32199201 Trauma From Occlusion Perio

of 27
-
Upload
geeth-sadasivam -
Category
Documents
-
view
527 -
download
3
Transcript of 32199201 Trauma From Occlusion Perio
TRAUMA FROM OCCLUSION
CONTENTS1. Definition 2. Classification (acute ,chronic ,primary ,secondary) 3. Stages of tissue response when occlusal force is increased. A. Injury B. Repair C. Adaptive remodeling of periodontium 4. Effect of insufficient occlusal force. 5. Influence of trauma from occlusion on progression of marginal periodontitis. 6. Diagnosis 7. Treatment 8. References
TRAUMA FROM OCCLUSION:OCCLUSION:Definition:Definition:Trauma from occlusion refers to a condition where injury results to the supporting structures of teeth by the act of bringing jaws into a closed position. STILLMAN (1917) Trauma from occlusion is defined as damage in periodontium caused by stress on teeth produced directly or indirectly by teeth of opposing jaw. WHO (1978) Occlusal trauma was defined as an injury to the attachment apparatus as a result of excessive occlusal force. AMERICAN ACADEMY OF PERIODENTOLOGY(1986)
TRAUMA FROM OCCLUSION:OCCLUSION:Trauma from occlusion is defined as when occlusal forces exceed the adaptive capacity of tissue, tissue injury results. This injury is termed trauma from occlusion. --CARRANZA --CARRANZA Other terms often used for trauma from occlusion are: 1. 2. 3. 4. 5. Traumatizing occlusion. Occlusal trauma. Traumatogenic. Traumatogenic. Periodontal traumatism. Overload.
Traumatic OcclusionAn occlusion that produces such injury is called as a traumatic occlusion. occlusion. Other terms used for traumatic occlusion are:are:1. Occlusal disharmany. 2. Functional imbalance. 3. Occlusal Dystrophy.
CLASSIFICATION:CLASSIFICATION:
Acute trauma from occlusion Chronic trauma from occlusion Primary trauma from occlusion Secondary trauma from occlusion
ACUTE TRAUMA FROM OCCLUSION Less common
CHRONIC TRAUMA FROM OCCLUSION More common Result from gradual change in occlusion Tooth wear Drifting movement Tooth mobility
Definition:Cause:Clinical Features:Management:-
Result from abrupt change in occlusal force Biting on a hard object Restoration Prosthetic appliances Tooth pain Sensitivity to percussion Increased tooth mobility Cementum tears. Dissipate the force by shift in the position of tooth By wearing away or correction of restoration. Periodontal injury may worsen & develop into necrosis accompanied by periodontal abscess. .
Removal of cause
Complications:-
Periodontal injury may worsen & develop into necrosis accompanied by periodontal abscess.
PRIMARY TRAUMA FROM OCCLUSION Definition:When trauma from occlusion is the result of alterations in occlusal forces. Insertion of high filling insertion of prosthetic replacement Drifting movement or extrusion of teeth into spaces created by unreplaced missing teeth. Orthodontic movement of teeth into functionally unacceptable position.
SECONDARY TRAUMA FROM OCCLUSION When trauma from occlusion results from reduced ability of tissue to resist occlusal forces. Bone loss resulting from marginal inflammation.
Etiology:-
Situation with excessive occlusal force can be superimposed:-
Normal periodontium with normal height of bone
Normal periodontium with reduced height of bone
Marginal periodontitis with reduced height of bone
Healing :-
Reversible
Irreversible
STAGES OF TISSUE RESPONSE WHEN OCCLUSAL FORCE IS INCREASED
1) 2) 3)
Tissue response occur in 3 stages:stages:Injury Repair Adaptive remodeling of the periodontium
STAGE I:- INJURY (increase in area of I:resorption & decrease in bone formation)
Produced by excessive occlusal forces Ligament is widened at the expense of bone resulting in 1) Angular bone destruction without periodontal pocket 2) Tooth become loose 3) Most susceptible site-Fulcrum siteDue to the occlusal forces, tooth rotates around a fulcrum.
Different lesions produced due to different degree of pressure:1) slightly excessive pressurea) b) resorption of alveolar bone widening of PDL space B.V. are numerous & reduced Compression of fibres Increases resorption of alveolar bone Increases resorption of tooth surface
2) 3)
Increased pressure.a) a) b) c)
Greater pressure
4)
Severe pressurea) Necrosis of PDL and bone
STAGE II:- REPAIR ( increase resorption & II:increase bone formation)
Constantly occurring in healthy periodontium by replacing of damaged tissue to new tissues
Buttressing bone formationDefinition:Definition:when the bone is resorbed by excessive occlusal force, the body attempt to reinforce the thinned bony trabeculae with new bone.
BUTTRESSING BONE FORMATIONCentral Endosteal cells deposit in new bone. Restore bony trabeculae Reduces size of marrow spaces Peripheral Occur on facial & lingual surface of alveolar plate. Lipping- shelf like thickening of alveolar margin. Pronounced bulge.
STAGE III:III:ADAPTIVE REMODELLING OF PERIODONTIUM (resorption & formation returns to normal)
If repair process cannot keep pace with the destruction cause by occlusion, the periodontium is remodeled in an effort to create structural relationship in which forces are no longer injurious to the tissues. Results in : a) Thickened PDL which is funnel shaped at crest b) Angular defects in bone with no pocket formation c) Involved teeth become loose d) Increased vascularization
EFFECTS OF INSUFFICIENT OCCLUSAL FORCEEtiology: a) b) c) open bite relationship absence of functional antagonist unilateral chewing habits
Clinical features: 1) 3) 4) 5) Thinning of PDL Atrophy of fibres Osteoporosis of alveolar bone Reduction in bone height
INFLUENCE OF TRAUMA FROM OCCLUSION ON PROGRESSION OF MARGINAL PERIODONTITIS:PERIODONTITIS:Local irritant:- initiate gingivitis & periodontal pocket irritant:(affect marginal gingiva) Trauma from occlusion:- affect only supporting tissue. occlusion:
Marginal gingiva is unaffected by trauma from occlusion because its blood supply is sufficient to maintain it. When inflammation extends from the gingiva into the supporting periodontal tissues{ when gingivitis become periodontitis} plaque induced inflammation enter the zone influenced by occlusion. It is important to eliminate the marginal inflammatory component in case of trauma from occlusion because presence or absence of inflammation affects bone regeneration after removal of traumatizing contact.
DIAGNOSIS:DIAGNOSIS:1)
Increase tooth mobility. Presence of excessive occlusal wear. Tilting and migration of individual teeth or complete segment. Hypertrophy diagnosed on palpation of muscles of mastication. Palpation of TMJ and observation of any deviation of the mandible in various path of closure. Fremitus Test : Place wet index finger on the labial surface of maxillary anterior teeth. Ask the patient to close his mouth in centric relation position. Vibration felt on the finger due to prematurities suggest fremitus test positive.
2)
3)
4)
5)
6)
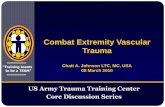
RADIOGRAPHIC SIGNS OF TRAUMA FROM OCCLUSION:OCCLUSION:A) B) Increase width of periodontal space. Thickening of lamina dura ::1) In bifurcation area 2) In apical region 3) Lateral aspect of root Vertical rather than horizontal destruction of interdental septum. Radiolucence & condensation of alveolar bone. Root resorption.
C) D) E)
Arrow shows Widening of periodontal ligament space
TREATMENTDefinition:Definition:Coronoplasty is the mechanical elimination of occlusal supracontacts that may be present during functional movement. It is achieved by reshaping the crown surfaces and eliminating undesirable occlusal supracontact and creation of stable mandibular position. Coronoplasty is generally performed after the gingival inflammation and periodontal pockets have been eliminated. When infra bony defects associated with trauma from occlusion are being treated coronoplasty has to be performed prior to or at the time of pocket elimination. CORONOPLASTY:CORONOPLASTY:-
SCHEDULE OF CORONOPLASTY:CORONOPLASTY:-
Step 1:- Remove retrusive prematurities and eliminate the 1:deflective shift from RCP to ICP.( the retrusive pathway prematurities are eliminated) [RCP[RCP-Retruded contact position; ICP-Intercuspal position] ICPStep 2:- Adjust ICP to achieve stable, simultaneous, multipointed, 2:widely distributed contacts. Step 3:- Test for excessive contact (fremitus) on the incisor teeth. 3:Step 4:- Remove posterior protrusive supracontacts and establish 4:contacts that are bilaterally distributed on the anterior teeth.
Step 5:- Remove or lessen mediotrusive 5:(balancing) interferences. Step 6:- Reduce excessive, cusp steepness on 6:the laterotrusive (working) contacts. Step 7:- Eliminate gross occlusal disharmonies. 7:Step 8:- Recheck tooth contact relationships. 8:Step 9:- Polish all rough tooth surfaces. 9:-
CONCLUSIONTrauma
from occlusion does not initiate gingivitis or periodontal pockets, but it may affect the progress and severity of periodontal pockets started by local irritation.
REFERENCES:REFERENCES:Clinical periodontology Fermin Carranza Michael Newman Takei B.R.R Verma R.P. Nayak Jan Lindhe
current concepts in periodontics Clinical periodontology and implant dentistry -