30024569.pdf
11
REVIEW ARTICLE Stevens-Johnson syndrome: Pathogenesis, diagnosis, and management RIBHI HAZIN 1 , OMAR A. IBRAHIMI 2 , MOUSTAFA I. HAZIN 3 & ARASH KIMYAI-ASADI 4 1 Harvard University, Faculty of Arts and Sciences, Cambridge, MA, USA, 2 Harvard Medical School, Department of Dermatology, Massachusetts General Hospital, Boston, MA, USA, 3 Department of Internal Medicine, St. Joseph’s Hospital & Medical Center, Phoenix, AZ, USA, and 4 DermSurgery Associates, Houston, Texas, USA Abstract Cutaneous drug reactions are the most common type of adverse drug reaction. These reactions, ranging from simple pruritic eruptions to potentially life-threatening events, are a significant cause of iatrogenic morbidity and mortality. Stevens- Johnson syndrome (SJS) is a serious and potentially life-threatening cutaneous drug reaction. Although progress has been made in the management of SJS through early detection, prompt hospitalization, and immediate cessation of offending agents, the prevalence of permanent disabilities associated with SJS remains unchanged. Nevertheless, despite being a problem that is global in scope, government and health care agencies worldwide have yet to find a consensus on either diagnostic criteria or therapy for this disorder. Here, we provide the internist and emergency room physician with a brief review the SJS literature and summarize the latest recommended interventions with the hope of improving early recognition of this disease and prevention of permanent sequelae and mortality that frequently complicate SJS. Key words: Stevens-Johnson syndrome, toxic epidermal necrolysis, erythema multiforme, intravenous immunoglobulins, adverse drug reaction, drug hypersensitivity, dermatological emergencies, mucocutaneous lesions, HLA B1501/HLA B1502, keratinocyte apoptosis Introduction Stevens-Johnson Syndrome (SJS) is a life-threaten- ing inflammatory mucocutaneous drug reaction (1– 3). SJS, also known as erythema multiforme major, lies on a continuum between erythema multiforme minor, characterized by targetoid cutaneous lesions encompassing less than 10% of the body surface area, and toxic epidermal necrolysis, characterized by widespread mucocutaneous involvement affect- ing 30%–100% of the skin surface (Table I) (4). The initial diagnosis of SJS is based on clinical presenta- tion, but skin biopsies and direct immunofluores- cence studies of the skin are essential to rule out other conditions such as autoimmune bullous dis- ease (5,6). Clinical manifestations SJS characteristically begins with vague upper respiratory tract symptoms lasting up to 2 weeks. During this period, patients may complain of fever, sore throat, chills, headaches, and malaise (7). Persistent fever lasting longer than 4 weeks should raise suspicion of a concomitant infection, but studies have demonstrated that continued fever may occur in up to 85% of cases even in the absence of an associated infection (8). This is followed by the rapid onset of mucocutaneous lesions. Painful erosions of the mucous membranes are common and may affect any combination of the lip, oral cavity, conjunctiva, nasal cavity, urethra, vagina, gastrointestinal tract, and respiratory tract during the course of the illness (9–11). Involvement of mucous membranes is evident in approximately 90% of affected patients, and the absence of mucous membrane involvement should cast doubt on the diagnosis of SJS. Mucous membrane involvement can result in both short-term dysfunction and morbidity, as well as long-term complications due to fibrosis and strictures. The characteristic skin lesions seen in SJS are diffuse erythematous macules Correspondence: Arash Kimyai-Asadi MD, DermSurgery Associates, 7515 Main, Suite 210, Houston, Texas 77030, USA. Fax: +1-713 791-9927. E-mail: [email protected] Annals of Medicine. 2008; 40: 129–138 ISSN 0785-3890 print/ISSN 1365-2060 online # 2008 Informa UK Ltd. (Informa Healthcare, Taylor & Francis AS) DOI: 10.1080/07853890701753664
-
Upload
syalalaaalalaaa -
Category
Documents
-
view
4 -
download
1
description
nxjfefherhf
Transcript of 30024569.pdf

REVIEW ARTICLE
Stevens-Johnson syndrome: Pathogenesis, diagnosis, and management
RIBHI HAZIN1, OMAR A. IBRAHIMI2, MOUSTAFA I. HAZIN3 & ARASH KIMYAI-ASADI4
1Harvard University, Faculty of Arts and Sciences, Cambridge, MA, USA, 2Harvard Medical School, Department of
Dermatology, Massachusetts General Hospital, Boston, MA, USA, 3Department of Internal Medicine, St. Joseph’s Hospital
& Medical Center, Phoenix, AZ, USA, and 4DermSurgery Associates, Houston, Texas, USA
AbstractCutaneous drug reactions are the most common type of adverse drug reaction. These reactions, ranging from simple pruriticeruptions to potentially life-threatening events, are a significant cause of iatrogenic morbidity and mortality. Stevens-Johnson syndrome (SJS) is a serious and potentially life-threatening cutaneous drug reaction. Although progress has beenmade in the management of SJS through early detection, prompt hospitalization, and immediate cessation of offendingagents, the prevalence of permanent disabilities associated with SJS remains unchanged. Nevertheless, despite being aproblem that is global in scope, government and health care agencies worldwide have yet to find a consensus on eitherdiagnostic criteria or therapy for this disorder. Here, we provide the internist and emergency room physician with a briefreview the SJS literature and summarize the latest recommended interventions with the hope of improving early recognitionof this disease and prevention of permanent sequelae and mortality that frequently complicate SJS.
Key words: Stevens-Johnson syndrome, toxic epidermal necrolysis, erythema multiforme, intravenous immunoglobulins,adverse drug reaction, drug hypersensitivity, dermatological emergencies, mucocutaneous lesions, HLA B1501/HLA B1502,keratinocyte apoptosis
Introduction
Stevens-Johnson Syndrome (SJS) is a life-threaten-
ing inflammatory mucocutaneous drug reaction (1–
3). SJS, also known as erythema multiforme major,
lies on a continuum between erythema multiforme
minor, characterized by targetoid cutaneous lesions
encompassing less than 10% of the body surface
area, and toxic epidermal necrolysis, characterized
by widespread mucocutaneous involvement affect-
ing 30%–100% of the skin surface (Table I) (4). The
initial diagnosis of SJS is based on clinical presenta-
tion, but skin biopsies and direct immunofluores-
cence studies of the skin are essential to rule out
other conditions such as autoimmune bullous dis-
ease (5,6).
Clinical manifestations
SJS characteristically begins with vague upper
respiratory tract symptoms lasting up to 2 weeks.
During this period, patients may complain of fever,
sore throat, chills, headaches, and malaise (7).
Persistent fever lasting longer than 4 weeks should
raise suspicion of a concomitant infection, but
studies have demonstrated that continued fever
may occur in up to 85% of cases even in the absence
of an associated infection (8). This is followed by the
rapid onset of mucocutaneous lesions. Painful
erosions of the mucous membranes are common
and may affect any combination of the lip, oral
cavity, conjunctiva, nasal cavity, urethra, vagina,
gastrointestinal tract, and respiratory tract during
the course of the illness (9–11). Involvement of
mucous membranes is evident in approximately 90%
of affected patients, and the absence of mucous
membrane involvement should cast doubt on the
diagnosis of SJS. Mucous membrane involvement
can result in both short-term dysfunction and
morbidity, as well as long-term complications due
to fibrosis and strictures. The characteristic skin
lesions seen in SJS are diffuse erythematous macules
Correspondence: Arash Kimyai-Asadi MD, DermSurgery Associates, 7515 Main, Suite 210, Houston, Texas 77030, USA. Fax: +1-713 791-9927. E-mail:
Annals of Medicine. 2008; 40: 129–138
ISSN 0785-3890 print/ISSN 1365-2060 online # 2008 Informa UK Ltd. (Informa Healthcare, Taylor & Francis AS)
DOI: 10.1080/07853890701753664

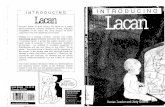
with purpuric, necrotic centers and overlying blister-
ing (Figure 1). These cutaneous lesions often
become confluent in some areas, and often demon-
strate a positive Nikolsky sign, which is further
detachment of the epidermis with slight lateral
pressure. Targetoid lesions are typically present
and are caused by epidermal necrosis in the center
of lesions (4,12). As involvement progresses,
affected portions of the skin slough, resulting in
widespread superficial ulcers and loss of the epider-
mal barrier (13).
The characteristic mucocutaneous lesions
(Figure 1) tend to develop suddenly during the
prodrome, and new lesions may continue to erupt for
up to 4 weeks. Thereafter, the lesions reepithelialize.
The mucocutaneous lesions seen in the prodromal
period are often the predominant feature and may exist
in the absence of skin lesions. Arriving at an accurate
diagnosis can be challenging in cases that lack notice-
able skin lesions (14). Thus, cultures of oral mucosa
are indicated to help differentiate SJS from other
causes of sore lesions in the oral mucosa including
stomatitis, or virus-induced sloughing (15,16).
For most patients, the most clinically significant
elements of SJS are the sequelae of mucosal
ulceration followed by scarring and stricture, result-
ing in significant deterioration of function of the
affected organ systems. The organ most commonly
affected in this manner is the eye, where corneal
involvement affects the majority of patients and may
result in corneal ulceration, perforation, and perma-
nent sclerotic changes (17–19). Indeed, the majority
of patients with SJS have long-term ocular compli-
cations. Less common and generally less debilitating
ocular complications of SJS include anterior uveitis,
iritis, keratitis, and conjunctivitis (17). Early con-
sultation with and continued care by an ophthalmol-
ogist is critical in all patients with significant ocular
involvement or injury (17–19). Urethral erosions are
another common complication of SJS and may result
in genitourinary strictures (15,20–22). In the acute
setting, placement of a Foley catheter to maintain a
patent urinary tract should be considered.
Figure 1. SJS in a patient on carbamazepine: Skin lesions demonstrating characteristic diffuse erythematous macules seen in SJS. The
macules are typically targetoid with necrotic centers, and overlying flaccid blisters.
Key messages
N Early recognition and immediate withdrawal
of offending agents are critical to minimizing
debilitating or potentially life-threatening
consequences of Stevens-Johnson syndrome
(SJS).
N Pharmaceutical treatment of SJS remains
controversial, although intravenous immuno-
globulins (IVIg) are thought to hold promise
for the management of SJS.
N A multidisciplinary approach, including
prompt transfer to a burns unit in severe
cases, is key to reducing the morbidity and
mortality associated with SJS.
Table I. Classification of Stevens-Johnson syndrome and toxic
epidermal necrolysis (48,49).
Classification
Body surface area
involved
Stevens-Johnson syndrome v10%
Overlap Stevens-Johnson syndrome/Toxic
epidermal necrolysis
10%–29%
Toxic epidermal necrolysis w30%
130 R. Hazin et al.

Consultation with a urologist for evaluation and
management of urethral ulceration and strictures is
therefore warranted in patients with SJS (19–23).
Gastrointestinal involvement has also been
described, primarily affecting the esophagus, and
often results in the development of esophageal
webbing or stricture (24–26). In rare cases SJS
may cause ulceration of the mucosa of other
gastrointestinal organs such as the colon (27).
Respiratory involvement in SJS has been reported
in rare cases and is associated with poor prognosis
(28,29). Pulmonary restriction may develop second-
ary to SJS-induced scarring of the pulmonary tract
(30,31).
Incidence
SJS occurs at a rate of approximately 1–7 cases per
million people per year (32–34). The risk of Stevens-
Johnson syndrome remains low with any of its
associated causes (32). SJS is fatal in approximately
5%–15% of cases (35). Both the incidence of the
condition and the associated mortality rate appear to
be elevated in immunocompromised patients with
these risks correlating with worsening immune func-
tion (36,37). Chronic viral infections, such as Epstein
Barr virus and Human Immunodeficiency Virus
(HIV), may also increase the risk of SJS indepen-
dently of the degree of immunosuppression (38–40).
Autoimmune disorders, such as systemic lupus
erythematosus, have also been reported to predispose
to the development of SJS (1,41,42).
A certain genetic predisposition may also confer
increased risk of developing SJS on patients. In one
study, the human leukocyte antigen (HLA) B1502
allele was found in 100% of SJS patients, placing
individuals with that particular HLA allele at a 900
times greater risk of developing SJS than the general
population (1). Given this genetic predisposition,
certain ethnic groups in Asia have been identified as
having an increased risk for SJS in comparison to the
general population (43). This genetic susceptibility
seems to have a strong association with specific
drugs such as carbamazepine (44). Although HLA-
B*1502 confers greater risk of SJS on patients, this
susceptibility is phenotype-specific. For instance,
Caucasian patients with the HLA-B*1502 allele do
not demonstrate the same susceptibility to SJS as
Asian patients with the same genotype (44,45).
Caucasian patients with the HLA-B*1502 genotype
tolerate carbamazepine relatively well while 100%
of the Han Chinese patients with the genotype
developed SJS following carbamazepine administra-
tion (44,45). The presence of the HLA-B*1501
allele also confers an increased risk of developing
SJS but in the presence of allopurinol, further
strengthening the genetic association of the disorder
(46). The increased frequency of HLA-B*1501 and
HLA-B*1502 alleles amongst certain Asian popula-
tions has prompted health care officials in endemic
regions to begin developing inexpensive tests to
identify at-risk individuals prior to prescribing them
allopurinol or carbamazepine (44). Furthermore, the
presence of the HLA-DQB1*0601 allele places
individuals at greater risk for the development of
SJS with ocular complications and strengthens the
notion of an underlying immunogenetic susceptibil-
ity to the development of SJS (46,47). These
findings may aid clinicians in assigning appropriate
therapy and yield improved benefit-to-harm ratios in
patients with SJS.
Diagnosis
Considering an appropriate differential diagnosis in
patients with mucocutaneous erosions can help
eliminate misdiagnoses associated with these condi-
tions (5,48). Among the most common disorders
mistaken for SJS are staphylococcal scalded skin
syndrome, toxic shock syndrome, exfoliative derma-
titis, erythema multiforme, autoimmune bullous
diseases, and chemical burns. Toxic shock syndrome
and scalded skin syndrome, which are bacterial in
nature, result in similar-appearing epidermolysis but
are readily distinguishable from SJS following biopsy
and immunofluorescence studies. Similarly, auto-
immune bullous disease can be distinguished from
SJS by the presence of IgA deposition in the former
conditions (48). The absence of IgA deposition is
characteristic of skin specimens of SJS patients
(48,49). Graft-versus-host disease (GVHD) is
another established cause of SJS independently of
drug administration (50,51). Like SJS, graft-versus-
host disease is mediated by cytotoxic T cells that
result in epidermal necrosis and keratinolysis (52–
54). Furthermore, the clinical and histological
appearance of GVHD can mimic SJS making
distinguishing the two disorders challenging (54).
For instance, the blister fluid of both conditions
demonstrate the presence of CD8+ T cells, further
complicating the ability of clinicians to distinguish
the two (55). Histologically, both GVHD and SJS
result in apoptosis of epidermal Langerhans cells
(LCs) and often show decreased numbers of such
cells in the dermis (56). Because of the difficulty in
distinguishing the two disorders clinically and
histologically, conducting a thorough history and
physical examination as well as early dermatologic
consultation remain the cornerstone of diagnosis in
instances where both SJS and GVHD are part of the
A review of Stevens-Johnson syndrome 131

differential diagnosis (6,54). Incidentally, Lyme
disease also presents with targetoid lesions.
However, unlike SJS, which is associated with
numerous targetoid lesions, Lyme disease typically
presents with a single or small number of targetoid
lesions that surround a central dusky area represent-
ing a tick bite site (57,58). Furthermore, mucosal
involvement is not present in Lyme disease, and
patients with SJS are generally ill and have a very
rapid onset of lesions as compared to patients with
erythema chronicum migrans.
The diagnosis of SJS is generally made on clinical
grounds based on the presence of classic mucocu-
taneous lesions. In most cases confirmation of
the diagnosis should be sought by skin biopsies,
which typically reveal vacuolization of basal layer
keratinocytes associated with lymphocytes along the
dermal-epidermal junction and necrotic spinous
layer keratinocytes (49,59–61). The typical histo-
pathological appearance of SJS is characterized by
apoptosis and necrosis of keratinocytes along with
dermoepidermal detachment and lymphocytic infil-
tration of perivascular regions (4,6). Intraepidermal
vesicles and papillary dermal edema may be noted
in more papular lesions. In severe cases, subepider-
mal blistering associated with full-thickness epider-
mal necrosis may be present, but this is generally
considered the hallmark of toxic epidermal necro-
lysis. To distinguish this condition from autoim-
mune blistering disorders, biopsies should be
submitted both for routine histopathology as well
as for direct immunofluorescence studies.
Etiology
Although a variety of etiologies, such as infections
and underlying malignancies, have been implicated
as potential causes of SJS, drugs remain the
predominant inciting agent (Table II). The most
commonly implicated drugs are sulfa derivatives,
nonsteroidal anti-inflammatory agents, penicillin-
related and cephalosporin antibiotics, antiepileptics,
allopurinol, and terbinafine. There also appears to
be an increased risk of developing SJS with higher
dosages of offending medications (62,63).
Although they have been implicated in rare cases,
overall, vaccine administration and chemical expo-
sure are rarely associated with SJS (64–66).
Cyclooxygenase-2 inhibitors have also been impli-
cated as potential underlying sources of the disorder
(67). Recreational drugs such as cocaine (68) as well
as over-the-counter and alternative medicines have
also recently been implicated as causes of SJS (69).
According to recent studies, as many as 64% of
individuals diagnosed with SJS have been exposed to
drugs suggesting that in up to one-third of cases no
specific etiology has been identified (70). Although
medications are the most common causative agents
in adults, similar trends do not apply in the pediatric
population (5). In fact, SJS in pediatric patients is
more commonly triggered by infectious organisms
than adverse drug reaction (5). An awareness of this
distinction is critical to arriving at an accurate
diagnosis and treatment of the condition.
Underlying infections are the second most com-
mon cause of SJS. The most commonly associated
infectious agents are listed in Table II. The most
common implicated organism is Mycoplasma pneu-
moniae which is oftentimes seen in children and may
be the reason for widespread cases of SJS during
Mycoplasma epidemics (71,72). Although other
infectious etiologies have been identified as causative
agents for the condition, most remain uncommon
with the exception of herpes simplex virus which has
been implicated in acute as well as recurrent bouts of
SJS in adults and children (71,73,74). Moreover, a
number of underlying malignancies, such as squa-
mous cell carcinoma of the lung, Hodgkin’s lym-
phoma, and certain forms of leukemia have been
associated with SJS (75–77).
Pathophysiology
The exact pathophysiologic mechanism of SJS
remains unknown. Various theories have implicated
Table II. Etiologies of Stevens-Johnson syndrome.
Etiologic agent Most frequently described
Viral AIDS, herpes simplex virus, Epstein-Barr, influenza, coxsackie, lymphogranuloma venereum, and variola
Bacterial Mycoplasma pneumoniae, typhoid, tularemia, diphtheria, and group A streptococci
Fungal Dermatophytosis, histoplasmosis, and coccidiomycosis
Protozoal Trichomoniasis, plasmodium
Drugs Sulfas, nonsteroidal anti-inflammatory drugs (NSAIDs), antiepileptics, barbiturates, allopurinol,
tetracyclines, antiparasiticsa
aSulfa drugs (96,107,120), antiepileptics (97,102,123,124,130), allopurinol (103,130), tetracyclines (104) are more common in the setting
of a compromised immune system (19,20,25,134), antiparasitic and antibacterial drugs (23,104,105), antiviral agents (48,119,120),
antifungal agents (24), NSAIDS (31,46,121,122), infectious etiologies (4,108,109,117,118).
132 R. Hazin et al.

both immunological and nonimmunological mecha-
nisms, with the prevailing evidence suggesting
primary involvement of the immunologic response
(78), in particular those mediated by memory
cytotoxic T cells (79). Although it was originally
classified as a type IV, delayed hypersensitivity
reaction, it now appears that the immunological
mechanisms governing the SJS reaction are initiated
by the Fas antigen, a cell surface molecule that can
mediate apoptosis (80,81). Activation of the Fas
signaling cascade leads to widespread keratinocyte
apoptosis and subsequent epithelial necrosis. Early
treatment of SJS via intravenous immunoglobulins
(IVIg) blocks the activation of the Fas pathway, thus
underscoring the potential effectiveness of IVIg in
treating the disorder (35,82,83). Recent studies have
also linked perforin, a pore-making monomeric
granule released from natural killer T-lymphocytes
in the development of SJS. Perforin is believed to
initiate the keratinolysis seen early in the develop-
ment of SJS (84). Some evidence also exists linking
IgE-mediated mechanisms and mast cell activation
contributing to SJS (85).
Genetic factors may play a role in the development
of SJS. It has been postulated that patients with slow
intrinsic acetylation rates and those taking medica-
tions such as azoles, protease inhibitors, serotonin-
specific reuptake inhibitors, and quinolones are at
increased risk of developing SJS (1,86–88). Slow
acetylation may indeed be a factor in the develop-
ment of a number of adverse cutaneous drug
reactions (89), as the reduced rate of acetylation
causes the accumulation of reactive metabolites that
induce cell-mediated cytotoxic reactions directed
against the epidermis, resulting in keratinocyte
apoptosis (90).
Treatment
SJS is a serious systemic disorder with the potential
for severe morbidity and mortality. In approximately
5%–15% of cases SJS is fatal (35,39). In order to
determine a patient’s risk of death with SJS, clinicians
are encouraged to use the SCORTEN (TEN-specific
severity of illness score) scale which employs impor-
tant prognostic indicators including heart rate, age,
and renal function (91,92) (Table III). Assessing the
SCORTEN score requires giving the patient one
point for each positive variable his condition fulfills.
The total points are tallied, with increased scores
correlated with poorer prognosis.
Effective management of SJS begins with prompt
recognition of the entity, combined with attention to
each of the major organs that may be affected, as
well as potential comorbidities. Since medications
are the most common cause of SJS, a thorough drug
history must be obtained, and all potential offending
agents must be immediately discontinued (32,39).
Indeed, immediate cessation of involved medica-
tions appears to improve the prognosis (93).
Comprehensive SJS treatment requires a skilled,
collaborative, multidisciplinary approach that
addresses the highly complex, systemic response to
the condition. A multispecialty team may also assist
in subsequent postdischarge management including
psychosocial issues that may arise from SJS-induced
disfigurations or scarring. The management of
milder cases of SJS may occur in an inpatient ward
with the same fundamental therapeutic protocol
used for burns: warming of the environment,
minimizing transepidermal water loss, treatment of
electrolyte imbalances, administration of high-cal-
orie nutrition and intravenous fluids to prevent
dehydration, and prevention of sepsis (38,39,94–
96). For patients with extensive cutaneous involve-
ment, prompt referral to a burns unit has been
shown to reduce the risk of infection, mortality, and
the length of hospitalization (94,96–101). This is
particularly true for SJS caused by drugs with short
half-lives, which represent a positive prognostic
factor for SJS (94). Patients must be counseled
regarding strict future avoidance of agents respon-
sible for the outbreak as well as chemically similar
compounds. Given the suspected hereditary associa-
tion with SJS, first-degree relatives should also be
encouraged to avoid similar chemical compounds.
Targeted nursing care including adequate main-
tenance of topical management reduces associated
morbidity and allows a more rapid reepithelialization
of skin lesions and the prevention of scarring,
synechia formation, and infection (39,100). Skin
erosions should be covered with moisture-retentive
ointments and/or topical antibiotics to improve
barrier function and to prevent bacterial infection.
Given the involvement of the lips and oral mucosa in
Table III. SCORTEN scale (91,92). One point is added for each
positive variable. A patient’s mortality can be predicted by the
total number of points according to the following breakdown: 0–1
points53.2% mortality; 2 points512.1% mortality; 3
points535.3% mortality; 4–5 points58.3% mortality; w5
points590% mortality.
Variable Value
Age w40 year
Malignancy Present
Heart rate w120 per minute
Body surface area involved at day 1 w10%
Serum blood urea nitrogen (BUN) w10 mg/dL
Serum bicarbonate v20 mg/dL
Serum glucose w14 mg/dL
A review of Stevens-Johnson syndrome 133

many patients with SJS, adequate emphasis on
alleviating pain associated with lesions in the mouth
is an integral part of treating the disorder.
Application of petroleum jelly and sterile saline
compresses can promote rapid reepithelialization of
the lips. The use of viscous lidocaine on the oral
mucosa in combination with diphenhydramine or
sodium bicarbonate mouthwashes can dramatically
relieve pain associated with friable mucocutaneous
ulcerations and prevent the onset of odynophagia
(102–104).
For patients with ocular involvement, daily
erythromycin eye drops are recommended to prevent
bacterial infections, and corticosteroid eye drops are
administered to reduce inflammation (4). Continued
ophthalmologic care is recommended even after
recovery in order to monitor and minimize irrever-
sible ocular complications including visual loss.
Involvement of other organs is addressed with
appropriate supportive care as well as treatment of
any strictures, adhesions, or scarring that may
complicate the course of the disease. Respiratory
involvement may require prompt intubation and
ventilatory support (28,29).
The use of medications to treat SJS has met with
intense debate over the years. Treatment with
corticosteroids, while effective in most other acute
inflammatory disorders, is controversial (105–110).
Furthermore, numerous other anti-inflammatory,
immunosuppressive, and immunomodulatory agents,
such as cyclosporin, cyclophosphamide, thalido-
mide, and intravenous immunoglobulins (IVIg),
have been administered as possible means to arrest
underlying immunological mechanisms promoting
SJS (39,111,112). However, the efficacy of these
agents in the treatment of SJS has not been
demonstrated by any controlled clinical trial. In
the absence of strong evidence, none of these
regimens can be definitively proposed as a treat-
ment of choice. This notwithstanding, IVIg admi-
nistered early after the onset of mucocutaneous
lesions is thought to hold the most promise for
improvement in survival and a reduction in long-
term morbidity (82,83,113). The dose of IVIg
administered varies, but typically is 1–3 g/kg/day for
3–5 days, with a mean total dose of 2.7 g/kg
divided over 1–5 days (23,70,114,115). Studies
have demonstrated that IVIg arrests Fas-mediated
keratinolysis in vitro, which provides a pathophy-
siologic explanation of why it may improve SJS
through disruption of Fas-induced keratinocyte
apoptosis (83,109). Moreover, intravenous immu-
noglobulins have yielded promising results in
controlled studies involving children (111) as well
as adults (115). For example, a recent retrospective
analysis reported a 100% survival rate and com-
plete skin healing in 12 patients with SJS after
treatment with IVIg (115). However, the absence of
large or controlled trials raises questions regarding
the efficacy of IVIg, particularly given the high cost
of this treatment (116). In the absence of clear-cut
benefits, potential risks of IVIg should be reviewed
with the patient prior to treatment.
Sepsis is a major source of mortality in SJS
patients. However, prophylactic antibiotics are not
recommended in the treatment of acute SJS except
when the etiologic agent is identified as an infectious
agent. For example, although supportive therapy
was once considered treatment of choice for
Mycoplasma-induced SJS, antibiotic therapy is now
typically administered to treat the infection (72).
The presence of an opportunistic infection due to
HIV or immunosuppression represents a poor
prognosis in the evolution of SJS and toxic epidermal
necrolysis (TEN) (36,37,40).
Although prophylactic antibiotics are not recom-
mended, the use of skin cultures on the first day and
every 48 hours thereafter is recommended as a
means of monitoring possible bacterial growth.
Topical antibiotic treatment should begin if there
is an increased number of bacteria cultured from the
skin with selection of a single strain, a sudden drop
in temperature, and/or deterioration in the patient’s
condition.
Prompt and uninterrupted enteral nutrition
reduces the incidence of stress ulcers and bacterial
translocation, and allows earlier discontinuation of
intravenous lines (39). Finally, treating the patient’s
existing health concerns is paramount. For example,
regardless of whether SJS is suspected to be secondary
to a drug reaction, prophylactic use of anticoagulants
maybe indicated due to the risk of thromboembolism-
induced morbidity and mortality (1). Furthermore,
based on the severity of the disease, analgesics along
with supportive emotional and psychological care
should be provided as needed.
Conclusions
SJS is a rare but serious adverse cutaneous reaction
most commonly due to medications and infectious
agents. Prompt recognition is critical for the initia-
tion of appropriate care. The mainstay of treatment
remains addressing the causative agent as well as
supportive care for the mucocutaneous ulcerations.
This requires a multidisciplinary approach to all
organ systems that may be affected by this disease.
In severe cases, prompt transfer to a burns unit is
necessary in order to decrease both morbidity and
mortality. While systemic corticosteroids should be
134 R. Hazin et al.

avoided in the management of SJS, IVIg should be
considered early in the disease, even though its
efficacy has not been definitively established.
Patients at risk of or those previously afflicted by
SJS should receive counseling on the importance of
completely avoiding responsible agents or similar
compounds. Furthermore, physicians and health
care workers are encouraged to improve documenta-
tion of offending agents in patient charts in order to
minimize the risk of repeat outbreaks of the disease.
References
1. Chung WH, Hung SI, Hong HS, Hsih MS, Yang LC,
Ho HC, et al. Medical genetics: a marker for Stevens-
Johnson syndrome. Nature. 2004;428:486.
2. Ruiz-Maldonado R. Acute disseminated epidermal necrosis
types 1, 2, and 3: study of sixty cases. J Am Acad Dermatol.
1985;13:623–35.
3. Hussain W, Craven NM. Toxic epidermal necrolysis and
Stevens-Johnson syndrome. Clin Med. 2005;5:555–8.
4. Kumar G, Fadel HJ, Beckman TJ. 36-year-old man with
productive cough and diffuse rash. Mayo Clin Proc.
2006;81:945–8.
5. Leaute-Labreze C, Lamireau T, Chawki D, Maleville J,
Taieb A. Diagnosis, classification, and management of
erythema multiforme and Stevens-Johnson syndrome. Arch
Dis Child. 2000;83:347–52.
6. Paquet P, Pierard GE. Erythema multiforme and toxic
epidermal necrolysis: a comparative study. Am J Dermato-
pathol. 1997;19:127–32.
7. Kasper M. Stevens-Johnson syndrome. Clin J Oncol Nurs.
2001;5:25–6.
8. Wolf R, Davidovici B, Matz H, Mahlab K, Orion E,
Sthoeger ZM. Drug Rash with eosinophilia and systemic
symptoms versus Stevens-Johnson Syndrome—a case that
indicates a stumbling block in the current classification. Int
Arch Allergy Immunol. 2006;141:308–10.
9. Hansen RC. Blindness, anonychia, and oral mucosal
scarring as sequelae of the Stevens-Johnson syndrome.
Pediatr Dermatol. 1984;1:298–300.
10. Powell N, Munro JM, Rowbotham D. Colonic involvement
in Stevens-Johnson syndrome. Postgrad Med J. 2006;82:
e10.
11. Hart R, Minto C, Creighton S. Vaginal adhesions caused by
Stevens-Johnson syndrome. J Pediatr Adolesc Gynecol.
2002;15:151–2.
12. Ayangco L, Rogers RS 3rd. Oral manifestations of erythema
multiforme. Dermatol Clin. 2003;21:195–205.
13. Manders SM. Serious and life-threatening drug eruptions.
Am Fam Physician. 1995;51:1865–72.
14. Vanfleteren I, Van Gysel D, De Brandt C. Stevens-Johnson
syndrome: a diagnostic challenge in the absence of skin
lesions. Pediatr Dermatol. 2003;20:52–6.
15. Lowndes S, Darby A, Mead G, Lister A. Stevens-Johnson
syndrome after treatment with rituximab. Ann Oncol.
2002;13:1948–50.
16. Singla R, Brodell RT. Erythema multiforme due to herpes
simplex virus. Recurring target lesions are clue to diagnosis.
Postgrad med. 1999;106:151–4.
17. Dart J. PL3 Stevens Johnson syndrome and mucous
membrane pemphigoid: ocular manifestations and their
management. Oral Dis. 2006;12 Suppl 1:1.
18. Di Pascuale MA, Espana EM, Liu DT, Kawakita T, Li W,
Gao YY, et al. Correlation of corneal complications with
eyelid cicatricial pathologies in patients with Stevens-Johnson
syndrome and toxic epidermal necrolysis syndrome.
Ophthalmology. 2005;112:904–12.
19. Wall V, Yen MT, Yang MC, Huang AJ, Pflugfelder SC.
Management of the late ocular sequelae of Stevens-Johnson
syndrome. Ocul Surf. 2003;1:192–201.
20. Graham-Brown RA, Cochrane GW, Swinhoe JR, Sarkany I,
Epsztejn LJ. Vaginal stenosis due to bullous erythema
multiforme (Stevens-Johnson syndrome). Case report. Br J
Obstet Gynaecol. 1981;88:1156–7.
21. Wilson EE, Malinak LR. Vulvovaginal sequelae of Stevens-
Johnson syndrome and their management. Obstet Gynecol.
1988;71:478–80.
22. Murphy MI, Brant WE. Hematocolpos caused by genital
bullous lesions in a patient with Stevens-Johnson syndrome.
J Clin Ultrasound. 1998;26:52–4.
23. Noel JC, Buxant F, Fayt I, Bebusschere G, Parent D. Vulval
adenosis associated with toxic epidermal necrolysis. Br J
Dermatol. 2005;153:457–8.
24. Tan YM, Goh KL. Esophageal stricture as a late complica-
tion of Stevens-Johnson syndrome. Gastrointest Endosc.
1999;50:566–8.
25. Rottermann EM, Julia MV, Rovira J, Pari FJ, Morales L.
Esophageal stenosis following Stevens-Johnson syndrome.
Treatment with balloon dilation. Clin Pediatr (Phila).
1990;29:336–8.
26. Clayton NA, Kennedy PJ. Management of Dysphagia in
Toxic Epidermal Necrolysis (TEN) and Stevens-Johnson
Syndrome (SJS). Dysphagia. 2007;22:187–92.
27. Zweiban B, Cohen H, Chandrasoma P. Gastrointestinal
involvement complicating Stevens-Johnson syndrome.
Gastroenterology. 1986;91:469–74.
28. Kamada N, Kinoshita K, Togawa Y, Kobayashi T,
Matsubara H, Kohno M, et al. Chronic pulmonary
complications associated with toxic epidermal necrolysis:
report of a severe case with anti-Ro/SS-A and a review of the
published work. J Dermatol. 2006;33:616–22.
29. Martin L, Hazouard E, Michalak-Provost S, Maurage C,
Machet L. [Fatal toxic respiratory epitheliolysis. Subacute
tracheo-bronchial desquamation in Stevens-Johnson syn-
drome]. Rev Pneumol Clin. 2001;57:297–301.
30. Shah AP, Xu H, Sime PJ, Trawick DR. Severe airflow
obstruction and eosinophilic lung disease after Stevens-
Johnson syndrome. Eur Respir J. 2006;28:1276–9.
31. Peters ME, Gourley G, Mann FA. Esophageal stricture and
web secondary to Stevens-Johnson syndrome. Pediatr
Radiol. 1983;13:290–1.
32. Roujeau JC, Stern RS. Severe adverse cutaneous reactions to
drugs. N Engl J Med. 1994;331:1272–85.
33. Rzany B, Mockenhaupt M, Baur S, Schroder W, Stocker U,
Mueller J, et al. Epidemiology of erythema exsudativum
multiforme majus, Stevens-Johnson syndrome, and toxic
epidermal necrolysis in Germany (1990–1992): structure
and results of a population-based registry. J Clin Epidemiol.
1996;49:769–73.
34. Chan HL, Stern RS, Arndt KA, Langlois J, Jick SS, Jick H,
et al. The incidence of erythema multiforme, Stevens-
Johnson syndrome, and toxic epidermal necrolysis. A
population-based study with particular reference to reactions
caused by drugs among outpatients. Arch Dermatol.
1990;126:43–7.
35. Parrillo SJ, Parrillo CV, Stevens-Johnson Syndrome.
Emedicine website. Available at: http://www.emedicine.
com/emerg/topic555.htm (accessed December 17, 2006).
A review of Stevens-Johnson syndrome 135

36. Shilad A, Predanic M, Perni SC, Houlihan C, Principe D.
Human immunodeficiency virus, pregnancy, and Stevens-
Johnson syndrome. Obstet Gynecol. 2005;105:1254–6.
37. Coopman SA, Johnson RA, Platt R, Stern RS. Cutaneous
disease and drug reactions in HIV infection. N Engl J Med.
1993;328:1670–4.
38. Gonzalez-Delgado P, Blanes M, Soriano V, Montoro D,
Loeda C, Niveiro E. Erythema multiforme to amoxicillin
with concurrent infection by Epstein-Barr virus. Allergol
Immunopathol (Madr). 2006;34:76–8.
39. Ghislain PD, Roujeau JC. Treatment of severe drug
reactions: Stevens-Johnson syndrome, toxic epidermal
necrolysis and hypersensitivity syndrome. Dermatol Online
J. 2002;8:5.
40. Sanwo M, Nwadiuko R, Beall G. Use of intravenous
immunoglobulin in the treatment of severe cutaneous drug
reactions in patients with AIDS. J Allergy Clin Immunol.
1996;98:1112–5.
41. Samimi SS, Siegfried E. Stevens-Johnson syndrome devel-
oping in a girl with systemic lupus erythematosus on high-
dose corticosteroid therapy. Pediatr Dermatol. 2002;19:
52–5.
42. Matsushita K, Ozaki A, Inoue H, Kaieda T, Akimoto M,
Satomura A, et al. Stevens-Johnson syndrome induced by
mizoribine in a patient with systemic lupus erythematosus.
Mod Rheumatol. 2006;16:113–6.
43. Lonjou C, Thomas L, Borot N, Ledger N, de Toma C,
LeLouet H, et al. A marker for Stevens-Johnson syndrome
…: ethnicity matters. Pharmacogenomics J. 2006;6:265–8.
44. Hung SI, Chung WH, Jee SH, Chen WC, Chang YT,
Lee WR, et al. Genetic susceptibility to carbamazepine-
induced cutaneous adverse drug reactions. Pharmacogenet
Genomics. 2006;16:297–306.
45. Alfirevic A, Jorgensen AL, Williamson PR, Chadwick DW,
Park BK, Pirmohamed M. HLA-B locus in Caucasian
patients with carbamazepine hypersensitivity. Pharmaco-
genomics. 2006;7:813–8.
46. Hung SI, Chung WH, Liou LB, Chu CC, Lin M,
Huang HP, et al. HLA-B*5801 allele as a genetic marker
for severe cutaneous adverse reactions caused by allopurinol.
Proc Natl Acad Sci U S A. 2005;102:4134–9.
47. Power WJ, Saidman SL, Zhang DS, Vamvakas EC, Merayo-
Lloves JM, Kaufman AH, et al. HLA typing in patients with
ocular manifestations of Stevens-Johnson syndrome.
Ophthalmology. 1996;103:1406–9.
48. Bachot N, Roujeau JC. Differential diagnosis of severe
cutaneous drug eruptions. Am J Clin Dermatol.
2003;4:561–72.
49. French LE. Toxic epidermal necrolysis and Stevens Johnson
syndrome: our current understanding. Allergol Int.
2006;55:9–16.
50. DiSesa VJ, Kirkman RL, Tilney NL, Mudge GH, Collins JJ
Jr, Cohn LH. Management of general surgical complications
following cardiac transplantation. Arch Surg. 1989;124:
539–41.
51. Ostlere LS, Harris D, Burroughs AK, Rolles K. Toxic
epidermal necrolysis after hepatic transplantation. Arch
Dermatol. 1992;128:1550–1.
52. Revuz JE, Roujeau JC. Advances in toxic epidermal
necrolysis. Semin Cutan Med Surg. 1996;15:258–66.
53. Mockenhaupt M, Norgauer J. Cutaneous Adverse Drug
Reactions. Stevens-Johnson syndrome and Toxic Epidermal
Necrolysis. Allergy Clin Immunol Int. 2002;14:143–50.
54. Schulz JT, Sheridan RL. Severe desquamating disorder after
liver transplant: toxic epidermal necrolysis or graft versus
host disease? J Burns Wounds. 2006;5:e1.
55. Correia O, Delgado L, Barbosa IL, Domingues JC,
Azevedo R, Vaz CP, et al. CD8+ lymphocytes in the blister
fluid of severe acute cutaneous graft-versus-host disease:
further similarities with toxic epidermal necrolysis.
Dermatology. 2001;203:212–6.
56. Asagoe K, Takahashi K, Yoshino T, Kondo E, Tanaka R,
Arata J, et al. Numerical, morphological and phenotypic
changes in Langerhans cells in the course of murine
graft-versus-host disease. Br J Dermatol. 2001;145:918–27.
57. Bennet L, Halling A, Berglund J. Increased incidence of
Lyme borreliosis in southern Sweden following mild winters
and during warm, humid summers. Eur J Clin Microbiol
Infect Dis. 2006;25:426–32.
58. Hubalek Z. North Atlantic weather oscillation and human
infectious diseases in the Czech Republic, 1951–2003. Eur J
Epidemiol. 2005;20:263–70.
59. Hilas O, Charneski L. Lamotrigine-induced Stevens-Johnson
syndrome. Am J Health Syst Pharm. 2007;64:273–275.
60. Caproni M, Torchia D, Schincaglia E, Volpi W,
Frezzolini A, Schena D, et al. The CD40/CD40 ligand
system is expressed in the cutaneous lesions of erythema
multiforme and Stevens-Johnson syndrome/toxic epidermal
necrolysis spectrum. Br J Dermatol. 2006;154:319–24.
61. Hockett KC. Stevens-Johnson syndrome and toxic epider-
mal necrolysis: oncologic considerations. Clin J Oncol Nurs.
2004;8:27–30, 55.
62. Severino G, Chillotti C, De Lisa R, Del Zompo M, Ardau R.
Adverse reactions during imatinib and lansoprazole treat-
ment in gastrointestinal stromal tumors. Ann Pharmacother.
2005;39:162–4.
63. Famularo G, De Simone C, Minisola G. Stevens-Johnson
syndrome associated with single high dose of lamotrigine in a
patient taking valproate. Dermatol Online J. 2005;11:25.
64. Vincenzi B, Santini D, Grilli C, La Cesa A, Dianzani C,
Tonini G. Complications of therapy in cancer patients: Case
3. Toxic epidermal necrolysis induced by oral phenobarbital
and whole-brain radiotherapy in a breast cancer patient. J
Clin Oncol. 2004;22:4649–51.
65. Ridgway HB, Miech DJ. Erythema multiforme (Stevens-
Johnson syndrome) following deep radiation therapy. Cutis.
1993;51:463–4.
66. Chopra A, Drage LA, Hanson EM, Touchet NL. Stevens-
Johnson syndrome after immunization with smallpox,
anthrax, and tetanus vaccines. Mayo Clin Proc. 2004;79:
1193–6.
67. Layton D, Marshall V, Boshier A, Friedmann P, Shakir SA.
Serious skin reactions and selective COX-2 inhibitors: a case
series from prescription-event monitoring in England. Drug
Saf. 2006;29:687–96.
68. Hofbauer GF, Burg G, Nestle FO. Cocaine-related Stevens-
Johnson syndrome. Dermatology. 2000;201:258–60.
69. Ventura MT, Viola M, Calogiuri G, Gaeta F, Pesole O,
Romano A. Hypersensitivity reactions to complementary
and alternative medicine products. Curr Pharm Des.
2006;12:3393–9.
70. Bastuji-Garin S, Rzany B, Stern RS, Shear NH, Naldi L,
Roujeau JC. Clinical classification of cases of toxic epider-
mal necrolysis, Stevens-Johnson syndrome, and erythema
multiforme. Arch Dermatol. 1993;129:92–6.
71. Levy M, Shear NH. Mycoplasma pneumoniae infections
and Stevens Johnson syndrome: report of eight cases and
review of the literature. Clin Pediatr. 1991;30:42–9.
72. Ravin KA, Rappaport LD, Zuckerbraun NS, Wadowsky RM,
Wald ER, Michaels MM. Mycoplasma pneumoniae and
atypical Stevens-Johnson syndrome: a case series. Pediatrics.
2007;119:e1002–5.
136 R. Hazin et al.

73. Detjen PF, Patterson R, Noskin GA, Phair JP,
Loyd SO. Herpes simplex virus associated with recurrent
Stevens-Johnson syndrome. A management strategy. Arch
Intern Med. 1992;152:1513–6.
74. Ng PP, Sun YJ, Tan HH, Tan SH. Detection of herpes
simplex virus genomic DNA in various subsets of Erythema
multiforme by polymerase chain reaction. Dermatology.
2003;207:349–53.
75. Hanno R, Bean SF. Hodgkin’s disease with specific bullous
lesions. Am J Dermatopathol. 1980;2:363–6.
76. Margolis RJ, Bhan A, Mihm MC Jr, Bernhardt M. Erythema
multiforme in a patient with T cell chronic lymphocytic
leukemia. J Am Acad Dermatol. 1986;14:618–27.
77. Klein PA, Stevens-Johnson Syndrome. Emedicine website.
Available at: http://www.emedicine.com/derm/topic405.htm
(accessed August 30, 2007).
78. Roychowdhury S, Svensson CK. Mechanisms of drug-
induced delayed-type hypersensitivity reactions in the skin.
AAPS J. 2005;7:E834–46.
79. Roujeau JC. Clinical heterogeneity of drug hypersensitivity.
Toxicology. 2005;209:123–9.
80. Itoh N, Yonehara S, Ishii A, Yonehara M, Mizushima S,
Sameshima M, et al. The polypeptide encoded by the cDNA
for human cell surface antigen Fas can mediate apoptosis.
Cell. 1991;66:233–43.
81. Iwai K, Miyawaki T, Takizawa T, Konno A, Ohta K,
Yachie A, et al. Differential expression of bcl-2 and
susceptibility to anti-Fas-mediated cell death in peripheral
blood lymphocytes, monocytes, and neutrophils. Blood.
1994;84:1201–8.
82. Khalili B, Bahna SL. Pathogenesis and recent therapeutic
trends in Stevens-Johnson syndrome and toxic epidermal
necrolysis. Ann Allergy Asthma Immunol. 2006;97:272–80.
83. French LE, Trent JT, Kerdel FA. Use of intravenous
immunoglobulin in toxic epidermal necrolysis and Stevens-
Johnson syndrome: our current understanding. Int
Immunopharmacol. 2006;6:543–9.
84. Inachi S, Mizutani H, Shimizu M. Epidermal apoptotic cell
death in erythema multiforme and Stevens-Johnson syn-
drome. Contribution of perforin-positive cell infiltration.
Arch Dermatol. 1997;133:845–9.
85. Greenberger PA. Drug allergy. J Allergy Clin Immunol.
2006;117:S464–70.
86. Nakajima T, Yamanoshita O, Kamijima M, Kishi R,
Ichihara G. Generalized skin reactions in relation to
trichloroethylene exposure: a review from the viewpoint of
drug-metabolizing enzymes. J Occup Health. 2003;45:8–14.
87. Liechty CA, Solberg P, Mwima G, Were W, Weidle PJ,
Mermin J. Nevirapine-induced Stevens-Johnson syndrome
in a mother and son. AIDS. 2005;19:993–4.
88. Pirmohamed M. Genetic factors in the predisposition to
drug-induced hypersensitivity reactions. AAPS J. 2006;8:
E20–6.
89. Evans DA. Survey of the human acetylator polymorphism in
spontaneous disorders. J Med Genet. 1984;21:243–53.
90. Nassif A, Bensussan A, Dorothee G, Mami-Chouaib F,
Bachot N, Bagot M, et al. Drug specific cytotoxic T-cells in
the skin lesions of a patient with toxic epidermal necrolysis. J
Invest Dermatol. 2002;118:728–33.
91. Guegan S, Bastuji-Garin S, Poszepczynska-Guigne E,
Roujeau JC, Revuz J. Performance of the SCORTEN during
the first five days of hospitalization to predict the pro-
gnosis of epidermal necrolysis. J Invest Dermatol.
2006;126:272–6.
92. Bastuji-Garin S, Fouchard N, Bertocchi M, Roujeau JC,
Revuz J, Wolkenstein P. SCORTEN: a severity-of-illness
score for toxic epidermal necrolysis. J Invest Dermatol.
2000;115:149–53.
93. Garcia-Doval I, LeCleach L, Bocquet H, Otero XL,
Roujeau JC. Toxic epidermal necrolysis and Stevens-
Johnson syndrome: does early withdrawal of causative drugs
decrease the risk of death? Arch Dermatol. 2000;136:323–7.
94. Becker DS. Toxic epidermal necrolysis. Lancet. 1998;351:
1417–20.
95. Prendiville JS, Hebert AA, Greenwald MJ, Esterly MB.
Management of Stevens-Johnson syndrome and toxic
epidermal necrolysis in children. J Pediatr. 1989;115:881–7.
96. Peng YZ, Yuan ZQ, Xiao GX. Effects of early enteral
feeding on the prevention of enterogenic infection in severely
burned patients. Burns. 2001;27:145–9.
97. Kelemen JJ 3rd, Cioffi WG, McManus WF. Burn center
care for patients with toxic epidermal necrolysis. J Am Coll
Surg. 1995;180:273–8.
98. Murphy JT, Purdue GF, Hunt JL. Toxic epidermal
necrolysis. J Burn Care Rehabil. 1997;18:417–20.
99. McGee T, Munster A. Toxic epidermal necrolysis syn-
drome: mortality rate reduced with early referral to regional
burn center. Plast Reconstr Surg. 1998;102:1018–22.
100. Paquet P, Jacob E, Quatresooz P, Jacquemin D, Pierard GE.
Delayed reepithelialization and scarring deregulation follow-
ing drug-induced toxic epidermal necrolysis. Burns. 2007;
33:100–4.
101. Sheridan RL, Weber JM, Schulz JT, Ryan CM, Low HM,
Tompkins RG. Management of severe toxic epidermal
necrolysis in children. J Burn Care Rehabil. 1999;20:
497–500.
102. Stoschus B, Allescher HD. Drug-induced dysphagia.
Dysphagia. 1993;8:154–159.
103. Hallgren J, Tengvall-Linder M, Persson M, Wahlgren CF.
Stevens-Johnson syndrome associated with ciprofloxacin: a
review of adverse cutaneous events reported in Sweden as
associated with this drug. J Am Acad Dermatol.
2003;49:S267–9.
104. Yusin JS, Crawford WW, Klaustermeyer WB. Facial edema,
oral ulcers, and a cutaneous eruption following a dental
procedure utilizing diflunisal and mepivacaine. Ann Allergy
Asthma Immunol. 1999;83:353–5.
105. Hynes AY, Kafkala C, Daoud YJ, Foster CS. Controversy in
the use of high-dose systemic steroids in the acute care of
patients with Stevens-Johnson syndrome. Int Ophthalmol
Clin. 2005;45:25–48.
106. Patterson R, Grammer LC, Greenberger PA, Lawrence ID,
Zeiss CR, Detjen PF, et al. Stevens-Johnson syndrome
(SJS): effectiveness of corticosteroids in management and
recurrent SJS. Allergy Proc. 1992;13:89–95.
107. Tripathi A, Ditto AM, Grammer LC, Greenberger PA,
McGrath KG, Zeiss CR, et al. Corticosteroid therapy in an
additional 13 cases of Stevens-Johnson syndrome: a total
series of 67 cases. Allergy Asthma Proc. 2000;21:101–5.
108. Roujeau JC. Treatment of severe drug eruptions. J
Dermatol. 1999;26:718–22.
109. Halebian PH, Corder VJ, Madden MR, Finklestein JL,
Shires GT. Improved burn center survival of patients with
toxic epidermal necrolysis managed without corticosteroids.
Ann Surg. 1986;204:503–12.
110. Engelhardt SL, Schurr MJ, Helgerson RB. Toxic epidermal
necrolysis: an analysis of referral patterns and steroid usage.
J Burn Care Rehabil. 1997;18:520–4.
111. Metry DW, Jung P, Levy ML. Use of intravenous
immunoglobulin in children with Stevens-Johnson syn-
drome and toxic epidermal necrolysis: seven cases and
review of the literature. Pediatrics. 2003;112:1430–6.
A review of Stevens-Johnson syndrome 137

112. Viard I, Wehrli P, Bullani R, Schneider P, Holler N,
Salomon D, et al. Inhibition of toxic epidermal necrolysis by
blockade of CD95 with human intravenous immunoglobu-
lin. Science. 1998;282:490–3.
113. Letko E, Papaliodis DN, Papaliodis GN, Daoud YJ,
Ahmed AR, Foster CS. Stevens-Johnson syndrome and
toxic epidermal necrolysis: a review of the literature. Ann
Allergy Asthma Immunol. 2005;94:419–36.
114. Yeung CK, Lam LK, Chan HH. The timing of intravenous
immunoglobulin therapy in Stevens-Johnson syndrome and
toxic epidermal necrolysis. Clin ExpDermatol. 2005;30:
600–2.
115. Prins C, Vittorio C, Padilla RS, Hunziker T, Itin P, Forster J,
et al. Effect of high-dose intravenous immunoglobulin
therapy in Stevens-Johnson syndrome: a retrospective,
multicenter study. Dermatology. 2003;207:96–9.
116. Daoud YJ, Amin KG. Comparison of cost of immune
globulin intravenous therapy to conventional immunosup-
pressive therapy in treating patients with autoimmune
mucocutaneous blistering diseases. Int Immunopharmacol.
2006;6:600–6.
117. Tay YK, Huff JC, Weston WL. Mycoplasma pneumoniae
infection is associated with Stevens-Johnson syndrome, not
erythema multiforme. J Am Acad Dermatol. 1996;35:
757–60.
118. Pitche P, Padonou CS, Kombate K, Mouzou T, Tchangai-
Walla K. Stevens-Johnson syndrome and toxic epidermal
necrolysis in Lome (Togo). Evolutional and etiological
profiles of 40 cases. Ann Dermatol Venereol. 2005;132:
531–4.
119. Borras-Blasco J, Navarro-Ruiz A, Devesa P, Montesinos-
Ros A, Gonzalez-Delgado M. Photo-induced Stevens-
Johnson syndrome due to sulfasalazine therapy. Ann
Pharmacother. 2003;37:1241–3.
120. Gimnig JE, MacArthur JR, M’bang’ombe M, Kramer MH,
Chizani N, Stern RS, et al. Severe cutaneous reactions to
sulfadoxine-pyrimethamine and trimethoprim-sulfamethoxazole
in Blantyre District, Malawi. Am J Trop Med Hyg. 2006;
74:738–43.
121. La Grenade L, Lee L, Weaver J, Bonnel R, Karwoski C,
Governale L, et al. Comparison of reporting of Stevens-
Johnson syndrome and toxic epidermal necrolysis in
association with selective COX-2 inhibitors. Drug Saf.
2005;28:917–24.
122. Goldberg D, Panigrahi D, Barazi M, Abelson M, Butrus S.
A case of rofecoxib-associated stevens-johnson syndrome
with corneal and conjunctival changes. Cornea. 2004;23:
736–7.
123. Sarris BM, Wong JG. Multisystem hypersensitivity reaction
to lamotrigine. Neurology. 1999;53:1367.
124. Chia FL, Leong KP. Severe cutaneous adverse reactions to
drugs. Curr Opin Allergy Clin Immunol. 2007;7:304–9.
125. Mockenhaupt M, Messenheimer J, Tennis P, Schlingmann J.
Risk of Stevens-Johnson syndrome and toxic epidermal
necrolysis in new users of antiepileptics. Neurology.
2005;64:1134–8.
126. Chen KT, Twu SJ, Chang HJ, Lin RS. Outbreak of Stevens-
Johnson syndrome/toxic epidermal necrolysis associated
with mebendazole and metronidazole use among Filipino
laborers in Taiwan. Am J Public Health. 2003;93:
489–92.
127. Narayan VS, Mamatha GP, Ashok L, Rajashekar N. Stevens
Johnson syndrome due to I.V Ceftriaxone—a case report.
Indian J Dent Res. 2003;14:220–3.
128. Liberopoulos EN, Liamis GL, Elisaf MS. Possible cefotaxime-
induced Stevens-Johnson syndrome. Ann Pharmacother.
2003;37:812–4.
129. Cac NN, Messingham MJ, Sniezek PJ, Walling HW.
Stevens-Johnson syndrome induced by doxycycline. Cutis.
2007;79:119–22.
130. Chang YS, Huang FC, Tseng SH, Hsu CK, Ho CL,
Sheu HM. Erythema multiforme, Stevens-Johnson syn-
drome, and toxic epidermal necrolysis: acute ocular mani-
festations, causes, and management. Cornea. 2007;26:
123–9.
131. Marazzi MC, Germano P, Liotta G, Guidotti G,
Loureiro S, da Gruz Gomes A, et al. Safety of nevirapine–
containing antiretroviral triple therapy regimens to
prevent vertical transmission in an African cohort of
HIV-1 infected pregnant women. HIV Med. 2006;7:
338–44.
132. Colebunders R, Vanwolleghem T, Meurrens P, Moerman F.
Efavirenz-associated Stevens-Johnson syndrome. Infection.
2004;32:306–7.
133. Terrab Z, El Ouazzani T, Zouhair K, El Kabli H,
Lakhdar H. Terbinafine-induced Stevens-Johnson syn-
drome and aggravation of systemic lupus erythematosus.
Ann Dermatol Venereol. 2006;133:463–6.
134. Davis MD, Rogers RS 3rd. Pittelkow MR. Recurrent
erythema multiforme/Stevens-Johnson syndrome: response
to mycophenolate mofetil. Arch Dermatol. 2002;138:
1547–50.
138 R. Hazin et al.