakeholders; and
Mobilise support resources and attention from leaders and financing
actors towards of quality of care improvement.
The conference was grounded in that a strong healthcare system can only be
achieved and sustained by well-trained, accountable, and innovative leaders.
Efforts to strengthen leadership in healthcare systems in Uganda must revolve
around building a new generation of leaders who are innovative, ethical, and
committed to improving health outcomes.
The Hon. Minister kicked off the conference with the launch of the Service
Standards and Service Delivery Standards and Maternal and Perinatal Death
Surveillance and Response (MPDSR), and a new and improved Ministry of
Health online knowledge management platform.
Key takeaways Three keynote speakers were carefully selected based on their extensive
experience in implementing quality improvement interventions in Uganda and

9 | P a g e
internationally. They articulated experiences in the context of the session
theme, discussing successful stories of leadership, innovations, and
accountability.
On Day 1, Dr. M. Rashad Massoud, Director
of the USAID ASSIST Project and Senior Vice
President for University Research Co., LLC.
(URC) gave a presentation titled
Demystifying quality improvement. Dr.
Massoud went over the core principles of
quality and improvement, reminding
participants to not forget the foundation of
quality improvement and not get lost in the
confusing terminology used within the field.
He shared experiences of successes internationally, including in the United
States, Scotland, Mali, and South Africa and the direction the global sphere is
headed in terms of improvement.
On Day 2, Professor Gerald Karyeija, Uganda Management Institute (UMI) gave
a presentation on Leadership and accountability for quality health care. He
discussed the use (demand and uptake) of health services is sometimes a
problem, however the use of leadership, accountability and stewardship can
help overcome these challenges. He emphasised the need to see the provision
of quality care as more than just “good surgeries and procedures”, but as a
culture within and outside the health facility. It must also include how health
workers speak to their patients, by understanding the value of satisfying the
patient. Professor Gerald’s helped the audience to unpack what transformative
leadership could look like, within the resource constrained Ugandan health
system. Connecting leadership with accountability, the Professor noted that, as
decision-makers and agenda setters, leaders are obligated to answer any
questions regarding their decisions or actions. This makes leaders accountable
to the health system, to their colleagues, and to the patients and communities
who utilise the health services.
Dr. M. Rashad Massoud
“enabled me to understand
that quality care is what
happens at all points of service
and meets client needs”.
– Evaluation respondent

10 | P a g e
On Day 3, Dr. Eleuter Samky, Mbeya
Regional Referral Hospital, Tanzania,
discussed Mbeya Regional Referral
Hospital’s experience implementing Sort,
Set, Shine, Standardise, and Sustain (5S)
since 2007, when the concept was first
introduced to staff. Before 2007, Dr. Samky
showed visuals of the dire state of the
hospital, where medical records were not
filed but actually over flowing and in a
completely disorganized manner. Beds and trolleys had been waiting to be
repaired for over 6 months, and Dr. Samky noted that staff minds and current
processes were equally disorganised. During this time, multiple quality
improvement interventions were being implemented, however there was no
clear leadership, coordination, or management, thus resulting in lack of
accountability and motivation of staff to improve quality.
The hospital saw increased ownership of work processes, attitude change,
decreased conflicts at work, and strong team work. The safety at the workplace
increased, as well as increased engagement, professionalism and excellence.
Leadership Leadership is about
motivating staff, leading
by example, and
competently directing
health resources and
working across sectors
to get healthcare that is
acceptable, equitable,
and safe. Most
presentations
emphasised the role of
leadership, including
district influences, in
the creation and
functionalisation of
“He made me understand why I
was getting stuck at one point in
progressing with 5s.”
– Evaluation respondent on Dr.
Eleuter Samky’s key note address
Figure 2- Participants were actively engaged throughout the three-day conference. (Photo: Bryan Tumusiime, URC)

11 | P a g e
quality improvement teams/committees to implement quality improvement
initiatives.
A common finding was financial motivation is not enough to motivate health
workers, non-financial motivation is also essential for improved quality service
delivery, which is where leadership comes in. Leaders must understand their
health workers’ needs, priorities, perspectives. By involving them in leadership
decisions, or in the understanding of leadership decisions, they will produce
higher quality results. For example, while establishing working schedules,
health workers should be consulted and schedules modified to best fit their
needs (where possible). This section further highlights some of the strong
leadership examples shared over the three days of the conference.
In Isingiro South Health sub-district, Nyakitunda Health Center III was able to
improve elimination of mother to child transmission (EMTCT) outcomes
through recognition and reward of frontline providers and patients. All
children who tested negative at the end of 18 months were recognised and
rewarded during the annual graduation ceremonies, and staff who gave care to
mother-baby pairs were also recognized by presentation of a certificate.
Through this recognition of facility leadership and the results of their efforts,
exceptional prevention occurred. Families and providers were both motivated
to eliminate transmission from mother to child.
Another leadership example was shared by Kanungu Health Centre IV. They
were able to reduce irrational drug use at the facility by the in-charge providing
strong leadership and guidance of her facility staff. She would personally
follow-up on their diagnoses of patients, by checking their notes and
prescription of drugs to malaria patients. Through patience, hard work, and
mentorship, she was able to reduce irrational drug use and improve health
worker confidence in diagnosis and prescription of medication.
Mbale District cited a direct relationship between leadership involvement and
the success of their quality improvement efforts. He emphasised the role of
support/supervision meetings with the health facilities and quality
improvement teams throughout for their success.
Although many presentations and discussions surrounded examples of
successful leadership across Uganda, common challenges faced by leadership
also arose.

12 | P a g e
Limited resources for rolling out policies and quality improvement
initiatives
Weak information systems in place
Innovation Over the three days, evidence of many low-cost innovations used in areas
throughout Uganda and internationally were shared. From using SMS services
to increase voluntary male medical circumcision (VMMC) uptake by young men
to using patient advocates to demand quality services to graduation
ceremonies that reward both health workers and patients for eliminating
mother to child transmission of HIV. This section highlights some of the
successful innovations shared to improve quality.
Technology
The USAID-HIWA project discussed the use of mobile health (mHealth) to
improve uptake and post-operative outcomes of VMMC in Uganda. The project
used mHealth tools such as mobile phone text messages, which improved
uptake of VMMC in men. 80% of men who received an SMS, returned for the
service.
Another mHealth example was the use of m-TRAC, the government-led
initiative to track and send messages to the health centre giving out malaria
drugs when drugs are used without patients being positive for malaria. m-TRAC
can also be used to assess stock outs and excess drugs.
Community engagement
Using existing community structures, such as Village Health Teams (VHTs) to
do sensitisation and active case finding was found to be very helpful to
“Innovation does not have to be complex, it
can be the use of existing resources in an
innovative manner to positively transform
health care.”
– Hon. Dr. Jane Ruth Aceng, Minister of
Health

13 | P a g e
minimise use of resources. One example of using existing community structures
given was the use of “sputum riders” or boda boda drivers who collected
sputum from the community during active TB case finding.
Buhweju District used prisoners to clean health facilities in exchange for free
screening services. Prisoners were provided technical gear when cleaning and
there was a supervisor to ensure safety. If facilities had no access to prison
services, they organized their own citizens to participate in periodic cleaning
as a social responsibility. This motivated staff members as the environment
they worked in was clean, safe, and secure.
Masafu Hospital utilised an adolescent peer support group, whereby
adolescents volunteered at the hospital, supported registration, filing, and
other administration duties. This helped get adolescents directly involved,
interested, and informed about health service delivery.
Including special groups, such as adolescents, in the development of
interventions that target them was found to be crucial to the success quality
improvement. ASSIST developed a process to engage adolescents in service
delivery that included adolescent feedback and input throughout the process.
This resulted in higher adolescent attendance and retention at the health
facilities and consequently, increased adolescent ownership of programming,
improved livelihood development of adolescents, creation of adolescent
feedback loop, and increased awareness of adolescent services.
In general, using advocates for patient safety is an effective way to increase
ability to identify, report and resolve patient safety issues, as well create a link
between patients and health workers.
Low-cost solutions
In a high patient volume facility in Rakai, facility staff were able to improve viral
load testing and uptake by use of viral load VL month stickers to remind clients
and providers of annual viral load due dates. Client files were checked and then
stickers were given to determine when clients should come back in. For virally
unsuppressed clients, no stickers were placed. Facility staff saw a 73% increase
in routine viral load testing over a year period. This also is an example of
strengthening accountability for both the patient and health facility in
conducting follow-up.

14 | P a g e
The Kabale District quality improvement team conducted a root cause analysis
to identify gaps in procedures that limit uptake of IPTp2. They tested changes
and determined they should stock check for Fansidar at health facilities,
conduct monthly data reviews, distribute multi-use metallic cups and water for
directly observed treatment- short-term (DOTS) so mothers could take
medicines there and then, and track performance and employ corrective
measures where necessary. Through the process improvement and
introduction of the innovative use of multi-use metallic cups, Kabale District
saw an increase in IPTp2 uptake from 67% to 98% since 2015.
These examples confirm the Hon. Minister of Health, Dr. Jane Ruth Aceng’s
statement “innovation does not have to be complex, it can be the use of existing
resources in an innovative manner to positively transform health care”.
Accountability Examples of increasing
accountability to improve
care also came out strong
throughout the conference.
However, they were
strongly interlinked with
examples of leadership and
difficult to separate the two.
Examples were shared
regarding strengthening
governance structures, including
the establishment of committees
and supportive supervision, to establishment of a regional learning network.
Many presenters shared the importance of using quality improvement teams
and/ or committees to establish culturally and contextually appropriate
targets, monitor progress and follow-up on actions. These committees also
assisted in the assurance that targets were in line with national standards.
Overall, governance enacted by the district level government, and public health
facilities, with goals outlined by national standards/ Ministry of Health
demonstrated good governance and accountability.
Figure 3-Dr. Alex Muhereza, Technical Adviser, USAID ASSIST Project. (Photo: Bryan Tumusiime, URC)

15 | P a g e
Mbale District noted the formation and functionalisation of quality
improvement teams at health facilities in Mbale was a prerequisite for
sustainable health outcomes. The use of the quality improvement teams
allowed them to track work and progress and hold team members accountable.
Additionally, the constant engagement with stakeholders in the health sector
was cited as necessary for buy in, support, and accountability of the work. As
stakeholders include donors, implementing partners, and communities all hold
an interest in seeing quality improved continuously.
Kamwenge District noted that districts are very busy with many competing
activities. In response to this challenge, Kamwenge District coordinated a joint
planning meeting with all implementers to avoid conflict, track ongoing
projects, and increase transparency among all partners. They integrated the
movement plans and enriched the mentorship content to include multiple
thematic areas (HIV/AIDS, TB, and leprosy). This allowed for all partners to
understand the work that was currently ongoing and for all to assist in the
strengthening of mentorship training across all programmes.
The Uganda Regional Learning Network (URLN) across 14 facilities identified
critical gaps in maternal child health and developed trainings, skills labs, and
mentorship and supervision programmes. The six training programmes
covered partograph use, essential newborn care, newborn resuscitation,
kangaroo care, antenatal corticosteroids, and infection prevention. Equipping
staff with knowledge and skills and holding them accountable to their work can
improve their confidence, health service delivery, and reduce external referrals.
The partograph is a good documentation tool useful during audits. In high
volume facilities in Southwestern Uganda, worked to establish the core reasons
why providers were not using partographs, even when they were available.
They assessed the barriers to use and then developed strategies to increase
utilisation. These barriers varied by site and therefore the interventions had to
be adapted to the needs of the facility. Monthly team reviews were conducted
to appreciate efforts and achievements as well as hold health workers
accountable for using the partographs.

16 | P a g e
Conclusion This conference reviewed successful leadership, innovations, and
accountability in improving quality across the health sector. The conference
created a platform for scientists, clinicians, activists, and community workers
to showcase their significant contribution towards improving quality of health
care in Uganda and featured a wide range of sessions and learning
opportunities on the current methods, approaches and developments in quality
improvement. However, it also served as a platform for participants to discuss
the challenges in relation
to quality service delivery
and strengthening
systems for sustained
quality improvement.
Improved service delivery
and health worker
motivation and retention
does not only require
financial incentives. A
conducive work
environment and strong
interpersonal
relationships are key factors. It does not matter the location and level of
development of a district, but rather the existence of strong leadership and
implementation of a plan for human resources for health and a positive work
environment.
The Hon. Minister of Health, Dr. Jane Ruth Aceng, closed the meeting with
powerful and inspiring closing remarks. She reminded participants to stay
grounded in the foundation for quality improvement and realities of
implementation, noting the closing panel presentation featuring leaders across
the continuum of care discussing improving quality from their own
perspectives. She said, “we all have a unique role to play. I encourage you all to
reflect not only on what you can do as an individual to improve quality, but also
understand the realities our colleagues are facing in their efforts. It is critical
that we understand each other’s perspectives in order to work together as a
Figure 4- Panel presenters discuss improving quality from various perspectives across the health system. (Photo: Bryan Tumusiime, URC)

17 | P a g e
team to improve quality of care. We can all be leaders and advocates of quality
and I encourage you to do so”.
She thanked the Quality Assurance and Inspection Department at the Ministry
of Health for leading the efforts in organising a successful 4th National Health
Care Quality Improvement Conference. She also gave special thanks to the
USAID ASSIST Project, JICA, METS, PEPFAR and other health development
partners for their support to make the conference a success. And lastly, but not
least, she thanked the key note speakers for accepting to attend and present in
the conference.
Way forward Uganda has many small islands of excellence, but there is a need to focus on
system-wide improvements. This conference emphasised that leadership and
execution are of the essence to the success of improvement. Moving forward, as
a community, we must work to:
Differentiate methods for measuring quality of care and methods for
improving quality of care. Measurement on its own does not lead to
improvement, we need to make changes in the process of what we are
doing to see changes.
End terminology and methodology confusion in Uganda. Instead
everyone must focus on the core principles and foundation of quality
improvement.
Ensure that lessons learned are properly harvested, managed, and
shared with a strong focus on attribution and generalisability.
The conference organisers distributed conference evaluation forms on the final
day of the conference, receiving 94 completed evaluations. Out of the responses
received, participants were overwhelmingly satisfied with the organisation,
content, and venue of the conference.

18 | P a g e
However, in the spirit of improvement, there is always area to improve. The
MOH is focused and committed on strengthening and improving the leadership
and accountability structures at all levels through innovative approaches to
ensure high quality of care for every person in Uganda. Moving forward, the
annual conference will resume, taking into account participant feedback
received to continuously improve the forum to facilitate and enable shared
learning across all stakeholders.
Box 2: Evaluation highlights
90% of respondents were satisfied with all three keynote speakers.
On average, 94.5% of respondents were somewhat or very satisfied with
organisation and content of the conference.
87% of respondents were satisfied with the learning opportunities at the
conference, with the large majority being very satisfied.
88% of respondents were somewhat or very satisfied with the panel session
on Day 3.

19 | P a g e
Annex I: List of conference organisers
1. Dr. Ssendyona Martin, MOH 2. Dr. Kakala Mushiso Alex, MOH 3. Dr. Okware Joseph, MOH 4. Ms. Florence Nampala, MOH 5. Dr. Herbert Kadama, MOH 6. Dr. Herbert Kisamba, USAID ASSIST Project 7. Dr. John Byabagambi, USAID ASSIST Project 8. Ms. Clare Asiimwe, JICA 9. Dr. Tumwesigye T. Benson, MOH
10. Dr. Esther Karamagi Nkolo, USAID ASSIST Project 11. Dr. Sarah K. Byakika, MOH 12. Dr. Mwebesa G. Henry, MOH 13. Ms. Charity Kyomugisha- Nuwagaba 14. Ms. Barbara Komujuni, USAID ASSIST Project 15. Ms. Amanda Ottosson, MOH 16. Mr. Naoki Take, JICA 17. Mr. Julius Ssendiwala, METSS 18. Mr. Hiroshi Tasei, JICA 19. Dr. Julius Amumpe, MOH 20. Dr. Simon Muhumuza, METSS 21. Ms. Tamara Nyombi Nsubuga, USAID ASSIST Project 22. Dr. Richard Kagimu, USAID ASSIST Project 23. Mr. Alfred Awio, USAID ASSIST Project 24. Ms. Martha Stacey Kiryewala, USAID ASSIST Project 25. Dr. Juliet Tumwikirize, USAID ASSIST Project

Anex II: Evaluation results
Category
Background information
First time attending compared to last conference Why did you attend Fulfill reason for
attendance
1-yes, 2-no Breakdown
0-not applicable, 1-better, 2- same, 3-
worse Breakdown
1-speaker oral, 2-speaker poster, 3-
networking, 4-content, 5-personal
growth and development Breakdown
1-yes absolutely, 2-yes but not full
extent, 3-no Breakdown
Total
1 75
0 75 1 22
1 75 1 14 2 22
2 19
2 5 3 39
2 15 3 0 4 53
Total response 94 Total response 94
5 65
3 1 1 reason for attending 42
2 reasonns for attending 15
Total response 91
Blank 0 Blank 0 3 or more reasons for
attending 37 Blank 3
Total responses 94
Percentage breakdown
% First time
attendance 80%
% 2nd or more time attendee considered
conference better 74% % with only 1 reason
for attending 45%
% completely
fulfilled reason to
attend 82%

1 | P a g e
% attended
in the past 20%
% 2nd or more time attendee considered
conference same 26% % for 2 reasons for
attending 16%
% partially fulfilled
reason to attend 16%
% 2nd or more time attendee considered
conference worse 0% % for 3 or more
reasons for attending 39%
% not fulfilled
reason to attend 1%
Findings
80% of respondents were first time attendees, 20% had attended at least 1 previous QI Conference.
Of respondents who had attended a previous QI conference, 74% felt the 4th National QI Conference was better than the previously attended conference(s). 26% felt the 4th National QI Conference was the same as past conference(s).
Majority of respondents had attended the conference for personal growth and development and content. 45% had only one reason to attend, 39% had 3 or more reasons to attend.
82% of respondents felt the conference completely fulfilled their reason for attendance, 16% felt it partially fulfilled their reason to attend.

2 | P a g e
Satisfaction with content
Organisation Overall content Day 1 keynote Day 2 Keynote Day 3 keynote
1- very satisfied, 5-
very dissatisfied,
0-did not attend Breakdown
1- very satisfied, 5-
very dissatisfied,
0-did not attend Breakdown
1- very satisfied, 5-
very dissatisfied,
0-did not attend Breakdown
1- very satisfied, 5-
very dissatisfied,
0-did not attend Breakdown
1- very satisfied, 5-
very dissatisfied,
0-did not attend Breakdown
1 66 1 52 1 64 1 60 1 60
2 24 2 31 2 18 2 21 2 20
3 2 3 5 3 5 3 7 3 6
4 2 4 1 4 0 4 0 4 0
5 0 5 0 5 0 5 0 5 0
0 0 0 0 0 4 0 2 0 3
Total response 94
Total response 89
Total response 91
Total response 90
Total response 89
Blank 0 Blank 5 Blank 3 Blank 3 Blank 5
% very satisfied 70%
% very satisfied 58%
% very satisfied 70%
% very satisfied 67%
% very satisfied 67%

3 | P a g e
% somewhat satisfied 26%
% somewhat satisfied 35%
% somewhat satisfied 20%
% somewhat satisfied 23%
% somewhat satisfied 22%
% neutral 2% % neutral 6% % neutral 5% % neutral 8% % neutral 7%
% somewhat dissatisfied 2%
% somewhat dissatisfied 1%
% somewhat dissatisfied 0%
% somewhat dissatisfied 0%
% somewhat dissatisfied 0%
% very dissatisified 0%
% very dissatisified 0%
% very dissatisified 0%
% very dissatisified 0%
% very dissatisified 0%
Breakout session content Day 3 panel session Networking opportunities Learning opportunities
1- very satisfied, 5-
very dissatisfied,
0-did not attend Breakdown
1- very satisfied, 5-
very dissatisfied,
0-did not attend Breakdown
1- very satisfied, 5-
very dissatisfied,
0-did not attend Breakdown
1- very satisfied, 5-
very dissatisfied,
0-did not attend Breakdown
1 42 1 52 1 26 1 54
2 35 2 29 2 36 2 21
3 13 3 8 3 21 3 8
4 1 4 2 4 2 4 2
5 0 5 0 5 0 5 0
0 1 0 1 0 2 0 1

4 | P a g e
Total response 92
Total response 92
Total response 87
Total response 86
Blank 2 Blank 2 Blank 7 Blank 8
% very satisfied 46%
% very satisfied 57%
% very satisfied 30%
% very satisfied 63%
% somewhat satisfied 38%
% somewhat satisfied 32%
% somewhat satisfied 41%
% somewhat satisfied 24%
% neutral 14% % neutral 9% % neutral 2% % neutral 9%
% somewhat dissatisfied 1%
% somewhat dissatisfied 2%
% somewhat dissatisfied 2%
% somewhat dissatisfied 2%
% very dissatisified 0%
% very dissatisified 0%
% very dissatisified 0%
% very dissatisified 0%
Findings
On average, 94.5% of respondents were somewhat or very satisfied with organisation and content of the conference.
90% of respondents were satisfied with all three keynote speakers.

5 | P a g e
88% of respondents were somewhat or very satisfied with the panel session on Day 3
Networking opportunities received the least amount of satisfaction among participants, only 77% were somewhat or very satisfied with networking opportunities available, with the majority only somewwhat satisfied
87% of respondents were satisfied with the learning opportunities at the conference, with the large majority being very satisfied.