2013-40-4_17-30
14
Effect of Pharmacist’s Interventions on Glycemic Control in Diabetic Patients: A Systematic Review and Meta-analysis of Randomized Controlled Trials Nalinee Poolsup, 1 Naeti Suksomboon, 2 * Methinee Intarates 2 1 Department of Pharmacy, Faculty of Pharmacy, Silpakorn University, Nakhon-Pathom, 73000, Thailand 2 Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok, 10400, Thailand Abstract Several clinical trials have evaluated the effect of pharmacists’ interventions. However, the results have been inconsistent. We performed a systematic review to evaluate the effect of pharmacists’ interventions on glycemic control in diabetes. Clinical trials of pharmacists’ interventions aimed at improving glycemic control in diabetes patients were identified through a systematic search of MEDLINE, CINAHL, Web of Science, the Cochrane Library, and THAILIS. The bibliographic databases were searched from their inceptions to the end of February 2012. The references lists of relevant articles were checked and experts were consulted. Studies were included if they were: i) randomized controlled trials of pharmacists’ interventions aimed at improving glycemic control in diabetes patients, ii) reporting HbA 1c as an outcome measure, iii) published in English or Thai, and iv) clearly describing details of pharmacists’ intervention. Treatment effect was estimated with the mean difference in the change of HbA 1c levels from baseline between the intervention and the control groups. Twenty-two trials involving 2,808 patients were included. Pharmacists’ interventions included an assessment and adjustment of anti-diabetic medications, identification of drug-related problems, co-operation with physicians and other members of the health care team, offering diabetes booklets and special medication containers, providing education concerning self- management of diabetes, and reinforcement of diabetes management with pharmacotherapy and non-pharmacotherapy. This meta-analysis showed that pharmacists’ interventions can improve glycemic control in diabetes patients (mean difference -0.68%, 95% CI -0.87% to -0.49%, p < 0.00001). Thus, pharmacists can play an important role in diabetes management. Keyword: systematic review, pharmaceutical care, glycemic control, diabetes INTRODUCTION Uncontrolled diabetes leads to micro- vascular complications, namely, retinopathy, nephropathy, and neuropathy, and macrovascular complications, namely, congestive heart failure (CHF), cerebrovascular disease (CVD), and peripheral arterial disease (PAD). 1 Pharmacist has recently been involved in multidisciplinary team. The role of pharmacist in diabetes care, including discharged counseling and providing patient education regarding disease and medication, especially, drug related problem (DRP) monitoring, 2-4 is the most important responsibility of pharmacist to their patients for positive outcomes such as improving quality of life and keeping targeted goal of hemoglobin A 1c (HbA 1c ). Evidence is clear that improving glycemic control and preventing complications result in significant cost saving and improved quality of life. 5 There have been a large number of clinical trials evaluating pharmacists’ *Corresponding author: Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok 10400, Thailand. E-mail: [email protected] Original Article Mahidol University Journal of Pharmaceutical Sciences 2013; 40 (4), 17-30
description
fvfc
Transcript of 2013-40-4_17-30
-
Effect of Pharmacists Interventions on Glycemic Control in Diabetic Patients: A Systematic Review and Meta-analysis of Randomized Controlled TrialsNalinee Poolsup,1 Naeti Suksomboon,2* Methinee Intarates2 1 Department of Pharmacy, Faculty of Pharmacy, Silpakorn University, Nakhon-Pathom, 73000, Thailand 2 Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok, 10400, Thailand
Abstract Several clinical trials have evaluated the effect of pharmacists interventions. However, the results have been inconsistent. We performed a systematic review to evaluate the effect of pharmacists interventions on glycemic control in diabetes. Clinical trials of pharmacists interventions aimed at improving glycemic control in diabetes patients were identified through a systematic search of MEDLINE, CINAHL, Web of Science, the Cochrane Library, and THAILIS. The bibliographic databases were searched from their inceptions to the end of February 2012. The references lists of relevant articles were checked and experts were consulted. Studies were included if they were: i) randomized controlled trials of pharmacists interventions aimed at improving glycemic control in diabetes patients, ii) reporting HbA1c as an outcome measure, iii) published in English or Thai, and iv) clearly describing details of pharmacists intervention. Treatment effect was estimated with the mean difference in the change of HbA1c levels from baseline between the intervention and the control groups. Twenty-two trials involving 2,808 patients were included. Pharmacists interventions included an assessment and adjustment of anti-diabetic medications, identification of drug-related problems, co-operation with physicians and other members of the health care team, offering diabetes booklets and special medication containers, providing education concerning self-management of diabetes, and reinforcement of diabetes management with pharmacotherapy and non-pharmacotherapy. This meta-analysis showed that pharmacists interventions can improve glycemic control in diabetes patients (mean difference -0.68%, 95% CI -0.87% to -0.49%, p < 0.00001). Thus, pharmacists can play an important role in diabetes management.
Keyword: systematic review, pharmaceutical care, glycemic control, diabetes
INTRODUCTION Uncontrolled diabetes leads to micro-vascular complications, namely, retinopathy, nephropathy, and neuropathy, and macrovascular complications, namely, congestive heart failure (CHF), cerebrovascular disease (CVD), and peripheral arterial disease (PAD).1 Pharmacist has recently been involved in multidisciplinary team. The role of pharmacist in diabetes care, including discharged counseling and providing patient education regarding disease
and medication, especially, drug related problem (DRP) monitoring,2-4 is the most important responsibility of pharmacist to their patients for positive outcomes such as improving quality of life and keeping targeted goal of hemoglobin A1c (HbA1c). Evidence is clear that improving glycemic control and preventing complications result in significant cost saving and improved quality of life.5 There have been a large number of clinical trials evaluating pharmacists
*Corresponding author: Department of Pharmacy, Faculty of Pharmacy, Mahidol University, Bangkok 10400, Thailand. E-mail: [email protected]
Original Article Mahidol University Journal of Pharmaceutical Sciences 2013; 40 (4), 17-30
-
N. Poolsup et al.18
interventions in diabetes mellitus (DM). However, the outcomes of these studies remain controversial. We conducted a systematic review and meta-analysis to assess the effect of pharmacists interventions on HbA1c level in diabetes patients.
METHODS Data sources
Reports of randomized controlled trials of pharmacists interventions aimed for good glycemic control in diabetes patients were identified through a systematic literature search of MEDLINE, CINAHL, the Cochrane Library, Web of Science, and the THAIland Library Integrated System (THAILIS). Literature searches were conducted from inception to the end of February 2012. The MeSH terms pharmaceutical services, pharmacists, and diabetes mellitus were used together with keywords pharmaceutical care and pharmacy counseling. Hand search was also performed on relevant journals in Thailand such as Journal of the Medical Association of Thailand, Thai Journal of Hospital Pharmacy. References of retrieved studies and reviews of the topic were hand searched and experts in the field were contacted for additional papers not captured by the search strategy.
Study selection
The studies were included in the review if they: 1) were randomized controlled trials of any pharmacists interventions compared with usual care in diabetes patients, including type 1, type 2, Gestational diabetes mellitus (GDM), or unspecified DM; 2) reported HbA1c as an outcome measure; 3) were published in English or Thai language; and 4) clearly described pharmacists intervention. Abstract presenta-tion was excluded.
Data extraction and quality assessment
Data extraction and study quality assessment were performed independently by two investigators using a standardized form. Disagreements were resolved by a third investigator. Data from individual studies were abstracted. Data recorded were
the year of publication, setting, country, duration of study, intervention frequency, number of visit, inclusion criteria and exclusion criteria of each trial, type of DM, concomitant drug and disease, sample size, age, duration of DM, details of pharmacists interventions and control intervention, and primary outcomes. Quality of randomized controlled trials included in this review was assessed using Maastricht-Amsterdam scale.6 The scale comprises 11 items to evaluate internal validity of the study results. Studies that met at least 6 of 11 quality criteria were of high quality. Those scoring less than 6 of the criteria were of low quality.
Statistical analysis
Treatment effect was estimated with a mean difference in the change of HbA1c level from baseline to final assessment between the intervention group and the control group. If the variances of change values were not provided, but the exact p-value of the mean difference between the intervention and the control groups was available, the p-value was used to impute the variance.7 If the variances of change values and the exact p-values of the mean difference were not provided, the pooled interstudy variances were imputed from studies reporting variances. The inverse variance-weighted method was used for the pooling of mean difference and the estimation of 95% confidence interval (CI).8 A random effects model was used when the Q-statistic for heterogeneity was significant at the level of 0.1,9 otherwise the fixed effects model was used.8 The degree of heterogeneity was quantified using the I2 statistic which is the percentage of total variation across studies due to heterogeneity.10 A funnel plot and Eggers method11 were performed to assess publication bias. Statistical analysis was undertaken with RevMan version 5.1 (Cochrane Collaboration, Oxford, UK). The significant level was set at p < 0.05.
RESULTS Study characteristics
The initial search of the computerized
-
19Effect of Pharmacists Interventions on Glycemic Control in Diabetic Patients: A Systematic Review and Meta-analysis of Randomized Controlled Trials
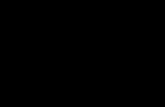
database and hand search identified a total of 1,160 articles (Figure 1). After the initial screening, 44 trials were attained in the selection process. Among the 44 trials, 16 trials were excluded because they did not report glycemic control/HbA1c. Five trials were further excluded because they did not state clearly the role of pharmacist in the intervention group. One trial reported results in terms of median and interquartile range
and was then excluded. Only 22 randomized controlled trials met inclusion criteria and were included in the systematic review and meta-analysis. Characteristics of these trials are presented in Table 1. In general, there were no significant differences between patients in the intervention group and those in the control group with respect to age and duration of diabetes.
Figure 1. Flow diagram of study selection for meta-analysis
Those trials, involved patients with type 1, type 2, GDM, or unspecified DM and were reported between 1996 and 2012. The setting of trials included primary care unit, home care, community pharmacy, primary care hospital, tertiary care hospital, a university-affiliated internal medicine outpatient clinic, endocrine clinic, military hospital, and veteran medical center in the USA, Canada, Australia, Sweden, Spain, UAE, and Thailand. The duration of trials varied from 3 months to 2 years. Pharmacists intervention was given at different frequency, for example, once a week and once every 6 months. Number of visit ranged between 1 and 24 times. Pharmacists involved included registered pharmacist,12,20,26,32 clinical pharmacist,14,16-18,21,23,25,27,29,30 community pharmacist,22,24,28,32 clinical pharmacist with multidisciplinary team,19,31 certified diabetes educator pharmacists,13 specially trained pharmacists.15 The methods of follow-up were
face-to-face encounter and/or by telephone. Details of pharmacist interventions differed from trial to trial (Table 2 and 3) and encompassed the followings: diabetes education and counseling about drug, disease, diet, exercise, life style modification, and self-management, assessment and adjustment of antidiabetic medications, identifying and solving drug-related problems, co-operating with physician and other diabetes health care team, providing materials, leaflet, diabetes booklet and special medication containers, and monthly newsletter that enforced patients to achieve a target goal, reminding about annual eye and foot examinations, and providing additional information about smoking cessation, stop drinking alcohol. For the usual care group, patients continued to receive standard medical care provided by their physicians, other health care team, and with/without pharmacists depending on each study design (Table 2).
-
N. Poolsup et al.20
No.
St
udy
Setti
ng
Cou
ntry
D
urat
ion
In
terv
entio
n In
clusio
n
of st
udy
frequ
ency
cr
iteria
1
Jabe
r LA
199
612
A U
nive
rsity
-affi
liate
d in
tern
al
US
4 m
o 2-
4 w
eeks
/tim
e T2
DM
m
edic
ine o
utpa
tient
clin
ic
2
Gui
rgui
s LM
200
113
Chai
n ph
arm
acy,
shop
pers
Ca
nada
; 6
mo
< 1
mon
th/ti
me
T2D
M fo
r Alb
erta
a m
inim
um
drug
mar
t Ed
mon
ton,
of
1 y
ear,
non-
insti
tutio
naliz
ed
3 Cl
iffor
d RM
200
214
Frem
entle
Hos
pita
l,
Austr
alia
6
mo
6 w
eeks
/tim
e A
ged
> 18
yea
rs w
ith ei
ther
T1D
M
diab
etes
out
patie
nt cl
inic
or T
2DM
and
was
hig
h-ris
k
for t
he d
evelo
pmen
t of d
iabe
tes
co
mpl
icat
ions
.
4 Sa
rkad
i A 2
0041
5 St
ockh
olm
Dia
bete
s Ass
ocia
tion
Swed
en
24 m
o 6
mon
ths/
time
T2D
M an
d, if
trea
ted
with
insu
lin,
on
ly fo
r 2 y
ears
or l
ess
5
Cliff
ord
RM 2
0051
6 Fr
emen
tle H
ospi
tal,
Frem
entle
Au
stral
ia
12 m
o 6
wee
ks/ti
me
T2D
M
Dia
bete
s Stu
dy (F
DS)
6 Ch
oe H
M 2
0051
7 U
nive
rsity
-affi
liate
d pr
imar
y
US
24 m
o 1
mon
th/ti
me
T2D
M, H
bA1c
leve
ls >
8.0%
ca
re in
tern
al m
edic
ine c
linic
7 O
dega
rd P
S 20
0518
Th
e Uni
vers
ity o
f Was
hing
ton
US
6 m
o 1
wee
k/tim
e A
ged
18
yea
rs, T
2DM
, tak
ing
at
med
icin
e clin
ics
le
ast o
ne o
ral d
iabe
tes m
edic
atio
n,
with
an H
bA1c
9%
8
Suks
ombo
on N
2005
19
Prim
ary
care
uni
t, Sa
mut
sako
rn
Thai
land
3
mo
3 m
onth
s/tim
e T2
DM
, 18-
60 y
ears
old
, tak
e OA
D
Hos
pita
l
as m
etfo
rmin
, glip
izid
e and
/or
gl
iben
clam
ide,
HbA
1c >
7%
9
Supp
apiti
porn
S 2
0052
0 En
docr
ine c
linic
in K
ing
Th
aila
nd
6 m
o 3
mon
ths/
time
T2D
M, a
ged
> 40
yea
rs
Chul
alon
gkor
n M
emor
ial
H
ospi
tal (
out p
atie
nts)
10
Ro
thm
an R
L 20
0521
U
nive
rsity
of N
orth
Car
olin
a U
S 12
mo
2-4
wee
ks/ti
me
Age
d >1
8 ye
ars o
ld, T
2DM
, HbA
1c
Gen
eral
Inte
rnal
Med
icin
e
leve
l >8.
0%, l
ife ex
pect
ancy
>6
Pr
actic
e
mon
ths
11
Forn
os JA
200
622
Com
mun
ity p
harm
acie
s Sp
ain;
13
mo
1 m
onth
/tim
e tre
atm
ent w
ith o
ral a
ntid
iabe
tics
Pont
eved
ra
for m
ore t
han
2 m
onth
s
12
Scot
t DM
200
623
Siou
xlan
d C
omm
unity
Hea
lth
US
9 m
o 2
wee
ks/ti
me
T2D
M, a
ged
> 18
yea
rs
Cen
ter (
SCH
C)
Tabl
e 1. C
hara
cter
istic
s of t
he st
udie
s inc
lude
d in
the m
eta-
anal
ysis
-
21Effect of Pharmacists Interventions on Glycemic Control in Diabetic Patients: A Systematic Review and Meta-analysis of Randomized Controlled Trials
No.
St
udy
Setti
ng
Cou
ntry
D
urat
ion
In
terv
entio
n In
clusio
n
of st
udy
frequ
ency
cr
iteria
13
Kr
ass I
200
724
Com
mun
ities
pha
rmac
ies
Au
stral
ia
6 m
o 1
mon
th/ti
me
T2D
M, H
bA1c
7
.5%
, tak
ing
at le
ast
on
e ora
l glu
cose
lowe
ring m
edica
tion
or
insu
lin, o
r HbA
1c
7.0%
, tak
ing a
t lea
st
one o
ral g
luco
se lo
werin
g m
edic
atio
n
or in
sulin
, on
at le
ast o
ne an
ti-hy
per-
te
nsiv
e, an
gina
or l
ipid
-lowe
ring
drug
.
14
Elno
ur A
A 2
0082
5 A
l Ain
Hos
pita
l, gy
naec
olog
y
UAE
6 m
o 1
mon
th/ti
me
Patie
nt pr
ovid
ed w
ithin
the fi
rst 20
wee
ks
outp
atie
nt cl
inic
s
of g
esta
tion,
dia
gnos
is of
GD
M, a
nd
ag
ed 2
0- 3
9 ye
ars
15
Ph
umip
amor
n S
2008
26
Com
mun
ity h
ospi
tal i
n Kr
abi
Thai
land
10
mo
2 m
onth
s/tim
e M
uslim
dia
betic
pat
ient
s, ag
ed >
18
pr
ovin
ce
ye
ars,
and
HbA
1c >
7%
16
Pava
sudt
hipa
isit A
200
927 D
iabe
tes C
linic
, Out
-pat
ient
Th
aila
nd
12 m
o 6
mon
ths/
time
T2D
M, H
bA1c
leve
ls >
8.0%
with
out
de
part
men
t, N
ongb
uala
mph
u
mac
rova
scul
ar co
mpl
icat
ions
ho
spita
l
17
Dou
cette
WR
2009
28
Com
mun
ity p
harm
acy p
ract
ice si
te U
S; IO
WA
12
mo
3 m
onth
s/tim
e T2
DM
, HbA
1c >
7.0
%
18
Maz
roui
NRA
200
929
Zaye
d M
ilita
ry H
ospi
tal,
gene
ral
UAE
12 m
o 4
mon
ths/
time
T2D
M, r
ecei
ving
ora
l hyp
ogly
caem
ic
med
ical
war
ds an
d en
docr
inol
ogy
th
erap
y
& m
edic
al o
utpa
tient
clin
ics
19
Tave
ira T
H 2
0103
0 Ve
tera
ns H
ealth
Affa
irs
US
22 m
o 4
wee
ks/ti
me
T2DM
, age
d >
18 ye
ars,
or H
bA1c
7%-9
%
with
in th
e pre
viou
s 6 m
onth
s
20
Ed
elman
D 2
0103
1 Ve
tera
ns A
ffairs
Med
ical
Cen
ters
US;
Car
olin
a 12
.8 m
o 2
mon
ths/
time
Patie
nts h
ad b
oth
diab
etes
and
hype
r-
&
Virg
inia
te
nsio
n, r
ecei
ving
med
icat
ion
for
di
abet
es, a
nd H
bA1c
leve
l >7.
5% a
nd
hy
pert
ensio
n (S
BP >
140
mm
Hg
or
D
BP >
90 m
m H
g)
21
Meh
uys E
201
132
Com
mun
ity p
harm
acie
s Be
lgiu
m
6 m
o 6
wee
ks/ti
me
T2D
M, r
ecei
ving
ora
l hyp
ogly
caem
ic
m
edica
tion
for a
t lea
st 12
mon
ths,
aged
45
75
year
s, BM
I> 2
5 kg
/m2,
and
regu
lar v
isito
r of p
harm
acy
22
Srira
m S
201
133
A p
rivat
e ter
tiary
care
hos
pita
l S
outh
Indi
a 8
mo
3 m
onth
s/tim
e In
dian
, T2D
M, a
ged
> 18
yea
rs, w
ith
or w
ithou
t oth
er d
iseas
es
Tabl
e 1. C
hara
cter
istic
s of t
he st
udie
s inc
lude
d in
the m
eta-
anal
ysis
(con
t.)
-
N. Poolsup et al.22
No.
St
udy
Phar
mac
ist in
terv
entio
n U
sual
care
1 J
aber
LA
199
612
Dia
bete
s edu
catio
n, m
edic
atio
n co
unse
ling,
instr
uctio
ns o
n di
etar
y C
ontin
ued
to re
ceiv
e sta
ndar
d m
edic
al ca
re p
rovi
ded
by
regu
latio
n, ex
erci
se, a
nd h
ome b
lood
glu
cose
mon
itorin
g, an
d
thei
r phy
sicia
ns.
ev
alua
tion
and
adju
stmen
t of t
heir
hypo
glyc
emic
regi
men
.
2 G
uirg
uis L
M 20
0113
Usu
al ca
re p
lus s
ervi
ce p
rovi
de; d
iabe
tes a
nd it
s com
plic
atio
n,
Con
trol p
harm
acie
s pro
vide
d us
ual c
are,
phar
mac
ist
hypo
glyc
emia
, mon
itorin
g bl
ood
gluc
ose l
evel,
use
of
offer
ed p
atie
nts s
ome f
orm
of b
lood
glu
cose
bl
ood
gluc
ose m
onito
r, nu
triti
on, e
xerc
ise, i
nsul
in u
se, i
nsul
in
met
er tr
aini
ng ,
othe
r tra
inin
g on
dia
bete
s man
agem
ent
de
vice
, med
icat
ion
use,
and
foot
care
; and
teac
hing
pro
vide
; (in
-sto
re co
urse
s or c
ontin
uing
educ
atio
n co
urse
).
eval
uate
d te
achi
ng n
eeds
, add
ress
ed p
artic
ipan
t con
cern
s,
re
view
ed b
lood
glu
cose
leve
ls, re
view
ed H
bA1c
, mea
sure
d BP
,
revi
ewed
chol
este
rol l
evels
, scr
eene
d fo
r mic
roal
bum
inur
ia, r
evie
wed
med
icat
ion
profi
le, ad
vise
d on
non
-pre
scrip
tion
med
icat
ions
,
cont
acte
d ph
ysic
ian,
cont
acte
d ot
her m
embe
rs o
f dia
bete
s tea
m, a
nd
m
eter
mai
nten
ance
. 3
Cliff
ord
RM 20
0214
Com
plet
ed a
com
preh
ensiv
e, se
lf-di
rect
ed re
visio
n of
dia
bete
s Re
ceiv
ed st
anda
rd o
utpa
tient
care
, not
com
plet
ed
man
agem
ent p
rior t
o th
e stu
dy, s
aw ea
ch p
atie
nt at
ever
y vi
sit, a
nd
the p
atie
nt sa
tisfa
ctio
n su
rvey
.
co-o
pera
tion
with
the d
iabe
tes p
hysic
ian
and
othe
r hea
lth te
am.
4 S
arka
di A
200
415
The e
duca
tiona
l pro
gram
; a v
ideo
on
how
to l
ive w
ell
with
dia
bete
s, U
sual
care
and
assig
ned
to a
wai
ting
list o
f 2 y
ears
, the
n
exem
plify
ing
lifes
tyle
chan
ges m
ade b
y th
ose i
nter
view
ed, a
dic
e gam
e th
ey w
ere i
nvite
d to
par
ticip
ate i
n th
e edu
catio
nal p
rogr
am.
w
here
que
stion
s had
to b
e ans
wer
ed, a
nd a
book
let o
r gui
de o
n
how
to m
anag
e you
r dia
bete
s. 5
Cliff
ord
RM 20
0516
Fac
e-to
-face
mee
ting g
oal-d
irect
ed m
edica
tion
and
lifes
tyle
coun
selin
g,
Had
a sta
ndar
d as
sess
men
t by
prim
ary
care
phy
sicia
n.
tele
phon
e ass
essm
ents
and
prov
ision
of o
ther
educ
atio
nal m
ater
ial
6 C
hoe H
M 20
0517
Ph
arm
acist
s pro
vide
d ev
alua
tion
and
mod
ifica
tion
of p
harm
acot
hera
py, K
ept a
s a n
atur
al co
ntro
l, th
ey re
ceiv
ed o
nly
regu
lar c
are
se
lf-m
anag
emen
t dia
bete
s edu
catio
n, an
d re
info
rcem
ent o
f dia
bete
s in
cludi
ng re
gula
r fol
low
up
visit
s with
thei
r prim
ary
care
co
mpl
icatio
ns sc
reen
ing p
roce
sses t
hrou
gh cl
inic
visits
and
telep
hone
follo
w-up
. phy
sicia
ns, r
ecei
ved
no sp
ecia
l con
tact
dur
ing
the
in
terv
entio
n, d
id n
ot h
ave e
xit i
nter
view
s or p
roce
ss
mea
sure
men
ts at
the e
nd o
f the
stud
y.
Tabl
e 2. D
etai
ls of
pha
rmac
ists
inte
rven
tion
and
usua
l car
e of e
ach
tria
l
-
23Effect of Pharmacists Interventions on Glycemic Control in Diabetic Patients: A Systematic Review and Meta-analysis of Randomized Controlled Trials
No.
St
udy
Phar
mac
ist in
terv
entio
n U
sual
care
7 O
dega
rd P
S 200
518
The p
harm
acist
inte
rven
tion
was
com
pose
d of
dev
elopm
ent o
f a
Patie
nts w
ere c
onstr
ucte
d to
cont
inue
nor
mal
care
di
abet
es ca
re p
lan
(DCP
), re
gula
r pha
rmac
ist-p
atie
nt co
mm
unic
atio
n on
with
thei
r prim
ary
care
pro
vide
r. D
iabe
tes e
duca
tion
di
abet
es ca
re p
rogr
ess,
phar
mac
ist-p
rovi
der c
omm
unica
tion
on th
e sub
jects
was
not
pro
vide
d du
ring t
he b
aseli
ne in
terv
iew to
avoi
d
diab
etes
care
pro
gres
s, an
d D
RP.
intro
ducin
g an
inter
vent
ion
for p
atien
ts in
the c
ontro
l gro
up.
8 S
ukso
mbo
on
Self-
effica
cy tr
aini
ng p
rogr
am b
y m
ultid
iscip
linar
y te
am in
cludi
ng
The c
ontro
l gro
up d
id n
ot en
ter p
erce
ived
self-
effica
cy
N
2005
19
phar
mac
ist, p
harm
acist
also
pro
vide
d ed
ucat
ion
on se
lf-ca
re b
ehav
iors
, tr
aini
ng p
rogr
am.
se
lf-m
onito
ring
of b
lood
glu
cose
, and
kno
wle
dge i
n di
abet
es.
9 S
uppa
pitip
orn
U
sual
care
plu
s dia
betic
dru
g co
unse
ling,
adde
d di
abet
es b
ookl
et, s
peci
al P
atie
nts w
ere i
nter
view
ed d
emog
raph
ic in
form
atio
n,
S
2005
20
med
icat
ion
cont
aine
rs.
bloo
d te
st, an
d m
edic
al re
cord
s. 1
0 Ro
thm
an
Inte
nsiv
e edu
catio
n se
ssio
ns, e
vide
nce-
base
d al
gorit
hm, p
roac
tive
Patie
nts r
ecei
ved
usua
l car
e fro
m th
eir p
rimar
y ca
re
RL
200
521
man
agem
ent.
prov
ider
and
had
no fu
rthe
r man
agem
ent f
rom
the
dise
ase m
anag
emen
t tea
m.
11
Forn
os
Usu
al ca
re p
lus p
harm
acot
hera
py fo
llow
up
prog
ram
(ind
ivid
ualiz
ed
Usu
al d
ispen
sing
by p
harm
acist
.
JA
200
6 22
pr
ogra
m) w
hich
cons
ists o
f the
det
ectio
n an
d re
solu
tion
of D
RPs
an
d di
abet
es ed
ucat
ion,
invo
lves
pat
ient
s in
thei
r ow
n ca
re in
ord
er to
obta
in m
axim
um b
enefi
t fro
m th
e med
icat
ion.
12
Scot
t Pa
tient
educ
atio
n ab
out d
iseas
e, te
sting
blo
od gl
ucos
e lev
els, d
rug t
hera
py,
Patie
nts r
ecei
ved
stand
ard
diab
etes
care
and
wer
e
D
M 2
0062
3 ps
ycho
logi
cal a
djus
tmen
t in
diab
etes
, sig
ns an
d sy
mpt
oms o
f hyp
er-
man
aged
by
a nur
se.
gl
ycem
ia, h
yper
glyc
emia
, and
dia
betic
ket
oaci
dosis
and
cour
se o
f act
ion.
13
Kras
s I 2
0072
4 Se
rvic
es fr
om p
harm
acist
s inc
lude
d of
revi
ew o
f self
mon
itorin
g of
Th
e con
trol p
atien
ts ha
d tw
o vi
sits w
ith th
e pha
rmac
ist,
bl
ood
gluc
ose;
dise
ase,
med
icat
ion,
and
lifes
tyle
educ
atio
n; ad
here
nce
one a
t the
beg
inni
ng an
d on
e at t
he en
d of
the s
tudy
.
supp
ort a
nd d
etec
tion
of d
rug-
rela
ted
prob
lem
s; an
d re
ferr
als t
o th
e D
urin
g the
inter
veni
ng 6
mon
ths,
they
rece
ived
usua
l car
e
patie
nts
GPs
whe
n ap
prop
riate
. (
i.e. n
o sp
ecia
lized
dia
bete
s ser
vice
in th
e pha
rmac
y).
14
Elno
ur
Ensu
red
that
inte
rven
tion
patie
nts r
ecei
ved
base
d tre
atm
ent a
nd
Patie
nts r
ecei
ved
trad
ition
al ca
re: m
onth
ly cl
inic
visi
ts
A
A 2
0082
5 tre
atm
ent f
or an
y ot
her c
onco
mita
nt il
lnes
s, ed
ucat
ed o
n G
DM
an
d se
lf-m
onito
ring
of p
lasm
a glu
cose
usin
g di
ary
card
s.
and
its m
anag
emen
t, ed
ucat
iona
l boo
klet
, Clin
ical
asse
ssm
ents.
Tabl
e 2. D
etai
ls of
pha
rmac
ists
inte
rven
tion
and
usua
l car
e of e
ach
tria
l (co
nt.)
-
N. Poolsup et al.24
No.
St
udy
Phar
mac
ist in
terv
entio
n U
sual
care
15
Phum
ipam
orn
U
sual
care
plu
s rem
inde
d th
e pat
ient
s, re
fille
d pr
escr
iptio
ns,
Patie
nts r
ecei
ved
usua
l sch
edul
e car
e by
prim
ary
care
S 20
0826
di
scus
sed
the u
ses o
f med
icat
ion,
chec
k th
e pill
coun
t, ed
ucat
ion
on
phys
icia
n ev
ery
4-8
wee
ks.,
disp
ensin
g by
pha
rmac
ist
diab
etes
abou
t app
ropr
iate l
ifesty
le, co
rrec
t diet
, and
pro
vide
d di
abet
ic fil
led
and
gave
gen
eral
advi
ce o
n m
edic
atio
n us
es o
ver
pa
mph
let; d
iabe
tic co
mpl
icat
ions
, tar
get o
f tre
atin
g di
abet
es, l
ife st
yle
the d
ispen
sary
coun
ter o
n a r
outin
e bas
is.
chan
ge, a
nd d
iabe
tic m
edic
atio
ns.
16
Pava
sudt
hipa
isit
Inte
rven
tion
grou
p re
ceiv
ed in
tens
ive m
anag
emen
t fro
m p
harm
acist
Pa
tient
s wer
e pro
vide
d ca
re b
y the
ir ph
ysici
ans o
f int
erns
.
A
200
927
prac
titio
ners
; rec
eived
an as
sess
men
t of m
edica
tion-
taki
ng ad
here
nce
an
d th
eir u
nder
stand
ing
of d
iabe
tes t
hen
appl
ied
algo
rithm
s for
m
anag
ing
gluc
ose c
ontro
l and
oth
er ca
rdio
vasc
ular
risk
fact
ors.
17
Dou
cette
D
iscus
sing m
edica
tions
, clin
ical g
oals,
self-
care
activ
ities
with
pat
ients
Patie
nts r
ecei
ved
usua
l dia
bete
s car
e fro
m th
eir p
rimar
y
W
R 20
0928
an
d re
com
men
ding
med
icatio
n ch
ange
s to
phys
ician
s whe
n ap
prop
riate
. ca
re p
rovi
der.
18
Maz
roui
Th
e res
earc
h ph
arm
acist
had
disc
ussio
ns w
ith th
eir p
hysic
ians r
egar
ding
Pa
tient
s rec
eive
d no
rmal
care
from
med
ical
and
nurs
ing
NRA
200
929
drug
ther
apy,
treat
men
t mod
ifica
tion,
educ
ated
for i
llnes
s and
sta
ff, d
id n
ot re
ceiv
e the
clin
ical
pha
rmac
y se
rvic
e.
med
icat
ion,
prin
ted
leafl
et, a
nd b
ehav
iora
l mod
ifica
tion.
19
Tave
ira
Usu
al ca
re p
lus t
reat
men
t of h
yper
glyc
emia
, hyp
erte
nsio
n,
Patie
nts r
ecei
ved
the s
tand
ard
care
pro
vide
d by
prim
ary
TH 2
0103
0 hy
perli
pide
mia
, and
ciga
rette
smok
ing.
ca
re p
rovi
ders
, fre
quen
cy av
erag
e 4 m
onth
s. 2
0 Ed
elman
Ph
arm
acist
revi
ewed
pat
ient
med
ical
reco
rds,
BP, a
nd h
ome b
lood
Pa
tient
s con
tinue
d to
rece
ive t
heir
usua
l prim
ary
care
,
D
201
031
gluc
ose r
eadi
ngs d
urin
g ea
ch se
ssio
n an
d de
velo
ped
indi
vidu
aliz
ed
no ac
tive i
nter
vent
ion.
pl
ans f
or m
edica
tion
or li
festy
le m
anag
emen
t. Ph
arm
acist
and
phys
ician
adju
sted
med
icat
ion
to m
anag
e eac
h pa
tient
HbA
1c le
vel a
nd B
P. 2
1 M
ehuy
s Ed
ucat
ion
abou
t T2D
M an
d co
mpl
icat
ions
, cor
rect
use
of o
ral
Patie
nts r
ecei
ved
usua
l pha
rmac
ist ca
re.
E 20
1132
hy
pogl
ycae
mic
agen
ts, fa
cilit
atio
n of
med
icat
ion
adhe
renc
e, he
alth
y
lifes
tyle
educ
atio
n, an
d re
min
ders
abou
t ann
ual e
ye an
d fo
ot
exam
inat
ions
. 2
2 Sr
iram
S 2
0113
3 Pa
tient
s rec
eived
pha
rmac
eutic
al ca
re; m
edica
tion
coun
selin
g ins
truct
ions
Pat
ient
s rec
eive
d us
ual d
iabe
tes c
are.
on
die
tary
regu
latio
n, ex
erci
se an
d ot
her l
ifesty
le m
odifi
catio
n.
Tabl
e 2. D
etai
ls of
pha
rmac
ists
inte
rven
tion
and
usua
l car
e of e
ach
tria
l (co
nt.)
-
25Effect of Pharmacists Interventions on Glycemic Control in Diabetic Patients: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Effect on HbA1c
Twenty two trials involving a total of 2,808 diabetes patients were pooled. HbA1c levels at baseline, final assessment are presented in Table 4. HbA1c levels were significantly reduced with pharmacists interventions
compared with usual care. The pooled mean difference in the change of HbA1c was -0.68% (95%CI, -0.87% to -0.49%; p< 0.00001) (Figure 2). No publication bias was detected (Egger bias -0.35; 95% CI -2.89 to 2.19, P= 0.7785).
Table 3. Component of pharmacists intervention in individual trials
Education Identifying and Study Materials provided and counseling resolving drug- related problems
Jaber LA 199612 - Guirguis LM 200113 glucose meter maintenance - Clifford RM 200214 - Sarkadi A 200415 video, booklet Clifford RM 200516 educational material Choe HM 200517 - Odegard PS 200518 - - Suksomboon N 200519 - - Suppapitiporn S 200520 booklet, containers - Rothman RL 200521 - - Fornos JA 200622 - Scott DM 200623 - Krass I 200724 monthly newsletter Elnour AA 200825 booklet Phumipamorn S 200826 pamphlet Pavasudthipaisit A 200927 - Doucette WR 200928 - Mazroui NRA 200929 leaflet - Taveira TH 201030 smoking cessation handout - Edelman D 201031 - Mehuys E 201132 educational material -
Sriram S 201133 leaflet, diabetic diet chart, diabetic diary
-
N. Poolsup et al.26
HbA1c (%)
Study Control Intervention
Baseline Final Baseline Final
Jaber LA 199612 11.52.9 12.13.3 12.23.5 9.22.1 Guirguis LM 200113 7.9* 7.1* 7.9* 6.9* Clifford RM 200214 8.51.6 8.11.6 8.41.4 8.21.5 Sarkadi A 200415 6.44* 6.60* 6.44* 6.09* Clifford RM 200516 7.1* 6.7* 7.5* 7.3* Choe HM 200517 10.21.7 9.32.1 10.11.8 8.01.4 Odegard PS 200518 10.61.4 9.2* 10.20.8 8.7* Suksomboon N 200519 9.731.88 10.232.59 9.031.67 8.691.82 Suppapitiporn S 200520 8.011.51 8.801.36 8.161.44 7.911.27 Rothman RL 200521 112 9.4* 113 8.5* Fornos JA 200622 7.81.7 8.51.9 8.41.8 7.91.7 Scott DM 200623 8.7* 8.0* 8.8* 7.08* Krass I 200724 8.31.3 8.01.2 8.91.4 7.91.2 Elnour AA 200825 6.87 6.55 6.85 6.38 (95%CI (95%CI (95%CI (95%CI 6.81, 6.93) 6.43, 6.67) 6.78, 6.90) 6.33, 6.42) Phumipamorn S 200826 8.71.6 8.11.9 8.71.5 7.91.4 Pavasudthipaisit A 201127 9.91.6 9.1* 9.81.4 7.8* Doucette WR 200928 7.911.91 8.03* 7.991.45 7.72* Mazroui NRA 200929 8.4 8.3 8.5 6.9 (95%CI (95%CI (95%CI (95%CI 8.6, 8.6) 8.1, 8.5) 8.3, 8.7) 6.7, 7.1) Taveira TH 201030 7.91.1 7.9* 8.11.5 7.2* Edelman D 201031 9.21.3 8.6* 9.21.5 8.3* Mehuys E 201132 7.3 1.2 7.2 1.0 7.7 1.7 7.1 1.1 Sriram S 201133 9.03 0.46 8.31 0.16 8.44 0.29 6.73 0.21
Data are meanSD, * mean value
Table 4. HbA1c levels at baseline and final assessment reported in individual trials
-
27Effect of Pharmacists Interventions on Glycemic Control in Diabetic Patients: A Systematic Review and Meta-analysis of Randomized Controlled Trials
DISCUSSION
Pharmacist is part of a multidiscip-linary team. This team normally consists of pharmacist, physician, nurse, technician, nutritionist, and other health care professions. All of the members in multidisciplinary team have important roles in diabetes management in achieving the goal of treatment, improving quality of life, controlling disease and its complications, delaying complication, and decreasing mortality and morbidity. Pharma-cists interventions are an important factor to improve glycemic control in diabetic patients. Pharmacists interventions include diabetes education and counseling on drug, disease, diet, exercise, life style modification, and self-management, assessment and adjustment of anti-diabetic medications, identifying and solving drug-related problems, co-operation with physician and other diabetes health care team, providing materials that reinforce patients to achieve a target goal, providing additional information on smoking cessation. All of these interventions aimed at improving glycemic control. In our study, HbA1c levels significantly reduced with pharmacists interventions compared with usual care. The pooled mean
difference in the change of HbA1c was -0.68% (95%CI, -0.87% to -0.49%; p< 0.00001). This reduction is the same as the ability in reducing HbA1c by taking some oral anti-hyperglycemic drugs for example, DPP-4 inhibitors and alpha-glucosidase inhibitors. This would help patients meeting the target of their treatment. To ensure that the meta-analysis included quality study, the Maastricht Amsterdam scale was used to assess the quality of individual study. The majority of the studies12-13, 15-20, 22-31,33 were rated as low quality, only three studies14, 21, 32 were of high quality. Most of these studies were open (not blinded) in study design. Performance bias in both intervention and control groups was likely in these trials as patients may seek other interventions to help control their blood glucose. This was evident when only high quality studies14, 21, 32 were pooled, showing a slight reduction in the effect of pharmacists interventions on HbA1c (mean difference -0.39%, 95% CI -0.61% to -0.17%, p = 0.0005). There were limitations in individual studies included in this meta-analysis. In most of the trials, both pharmacists and patients were not blinded and therefore,
Figure 2. Mean difference (95% confidence interval) of HbA1c between pharmacist intervention group and usual care group
-
N. Poolsup et al.28
contamination between groups was possible. This may affect the final outcomes. Secondly, Hawthorne effect may occur when study participants improved because of the only fact that they were participating in a research study. The findings of our study suggest several practice implications. First, pharma-cists interventions effectively improve glycemic control when compared with usual care; and thus, pharmacist should be part of a diabetes care team. Second, the approprite components of intervention should include both pharmacotherapy and non-pharmaco-therapy. Interventions on pharmacotherapy are screening and solving drug-related problems; if necessary, pharmacists provide feedback to physician, deliver patient education and counseling on medication. Non-pharmacotherapy interventions include education and counseling on diet, exercise, disease, adherence, and life-style modification.
CONCLUSION The available evidence suggests that pharmacists interventions are more effective than usual care in decreasing HbA1c levels in diabetes patients. Pharmacists interventions included diabetes education and counseling on drug, disease, diet, exercise, life style modification, and self-management, an assessment and adjustment of anti-diabetic medications, identifying and solving drug-related problems, co-operation with physician and other diabetes health care team.
REFERENCES 1. American Diabetes Association. Standards of medical care in diabetes 2010. Diabetes Care 2010;33(1):S11 61. 2. Glasgow RE, Peeples M, Skovlund SE. Where is the patient in diabetes performance measures? The case for including patient-centered and self- management measures. Diabetes Care 2008;31:104650.
3. American Society of Health-System Pharmacists. ASHP statement on the pharmacists role in primary care. Am J Health-Syst Pharm 1999;56:1665-7. 4. Sisson E, Kuhn C. Pharmacist roles in the management of patients with type 2 diabetes. J Am Pharm Assoc 2009;49(1):S415. 5. Norris SL, Nichols PJ, Caspersen CJ, et al. The effectiveness of disease and case management for people with diabetes: a systematic review. Am J Prev Med 2002;22(4):1538. 6. van Tulder M, Furlan A, Bombardier C, et al. Updated method guidelines for systematic reviews in the Cochrane collaboration back review group. Spine 2003; 28(12):1209-9. 7. Higgins JPT, Deeks JJ. Selecting studies and collecting data. In: Higgins JPT, Green S, editors. Cochrane handbook for systematic reviews of interventions. United Kingdom: John Wiley & Sons, 2009;174-5. 8. Whitehead A, Whitehead J. A general parametric approach to the meta- analysis of randomized clinical trials. Stat Med 1991;10(11):1665-77. 9. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7(3):177-88. 10. Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta- analyses. BMJ 2003;327:55760. 11. Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 2003; 327(7414):557-60.12. Jaber LA, Halapy H, Fernet M, et al. Evaluation of a pharmaceutical care model on diabetes management. Ann Pharmacother 1996;3(3):238-43.13. Guirguis LM, Johnson JA, Farris KB, et al. A pilot study to evaluate the impact of pharmacists as certified diabetes educators on the clinical and humanistic outcomes of people with diabetes. Can J Diabetes 2001;25(4):266-76.
-
29Effect of Pharmacists Interventions on Glycemic Control in Diabetic Patients: A Systematic Review and Meta-analysis of Randomized Controlled Trials
14. Clifford RM, Batty KT, Davis TME, et al. A randomized controlled trial of a pharmaceutical care programme in high-risk diabetic patients in an out- patient clinic. Int J Pharm Pract 2002; 10:85-9.15. Sarkadi A, Rosenqvist U. Experience- based group education in Type 2 diabetes: a randomised controlled trial. Patient Educ Couns 2004;53:291-8.16. Clifford RM, Batty KT, Davis WA, et al. Effect of a pharmaceutical care program on vascular risk factors in type 2 diabetes. Diabetes Care 2005;28:77 1-6.17. Choe HM, Mitrovich S, Dubay D, et al. Proactive case management of high- risk patients with type 2 diabetes mellitus by a clinical pharmacist: a randomized controlled trial. Am J Manag Care 2005; 11:253-60. 18. Odegard PS, Goo A, Hummel J, et al. Caring for poorly controlled diabetes mellitus: a randomized pharmacist intervention. Ann Pharmacother 2005; 39:433-40. 19. Suksomboon N, Luckanajantachote P, Poolsup N, et al. Effects of training programme on perceived self-efficacy, self-care behavior and diabetes know- ledge among type 2 diabetics. SWU J Pharm Sci 2005;10(2):145-53. 20. Suppapitiporn S, Chindavijak B, Onsanit S. Effect of diabetes drug counseling by pharmacist, diabetic disease booklet and special medication containers on glycemic control of type 2 diabetes mellitus: a randomized controlled trial. J Med Assoc Thai 2005;88(4):S134-41. 21. Rothman RL, Malone R, Bryant B, et al. A randomized trial of a primary care- based disease management program to improve cardiovascular risk factors and glycated hemoglobin levels in patients with diabetes. Am J Med 2005;118:276- 83. 22. Fornos JA, Andres NF, Andres JC, et al. A pharmacotherapy follow-up program
in patients with type-2 diabetes in community pharmacies in Spain. Pharm World Sci 2006;28:65-72. 23. Scott DM, Boyd ST, Stephan M, et al. Outcomes of pharmacist-managed diabetes care services in a community health center. Am J Health-Syst Pharm 2006;63:2116-22. 24. Krass I, Armour CL, Mitchell B, et al. The Pharmacy Diabetes Care Program: assessment of a community pharmacy diabetes service model in Australia. Diabet Med 2007;24:67783. 25. Elnour AA, Mugammar ITE, Jaber T, et al. Pharmaceutical care of patients with gestational diabetes mellitus. J Eval Clin Pract 2008;14:131-40. 26. Phumipamorn S, Pongwecharak J, Soorapan S, et al. Effects of the pharma- cists input on glycaemic control and cardiovascular risks in Muslim diabetes. Prim Care Diabetes 2008;2:31-7. 27. Pavasudthipaisit A, Awiphan R, Niwata- nanan K, et al. A randomized trial of a pharmacist practitioner model to improve glycemic control in type 2 diabetic patients. Faculty of Pharmacy, Chiang Mai University 2009. 28. Doucette WR, Witry MJ, Farris KB, et al. Community pharmacist-provided extended diabetes care. Ann Pharmacother 2009;4:882-9. 29. Mazroui NRA, Kamal MM, Ghabash NM, et al. Influence of pharmaceutical care on health outcomes in patients with type 2 diabetes mellitus. Br J Clin Pharmacol 2009;67(5):547-57. 30. Taveira TH, Friedmann PD, Cohen LB, et al. Pharmacist-led group medical in type 2 diabetes. Diabetes Educ 2010: 36(1):109-17. 31. Edelman D, Fredrickson SK, Melnyk SD, et al. Medical clinics versus usual care for patients with both diabetes and hypertension. Ann Intern Med 2010;152: 689-96. 32. Mehuys E, Bortel LV, Bolle LD, et al. Effectiveness of a community pharmacist
-
N. Poolsup et al.30
intervention in diabetes care: a randomized controlled trial. J Clin Pharm Ther 2011; 36:602-13. 33. Sriram S, Chack LN, Ramasamy R,
et al. Impact of pharmaceutical care on quality of life in patients with type 2 diabetes mellitus. JRMS 2011;16(Special Issue):412-8.