
4. Ian Triplow - developing good governance... GOV011015
61
How to open a new hospital Successes and lessons at North Bristol NHS Trust Ian Triplow Associate Director of Programme Management Office
-
Upload
association-for-project-management -
Category
Business
-
view
759 -
download
1
Transcript of 4. Ian Triplow - developing good governance... GOV011015

How to open a new hospital
Successes and lessons at
North Bristol NHS Trust
Ian Triplow
Associate Director of Programme Management Office
Overview
This presentation will provide an overview of the learning from the building, commissioning, move and opening of the new £432m Brunel building at Southmead Hospital, North Bristol NHS Trust.
On 28th May 2014, the Brunel building – with 800 beds, 24 operating theatres, over 7000 staff, costing £432m – was declared fully open. This was the culmination of almost a decade of design, building, planning and business transformation at North Bristol NHS Trust, and a final 3 months spent commissioning the new building, installing over £12m of equipment and finally moving all the services (and 540 inpatients) to their new home.
This talk will present a summary of the final report from the move & transformation programme which oversaw the final few months from February to May 2014. This will include an overview of the journey that the organisation went through to build and open the Brunel building, lessons learned along the way, and changes that were made to project and programme governance through its timeline. Why a single SRO is never sufficient
What to do with gateway review outcomes
How to maintain control but also empower on an organisation-wide scale

Background

Background - NHS
Since its launch in 1948, the NHS has grown to become
the world’s largest publicly funded health service. It is
also one of the most efficient, most egalitarian and most
comprehensive.
The NHS was born out of a long-held ideal that good
healthcare should be available to all, regardless of
wealth – a principle that remains at its core.

Background – Acute Hospitals
Formal definition
Acute care may require a stay in a hospital emergency
department, ambulatory surgery centre, urgent care centre or
other short-term stay facility, along with the assistance of
diagnostic services, surgery, or follow-up outpatient care in the
community
Informal
It’s a place you wish not to go to but need to know its there for
you to keep you healthy from age 0 to 100+
It’s the specialised end of the NHS – specialising in emergency
unplanned care – and the follow up through in and outpatient
work


North Bristol NHS Trust

North Bristol NHS Trust
North Bristol NHS Trust is the largest hospital trust in the
South West of England, providing hospital and
community healthcare to the residents of Bristol, South
Gloucestershire and North Somerset.
We are also a specialist regional centre for a number of services
including neurosurgery, renal medicine, plastics, burns,
orthopaedics and major trauma.
The Trust provides services to a local catchment
population of 905,000
The Trust has a wider catchment population of
approximately 3 million for our specialist services

Facts and figures
The Trust has a workforce of over 9,000 with a funded
establishment in 2013/14 of 7,753 whole time
equivalents.
Medical Staff – 928 wte
Nursing, midwives healthcare assistants – 3,085 wte
Scientists and Therapies – 1,299 wte
Ancillary and estates – 885 wte
Administration – 1,395 wte
Managers – 161 wte

Frenchay Hospital History
The hospital, situated in the grounds of a Georgian mansion, Frenchay Park, started life as a TB hospital in 1921
In 1931, five purpose-built buildings were constructed to extend the hospital beyond the original house. Concerns about the possibility of heavy bombing casualties led to the hospital being greatly
expanded between 1938 and early 1942. Although Bristol was severely bombed, the new facilities remained unused
When US forces arrived in 1942, the city handed the new hospital facilities over to the Americans. Further expansion to the facilities including 27 wards, occurred in late 1942. The Americans
used the hospital mainly as training facility for their medical staff.
After D-Day the hospital was used in earnest. Casualties were flown into Filton or arrived by train from the channel ports. Between 5 August and 31 December 1944 a total of 4,954 patients were discharged from
Frenchay.
The National Health Service acquired the hospital in 1948
Over the last 60 years, the hospital facilities have been slowly modernised, but many wartime buildings were still very much in evidence this year

New and old together

A New Hospital

New Facilities
A decision was made in 2005 to create a single acute
hospital at Southmead and transform the Frenchay
hospital into a community facility
In 2010, Carillion was formally selected to design and
build the new hospital and construction work began
Completion of the main building was in March 2014
The Brunel building comprises 114,000 m2 with a capital
cost of £432 million
It includes 800 beds, 24 theatres and a full range of
services for a population of 400,000 people.

Brunel Building Programme
The Brunel Building is a private finance initiative (PFI)
After 10 years of focus on the completion of the new
acute hospital at Southmead the Brunel building was
handed over to North Bristol Trust on 26th March 2014.
This work was undertaken by the NBT capital planning
team with a mix of specialists in building, clinical design,
operational pathways and more
The majority of this team were recruited from with the
NHS and more specifically NBT

Brunel Building – December 2010

Brunel Building – June 2011

Brunel Building – July 2012

Brunel Building – August 2013

A new way of working

Change programme
A major change programme “Road to 2014” was set up to design and delivery services in new ways of working in time for the new building utilising the new facilities, capability and staffing models that the building allowed
This programme “Building Our Future” was resourced through a mix of project managers internal and external to the NHS – supported with clinical redesign experts
To deliver this Building Our Future was set up as a completely independent governance structure to the Trust Seperate Board, SRO, Management Team and Standing Orders
and SFI’s

What had to change?
The clinical models changed for Inpatients
Both emergency and elective
Outpatients
Equipment
Storage
Support
The workforce models (and teams) changed for Wards
Theatres
Administration
Support

Gateway Review

All into One programme
The Project Assessment Review Team, in December
2013, recognised that the separate components within
the overall Move Programme had to be combined single
entity, with one critical path and one governance.
In effect the building and the services that were going to be
together – now needed to be together
Building Our Future was no longer needed – the Future had arrived
The Trust concentrated on the Move and the building alone
Suspension of a lot of national reporting and controls
The Move and Transformation Programme was formed –
and run at high pace from January 2014 until June 2014

Governance Structure
Trust Board
MOVE and Transformation
Board
MOVE Delivery Board
Existing Sub-structure
Reporting Workstreams
Single Programme
Plan
Brunel Construction
MOVE projects
Facilities Portfolio
IM&T projects
Themes
Directorates
JIGSAW
Service Transfers

Summary Reporting – Exception Based
Brunel Construction
MOVE projects
Facilities Portfolio
IM&T projects Themes Directorates JIGSAW Service
Transfers
Single Programme Summary and Highlight report
Risk review Action
Chasing Programme Overview
Decision Planning
Interdependency Management
Communication Assumption
Management Upward
Reporting
WORKSTREAMS
PMO
INTRANET SITE
(WEEKLY)

All heading in the same direction

Governance - detail
Risk management Both Move and BAU are managed through the single overview
Riskweb system
All Trust risks recorded, now including high-level CCG risks
Weekly check of high risks, daily chasing of mitigating actions
Issue management Central issues log for Move, daily chasing of mitigating actions
Decision management All Committee / Executive level and significant decisions logged
Daily system to remind decision makers and record decisions
Centralised daily reporting by PMO on all matters
Single programme plan established with critical tasks for Move identified and tracked

Business as Usual incl. Capital Programmes
Governance All directorates continue to have monthly performance executive
review meetings covering the balance reporting of performance / activity / quality / workforce / finances
This continued throughout the Move preparation and into the new hospital
All other capital developments managed through our “Jigsaw Programme”
Integrated Performance Report The Trust had an integrated performance report covering all
executive performance reports to the board in a single format
This is used throughout the organisation and board
The report will continues to develop based on evolving issues and areas of focus – with a rotation through other areas as applicable by time in reporting year
Simple Reporting

Go/No Go checklist Last date for Go No Go decision: 30 March 2014 RAG
Reason: Leaflets advising the public of the dates of the move will be issued.
General
1
The building will be handed over in a good state of repair, with all key systems fully functioning (lifts, heating,
lighting etc) and free of major defectsGreen
2
The list of items on the snagging list requiring remedy are acceptable in terms of volume and complexity for
operation of the building Green
3 The fire strategy for Brunel has been approved Amber
4 Contingency plans are in place for major incidents to enable business continuity Amber
5 Critical operational policies are in place Amber
People and Services
6 The order of moves is finalised and all services know the date of their move Green
7 Move plans for each service are in place and understood by the service teams Green
8
All necessary transport arrangements for transferring patients are in place and are in conjunction with the order
of moves, and there is written commitment from the service provider to meet the requirementsAmber
9 Contingency plans are in place in the event of unavailability of planned transport Amber
10 All staff have been trained to use and orientated to the building Green
Equipping & Environments
11 Any certificates, licenses and approvals necessary in advance of building occupation or use have been issuedAmber
12
All equipment necessary to run Brunel is ordered, in place (including transferred equipment) and
commissioned ready for useAmber
13 There are sufficient fittings in place to provide a comfortable environment for patients Green
14 The removals company has an agreed and finalised schedule of equipment moves for the full move period Green
15 Contingency plans are in place with the removals company to manage delays, increases in activity etc Green
16 All specialist removals companies have an agreed and finalised schedule of transfers for the full move periodGreen

Go/No Go checklist IM&T
17 All essential IM&T systems are in operation including wireless system, Cerner etc Red
18 Sufficient hardware (and software) necessary to get services underway within Brunel is in place Amber
19 All corporate IM&T systems are amended for the new operation in Brunel Green
20 Telephone systems are operational Green
Facilities Management
21 The building has had a clinical clean and has been signed off as ready for use by infection control Green
22 The soft FM team are trained to operate in Brunel Green
23
The building is stocked through a first fill and ready for operation for all areas - pharmacy and each zone
(theatres, critical care, wards etc)Amber
24 Catering systems and prep areas are cleaned, stocked, tested and ready to feed patients and staff Amber
25 A process flow is in place to govern safe flow of instrumentation between SSD and Brunel Amber
26 The service yard is operational with an agreed schedule of deliveries and management processes in place Green
27 A system is in place to move supplies, consumables etc through the building (e.g. AGV) Amber
28 Parking arrangements for patients and visitors are in place Green
29 Transport arrangements for staff are in place Amber
Communications
30
Communications are prepared and processes in place ready to communicate the date of the move to patients
and the public (including GPs, patients, general public)Green
Operational
31 All schedules and staffing rotas are in place for theatres, outpatients and specialist diagnostics Green
32
There is sufficient staffing in place to operate a safe service across all key areas: outpatients, inpatients,
theatres, diagnostics, emergency department, critical careAmber
33 Administrative processes are in place to safely manage patients through the systems Red
34 Activity profiles are agreed in the period up to the move to Brunel to minimise risk to move Amber
35 All staff are allocated to their area of work Green
36 All staff have been trained in how their service will operate in terms of every task in the working day Amber
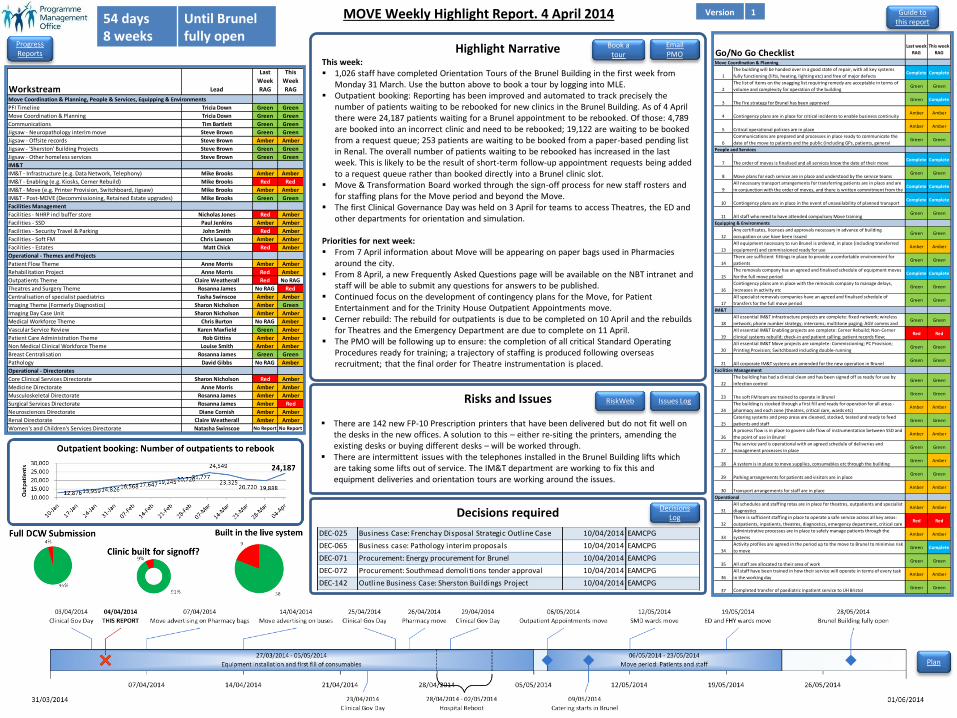
Highlight Narrative This week: 1,026 staff have completed Orientation Tours of the Brunel Building in the first week from
Monday 31 March. Use the button above to book a tour by logging into MLE. Outpatient booking: Reporting has been improved and automated to track precisely the
number of patients waiting to be rebooked for new clinics in the Brunel Building. As of 4 April there were 24,187 patients waiting for a Brunel appointment to be rebooked. Of those: 4,789 are booked into an incorrect clinic and need to be rebooked; 19,122 are waiting to be booked from a request queue; 253 patients are waiting to be booked from a paper-based pending list in Renal. The overall number of patients waiting to be rebooked has increased in the last week. This is likely to be the result of short-term follow-up appointment requests being added to a request queue rather than booked directly into a Brunel clinic slot.
Move & Transformation Board worked through the sign-off process for new staff rosters and for staffing plans for the Move period and beyond the Move.
The first Clinical Governance Day was held on 3 April for teams to access Theatres, the ED and other departments for orientation and simulation.
Priorities for next week: From 7 April information about Move will be appearing on paper bags used in Pharmacies
around the city. From 8 April, a new Frequently Asked Questions page will be available on the NBT intranet and
staff will be able to submit any questions for answers to be published. Continued focus on the development of contingency plans for the Move, for Patient
Entertainment and for the Trinity House Outpatient Appointments move. Cerner rebuild: The rebuild for outpatients is due to be completed on 10 April and the rebuilds
for Theatres and the Emergency Department are due to complete on 11 April. The PMO will be following up to ensure: the completion of all critical Standard Operating
Procedures ready for training; a trajectory of staffing is produced following overseas recruitment; that the final order for Theatre instrumentation is placed.
Risks and Issues
There are 142 new FP-10 Prescription printers that have been delivered but do not fit well on the desks in the new offices. A solution to this – either re-siting the printers, amending the existing desks or buying different desks – will be worked through.
There are intermittent issues with the telephones installed in the Brunel Building lifts which are taking some lifts out of service. The IM&T department are working to fix this and equipment deliveries and orientation tours are working around the issues.
MOVE Weekly Highlight Report. 4 April 2014 54 days 8 weeks
Until Brunel fully open
Decisions required
Guide to this report
Decisions Log
Issues Log RiskWeb
Email PMO
Progress Reports
Version 1
Plan
Workstream Lead
Last
Week
RAG
This
Week
RAG
Move Coordination & Planning, People & Services, Equipping & Environments
PFI Timeline Tricia Down Green Green
Move Coordination & Planning Tricia Down Green Green
Communications Tim Bartlett Green Green
Jigsaw - Neuropathology interim move Steve Brown Green Green
Jigsaw - Offsite records Steve Brown Amber Amber
Jigsaw - 'Sherston' Building Projects Steve Brown Green Green
Jigsaw - Other homeless services Steve Brown Green Green
IM&T
IM&T - Infrastructure (e.g. Data Network, Telephony) Mike Brooks Amber Amber
IM&T - Enabling (e.g. Kiosks, Cerner Rebuild) Mike Brooks Red Red
IM&T - Move (e.g. Printer Provision, Switchboard, Jigsaw) Mike Brooks Amber Amber
IM&T - Post-MOVE (Decommissioning, Retained Estate upgrades) Mike Brooks Green Green
Facilities Management
Facilities - NHRP incl buffer store Nicholas Jones Red Amber
Facilities - SSD Paul Jenkins Amber Amber
Facilities - Security Travel & Parking John Smith Red Amber
Facilities - Soft FM Chris Lawson Amber Amber
Facilities - Estates Matt Chick Red Amber
Operational - Themes and Projects
Patient Flow Theme Anne Morris Amber Amber
Rehabilitation Project Anne Morris Red Amber
Outpatients Theme Claire Weatherall Red No RAG
Theatres and Surgery Theme Rosanna James No RAG Red
Centralisation of specialist paediatrics Tasha Swinscoe Amber Amber
Imaging Theme (Formerly Diagnostics) Sharon Nicholson Amber Green
Imaging Day Case Unit Sharon Nicholson Amber Amber
Medical Workforce Theme Chris Burton No RAG Amber
Vascular Service Review Karen Maxfield Green Amber
Patient Care Administration Theme Rob Gittins Amber Amber
Non Medical Clinical Workforce Theme Louise Smith Amber Amber
Breast Centralisation Rosanna James Green Green
Pathology David Gibbs No RAG Amber
Operational - Directorates
Core Clinical Services Directorate Sharon Nicholson Red Amber
Medicine Directorate Anne Morris Amber Amber
Musculoskeletal Directorate Rosanna James Amber Amber
Surgical Services Directorate Rosanna James Amber Red
Neurosciences Directorate Diane Cornish Amber Amber
Renal Directorate Claire Weatherall Amber Amber
Women's and Children's Services Directorate Natasha Swinscoe No Report No Report
Go/No Go ChecklistLast week
RAG
This week
RAG Date Outstanding
Move Coordination & Planning
1
The building will be handed over in a good state of repair, with all key systems
fully functioning (lifts, heating, lighting etc) and free of major defectsComplete Complete
2
The list of items on the snagging list requiring remedy are acceptable in terms of
volume and complexity for operation of the building Green Green
3 The fire strategy for Brunel has been approvedGreen Complete
4 Contingency plans are in place for critical incidents to enable business continuityAmber Amber
5 Critical operational policies are in placeAmber Amber
6
Communications are prepared and processes in place ready to communicate the
date of the move to patients and the public (including GPs, patients, general Green Green
People and Services
7 The order of moves is finalised and all services know the date of their moveComplete Complete
8 Move plans for each service are in place and understood by the service teamsGreen Green
9
All necessary transport arrangements for transferring patients are in place and are
in conjunction with the order of moves, and there is written commitment from the Complete Complete
10 Contingency plans are in place in the event of unavailability of planned transportComplete Complete
11 All staff who need to have attended compulsory Move trainingGreen Green
Equipping & Environments
12
Any certificates, licenses and approvals necessary in advance of building
occupation or use have been issuedGreen Green
13
All equipment necessary to run Brunel is ordered, in place (including transferred
equipment) and commissioned ready for useAmber Amber
14
There are sufficient fittings in place to provide a comfortable environment for
patientsGreen Green
15
The removals company has an agreed and finalised schedule of equipment moves
for the full move periodComplete Complete
16
Contingency plans are in place with the removals company to manage delays,
increases in activity etcGreen Green
17
All specialist removals companies have an agreed and finalised schedule of
transfers for the full move periodGreen Green
IM&T
18
All essential IM&T infrastructure projects are complete: fixed network; wireless
network; phone number strategy; intercoms; multitone paging; AGV comms and Green Green
19
All essential IM&T Enabling projects are complete: Cerner Rebuild; Non-Cerner
clinical systems rebuild; check-in and patient calling; patient records flow; Red Red
20
All essential IM&T Move projects are complete: Commissioning; PC Provision;
Printing Provision; Switchboard including double-runningGreen Green
21 All corporate IM&T systems are amended for the new operation in BrunelGreen Green
Facilities Management
22
The building has had a clinical clean and has been signed off as ready for use by
infection controlGreen Green
23 The soft FM team are trained to operate in BrunelGreen Green
24
The building is stocked through a first fill and ready for operation for all areas -
pharmacy and each zone (theatres, critical care, wards etc)Amber Amber
25
Catering systems and prep areas are cleaned, stocked, tested and ready to feed
patients and staffGreen Green
26
A process flow is in place to govern safe flow of instrumentation between SSD and
the point of use in BrunelAmber Amber
27
The service yard is operational with an agreed schedule of deliveries and
management processes in placeGreen Green
28 A system is in place to move supplies, consumables etc through the buildingGreen Amber
29 Parking arrangements for patients and visitors are in placeGreen Green
30 Transport arrangements for staff are in placeAmber Amber
Operational
31
All schedules and staffing rotas are in place for theatres, outpatients and specialist
diagnosticsAmber Amber
32
There is sufficient staffing in place to operate a safe service across all key areas:
outpatients, inpatients, theatres, diagnostics, emergency department, critical careRed Red
33
Administrative processes are in place to safely manage patients through the
systemsAmber Amber
34
Activity profiles are agreed in the period up to the move to Brunel to minimise risk
to moveGreen Complete
35 All staff are allocated to their area of workGreen Green
36
All staff have been trained in how their service will operate in terms of every task
in the working dayAmber Amber
37 Completed transfer of paediatric inpatient service to UH BristolGreen Green
DEC-025 Business Case: Frenchay Disposal Strategic Outline Case 10/04/2014 EAMCPG
DEC-065 Business case: Pathology interim proposals 10/04/2014 EAMCPG
DEC-071 Procurement: Energy procurement for Brunel 10/04/2014 EAMCPG
DEC-072 Procurement: Southmead demolitions tender approval 10/04/2014 EAMCPG
DEC-142 Outline Business Case: Sherston Buildings Project 10/04/2014 EAMCPG
Book a tour

Move Period

Manager Checklist - April
Final sign-off from General Managers
To be completed pre-Move for every area
Includes:
Workforce
Training & Orientation
SLAs with Support Services
Workflows, Systems & Processes
Equipment, storage & consumables
Information technology
Clinician Checklist - April
Final sign-off from Clinicians
To be completed pre-Move for every clinical area
Includes: Clinical assessment tools
Documentation
Clinical pathways
Medical records flow
Information flow
Team Processes
SLAs with other services
Clinical rotas
Clinical competencies
Clinical equipment
Training, Orientation and
System Test

36
Order of Moves
• Southmead moved first
• Elective
• Logistically more straightforward
• Requirement for rapid decommissioning
• Frenchay followed
• Maintain Emergency Department access
• Clinical dependencies paramount
• Key Partners
• Harrow Green
• SWAST
• RAF

37

38
39
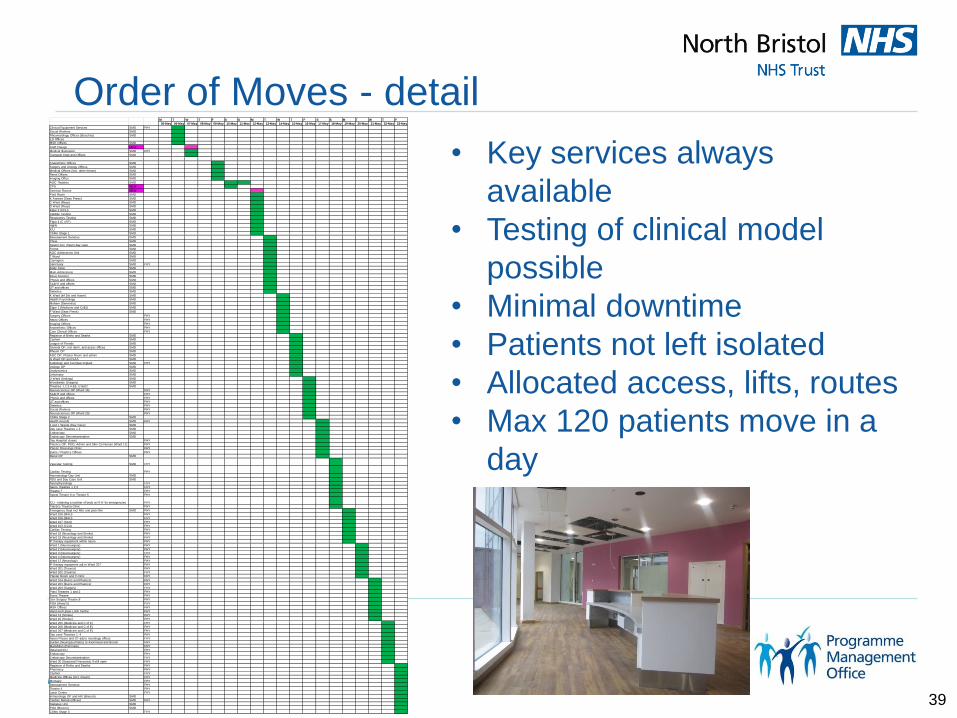
Order of Moves - detail
• Key services always
available
• Testing of clinical model
possible
• Minimal downtime
• Patients not left isolated
• Allocated access, lifts, routes
• Max 120 patients move in a
day
M T W T F S S M T W T F S S M T W T F
05-May 06-May 07-May 08-May 09-May 10-May 11-May 12-May 13-May 14-May 15-May 16-May 17-May 18-May 19-May 20-May 21-May 22-May 23-May
Clinical Equipment Services SMD FHY
Social Workers SMD
Rheumatology Offices (Beeches) SMD
ED Offices
MSK Offices SMD
Staff Change NEW
Medical Illustration SMD FHY
Transport Dept and Offices SMD
Anaesthetic Offices SMD
Surgery and Urology Offices SMD
Medical Offices (incl. other rheum) SMD
Renal Offices SMD
Imaging Office SMD
AOC Theatres SMD
CPU NEW
Seminar Rooms NEW
Post Room SMD
K Annexe (Seas Press) SMD
C Ward (Resp) SMD
D Ward (Resp) SMD
Elgar 2 (CCU) SMD
Cardiac Testing SMD
Respiratory Testing SMD
Elgar 4 (C of E) SMD
H@N SMD
ICU SMD
CSMs Stage 1 SMD
Bereavement Services SMD
Chew SMD
Severn incl. rheum day case SMD
Frome SMD
AOC Admissions Unit SMD
T Ward SMD
Carrington SMD
Sanctuary SMD FHY
Body Store SMD
Main Admissions SMD
Dexa Scanner SMD
Physio and offices SMD
SL&HT and offices SMD
OT and offices SMD
Dietetics SMD
K Ward (Inf Dis and Haem) SMD
Health Psychology SMD
Malvern (Dementia) SMD
Elgar 1 (Medicine and CoE)) SMD
F Ward (Seas Press) SMD
Surgery Offices FHY
Neuro Offices FHY
Imaging Offices FHY
Anaesthetic Offices FHY
Core Clinical Offices FHY
Registrar of Births and Deaths SMD
Cashier SMD
League of Friends SMD
General OP, incl derm, and assoc offices SMD
Rheum OP SMD
AOC OP, Plaster Room and admin SMD
G Ward OP and SAA SMD
Audiology and Cochlear Implant SMD FHY
Urology OP SMD
Urodynamics SMD
Lithotripsy SMD
U Ward (Urology) SMD
Woodlands (Surgery) SMD
Theatres 1,2,3,4 &8, U1&U2 SMD
Neurosciences OP (Ward 16) FHY
SL&HT and offices FHY
Physio and offices FHY
OT and offices FHY
Dietetics FHY
Social Workers FHY
Neurosciences OP (Ward 20) FHY
CSMs Stage 2 SMD
Health records SMD FHY
J and L Wards (Day Case) SMD
Day case Theatres x 2 SMD
Endoscopy SMD
Endoscopy Decomtamination SMD
Day Hospital closes FHY
Plastics OP, POD, Admin and Skin Ca Nurses (Ward 11) FHY
Plastic Dressings Clinic FHY
Burns / Plastics Offices FHY
Renal OP SMD
Vascular Testing SMD FHY
Cardiac Testing FHY
Haematology Day Unit SMD
RDU and Day Case Unit SMD
Neurophysiology FHY
Neuro Theatres 1,2,3 FHY
Theatre 7 FHY
Spinal Theatre 6 or Theatre 5 FHY
ICU - retaining a number of beds at FHY for emergencies FHY
Plastics Trauma Clinic FHY
Emergency Dept incl MIU and plain film SMD FHY
Ward 105 (MAU) FHY
Ward 106 (MAU) FHY
Ward 107 (SAU) FHY
Ward 103 (CCU) FHY
Cardiac Testing FHY
Ward 18 (Neurology and Stroke) FHY
Ward 19 (Neurology and Stroke) FHY
IP therapy equipment within neuro FHY
Ward 1 (Neurosurgery) FHY
Ward 2 (Neurosurgery) FHY
Ward 3 (Neurosurgery) FHY
Ward 4 (Neurosurgery) FHY
Ward 12 (Neurology) FHY
IP therapy equipment adj to Ward 207 FHY
Ward 201 (Trauma) FHY
Ward 202 (Trauma) FHY
Plaster Room and # clinic FHY
Ward 104 (Burns and Plastics) FHY
Ward 204 (Burns and Plastics) FHY
Ward 203 (Surgery) FHY
Plast Theatres 1 and 2 FHY
Burns Theatre FHY
Gen Surgery Theatre 8 FHY
POA (Ward 5) FHY
MSK Offices FHY
Hand and Upper Limb Centre FHY
Ward 13 (Stroke) FHY
Ward 15 (Stroke) FHY
Ward 205 (Medicine and C of E) FHY
Ward 206 (Medicine and C of E) FHY
Ward 207 (Medicine and C of E) FHY
Day case Theatres 1 -4 FHY
Neuro Physio and OT adj to neurology offices FHY
Burden (Neuropsychiatry) to Avonmead and Brunel FHY
MacMillan (Pall Care) FHY
Retained ICU FHY
Endoscopy FHY
Endoscopy Decomtamination FHY
Ward 30 (Seasonal Pressures) if still open FHY
Registrar of Births and Deaths FHY
Pharmacy FHY
Cashier FHY
Medicine Offices (incl. rheum) FHY
Mortuary FHY
Bereavement Services FHY
Theatre 4 FHY
Laser Centre FHY
Immunology OP and HIV (Brecon) SMD
Cardiac Rehab (offices) SMD FHY
Diabetes Unit SMD
POA (Brecon) SMD
CSMs Stage 3 FHY

40

Reflections and Lessons

42

Move Reflections – CEO comments
Moving into the Brunel hospital showed North Bristol NHS Trust at its very best. Over 500 patients, 24 of whom were critically ill, were successfully and
safely moved from Frenchay or Southmead into the new hospital over a two week period.
The values of our staff were fundamental to making this undertaking go so well. But significantly our approach to planning; which was inclusive, honest, when things needed attention, rigorous but not overwhelmingly bureaucratic, with decisions being taken quickly and communicated widely was pivotal in aligning effort, and building confidence as we got nearer to move date.
We had, and have, some brilliant skills and expertise but bringing in outside perspective and skills was a pivotal decision, it showed us willing to be open and to learn, and it helped us provide a single critical path, to ensure objective oversight and a single point of contact when things could fall between individuals or overlap.

So what were the lessons?
Communications
In an organisation over multiple sites communication (and
rumour control) are key and difficult
Keep it simple
Keep it frequent
1 page highlight is all that is needed
When moving – email isn’t there
Every external group will ask questions
There is never enough reassurance

Lessons Continued
Single Change Programme
The need for strong governance with a single SRO and single
critical path
That supports – not demands
The benefits of running the Command Centre structure
The lack of concern about hierarchy, meritocracy got things
done, not rank
Control with Empowerment
Delivering decisions and sticking to them
Monitoring and making clear and bound decisions is crucial, as
is the recording of these
Gateway reviews (internal and external) are crucial
Lessons Continued
Operational Focus
Target Standard Operating Procedures (SOPs) should be bedded in and routine before any physical move
Greater clinical & surgical design involvement would have avoided rumours and distraction
All major cross cutting work should be have an operational and clinical lead (if not the same person) and where identified project support for the life of the work
Ambitious timescales
That a 6 week period from handover to move was a real challenge
You can move a hospital in 2 weeks (just)
People have lives, the impact of 7 day working should not be overlooked - we need to look after all our people

Lessons Continued
Resources
Annual Leave control works
The importance of building a strong sense of team, based on
continuity – colleagues, programme, suppliers and business –
the positive attitudes and cooperative interpersonal skills
exhibited have been a real success
There is a difference between subject matter expert and project
management
And BOTH are needed
External support when needed should be used

Last Thoughts

49

50


Fun things that you would never predict
Trainers
Everyone involved in the move needed comfy shoes
But all are healthily now!
Helicopter testing
Start small and increase in size
Big means BIG
Swipe access doors
Great for security
Not so much for tours
The restaurant
Serious things we learnt
We did lose beds
Not patients – but beds
Boxes boxes everywhere
100’s just dissappeared
Packing everything
Even the clocks – you can’t spring clean enough
Less meetings is good
And sticking to it
No really

Final thoughts
It’s a beautiful building
With outstanding staff
Its here for the population of Bristol
For a long time

But don’t come if you don’t need to

Q&A

Workshop

Workshop
As with every project and every organisation we’ve all
worked in – there is no one right answer to the tough
questions
In fact the right answer for one – may be the wrong for another
Project governance is not about sticking to a playbook
Its about ensure that the plays deliver the goals
Neithertheless – lets see if we can all go away with some
more plays

Group sessions
From now to 3.25 – split into 3 groups
At 3.25 we will discuss each topic as a room – so before
that pick / punish a speaker
Ten minutes feedback and Q&A per topic

Workshop Groups
1. Why a single SRO is never sufficient . . .
Conflict v collaboration – top tips?
What’s the best way to deal with multiple leaders?
2. What to do with gateway review outcomes?
Who addresses the outcomes?
Who reassurance on the actions?
3. How to maintain control but also empower on an organisation-wide scale . . .
How do projects empower?
What control is then needed?

This presentation was delivered
at an APM event
To find out more about
upcoming events please visit our
website www.apm.org.uk/events


















