3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside

of 12
Transcript of 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
1/12
Neuroprotection for ischaemic stroke: Translation fromthe bench to the bedside
Brad A. Sutherland1†, Jens Minnerup2†, Joyce S. Balami3, Francesco Arba1,Alastair M. Buchan1*‡, and Christoph Kleinschnitz4‡
Neuroprotection seeks to restrict injury to the brain paren-
chyma following an ischaemic insult by preventing salvage-
able neurons from dying. The concept of neuroprotection
has shown promise in experimental studies, but has failed to
translate into clinical success. Many reasons exist for this
including the heterogeneity of human stroke and the lack ofmethodological agreement between preclinical and clinical
studies. Even with the proposed Stroke Therapy Academic
Industry Roundtable criteria for preclinical development of
neuroprotective agents for stroke, we have still seen limited
success in the clinic, an example being NXY-059, which ful-
filled nearly all the Stroke Therapy Academic Industry
Roundtable criteria. There are currently a number of ongoing
trials for neuroprotective strategies including hypothermia
and albumin, but the outcome of these approaches remains
to be seen. Combination therapies with thrombolysis also
need to be fully investigated, as restoration of oxygen and
glucose will always be the best therapy to protect against
cell death from stroke. There are also a number of promising
neuroprotectants in preclinical development including hae-
matopoietic growth factors, and inhibitors of the nicotina-
mide adenine dinucleotide phosphate oxidases, a source of
free radical production which is a key step in the pathophysi-
ology of acute ischaemic stroke. For these neuroprotectants
to succeed, essential quality standards need to be adhered
to; however, these must remain realistic as the evidence that
standardization of procedures improves translational success
remains absent for stroke.
Key words: acute stroke therapy, ischaemic cascade, ischaemicstroke, neuroprotection, STAIR, translation
Introduction to neuroprotection
Currently, the only approved measures for the treatment of
acute ischaemic stroke are thrombolysis and antiplatelet
therapy. However, the concept of neuroprotection has received
significant attention over the past 30 years, with many experi-
mental neuroprotectants being trialled preclinically and clini-
cally. Where thrombolysis aims to break down the occluding
clot to restore blood flow to the ischaemic brain, neuroprotec-
tion seeks to limit ischaemic injury by preventing the salvage-able neurons in the penumbra that surrounds the core from
dying. Rapid restoration of oxygen and glucose by thromboly-
sis will always provide the most effective neuroprotection, but
directly targeting the brain parenchyma to confer neuropro-
tection may be a viable method, particularly in conjunction
with thrombolysis. Many well-defined molecular targets
(Fig. 1) now exist within the ischaemic cascade that can, in
theory, be pharmacologically altered to produce neuroprotec-
tion (1). Neuroprotective agents aim to salvage ischaemic
tissue, limit infarct size, prolong the time window for throm-
bolytic therapy or minimize post-ischaemic reperfusion
injury or inflammation. Over 1000 neuroprotective agents
have been tested in basic stroke studies (2) with many showing
promise. Despite this, neuroprotection in the clinic has failed
to eventuate, disappointing clinicians, researchers, and stroke
patients alike. Nearly 200 neuroprotection clinical trials are
ongoing or have been completed, with none achieving success-
ful translation to clinical practice so far (3).
This review attempts to define neuroprotection and outline
the current status of the neuroprotection field both preclini-
cally and clinically, while identifying the problems associated
with translating neuroprotection from the bench to bedside. It
also describes some promising neuroprotectants, the use of
Correspondence: Alastair M Buchan*, Acute Stroke Programme, Level 7
John Radcliffe Hospital, Oxford Biomedical Research Centre, Nuffield
Department of Clinical Medicine, University of Oxford, Headley Way,
Oxford, OX3 9DU, UK.
E-mail: [email protected] 1Acute Stroke Programme, Nuffield Department of Clinical Medicine,
University of Oxford, Oxford, UK2Department of Neurology, University of Münster, Münster, Germany 3Acute Stroke Programme, Department of Medicine and Clinical
Geratology, Oxford University NHS Trust, Oxford, UK4Department of Neurology, University of Würzburg, Würzburg,
Germany
Conflict of interest: The authors declare no conflict of interest with this
manuscript.
†Equal contribution;
‡ joint senior authors.
DOI: 10.1111/j.1747-4949.2012.00770.x
Review
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke OrganizationVol 7, July 2012, 407–418 407
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
2/12
neuroprotection alongside thrombolysis, and finally some
concerns with the current criteria for preclinical neuroprotec-
tion studies.
How to define and measure neuroprotection
As described earlier, neuroprotection is designed to restrict
injury to the brain following an injurious ischaemic insult by
preventing neuronal cell death, especially in the salvageable
penumbral region. This leads to the working definition of
neuroprotection as ‘any strategy, or combination of strate-
gies, that antagonizes, interrupts, or slows the sequence of
injurious biochemical and molecular events that, if left
unchecked, would eventuate in irreversible ischemic injury’
(4). According to this definition, protection from injury
originates at the neuron itself (endogenous or direct neuro-
protection). Consequently, it does not include treatment
approaches that primarily target the cerebral vasculature,
such as thrombolytics, antithrombotics, and antiplatelet
drugs (extrinsic or indirect neuroprotection) (4). Even
though these agents do protect the brain by restoring blood
flow and preventing clot formation, their mechanisms of
action are vascular-based and do not target the brain paren-
chyma itself. Nevertheless, given the wide array of biochemi-
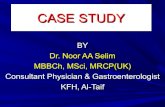
Fig. 1 The cascade of biochemical events leading to apoptosis or necrosis following cerebral ischaemia. Vascular occlusion in a blood vessel initiates a
complex signalling cascade that leads to neuronal cell death. The reduction in blood flow produces ionic pump failure and anoxic depolarization leading
to enhanced glutamate release and a sudden increase in intracellular calcium. This rise in calcium triggers mitochondrial collapse, free radical production,
cytotoxic oedema, and increased NO generation. Reperfusion also produces injury by augmenting BBB breakdown, inflammation, and free radical
production leading to apoptosis. Red borders signify important events in the cascade. The blue border indicates reperfusion. This figure has been adapted
from Durukan & Tatlisumak (1). AA, arachidonic acid; AMPA, a -amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid; BBB, blood-brain barrier; iNOS,
inducible nitric oxide synthase; NMDA, N-methyl-D-aspartate; nNOS, neuronal nitric oxide synthase; NO, nitric oxide; PLA 2, phospholipase A2.
Review B. A. Sutherland et al .
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke Organization408 Vol 7, July 2012, 407–418
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
3/12
cal pathways that have been elucidated to play a role inischaemic cell death (Fig. 1), this working definition still
covers an extensive variety of potential neuroprotective
agents.
In the scope of published neuroprotective preclinical
studies, there is significant variability in the quantity of neu-
roprotection achieved. Some agents produced substantial pro-
tection of the brain following ischaemia (e.g. NXY-059), while
others showed minimal neuroprotection (e.g. edaravone) (2).
Also, based on the Stroke Therapy Academic Industry Round-
table (STAIR) criteria (5,6), many neuroprotective studies
exhibit low methodological quality (2) with a wide heteroge-
neity in the methodology used. This has led to increasingly variable results meaning many neuroprotective agents pro-
ceeded to clinical investigation with only weak preclinical evi-
dence and so were doomed to fail. There are many other
reasons why clinical neuroprotection has not eventuated given
the preclinical success, which are described in Table 1 and in
many other reports (7–9).
It is hard to gauge from the experimental evidence and the
low methodological quality whether there are really any
drugs that can induce ‘true’ neuroprotection. It is possible
that many of the neuroprotective effects observed could be
due to a manifestation of physiological/pathophysiological
changes following ischaemia. These changes could include
modulating temperature (hypothermia), cerebral blood flow
(CBF; hyperperfusion), inflammation (anti-inflammatory
effects), and blood-brain barrier (BBB) damage (reducing
BBB disruption and vascular permeability). One example is
the N-methyl-D-aspartate (NMDA) receptor antagonist
MK-801, which induced hypothermia to produce neuropro-
tection instead of directly targeting the neuron (10). Inter-
estingly, the same compound also raised CBF in the
ischaemic region which may have contributed to its neuro-
protective effects (11). The concept of neuroprotection pro-
duced by enhancing CBF rather than inhibiting the
ischaemic cascade has recently been discussed (12). Sophis-ticated imaging tools might help to delineate genuine neu-
roprotection from within the neuron from secondary or
non-specific effects in the future. This was demonstrated in a
mouse model of multiple sclerosis where a new form of early
but reversible axonal damage caused by oxidative stress and
successive mitochondrial dysfunction was visualized in vivo
by serial two-photon microscopy (13).
Another problem in animal studies is how neuroprotection
is assessed. Infarct volume is most commonly used as the
primary end-point and is quantified by using a histological
stain. The majority of experiments claim that neuroprotection
has been achieved when there is a reduction in infarct volume.However, this is difficult to translate to human studies where
neuroprotection would be reached if stroke patients received
sustainable functional benefit. So what does neuroprotection
really mean if infarct volume is reduced but functional
improvement is lacking? Clearly, functional assessment
including mortality rates in preclinical studies should be a
mandatory outcome parameter for the investigation of any
neuroprotective drug, as outlined by STAIR (5,6). Unfortu-
nately, meaningful functional testing in small laboratory
animals, especially mice, is frequently hampered by stroke
severity and the limited correlation with higher brain func-
tioning in humans, and so representative tests must be care-
fully selected.
The current status of neuroprotection
Even after 30 years of neuroprotection research, no neuro-
protective therapy has been brought into clinical practice.
However, there are some exciting new developments in the
neuroprotection field, and this section will describe the
current status of neuroprotection in both preclinical animal
research and clinical human research.
Table 1 Reasons for translational failure of neuroprotective agents from pre-clinical to clinical studies
Animal models Human studies
Highly control led, homogeneous population Variable, heterogeneous population
Younger animals Older patients
Limited comorbidities Numerous comorbidities
Induced onset of stroke Spontaneous onset of strokeUniform aetiology Variable aetiologies
Ischaemic territory usually from middle cerebral artery Ischaemic territory not restricted to middle cerebral artery
Control over therapeutic time window (usually early treatment) Less control over therapeutic time window (usually delayed treatment)
Controlled occlusion duration Variable occlusion duration
Adequate sample size Inadequate sample size
Wide scope for dose optimization Reduced scope for dose optimization
Multiple routes of administration Limited routes of administration
Rapid availability of the drugs to the target area Slow availability of the drugs to the target area
Infarct volume as outcome Function as outcome
ReviewB. A. Sutherland et al .
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke OrganizationVol 7, July 2012, 407–418 409
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
4/12
Preclinical animal research
The development of new neuroprotective therapies for stroke
involves the evaluation of candidate drugs from in vitro
models to animal experiments and, finally, testing in clinical
trials. Animal studies not only allow the determination of a
drug’s efficacy but also can elucidate its underlying mecha-
nisms in stroke pathophysiology. Up to now, numerous drugstargeting different aspects of the ischaemic cascade (Fig. 1)
were tested in animal models of focal cerebral ischaemia. Drug
mechanisms that were found to be successful in experimental
studies regarding both infarct size reduction and improved
functional outcome include impeding excitotoxicity, local
inflammation, neuronal apoptosis, free radical damage, and
calcium influx into cells. As reviewed by O’Collins et al . (2),
some of these mechanisms of brain injury were targeted by
more than 10 different agents in hundreds of experiments. For
example, the authors identified 277 studies of 21 drugs aiming
to attenuate excitotoxicity in experimental stroke and 114
studies relating to nine drugs with anti-inflammatory activi-ties (2). Overall, 1026 candidate stroke drugs have been iden-
tified in the period covering 1957 to 2003 (2). A more recent
survey of Pubmed-referenced publications showed that the
number of experimental studies of candidate neuroprotective
drugs for stroke therapy has particularly increased over the last
15 years (4). Nearly two-thirds of the published studies report
an improved outcome with a neuroprotective compound
compared to control treatment in animal models of focal cer-
ebral ischaemia (2). However, there appears to be significant
publication bias in preclinical stroke studies which may
account for approximately one-third of the efficacy reported
in meta-analyses, leading to an overstatement of efficacy (14).
In contrast, in clinical trials, drugs targeting only one key
mechanism of cerebral ischaemia have failed to improve
outcome as discussed later in this review. One plausible reason
for this failure might be the multiplicity of mechanisms
involved in causing neuronal damage following stroke (Fig. 1).
Therefore, a novel approach for the development of neuropro-
tective drugs includes the evaluation of compounds with a
multimodal mode of action. This concept also considers the
use of agents with recovery-enhancing properties in addition
to neuroprotective actions (15,16). A recent trend for judging
the potency of neuroprotectants is to pool results from differ-
ent animal studies for meta-analysis. This method, originally
applied for clinical trials in humans, was recently used toobtain further information on the efficacy, the dose–response
relationship, and the therapeutic time window of promising
stroke drugs for potential guidance of clinical trials (17–19).
Clinical human research
A considerable number of neuroprotection clinical trials for
ischaemic stroke are ongoing or have been completed. Viewing
the Internet Stroke Centre Stroke Trials Registry (3), a number
of agents possessing a wide variety of mechanisms of action
have been tried. Unfortunately, none of these agents have
achieved clinical success for neuroprotection. However, there
are some promising ongoing studies that, among others,
include the use of hypothermia, albumin, magnesium, mino-
cycline, and statins as potential approaches to neuroprotection
in the clinical setting. The ongoing clinical trials investigating
neuroprotection for acute ischaemic stroke have been outlinedin Table 2. A list of neuroprotective strategies that have under-
gone completed studies for acute ischaemic stroke and that
have all failed to show neuroprotection in the clinic is shown
in Supporting Information Table S1.
Hypothermia
Hypothermia is one of the most promising neuroprotective
approaches, which has consistently shown benefit in animal
models of cerebral ischaemia, reducing infarct volume by
more than 40% (21). Hypothermia is thought to be neuropro-
tective through several mechanisms including decreasing exci-
tatory amino acid release, reducing free radical formation,enhancing small ubiquitin-related modifier (SUMO)-related
pathways, attenuating protein kinase C activity, and slowing
cellular metabolism (22–24).
The Cooling for Acute Ischaemic Brain Damage (COOL-
AID) studies, COOL-AID I (using surface cooling) (25), and
COOL-AID II (using endovascular cooling) (26) showed that
mild therapeutic hypothermia for acute ischaemic stroke was
feasible, but with no change in clinical outcome. The recent
Intravascular Cooling in the Treatment of Stroke – Longer
recombinant tissue plasminogen activator (rtPA) window
study showed that catheter-based cooling within 6 h of
symptom onset of acute stroke was well tolerated in patients
given rtPA, but there were no differences in 90-day outcomes
(27). Other safety and efficacy clinical studies such as Control-
led Hypothermia in Large Infarction and Cooling in Acute
Stroke are ongoing (3).
Despite the encouraging results from hypothermia studies
in humans, there are a number of limitations in applying
hypothermia to stroke patients. Stroke patients are generally
awake and do not tolerate cooling in contrast to cardiac arrest
and brain injury patients. Attaining target temperature and
prolonging or maintaining that temperature stroke patients
while awake is challenging. There are frequent complications
such as pneumonia, hypotension, cardiac arrhythmias, elec-
trolyte derangements, and infections (27–29). A number of patients also experience shivering during cooling which can
be controlled with anti-shivering agents such as buspirone
and meperidine (28). Another problem is the rebound
increase in intracranial pressure experienced during re-
warming; a phenomenon that is not well studied in laboratory
models (30).
Albumin
Albumin, a protein involved in the transport of small mol-
ecules in the blood, plays a key role in restricting fluid leaking
Review B. A. Sutherland et al .
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke Organization410 Vol 7, July 2012, 407–418
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
5/12
from the vasculature into the tissue (31). In animal studies,
albumin was shown to diminish infarct volume significantly
with a therapeutic time window of four-hours poststroke (32).
Albumin produces its neuroprotective effect through several
mechanisms including ameliorating brain swelling, enhancing
blood flow to sub-occlusive microvascular lesions, maintain-
ing vascular patency, and preventing re-occlusion after suc-
cessful thrombolysis (4).
The pilot study Albumin in Acute Stroke (ALIAS) demon-
strated that high-dose human albumin therapy is safe and may
confer a neuroprotective effect within five-hours after acute
ischaemic stroke (33,34). These encouraging results have led
to a large placebo-controlled randomized multicentre phase lll
trial of albumin therapy in acute ischaemic stroke – ALIAS-
Part 2 – which is ongoing (35).
The preclinical evidence for the validity of albumin as a
neuroprotective agent is limited in that albumin efficacy in
focal cerebral ischaemia was mainly described by only one
group and independent confirmation by others is pending.
Magnesium
Magnesium may have significant neuroprotective properties
in stroke, with preclinical evidence revealing a 25% level of
protection (36). Magnesium produces this protection through
a number of mechanisms including antagonism of calcium
channels, noncompetitive antagonism of NMDA receptors,
inhibition of excitatory neurotransmitter release, and vascular
smooth muscle relaxation (37). However, magnesium can
also produce post-ischaemic hypothermia which could con-
tribute to its neuroprotective effects in studies that were not
temperature-controlled (38). Looking at studies that were
temperature-controlled, magnesium was largely ineffective
(38) suggesting that magnesium may only produce neuropro-
tection in concert with hypothermia.
Much of the failure of previous neuroprotective trials may
be due to the delayed delivery of agents to stroke patients. The
Field Administration of Stroke Therapy–Magnesium (FAST-
MAG) Pilot Trial attempted to overcome this by having para-
medics initiate magnesium sulphate therapy in acute stroke
patients in the field before arrival to the hospital (39). The
field-based magnesium intervention was feasible and safe with
no serious adverse effects, and was associated with a beneficial
functional outcome at three-months. Based on these positive
results, a large phase lll clinical trial is already in progress
(FAST-MAG) (3).
Although magnesium might act pleiotropically on ischae-
mic neurons, powerful effects of this naturally occurring elec-
trolyte on stroke outcome in clinical practice may be
surprising, especially when given as a monotherapy. A combi-
natory approach with other neuroprotective or clot-breakingagents may be more promising.
Minocycline
Minocycline is a tetracycline antibiotic, which has been shown
to produce a 30% reduction in infarct size in models of cer-
ebral ischaemia (36). The proposed mechanisms of action of
minocycline include anti-inflammatory effects, reduction of
microglial activation, matrix metalloproteinase activity, and
nitric oxide (NO) production, and inhibition of apoptosis
(40). Moreover, via its antibacterial properties, minocycline
Table 2 Neuroprotective compounds currently undergoing clinical trials*
Category Name(s) Mechanism
Clinical
phase Manufacturer
Antioxidant Ebselen Free radical scavenger III Daiichi Pharmaceutical Co., LTD
Edaravone (MCI-186) Free radical scavenger III Mitsubishi Pharma Corporation
Anti-apoptotic/ regeneration AX200 (filgrastim, G-CSF analogue) Growth factor II Sygnis Bioscience GmbH & Co KGHuman Chorionic Gonadotropin
(hCG)/Erythropoietin (NTx-265)
Growth factors, oxygen delivery I I Stem Cel l Therapeutics Corp.
Excitotoxicity Magnesium sulphate NMDA ion channel blocker III Many manufacturers (Abbott
Laboratories for FAST-MAG)
Fluid regulators Albumin Haemodiluting agent III Baxter Bioscience
Others Citicoline (CDP choline) Membrane stabilizer III Ferrer Grupo
Deferoxamine mesylate Iron chelator II Novartis Pharma
DP-b99 Metal ion chelator III D-Pharm Ltd
Hemicraniectomy Reduce cerebral oedema and intracranial
pressure
III None
Hypothermia Reduce cerebral oxygen metabolism,
synaptic inhibitor
III None
Insulin Reduce glucose and brain damage III Eli Lilly
Lovastatin HMG CoA reductase inhibitor, antioxidant II Many manufacturers
Minocycline Antibiotic, pleiotropic protective effects III WyethSimvastatin HMG CoA reductase inhibitor, antioxidant III Many manufacturers
*Information gathered from Stroke Trials Registry (3), O’Collins et al . (2), and Cochrane Clinical Trials Database (20).
ReviewB. A. Sutherland et al .
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke OrganizationVol 7, July 2012, 407–418 411
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
6/12
could reduce infections such as pneumonia or urinary tract
infections resulting from stroke-induced immunosuppression
(41).
In an open-label evaluator study, minocycline administra-
tion led to a significantly better outcome in acute stroke
patients compared to placebo (40). Similarly, in Minocycline
to Improve Neurological Outcome in Stroke, minocycline wassafe and well tolerated alone and in combination with rtPA
(42). Encouraging results from these trials have led to the
ongoing Phase III Neuroprotection with Minocycline Therapy
for Acute Stroke Recovery Trial (43).
While the efficacy and neuroprotective potential of mino-
cycline in acute ischaemic stroke still need to be established,
this antibiotic has been used in clinical practice for many
years without serious safety concerns. Nevertheless, wide-
spread and uncritical application of anti-infective agents
could promote the occurrence of multiresistant and invasive
pathogens especially in the setting of intensive care units or
stroke wards.
Statins
Hydroxymethylglutaryl–coenzyme A (HMG-CoA) reductase
inhibitors (statins) are the most widely used cholesterol-
lowering drugs. In addition to their well-established role for
stroke prevention, statins may also be protective in acute
ischaemic stroke (2,44). The main proposed mechanism of
action is due to an increase in NO bioavailability that regulates
cerebral perfusion and improves endothelial function (45).
Other possible mechanisms include antioxidant properties,
atherosclerotic plaque stabilization, and anti-inflammatory
effects (45).
Neuroprotection with Statin Therapy for Acute Recovery
Trial (NeuSTART) was a phase 1B dose-escalation study that
showed that lovastatin administration was safe and feasible up
to three-days after an acute ischaemic stroke (46). Now, a
phase ll trial (NeuSTART II) is in progress to confirm lovas-
tatin safety and efficacy in improving functional outcome after
stroke (3).
Although HMG-CoA reductase inhibitors clearly act
beyond their sole lipid-lowering properties, the concept of
statins as powerful neuroprotectants or anti-inflammatory
drugs was recently called into question in another frequent
neurological disease. Surprisingly, patients suffering from
multiple sclerosis and treated with statins in combination withinterferon-b showed a trend towards increased disease activity
and lesion size compared with patients receiving placebo plus
interferons (47).
DP-b99
DP-b99 is a novel therapeutic that chelates membrane-
activated divalent metal ions such as calcium and zinc (48). As
cell death following cerebral ischaemia is in part mediated by
these toxic metals, DP-b99 administration was shown to
provide significant neuroprotection in animal models of
stroke (48). This promising compound underwent a phase II
trial showing that patients receiving DP-b99 had improve-
ments in a number of secondary end-points following acute
ischaemic stroke (49). Now, the phase III Membrane Activator
Chelator Stroke Intervention trial is underway investigating
the capacity of DP-b99 to improve functional outcome follow-
ing acute ischaemic stroke (3).
Difficulties in translation intoclinical practice
Examples of neuroprotective therapies frompreclinical to clinical
As outlined earlier, a wide variety of neuroprotective drugs
have been tested in preclinical animal studies with about 100
of these being trialled in human studies (2). Even in cases
where the drug showed neuroprotection in animal experi-
ments, all have failed to achieve the primary end-point of neuroprotection in humans. Described later are two case
examples, tirilazad and NXY-059, which are drugs that have
shown a good level of protection preclinically, that have pro-
ceeded into clinical trials with limited success.
Tirilazad
Tirilazad (U74006F) is a 21-aminosteroid that can inhibit
lipid peroxidation by acting as a free radical scavenger (50). In
transient focal ischaemia, Xue et al . (51) showed that tirilazad
reduced cortical infarct size in rats, but this was not observed
in permanent ischaemia. An overall analysis of all tirilazad
preclinical studies showed that tirilazad reduced injury by 29% and had more significant effects following transient
occlusion compared to permanent ischaemia (52). This sug-
gests that tirilazad required revascularization so that it could
reach the ischaemic penumbra to achieve neuroprotection.
The efficacy of tirilazad was greater when given pre-ischaemia,
but some efficacy was observed in delayed treatment out to
six-hours post-ischaemia (52).
The preclinical evidence earlier convincingly showed pro-
tection, while the clinical evidence failed to reproduce these
results. The Randomized Trial of Tirilazad mesylate in patients
with Acute Stroke (RANTTAS) trial (53) was a multicentre,
randomized, double-blinded, vehicle-controlled trial investi-
gating tirilazad in acute stroke patients. Patients were not
thrombolysed, and so were not stratified between transient
and permanent ischaemia, although preclinical evidence sug-
gested that this was important. Tirilazad was administered
within-six hours (median time of 4·3 h) with subsequent
administrations every six-hours for 11 additional doses. The
study was prematurely terminated after inclusion of 556
patients due to lack of any functional benefit at three-months.
Further systematic analysis of all clinical trials investigating
tirilazad showed that tirilazad actually increased disability and
death in acute stroke patients (54). This is at odds with the
Review B. A. Sutherland et al .
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke Organization412 Vol 7, July 2012, 407–418
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
7/12
preclinical data and may be due to not using patients that had
recanalization, and administering the treatments much later
compared to the preclinical setting (median over all studies:
five-hours clinical vs. 10 mins preclinical) (52). In order for
neuroprotection to translate, methodologies between animal
and human studies need to be more consistent and tightly
controlled.
NXY-059
NXY-059 is a nitrone that exhibits free radical scavenging
properties and inhibits many stages of the ischaemic cascade
(55). NXY-059 has shown significant neuroprotective effects
in animal models of both transient and permanent occlusion
of the middle cerebral artery (MCA) (56), with an overall
reduction in infarct volume of 43% (18). The protective effects
of NXY-059 in rodents were confirmed in nonhuman pri-
mates (marmosets), which follow the STAIR criteria (57). The
time course of effects of NXY-059 is similar to rtPA with
efficacy within four-hours of occlusion (58). Therefore, due to
their distinct mechanisms, NXY-059 could potentially be usedin concert with thrombolytic treatment for acute ischaemic
stroke in humans.
Two trials were performed to assess the neuroprotective
activity of NXY-059 on human stroke: SAINT I and SAINT II.
The SAINT I trial (59) was a phase III double-blinded, rand-
omized, placebo-controlled trial that revealed a small but sig-
nificant improvement in disability (modified Rankin scale)
with NXY-059 three-months following stroke, but it did not
improve neurological outcome (National Institute of Health
Stroke Scale). Post hoc analysis showed that patients who
underwent thrombolysis and treatment with NXY-059 had
reduced incidence of haemorrhagic transformation. SAINT II(60) was a statistically more powerful study but disappoint-
ingly failed to confirm the data reported in SAINT I. In SAINT
II, there was no difference in disability at three-months, and
the reduction in haemorrhagic transformation with rtPA by
NXY-059 could not be reproduced. There was a higher fre-
quency of rtPA use in SAINT II (44% vs. 28%) (61) which may
have contributed to the difference in results. Only a small
proportion of NXY-059 may cross the BBB, and the neuropro-
tective action of NXY-059 may be mediated in the endothe-
lium and neurovascular unit (58,62). This would also explain
the reduced risk of haemorrhage in thrombolysed patients
(62). However, there was no preclinical evidence that NXY-059
exerted its effects by altering CBF in experimental models
(63).
There were a number of methodological weaknesses in the
preclinical NXY-059 studies that potentially affected the
human trials. Methodological quality was low (18) and only
9% of studies with NXY-059 measured CBF (64). The lack of
infarction observed in many NXY-059 studies may be due to
not confirming MCA occlusion with CBF measurements,
rather than a neuroprotective effect of NXY-059 (65). Many
studies were not blinded or randomized (18), and further
analysis suggests that there may have been significant publica-
tion bias (56). Interestingly, out of all the current drugs in
phase II/III trials,only NXY-059 fulfilled the STAIR criteria for
adequate translation into clinical trials (64), even with these
methodological weaknesses.
A potential reason for clinical failure of the SAINT trials is
the difference in methodology compared to animal studies.
The SAINT trials enrolled patients up to six-hours post-ischaemia onset, while a maximum of four-hours time
window was chosen in animal studies (66). In animal studies,
only occlusion of the MCA was performed, while the SAINT
trials enrolled patients with different types of stroke, such as
posterior or lacunar strokes. The SAINT trials perhaps should
have selected stroke patients that more closely resembled what
had previously worked in animal experiments, e.g. patients
with MCA occlusion (66).
Both tirilazad and NXY-059 are antioxidants that were sup-
posedly neuroprotective by scavenging free radicals and pre-
venting oxidative stress. Although oxidative stress has been
suggested for many years to cause tissue damage and neuronal
death, there is still no successful therapeutic application. Todate, all clinical attempts to scavenge reactive oxygen or nitro-
gen species (ROS/RNS) by applying antioxidants have not
resulted in clinical benefit and have even caused harm. Given
that ROS/RNS are extremely short-lived molecules that form
at multiple sites of the brain upon ischaemia, this is in fact not
surprising. However, the characterization of the relevant enzy-
matic sources of oxidative stress such as nicotinamide adenine
dinucleotide phosphate (NADPH) oxidases (see later) may
allow therapeutic targeting of oxidative stress by preventing
the formation of ROS initially instead of scavenging ROS after
they have been formed (67).
Clinical neuroprotection – why it has failed
The two case examples of preclinical to clinical neuroprotec-
tion assessment outlined the problems associated with trans-
lation. The reasons for translational failure are numerous
(Table 1), ranging from flaws in clinical trial design, delayed
treatment time window, small sample sizes, different
outcome measures, insufficient dosing, and failure to achieve
adequate plasma levels of study medications (7,68,69). Also,
the heterogeneous nature of human stroke is at odds with
the homogeneous animal models currently used (70).
Animal models of stroke mimic at best less than 25% of all
strokes, with the rat model of MCA occlusion probably
reflecting the Total Anterior Circulation Stroke Syndrome in
humans (71). Therefore, there is a need to create new animal
models that better reflect the heterogeneity of ischaemic
stroke in humans. In addition, preclinical studies are usually
performed on young healthy animals, whereas patients are
mostly elderly with possible comorbidities. Ageing is associ-
ated with significant structural and functional changes in the
brain, which affects outcome and the ability to recover after
an ischaemic event (72).
ReviewB. A. Sutherland et al .
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke OrganizationVol 7, July 2012, 407–418 413
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
8/12
Experimental studies require a more rigorous design with
higher quality standard levels to avoid bias, and a careful
control of physiological variables to distinguish genuine drug
mode of action from other non-specific effects (4,56). In clini-
cal studies, the treatment time window should be restricted to
a period similar to that shown to be effective experimentally.
Unfortunately, most neuroprotective agents target early eventsin the ischaemic cascade, which require rapid administration
following stroke onset, which is challenging in acute ischaemic
stroke patients. Therefore, agents that have long therapeutic
time windows are optimal.
Combining neuroprotection with thrombolysis
A crucial protective strategy following stroke is the early reca-
nalization of the blood vessel to restore flow back into the
ischaemic region of the brain. This is usually achieved by
thrombolysis, and rtPA is currently the only United States
Food and Drug Administration-approved thrombolytic
therapy. Unfortunately, less than 15% of patients actually receive this therapy (73) because of the short time window of
treatment (4·5 h) and the risk of haemorrhagic transforma-
tion. Therefore, treatment strategies that can improve post-
ischaemic CBF, reduce cerebral injury, restrict adverse effects,
and extend the therapeutic time window may prove useful to
improve rtPA therapy. Thrombolysis may improve delivery of
the neuroprotectant to the penumbral region increasing the
chances of a beneficial effect. Many neuroprotective agents
exhibit synergistic effects with rtPA preclinically including
matrix metalloprotease inhibitors (74), free radical scaven-
gers (75,76), NMDA receptor antagonists (77), a -amino-3-
hydroxy-5-methyl-4-isoxazolepropionic acid receptor antago-nists (78), antioxidant agents (79), anti-inflammatory agents
(80), and antiplatelet agents (80–83).
The concept of thrombolysis combined with neuroprotec-
tive therapy has not been extensively explored in human
clinical trials. As outlined earlier, SAINT I showed that NXY-
059 administration in stroke patients who had received rtPA
reduced haemorrhagic transformation compared to NXY-059
alone (59). However, there was no additive benefit observed
with lubeluzole (sodium channel blocker) and rtPA, even
though combination therapy did not increase adverse effects
(84). Other combination studies with rtPA include clom-
ethiazole (g -aminobutyric acid agonist that showed no
benefit) (85) and UK-279276 (neutrophil inhibitory factor
that showed no benefit) (86). Much like neuroprotection
itself, the promise of combination therapy of thrombolysis
and neuroprotection is tempting, but this needs further
investigation in clinical trials before the viability of this strat-
egy can be confirmed.
One major drawback of testing combination therapies is
that any observed effect or side effect often cannot be
unequivocally assigned to one or the other partner. Moreover,
it is difficult to foresee whether the two (or more) compounds
will act synergistically (multiplicative effect), independently
from each other (additive effect) or even in an antagonistic
manner (neutralizing effect). Even though rtPA is a thrombo-
lytic, it has many effects independent of thrombolysis, which
may be due to the L-arginine present in the rtPA formulation
(87). Every stroke patient receiving rtPA also receives
L-arginine, which is a substrate for NO synthesis, and may
affect outcome following ischaemia (87). Therefore, it will bedifficult to elicit individual effects of compounds, even if rtPA
is part of the combination therapy.
Promising neuroprotectants
There are still many potential neuroprotective compounds
that are currently being investigated for the treatment of acute
ischaemic stroke. Discussed later are two groups of neuropro-
tective agents that have shown promising effects.
Haematopoietic growth factors
Haematopoietic growth factors are a group of regulatory molecules that are responsible for the mobilization, prolif-
eration, maturation, and survival of bone marrow-derived
cells (88). Receptors of several haematopoietic growth factors
are expressed on neurons. Moreover, functions of growth
factors paralleling those in the haematopoietic system were
identified in the brain (89,90). Among the haematopoietic
growth factors, the granulocyte-colony-stimulating factor
(G-CSF) and erythropoietin (EPO) were particularly well
investigated for their effects in cerebral ischaemia. Both
G-CSF and EPO reduced glutamate-induced neuronal cell
death in vitro and prevented apoptosis of neurons in vivo by
activating several anti-apoptotic pathways (89,91). G-CSFand EPO also demonstrated anti-inflammatory actions after
ischaemia (92,93). Besides having neuroprotective properties,
G-CSF and EPO facilitate functional recovery poststroke by
enhancing neurogenesis and angiogenesis (89,94,95). Meta-
analyses of EPO and G-CSF in animal experimental stroke
showed that both factors reduced infarcts and improved
functional outcomes (19,96–98). However, when the impact
of common sources of bias, e.g. unblinded outcome assess-
ment, was considered for analysis, the efficacy of EPO was
lowered, suggesting that the benefit of EPO might be over-
estimated (97).
A small clinical trial showed that EPO is safe and might be
beneficial in acute ischaemic stroke (99). However, these
promising results were not confirmed by a larger phase II/III
German multicentre stroke trial which investigated stroke
patients that had received either EPO or placebo within six-
hours of symptom onset (100). The primary end-point,
change in Barthel Index on day 90, and all secondary out-
comes failed to show any benefit of EPO. Moreover, an
increased mortality rate was observed after EPO treatment.
Potential reasons for the differences between preclinical
studies and the clinical trial could be due to an overestimated
efficacy of EPO in animal studies through neglected quality
Review B. A. Sutherland et al .
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke Organization414 Vol 7, July 2012, 407–418
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
9/12
characteristics and unexpected side effects of EPO in patients,
i.e. an intrinsic stroke-inducing capacity of EPO (101). A
recent phase IIa clinical trial demonstrated that G-CSF is well
tolerated even at high doses in stroke patients (102). Explora-
tory analysis revealed a dose-dependent beneficial effect of
G-CSF in patients with large infarcts (102). A phase II trial on
AX200 (filgrastim, a G-CSF analogue) for ischaemic strokepatients (AXIS-2) is currently ongoing, and results are
expected soon (103).
NADPH oxidase inhibitors
The concept that free radicals including ROS are involved in
the pathophysiology of acute ischaemic stroke and account for
secondary infarct growth is over 30 years old (104) but still
valid and based on solid experimental data (105,106). If ROS
are the trigger that causes neurotoxicity in the ischaemic brain,
the question regarding the main sources of ROS arises. Some
of the most attractive candidates are NADPH oxidases, the
only known enzyme family solely dedicated to ROS produc-
tion. Many other enzymes are able to form ROS, e.g. xanthineoxidase, uncoupled NO synthase, and cytochrome P450
enzymes. However, in all these cases, ROS formation requires
an initial oxidation step to occur and none of them forms ROS
natively (107). The structure and function of the NADPH
oxidases were initially characterized in neutrophils, where the
enzyme plays a pivotal role in immunological host defence.
Recently, it has been discovered that the catalytic sub-unit of
the phagocytic NADPH-oxidase is only one member of a
family of four homologous proteins known as NOX1-4 (for
NADPH-oxidase).
By strictly adhering to current quality standards in experi-
mental stroke research (5), we could demonstrate thatNOX4-derived oxidative stress is a crucial player in the
pathophysiology of cerebral ischaemia (67,108). NOX4 was
massively induced in neurons and brain vessels in human
stroke patients and mice subjected to transient MCAO. Mice
deficient in NOX4, but not those deficient for NOX1 or
NOX2, were largely protected from oxidative stress and neu-
ronal apoptosis, after both transient and permanent cerebral
ischaemia. This was independent of gender and age as elderly
mice were equally protected. Interestingly from a transla-
tional perspective, application of the only validated pharma-
cological NADPH oxidase inhibitor, VAS2870, several hours
after ischaemia had the same beneficial effect as deleting
NOX4 (67). The extent of neuroprotection was exceptional
(~70% reduction of stroke volumes), resulting in signifi-
cantly improved long-term neurological function and
reduced mortality.
Targeting the right enzymatic source of ROS rather than
applying non-specific antioxidants after radicals have already
been generated may represent an attractive treatment option
in acute ischaemic brain damage and other disease states
related to oxidative stress (109). Novel and sub-type-specific
NADPH oxidase inhibitors on a small molecule base with
improved pharmacological properties are currently under
development and bear a realistic chance to enter clinical trials
within the next few years.
Conclusions – the future of neuroprotectionin ischaemic stroke
The translational disappointments have created a great deal of
pessimism regarding the future of neuroprotection trials in
humans and have cast doubt on the neuroprotection hypoth-
esis. Some have even suggested that the initially favourable
results of several of the trials, e.g. SAINT I, were likely chance
findings and that the idea of neuroprotection as a form of
treatment for acute stroke should be abandoned. However,
looking into the past, despite the initial scepticism about
stroke care, the landmark National Institute of Neurological
Disorders and Stroke alteplase trial (110) not only revolution-
ized stroke treatment but also reinvigorated enthusiasm in
stroke care and research. While recent progress in stroke trials
has not directly yielded new clinical drugs, they have providedimportant mechanistic insights into the complex pathophysi-
ology of ischaemic stroke which will pave the way for upcom-
ing studies. Future neuroprotection experiments must be
methodologically sound and learn from previous failed
attempts, while clinical trials must take into account the
success achieved in preclinical studies.
With this respect, the implementation of essential quality
standards in experimental stroke research is without doubt a
meaningful measure. However, one has to keep the balance
between high quality on the one hand, and practicability in an
academic laboratory environment on the other hand. The
postulation to validate rodent findings in primates, forexample, is easily spoken but nearly impossible to realize given
that only a few primate facilities are available across Europe
(111). Ethical aspects have to be carefully considered as well
when using higher animal species in injuring and disabling
disease models. In order to provide proof-of-principle evi-
dence, it is in most cases neither necessary nor feasible to plan
and perform basic stroke studies like large controlled rand-
omized clinical trials. This is also frequently prevented by the
increasing numbers of budget cuts the scientific community
currently has to face, limited animal housing and breeding
space, lack of qualified staff, rough scientific competition, and
the strict domestic and international regulations for animal
care and use. Finally, more than 10 years after the first STAIR
recommendations were published, the ultimate proof that
plain standardization of procedures in fact increases the rate
of successful translation from bench to bedside in stroke
research is still missing. Some critics even raise the provocative
question of whether excessive methodological uniformity
counteracts innovation and only prevents promising drug
candidates from entering into clinical trials and renowned
scientific journals. Positive experiences from other neurologi-
cal diseases like multiple sclerosis should teach the stroke com-
munity that even imperfect animal models can serve as a basis
ReviewB. A. Sutherland et al .
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke OrganizationVol 7, July 2012, 407–418 415
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
10/12
for hypothesis-driven research that ultimately facilitates the
development of new drugs.
Acknowledgements
The authors were supported by Fondation Leducq (BAS and
AMB), Medical Research Council UK (AMB), the National
Institute for Health Research Biomedical Research Centre
(JSB, FA and AMB), the Deutsche Forschungsgemeinschaft
(SFB 688, TPA13 and KL 2323/4-1, CK), the Wilhelm-Sander
Stiftung (2009·017·1, CK), the European Union (Seventh
Framework Programme FP7, HEALTH-F2-2009-241778,
CK), and the Bundesministerium für Bildung und Forschung
(BMBF, 01GN0980, JM).
References
1 Durukan A, Tatlisumak T. Acute ischemic stroke: overview of major
experimental rodent models, pathophysiology, and therapy of focal
cerebral ischemia. Pharmacol Biochem Behav 2007; 87:179–97.
2 O’Collins VE, Macleod MR, Donnan GA, Horky LL, van der Worp
BH,Howells DW. 1,026 experimental treatments in acute stroke. Ann
Neurol 2006; 59:467–77.
3 Strokecenter.org, Stroke Trials Registry, Dallas: UT Southwestern
Medical Center. 1997 Availableat: http://www.strokecenter.org/trials/
(accessed April 2011).
4 GinsbergMD. Neuroprotection for ischemic stroke: past, presentand
future. Neuropharmacology 2008; 55:363–89.
5 Fisher M, Feuerstein G, Howells DW et al . Update of the stroke
therapy academic industry roundtable preclinical recommendations.
Stroke 2009; 40:2244–50.
6 STAIR.Recommendations for standards regarding preclinical neuro-
protective and restorative drug development. Stroke 1999; 30:2752–8.
7 Cheng YD, Al-Khoury L, Zivin JA. Neuroprotection for ischemic
stroke: two decades of success and failure. NeuroRx 2004; 1:36–45.
8 Endres M, Engelhardt B, Koistinaho J et al . Improving outcome after
stroke: overcoming the translational roadblock. CerebrovascDis 2008;
25:268–78.
9 Hoyte L, Kaur J, Buchan AM. Lost in translation: taking neuropro-
tection from animal models to clinical trials. Exp Neurol 2004;
188:200–4.
10 Buchan A, Pulsinelli WA. Hypothermia but not the N-methyl-D-
aspartate antagonist, MK-801, attenuates neuronal damage in gerbils
subjected to transient global ischemia. J Neurosci 1990; 10:311–6.
11 Buchan AM, Slivka A, Xue D. The effect of the NMDA receptor
antagonist MK-801 on cerebral blood flow and infarct volume in
experimental focal stroke. Brain Res 1992; 574:171–7.
12 Sutherland BA, Papadakis M, Chen R-L, Buchan AM. Cerebral blood
flow alteration in neuroprotection following cerebral ischemia. J
Physiol 2011; 589:4105–14.
13 Nikic I, Merkler D, Sorbara C et al . A reversible form of axon damage
in experimental autoimmune encephalomyelitis and multiple sclero-
sis. Nat Med 2011; 17:495–9.
14 Sena ES, van der Worp HB, Bath PM, Howells DW, Macleod MR.
Publication bias in reports of animal stroke studies leads to major
overstatement of efficacy. PLoS Biol 2010; 8:e1000344.
15 Fisher M. New approaches to neuroprotective drug development.
Stroke 2011; 42(Suppl. 1):S24–7.
16 Minnerup J, Schabitz WR. Multifunctional actions of approved and
candidate stroke drugs. Neurother 2009; 6:43–52.
17 Dirnagl U, Macleod MR. Stroke research at a road block: the streets
from adversity should be paved with meta-analysis and good labo-
ratory practice. Br J Pharmacol 2009; 157:1154–6.
18 Macleod MR, van der Worp HB, Sena ES, Howells DW, Dirnagl U,
Donnan GA. Evidence for the efficacy of NXY-059 in experimental
focal cerebral ischaemia is confounded by study quality. Stroke 2008;
39:2824–9.
19 Minnerup J, Heidrich J, Wellmann J, Rogalewski A, Schneider A,
Schabitz WR. Meta-analysis of the efficacy of granulocyte-colony
stimulating factor in animal models of focal cerebral ischemia. Stroke
2008; 39:1855–61.
20 Thecochranelibrary.com, The Cochrane Library, Chichester, UK:
John wiley & Sons Ltd. 1996 Available at: http://www.
thecochranelibrary.com/ (accessed April 2011).
21 van der Worp HB, Sena ES, Donnan GA, Howells DW,Macleod MR.
Hypothermia in animal models of acute ischaemic stroke: a system-
atic review and meta-analysis. Brain 2007; 130(Pt 12):3063–74.
22 Yenari M, Kitagawa K, Lyden P, Perez-Pinzon M. Metabolic down-
regulation: a key to successful neuroprotection? Stroke 2008;
39:2910–7.
23 Berger C, Schabitz WR, Georgiadis D, Steiner T, Aschoff A,
Schwab S. Effects of hypothermia on excitatory amino acids and
metabolism in stroke patients: a microdialysis study. Stroke 2002;
33:519–24.
24 Globus MY, Alonso O, Dietrich WD, Busto R, Ginsberg MD.
Glutamatereleaseand free radical production following brain injury:
effects of posttraumatic hypothermia. J Neurochem 1995; 65:1704–
11.
25 Krieger DW, De Georgia MA, Abou-Chebl A et al . Cooling for acute
ischemic brain damage (cool aid): an open pilot study of induced
hypothermia in acute ischemic stroke. Stroke 2001; 32:1847–54.
26 De Georgia MA, Krieger DW, Abou-Chebl A et al . Cooling for Acute
Ischemic Brain Damage (COOL AID): a feasibility trial of endovas-
cular cooling. Neurology 2004; 63:312–7.
27 Hemmen TM, Raman R, Guluma KZ et al . Intravenous thrombolysis
plus hypothermia for acute treatment of ischemic stroke (ICTuS-L):
final results. Stroke 2010; 41:2265–70.
28 Hemmen TM, Lyden PD. Induced hypothermia for acute stroke.
Stroke 2007; 38(Suppl. 2):794–9.
29 Lyden PD, Krieger D, Yenari M, Dietrich WD. Therapeutic hypother-
mia for acute stroke. Int J Stroke 2006; 1:9–19.
30 Schwab S, Georgiadis D, Berrouschot J, Schellinger PD, Graffagnino
C, Mayer SA. Feasibility and safety of moderate hypothermia after
massive hemispheric infarction. Stroke 2001; 32:2033–5.
31 He P, Curry FE. Albumin modulation of capillary permeability:
role of endothelial cell [Ca2+]i. Am J Physiol 1993; 265(1 Pt 2):H74–
82.
32 Belayev L, Liu Y, Zhao W, Busto R, Ginsberg MD. Human albumin
therapy of acute ischemic stroke: marked neuroprotective efficacy at
moderate doses and with a broad therapeutic window. Stroke 2001;
32:553–60.
33 Ginsberg MD, Hill MD, Palesch YY, Ryckborst KJ, Tamariz D. The
ALIAS Pilot Trial: a dose-escalation and safety study of albumin
therapy for acute ischemic stroke – I: Physiological responses and
safety results. Stroke 2006; 37:2100–6.
34 Palesch YY, Hill MD, Ryckborst KJ, Tamariz D, Ginsberg MD. The
ALIAS Pilot Trial: a dose-escalation and safety study of albumin
therapy for acute ischemic stroke – II: neurologic outcome and effi-
cacy analysis. Stroke 2006; 37:2107–14.
35 Ginsberg MD, Palesch YY, Hill MD. The ALIAS (ALbumin In Acute
Stroke) Phase III randomized multicentre clinical trial: design and
progress report. Biochem Soc Trans 2006; 34(Pt 6):1323–6.
36 O’Collins VE, Macleod MR, Cox SF et al . Preclinical drug evaluation
for combination therapy in acute stroke using systematic review,
meta-analysis, and subsequent experimental testing. J Cereb Blood
Flow Metab 2011; 31:962–75.
37 Ovbiagele B, Kidwell CS, Starkman S, Saver JL. Neuroprotective
agents for the treatment of acute ischemic stroke. Curr Neurol Neu-
rosci Rep 2003; 3:9–20.
Review B. A. Sutherland et al .
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke Organization416 Vol 7, July 2012, 407–418
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
11/12
38 Meloni BP, Zhu H, Knuckey NW. Is magnesium neuroprotective
following global and focal cerebral ischaemia? A review of published
studies. Magnes Res 2006; 19:123–37.
39 Saver JL, Kidwell C, Eckstein M, Starkman S. Prehospital neuropro-
tective therapy for acute stroke: results of the Field Administration of
Stroke Therapy-Magnesium (FAST-MAG) pilot trial. Stroke 2004;
35:e106–8.
40 Lampl Y, Boaz M, Gilad R et al . Minocycline treatment in acute
stroke: an open-label, evaluator-blinded study. Neurology 2007;
69:1404–10.
41 Prass K, Meisel C, Hoflich C et al . Stroke-induced immunodeficiency
promotes spontaneous bacterial infections and is mediated by sym-
pathetic activation reversal by poststroke T helper cell type 1-like
immunostimulation. J Exp Med 2003; 198:725–36.
42 Fagan SC, Waller JL, Nichols FT et al . Minocycline to improve neu-
rologic outcome in stroke (MINOS): a dose-finding study. Stroke
2010; 41:2283–7.
43 Clinicaltrials.gov. Neuroprotection With Minocycline Therapy for
Acute Stroke Recovery Trial (NeuMAST), Bethesda: US National
Institutes of Health. 2009 Available at: http://clinicaltrials.gov/ct2/
show/study/NCT00930020 (accessed April 2011).
44 Cimino M, Balduini W, Carloni S et al . Neuroprotective effect
of simvastatin in stroke: a comparison between adult and neonatal
rat models of cerebral ischemia. Neurotoxicology 2005; 26:929–33.
45 Cimino M,Gelosa P,Gianella A,Nobili E, Tremoli E,Sironi L.Statins:
multiple mechanisms of action in the ischemic brain. Neuroscientist
2007; 13:208–13.
46 Elkind MS, Sacco RL, Macarthur RB et al . High-dose lovastatin for
acute ischemic stroke: results of the phase I dose escalation neuro-
protection with statin therapy for acute recovery trial (NeuSTART).
Cerebrovasc Dis 2009; 28:266–75.
47 Birnbaum G, Cree B, Altafullah I, Zinser M, Reder AT. Combining
beta interferon and atorvastatin may increase disease activity in mul-
tiple sclerosis. Neurology 2008; 71:1390–5.
48 Angel I, Bar A, Horovitz T et al . Metal ion chelation in neurodegen-
erative disorders. Drug Dev Res 2002; 56:300–9.
49 Diener HC, Schneider D, Lampl Y, Bornstein NM, Kozak A,
Rosenberg G. DP-b99, a membrane-activated metal ion chelator,
as neuroprotective therapy in ischemic stroke. Stroke 2008;
39:1774–8.
50 Braughler JM, Pregenzer JF, Chase RL, Duncan LA, Jacobsen EJ,
McCall JM. Novel 21-amino steroids as potent inhibitors of iron-
dependent lipid peroxidation. J Biol Chem 1987; 262:10438–40.
51 Xue D, Slivka A, Buchan AM. Tirilazad reduces cortical infarction
after transient but not permanent focal cerebral ischemia in rats.
Stroke 1992; 23:894–9.
52 Sena E, Wheble P, Sandercock P, Macleod M. Systematic review and
meta-analysis of the efficacy of tirilazad in experimental stroke.
Stroke 2007; 38:388–94.
53 RANTTAS. A randomized trial of tirilazad mesylate in patients with
acute stroke (RANTTAS). The RANTTAS Investigators. Stroke 1996;
27:1453–8.
54 TISC. Tirilazad mesylate in acute ischemic stroke: A systematicreview. Tirilazad International Steering Committee. Stroke 2000;
31:2257–65.
55 Green AR, Ashwood T, Odergren T, Jackson DM. Nitrones as neu-
roprotective agents in cerebral ischemia, with particular reference to
NXY-059. Pharmacol Ther 2003; 100:195–214.
56 Bath PM, Gray LJ, Bath AJ, Buchan A,Miyata T, Green AR.Effects of
NXY-059 in experimental stroke: an individual animal meta-analysis.
Br J Pharmacol 2009; 157:1157–71.
57 Marshall JW,Cummings RM, Bowes LJ, Ridley RM, Green AR. Func-
tional and histological evidence for the protective effect of NXY-059
in a primate model of stroke when given 4 hours after occlusion.
Stroke 2003; 34:2228–33.
58 Papadakis M, Nagel S, Buchan AM. Development and efficacy of
NXY-059 for the treatment of acute ischemic stroke. Future Neurol
2008; 3:229–40.
59 Lees KR, Zivin JA, Ashwood T et al . NXY-059 for acute ischemic
stroke. N Engl J Med 2006; 354:588–600.
60 Shuaib A, Lees KR, Lyden P et al . NXY-059 for the treatment of acute
ischemic stroke. N Engl J Med 2007; 357:562–71.
61 Diener HC, Lees KR, Lyden P et al . NXY-059 for the treatment of
acute stroke: pooled analysis of the SAINT I and II Trials. Stroke 2008;
39:1751–8.
62 Papadakis M, Buchan AM. NXY-059: brain or vessel protection.
Stroke 2006; 37:2189–90.
63 Zhao Z, Cheng M, Maples KR, Ma JY, Buchan AM. NXY-059, a novel
free radical trapping compound, reduces cortical infarction after
permanent focal cerebral ischemia in the rat. Brain Res 2001; 909:46–
50.
64 Philip M, Benatar M, Fisher M, Savitz SI. Methodological quality of
animal studies of neuroprotective agents currently in phase II/III
acute ischemic stroke trials. Stroke 2009; 40:577–81.
65 Savitz SI. Cosmic implications of NXY-059. Stroke 2009; 40(Suppl.
3):S115–8.
66 Savitz SI. A critical appraisal of the NXY-059 neuroprotection studies
for acute stroke: a need for more rigorous testing of neuroprotective
agents in animal models of stroke. Exp Neurol 2007; 205:20–5.
67 Kleinschnitz C, Grund H, Wingler K et al . Post-stroke inhibition of
induced NADPH oxidase type 4 prevents oxidative stress and neuro-
degeneration. PLoS Biol 2010; 8:pii:e1000479.
68 Tymianski M. Can molecular and cellular neuroprotection be trans-
lated into therapies for patients?: yes, but not the way we tried it
before. Stroke 2010; 41(Suppl. 10):S87–90.
69 Wahlgren NG, Ahmed N. Neuroprotection in cerebral ischaemia:
facts and fancies–the need for new approaches. Cerebrovasc Dis 2004;
17(Suppl. 1):153–66.
70 Lyden P, WahlgrenNG. Mechanisms of action of neuroprotectants in
stroke. J Stroke Cerebrovasc Dis 2000; 9(6 Pt 2):9–14.
71 Small DL, Buchan AM. Animal models. Br Med Bull 2000; 56:307–
17.
72 Chen RL, Balami JS, Esiri MM, Chen LK, Buchan AM. Ischemic
stroke in the elderly: an overview of evidence. Nat Rev Neurol 2010;
6:256–65.
73 Grotta JC, Burgin WS, El-Mitwalli A et al . Intravenous tissue-type
plasminogen activator therapy for ischemic stroke: Houston experi-
ence 1996 to 2000. Arch Neurol 2001; 58:2009–13.
74 Sumii T, Involvement LEH. of matrix metalloproteinase in
thrombolysis-associated hemorrhagic transformation after embolic
focal ischemia in rats. Stroke 2002; 33:831–6.
75 Asahi M, Asahi K, Wang X, Lo EH. Reduction of tissue plasminogen
activator-induced hemorrhage and brain injury by free radical spin
trapping after embolic focal cerebral ischemia in rats. J Cereb Blood
Flow Metab 2000; 20:452–7.
76 Lapchak PA, Araujo DM, Song D, Wei J, Zivin JA. Neuroprotective
effects of the spin trap agent disodium-[(tert-butylimino)
methyl]benzene-1,3-disulfonate N-oxide (generic NXY-059) in arabbit small clot embolic stroke model: combination studies with the
thrombolytic tissue plasminogen activator. Stroke 2002; 33:1411–5.
77 Lekieffre D, Benavides J, Scatton B, Nowicki JP. Neuroprotection
afforded by a combination of eliprodil and a thrombolytic agent,
rt-PA, in a rat thromboembolic stroke model. Brain Res 1997;
776:88–95.
78 Suzuki M, Sasamata M, Miyata K. Neuroprotective effects of YM872
coadministered with t-PA in a rat embolic stroke model. Brain Res
2003; 959:169–72.
79 Lapchak PA, Zivin JA. Ebselen, a seleno-organic antioxidant, is neu-
roprotective after embolic strokes in rabbits: synergism with low-
dose tissue plasminogen activator. Stroke 2003; 34:2013–8.
ReviewB. A. Sutherland et al .
© 2012 The Authors.
International Journal of Stroke © 2012 World Stroke OrganizationVol 7, July 2012, 407–418 417
-
8/16/2019 3. Neuroprotection for Ischaemic Stroke Translation From the Bench to the Bedside
12/12
80 Zhang RL, Zhang ZG, Chopp M. Increased therapeutic efficacy with
rt-PA and anti-CD18 antibody treatment of stroke in the rat. Neu-
rology 1999; 52:273–9.
81 Ding G, Jiang Q, Zhang L et al . Analysis of combined treatment of
embolic stroke in rat with r-tPA and a GPIIb/IIIa inhibitor. J Cereb
Blood Flow Metab 2005; 25:87–97.
82 Shuaib A, Yang Y, Nakada MT, Li Q, Yang T. Glycoprotein IIb/IIIa
antagonist, murine 7E3 F(ab’) 2, and tissue plasminogen activator in
focal ischemia: evaluation of efficacy and risk of hemorrhage with
combination therapy. J Cereb Blood Flow Metab 2002; 22:215–22.
83 Stoll G, Kleinschnitz C, Nieswandt B. Molecular mechanisms of
thrombus formation in ischemic stroke: novel insights and targets for
treatment. Blood 2008; 112:3555–62.
84 Grotta J. Combination TherapyStroke Trial: recombinant tissue-type
plasminogen activator with/without lubeluzole. Cerebrovasc Dis
2001; 12:258–63.
85 Lyden P, Jacoby M, Schim J et al . The Clomethiazole Acute Stroke
Study in tissue-type plasminogen activator-treated stroke (CLASS-
T): final results. Neurology 2001; 57:1199–205.
86 Krams M, Lees KR, Hacke W, Grieve AP, Orgogozo JM, Ford GA.
Acute Stroke Therapy by Inhibition of Neutrophils (ASTIN): an
adaptive dose-response study of UK-279,276 in acute ischemic
stroke. Stroke 2003; 34:2543–8.
87 Harston GW, Sutherland BA, Kennedy J, Buchan AM. The contribu-
tion of L-arginine to the neurotoxicity of recombinant tissue plas-
minogen activator following cerebral ischemia: a review of rtPA
neurotoxicity. J Cereb Blood Flow Metab 2010; 30:1804–16.
88 Sachs L. The molecular control of hematopoiesis: from clonal devel-
opment in culture to therapy in the clinic. Int J Cell Cloning 1992;
10:196–204.
89 Schneider A, Kruger C, Steigleder T et al . The hematopoietic factor
G-CSF is a neuronal ligand that counteracts programmed cell death
and drives neurogenesis. J Clin Invest 2005; 115:2083–98.
90 Siren AL, Knerlich F, Poser W, Gleiter CH, Bruck W, Ehrenreich H.
Erythropoietin and erythropoietin receptor in human ischemic/
hypoxic brain. Acta Neuropathol 2001; 101:271–6.
91 Ruscher K, Freyer D, Karsch M et al . Erythropoietin is a paracrine
mediator of ischemic tolerance in thebrain:evidence from an in vitro
model. J Neurosci 2002; 22:10291–301.
92 Solaroglu I, Cahill J, Tsubokawa T, Beskonakli E, Zhang JH.
Granulocyte colony-stimulating factor protects the brain against
experimental stroke via inhibition of apoptosis and inflammation.
Neurol Res 2009; 31:167–72.
93 Villa P, Bigini P, Mennini T et al . Erythropoietin selectively attenu-
ates cytokine production and inflammation in cerebral ischemia by
targeting neuronal apoptosis. J Exp Med 2003; 198:971–5.
94 Lee ST, Chu K, Jung KH et al . Granulocyte colony-stimulating factor
enhances angiogenesis after focal cerebral ischemia. Brain Res 2005;
1058:120–8.
95 Wang L, Zhang Z, Wang Y, Zhang R, Chopp M. Treatment of stroke
with erythropoietin enhances neurogenesis and angiogenesis and
improves neurological function in rats. Stroke 2004; 35:1732–7.
96 England TJ, Gibson CL, Bath PM. Granulocyte-colony stimulatingfactor in experimental stroke and its effects on infarct size and func-
tional outcome: a systematic review. Brain Res Rev 2009; 62:71–82.
97 Jerndal M, Forsberg K, Sena ES et al . A systematic review and meta-
analysis of erythropoietin in experimental stroke. J Cereb Blood Flow
Metab 2010; 30:961–8.
98 Minnerup J,Heidrich J,Rogalewski A,Schabitz WR,Wellmann J.The
efficacy of erythropoietin and its analogues in animal stroke models:
a meta-analysis. Stroke 2009; 40:3113–20.
99 Ehrenreich H, Hasselblatt M, Dembowski C et al . Erythropoietin
therapy for acute stroke is both safe and beneficial. Mol Med 2002;
8:495–505.
100 Ehrenreich H, Weissenborn K, Prange H et al . Recombinant human
erythropoietin in the treatment of acute ischemic stroke. Stroke 2009;
40:e647–56.
101 Minnerup J, Wersching H, Schabitz WR. EPO for stroke therapy – Is
there a futurefor further clinical development? ExpTranslStroke Med
2010; 2:10.
102 Schabitz WR, Laage R, Vogt G et al . AXIS: a trial of intravenous
granulocyte colony-stimulating factor in acute ischemic stroke.
Stroke 2010; 41:2545–51.
103 Clinicaltrials.gov. AXIS 2: AX200 for the Treatment of Ischemic
Stroke (AXIS-2), Bethesda: US National Institute for Health.
2009 Available at: http://clinicaltrials.gov/ct2/show/NCT00927836
(accessed April 2011).
104 Flamm ES, Demopoulos HB, Seligman ML, Poser RG, Ransohoff J.
Free radicals in cerebral ischemia. Stroke 1978; 9:445–7.
105 Crack PJ, Taylor JM. Reactive oxygen species and the modulation of
stroke. Free Radic Biol Med 2005; 38:1433–44.
106 Dhalla NS, Temsah RM, Netticadan T. Role of oxidative stress in
cardiovascular diseases. J Hypertens 2000; 18:655–73.
107 Miller AA, Drummond GR, Sobey CG. Novel isoforms of NADPH-
oxidase in cerebral vascular control. Pharmacol Ther 2006; 111:928–
48.
108 Sedwick C. NOX4: a guilty party in stroke damage. PLoS Biol 2010;
8:pii:e1000478.
109 Sancho P, Fabregat I. The NADPH oxidase inhibitor VAS2870
impairs cell growth and enhances TGF-beta-induced apoptosis of
liver tumor cells. Biochem Pharmacol 2011; 81:917–24.
110 NINDS. Tissue plasminogen activator for acute ischemic stroke. The
National Institute of Neurological Disorders and Stroke rt-PA Stroke
Study Group. N Engl J Med 1995; 333:1581–7.
111 Schiermeier Q. Primate work faces German veto. Nature 2007;
446:955.
Supporting Information
Additional Supporting Information may be found in the
online version of this article:
Table S1. Neuroprotective strategies that have completed
trials for acute ischaemic stroke.1 All neuroprotective strate-
gies have thus far failed to show an improvement in clinical
benefit following acute ischaemic stroke.
Please note: Wiley-Blackwell are not responsible for the
content or functionality of any supporting materials supplied
by the authors. Any queries (other than missing material)
should be directed to the corresponding author for the article.
Review B. A. Sutherland et al .
© 2012 The Authors.418 Vol 7 July 2012 407–418