241 Early management of brachial plexus inries
27
Early Management of Brachial Plexus Injuries Youmans Chapter 241 Allan Belzberg Martin J. A Malessy
-
Upload
neurosurgery-vajira -
Category
Health & Medicine
-
view
30 -
download
2
Transcript of 241 Early management of brachial plexus inries

Early Management of Brachial Plexus Injuries
Youmans Chapter 241Allan Belzberg
Martin J. A Malessy

Brachial plexus lesion• Shoulder-neck angle is forcefully widened entire
plexus or a part of the BP nerves is elongated• Cause
– Motor cycle accident– Neoplasm– Missile injury– Birth-related injury
• Surgical treatment– end-to-end neurotization– interpositional nerve grafting– intraplexus/extraplexus nerve transfer

Anatomy

Anatomy

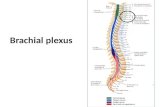
Anatomy• Roots
– anterior divisions of spinal nerves C5-T1 – pass between the anterior and medial scalene muscles
• Trunks– Superior trunk: A combination of C5 and C6 roots.– Middle trunk: A continuation of C7.– Inferior trunk: A combination of C8 and T1 roots.– move laterally, crossing the posterior triangle of the neck
• Divisions– Anterior division– Posterior division

Anatomy• Cords
– The lateral cord is formed by:• The anterior division of the superior trunk• The anterior division of the middle trunk
– The posterior cord is formed by:• The posterior division of the superior trunk• The posterior division of the middle trunk• The posterior division of the inferior trunk
– The medial cord is formed by:• The anterior division of the inferior trunk

Anatomy• Branchs
– Musculocutaneous Nerve(C5,C6,C7)– Axillary Nerve(C5,C6)– Median Nerve(C6,C7,C8,T1)– Radial Nerve(C5,C6,C7,C8,T1)– Ulnar Nerve(C8,T1)

Pathophysiology and classification
• Traction injuries : head and neck move away from the ipsilateral shoulder C5,C6 spinal nerves or upper trunk
• Arm abduct over the head : lower element of BP• C5-6-7 have fibrous attachment at cervical transverse
process, C8-T1 absent• T1 sympathetic component of head and neck injury to
T1 result in sympathetic ganglion loss and Bernad-Horner syndrome(miosis, ptosis and anhidrosis)

Greenberg,7th page 802

Clinical• Trauma and associate injury• Time course• Factor impede nerve regeneration : age, neuropathy,
metabolic disturbance, systemic disease• Medical record : surgical of subclavian artery, fracture
spine

Clinical

Clinical• Preserve dorsal scapular n.(Rhomboid m.), long thoracic
n.(serratus anterior m) but loss external rotation of the shoulder(infraspinatus m.) first 30 degree of shoulder abduction(supraspinatus m.) : distal to spinal nerve and into the upper trunk
• Atrophy of Pectoralis m is innervated by medial and lateral pectoral n (branch of medial and lateral cord) pan-plexus injury
• Bernard-Horner sign high indicative for avulsion of C8 and T1 : false negative more common, may not be present in 48 hr after injury

Clinical• Regeneratee nerve fiber develop mechanosensitivity• Hoffman-Tinel or Tinel’s sign : percussion over the
course of the nerve tingling paresthesia (distal to lesion site)
• Tinel sign does not indicative the number or quality of regenerating axon and does not guarantee functional outcome
• Lack of tinel sign poor prognosis

Clinical• Plain film cervical, chest
– spinal transvere process fx : nerve root injury– Elevate hemidiaphragm : phrenic n. C3,C4,C5– Clavicular Fx : traumatic BPI

Therapy/Management• nonoperative care
– ROM joint, muscle, tendon– Neuropathic pain : anticonvulsant with narcotic
• appropriate selection of surgical candidates– Avulsion of nerve root severe pain surgical manage at
DREZ• timing of surgery
– Sunder land gr.V by Sharp laceration and transection : immediate exploration and repair
– Sunder land gr.V by Stretch mechanism : 2-3 wk after injury– Strecth : observe for 3-4 mo for regeneration

Therapy/Management• priorities of the surgical targets
– Elbow flexion– Shoudler abduction– Sensation of hand– Wrist extension, finger flexion, wrist flexion,finger
extension• method of nerve repair
– Differentiate Sunderland grade III from IV : need for surgical resection and nerve repair

Therapy/Management• Timing of and Selection for Surgery in Patients with
Birth-Related Brachial Plexus Injuries• Surgical Exposure• Nerve Transfer Surgery• Outcomes after Treatment of Brachial Plexus Birth Injury

Timing of and Selection for Surgery in Patients with Birth-Related Brachial Plexus Injuries(BRBPI)
• Neurapraxia, axonotmesis : complete or nearly complete recovery
• Neurotmesis and root avulsion : permanent loss of arm function
• 2- 3 month of age, before 7 mo• Paralysis of the bicep m at 3 mo : wrist drop

Surgical Exposure
• Supraclavicular exposure• Infraclavicular exposure• Posterior exposure

Supraclavicular exposure• 2 cm above and parallel to clavicle• Omohyoid m. : upper border• Anterior scalene m. : phrenic n. coursing,C5 nerve root• Upper trunk : lateral border of Anterior scalene m. • Middle and lower trunk• Protect long thoracic n.

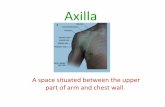
Infraclavicular exposure• Incision at deltoid-pectoral groove• Pectoralis major : blunt• Pectoralis minor : retract upward or downward• Infraclavicular BP : lateral cord seen first, then posterior
cord• Subclavian a.• Median n., MCN m. : retract lateral cord

Posterior exposure• Prone position, Parascapular incision• Trapezius and rhomboid m. resection• Paraspinal m. retract• Proximal spinal n.

Nerve transfer surgery• Spinal accessory transfer• Intercostal transfer• Contralateral C7 transfer

Spinal accessory transfer• Often used to Innervate SSN, MCN• End-to-end transfer• Exit under sternocleidomastoid and cross the posterior
triangle

Intercostal transfer
• Often T3,T4,T5 because to mobilized to end-to-end transfer to MCN

A : incision at inferior border of major pectoralis mB.identify MCNC.ICN transect from sternum c sensory branch, MCN cut from lateral cordD.ICN was tunnel to MCN

Outcome of function• Shoulder function : fairy good recovery• Elbow flexion : good recovery• Recovery of Hand function : maximal function to use
affect limb as hook