
2010 - University of Auckland
140
Antenatal Magnesium Sulphate Prior to Preterm Birth for Neuroprotecon of the Fetus, Infant and Child Antenatal Magnesium Sulphate Prior to Preterm Birth for Neuroprotecon of the Fetus, Infant and Child Prepared by the Antenatal Magnesium Sulphate For Neuroprotecon Guideline Development Panel 2010 N a o n a l C li n i c a l Pr a c ce G u i d e l i n e s
Transcript of 2010 - University of Auckland

Antenatal Magnesium SulphatePrior to Preterm Birth for Neuroprotection
of the Fetus, Infant and Child
Antenatal M
agnesium Sulphate Prior to Preterm
Birth for Neuroprotection of the Fetus, Infant and Child
Prepared by the
Antenatal Magnesium Sulphate
For Neuroprotection
Guideline Development Panel
2010
Nati onal Clinical Practi ce Guidelines

©AustralianResearchCentreforHealthofWomenandBabies,TheUniversityofAdelaide2010
Printeddocument
Thisworkiscopyright.ApartfromanyuseaspermittedundertheCopyrightAct1968,nopartmay
bereproducedbyanyprocesswithoutpriorwrittenpermissionfromtheAustralianResearchCentre
forHealthofWomenandBabies,TheUniversityofAdelaide.Requestsandinquiriesconcerning
reproductionandrightsshouldbeaddressedtoARCH,DisciplineofObstetricsandGynaecology,
Women’sandChildren’sHospitalAdelaide,72KingWilliamRoad,NorthAdelaide,SA,5006.
ISBNPrint:978‐0‐86396‐720‐7
Electronicdocument
Thisworkiscopyright.Youmaydownload,display,printandreproducethismaterialinunaltered
formonly(retainingthisnotice)foryourpersonal,non‐commercialuseorusewithinyour
organisation.ApartfromanyuseaspermittedundertheCopyrightAct1968,allotherrightsare
emailed,reserved.Requestsandinquiriesconcerningreproductionandrightsshouldbeto [email protected]
ISBNPrint:978‐0‐86396‐720‐7
Forfurtherinformation:
Web:www.auckland.ac.nz/en/liggins/our-research/research-themes/healthy-mothers-healthy-babies/research-synthesis.html
Email:[email protected]
Suggestedcitation:
TheAntenatalMagnesiumSulphateforNeuroprotectionGuidelineDevelopmentPanel.Antenatal
magnesiumsulphatepriortopretermbirthforneuroprotectionofthefetus,infantandchild:
Nationalclinicalpracticeguidelines.Adelaide:TheUniversityofAdelaide,2010.
Disclaimer
Theseguidelinesareageneralguidetoappropriatepracticetobeusedsubjecttothehealth
practitioner’sclinicaljudgementandtheindividualwoman’spreference.Thedocumentisdesigned
togiveinformationtoassistclinicaldecision‐makingandisbasedonthebestavailableevidenceat
thetimeofrelease.
PublicationApproval
TheseguidelineswereapprovedbytheChiefExecutiveOfficeroftheNationalHealthandMedical
ResearchCouncil(NHMRC)on17November2010underSection14AoftheNationalHealthand
MedicalResearchCouncilAct1992.InapprovingtheseguidelinestheNHMRCconsidersthatthey
meettheNHMRCstandardforclinicalpracticeguidelinesinthattheyarebasedonthesystematic
identificationandsynthesisofthebestavailablescientificevidenceandmakeclear
recommendationsforhealthprofessionalspractisinginanAustralianhealthcaresetting.The
NHMRCexpectsthatallguidelineswillbereviewednolessthanonceeveryfiveyears.
ThispublicationreflectstheviewsoftheauthorsandnotnecessarilytheviewsoftheAustralianGovernment.
©AustralianResearchCentreforHealthofWomenandBabies,TheUniversityofAdelaide2010
Printeddocument
Thisworkiscopyright.ApartfromanyuseaspermittedundertheCopyrightAct1968,nopartmay
bereproducedbyanyprocesswithoutpriorwrittenpermissionfromtheAustralianResearchCentre
forHealthofWomenandBabies,TheUniversityofAdelaide.Requestsandinquiriesconcerning
reproductionandrightsshouldbeaddressedtoARCH,DisciplineofObstetricsandGynaecology,
Women’sandChildren’sHospitalAdelaide,72KingWilliamRoad,NorthAdelaide,SA,5006.
ISBNPrint:978‐0‐86396‐720‐7
Electronicdocument
Thisworkiscopyright.Youmaydownload,display,printandreproducethismaterialinunaltered
formonly(retainingthisnotice)foryourpersonal,non‐commercialuseorusewithinyour
organisation.ApartfromanyuseaspermittedundertheCopyrightAct1968,allotherrightsare
reserved.RequestsandinquiriesconcerningreproductionandrightsshouldbeaddressedtoARCH,
DisciplineofObstetricsandGynaecology,Women’sandChildren’sHospitalAdelaide,72King
WilliamRoad,NorthAdelaide,SA,5006.
ISBNPrint:978‐0‐86396‐720‐7
Forfurtherinformation:
Web:www.adelaide.edu.au/arch
Email:[email protected]
Suggestedcitation:
TheAntenatalMagnesiumSulphateforNeuroprotectionGuidelineDevelopmentPanel.Antenatal
magnesiumsulphatepriortopretermbirthforneuroprotectionofthefetus,infantandchild:
Nationalclinicalpracticeguidelines.Adelaide:TheUniversityofAdelaide,2010.
Disclaimer
Theseguidelinesareageneralguidetoappropriatepracticetobeusedsubjecttothehealth
practitioner’sclinicaljudgementandtheindividualwoman’spreference.Thedocumentisdesigned
togiveinformationtoassistclinicaldecision‐makingandisbasedonthebestavailableevidenceat
thetimeofrelease.
PublicationApproval
TheseguidelineswereapprovedbytheChiefExecutiveOfficeroftheNationalHealthandMedical
ResearchCouncil(NHMRC)on17November2010underSection14AoftheNationalHealthand
MedicalResearchCouncilAct1992.InapprovingtheseguidelinestheNHMRCconsidersthatthey
meettheNHMRCstandardforclinicalpracticeguidelinesinthattheyarebasedonthesystematic
identificationandsynthesisofthebestavailablescientificevidenceandmakeclear
recommendationsforhealthprofessionalspractisinginanAustralianhealthcaresetting.The
NHMRCexpectsthatallguidelineswillbereviewednolessthanonceeveryfiveyears.
ThispublicationreflectstheviewsoftheauthorsandnotnecessarilytheviewsoftheAustralianGovernment.

CONTENTS
Abbreviations .......................................................................................................................................... 1
Glossary of Terms.................................................................................................................................... 2
Guideline Panel Membership ................................................................................................................. 6
Summary of Clinical Recommendations, Good Practice Points, Implementation Implications and
Research Recommendations .................................................................................................................. 8
Clinical Recommendations .................................................................................................................. 8
Good Practice Points ........................................................................................................................... 8
Implementation Implications ............................................................................................................ 10
Research Recommendations ............................................................................................................ 12
Chapter 1: Need for these Guidelines................................................................................................... 14
Chapter 2: Summary of Guideline Development Process..................................................................... 16
Chapter 3: Background ......................................................................................................................... 17
Chapter 4: Improving Health Outcomes for the Fetus, Infant, and Child (Question 1) ........................ 20
Chapter 5: Adverse Outcomes for the Women (Question 2) ............................................................... 22
Chapter 6: Adverse Outcomes for Fetus, Infant, and Child (Question 3) ............................................. 23
Chapter 7: Summary of Evidence for Questions 1-3 ............................................................................. 24
Chapter 8: Gestational Age (Question 4) .............................................................................................. 26
Chapter 9: Timing (Question 5) ............................................................................................................. 28
Chapter 10: Regimens (Question 6) ...................................................................................................... 31
Chapter 11: Number of Babies in Utero (Question 7) .......................................................................... 36
Chapter 12: Reasons Women (at less than 30 weeks gestation) Considered at Risk of Preterm Birth
(Question 8) .......................................................................................................................................... 38
Chapter 13: Parity (Question 9) ............................................................................................................ 39
Chapter 14: Mode of Birth (Question 10) ............................................................................................. 40
Chapter 15: Effect of Antenatal Corticosteroids (Question 11) ............................................................ 42
References ............................................................................................................................................ 43
References to included RCTs ............................................................................................................. 43
Other References .............................................................................................................................. 46
Appendix A: Process and Methods ....................................................................................................... 50
Appendix B: How to use the NHMRC Evidence Statement Form ......................................................... 54
Appendix C: NHMRC Evidence Statement Form ................................................................................... 56
Appendix D: New Zealand Processes .................................................................................................... 60

Appendix E: Tocolysis Intent and Maternal Neuroprotective Intent .................................................... 61
Q1-Q3: Effectiveness Summary for Cochrane Reviews .................................................................... 63
Appendix F: Evidence Statements and Tables – Questions 1 to 11 ...................................................... 65
Q1 – Q3: Effectiveness Summary For Cochrane Reviews ................................................................. 65
Q4: Gestational Age .......................................................................................................................... 71
Q5: Time Magnesium Sulphate Planned To Be Given Prior To Preterm Birth .................................. 86
Q6: Regimens .................................................................................................................................... 95
Q7: Number of babies in utero ....................................................................................................... 104
Q8: Reason for treatment ............................................................................................................... 109
Q9: Parity Of Women ...................................................................................................................... 111
Q10: Mode Of Birth ......................................................................................................................... 113
Q11: Combined Effect Of Antenatal Corticosteroids ...................................................................... 116
Appendix G: Harms – Maternal; and Fetus, Infant, and Child ............................................................ 120
Maternal Harms .............................................................................................................................. 120
Fetus, Infant and Child .................................................................................................................... 122
Appendix H: Additional Information about Regimens and Monitoring for giving Magnesium Sulphate
to Prevent Eclampsia from Clinical Practice Guidelines and Management Protocols ........................ 124
Appendix I: Public consultation comments and Panel responses ...................................................... 134

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 1
Abbreviations
ACMI Australian College of Midwives Inc.
ACNN Australian College of Neonatal Nurses
ACP Australian College of Pharmacy
ARCH Australian Research Centre for Health of Women and Babies, The University of Adelaide
BP Blood pressure
CI Confidence interval
DNA Deoxyribonucleic acid
g Gram/s
IPD Individual patient data
IQR Interquartile range
IV Intravenous
IVH Intraventricular haemorrhage
MgSO4 Magnesium sulphate
mL Millilitre
mm Hg Millimetres of mercury
mmol/L Millimoles per litre
NHMRC National Health and Medical Research Council
NNTB Number needed to treat to benefit
NZCOM New Zealand College of Midwives
NZGG New Zealand Guidelines Group
PPROM Preterm prelabour rupture of the membranes
RANZCOG Royal Australian and New Zealand College of Obstetrics and Gynaecology
RCNA Royal College of Nursing, Australia
RCOG Royal College of Obstetricians and Gynaecologists
RCPA Royal College of Pathologists Australasia
RCT Randomised controlled trial
RNA Ribonucleic acid
RR Risk ratio
SOGC Society of Obstetricians and Gynaecologists of Canada
SOMANZ Society of Obstetric Medicine of Australia and New Zealand
soln Solution
US United States
WHA Women’s Hospitals Australasia
WHO World Health Organization

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 2
Glossary of Terms
Adverse event An adverse outcome that occurs during or after the use of a drug or other intervention but is not necessarily caused by it.
Antenatal Occurring before birth; concerned with the care and treatment of the unborn child and pregnant women.
Antenatal corticosteroids Betamethasone and dexamethasone are corticosteroids, also called glucocorticoids, given before birth (antenatally) to improve lung development and function in the fetus at risk of preterm birth.
Antepartum haemorrhage Bleeding from the vagina during pregnancy from 20 weeks’ gestation to birth.
Applicability The degree to which a body of evidence is relevant to a particular health care context.
Arm (of a clinical study) Group of individuals within a study who are allocated to one particular intervention, for example the placebo arm.
Bias Systematic (as opposed to random) – deviation of the results of a study from the ‘true’ results.
Biological plausibility A method of reasoning to suggest a causal association between a biologic factor and a particular disease or health outcome.
Bolus A large dose of a drug given by injection for the purpose of rapidly achieving the needed therapeutic concentration in the bloodstream.
Calcium channel A structure in the body which allows cells to transmit electrical charges to each other. These charges are carried on a calcium ion which can travel freely back and forth through the calcium channel.
Case-control study A study that compares people with a specific disease or outcome of interest (cases) to people from the same population without that disease or outcome (controls), and which seeks to find associations between the outcome and prior exposure to particular risk factors. This design is particularly useful where the outcome is rare and past exposure can be reliably measured. Case-control studies are usually retrospective.
Cerebral palsy Cerebral palsy describes a group of permanent disorders of the development of movement and posture, causing activity limitation, that are attributed to nonprogressive disturbances that occurred in the developing fetal or infant brain. The motor disorders of cerebral palsy are often accompanied by disturbances of sensation, perception, cognition, communication, and behaviour, by epilepsy, and by secondary musculoskeletal problems.
Clinical impact Measure of potential benefit from application of the guideline to a population.
Cochrane Library A regularly updated electronic collection of evidence-based healthcare databases, including the Cochrane Database of Systematic Reviews.
Cochrane Review/Cochrane Systematic Review
A systematic review of the evidence usually from randomised controlled trials relating to a particular health problem or healthcare intervention, produced by the Cochrane Collaboration. Available electronically as part of the Cochrane Library.
Cognitive dysfunction Poor mental function, such as, difficulties with lack of attention, memory and problem solving.
Confidence interval Gives a range of values for an unknown population outcome estimated from a study. It will depend on the number of study recruits and the variation in the outcome data. A 95% confidence interval (CI) means that if the study was repeated 100 times with a different sample of recruits and a CI calculated each time, the interval would contain

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 3
the ‘true’ value of the population outcome 95 times.
Controls A group of patients recruited into a study that receives no treatment, a treatment of known effect, or a placebo (dummy treatment) – in order to provide a comparison for a group receiving an experimental treatment, such as a new drug.
Deoxyribonucleic Acid The molecules inside cells that carry genetic information and pass it from one generation to the next.
Developmental delay Any significant lag in a child's physical, cognitive, behavioural, emotional, or social development, in comparison with norms.
Eclampsia Seizures (convulsions) in a pregnant woman related to hypertensive disease in pregnancy.
Evidence-based The best available evidence gained from the scientific method to inform medical decision making. It seeks to assess the quality of evidence of the risks and benefits of treatments (including lack of treatment).
Evidence statement A table summarising the results of a collection of studies which, taken together, represent the evidence supporting a particular recommendation or series of recommendations in a guideline.
Fetal Of or pertaining to a fetus or to the period of its development.
Fetal compromise The fetus not being well.
Fetus The unborn young.
Gestational age The period of time between last menstrual period and birth.
Glutamate A neurotransmitter normally involved in learning and memory. It also is an excitatory neurotransmitter, which means it stimulates areas in the brain or other parts of the nervous system.
Harms Adverse effects.
Higher order More than two fetuses in the womb.
Hypermagnesaemia An abnormally elevated concentration of magnesium in the blood.
Hyporeflexia The condition of below normal or absent reflexes.
Hypotension Abnormally low blood pressure.
Hypotonia A condition of low muscle tone (the amount of tension or resistance to movement in a muscle), often involving reduced muscle strength.
Individual patient data The central collection, validation and re-analysis of ‘raw’ data from existing trials addressing the same research question to allow further exploration of patient factors or groups that are more or less likely to benefit from treatment.
Intellectual impairment A condition where powers of comprehension and information processing abilities are affected to the point where it impairs the person’s ability to perform.
Interquartile range Difference between the first quartile (25th percentile) and the third quartile (75th percentile) of an ordered range of data.
Intraventricular haemorrhage
Bleeding inside or around the ventricles, the spaces in the brain containing the cerebrospinal fluid. Intraventricular haemorrhage can be graded based on the severity of the haemorrhage. Grades 3 and 4 represent more severe haemorrhage causing ventriculomegaly or venous infarction of the brain respectively and are more likely to be associated with neurologic disability.
In utero Within the uterus.
Loading dose One or a series of doses that may be given at the onset of therapy with the aim of achieving the target concentration rapidly.
Maternal neuroprotective intent
Magnesium sulphate given to a pregnant woman with the intention of preventing eclampsia.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 4
Mechanical ventilation To mechanically assist or replace spontaneous breathing.
Necrotising enterocolitis A medical condition primarily seen in premature infants, where portions of the bowel undergo tissue death (necrosis).
Neonatal Pertaining to the newborn period which is the first four weeks after birth.
Neonate An infant in the first 4 weeks of life.
Neurologic impairment A group of disorders that relate to the central nervous system (brain and spinal cord). Among the more common diagnostic categories for children are cerebral palsy, epilepsy, blindness, deafness and developmental delay. A neurological impairment may affect an individual’s speech, motor skills, vision, memory, hearing, muscle actions and learning abilities.
Neurons Primary, impulse conducting cells of the nervous system; nerve cells.
Neuroprotection A therapeutic strategy aimed at protecting neurons from injury or degeneration.
Neuroprotective intent Magnesium sulphate given to women at risk of preterm birth helps to protect the baby’s brain and improve long-term outcomes.
Nifedipine Vasodilator agent (calcium channel blocker).
Number needed to treat to benefit
The number of patients who need to be treated with the new or intervention treatment (rather than the control treatment) for one patient to benefit from the new treatment.
Observational studies A study in which the investigators do not seek to intervene, and simply observe the course of events. Changes or differences in one characteristic (e.g. whether or not people received the intervention of interest) are studied in relation to changes or differences in other characteristic(s) (e.g. whether or not they died), without action by the investigator. There is a greater risk of selection bias than in experimental studies.
Odds In a simple situations the odds of an outcome are given by the number with the outcome divided by the number without the outcome.
Odds ratio The odds of the outcome in the intervention group to the odds of an outcome in the control group.
Oxidative phosphorylation The process during which nutrients are broken down into ATP (adenosine triphosphate) using the oxygen we breathe.
Parity The number of times a women has given birth to a fetus with a gestational age of 20 weeks or more, regardless of whether the child was born alive or was stillborn.
Peripheral vasodilator Medicines that act directly on muscles in blood vessel walls to make blood vessels widen (dilate).
Periventricular leukomalacia
A form of brain injury characterised by the death of white matter near the cerebral ventricles in newborns due to damage and softening of the brain tissue.
Placebo An inactive substance or preparation used as a control in an experiment or test to determine the effectiveness of a medicinal drug.
Plasma membrane integrity Integrity of body cell walls.
Post hypoxic brain injury Damage to the brain that impairs normal functions due to lack of oxygen.
Pre-eclampsia A pregnancy-induced condition, which can occur in the second half of pregnancy. It is characterised by high blood pressure, swelling that happens suddenly along with rapid weight gain due to fluid retention, and protein in the urine.
Preterm birth The birth of a baby of less than 37 weeks’ gestational age.
Preterm labour Labour before 37 weeks’ gestation.
Protein synthesis The process by which the genetic code puts together proteins in the cell.
p-value Used in hypothesis testing where initially it is assumed that there is no difference between two treatments. The p-value is the probability that the difference observed

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 5
in a study between the two treatments might have occurred by chance. Small p-values indicate evidence against an assumption of no difference. Large p-values indicate insufficient evidence against the assumption of no difference between treatments NOT that there is actually no difference between the treatments. P-values will depend on study size; large studies can detect small differences for instance.
Randomised controlled trial
A comparative study in which participants are randomly allocated to intervention and control groups and followed up to examine differences in outcomes between the groups.
Reduction in risk The extent to which a treatment reduces a risk of an outcome, in comparison with patients not receiving the treatment of interest.
Regimens A pattern of treatment e.g. dose, frequency of a drug.
Respiratory depression The rate and/or depth of respiration are insufficient to maintain adequate gas exchange in the lungs.
Ribonucleic acid One of two types of nucleic acid made by cells. It contains information that has been copied from DNA (the other type of nucleic acid). Many forms of ribonucleic acid have functions related to making proteins.
Risk The probability of an outcome which is given by the number with the outcome divided by the number with AND without the outcome.
Risk of bias Bias in the reported outcomes of a study may be caused by an inadequacy in the way the study is designed or conducted. For example, if any of the following aspects of the trial were not conducted properly then the trial may be said to have an increased risk of bias: the random allocation of the treatments, allocation concealment, blinding of researchers during invention and measurement of outcomes, missing outcome data, selective outcome reporting.
Risk ratio The ratio of risks in two treatment groups. In intervention studies, it is the ratio of the risk in the intervention group to the risk in the control group. A risk ratio of one indicates no difference between comparison groups. For undesirable outcomes, a risk ratio that is less than one indicates that the intervention was effective in reducing the risk of that outcome. (Also called relative risk, RR.).
Sample size The number of units (persons, animals, patients, specified circumstances, etc.) in a population to be studied. The sample size should be big enough to have a high likelihood of detecting a true difference between two groups.
Singleton A single baby.
Stillbirth Death in a fetus >400g or at least 20 weeks’ gestation age.
Substantial gross motor dysfunction
The inability to make the purposeful movements of the large muscles that are necessary to complete or master a prescribed task.
Synergistic effect Interaction between drugs that has a positive effect on an outcome.
Systematic review A review of a clearly formulated question that uses systematic and explicit methods to identify, select, and critically appraise relevant research, and to collect and analyse data from the studies that are included in the review. Statistical methods (meta-analysis) may or may not be used to analyse and summarise the results of the included studies.
Therapeutic range A concentration range that provides efficacy without unacceptable toxicity.
Tocolysis The inhibition of contractions of the uterus during labour.
Tocolytic A medication that can inhibit the contractions of the uterus during labour.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 6
Guideline Panel Membership
Members Expertise Work affiliation
Chairperson
Professor Caroline Crowther*
Maternal Fetal Medicine Specialist
Professor Maternal and Fetal Medicine, Director of the Australian Research Centre for Health of Women and Babies (ARCH), Discipline of Obstetrics and Gynaecology, The University of Adelaide
Ms Philippa Middleton* Epidemiologist
Research Methodologist
Research Leader with ARCH, Discipline of Obstetrics and Gynaecology, The University of Adelaide
Ms Tanya Bubner* Researcher Manager of ARCH, Discipline of Obstetrics and Gynaecology, The University of Adelaide
Dr Helena Oakey* Statistician Senior Statistician with ARCH, Discipline of Obstetrics and Gynaecology, The University of Adelaide
Ms Mary Paleologos Administrative Assistant Administration Assistant with ARCH, Discipline of Obstetrics and Gynaecology, The University of Adelaide
Dr Lisa Askie* Epidemiologist Senior Research Fellow/Manager, Australian New Zealand Clinical Trials Registry, NHMRC Clinical Trials Centre, University of Sydney
Professor Jonathan Morris* Maternal Fetal Medicine Subspecialist
Professor of Obstetrics and Gynaecology, Head of Discipline, Obstetrics, Gynaecology and Neonatology, University of Sydney
Professor Lex Doyle* Neonatologist
Developmental Paediatrician
Professor, Obstetrics and Gynaecology, University of Melbourne
Associate Professor Vicki Flenady* Epidemiologist
Research Methodologist
Neonatal Nurse
Mater Mothers’ Research Centre, Mater Health Services, University of Queensland
Mr Neil Hotham Senior Pharmacist Drug Information Specialist
Senior Specialist Drug Information Pharmacist, Women's and Children's Hospital, Adelaide
Ms Allison Rogers Midwife/SA Perinatal Practice Guidelines
Project Midwife, SA Perinatal Practice Guidelines, Women's and Children's Hospital, Adelaide
Professor Peter Davis* Neonatologist,
Royal Australian College of Physicians (RACP) representative
Consultant Neonatologist, Royal Women’s Hospital, University of Melbourne
Professor Lesley McCowan Maternal Fetal Medicine Subspecialist
Head of Department, Sub-specialist in Maternal Fetal Medicine, Department of Obstetrics and Gynaecology, University of Auckland
Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 7
Dr Jane Alsweiler Neonatologist Senior Lecturer in Paediatrics, University of Auckland
Ms Ruth Martis Midwife/New Zealand College of Midwives Representative/Lecturer
Lecturer, Christchurch Polytechnic Institute of Technology
Dr Dell Horey Epidemiologist
Consumer representative
Research Fellow, La Trobe University
Ms Rowena Crawford Consumer representative
Life’s Little Treasures Inc.
Ms Sonia Alix Consumer representative
Liggins Institute, University of Auckland
Associate Professor Susan Walker Royal Australian and New Zealand College of Obstetrics and Gynaecology (RANZCOG) representative
University of Melbourne
Dr Trudi Mannix Australian College of Neonatal Nurses (ACNN) Representative
Lecturer, Nursing and Midwifery, Flinders University
Professor David Ellwood Women’s Health Australasia (WHA) representative
Deputy Dean & Professor of Obstetrics & Gynaecology, The Australian National University Medical School, The Canberra Hospital
Ms Sarah McIntyre Cerebral Palsy Representative
Research Fellow, NSW/ACT CP Register
Cerebral Palsy Institute
University of Notre Dame Australia
* Executive panel members

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 8
Summary of Clinical Recommendations, Good Practice Points,
Implementation Implications and Research Recommendations
Clinical Recommendations
This set of clinical recommendations needs to be considered as a whole – recommendations should
not be applied in isolation.
CLINICAL RECOMMENDATIONS GRADE
Chapter
In women at risk of early preterm* imminent# birth, use magnesium
sulphate for neuroprotection of the fetus, infant and child:
* when gestational age is less than 30 weeks. #
when early preterm birth is planned or definitely expected within
24 hours. (When birth is planned, commence magnesium sulphate
as close to four hours before birth as possible).
A 4-7
B 8
A 9
intravenously with a 4 gram loading dose (slowly over 20-30 minutes) and 1 gram per hour maintenance dose via intravenous route, with no immediate repeat doses. Continue regimen until birth or for 24 hours, whichever comes first.
C 10
regardless of plurality (number of babies in utero). B 11
regardless of the reason women (at less than 30 weeks’ gestation) are considered to be at risk of preterm birth.
B 12
regardless of parity (number of previous births for the woman). B 13
regardless of anticipated mode of birth. B 14
whether or not antenatal corticosteroids have been given. B 15
Good Practice Points
Timing (Chapter 9)
If birth before 30 weeks is planned or expected to occur sooner than four hours (e.g. scheduled
caesarean or late presentation to hospital), administer magnesium sulphate to women at risk of
preterm birth, as there is still advantage likely from administration within this time.
Urgent delivery (Chapter 10)
In situations where urgent delivery is necessary because of actual or imminent maternal or fetal
compromise (e.g. severe fetal distress or antepartum haemorrhage), then birth should not be
delayed to administer magnesium sulphate.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 9
Repeat doses (Chapter 10)
In the event that birth does not occur after giving magnesium sulphate for neuroprotection of the
infant, and preterm birth (less than 30 weeks’ gestation) again appears imminent (planned or
definitely expected within 24 hours), a repeat dose of magnesium sulphate may be considered at the
discretion of the attending health professional.
Locations of administration of antenatal magnesium sulphate (Chapter 10)
The locations of administration of antenatal magnesium sulphate intravenously to women should be
determined by each individual maternity facility.
Monitoring (Chapter 10)
During administration of magnesium sulphate intravenously, women should be regularly assessed as
detailed in individual obstetric unit protocols. Resuscitation and ventilatory support should be
immediately available, if needed, during administration of magnesium sulphate. Should hypotension
or respiratory depression occur prompt medical review is recommended. This may include cessation
of magnesium sulphate.
Loading
A minimum assessment should include checking pulse, blood pressure, respiratory rate and patellar
reflexes before loading dose, 10 minutes after loading dose infusion has started and at the end of
the loading dose infusion (20-30 minutes). The infusion should be stopped if respiratory rate
decreases more than 4 breaths per minute below baseline, or is less than 12 breaths per minute; or
diastolic blood pressure decreases more than 15 mm Hg below baseline level.
Maintenance
While the maintenance infusion is running, observe for any adverse effects. The minimum
assessments should include checking pulse, blood pressure, respiratory rate, patellar reflexes and
urine output 4-hourly. Stop infusion if respiratory rate is less than 12 breaths per minute; if patellar
reflexes are absent, if hypotension occurs or if urine output is less than 100 mL over 4 hours.
Toxicity
Magnesium toxicity is unlikely with the regimens recommended in these guidelines and serum
magnesium concentrations do not need to be routinely measured (RCOG 2006). In women with
renal compromise, serum magnesium monitoring is recommended.
Calcium gluconate (1 g (10 mL of 10% solution) slowly via intravenous route over 10 minutes) can be
given if there is clinical concern over respiratory depression.
Potential interactions (Chapter 10) There is a potential theoretical interaction between magnesium sulphate and nifedipine of
hypotension and neuromuscular blockade effects, although this is seldom reported in clinical
practice (Snyder & Cardwell 1989; Ben-Ami 1994). Regular monitoring of the mother is
recommended as detailed in individual obstetric unit protocols. If hypotension occurs, nifedipine
and magnesium sulphate administration should cease and the woman reviewed by a medical
practitioner.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 10
Implementation Implications
Changes in usual care (Chapter 7)
While intravenous magnesium sulphate administration is standard care to prevent and treat
eclampsia, only a few obstetric units in Australia and New Zealand are using antenatal magnesium
sulphate for fetal, infant, and child neuroprotection.
Resource implications (Chapter 7) Although magnesium sulphate is an inexpensive drug, setting up, maintaining and monitoring
magnesium sulphate infusions will incur additional staff time. There will also be training needs, but
these should be minimal as all units will have experience with magnesium sulphate infusions to treat
or prevent eclampsia.
Less than 1.2% of all births occur at before 30 weeks’ gestation; around 3528 such births occur in
Australia (AIHW 2009) and 640 in New Zealand each year. Up to 10% of these babies will have been
exposed in utero to magnesium sulphate as treatment for prevention and treatment of eclampsia. If
all other women who gave birth before 30 weeks’ gestation were given magnesium sulphate for
neuroprotection of the fetus, infant, and child, up to 4104 more women in Australia and New
Zealand each year would need additional care and monitoring. (This figure does not include a small
number of women at less than 30 weeks’ gestation where birth is planned or definitely expected
within 24 hours and who do not actually give birth before 30 weeks’ gestation).
On the other hand, fewer cases of cerebral palsy will mean substantial savings at the overall health
systems and societal level.
Changes in the way care is currently organised (Chapter 7)
It is acknowledged that while all tertiary obstetric units dealing with babies likely to be born at or
before 30 weeks will already have established protocols and systems that will enable them to
administer magnesium sulphate intravenously to women at risk of preterm birth less than 30 weeks’
gestation, appropriate staffing structures may not be in place to enable the safe administration of
magnesium sulphate.
The ideal setting for babies to be born before 30 weeks is a tertiary specialist unit. Given that the
clinical indication for magnesium sulphate is planned or definitely expected preterm birth before 30
weeks then its use will generally be within tertiary obstetric units. Women threatening to give birth
before 30 weeks in other settings, and fulfilling all other guideline criteria, may be eligible to receive
magnesium sulphate after consultation with their tertiary obstetric network, depending on the non-
tertiary unit’s service capability and staffing.
Magnesium sulphate infusions should not be used during antenatal transfer unless resuscitation and
ventilator support are immediately available. If a clinical decision is made to transfer a woman who
has received magnesium sulphate in another setting to a tertiary obstetric unit, the magnesium
sulphate maintenance infusion can be stopped during the transfer.
Barriers to implementation (Chapter 7, 8 and 10)
Barriers to implementation will include finding the extra time and staff required to administer
magnesium sulphate to more women. However, as magnesium sulphate infusions, in the regimens

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 11
recommended, are already widely practised for treatment of severe pre-eclampsia and eclampsia at
these gestational ages, training needs should be minimal as all units will have experience.
Monitoring women after they have received antenatal infusions of magnesium sulphate is usually
recommended. Monitoring formed part of the published study methods for two of the included
randomised controlled trials (Crowther 2003 and Marret 2006, also see Appendix H.] There is,
however, no consensus on what form this monitoring should take. For example the Society of
Obstetric Medicine of Australia and New Zealand (SOMANZ) state that obstetric units should
determine their own protocols for monitoring outcomes [SOMANZ 2008, also see Appendix H]. As
toxicity is unlikely with the regimens recommended in these guidelines, routine monitoring of serum
magnesium sulphate concentrations should not be required.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 12
Research Recommendations
These research recommendations have been derived from Panel discussions during the course of
developing the Guidelines.
Prevention of Cerebral Palsy
How to prevent cerebral palsy and identifying causes and causal pathways are priority research
questions.
Follow up of children in existing trials
Continuing the follow up of children in the existing randomised trials is necessary to elucidate if the
benefits from antenatal magnesium sulphate seen in early childhood translate into later benefits.
Audit of antenatal magnesium sulphate use and rates of cerebral palsy
It will be important to monitor the antenatal use of magnesium sulphate for neonatal
neuroprotection, ideally through national audit; and to link data to national childhood cerebral palsy
registers and databases.
Existing trials
Individual triallists should be approached to provide unpublished data, for subsequent revisions of
the Cochrane review ‘Magnesium sulphate for women at risk of preterm birth for the
neuroprotection of the fetus’ (Doyle 2009), where possible, on:
optimal timing of magnesium sulphate administration.
optimal treatment regimens.
gestational age breakdown or available gestational age subgroups (at trial entry).
reasons women were considered to be at risk of preterm birth and health outcomes.
plurality and health outcomes.
parity and health outcomes.
mode of birth and health outcomes.
use of antenatal corticosteroids and health outcomes.
Individual patient meta-analyses
Individual patient meta-analyses through an international collaboration of triallists responsible for
the existing randomised trials will permit further exploration of:
gestational age when magnesium sulphate was administered and health outcomes.
whether differences in timing of magnesium sulphate administration result in
differences in outcomes such as cerebral palsy and combined death and cerebral
palsy.
whether different magnesium sulphate regimens result in different rates of adverse
outcomes such as cerebral palsy and combined death and cerebral palsy.
whether differences in plurality result in different rates of adverse outcomes such as
cerebral palsy and combined death and cerebral palsy.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 13
whether differences in reasons women were considered to be at risk of preterm
birth result in different rates of adverse outcomes such as cerebral palsy and
combined death and cerebral palsy.
influence of parity.
whether mode of birth modifies neurodevelopmental outcomes.
whether differences in use of antenatal corticosteroids result in different rates of
adverse outcomes such as cerebral palsy and combined death and cerebral palsy.
Biomarkers for cerebral palsy
Investigations to identify biomarkers for cerebral palsy in at risk groups to allow a more targeted use
of antenatal administration of magnesium sulphate.
Further randomised controlled trials
Further randomised trials are needed, comparing antenatal magnesium sulphate with placebo when
given to women at risk of preterm birth at 30 weeks’ gestation or more, that assess mortality,
cerebral palsy and combined death and cerebral palsy.
Further randomised controlled trials are required specifically comparing:
different speeds of administering the loading dose of magnesium sulphate to
establish if slower loading reduces maternal adverse effects.
optimal timing of the antenatal administration of magnesium sulphate prior to
preterm birth.
loading dose versus loading dose plus maintenance.
different loading doses (4 g versus 6 g).
use of repeat doses of magnesium sulphate.
treatment of the very preterm infant with magnesium sulphate after birth.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 14
Chapter 1: Need for these Guidelines
It is now 14 years since the publication of a case-control study first described the association of
antenatal magnesium sulphate prior to preterm birth and the prevention of cerebral palsy (Nelson
1995). The evidence available on this topic has been growing and has recently reached a
translational ‘flashpoint’. With the recent publication of the US trial (Rouse 2008), the updated
Cochrane review ‘Magnesium sulphate for women at risk of preterm birth for the neuroprotection of
the fetus’ (Doyle 2009) shows, for the first time, that magnesium sulphate given to women prior to
preterm birth can reduce the risk of cerebral palsy. This Cochrane review now contains five trials
(including the Australian and New Zealand randomised trial of antenatal magnesium sulphate for
neuroprotection of the fetus, funded through the National Health and Medical Research Council
(NHMRC) Project Grant 3503267 (Crowther 2003)).
The updated Cochrane review concludes that antenatal magnesium sulphate therapy given to
women at risk of preterm birth substantially reduced the risk of cerebral palsy in their child (risk
ratio (RR) 0.68 95% confidence interval (CI) 0.54 to 0.87; five trials, 6145 infants).
This is a very important finding, as few interventions have been found to prevent cerebral palsy
which can have devastating and long-term consequences. Over 120 children are diagnosed with
cerebral palsy in New Zealand each year and over 600 are similarly diagnosed in Australia. About
45% of all cases of cerebral palsy are related to preterm birth. Preventing cerebral palsy and
identifying causes and causal pathways have been identified as the lead priority for research by
consumers, clinicians and researchers (McIntyre 2009).
The prevention of cerebral palsy fits within the ‘Promoting and maintaining good health’ National
Research Priority; three of the four goals of this Priority are relevant, specifically;
a healthy start to life;
ageing well, ageing productively; and
preventive health.
Aim of the guideline
While it is now clear that magnesium sulphate has a role in reducing the risk of cerebral palsy, the
evidence for how and when to use magnesium sulphate is less clear. Colleges (such as the Royal
Australian and New Zealand College of Obstetricians and Gynaecologists), societies and individual
hospitals and clinicians have requested detailed evidence-based guidance in the form of a national
statement.
These Antenatal Magnesium Sulphate Prior to Preterm Birth for Neuroprotection of the Fetus,
Infant, and Child Guidelines specifically address whether the administration of magnesium sulphate
to women prior to preterm birth:
improves the health outcomes for the fetus, infant and child;
causes adverse outcomes for the women; or the fetus, infant and child;

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 15
varies by:
o gestational age magnesium sulphate is given;
o time magnesium sulphate is planned to be given prior to birth;
o regimen (dosing and routes of administration);
o number of babies in utero;
o reason women are considered to be at risk of preterm birth;
o parity of the women;
o mode of birth and interaction with magnesium sulphate;
o combined effect of antenatal corticosteroids and magnesium sulphate.
Outcomes to be considered:
Death and any neurological impairment (including cerebral palsy, blindness, deafness,
developmental delay) for the fetus/infant/child.
Harmful effects by the therapy for the woman and the child (maternal respiratory
depression, cardiac arrest, hypotension, side effects, and fetal/neonatal side effects.
Our purpose and rationale is to provide practical evidence-based guidance on the best practice for
clinical care in the use of magnesium sulphate prior to preterm birth. These guidelines will be
relevant for health professionals who care for women at risk of preterm birth and their babies; for
pregnant women and their partners and families; and for policy makers in maternity care.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 16
Chapter 2: Summary of Guideline Development Process
A multidisciplinary expert advisory panel (the Panel) was established to oversee the development of
these Guidelines (see p.7-8 for a list of members and their roles and affiliations).
The purpose of the Panel was to prepare an evidence-based guideline on best practice for clinical
care in the use of antenatal magnesium sulphate prior to preterm birth for the neuroprotection of
the fetus, infant and child.
The Guideline was developed according to the requirements of the Australian National Health and
Medical Research Council (NHMRC) and the New Zealand Guidelines Group (NZGG) – see appendices
A and D.
The Panel formulated a set of critical clinical questions which formed the framework for the
Guidelines (these questions are listed in Chapter 1). Each question is addressed in a separate
chapter* using the following format:
a description of the studies comprising the relevant evidence;
the main results from these studies;
a summary of the judgements from the evidence statements (see below);
using judgements to formulate recommendations (and good practice points);
the implications for implementing the recommendations;
further research required to address the specific question adequately.
*For Question 1 (Does administration of magnesium sulphate prior to preterm birth improve the
health outcomes for the fetus, infant, and child?) these components are included in four chapters
(Chapters 4-7).
Summary of timeline:
12 Oct 2009 - input sought by email from full panel.
16 Oct 2009 - subsequent drafts discussed by teleconference.
12 Nov 2009 - face to face meeting in Sydney.
12 Dec 2009 - open meeting in Adelaide.
19 Dec 2009 to 18 Jan 2010 - public consultation of draft guidelines.
Feb 2010 - final guideline document.
March 2010 – draft guidelines released.
17 November 2010 – NHMRC approved guidelines.
Updating the Guidelines
One source of new evidence in the future will be an individual patient data (IPD) meta-analysis.
Funding has been awarded through a NHMRC Project Grant to commence in 2010 (NHMRC 627228).
Therefore we anticipate a major update of these Guidelines in approximately two years using data
from the IPD.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 17
Chapter 3: Background
Cerebral palsy and link with preterm birth
Cerebral palsy and cognitive dysfunction are the most frequently occurring neurologic impairments
associated with preterm birth (before 37 weeks gestation), and any therapy that can reduce their
prevalence would substantially reduce overall neurologic impairments and disabilities among
surviving preterm infants. The cost to the Australian community of cerebral palsy including financial
cost and lost wellbeing is AUD$3.87 billion per annum. For the individual the financial and lost
wellbeing cost per annum is over AUD$115,000 (Access Economics 2008).
Cerebral palsy is a term which includes a number of different diseases or conditions that can arise at
any time during brain development. Cerebral palsy can involve a disorder of movement or posture,
or both, and a disorder of motor function which is permanent but may change over time (Oxford
Register 2001).
Approximately 42% of all cases of cerebral palsy are associated with preterm birth (Australian
Cerebral Palsy Register Group 2009) with the rate of cerebral palsy amongst neonatal survivors born
at less than 28 weeks gestation up to 30 times higher compared with infants born at term (Stanley
1992).
At present there is no cure for cerebral palsy, which makes effective preventive interventions of
paramount importance. Prevention of cerebral palsy has been identified by consumers, clinicians
and researchers as a top priority for research by the Cerebral Palsy Institute (McIntyre 2009).
Preterm birth and neurological outcome
Babies born preterm have a higher chance of dying in their first few weeks of life. Preterm infants
who survive have greater risk of neurologic impairments, such as cerebral palsy, blindness, deafness,
or cognitive dysfunction (either intellectual impairment or developmental delay), and a greater risk
of substantial disability as a result of these neurologic impairments (Doyle 2001; Saigal & Doyle
2008). Intraventricular haemorrhage (IVH) is a known risk factor for the later development of
cerebral palsy (Kuban 1992). The risk of IVH and periventricular leukomalacia increases the earlier
the gestational age at birth (Vermeulen 2001).
The rate of preterm birth is increasing in many countries, with recently reported rates of 12.8% in
the United States (National Center for Health Statistics 2009); over 8% in Australia (AIHW 2009) and
over 7% in New Zealand (New Zealand Health Information Service 2006), with corresponding
increases in the number of babies at risk of death or an adverse neurological outcome.
Biological plausibility for use of magnesium sulphate for fetal and infant neuroprotection
In humans, magnesium sulphate is essential for health through key cellular processes, including
glycolysis, oxidative phosphorylation, protein synthesis, DNA and RNA aggregation and maintenance
of plasma membrane integrity (Mildvan 1987; McIntosh et al 1989).
Animal studies have shown that magnesium sulphate can provide a neuroprotective effect
(McDonald 1990) preventing post-hypoxic brain injury by blocking the excess release of glutamate in
the calcium channel. The fetal and newborn brain seems more susceptible to damage from

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 18
glutamate release. Consequently, blocking glutamate receptors through agents, such as magnesium
sulphate, may reduce the risk of injury in the perinatal period (Espinoza 1991).
Possible role of magnesium sulphate for neuroprotection of the fetus, infant and child
Kuban and colleagues were the first to report that antenatal magnesium sulphate was associated
with a reduction in the risk of IVH in babies born with birthweights less than 1500 g (Kuban 1992). A
case-control analysis from the California Cerebral Palsy project investigated whether in utero
exposure to magnesium sulphate was associated with a lower prevalence of cerebral palsy among
infants born weighing less than 1500 g (Nelson 1995). Cases were singleton children with cerebral
palsy whose birthweight was less than 1500 g. Controls were randomly sampled from live births of
less than 1500 g from the same birth populations. Magnesium sulphate given to mothers during
labour was associated with a significantly marked reduction in the risk of cerebral palsy (odds ratio
0.14; 95% confidence interval 0.05 to 0.51).
Other observational studies have supported a reduction in cerebral palsy in preterm infants by
maternal administration of magnesium sulphate (Hauth 1995; Schendel 1996; Wiswell 1996) or
found a reduction in the risk of IVH (Finesmith 1997; Perlman 1994; Wiswell 1996) and perinatal
mortality (Grether 1998). However, not all observational studies have reported benefit for antenatal
magnesium sulphate for the risk of IVH (Canterino 1999; Kimberlin 1998; Paneth 1997; Weintraub
2001), cerebral palsy (Grether 2000; O'Shea 1998; Paneth 1997) or paediatric mortality (Kimberlin
1998).
Maternal adverse effects and side effects
Magnesium sulphate produces flushing, sweating, and a sensation of warmth by its peripheral
vasodilator effects when infused intravenously. Other reported maternal side effects, related to
dosage and speed of infusion, include nausea, vomiting, headache, palpitations and, rarely,
pulmonary oedema. Administration of magnesium sulphate to concentrations above the
recommended therapeutic range can lead to respiratory depression, respiratory arrest, cardiac
arrest and death.
Fetal, neonatal and infant adverse effects and side effects
In the neonate, hypermagnesaemia can lead to hyporeflexia, poor sucking, and, rarely, respiratory
depression needing mechanical ventilation (Levene 1995; Lipsitz 1971).
Magnesium sulphate use in pregnancy
The focus of these Guidelines is antenatal use of magnesium sulphate for neuroprotection of the
fetus, infant and child. The evidence for the effectiveness of magnesium sulphate for this purpose
comes from four trials (Crowther 2003; Marret 2006; Mittendorf 2002; Rouse 2008) which have
been pooled in the Cochrane systematic review ‘Magnesium sulphate for women at risk of preterm
birth for neuroprotection of the fetus’ (Doyle 2009).
Magnesium sulphate has also been used antenatally for:
Tocolysis (to inhibit contractions in threatened preterm labour)
In the relevant randomised trials from the Cochrane systematic review ‘Magnesium sulphate for
preventing preterm birth in threatened preterm labour’, Crowther 2002 found magnesium
sulphate to be ineffective at delaying birth or preventing preterm birth, and its use was

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 19
associated with an increased mortality for infants. (Preliminary results for the update of this
Cochrane review [currently in draft form] again indicate that magnesium sulphate was
ineffective at delaying or preventing preterm birth although no significant differences in fetal,
neonatal, infant or total mortality between magnesium sulphate and placebo/no treatment or
between magnesium sulphate and other drugs used for tocolysis were seen);
Maintenance therapy for preventing preterm birth after threatened preterm labour
In the Cochrane systematic review ‘Magnesium maintenance therapy for preventing preterm
birth after threatened preterm labour’ Crowther 1998 found insufficient evidence of any
differences between magnesium sulphate maintenance therapy and either placebo/no
treatment, or alternative therapies (ritodrine or terbutaline) to prevent preterm birth after an
episode of threatened preterm labour;
Neuroprotection of the mother (to prevent and treat pre-eclampsia)
The Cochrane systematic review ‘Magnesium sulphate and other anticonvulsants for women
with pre-eclampsia’ (Duley 2003) found that magnesium sulphate more than halved the risk of
eclampsia and probably reduced the risk of maternal death, but did not improve outcomes for
the baby in the short term.
Evidence summaries for the tocolytic and maternal neuroprotective use of magnesium sulphate can
be found in Appendix E.
Evidence relating to possible harms to the mother or the fetus/infant/child from any antenatal use
of magnesium sulphate (compared with placebo or no treatment) will be considered later (see
Chapters 5 and 6 and Appendix G).

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 20
Chapter 4: Improving Health Outcomes for the Fetus, Infant,
and Child (Question 1)
Question 1: Does the administration of magnesium sulphate to women prior to preterm birth improve the health outcomes for the fetus, infant, and child?
Magnesium sulphate is given to pregnant women at risk of preterm birth with the intention of
preventing cerebral palsy and other adverse neurodevelopmental outcomes.
As foreshadowed in Chapter 3, the four trials (Crowther 2003, Marret 2006, Mittendorf 2002
(neuroprotective arm only) and Rouse 2008) in the Doyle 2009 Cochrane systematic review
‘Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus’ form the
evidence base for the effectiveness of antenatal use of magnesium sulphate for fetal, infant or child
neuroprotective intent, the focus of these guidelines.
The evidence for potential harms was taken from a wider evidence base – from studies related to
fetal, infant and child neuroprotective intent, as well as tocolytic intent and maternal
neuroprotective intent (pre-eclampsia). These studies are contained in four Cochrane reviews
(Doyle 2009, Duley 2003, Crowther 2002 and Crowther 1998) – see Chapters 5 and 6.
The evidence for effectiveness outlined in this chapter was considered with the evidence for
potential harms in Chapter 7, where there is formulation of an overall recommendation about the
use of antenatal magnesium sulphate for neuroprotection of the fetus, infant and child.
NEUROPROTECTION (FETUS, INFANT, AND CHILD)
The Doyle 2009 Cochrane review compared magnesium sulphate with placebo or no treatment given
to women at risk of preterm birth and included four trials (4446 infants) which addressed infant
neuroprotection.
Death and cerebral palsy are competing outcomes as most perinatal deaths or those deaths that
occur later before cerebral palsy can be diagnosed. Therefore, the combined outcome of death or
cerebral palsy is commonly considered the most clinically relevant outcome for assessing
neuroprotection.
In Doyle 2009, the combined outcome of death or cerebral palsy or cerebral palsy alone showed
significant reductions where women who were at risk of preterm birth were given magnesium
sulphate antenatally with the intent of providing neuroprotection (see Table 1). The review showed
that 63 babies (95% confidence interval 44 to 155) need to be treated with magnesium sulphate for
one baby to avoid cerebral palsy. The corresponding number needed to treat to benefit (NNTB) for
combined death or cerebral palsy was 42 babies (95% confidence interval 24 to 346).

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 21
Table 1: Magnesium sulphate vs placebo/no treatment: primary outcomes (Doyle 2009 Cochrane Review)
Primary outcomes RR (95% CI) Number of trials; participants
Death or cerebral palsy 0.85 (0.74 to 0.98)* four trials; 4446 infants
Death (fetal and later) 0.95 (0.80 to 1.12) four trials; 4446 infants
Cerebral palsy 0.71 (0.55 to 0.91)* four trials; 4446 infants
Any neurological impairment 1.03 (0.87 to 1.21) one trial; 1255 infants
Death or substantial gross motor dysfunction 0.84 (0.71 to 1.00) three trials; 4387 infants
*significantly in favour of magnesium sulphate
See Appendix F.1-3: Evidence tables/graphs
Table 2: Magnesium sulphate vs placebo/no treatment: selected secondary outcomes (Doyle 2009 Cochrane Review)
Secondary outcomes RR (95% CI) Number of trials; participants
Neonatal outcomes
Intraventricular haemorrhage 0.96 (0.86 to 1.08) four trials; 4552 infants
Severe intraventricular haemorrhage (grade 3/4)
0.83 (0.62 to 1.13) two trials; 3699 infants
Periventricular leukomalacia 0.93 (0.68 to 1.28) four trials; 4552 infants
Infant/child outcomes
Substantial gross motor dysfunction 0.60 (0.43 to 0.83)* three trials; 4387 infants
Development delay or intellectual impairment 1.00 (0.91 to 1.09) three trials; 4387 infants
Major neurological disability 1.14 (0.86 to 1.51) one trial; 1255 infants
Blindness 0.97 (0.14 to 6.90) two trials; 1943 infants
Deafness 0.51 (0.05 to 4.96) two trials; 1943 infants
*significantly in favour of magnesium sulphate

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 22
Chapter 5: Adverse Outcomes for the Women (Question 2)
Question 2: Does the use of magnesium sulphate prior to preterm birth cause adverse outcomes for the women?
Evidence regarding potential maternal harms was extracted from those trials that compare
magnesium sulphate with placebo or no treatment in the four Cochrane reviews looking at the
various indications for antenatal use of magnesium sulphate (Crowther 1998, Crowther 2002, Doyle
2009 and Duley 2003).
Women given magnesium sulphate were about three times more likely to cease therapy compared
with women not given magnesium sulphate therapy (placebo or no treatment), mainly due to
flushing (20.4% vs 2.2%), nausea/vomiting (3.2% vs 0.4%) and headaches (0.7% vs 0.3%). Overall
cessation of therapy was 7.5% in the magnesium sulphate group compared with 2.7% in the
placebo/no treatment groups.
Hypotension (variously defined) and respiratory depression (variously defined) were also
significantly elevated among women given magnesium sulphate. Overall hypotension was 2.0% in
the magnesium sulphate groups compared to 1.2% in the placebo/no treatment groups. Overall
respiratory depression was 1.3% in the magnesium sulphate groups and 0.8% in the placebo/no
treatment groups.
In the Cochrane review on preventing eclampsia (Duley 2003), a small but significant absolute
increase of 2.5% in the caesarean rate was seen, from 47.2% in the placebo group to 49.7% in the
magnesium group (RR 1.05 95% CI 1.01 to 1.10). There was not a significant increase in the
caesarean rate in the Doyle 2009 Cochrane Review (48.8% for the magnesium sulphate group and
47.2% for the placebo group).
In very large doses, magnesium sulphate can have toxic, even life-threatening effects for women.
This has been documented in case reports (for example McDonnell 2009). Careful monitoring of the
woman’s magnesium sulphate administration is therefore advised (see Chapter 10).
See Appendix G.1: Evidence tables

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 23
Chapter 6: Adverse Outcomes for Fetus, Infant, and Child
(Question 3)
Question 3: Does the use of magnesium sulphate prior to preterm birth cause adverse outcomes for the fetus, infant, and child?
Evidence regarding potential harms to the fetus, infant or child was extracted from the trials
comparing magnesium sulphate with placebo or no treatment in the four Cochrane reviews looking
at the various indications for antenatal use of magnesium sulphate (Crowther 1998, Crowther 2002,
Doyle 2009 and Duley 2003).
None of the harms for the fetus, infant or child were significantly increased with antenatal use of
magnesium sulphate including total deaths (fetal, neonatal, or infant), intraventricular haemorrhage
or necrotising enterocolitis.
See Appendix G.2: Evidence tables

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 24
Chapter 7: Summary of Evidence for Questions 1-3
Summary of evidence statement judgements for fetal, infant, and child neuroprotection
The evidence base for using magnesium sulphate as an agent for fetal, infant, and child
neuroprotection has low risk of bias. Results between trials are fairly consistent. Benefits were
judged to outweigh potential harms and clinical impact considered to be very large, due to the
importance of reducing the risk of cerebral palsy.
While evidence was applicable to the context of Australian and New Zealand health care, it had less
generalisability in regard to the intended target population (women at risk of preterm birth) as the
majority of women in the largest trial had preterm prelabour rupture of membranes (PPROM) when
recruited to the trial (and so represented a narrower subset of women at risk of preterm birth).
Overall the body of evidence was considered sufficiently good enough to make the following grade A
recommendation:
CLINICAL RECOMMENDATION GRADE
In women at risk of early preterm* imminent# birth, use magnesium sulphate for neuroprotection of the fetus, infant and child.
*see chapter 8 #see chapter 9
A
Appendix F1-3: Evidence statements
IMPLEMENTATION IMPLICATIONS
Changes in usual care
While intravenous magnesium sulphate administration is standard care to prevent and treat
eclampsia, only a few obstetric units in Australia and New Zealand are using antenatal magnesium
sulphate for fetal, infant, and child neuroprotection.
Resource implications
Although magnesium sulphate is an inexpensive drug, setting up, maintaining and monitoring
magnesium sulphate infusions will incur additional staff time. There will also be training needs but
these should be minimal as all units will have experience with magnesium sulphate infusion to treat
or prevent eclampsia.
Less than 1.2% of all births occur at before 30 weeks’ gestation; around 3528 such births occur in
Australia (AIHW 2009) and 640 in New Zealand each year. Up to 10% of these babies will have been
exposed in utero to magnesium sulphate as treatment for prevention and treatment of eclampsia. If
all other women who gave birth before 30 weeks’ gestation were given magnesium sulphate for
neuroprotection of the fetus, infant, and child, up to 4104 more women in Australia and New
Zealand each year would need additional care and monitoring. (This figure does not include a small
number of women at less than 30 weeks’ gestation where birth is planned or definitely expected
within 24 hours and who do not actually give birth before 30 weeks’ gestation).
On the other hand, fewer cases of cerebral palsy will mean substantial savings at the overall health
systems and societal level.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 25
Changes in the way care is currently organised
It is acknowledged that while all tertiary obstetric units dealing with babies likely to be born at or
before 30 weeks will already have established protocols and systems that will enable them to
administer magnesium sulphate intravenously to women at risk of preterm birth less than 30 weeks’
gestation, appropriate staffing structures may not be in place to enable the safe administration of
magnesium sulphate.
The ideal setting for babies to be born before 30 weeks is a tertiary specialist unit. Given that the
clinical indication for magnesium sulphate is planned or definitely expected preterm birth before 30
weeks then its use will generally be within tertiary obstetric units. Women threatening to give birth
before 30 weeks in other settings, and fulfilling all other guideline criteria, may be eligible to receive
magnesium sulphate after consultation with their tertiary obstetric network, depending on the non-
tertiary unit’s service capability and staffing.
Magnesium sulphate infusions should not be used during antenatal transfer unless resuscitation and
ventilator support are immediately available. If a clinical decision is made to transfer a woman who
has received magnesium sulphate in another setting to a tertiary obstetric unit, the magnesium
sulphate maintenance infusion can be stopped during the transfer.
Barriers to implementation
Barriers to implementation will include finding the extra time and staff required to administer
magnesium sulphate to more women. However, as magnesium sulphate infusions, in the regimens
recommended, are already widely practised for treatment of severe pre-eclampsia and eclampsia at
these gestational ages, training needs should be minimal as all units will have experience.
FURTHER RESEARCH RECOMMENDATIONS AND AUDIT
Further analyses of the existing trials (such as subgroup analyses and individual patient data
meta-analyses) will provide evidence to elucidate optimal timing of magnesium sulphate
administration and its optimal regimens (see subsequent chapters).
A randomised trial comparing different speeds of administering the loading dose of
magnesium sulphate would establish if slower loading reduces maternal adverse effects.
Investigations to identify biomarkers for cerebral palsy in at risk groups to allow a more
targeted antenatal administration of magnesium sulphate.
It will be important to monitor the antenatal use of magnesium sulphate, ideally through
national audit; and to link data to national childhood registers and databases.
School-age outcomes will be available from some studies; results of these studies may lead
to modifications of these guidelines.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 26
Chapter 8: Gestational Age (Question 4)
Question 4: Do the improvements for the fetus, infant, and child vary by gestational age?
This chapter summarises the evidence available from the four individual neuroprotective intent trials
within the Doyle 2009 Cochrane Review that consider gestational age at trial entry and effect of
antenatal magnesium sulphate.
All women in the four trials included in the Doyle 2009 Cochrane review were given magnesium
sulphate before 34 weeks’ gestation. In Rouse 2008, all women were less than 32 weeks at trial
entry with the majority (68% of trial participants) less than 30 weeks gestation (Costantine 2009).
Table 3: Gestational age at trial entry for trials (Doyle 2009 Cochrane Review)
Study Gestational age
Mittendorf 2002 < 34 weeks at randomisation
Marret 2006 < 33 weeks
Rouse 2008 (32% of trial participants) 31- 32 weeks
Crowther 2003 & Rouse 2008 (68% of trial participants) < 30 weeks
However the data analyses published in a systematic review by Costantine 2009 did not include all
women and so only subgroup analyses for women at different gestational ages are possible at
present; women with a gestational age of less than 34 weeks, less than 33 weeks, less than 32 weeks
and less than 30 weeks. There is one trial with each subgroup available for each analysis but results
are inconclusive due to small sample sizes.
Table 4: Results of primary outcomes by gestational age subgroup (Doyle 2009 Cochrane Review)
Trial Gestational age DEATH or CEREBRAL PALSY
CEREBRAL PALSY DEATH
RR (95% CI) +Mittendorf 2002
(n=59)
< 34 weeks 4.83 (0.60 to 38.90) 6.77 (0.37 to 125.65) 1.93 (0.19 to 20.18)
Marret 2006
(n=688)
< 33 weeks 0.80 (0.58 to 1.10) 0.70 (0.41 to 1.19) 0.85 (0.55 to 1.32)
Rouse 2008
(n=2444)
< 32 weeks 0.90 (0.73 to 1.10) 0.59 (0.40 to 0.85)* 1.13 (0.87 to 1.48)
Crowther 2003
(n=1255)
< 30 weeks 0.82 (0.66 to 1.02) 0.85 (0.55 to 1.31) 0.81 (0.62 to 1.05)
OVERALL < 34 weeks 0.86 (0.75 to 0.98)* 0.71 (0.55 to 0.91)* 0.95 (0.80 to 1.12) +neuroprotective arm
See Appendix F.4 for evidence tables/graphs

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 27
Summary of evidence statement judgements for gestational age subgroup
The subgroup analyses are from trials with low risk of bias, and where results between trials are
fairly consistent. While the evidence is applicable to the Australian and New Zealand context,
generalisability was reduced as the majority of the women (87%) in the largest trial (Rouse 2008)
had PPROM and so represent a limited subset of women at risk of preterm birth.
Overall clinical impact was judged to be very large but since any differences in death and cerebral
palsy by gestational age are unclear at present, no particular subgroup was judged by the guideline
panel to have any more or less impact than another.
How recommendation was formulated To minimise the number of women exposed the guideline panel felt it would be prudent, at this
stage, to restrict magnesium sulphate administration to the subgroup containing the lowest
gestational age (less than 30 weeks) and therefore recommend that magnesium sulphate be given
only for neuroprotective intent when women are at risk of preterm birth (less than 30 weeks’
gestation).
If magnesium sulphate administration is restricted to women at less than 30 weeks’ gestation at risk
of preterm birth; this will be a smaller group than those at less than 34 weeks’ gestation, which will
have a somewhat smaller impact on resource allocations.
See Appendix F.4 for evidence statement
CLINICAL RECOMMENDATION GRADE
In women at risk of early preterm* imminent#
birth, use magnesium sulphate for neuroprotection of the fetus, infant or child:
*when gestational age is less than 30 weeks.
#see chapter 9
B
IMPLEMENTATION IMPLICATIONS
As for Chapter 7.
FURTHER RESEARCH RECOMMENDATIONS
Individual triallists should be approached to provide unpublished gestational age
breakdowns or be requested to provide available gestational age subgroup analyses.
Individual patient data meta-analysis by gestational age when magnesium sulphate was
administered and health outcomes needs to be conducted.
Further randomised trials are needed, comparing antenatal magnesium sulphate with
placebo when given to women at risk of preterm birth at 30 weeks’ gestation or more, that
assess mortality, cerebral palsy and combined death and cerebral palsy.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 28
Chapter 9: Timing (Question 5)
Question 5: Do improvements to the fetus, infant, and child vary by time magnesium sulphate is planned to be given prior to preterm birth?
This chapter summarises the evidence available from the four individual randomised
neuroprotective intent trials included in the Doyle 2009 Cochrane Review that looked at the time
magnesium sulphate was planned to be given prior to preterm birth.
In two of the four neuroprotective intent trials (Crowther 2003 and Marret 2006), magnesium
sulphate was given when birth was planned or expected within 24 hours. The median time from
randomisation to birth for women in the magnesium sulphate group was 3.7 hours (interquartile
range (IQR) 1.4 to 13.8) for Crowther 2003 and 1 hour 38 minutes (IQR 5 minutes to 25 hours and 5
minutes) for Marret 2006. In Rouse 2008, at the time of recruitment to the study only 3% of women
were planned or expected to give birth within 24 hours. Although a further 10% were in advanced
preterm labour, most (87%) women had PPROM with a median time to birth of 25 hours (IQR 11 to
63 hours) from rupture of membranes. Mittendorf 2002 did not specify the time prior to preterm
birth in which it was planned that magnesium sulphate was to be given (although women recruited
to the study were in advanced preterm labour with cervical dilatation of more than 4 cm).
Table 5: Timing of magnesium sulphate administration for trials (Doyle 2009 Cochrane Review)
Study Timing
Crowther 2003
Marret 2006
When birth was planned or definitely expected within 24 hours
Rouse 2008 when birth was planned or expected within 24 hours for indicated preterm birth (3.1% only);
advanced preterm labour, with cervical dilatation between 4 and 8 cm (10.3%);
PPROM 86.7% - median 25 hours, interquartile range 11 to 63 hours from rupture of membranes to birth interval
Mittendorf 2002 Not specified
At present subgroup analyses are unable to provide conclusive results on the optimal timing for the
administration of magnesium sulphate prior to anticipated preterm birth.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 29
Table 6: Results of primary outcomes by timing for trials (Doyle 2009 Cochrane Review)
See Appendix F.5: evidence tables/graphs
Summary of evidence statement judgements for timing of magnesium sulphate administration
subgroup
The subgroup analyses come from trials with low risk of bias, where the results between trials are
fairly consistent. The evidence from the subgroups in which birth was planned or expected within
24 hours (Crowther 2003 and Marret 2006) was judged to be directly generalisable to the target
population, and the overall evidence applicable.
Overall clinical impact was judged to be very large but since differences in death and cerebral palsy
based on the timing of planned magnesium sulphate administration are unclear at present, no
particular subgroup was judged to have any greater or lesser impact than another.
How recommendation was formulated
The subgroup in which preterm birth was planned or definitely expected within 24 hours (Crowther
2003 and Marret 2006) was judged to be most representative of all subgroups included in the
intended target groups for this guideline. In addition, this subgroup showed a reduction in death or
cerebral palsy (see Table 6), even though it contained only 44% of the total number of women across
all four trials. On the other hand, Rouse 2008 (with 56% of the total number of women in the
Cochrane review) individually showed a benefit for cerebral palsy with magnesium sulphate (see
table 6 above).
In a small side study of Crowther 2003, Smith 2003 found that antenatal infusions enabled prompt
transfer of magnesium sulphate to the mother (within 30 minutes) and that neonatal magnesium
sulphate concentrations remained elevated to 24 hours. This indicates that magnesium sulphate
crosses the placenta to the fetus promptly after commencing the infusion.
Based on this evidence, the guideline panel recommended that magnesium sulphate be administered when early preterm birth is planned or definitely expected within 24 hours. (When birth is planned, commence magnesium sulphate as close to four hours before birth as possible). see Appendix F.5: evidence statement
Trial Timing DEATH or CEREBRAL PALSY
CEREBRAL PALSY
DEATH
RR (95% CI)
Crowther 2003; Marret 2006 (n=1943)
If birth planned or definitely expected within 24 hours
0.81 (0.68 to 0.97)* 0.79 (0.56 to 1.10) 0.82 (0.66 to 1.03)
Rouse 2008 (n=2444)
Variable 0.90 (0.73 to 1.10) 0.59 (0.40 to 0.85)* 1.13 (0.87 to 1.48)
Mittendorf 2002 (n=59)
Not specified 4.83 (0.60 to 38.90) 6.77 (0.37 to 125.65) 1.93 (0.19 to 20.18)
OVERALL 0.86 (0.75 to 0.98)* 0.71 (0.55 to 0.91)* 0.95 (0.80 to 1.12) *significantly in favour of magnesium sulphate

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 30
CLINICAL RECOMMENDATION GRADE
In women at risk of early preterm* imminent#
birth, use magnesium sulphate for neuroprotection of the fetus, infant or child:
#when early preterm birth is planned or definitely expected within 24 hours. (When birth is planned, commence magnesium sulphate as close to four hours before birth as possible).
*see chapter 8
A
GOOD PRACTICE POINT
If birth before 30 weeks is planned or expected to occur sooner than four hours (e.g. scheduled
caesarean or late presentation to hospital), administer magnesium sulphate to women at risk of
preterm birth, as there is still advantage likely from administration within this time.
IMPLEMENTATION IMPLICATIONS As for chapter 7.
FURTHER RESEARCH RECOMMENDATIONS
Individual triallists should be approached to provide unpublished optimal timing of
magnesium sulphate administration
Individual patient data meta-analysis can be used to explore whether differences in timing of
magnesium sulphate administration result in different rates of adverse outcomes such as
cerebral palsy and combined death and cerebral palsy.
Further randomised trials evaluating the optimal timing of the antenatal administration of
magnesium sulphate prior to preterm birth are warranted.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 31
Chapter 10: Regimens (Question 6)
Question 6: Do improvements to the fetus, infant, and child vary by regimens?
This chapter summarises the evidence of the four individual neuroprotective intent trials in the
Doyle 2009 Cochrane Review for regimens used to administer magnesium sulphate.
In these trials, the loading doses of magnesium sulphate given were either 4 grams or 6 grams.
Two trials did not use a maintenance dose (Mittendorf 2002 and Marret 2006) and two trials gave
maintenance doses of either 1 gram per hour (Crowther 2003) or 2 grams per hour (Rouse 2008).
No repeat dosing was given in three of the four trials (Mittendorf 2002; Crowther 2003 and Marret
2006). All trials used intravenous magnesium sulphate.
Table 7: Regimens of trials (Doyle 2009 Cochrane Review)
Study Loading
Dose
Maintenance
Dose
Repeat dosing Route Actual regimen given (in magnesium group)
Marret 2006
(PREMAG)
4 g (over 30 mins) none none IV 91% (259/286) given full dose
2% (7/286) given partial dose only
7% (20/286) not given magnesium sulphate
Mittendorf 2002 (MagNET)
4 g bolus none none IV Not reported
Crowther 2003
(ACTOMgSO4)
4 g (over 20 mins) 1 g/hour;
until birth or up to 24 hours, whichever was first
none IV 91% (484/535) given full loading dose
7% (38/535) given partial loading dose
84% (451/535) started maintenance dose
2% (13/535) women not given magnesium sulphate
Rouse 2008
(BEAM)
6 g (over 20-30 mins) 2 g/hour;
stopped if birth had not occurred in 12 hours and was no longer considered imminent
If contractions recurred, infusion was resumed at 2 g/hour; if at least 6 hours had passed since the discontinuation of magnesium, another loading dose was given
IV 91% (996/1,096) given magnesium sulphate for 3 h or more
8% (82/1,096) given magnesium sulphate 3 h before birth
2% (18/1,096) not given magnesium sulphate
(42.2% given repeat dose)

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 32
There was a significant reduction in the combined outcome of death or cerebral palsy; and of
cerebral palsy across all trials (RR 0.85; 95% CI 0.74 to 0.98 and RR 0.71; 95% CI 0.52 to 0.97; 4446
infants). Rouse 2008, which was considerably larger than the other trials, significantly contributed to
the finding of the overall reduction in cerebral palsy (RR 0.59; 95% CI 0.40 to 0.85; 2444 infants).
Table 8: Results of primary outcomes by regimen for trials (Doyle 2009 Cochrane Review)
Trial Regimen DEATH OR CEREBRAL PALSY
RR (95% CI)
CEREBRAL PALSY DEATH
Marret 2006; Mittendorf 2002
(n=747)
4 g (no maintenance);
Marret 2006 (over 30 mins);
Mittendorf 2002 (bolus)
1.45 (0.27 to 7.72)
1.37 (0.18 to 10.70)
0.88 (0.57 to 1.35)
Crowther 2003
(n=1255)
4 g (over 20 mins) plus 1 g/hour maintenance
0.82 (0.66 to 1.02)
0.85 (0.55 to 1.31)
0.81 (0.62 to 1.05)
Rouse 2008
(n=2444)
6 g (over 20-30 mins) plus 2 g/hour maintenance
0.90 (0.73 to 1.10)
0.59 (0.40 to 0.85)*
1.13 (0.87 to 1.48)
OVERALL
(n=4446)
0.85 (0.74 to 0.98)*
0.71 (0.52 to 0.97)*
0.95 (0.80 to 1.12)
*significantly in favour of magnesium sulphate
see Appendix F.6: evidence tables/graphs
Summary of evidence statement judgements for regimens
The evidence base for regimens used to administer magnesium sulphate to women at risk of
preterm birth for neuroprotection of their fetus, infant or child was judged to have a low risk of bias
despite some unexplained inconsistency between Marret 2006 and Mittendorf 2002 in subgroups.
For the combined outcome of death and cerebral palsy; and the outcome of cerebral palsy alone, in
the 4 g no maintenance subgroups, the effect was in opposite directions in the two trials (in favour
of magnesium sulphate in Marret, in favour of no magnesium sulphate in Mittendorf, with neither
result statistically significant).
The evidence was judged by the guideline panel to be both generalisable and applicable to the
Australian and New Zealand healthcare context.
Overall the clinical impact was judged to be very large, however, since differences in death and
cerebral palsy by regimen are unclear at present, no particular regimen subgroup was judged to
have any greater or lesser impact than another.
How the recommendation was formulated
Although the trial with higher loading dose with repeat treatment permitted (Rouse 2008) was the
only study to show statistical significance on its own (RR of cerebral palsy 0.59 95% CI 0.40 to 0.85),
it was unclear whether this was due to a dose effect or due to the size of the trial, (which was the
largest in the meta-analysis and therefore had more power to detect differences). However, the
case for a dose effect is weakened by the lack of a significant finding for the combined outcome of
death or cerebral palsy (RR 0.90 95% CI 0.73 to 1.10).

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 33
Because of this uncertainty, the guideline panel felt it prudent to restrict magnesium sulphate
administration to the lowest loading dose (4 g) used with a maintenance dose (again based on the
lowest maintenance dose of 1 g/hour). Therefore the guideline panel recommends that magnesium
sulphate should only be given for neuroprotection as a 4 g loading dose slowly over 20-30 minutes
with 1 gram per hour maintenance dose and with no immediate repeat doses, via intravenous route.
This should be continued up until birth or within 24 hours, whichever comes first.
The loading regimen of 4 g magnesium sulphate is identical to loading doses commonly used
throughout Australia, New Zealand and elsewhere to treat women with pre-eclampsia (see Appendix
H). The maintenance dose of 1 g/hr of magnesium sulphate is consistent with maintenance doses
commonly used throughout Australia and New Zealand to treat women with pre-eclampsia and
eclampsia (see Appendix H).
There is considerable variation in the method of giving the loading doses (by either infusion pump or
syringe pump). A time period of 20-30 minutes for infusion of a 4 g loading dose is recommended
for women with pre-eclampsia (see Appendix H).
Appendix F. 6: Evidence tables/graphs
CLINICAL RECOMMENDATION GRADE
In women at risk of early preterm* imminent#
birth, use magnesium sulphate for neuroprotection of the fetus, infant or child:
intravenously with a 4 gram loading dose (slowly over 20-30 minutes) and 1 gram per hour maintenance dose via intravenous route, with no immediate repeat doses. Continue regimen up until birth or for 24 hours, whichever comes first.
*see chapter 8 #
see chapter 9
C
GOOD PRACTICE POINTS
Urgent delivery
In situations where urgent delivery is necessary because of actual or imminent maternal or fetal
compromise (e.g. severe fetal distress or antepartum haemorrhage), then birth should not be
delayed to administer magnesium sulphate.
Repeat doses
In the event that birth does not occur after giving magnesium sulphate for neuroprotection of the
infant, and preterm birth (less than 30 weeks’ gestation) again appears imminent (planned or
definitely expected within 24 hours), a repeat dose of magnesium sulphate may be considered at the
discretion of the attending health professional.
Locations of administration of antenatal magnesium sulphate (Chapter 10)
The locations of administration of antenatal magnesium sulphate intravenously to women should be
determined by each individual maternity facility.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 34
Monitoring
During administration of magnesium sulphate intravenously, women should be regularly assessed as
detailed in individual obstetric unit protocols. Resuscitation and ventilatory support should be
immediately available, if needed, during administration of magnesium sulphate. Should hypotension
or respiratory depression occur prompt medical review is recommended. This may include cessation
of magnesium sulphate.
Loading
A minimum assessment should include checking pulse, blood pressure, respiratory rate and patellar
reflexes before loading dose, 10 minutes after loading dose infusion has started and at the end of
the loading dose infusion (20-30 minutes). The infusion should be stopped if respiratory rate
decreases more than 4 breaths per minute below baseline, or is less than 12 breaths per minute; or
diastolic blood pressure decreases more than 15 mm Hg below baseline level (Crowther 2003).
Maintenance
While the maintenance infusion is running, observe for any adverse effects. The minimum
assessments should include checking pulse, blood pressure, respiratory rate, patellar reflexes and
urine output 4-hourly. Stop infusion if respiratory rate is less than 12 breaths per minute; if patellar
reflexes are absent, if hypotension occurs or if urine output is less than 100 mLs over 4 hours.
Toxicity
Magnesium toxicity is unlikely with the regimens recommended in these guidelines and serum
magnesium concentrations do not need to be routinely measured (RCOG 2006). In women with
renal compromise, serum magnesium monitoring is recommended.
Calcium gluconate (1 gram (10 mL of 10% solution) slowly via intravenous route over 10 minutes)
can be given if there is clinical concern over respiratory depression.
Potential interactions (Chapter 10) There is a potential theoretical interaction between magnesium sulphate and nifedipine of
hypotension and neuromuscular blockade effects (Snyder & Cardwell 1989; Ben-Ami 1994), although
this is seldom reported in clinical practice. Regular monitoring of the woman is recommended as
detailed in individual obstetric unit protocols. If hypotension occurs, nifedipine and magnesium
sulphate should cease and the woman reviewed by a medical practitioner.
IMPLEMENTATION IMPLICATIONS
Australian and New Zealand clinicians are less likely to be comfortable using loading doses higher
than 4 gram.
Monitoring women after they have been given antenatal infusions of magnesium sulphate is usually
recommended. Monitoring formed part of the published study methods for two of the included
randomised controlled trials (Crowther 2003 and Marret 2006) – see Appendix H. There is, however,
no consensus on what form this monitoring should take. For example the Society of Obstetric
Medicine of Australia and New Zealand (SOMANZ) state that obstetric units should determine their
own protocols for monitoring outcomes (SOMANZ 2008 [also see Appendix H]). As toxicity is
unlikely with the regimens recommended in these guidelines, routine monitoring of serum
magnesium sulphate concentrations should not be required.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 35
FURTHER RESEARCH RECOMMENDATIONS
Individual triallists should be approached to provide unpublished optimal treatment
regimens.
Individual patient data meta-analysis can be used to explore whether different magnesium
sulphate regimens result in different rates of adverse outcomes such as cerebral palsy and
combined death and cerebral palsy.
Further randomised trials of regimens are required, specifically comparing:
o loading dose versus loading dose plus maintenance
o different loading doses (4 gram versus 6 gram)
o use of repeat doses of magnesium sulphate.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 36
Chapter 11: Number of Babies in Utero (Question 7)
Question 7: Do improvements to the fetus, infant, and child vary by number of babies in utero?
This chapter summarises the evidence from the four individual neuroprotective intent trials within
the Doyle 2009 Cochrane review for the number of babies in utero.
All four trials included twins; two trials also included higher order multiple gestations (Crowther
2003 and Marret 2006). Only Crowther 2003 and Rouse 2008 reported death separately as an
outcome for single and multiple pregnancies and only Crowther 2003 reported cerebral palsy
outcomes separately for these groups.
Table 9: Plurality of trials (Doyle 2009 Cochrane Review)
Study Single Twin Higher order Reported separately
Crowther 2003 Yes Yes Yes (triplet+quad) Single vs multiple
Rouse 2008 Yes Yes No Single vs twin++
Marret 2006 Yes Yes Yes (triplet) No
Mittendorf 2002 Yes Yes No No
Table 10: Results of primary outcomes by plurality for trials (Doyle 2009 Cochrane Review)
Number of babies in utero
DEATH or CEREBRAL PALSY
CEREBRAL PALSY DEATH
RR (95% CI)
Multiple 0.73 (0.50 to 1.08)
Crowther 2003
0.52 (0.21 to 1.25)
Crowther 2003
0.90 (0.63 to 1.31)
Crowther 2003,
Rouse 2008
Single 0.86 (0.67 to 1.11)
Crowther 2003
1.01 (0.61 to 1.68)
Crowther 2003
0.96 (0.68 to 1.37)
Crowther 2003,
Rouse 2008
Multiple and single 0.88 (0.74 to 1.05)
Marret 2006, Mittendorf 2002, Rouse 2008
0.65 (0.48 to 0.88)*
Marret 2006, Mittendorf 2002, Rouse 2008
0.88 (0.57 to 1.35)
Marret 2006, Mittendorf 2002
OVERALL 0.86 (0.75 to 0.98)* 0.71 (0.55 to 0.91)* 0.94 (0.79 to 1.12) ++
Rouse 2008 reported only moderate to severe cerebral palsy, (not all cerebral palsy) so plurality data from Rouse can only be reported for the outcome of death.
Appendix F.7: Evidence tables/graphs

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 37
Summary of evidence statement judgements for number of babies in utero subgroup of infant
neuroprotection
The subgroup analyses come from trials with low risk of bias, and results between trials are fairly
consistent. While evidence is applicable, generalisability to the Australian and New Zealand context
was reduced since the majority of the women in the largest trial had PPROM (and therefore
represented a narrower subset of women at risk of preterm birth).
Overall clinical impact was judged to be very large, but since any differences in death and cerebral
palsy by number of babies in utero is unclear at present, no particular subgroup was judged to have
any greater or lesser impact than another.
The guideline panel therefore recommends that magnesium sulphate be used regardless of plurality.
Appendix F.7: Evidence statements
CLINICAL RECOMMENDATION GRADE
In women at risk of early preterm* imminent# birth, use magnesium sulphate for neuroprotection of the fetus, infant or child:
regardless of plurality (number of babies in utero).
*see chapter 8 # see chapter 9
B
IMPLEMENTATION IMPLICATIONS
As for Chapter 7.
FURTHER RESEARCH RECOMMENDATIONS
If triallists collected data on plurality, these data should be obtained and aggregate analyses
conducted.
Individual patient data meta-analysis can be used to explore whether differences in plurality
result in different rates of adverse outcomes such as cerebral palsy and combined death and
cerebral palsy.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 38
Chapter 12: Reasons Women (at less than 30 weeks gestation)
Considered at Risk of Preterm Birth (Question 8)
Question 8: Do improvements to the fetus, infant, and child vary by reason women (at less than 30 weeks gestation) considered to be at risk of preterm birth?
At this stage there is insufficient evidence to identify the reasons women were considered at risk of
preterm birth and included in studies relating to the administration of magnesium sulphate.
See Appendix F.8
CLINICAL RECOMMENDATION GRADE
In women at risk of early preterm* imminent# birth, use magnesium
sulphate for neuroprotection of the fetus, infant or child:
regardless of reason women considered (at less than 30 weeks’ gestation) to be at risk of preterm birth.
*see chapter 8 # see chapter 9
B
IMPLEMENTATION IMPLICATIONS
As for chapter 7.
FURTHER RESEARCH RECOMMENDATIONS
If triallists collected data on reasons women were considered to be at risk of preterm birth,
these data should be obtained and aggregate analyses conducted.
Individual patient data meta-analysis can be used to explore whether differences in reasons
women were considered to be at risk of preterm birth result in different rates of adverse
outcomes such as cerebral palsy and combined death and cerebral palsy.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 39
Chapter 13: Parity (Question 9)
Question 9: Do improvements to the fetus, infant, and child vary by parity of women?
Parity of women was not reported in any of the trials included in the Doyle 2009 Cochrane review.
At this stage there is insufficient evidence to identify whether parity is a significant factor in the use
of magnesium sulphate.
See Appendix F.9
CLINICAL RECOMMENDATION GRADE
In women at risk of early preterm* imminent#
birth, use magnesium sulphate for neuroprotection of the fetus, infant or child:
regardless of parity (number of previous births for the woman).
*see chapter 8 #
see chapter 9
B
IMPLEMENTATION IMPLICATIONS
As for Chapter 7.
FURTHER RESEARCH RECOMMENDATIONS
If triallists collected data on parity, these data should be obtained and aggregate analyses
conducted.
It may be possible to elucidate any influence of parity through individual patient data meta-
analysis.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 40
Chapter 14: Mode of Birth (Question 10)
Question 10: Do improvements to the fetus, infant, and child vary by mode of birth?
This chapter summarises the evidence from the four individual neuroprotective intent trials within
the Doyle 2009 Cochrane review for mode of birth.
Three of the four trials (Crowther 2003, Marret 2006 and Rouse 2008) reported mode of birth
(caesarean section and vaginal birth), but not outcomes for the child by mode of birth.
Mode of birth as an outcome
Overall there was no significant difference in mode of birth between women given magnesium
sulphate and those not given magnesium sulphate. When the three trials are pooled, the results are
non-significant, ranging from a 7% decrease to a 7% increase in the number of caesarean sections
(RR 1.00 95% CI 0.93 to 1.07).
At present there is insufficient evidence to show whether the use of magnesium sulphate has any
influence on the mode of birth.
See Appendix F:10
Table 11: Results of primary outcomes by mode of birth for trials (Doyle 2009 Cochrane Review)
Trial Caesarean Section Vaginal Birth
RR (95% CI)
Crowther 2003
(n=1062 women)
0.98 (0.88 to 1.10) 1.02 (0.90 to 1.17)
Marret 2006
(n=564 women)
1.17 (0.95 to 1.46) 0.91 (0.80 to 1.03)
Rouse 2008
(n=2241 women)
0.97 (0.88 to 1.08) 1.02 (0.95 to 1.09)
OVERALL (n=3867) 1.00 (0.93 to 1.07) 1.00 (0.95 to 1.06)
Mode of birth as an effect modifier
It is possible that the neuroprotective effect of antenatal magnesium sulphate may be modified by
mode of birth. Elective caesarean section has been shown to be associated with reduced neonatal
encephalopathy (Badawi 1998) and there is some suggestion in the literature that caesarean section
may be associated with improved survival and improved neurodevelopmental outcomes for
extremely low birthweight infants (Wilson-Costello 2007).

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 41
CLINICAL RECOMMENDATION GRADE
In women at risk of early preterm* imminent#
birth, use magnesium sulphate for neuroprotection of the fetus, infant or child:
regardless of anticipated mode of birth.
*see chapter 8 #
see chapter 9
B
IMPLEMENTATION IMPLICATIONS
As for Chapter 7.
FURTHER RESEARCH RECOMMENDATIONS
Any modifying effect of mode of birth on neurodevelopmental outcomes could be explored in the
trials included in the Doyle 2009 Cochrane review through a four-way comparison of:
o caesarean births in the magnesium sulphate groups
o caesarean births in the placebo/no treatment groups
o vaginal births in the magnesium sulphate groups
o vaginal births in the placebo/no treatment groups.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 42
Chapter 15: Effect of Antenatal Corticosteroids (Question 11)
Question 11: Do improvements to the fetus, infant, and child vary by combined effect of antenatal corticosteroids and magnesium sulphate?
Table 12: Results of primary outcomes by corticosteroid use for trials (Doyle 2009 Cochrane Review)
Trial High use of antenatal corticosteroids
Crowther 2003 yes
Rouse 2008 yes
Marret 2006 yes
Mittendorf 2002 unknown
At this stage there is insufficient evidence to identify any effect on outcomes when antenatal
corticosteroids have been used.
See Appendix F:11
CLINICAL RECOMMENDATION GRADE
In women at risk of early preterm* imminent# birth, use magnesium sulphate for neuroprotection of the fetus, infant or child:
whether or not antenatal corticosteroids have been given.
*see chapter 8 # see chapter 9
B
IMPLEMENTATION IMPLICATIONS
As for Chapter 7.
FURTHER RESEARCH RECOMMENDATIONS
Further data on antenatal corticosteroid use should be obtained from individual triallists and
aggregate analyses conducted.
Individual patient data meta-analysis can be used to explore whether differences in use of
antenatal corticosteroids result in different rates of adverse outcomes such as cerebral palsy
and combined death and cerebral palsy.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 43
References
References to included RCTs
Crowther 2003
a) Crowther CA, Hiller JE, Doyle LW, Haslam RR for the Australasian Collaborative Trial of
Magnesium Sulphate (ACTOMgSO4) Collaborative Group. Effect of magnesium sulfate given for
neuroprotection before preterm birth. JAMA 2003;290(20):2669-76.
b) Crowther CA, Hiller JE, Doyle LW for the ACTOMgSO4 Collaborators Group. Does prenatal
magnesium sulphate reduce the risk of mortality and cerebral palsy in infants born at less than
30 weeks' gestation? - The ACTOMgS04 trial. Perinatal Society of Australia and New Zealand 7th
Annual Congress; 2003 March 9-12; Tasmania, Australia. 2003:A4.
c) Paradisis M, Evans N, Osborn D, Kluckow M, ACTOMgSO4 Collaborators Group. The effect of
antenatal magnesium sulphate on early systemic blood flow in very preterm infants. Pediatric
Research 2004;55 Suppl:114.
d) Smith CA, Crowther CA, Willson K, Hiller JE, Doyle LW. Placental transfer of magnesium
sulphate: a randomised placebo controlled trial. Perinatal Society of Australia and New Zealand
7th Annual Congress; 2003 March 9-12; Tasmania, Australia. 2003:P48.
Marret 2006
a) Marret S, Marpeau L, Zupan-Simunek V, Eurin D, Lévêque C, Hellot MF, et al. Magnesium sulfate
given before very-preterm birth to protect infant brain: the randomized, controlled PREMAG
trial. BJOG: an international journal of obstetrics and gynaecology 2007; Vol. 114, issue 3:310-8.
b) Marret S, Marpeau L, Astruc D, Cambonie G, Follet C, Benichou J. Prenatal magnesium sulfate
(MgSO4) and follow up at two years of age in preterm infants: the randomised controlled
PREMAG trial. Pediatric Academic Societies Annual Meeting; 2007 May 5-8; Toronto, Canada.
c) Marret S, Marpeau L, Benichou J. Benefit of magnesium sulfate given before very preterm birth
to protect infant brain. Pediatrics 2008;121(1):225-6.
d) Marret S, Marpeau L, Follet-Bouhamed C, Cambonie G, Astruc D, Delaporte B, et al. for the
PREMAG Group. Effect of magnesium sulphate on mortality and neurologic morbidity of the
very=preterm newborn with two-year neurological outcome: results of the prospective
PREMAG trial [Effet du sulfate de magnésium sur la mortalité et la morbidité neurologique chez
le prématuré de moins de 33 semaines, avec recul è deux ans: résultats de l'essai prospectif
multicentrique contre placebo PREMAG]. Gynécologie Obstétrique & Fertilité 2008;36:278-88.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 44
e) Marret S, Zupan V, Marpeau L, Adde-Michel C, Benichou J, the Premag Trial Group. Prenatal
magnesium sulphate (MgSO4) and neuroprotection in preterm infants: a randomized controlled
trial. Pediatric Academic Societies Annual Meeting; 2005 May 14-17; Washington DC, USA.
Mittendorf 2002
a) Mittendorf R, Dambrosia J, Pryde PG, Lee KS, Gianopoulos JG, Besinger RE, et al. Association
between the use of antenatal magnesium sulfate in preterm labor and adverse health outcomes
in infants. American Journal of Obstetrics and Gynecology 2002;186(6):1111-8.
b) Mittendorf R, Bentz L, Borg M, Roizen N. Does exposure to antenatal magnesium sulfate
prevent cerebral palsy? American Journal of Obstetrics and Gynecology 2000;182(1 Pt 2):S20.
c) Mittendorf R, Bentz L, Kohn J, Covert R. Use of antenatal magnesium sulfate does not seem to
prevent intraventricular hemorrhage. American Journal of Obstetrics and Gynecology
2000;182(1 Pt 2):S34.
d) Mittendorf R, Besinger R, Santillan M, Gianopoulos J. When used in circumstance of preterm
labor, is there a paradoxical effect of varying exposures to magnesium sulfate (MGSO4) on the
developing human brain? American Journal of Obstetrics and Gynecology 2005;193(6
Suppl):S65.
e) Mittendorf R, Covert R, Boman J, Khoshnood B, Lee KS, Siegler M. Is tocolytic magnesium
sulphate associated with increased total paediatric mortality? Lancet 1997;350(9090):1517-8.
f) Mittendorf R, Covert R, Elin R, Pryde P, Khoshnood B, Sun-Lee K. Umbilical cord serum ionized
magnesium level and total pediatric mortality. Obstetrics & Gynecology 2001;98:75-8.
g) Mittendorf R, Dambrosia J, Dammann O, Pryde PG, Lee KS, Ben-Ami TE, et al. Association
between maternal serum ionized magnesium levels at delivery and neonatal intraventricular
hemorrhage. Journal of Pediatrics 2002;140(5):540-6.
h) Mittendorf R, Dambrosia J, Khoshnood B, Lee KS, Pryde P, Yousefzadeh D. Association between
magnesium and intraventricular haemorrhage. American Journal of Obstetrics and Gynecology
2001;184(1):S188.
i) Mittendorf R, Dambrosia J, Khoshnood B, Lee K-S, Pryde P, Yousefzadeh D. Magnesium sulfate is
no more efficacious than other tocolytic agents. American Journal of Obstetrics and Gynecology
2001;184(1):S188.
j) Mittendorf R, Janeczek S, Macmillan W, Gianopoulos J, Besinger R, Karlman R, et al.
Mechanisms of mortality in the magnesium and neurologic endpoints trial (Magnet trial): fetal
inflammatory response syndrome (firs). American Journal of Obstetrics and Gynecology
2001;185(6 Suppl):S151.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 45
k) Mittendorf R, Kuban K, Pryde PG, Gianopoulos JG, Yousefzadeh D. Antenatal risk factors
associated with the development of lenticulostriate vasculopathy (lsv) in neonates. Journal of
Perinatology 2005;25(2):101-7.
l) Mittendorf R, Pryde P, Khoshnood B, Lee KS. If tocolytic magnesium sulfate is associated with
excess total pediatric mortality, what is its impact? Obstetrics & Gynecology 1998;92(2):308-
11.
m) Mittendorf R, Pryde P, Lee KS, Besinger R, Macmillan W, Karlman R, et al. Umbilical cord serum
ionized magnesium levels at delivery are not correlated with neuroprotection in childhood.
American Journal of Obstetrics and Gynecology 2002;187(6 Pt 2):S74.
n) Mittendorf R, Pryde P, Lee K-S, Besinger R, MacMillan W, Karlman R, et al. Coagulase negative
staphylococci cultured from the placental chorioamnion space at delivery are associated with
lower bayley scores. American Journal of Obstetrics and Gynecology 2002;187(6 Pt 2):S131.
o) Santillan M, Besinger RE, Gianopoulos JG, Mittendorf R. An inverse correlation between
umbilical cord blood ionized magnesium (IMG) and interleukin-6 (IL-6) levels could not be
confirmed in the human. American Journal of Obstetrics and Gynecology 2005;193(6
Suppl):S183.
Rouse 2008
a) Rouse D, Hirtz D, Thom E, Varner M, Alexander J, Spong C, Mercer B, Iams J, Wapner R, Sorokin
Y, Harper M, Thorp J, Ramin S, Malone F, Carpenter M, Miodovnik A, Moawad A, O'Sullivan M,
Peaceman A, Hankins G, Langer O, Caritis S, Roberts J. Magnesium sulfate for the prevention of
cerebral palsy. New England Journal of Medicine 2008;359:895-905.
b) Rouse D. A randomized controlled trial of magnesium sulfate for the prevention of cerebral
palsy. American Journal of Obstetrics and Gynecology 2007;197(6):S2.
c) Rouse DJ, Hirtz DG, Thom E, Varner MW, Spong CY, Mercer BM et al. A randomized, controlled
trial of magnesium sulphate for the prevention of cerebral palsy. Obstetrical & Gynecological
Survey 2009;64(1):15-7.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 46
Other References
Access Economics 2008
Access Economics. The Economic Impact of Cerebral Palsy in Australia in 2007: Report for Cerebral
Palsy Australia. Sydney: Cerebral Palsy Australia, April 2008.
Australian Cerebral Palsy Register Group 2009
Australian Cerebral Palsy Register Group. Report of the Australian Cerebral Palsy Register, Birth Years
1993 – 2003, Sydney: CP Register, December 2009.
AIHW 2009
Australian Institute of Health and Welfare (AIHW). Australia’s mothers and babies 2007. Sydney:
AIHW National Perinatal Statistics, December 2009.
Badawi 1998
Badawi N, Kurinczuk JJ, Keogh JM, Alessandri LM, O’Sullivan F, Burton PR, Pemberton PJ, Stanley FJ.
Intrapartum risk factors for newborn encelopathy: the Western Australian case-control study. BMJ
1998;317:1554-8.
Ben-Ami 1994
Ben-Ami M, Giladi Y, Shalev E. The combination of magnesium sulphate and nifedipine: a cause of neuromuscular blockade. British Journal of ObstetrIcs and Gynaecology 1994;101(3):262-3.
Canterino 1999 Canterino JC, Verma UL, Visintainer PF, Figueroa R, Klein SA, Tejani NA. Maternal magnesium sulfate
and the development of neonatal periventricular leucomalacia and intraventricular hemorrhage.
Obstetrics & Gynecology 1999;93:396-402
Costantine 2009
Costantine MM, Weiner SJ. Effects of antenatal exposure to magnesium sulphate on
neuroprotection and mortality in preterm infants. Obstetrics and Gynecology 2009;114(2 part
1):354-64.
Crowther 1998
Crowther CA, Moore V. Magnesium maintenance therapy for preventing preterm birth after
threatened preterm labour. Cochrane Database of Systematic Reviews 1998, Issue 1.
Crowther 2002
Crowther CA, Hiller JE, Doyle LW. Magnesium sulphate for preventing preterm birth in threatened
preterm labour. Cochrane Database of Systematic Reviews 2002, Issue 4.
Doyle 2001
Doyle LW, for the Victorian Infant Collaborative Study Group. Outcome at 5 years of age of children
23 to 27 weeks' gestation: refining the prognosis. Pediatrics 2001;108(1):134-41.
Doyle 2009
Doyle LW, Crowther CA, Middleton P, Marret S, Rouse D. Magnesium sulphate for women at risk of
preterm birth for neuroprotection of the fetus. Cochrane Database of Systematic Reviews 2009,
Issue 1.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 47
Duley 2003 Duley L, Gülmezoglu AM, Henderson-Smart DJ. Magnesium sulphate and other anticonvulsants for
women with pre-eclampsia. Cochrane Database of Systematic Reviews 2003, Issue 2.
Espinoza 1991
Espinoza MI, Parer JT. Mechanisms of asphyxial brain damage, and possible pharmacologic
interventions, in the fetus. American Journal of Obstetrics and Gynecology 1991;164(6 Pt 1):1582-9.
Finesmith 1997
Finesmith RB, Roche K, Yellin PB, Walsh KK, Shen C, Zeglis M, et al. Effect of magnesium sulfate on
the development of cystic periventricular leukomalacia in preterm infants. American Journal of
Perinatology 1997;14(5):303-7.
Grether 1998
Grether JK, Hoogstrate J, Selvin S, Nelson KB. Magnesium sulfate tocolysis and risk of neonatal
death. American Journal of Obstetrics and Gynecology 1998;178(1 Pt 1):1-6.
Grether 2000
Grether JK, Hoogstrate J, Walsh-Greene E, Nelson KB. Magnesium sulfate for tocolysis and risk of
spastic cerebral palsy in premature children born to women without preeclampsia. American Journal
of Obstetrics and Gynecology 2000;183(3):717-25.
Hauth 1995
Hauth JC, Goldenberg RL, Nelson KG, DuBard MB, Peralta MA, Gaudier FL. Reduction of cerebral
palsy with maternal MgSO4 treatment in newborns weighing 500-1000g [abstract]. American Journal
of Obstetrics and Gynecology 1995;172(1 Pt 2):419.
Kimberlin 1998
Kimberlin DF, Hauth JC, Goldenberg RL, Bottoms SF, Iams JD, Mercer B, et al. The effect of maternal
magnesium sulfate treatment on neonatal morbidity in < or = 1000-gram infants. American Journal
of Perinatology 1998;15:635-41.
Kuban 1992
Kuban KCK, Leviton A, Pagano M, Fenton T, Strasfeld R, Wolff M. Maternal toxemia is associated with
reduced incidence of germinal matrix hemorrhage in premature babies. Journal of Child Neurology
1992;7:70-6.
Levene 1995
Levene M, Blennow M, Whitelaw A, Hanko E, Fellman V, Hartley R. Acute effects of two different
doses of magnesium sulphate in infants with birth asphyxia. Archives of Disease in Childhood. Fetal
Neonatal Edition 1995;73:F174-F177
Lipsitz 1971
Lipsitz P. The clinical and biochemical effects of excess magnesium in the newborn. Pediatrics
1971;47:501-9.
McDonald 1990
McDonald JW, Silverstein FS, Johnston MV. Magnesium reduces N-methyl-d-aspartate (NMDA)-
mediated brain injury in perinatal rats. Neuroscience Letters 1990, 109 234-238.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 48
McDonnell 2009
McDonnell NJ. Cardiopulmonary arrest in pregnancy: two case reports of successful outcomes in
association with perimortem Caesarean delivery. British Journal of Anaesthesia 2009;103(3):406-9.
McIntosh 1989
McIntosh T, Vink R, Yamakami I, Faden A. Magnesium protects against neurological deficit after brain
injury. Brain Research 1989;482:252-60.
McIntyre 2009
McIntyre S, Novak I, Cusick A. Consensus research priorities for cerebral palsy: a Delphi survey of
consumers, researchers, and clinicians. Developmental Medicine & Child Neurology 2009; August 20;
Ahead of print.
Mildvan 1987
Mildvan AS. Role of magnesium and other divalent cations in ATP-utilizing enzymes. Magnesium
1987;6(1):28-33.
National Center for Health Statistics 2009
National Center for Health Statistics, Births: Final data for 2006, National Vital Statistics Reports; Vol.
57, No.7.
Nelson 1995
Nelson KB, Grether JK. Can magnesium sulfate reduce the risk of cerebral palsy in very low
birthweight infants? Pediatrics 1995;95:1-1
New Zealand Health Information Service 2006
New Zealand Health Information Service (2006). Report on Maternity Maternal and Newborn
Information 2003. Wellington, NZ: NZHIS.
NZGG 2001
Handbook for the Preparation of Explicit Evidence-Based Clinical Practice Guidelines. New Zealand
Guideline Group. 2001.
O'Shea 1998
O'Shea TM, Klinepeter KL, Meis PJ, Dillard RG. Intrauterine infection and the risk of cerebral palsy in
very low-birthweight infants. Paediatric and Perinatal Epidemiology 1998;12(1):72-83.
Paneth 1997
Paneth N, Jetton J, Pinto-Martin J, Susser M. Magnesium sulfate in labor and risk of neonatal brain
lesions and cerebral palsy in low birth weight infants. The Neonatal Brain Hemorrhage Study Analysis
Group. Pediatrics 1997;99(5):E1.
Perlman 1994
Perlman J, Fermandez C, Gee J, LeVeno K, Risser R. Magnesium sulphate administered to mothers
with pregnancy-induced hypertension is associated with a reduction in periventricular-
intraventricular hemorrhage [abstract]. Pediatric Research 1994;37:231A.
RCOG 2006
RCOG. The management of severe preeclampsia/eclampsia. Royal College of Obstetricians and
Gynaecologists (RCOG) Guideline No. 10(A) March 2006. London, UK: RCOG, 2006.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 49
Saigal 2008
Saigal S, Doyle L. An overview of mortality and sequelae of preterm birth from infancy to adulthood.
Lancet 2008; 371: 261–9.
Schendel 1996
Schendel DE, Berg CJ, Yeargin-Allsopp M, Boyle CA, Decoufle P. Prenatal magnesium sulfate
exposure and the risk for cerebral palsy or mental retardation among very low-birth-weight children
aged 3 to 5 years. JAMA 1996;276(22):1805-10.
Snyder & Cardwell 1989
Snyder SW, Cardwell MS. Neuromuscular blockade with magnesium sulphate and nifedipine.
American Journal of Obstetrics and Gynecology 1989;161(1):35-6.
Stanley 1992
Stanley F. Survival and cerebral palsy in low birthweight infants: implications for perinatal care.
Paediatric and Perinatal Epidemiology 1992;6(2):298-310.
Vermeulen 2001
Vermeulen GM, Bruinse HW, de Vries LS. Perinatal risk factors for adverse neurodevelopmental
outcome after spontaneous preterm birth. European Journal of Obstetrics & Gynecology and
Reproductive Biology 2001; 99:207-12.
Weintraub 2001
Weintraub Z, Solovechick M, Reichman B, Rotschild A, Waisman D, Davkin O, et al. Effect of maternal
tocolysis on the incidence of severe periventricular/intraventricular haemorrhage in very low
birthweight infants. Archives of Disease in Childhood. Fetal and Neonatal Edition 2001;85:F13-7.
Wilson-Costello 2007
Wilson-Costello D, Friedman H, Minich N, Siner B, Taylor G, Schluchter M, Hack M. Improved
neurodevelopmental outcomes for extremely low birth weight infants in 2000-2002. Pediatrics
2007;119:37-45.
Wiswell 1996
Wiswell TE, Graziani LJ, Caddell JL, Vecchione N, Stanley C, Spitzer AR. Maternally administered
magnesium sulphate protects against early brain injury and long-term adverse neurodevelopmental
outcomes in preterm infants. A prospective study. Pediatric Research 1996;39:253A.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 50
Appendix A: Process and Methods
Overview of the guideline development process
There was a recognised urgent need for guidelines on the use of magnesium sulphate for
neuroprotection to assist clinical decision making. Since there were no known existing guidelines
suitable for adaptation, a group of experts in their fields met on 17 September 2009 at the University
of Adelaide to discuss developing guidelines. Present at the meeting were Professor Caroline
Crowther, Ms Philippa Middleton, Professor Peter Davis, Associate Professor Vicki Flenady, Dr Lisa
Askie, Dr Helena Oakey, Dr Neil Hotham, Dr Dell Horey and Dr Jane Alsweiler. At this meeting the
group discussed the establishment of a multidisciplinary expert advisory panel to oversee the
development of the guidelines, defined the Panel’s purpose, identified the clinical questions and
harms that needed to be considered and established a process for developing the guidelines.
Establishing the Expert Advisory Panel
A multidisciplinary panel was established to oversee the development of the guidelines.
Representation was invited from:
Health professionals in the fields of maternal fetal medicine, obstetrics, midwifery,
neonatology and neonatal nursing;
Relevant allied health practitioners e.g. pharmacist;
Research methodology experts including epidemiologists and a biostatistician;
Consumer representatives;
Representatives from professional colleges and bodies (RANZCOG; ACM; NZCOM; RACP;
ACNN; and WHA).
Purpose of the Panel
The purpose of the Antenatal Magnesium Sulphate Prior to Preterm Birth for Neuroprotection of the
Fetus, Infant, and Child Guideline Development Panel was to prepare a guideline on best practice for
clinical care on the use of magnesium sulphate prior to preterm birth. The guidelines are relevant for
health professionals who care for women at risk of preterm birth and their babies, pregnant women
and their partners, and policy makers in maternity care.
Clinical Questions Defined
Does the administration of magnesium sulphate to women prior to preterm birth:
Improve the health outcomes for the fetus/infant/child?
Cause adverse outcomes for the women?
Cause adverse outcomes for the fetus/infant/child?
Do any improvements for the fetus/infant/child vary by:
o Gestational age magnesium sulphate given?
o Time magnesium sulphate planned to be given prior to birth?
o Dose regimen planned?
o Number of babies in-utero?
o Reason women considered at risk of preterm birth (preterm labour, preterm
prelabour rupture of the membranes, antepartum haemorrhage, pre-eclampsia, fetal
compromise; maternal factors)?

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 51
o Parity of the women?
o Mode of birth?
o Use of antenatal corticosteroids?
Draft Health Outcomes Considered for the Guidelines:
Death and neurosensory disability (including cerebral palsy, blindness, deafness,
developmental delay) for the fetus, infant, and child.
Harmful effects by the therapy for the woman and the child (maternal respiratory
depression, cardiac arrest, hypotension, side effects, and fetal/neonatal side effects.
Resources needed and economic component.
Literature Review Process
It was agreed to follow NHMRC and NZGG guideline processes. There was a systematic identification
and synthesis of the best available scientific evidence. Evidence for effectiveness included systematic
reviews and randomised trials assessing outcomes of antenatal magnesium sulphate for fetal
neuroprotection. In addition, the substantial randomised literature for the use of magnesium
sulphate during pregnancy was assessed for evidence about harms of antenatal magnesium use for
mother and baby. Evidence statements (assessing evidence base, consistency, clinical impact,
generalisability, applicability and draft recommendations) were prepared, and then discussed by the
panel, for each of the clinical questions.
Summary of timeline:
12 Oct 2009 – input sought by email from full panel.
16 Oct 2009 – subsequent drafts discussed by teleconference.
12 Nov 2009 – face to face meeting in Sydney.
19 Dec 2009 – 18 Jan 2010: public consultation of draft guidelines.
12 Dec 2009 – open meeting in Adelaide.
Jan/Feb 2010 – final guideline document.
March 2010 – draft guidelines released.
17 November 2010 – NHMRC approved guidelines.
Appointment of the Panel
On 16 October 2009 the Guideline Panel met via teleconference. Prior to the meeting Panel
members were required to declare their conflict of interest (see p. 52). At the meeting the purpose
of the Panel was established, defined clinical questions were discuss and approved, the NHMRC
evidence statements process used to address these questions was explained and the ongoing process
for developing the guidelines was established.
Development of the Guidelines
Synthesis of new and existing evidence
The Cochrane Library was searched for relevant Cochrane reviews, other systematic reviews and
RCTs (last searched August 2008). PubMed was last searched in August 2008. References of
retrieved articles were checked for potentially relevant studies.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 52
Developing recommendations
The Guideline recommendations for each clinical question were developed using procedures outlined
in the “NHMRC additional levels of evidence and grades for recommendations for developers of
guidelines: Stage 2 consultation 2008 – 2010” (available from the NHMRC website). Each
recommendation was assigned a grade for ‘A’ to ‘D’. ‘A’ refers to a recommendation based on a
body of evidence that can be trusted to guide practice. ‘B’ refers to a recommendation based on a
body of evidence that can be trusted to guide practice in most situations. Grade ‘C’ means that the
body of evidence provides some support for the recommendation, but care should be taken in its
application. Grade ‘D’ means that the body of evidence is weak and the recommendation should be
applied with caution. Each recommendation was assigned a grade taking into account the volume,
consistency, generalisability, applicability and clinical impact of the body of evidence supporting each
recommendation. The standardised evidence statement form used to formulate and grade the
recommendations can be found in Appendix B.
Panel Member Input
Panel members provided input into the draft guideline document on an ongoing basis via email. The
executive group of the Panel met face to face on 12 November 2009 to consider the comments
received from the Panel and to consolidate the draft document. At this meeting the additional
clinical question ‘mode of birth’ was identified.
On 12 December 2009 a workshop was held in Adelaide attended by the Panel members and other
participants with an interest in magnesium sulphate guidelines. The purpose of the meeting was to
provide an overview of the evidence surrounding the use of magnesium sulphate for
neuroprotection, the need for the guidelines, the guideline development process and draft
recommendations, allow participants to provide input into the implementation implications, good
practice points, audit process and further research needed.
Public Consultation Process
The draft Guideline document was released for public consultation in December 2009, published
through The Australian national newspaper and made available on the Australian Research Centre
for Health of Women and Babies (ARCH) website. Public consultation closed on 18 January 2010.
Response to feedback and completion of final guideline document
Material provided through the public consultation process was incorporated into the Guideline
document. A summary of the public consultation comments and Panel member responses are
provided in Appendix I.
Declarations of competing interest of the guideline panel members
Professor Caroline Crowther
Chief Investigator for the Australian Collaborative Trial of Magnesium Sulphate (ACTOMgSO4)
funded through the National Health and Medical Research Council (NHMRC) Project Grant
3503267.
Co-author for the Cochrane Review ‘Magnesium sulphate for preventing preterm birth in
threatened preterm labour’.
Co-author for the Cochrane Review ‘Magnesium sulphate for women at risk of preterm birth
for neuroprotection of the fetus’.
Co-author for the Cochrane Review ‘Magnesium maintenance therapy for preventing
preterm birth after threatened preterm labour’.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 53
Co-author on updates of other Cochrane Reviews assessing antenatal use of magnesium
sulphate.
Professor Lex Doyle
Co-author for the Cochrane Review ‘Magnesium sulphate for women at risk of preterm birth
for neuroprotection of the fetus’.
Co-author for the Cochrane Review ‘Magnesium sulphate for preventing preterm birth in
threatened preterm labour’.
Investigator for the ACTOMgSO4 trial.
Co-author on updates of other Cochrane Reviews assessing antenatal use of magnesium
sulphate.
Professor Lesley McCowan
Assisted in the coordination of the ACTOMgSO4 trial in New Zealand.
Ms Philippa Middleton
Co-author for the Cochrane Review ‘Magnesium sulphate for women at risk of preterm birth
for neuroprotection of the fetus’.
Co-author on updates of other Cochrane Reviews assessing antenatal use of magnesium
sulphate.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 54
Appendix B: How to use the NHMRC Evidence Statement Form
Step 1 — Rate each of the five components
Applying evidence in real clinical situations is not usually straightforward. Consequently guideline
developers find that the body of evidence supporting a recommendation rarely consists of entirely one
rating for all the important components (outlined above). For example, a body of evidence may contain
a large number of studies with a low risk of bias and consistent findings, but which are not directly
applicable to the target population or Australian healthcare context and have only a limited clinical
impact. Alternatively, a body of evidence may only consist of one or two randomised trials with small
sample sizes that have a moderate risk of bias but have a very large clinical impact and are directly
applicable to the Australian healthcare context and target population. The NHMRC evidence grading
system is designed to allow for this mixture of components, while still reflecting the overall body of
evidence supporting a guideline recommendation.
The components described above should be rated according to the matrix shown in Table 1. Enter the
results into the NHMRC Evidence Statement Form (see Appendix C) along with any further notes
relevant to the discussions for each component.
Table 1: Body of evidence matrix
Component A B C D
Excellent Good Satisfactory Poor
Evidence base1 one or more level I
studies with a low risk of bias or several level II studies with a low risk of bias
one or two level II studies with a low risk of bias or a SR/several level III studies with a low risk of bias
one or two level III
studies with a low risk
of bias, or level I or II
studies with a
moderate risk of bias
level IV studies, or
level I to III
studies/SRs with a
high risk of bias
Consistency2 all studies consistent most studies consistent
and inconsistency may
be explained
some inconsistency
reflecting genuine
uncertainty around
clinical question
evidence is
inconsistent
Clinical impact very large substantial moderate slight or restricted
Generalisability population/s studied
in body of evidence
are the same as the
target population for
the guideline
population/s studied in
the body of evidence are
similar to the target
population for the
guideline
population/s studied in
body of evidence differ
to target population for
guideline but it is
clinically sensible to
apply this evidence to
target population3
population/s studied in
body of evidence differ to
target population and
hard to judge whether it
is sensible to generalise
to target population
Applicability directly applicable to
Australian healthcare
context
applicable to Australian
healthcare context with
few caveats
probably applicable to
Australian healthcare
context with some
caveats
not applicable to
Australian healthcare
context
SR = systematic review; several = more than two studies 1 Level of evidence determined from the NHMRC evidence hierarchy – Table 3, Part B
2 If there is only one study, rank this component as ‘not applicable’.
3 For example, results in adults that are clinically sensible to apply to children OR psychosocial outcomes for one cancer that may be applicable to patients with another cancer

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 55
The Evidence Statement Form also provides space to enter any other relevant factors that were taken into
account by the guideline developers when judging the body of evidence and developing the wording of the
recommendation.
Step 2 — Prepare an evidence statement matrix
In the ‘Evidence statement matrix ’ section of the form, summarise the guideline developers’ synthesis of
the evidence relating to each component at the right hand side of the form, and fill in the evidence matrix
at the left hand side of the form. Each recommendation should be accompanied by this matrix as well as
the overall grade given to the recommendation (see Step 3). Developers should indicate dissenting
opinions or other relevant issues in the space provided under the evidence matrix.
Step 3 — Formulate a recommendation based on the body of evidence
Develop wording for the recommendation. This should address the specific clinical question and ideally
be written as an action statement. The wording of the recommendation should reflect the strength of
the body of evidence. Words such as ‘must’ or ‘should’ are used when the evidence underpinning the
recommendation is strong, and words such as ‘might’ or ‘could’ are used when the evidence base is
weaker.
Step 4 — Determine the grade for the recommendation
Determine the overall grade of the recommendation based on a summation of the rating for each individual component of the body of evidence. A recommendation cannot be graded A or B unless the evidence base and consistency of the evidence are both rated A or B.
NHMRC overall grades of recommendation are intended to indicate the strength of the body of evidence underpinning the recommendation. This should assist users of the clinical practice guidelines to make appropriate and informed clinical judgments. Grade A or B recommendations are generally based on a body of evidence that can be trusted to guide clinical practice, whereas Grades C or D recommendations must be applied carefully to individual clinical and organisational circumstances and should be interpreted with care (see Table 2).
Table 2: Definition of NHMRC grades of recommendations
Grade of
recommendation
Description
A Body of evidence can be trusted to guide practice
B Body of evidence can be trusted to guide practice in most situations
C Body of evidence provides some support for recommendation(s) but care should be taken in its application
D Body of evidence is weak and recommendation must be applied with caution
Implementing guideline recommendations How the guidelines will be implemented should be considered at the time that the guideline
recommendations are being formulated. Guidelines require an implementation plan that ensures
appropriate roll out, supports and evaluation of guideline effectiveness in improving practice, and
guideline uptake. The Evidence Statement Form asks developers to consider four questions related to
the implementation of each recommendation:
Will this recommendation result in changes in usual care?
Are there any resource implications associated with implementing this recommendation?
Will the implementation of this recommendation require changes in the way care is currently organised?
Are the guideline development group aware of any barriers to the implementation of this recommendation?

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 56
Appendix C: NHMRC Evidence Statement Form
(If rating is not completely clear, use the space next to each criteria to note how the group came to a judgment).
Key question(s): Evidence table ref:
1. Evidence base (number of studies, level of evidence and risk of bias in the included studies)
A One or more level I studies with a low risk of bias or several level II studies with
a low risk of bias
B One or two Level II studies with a low risk of bias or SR/several Level III studies
with a low risk of bias
C One or two Level III studies with a low risk of bias or Level I or II studies with a
moderate risk of bias
D Level IV studies or Level I to III studies/SRs with a high risk of bias
2. Consistency (if only one study was available, rank this component as ‘not applicable’)
A All studies consistent
B Most studies consistent and inconsistency can be explained
C Some inconsistency, reflecting genuine uncertainty around question
D Evidence is inconsistent
NA Not applicable (one study only)
3. Clinical impact (Indicate in the space below if the study results varied according to some unknown factor (not simply study quality or sample size) and thus the clinical impact of the
intervention could not be determined)
A Very large
B Substantial
C Moderate
D Slight/Restricted

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 57
4. Generalisability (How well does the body of evidence match the population and clinical settings being targeted by the Guideline?)
A Evidence directly generalisable to target population
B Evidence directly generalisable to target population with some caveats
C Evidence not directly generalisable to the target population but could be
sensibly applied
D Evidence not directly generalisable to target population and hard to judge
whether it is sensible to apply
5. Applicability (Is the body of evidence relevant to the Australian healthcare context in terms of health services/delivery of care and cultural factors?)
A Evidence directly applicable to Australian healthcare context
B Evidence applicable to Australian healthcare context with few caveats
C Evidence probably applicable to Australian healthcare context with some
caveats
D Evidence not applicable to Australian healthcare context

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 58
Other factors (Indicate here any other factors that you took into account when assessing the evidence base (for example, issues that might cause the group to downgrade or upgrade
the recommendation)
EVIDENCE STATEMENT MATRIX Please summarise the development group’s synthesis of the evidence relating to the key question, taking all the above factors into account.
Component Rating Description
1. Evidence base
2. Consistency
3. Clinical impact
4. Generalisability
5. Applicability
Indicate any dissenting opinions
RECOMMENDATION
What recommendation(s) does the guideline development group draw from this evidence? Use action
statements where possible.
GRADE OF RECOMMENDATION

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 59
UNRESOLVED ISSUES
If needed, keep note of specific issues that arise when each recommendation is formulated and that require follow-up.
IMPLEMENTATION OF RECOMMENDATION
Please indicate yes or no to the following questions. Where the answer is yes please provide explanatory information about this. This information will be used to develop the
implementation plan for the guidelines.
Will this recommendation result in changes in usual care? YES
NO
Are there any resource implications associated with implementing this recommendation? YES
NO
Will the implementation of this recommendation require changes in the way care is currently organised? YES
NO
Are the guideline development group aware of any barriers to the implementation of this recommendation?
YES
NO

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 60
Appendix D: New Zealand Processes
The NZ guiding principles for guideline developers are detailed in the “Handbook for the Preparation of
Explicit Evidence-Based Clinical Practice Guidelines” (NZGG 2001).
ELICIT EVIDENCE-BASED CLINICAL PRACTICE GUIDELINES

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 61
Appendix E: Tocolysis Intent and Maternal Neuroprotective Intent
TOCOLYSIS
a) Crowther 2002 compared magnesium sulphate with no magnesium sulphate (either placebo or an
alternative tocolytic drug) for initial (acute) tocolysis in women thought to be in preterm labour.
This Cochrane review included 23 trials (with over 2000 women). The last search was conducted in
May 2002.
Magnesium sulphate was found to be ineffective at either delaying birth or preventing preterm birth,
and its use was associated with increased mortality for infants (of the 24 deaths (18 in the magnesium
group and 10 in the placebo group), all but two were neonates or infants).
Cochrane review of magnesium sulphate for tocolysis (Crowther 2002)
TOCOLYSIS RR (95% CI) Number of trials, participants
Birth within 48 hours of tocolysis 0.85 (0.58 to 1.25) 11 trials, 881 women
Preterm birth (< 37 weeks) 0.91 (0.75 to 1.11) 6 trials, 424 women
Perinatal mortality 2.82 (1.20 to 6.62) 7 trials, 727 infants
b) Crowther 1998 compared magnesium sulphate with no magnesium sulphate (either a placebo or an
alternative drug) used for maintenance in women who already had been given some medication to
stop early labour. The Cochrane review included three trials (303 women, 322 infants). The last
search for this review was conducted in August 2002.
No differences in the incidence of preterm birth or perinatal mortality were seen when magnesium
sulphate maintenance therapy was compared with either a placebo, or no treatment, or alternative
therapies (ritodrine or terbutaline).
Cochrane review of magnesium sulphate for maintenance of tocolysis (Crowther 1998)
TOCOLYSIS (MAINTENANCE) RR (95% CI) Number of trials, participants
Preterm birth < 37 weeks (magnesium v placebo/no treatment)
0.85 (0.47 to 1.51) 1 trial, 50 infants
Preterm birth < 37 weeks (magnesium v ritodrine or terbutaline)
0.98 (0.56 to 1.72) 2 trials, 100 infants
Perinatal mortality (magnesium v placebo/no treatment)
5.00 (0.25 to 99.16) 1 trial, 50 infants
Perinatal mortality (magnesium v ritodrine or terbutaline)
5.00 (0.25 to 99.16) 1 trial, 50 infants
Summary of evidence statement judgements for tocolysis
The evidence base for tocolysis was of poor to moderate quality (high to moderate risk of bias), with
some inconsistency between the results of different trials. Tocolysis with magnesium sulphate was
judged to have a substantial negative impact on outcomes, in particular, increased infant mortality. The
evidence was judged to be both generalisable and applicable.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 62
NEUROPROTECTION (MOTHER) – PRE-ECLAMPSIA
Magnesium sulphate is given to pregnant women with the intention of preventing eclampsia.
Duley 2003 compared magnesium sulphate with placebo or no anticonvulsant for preventing eclampsia
in women with pre-eclampsia. This Cochrane review included 11,444 women (six trials) and 9961
infants (three trials). The last search was conducted in November 2002.
Duley 2003 found that while magnesium sulphate more than halved the risk of eclampsia, and probably
reduced the risk of maternal death, the review did not demonstrate effects on improved infant
outcomes. However, there was no overall difference in the risk of stillbirth or neonatal death (RR 1.04,
95% CI 0.93 to 1.15) or other infant outcomes. This was also true for the subset of unpublished
outcome data provided by the trial investigators for the Doyle 2009 Cochrane review.
Summary of evidence statement judgements for maternal neuroprotection
The evidence base for maternal neuroprotection (preventing pre-eclampsia) with magnesium sulphate
has a mixed risk of bias and results are fairly consistent between trials. The impact on fetal and infant
outcomes was judged to be negligible. While the evidence may be applicable, it has lower
generalisability as most women in the largest trial were from low or middle income countries.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 63
Q1-Q3: Effectiveness Summary for Cochrane Reviews
Tocolysis
Crowther 2002
This Cochrane review included 23 trials (with over 2000 women). Magnesium sulphate was ineffective at
delaying birth or preventing preterm birth, and its use is associated with an increased mortality for the
infant.
DEATH
Crowther 1998 This Cochrane review included three trials (303 women) and no differences in the incidence of preterm
birth or perinatal mortality were seen when magnesium sulphate maintenance therapy was compared with
placebo or no treatment (2 trials (n=183 women); or alternative therapies (ritodrine or terbutaline).
DEATH
Study or Subgroup
Beall 1985
Cotton 1984
Cox 1990
Fox 1993
Glock 1993
Mittendorf 1997
Morales 1993
Total (95% CI)
Total events
Heterogeneity: Chi² = 5.89, df = 4 (P = 0.21); I² = 32%
Test for overall effect: Z = 2.38 (P = 0.02)
Events
0
1
8
0
0
8
1
18
Total
46
16
78
45
41
55
59
340
Events
0
1
2
0
2
0
1
6
Total
85
19
89
45
39
52
58
387
Weight
13.3%
27.2%
37.3%
7.5%
14.7%
100.0%
M-H, Fixed, 95% CI
Not estimable
1.19 [0.08, 17.51]
4.56 [1.00, 20.86]
Not estimable
0.19 [0.01, 3.85]
16.09 [0.95, 271.91]
0.98 [0.06, 15.35]
2.82 [1.20, 6.62]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.002 0.1 1 10 500
Favours magnesium Favours no magnesium
Study or Subgroup
10.1.1 Stillbirth
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
10.1.2 Death before discharge among live-born infants
Ricci 1991
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.06 (P = 0.29)
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.06 (P = 0.29)
Test for subgroup differences: Not applicable
Events
0
2
2
2
Total
0
25
25
25
Events
0
0
0
0
Total
0
25
25
25
Weight
100.0%
100.0%
100.0%
M-H, Fixed, 95% CI
Not estimable
5.00 [0.25, 99.16]
5.00 [0.25, 99.16]
5.00 [0.25, 99.16]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 64
Neuroprotection (Mother) – Pre-eclampsia
Duley 2003
This Cochrane review compared magnesium sulphate with placebo or no anticonvulsant for preventing eclampsia in women with pre-eclampsia. This review included 11,444 women (six trials) and 9961 infants (three trials) and found that magnesium sulphate more than halves the risk of eclampsia, and probably reduces the risk of maternal death. It does not influence short-term outcomes for the baby.
DEATH
Study or Subgroup
9.1.1 Stillbirth
South Africa 1994
South Africa 1998
Magpie 2002
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 2.18, df = 2 (P = 0.34); I² = 8%
Test for overall effect: Z = 0.20 (P = 0.84)
9.1.2 Perinatal death
South Africa 1994
Magpie 2002
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 0.56, df = 1 (P = 0.45); I² = 0%
Test for overall effect: Z = 0.28 (P = 0.78)
9.1.3 Neonatal death
Magpie 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.39 (P = 0.16)
9.1.4 Infant death (from 28 days to 1 year)
Magpie 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.14 (P = 0.89)
Total (95% CI)
Total events
Heterogeneity: Chi² = 4.78, df = 6 (P = 0.57); I² = 0%
Test for overall effect: Z = 0.25 (P = 0.80)
Test for subgroup differences: Not applicable
Events
13
38
373
424
20
518
538
187
187
16
16
1165
Total
117
348
4538
5003
117
4538
4655
4162
4162
4162
4162
17982
Events
14
28
384
426
25
516
541
159
159
15
15
1141
Total
118
354
4486
4958
118
4486
4604
4098
4098
4098
4098
17758
Weight
1.2%
2.4%
33.7%
37.3%
2.2%
45.2%
47.4%
14.0%
14.0%
1.3%
1.3%
100.0%
M-H, Fixed, 95% CI
0.94 [0.46, 1.91]
1.38 [0.87, 2.20]
0.96 [0.84, 1.10]
0.99 [0.87, 1.12]
0.81 [0.48, 1.37]
0.99 [0.88, 1.11]
0.98 [0.88, 1.10]
1.16 [0.94, 1.42]
1.16 [0.94, 1.42]
1.05 [0.52, 2.12]
1.05 [0.52, 2.12]
1.01 [0.93, 1.09]
Magnesium No Magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 65
Appendix F: Evidence Statements and Tables – Questions 1 to 11
Q1 – Q3: Effectiveness Summary For Cochrane Reviews
NHMRC Evidence Statement
Key question(s):
Q1: Does the administration of magnesium sulphate to women prior to preterm birth improve health outcomes for the fetus/infant/child?
Q2: Does the use of magnesium sulphate prior to preterm birth cause adverse outcome for women?
Q3: Does the use of magnesium sulphate prior to preterm birth cause adverse outcome for the fetus/infant/child?
1. Evidence base
NEUROPROTECTIVE INTENT Four RCTs (level ll intervention), generally with a low risk of bias, included in a systematic review (level I).
A (One or more Level I studies with a low risk of bias or several Level ll
studies with low risk of bias)
2. Consistency
There was some inconsistency between studies, which can probably mostly be explained (different regimens used in each of the four studies).
B (Most studies consistent and
inconsistency can be explained)
3. Clinical Impact
Neuroprotection and prevention of cerebral palsy in this vulnerable preterm population will have a very large potential impact.
The number of women needed to be treated to benefit one baby by avoiding cerebral palsy is 63 (95% confidence interval 44 to 155).
Women given magnesium sulphate were about three times more likely to cease therapy compared with women not given magnesium therapy mainly due to flushing, nausea/vomiting and headaches. Hypotension and respiratory depression were also increased with magnesium use.
No harms for the fetus, infant or child were significantly increased with antenatal use of magnesium.
A (very large)
4. Generalisability
One neuroprotective trial was conducted in Australia and New Zealand and most of the other trials had populations and settings directly generalisable to the target population (Australian women at risk of preterm birth); women in the large Rouse trial represented a narrower population (87% with PPROM).
B (Evidence directly generalisable to
target population with some caveats)
5. Applicability
Magnesium sulphate is already available in Australian and New Zealand maternity settings and therefore this evidence is directly applicable to the Australian health care context.
A (Evidence directly applicable to Australian healthcare context)
EVIDENCE STATEMENT MATRIX
Component Rating
Evidence base A
Consistency B
Clinical impact A
Generalisability B

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 66
Applicability A
RECOMMENDATION
In women at risk of early preterm* imminent# birth, use magnesium
sulphate for neuroprotection of the fetus, infant and child:
*when gestational age is less than 30 weeks. #when very preterm birth is planned or definitely expected within 24
hours. (When birth is planned, commence magnesium sulphate as close
to four hours before birth as possible).
A
UNRESOLVED ISSUES
See subsequent chapters
IMPLEMENTATION OF RECOMMENDATION
Will this recommendation result in changes in usual care?
Partially – some obstetric settings are already using magnesium sulphate for this indication.
YES
Are there any resource implications associated with implementing this recommendation?
Yes, setting up, maintaining and monitoring magnesium infusions will incur extra staff time.
(On the other hand, at an overall societal and health systems level, fewer cases of cerebral palsy will mean cost savings).
YES
Will the implementation of this recommendation require changes in the way care is currently organised?
Partially, midwifery/nursing staff will require extra time to manage the magnesium infusions.
YES
Are the guideline development group aware of any barriers to the implementation of this recommendation?
Yes, as above – extra time required, plus additional task in the busy and perhaps fraught setting of a preterm birth.
YES

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 67
Appendix F: Evidence Tables and Graphs: Q1-3: OVERALL
Doyle 2009
DEATH
CEREBRAL PALSY
DEATH OR CEREBRAL PALSY
Study or Subgroup
Crowther 2003
Marret 2006
Mittendorf 2002
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Chi² = 3.73, df = 3 (P = 0.29); I² = 20%
Test for overall effect: Z = 0.62 (P = 0.53)
Events
87
34
2
103
226
Total
629
352
30
1188
2199
Events
107
38
1
96
242
Total
626
336
29
1256
2247
Weight
44.6%
16.2%
0.4%
38.8%
100.0%
M-H, Fixed, 95% CI
0.81 [0.62, 1.05]
0.85 [0.55, 1.32]
1.93 [0.19, 20.18]
1.13 [0.87, 1.48]
0.95 [0.80, 1.12]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.05 0.2 1 5 20
Favours magnesium Favours no magnesium
Study or Subgroup
Crowther 2003
Marret 2006
Mittendorf 2002
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Chi² = 4.01, df = 3 (P = 0.26); I² = 25%
Test for overall effect: Z = 2.74 (P = 0.006)
Events
36
22
3
41
102
Total
629
352
30
1188
2199
Events
42
30
0
74
146
Total
626
336
29
1256
2247
Weight
29.0%
21.1%
0.3%
49.5%
100.0%
M-H, Fixed, 95% CI
0.85 [0.55, 1.31]
0.70 [0.41, 1.19]
6.77 [0.37, 125.65]
0.59 [0.40, 0.85]
0.71 [0.55, 0.91]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.001 0.1 1 10 1000
Favours magnesium Favours no magnesium
Study or Subgroup
Crowther 2003
Marret 2006
Mittendorf 2002
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 3.17, df = 3 (P = 0.37); I² = 5%
Test for overall effect: Z = 2.21 (P = 0.03)
Events
123
56
5
144
328
Total
629
352
30
1188
2199
Events
149
67
1
170
387
Total
626
336
29
1256
2247
Weight
39.9%
18.2%
0.5%
41.4%
100.0%
M-H, Random, 95% CI
0.82 [0.66, 1.02]
0.80 [0.58, 1.10]
4.83 [0.60, 38.90]
0.90 [0.73, 1.10]
0.85 [0.74, 0.98]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.02 0.1 1 10 50
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 68
F: Q1-3: OVERALL
SUBSTANTIAL GROSS MOTOR DYSFUNCTION
DEATH OR SUBSTANTIAL MOTOR DYSFUNCTION
ANY NEUROLOGICAL IMPAIRMENT
DEVELOPMENT DELAY OR INTELLECTUAL IMPAIRMENT
Study or Subgroup
Crowther 2003
Marret 2006
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Chi² = 1.01, df = 2 (P = 0.60); I² = 0%
Test for overall effect: Z = 3.08 (P = 0.002)
Events
18
18
20
56
Total
629
352
1188
2169
Events
34
22
38
94
Total
626
336
1256
2218
Weight
36.4%
24.1%
39.5%
100.0%
M-H, Fixed, 95% CI
0.53 [0.30, 0.92]
0.78 [0.43, 1.43]
0.56 [0.33, 0.95]
0.60 [0.43, 0.83]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours magnesium Favours no magnesium
Study or Subgroup
Crowther 2003
Marret 2006
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.01; Chi² = 2.67, df = 2 (P = 0.26); I² = 25%
Test for overall effect: Z = 1.95 (P = 0.05)
Events
105
52
123
280
Total
629
352
1188
2169
Events
141
60
134
335
Total
626
336
1256
2218
Weight
39.8%
21.4%
38.8%
100.0%
M-H, Random, 95% CI
0.74 [0.59, 0.93]
0.83 [0.59, 1.16]
0.97 [0.77, 1.22]
0.84 [0.71, 1.00]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.1 0.2 0.5 1 2 5 10
Favours magnesium Favours no magnesium
Study or Subgroup
Crowther 2003
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.31 (P = 0.75)
Events
193
193
Total
629
629
Events
187
187
Total
626
626
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.03 [0.87, 1.21]
1.03 [0.87, 1.21]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10
Favours magnesium Favours no magnesium
Study or Subgroup
Crowther 2003
Marret 2006
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.90, df = 2 (P = 0.64); I² = 0%
Test for overall effect: Z = 0.05 (P = 0.96)
Events
176
57
406
639
Total
629
352
1188
2169
Events
170
63
427
660
Total
626
336
1256
2218
Weight
26.2%
9.9%
63.9%
100.0%
M-H, Fixed, 95% CI
1.03 [0.86, 1.23]
0.86 [0.62, 1.20]
1.01 [0.90, 1.12]
1.00 [0.91, 1.09]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 69
F: Q1-3: OVERALL
MAJOR NEUROLOGICAL DISABILITY
INTRAVENTRICULAR HAEMORRHAGE
INTRAVENTRICULAR HAEMORRHAGE (grade 3/4)
PERIVENTRICULAR LEUKOMALACIA
Study or Subgroup
Crowther 2003
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.88 (P = 0.38)
Events
89
89
Total
629
629
Events
78
78
Total
626
626
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.14 [0.86, 1.51]
1.14 [0.86, 1.51]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10
Favours magnesium Favours no magnesium
Study or Subgroup
Crowther 2003
Marret 2006
Mittendorf 2002
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Chi² = 3.75, df = 3 (P = 0.29); I² = 20%
Test for overall effect: Z = 0.65 (P = 0.51)
Events
165
71
13
218
467
Total
629
352
85
1188
2254
Events
148
82
11
252
493
Total
626
336
80
1256
2298
Weight
30.4%
17.2%
2.3%
50.1%
100.0%
M-H, Fixed, 95% CI
1.11 [0.92, 1.34]
0.83 [0.62, 1.09]
1.11 [0.53, 2.34]
0.91 [0.78, 1.08]
0.96 [0.86, 1.08]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium
Study or Subgroup
Crowther 2003
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Chi² = 1.69, df = 1 (P = 0.19); I² = 41%
Test for overall effect: Z = 1.18 (P = 0.24)
Events
49
23
72
Total
629
1188
1817
Events
50
38
88
Total
626
1256
1882
Weight
57.6%
42.4%
100.0%
M-H, Fixed, 95% CI
0.98 [0.67, 1.42]
0.64 [0.38, 1.07]
0.83 [0.62, 1.13]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favours magnesium Favours no magnesium
Study or Subgroup
Crowther 2003
Marret 2006
Mittendorf 2002
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.80, df = 3 (P = 0.85); I² = 0%
Test for overall effect: Z = 0.43 (P = 0.67)
Events
22
27
1
21
71
Total
629
352
85
1188
2254
Events
21
28
0
27
76
Total
626
336
80
1256
2298
Weight
27.5%
37.5%
0.7%
34.3%
100.0%
M-H, Fixed, 95% CI
1.04 [0.58, 1.88]
0.92 [0.55, 1.53]
2.83 [0.12, 68.37]
0.82 [0.47, 1.45]
0.93 [0.68, 1.28]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 70
F: Q1-3: OVERALL
BLINDNESS
DEAFNESS
Study or Subgroup
Crowther 2003
Marret 2006
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.00, df = 1 (P = 0.98); I² = 0%
Test for overall effect: Z = 0.03 (P = 0.98)
Events
1
1
2
Total
629
352
981
Events
1
1
2
Total
626
336
962
Weight
49.5%
50.5%
100.0%
M-H, Fixed, 95% CI
1.00 [0.06, 15.88]
0.95 [0.06, 15.20]
0.97 [0.14, 6.90]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours magnesium Favours no magnesium
Study or Subgroup
Crowther 2003
Marret 2006
Total (95% CI)
Total events
Heterogeneity: Tau² = 1.77; Chi² = 2.42, df = 1 (P = 0.12); I² = 59%
Test for overall effect: Z = 0.58 (P = 0.56)
Events
8
0
8
Total
629
352
981
Events
7
4
11
Total
626
336
962
Weight
66.2%
33.8%
100.0%
M-H, Random, 95% CI
1.14 [0.41, 3.12]
0.11 [0.01, 1.96]
0.51 [0.05, 4.96]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.005 0.1 1 10 200
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 71
Q4: Gestational Age
NHMRC Evidence Statement
Key question(s):
Q4: Do improvements to the fetus/infant/child vary by gestational age magnesium sulphate given?
1. Evidence base
Subgroup analysis from 4 RCTs with low risk of bias; therefore the comparisons by gestational age are non-randomised comparisons (level III).
B (Several Level lll studies with
low risk of bias)
2. Consistency
B (Most studies consistent and
inconsistency can be explained)
3. Clinical Impact
Overall impact is very large. A (overall)
4. Generalisability
As for overall; women in the large Rouse trial represented a narrower population (87% with PPROM).
B (Evidence directly
generalisable to target population with some
caveats)
5. Applicability
As for overall A (Evidence directly applicable
to Australian healthcare context)
Other factors
In the absence of being able to distinguish different levels of clinical impact between the present gestational age subgroups, the choices are to:
a) make no recommendation regarding gestational age; b) make a recommendation that magnesium sulphate can be given up to 34 weeks; c) make a recommendation that magnesium sulphate be only given to women less than 32 weeks; d) make a recommendation that magnesium sulphate be only given to women less than 30 weeks
gestation.
EVIDENCE STATEMENT MATRIX
Component Rating
Evidence base B
Consistency B
Clinical impact A (overall)
Generalisability B
Applicability A

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 72
RECOMMENDATION
Magnesium sulphate be only given to women less than 30 weeks gestation.
B
UNRESOLVED ISSUES
Some of the trials have stratified by gestational age but have not published these analyses.
Individual patient data meta-analyses by gestational age are needed.
IMPLEMENTATION OF RECOMMENDATION
Will this recommendation result in changes in usual care? YES
Are there any resource implications associated with implementing this recommendation?
YES
Will the implementation of this recommendation require changes in the way care is currently organised?
YES
Are the guideline development group aware of any barriers to the implementation of this recommendation?
YES

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 73
Appendix F 4: Evidence Table and Graphs: GESTATIONAL AGE
Study Gestational age
Mittendorf 2002 < 34 weeks at randomisation
Marret 2006 < 33 weeks
Rouse 2008 < 32 weeks
Crowther 2003 < 30 weeks
DEATH
Study or Subgroup
11.1.1 < 34 weeks at randomisation
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.55 (P = 0.58)
11.1.2 < 33 weeks at randomisation
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.71 (P = 0.48)
11.1.3 < 32 weeks at randomisation
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.93 (P = 0.35)
11.1.4 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.59 (P = 0.11)
Total (95% CI)
Total events
Heterogeneity: Chi² = 3.73, df = 3 (P = 0.29); I² = 20%
Test for overall effect: Z = 0.62 (P = 0.53)
Events
2
2
34
34
103
103
87
87
226
Total
30
30
352
352
1188
1188
629
629
2199
Events
1
1
38
38
96
96
107
107
242
Total
29
29
336
336
1256
1256
626
626
2247
Weight
0.4%
0.4%
16.2%
16.2%
38.8%
38.8%
44.6%
44.6%
100.0%
M-H, Fixed, 95% CI
1.93 [0.19, 20.18]
1.93 [0.19, 20.18]
0.85 [0.55, 1.32]
0.85 [0.55, 1.32]
1.13 [0.87, 1.48]
1.13 [0.87, 1.48]
0.81 [0.62, 1.05]
0.81 [0.62, 1.05]
0.95 [0.80, 1.12]
Favours magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.05 0.2 1 5 20
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 74
F 4: GESTATIONAL AGE
CEREBRAL PALSY
Study or Subgroup
11.2.1 < 34 weeks at randomisation
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.28 (P = 0.20)
11.2.2 < 33 weeks at randomisation
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.32 (P = 0.19)
11.2.3 < 32 weeks at randomisation
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.81 (P = 0.005)
11.2.4 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.72 (P = 0.47)
Total (95% CI)
Total events
Heterogeneity: Chi² = 4.01, df = 3 (P = 0.26); I² = 25%
Test for overall effect: Z = 2.74 (P = 0.006)
Events
3
3
22
22
41
41
36
36
102
Total
30
30
352
352
1188
1188
629
629
2199
Events
0
0
30
30
74
74
42
42
146
Total
29
29
336
336
1256
1256
626
626
2247
Weight
0.3%
0.3%
21.1%
21.1%
49.5%
49.5%
29.0%
29.0%
100.0%
M-H, Fixed, 95% CI
6.77 [0.37, 125.65]
6.77 [0.37, 125.65]
0.70 [0.41, 1.19]
0.70 [0.41, 1.19]
0.59 [0.40, 0.85]
0.59 [0.40, 0.85]
0.85 [0.55, 1.31]
0.85 [0.55, 1.31]
0.71 [0.55, 0.91]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 75
F 4: GESTATIONAL AGE
DEATH OR CEREBRAL PALSY
Study or Subgroup
11.5.1 < 34 weeks at randomisation
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.48 (P = 0.14)
11.5.2 < 33 weeks at randomisation
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.38 (P = 0.17)
11.5.3 < 32 weeks at randomisation
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.04 (P = 0.30)
11.5.4 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.82 (P = 0.07)
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 3.17, df = 3 (P = 0.37); I² = 5%
Test for overall effect: Z = 2.21 (P = 0.03)
Events
5
5
56
56
144
144
123
123
328
Total
30
30
352
352
1188
1188
629
629
2199
Events
1
1
67
67
170
170
149
149
387
Total
29
29
336
336
1256
1256
626
626
2247
Weight
0.5%
0.5%
18.2%
18.2%
41.4%
41.4%
39.9%
39.9%
100.0%
M-H, Random, 95% CI
4.83 [0.60, 38.90]
4.83 [0.60, 38.90]
0.80 [0.58, 1.10]
0.80 [0.58, 1.10]
0.90 [0.73, 1.10]
0.90 [0.73, 1.10]
0.82 [0.66, 1.02]
0.82 [0.66, 1.02]
0.85 [0.74, 0.98]
Favours magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.05 0.2 1 5 20
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 76
F 4: GESTATIONAL AGE
SUBSTANTIAL GROSS MOTOR DYSFUNCTION
Study or Subgroup
11.8.3 < 34 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.8.4 < 33 weeks at randomisation
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.80 (P = 0.42)
11.8.5 < 32 weeks at randomisation
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.15 (P = 0.03)
11.8.6 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.24 (P = 0.03)
Total (95% CI)
Total events
Heterogeneity: Chi² = 1.01, df = 2 (P = 0.60); I² = 0%
Test for overall effect: Z = 3.08 (P = 0.002)
Events
0
18
18
20
20
18
18
56
Total
0
352
352
1188
1188
629
629
2169
Events
0
22
22
38
38
34
34
94
Total
0
336
336
1256
1256
626
626
2218
Weight
24.1%
24.1%
39.5%
39.5%
36.4%
36.4%
100.0%
M-H, Fixed, 95% CI
Not estimable
0.78 [0.43, 1.43]
0.78 [0.43, 1.43]
0.56 [0.33, 0.95]
0.56 [0.33, 0.95]
0.53 [0.30, 0.92]
0.53 [0.30, 0.92]
0.60 [0.43, 0.83]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 77
F 4: GESTATIONAL AGE
DEATH OR SUBSTANTIAL MOTOR DYSFUNCTION
Study or Subgroup
11.9.3 < 34 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.9.4 < 33 weeks at randomisation
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.09 (P = 0.27)
11.9.5 < 32 weeks at randomisation
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.25 (P = 0.80)
11.9.6 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.59 (P = 0.010)
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.01; Chi² = 2.67, df = 2 (P = 0.26); I² = 25%
Test for overall effect: Z = 1.95 (P = 0.05)
Events
0
52
52
123
123
105
105
280
Total
0
352
352
1188
1188
629
629
2169
Events
0
60
60
134
134
141
141
335
Total
0
336
336
1256
1256
626
626
2218
Weight
21.4%
21.4%
38.8%
38.8%
39.8%
39.8%
100.0%
M-H, Random, 95% CI
Not estimable
0.83 [0.59, 1.16]
0.83 [0.59, 1.16]
0.97 [0.77, 1.22]
0.97 [0.77, 1.22]
0.74 [0.59, 0.93]
0.74 [0.59, 0.93]
0.84 [0.71, 1.00]
Favours magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 78
F 4: GESTATIONAL AGE
ANY NEUROLOGICAL IMPAIRMENT
Study or Subgroup
11.3.3 < 34 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.3.4 < 33 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.3.5 < 32 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.3.6 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.31 (P = 0.75)
Events
0
0
0
193
193
Total
0
0
0
629
629
Events
0
0
0
187
187
Total
0
0
0
626
626
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
Not estimable
Not estimable
Not estimable
1.03 [0.87, 1.21]
1.03 [0.87, 1.21]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 79
F 4: GESTATIONAL AGE
DEVELOPMENT DELAY OR INTELLECTUAL IMPAIRMENT
Study or Subgroup
11.12.1 < 34 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.12.2 < 33 weeks at randomisation
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.88 (P = 0.38)
11.12.3 < 32 weeks at randomisation
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.09 (P = 0.93)
11.12.4 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.33 (P = 0.74)
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.90, df = 2 (P = 0.64); I² = 0%
Test for overall effect: Z = 0.05 (P = 0.96)
Events
0
57
57
406
406
176
176
639
Total
0
352
352
1188
1188
629
629
2169
Events
0
63
63
427
427
170
170
660
Total
0
336
336
1256
1256
626
626
2218
Weight
9.9%
9.9%
63.9%
63.9%
26.2%
26.2%
100.0%
M-H, Fixed, 95% CI
Not estimable
0.86 [0.62, 1.20]
0.86 [0.62, 1.20]
1.01 [0.90, 1.12]
1.01 [0.90, 1.12]
1.03 [0.86, 1.23]
1.03 [0.86, 1.23]
1.00 [0.91, 1.09]
Favours magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 80
F 4: GESTATIONAL AGE
MAJOR NEUROLOGICAL DISABILITY
Study or Subgroup
11.4.3 < 34 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.4.4 < 33 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.4.5 < 32 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.4.6 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.88 (P = 0.38)
Events
0
0
0
89
89
Total
0
0
0
629
629
Events
0
0
0
78
78
Total
0
0
0
626
626
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
Not estimable
Not estimable
Not estimable
1.14 [0.86, 1.51]
1.14 [0.86, 1.51]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.1 0.2 0.5 1 2 5 10
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 81
F 4: GESTATIONAL AGE
INTRAVENTRICULAR HAEMORRHAGE
Study or Subgroup
11.13.1 < 34 weeks at randomisation
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.28 (P = 0.78)
11.13.2 < 33 weeks at randomisation
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.33 (P = 0.18)
11.13.3 < 32 weeks at randomisation
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.07 (P = 0.28)
11.13.4 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.06 (P = 0.29)
Total (95% CI)
Total events
Heterogeneity: Chi² = 3.75, df = 3 (P = 0.29); I² = 20%
Test for overall effect: Z = 0.65 (P = 0.51)
Events
13
13
71
71
218
218
165
165
467
Total
85
85
352
352
1188
1188
629
629
2254
Events
11
11
82
82
252
252
148
148
493
Total
80
80
336
336
1256
1256
626
626
2298
Weight
2.3%
2.3%
17.2%
17.2%
50.1%
50.1%
30.4%
30.4%
100.0%
M-H, Fixed, 95% CI
1.11 [0.53, 2.34]
1.11 [0.53, 2.34]
0.83 [0.62, 1.09]
0.83 [0.62, 1.09]
0.91 [0.78, 1.08]
0.91 [0.78, 1.08]
1.11 [0.92, 1.34]
1.11 [0.92, 1.34]
0.96 [0.86, 1.08]
Favours magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 82
F 4: GESTATIONAL AGE
INTRAVENTRICULAR HAEMORRHAGE (grade 3/4)
Study or Subgroup
11.13.1 < 34 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.13.2 < 33 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.13.3 < 32 weeks at randomisation
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.71 (P = 0.09)
11.13.4 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.13 (P = 0.90)
Total (95% CI)
Total events
Heterogeneity: Chi² = 1.69, df = 1 (P = 0.19); I² = 41%
Test for overall effect: Z = 1.18 (P = 0.24)
Events
0
0
23
23
49
49
72
Total
0
0
1188
1188
629
629
1817
Events
0
0
38
38
50
50
88
Total
0
0
1256
1256
626
626
1882
Weight
42.4%
42.4%
57.6%
57.6%
100.0%
M-H, Fixed, 95% CI
Not estimable
Not estimable
0.64 [0.38, 1.07]
0.64 [0.38, 1.07]
0.98 [0.67, 1.42]
0.98 [0.67, 1.42]
0.83 [0.62, 1.13]
Favours magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 83
F 4: GESTATIONAL AGE
PERIVENTRICULAR LEUKOMALACIA
Study or Subgroup
11.7.1 < 34 weeks at randomisation
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.64 (P = 0.52)
11.7.2 < 33 weeks at randomisation
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.32 (P = 0.75)
11.7.3 < 32 weeks at randomisation
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.68 (P = 0.50)
11.7.4 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.14 (P = 0.89)
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.80, df = 3 (P = 0.85); I² = 0%
Test for overall effect: Z = 0.43 (P = 0.67)
Events
1
1
27
27
21
21
22
22
71
Total
85
85
352
352
1188
1188
629
629
2254
Events
0
0
28
28
27
27
21
21
76
Total
80
80
336
336
1256
1256
626
626
2298
Weight
0.7%
0.7%
37.5%
37.5%
34.3%
34.3%
27.5%
27.5%
100.0%
M-H, Fixed, 95% CI
2.83 [0.12, 68.37]
2.83 [0.12, 68.37]
0.92 [0.55, 1.53]
0.92 [0.55, 1.53]
0.82 [0.47, 1.45]
0.82 [0.47, 1.45]
1.04 [0.58, 1.88]
1.04 [0.58, 1.88]
0.93 [0.68, 1.28]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 84
F 4: GESTATIONAL AGE
BLINDNESS
Study or Subgroup
11.10.1 < 34 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.10.2 < 33 weeks at randomisation
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.03 (P = 0.97)
11.10.3 < 32 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.10.4 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.00 (P = 1.00)
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.00, df = 1 (P = 0.98); I² = 0%
Test for overall effect: Z = 0.03 (P = 0.98)
Events
0
1
1
0
1
1
2
Total
0
352
352
0
629
629
981
Events
0
1
1
0
1
1
2
Total
0
336
336
0
626
626
962
Weight
50.5%
50.5%
49.5%
49.5%
100.0%
M-H, Fixed, 95% CI
Not estimable
0.95 [0.06, 15.20]
0.95 [0.06, 15.20]
Not estimable
1.00 [0.06, 15.88]
1.00 [0.06, 15.88]
0.97 [0.14, 6.90]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.05 0.2 1 5 20
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 85
F 4: GESTATIONAL AGE
DEAFNESS
Study or Subgroup
11.11.1 < 34 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.11.2 < 33 weeks at randomisation
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.51 (P = 0.13)
11.11.3 < 32 weeks at randomisation
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
11.11.4 < 30 weeks at randomisation
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.25 (P = 0.80)
Total (95% CI)
Total events
Heterogeneity: Tau² = 1.77; Chi² = 2.42, df = 1 (P = 0.12); I² = 59%
Test for overall effect: Z = 0.58 (P = 0.56)
Events
0
0
0
0
8
8
8
Total
0
352
352
0
629
629
981
Events
0
4
4
0
7
7
11
Total
0
336
336
0
626
626
962
Weight
33.8%
33.8%
66.2%
66.2%
100.0%
M-H, Random, 95% CI
Not estimable
0.11 [0.01, 1.96]
0.11 [0.01, 1.96]
Not estimable
1.14 [0.41, 3.12]
1.14 [0.41, 3.12]
0.51 [0.05, 4.96]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.005 0.1 1 10 200
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 86
Q5: Time Magnesium Sulphate Planned To Be Given Prior To Preterm Birth
NHMRC Evidence Statement
Key question(s):
Q5: Do improvements to the fetus/infant/child vary by time magnesium sulphate planned to be given prior to preterm birth?
1. Evidence base
Subgroup analysis from four RCTs with low risk of bias; therefore some of the comparisons by time magnesium is planned are non-randomised comparisons (level III).
B (Several Level II and lll studies
with low risk of bias)
2. Consistency
B (Most studies consistent and
inconsistency can be explained)
3. Clinical Impact
Overall impact is very large A (overall)
4. Generalisability
B overall; but A for the birth planned within 24 hours subgroup A (Evidence directly
generalisable to target population with some
caveats)
5. Applicability
As for overall A (Evidence directly applicable
to Australian healthcare context)
Other factors
In the absence of being able to assess clinical impact, the choices are:
a) To make no recommendation regarding the timing of administration of magnesium; b) To make a recommendation that magnesium sulphate be only given to women where birth is planned
or expected within 24 hours; c) To make a recommendation that magnesium sulphate be given where birth is definitely expected
within 24 hours, ideally within 4 hours of a planned birth.
EVIDENCE STATEMENT MATRIX
Component Rating
Evidence base B
Consistency B
Clinical impact A (overall)
Generalisability A
Applicability A

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 87
RECOMMENDATION
In women at risk of early preterm* imminent# birth, use magnesium sulphate for neuroprotection of the fetus, infant and child:
o When early preterm birth is planned or definitely expected within 24 hours. (When birth is planned, commence magnesium sulphate as close to four hours before birth as possible).
*when gestational age is less than 30 weeks
#when early preterm birth is planned or definitely expected within 24 hours.
A
UNRESOLVED ISSUES
Need to try to get more detailed timings from trials.
Individual patient data meta-analysis needed.
IMPLEMENTATION OF RECOMMENDATION
Will this recommendation result in changes in usual care? YES
Are there any resource implications associated with implementing this recommendation?
YES
Will the implementation of this recommendation require changes in the way care is currently organised?
YES
Are the guideline development group aware of any barriers to the implementation of this recommendation?
YES

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 88
Appendix F 5: Evidence table and Graphs: TIMING
Study Timing
Crowther 2003,
Marret 2006
Where birth was planned or expected within 24 hours
Rouse 2008 Where birth was planned or expected within 24 hours for indicated preterm birth (3.1% only); otherwise advanced preterm labour, with cervical dilatation between 4 and 8 cm (10.3%); PPROM 86.7% - median 25 hours, interquartile range 11 to 63 hours from rupture)
Mittendorf 2002 Not specified
DEATH
Study or Subgroup
12.1.1 within 24 hours
Crowther 2003
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 0.04, df = 1 (P = 0.84); I² = 0%
Test for overall effect: Z = 1.73 (P = 0.08)
12.1.2 up to 63 hours
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.93 (P = 0.35)
12.1.3 not specified
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.55 (P = 0.58)
Total (95% CI)
Total events
Heterogeneity: Chi² = 3.73, df = 3 (P = 0.29); I² = 20%
Test for overall effect: Z = 0.62 (P = 0.53)
Events
87
34
121
103
103
2
2
226
Total
629
352
981
1188
1188
30
30
2199
Events
107
38
145
96
96
1
1
242
Total
626
336
962
1256
1256
29
29
2247
Weight
44.6%
16.2%
60.8%
38.8%
38.8%
0.4%
0.4%
100.0%
M-H, Fixed, 95% CI
0.81 [0.62, 1.05]
0.85 [0.55, 1.32]
0.82 [0.66, 1.03]
1.13 [0.87, 1.48]
1.13 [0.87, 1.48]
1.93 [0.19, 20.18]
1.93 [0.19, 20.18]
0.95 [0.80, 1.12]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.05 0.2 1 5 20
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 89
F 5: TIMING
CEREBRAL PALSY
DEATH OR CEREBRAL PALSY
Study or Subgroup
12.2.1 within 24 hours
Crowther 2003
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 0.32, df = 1 (P = 0.57); I² = 0%
Test for overall effect: Z = 1.39 (P = 0.16)
12.2.2 up to 63 hours
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.81 (P = 0.005)
12.2.6 not specified
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.28 (P = 0.20)
Total (95% CI)
Total events
Heterogeneity: Chi² = 4.01, df = 3 (P = 0.26); I² = 25%
Test for overall effect: Z = 2.74 (P = 0.006)
Events
36
22
58
41
41
3
3
102
Total
629
352
981
1188
1188
30
30
2199
Events
42
30
72
74
74
0
0
146
Total
626
336
962
1256
1256
29
29
2247
Weight
29.0%
21.1%
50.1%
49.5%
49.5%
0.3%
0.3%
100.0%
M-H, Fixed, 95% CI
0.85 [0.55, 1.31]
0.70 [0.41, 1.19]
0.79 [0.56, 1.10]
0.59 [0.40, 0.85]
0.59 [0.40, 0.85]
6.77 [0.37, 125.65]
6.77 [0.37, 125.65]
0.71 [0.55, 0.91]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.005 0.1 1 10 200
Favours magnesium Favours no magnesium
Study or Subgroup
12.5.1 within 24 hours
Crowther 2003
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 0.02, df = 1 (P = 0.88); I² = 0%
Test for overall effect: Z = 2.28 (P = 0.02)
12.5.2 up to 63 hours
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.04 (P = 0.30)
12.5.3 not specified
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.48 (P = 0.14)
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 3.17, df = 3 (P = 0.37); I² = 5%
Test for overall effect: Z = 2.21 (P = 0.03)
Events
123
56
179
144
144
5
5
328
Total
629
352
981
1188
1188
30
30
2199
Events
149
67
216
170
170
1
1
387
Total
626
336
962
1256
1256
29
29
2247
Weight
39.9%
18.2%
58.1%
41.4%
41.4%
0.5%
0.5%
100.0%
M-H, Random, 95% CI
0.82 [0.66, 1.02]
0.80 [0.58, 1.10]
0.81 [0.68, 0.97]
0.90 [0.73, 1.10]
0.90 [0.73, 1.10]
4.83 [0.60, 38.90]
4.83 [0.60, 38.90]
0.85 [0.74, 0.98]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.01 0.1 1 10 100
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 90
F 5: TIMING
SUBSTANTIAL GROSS MOTOR DYSFUNCTION
DEATH OR SUBSTANTIAL MOTOR DYSFUNCTION
Study or Subgroup
12.8.1 within 24 hours
Crowther 2003
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 0.88, df = 1 (P = 0.35); I² = 0%
Test for overall effect: Z = 2.23 (P = 0.03)
12.8.2 up to 63 hours
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.15 (P = 0.03)
12.8.3 not specified
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Chi² = 1.01, df = 2 (P = 0.60); I² = 0%
Test for overall effect: Z = 3.08 (P = 0.002)
Events
18
18
36
20
20
0
56
Total
629
352
981
1188
1188
0
2169
Events
34
22
56
38
38
0
94
Total
626
336
962
1256
1256
0
2218
Weight
36.4%
24.1%
60.5%
39.5%
39.5%
100.0%
M-H, Fixed, 95% CI
0.53 [0.30, 0.92]
0.78 [0.43, 1.43]
0.63 [0.42, 0.95]
0.56 [0.33, 0.95]
0.56 [0.33, 0.95]
Not estimable
0.60 [0.43, 0.83]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favours magnesium Favours no magnesium
Study or Subgroup
12.9.1 within 24 hours
Crowther 2003
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 0.28, df = 1 (P = 0.60); I² = 0%
Test for overall effect: Z = 2.76 (P = 0.006)
12.9.2 up to 63 hours
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.25 (P = 0.80)
12.9.3 not specified
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.01; Chi² = 2.67, df = 2 (P = 0.26); I² = 25%
Test for overall effect: Z = 1.95 (P = 0.05)
Events
105
52
157
123
123
0
280
Total
629
352
981
1188
1188
0
2169
Events
141
60
201
134
134
0
335
Total
626
336
962
1256
1256
0
2218
Weight
39.8%
21.4%
61.2%
38.8%
38.8%
100.0%
M-H, Random, 95% CI
0.74 [0.59, 0.93]
0.83 [0.59, 1.16]
0.77 [0.63, 0.93]
0.97 [0.77, 1.22]
0.97 [0.77, 1.22]
Not estimable
0.84 [0.71, 1.00]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 91
F 5: TIMING
ANY NEUROLOGICAL IMPAIRMENT
DEVELOPMENT DELAY OR INTELLECTUAL IMPAIRMENT
Study or Subgroup
12.3.2 within 24 hours
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.31 (P = 0.75)
12.3.3 up to 63 hours
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
12.3.6 not specified
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Events
193
193
0
0
Total
629
629
0
0
Events
187
187
0
0
Total
626
626
0
0
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.03 [0.87, 1.21]
1.03 [0.87, 1.21]
Not estimable
Not estimable
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium
Study or Subgroup
12.12.1 within 24 hours
Crowther 2003
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 0.87, df = 1 (P = 0.35); I² = 0%
Test for overall effect: Z = 0.19 (P = 0.85)
12.12.2 up to 63 hours
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.09 (P = 0.93)
12.12.6 not specified
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.90, df = 2 (P = 0.64); I² = 0%
Test for overall effect: Z = 0.05 (P = 0.96)
Events
176
57
233
406
406
0
639
Total
629
352
981
1188
1188
0
2169
Events
170
63
233
427
427
0
660
Total
626
336
962
1256
1256
0
2218
Weight
26.2%
9.9%
36.1%
63.9%
63.9%
100.0%
M-H, Fixed, 95% CI
1.03 [0.86, 1.23]
0.86 [0.62, 1.20]
0.98 [0.84, 1.15]
1.01 [0.90, 1.12]
1.01 [0.90, 1.12]
Not estimable
1.00 [0.91, 1.09]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 92
F 5: TIMING
MAJOR NEUROLOGICAL DISABILITY
INTRAVENTRICULAR HAEMORRHAGE
Study or Subgroup
12.13.1 within 24 hours
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.88 (P = 0.38)
12.13.2 up to 63 hours
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
12.13.6 not specified
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Events
89
89
0
0
Total
629
629
0
0
Events
78
78
0
0
Total
626
626
0
0
Weight
100.0%
100.0%
M-H, Fixed, 95% CI
1.14 [0.86, 1.51]
1.14 [0.86, 1.51]
Not estimable
Not estimable
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium
Study or Subgroup
12.6.1 within 24 hours
Crowther 2003
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 0.03; Chi² = 2.88, df = 1 (P = 0.09); I² = 65%
Test for overall effect: Z = 0.17 (P = 0.86)
12.6.2 up to 63 hours
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.07 (P = 0.28)
12.6.6 not specified
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.28 (P = 0.78)
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 3.75, df = 3 (P = 0.29); I² = 20%
Test for overall effect: Z = 0.52 (P = 0.60)
Events
165
71
236
218
218
13
13
467
Total
629
352
981
1188
1188
85
85
2254
Events
148
82
230
252
252
11
11
493
Total
626
336
962
1256
1256
80
80
2298
Weight
34.5%
19.2%
53.7%
43.1%
43.1%
3.2%
3.2%
100.0%
M-H, Random, 95% CI
1.11 [0.92, 1.34]
0.83 [0.62, 1.09]
0.98 [0.73, 1.30]
0.91 [0.78, 1.08]
0.91 [0.78, 1.08]
1.11 [0.53, 2.34]
1.11 [0.53, 2.34]
0.96 [0.84, 1.10]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.2 0.5 1 2 5
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 93
F 5: TIMING
INTRAVENTRICULAR HAEMORRHAGE (grade 3/4)
PERIVENTRICULAR LEUKOMALACIA
Study or Subgroup
12.14.1 within 24 hours
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.13 (P = 0.90)
12.14.2 up to 63 hours
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.71 (P = 0.09)
12.14.6 not specified
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Chi² = 1.69, df = 1 (P = 0.19); I² = 41%
Test for overall effect: Z = 1.18 (P = 0.24)
Events
49
49
23
23
0
72
Total
629
629
1188
1188
0
1817
Events
50
50
38
38
0
88
Total
626
626
1256
1256
0
1882
Weight
57.6%
57.6%
42.4%
42.4%
100.0%
M-H, Fixed, 95% CI
0.98 [0.67, 1.42]
0.98 [0.67, 1.42]
0.64 [0.38, 1.07]
0.64 [0.38, 1.07]
Not estimable
0.83 [0.62, 1.13]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favours magnesium Favours no magnesium
Study or Subgroup
12.7.1 within 24 hours
Crowther 2003
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 0.10, df = 1 (P = 0.75); I² = 0%
Test for overall effect: Z = 0.14 (P = 0.89)
12.7.2 up to 63 hours
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.68 (P = 0.50)
12.7.6 not specified
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.64 (P = 0.52)
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.80, df = 3 (P = 0.85); I² = 0%
Test for overall effect: Z = 0.43 (P = 0.67)
Events
22
27
49
21
21
1
1
71
Total
629
352
981
1188
1188
85
85
2254
Events
21
28
49
27
27
0
0
76
Total
626
336
962
1256
1256
80
80
2298
Weight
27.5%
37.5%
65.0%
34.3%
34.3%
0.7%
0.7%
100.0%
M-H, Fixed, 95% CI
1.04 [0.58, 1.88]
0.92 [0.55, 1.53]
0.97 [0.66, 1.43]
0.82 [0.47, 1.45]
0.82 [0.47, 1.45]
2.83 [0.12, 68.37]
2.83 [0.12, 68.37]
0.93 [0.68, 1.28]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 94
F 5: TIMING
BLINDNESS
DEAFNESS
Study or Subgroup
12.10.1 within 24 hours
Crowther 2003
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 0.00, df = 1 (P = 0.98); I² = 0%
Test for overall effect: Z = 0.03 (P = 0.98)
12.10.2 up to 63 hours
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
12.10.6 not specified
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.00, df = 1 (P = 0.98); I² = 0%
Test for overall effect: Z = 0.03 (P = 0.98)
Events
1
1
2
0
0
2
Total
629
352
981
0
0
981
Events
1
1
2
0
0
2
Total
626
336
962
0
0
962
Weight
49.5%
50.5%
100.0%
100.0%
M-H, Fixed, 95% CI
1.00 [0.06, 15.88]
0.95 [0.06, 15.20]
0.97 [0.14, 6.90]
Not estimable
Not estimable
0.97 [0.14, 6.90]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours magnesium Favours no magnesium
Study or Subgroup
12.11.1 within 24 hours
Crowther 2003
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 1.77; Chi² = 2.42, df = 1 (P = 0.12); I² = 59%
Test for overall effect: Z = 0.58 (P = 0.56)
12.11.2 up to 63 hours
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
12.11.6 not specified
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Tau² = 1.77; Chi² = 2.42, df = 1 (P = 0.12); I² = 59%
Test for overall effect: Z = 0.58 (P = 0.56)
Events
8
0
8
0
0
8
Total
629
352
981
0
0
981
Events
7
4
11
0
0
11
Total
626
336
962
0
0
962
Weight
66.2%
33.8%
100.0%
100.0%
M-H, Random, 95% CI
1.14 [0.41, 3.12]
0.11 [0.01, 1.96]
0.51 [0.05, 4.96]
Not estimable
Not estimable
0.51 [0.05, 4.96]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.005 0.1 1 10 200
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 95
Q6: Regimens
NHMRC Evidence Statement
Key question(s):
Q6: Do improvements to the fetus/infant/child vary by regimens?
1. Evidence base
Subgroup analysis from 4 RCTs; therefore the comparisons by regimens are non-randomised comparisons (level III).
B (Several Level lll studies with low
risk of bias) 2. Consistency
Unable to explain inconsistent results between Marret (2006) and Mittendorf (2002) for combined death and cerebral palsy; and cerebral palsy.
C (Some
inconsistency, reflecting genuine
uncertainty around question)
3. Clinical Impact
A (overall)
4. Generalisability
As for overall. B (Evidence directly generalisable to
target population with some caveats)
5. Applicability
Australian and NZ clinicians may not be as comfortable with a 6 g loading dose and 2 g/hr maintenance dose.
A (Evidence directly
applicable to Australian
healthcare context)
Other factors
In the absence of being able to assess clinical impact, the choices are:
a) To make no recommendation regarding magnesium regimens b) To recommend that magnesium be given from 4 g to 6 g as loading dose and from 1 g to 2 g/hour
as a maintenance dose; with repeat doses possible with IV route c) To make a cautious recommendation that magnesium sulphate be only given as a 4 g loading dose
(over 20 minutes) and 1 g/hour maintenance dose with no repeat doses with IV route (up until birth or 24 hours whichever comes first).
EVIDENCE STATEMENT MATRIX
Component Rating
Evidence base B
Consistency C
Clinical impact A (overall)
Generalisability B
Applicability A

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 96
RECOMMENDATION
Magnesium sulphate be given intravenously with a 4 gram loading dose (slowly over 20-30 minutes) and 1 gram per hour maintenance dose via intravenous route, with no immediate repeat doses. Continue regimen up until birth or 24 hours whichever comes first.
C
UNRESOLVED ISSUES
IMPLEMENTATION OF RECOMMENDATION
Will this recommendation result in changes in usual care? YES
Are there any resource implications associated with implementing this recommendation?
YES
Will the implementation of this recommendation require changes in the way care is currently organised?
YES
Are the guideline development group aware of any barriers to the implementation of this recommendation?
YES

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 97
Appendix F 6: Evidence Table and Graphs: REGIMENS
Study Loading
dose
Maintenance
dose
Repeat dosing Route
Marret 2006 4 g none none IV
Mittendorf 2002 4 g none none IV
Crowther 2003 4 g 1 g/hr none IV
Rouse 2008 6 g 2 g/hr 42.2% received repeat dose IV
IV= Intravenous
DEATH
Study or Subgroup
13.1.1 Loading dose 4 g (no maintenance)
Marret 2006
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 0.45, df = 1 (P = 0.50); I² = 0%
Test for overall effect: Z = 0.58 (P = 0.56)
13.1.2 Loading 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.59 (P = 0.11)
13.1.3 Loading dose 6 g (then 2 g/hr maintenance)
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.93 (P = 0.35)
Total (95% CI)
Total events
Heterogeneity: Chi² = 3.73, df = 3 (P = 0.29); I² = 20%
Test for overall effect: Z = 0.62 (P = 0.53)
Events
34
2
36
87
87
103
103
226
Total
352
30
382
629
629
1188
1188
2199
Events
38
1
39
107
107
96
96
242
Total
336
29
365
626
626
1256
1256
2247
Weight
16.2%
0.4%
16.6%
44.6%
44.6%
38.8%
38.8%
100.0%
M-H, Fixed, 95% CI
0.85 [0.55, 1.32]
1.93 [0.19, 20.18]
0.88 [0.57, 1.35]
0.81 [0.62, 1.05]
0.81 [0.62, 1.05]
1.13 [0.87, 1.48]
1.13 [0.87, 1.48]
0.95 [0.80, 1.12]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.05 0.2 1 5 20
Favours magnesium Favours no magnesium
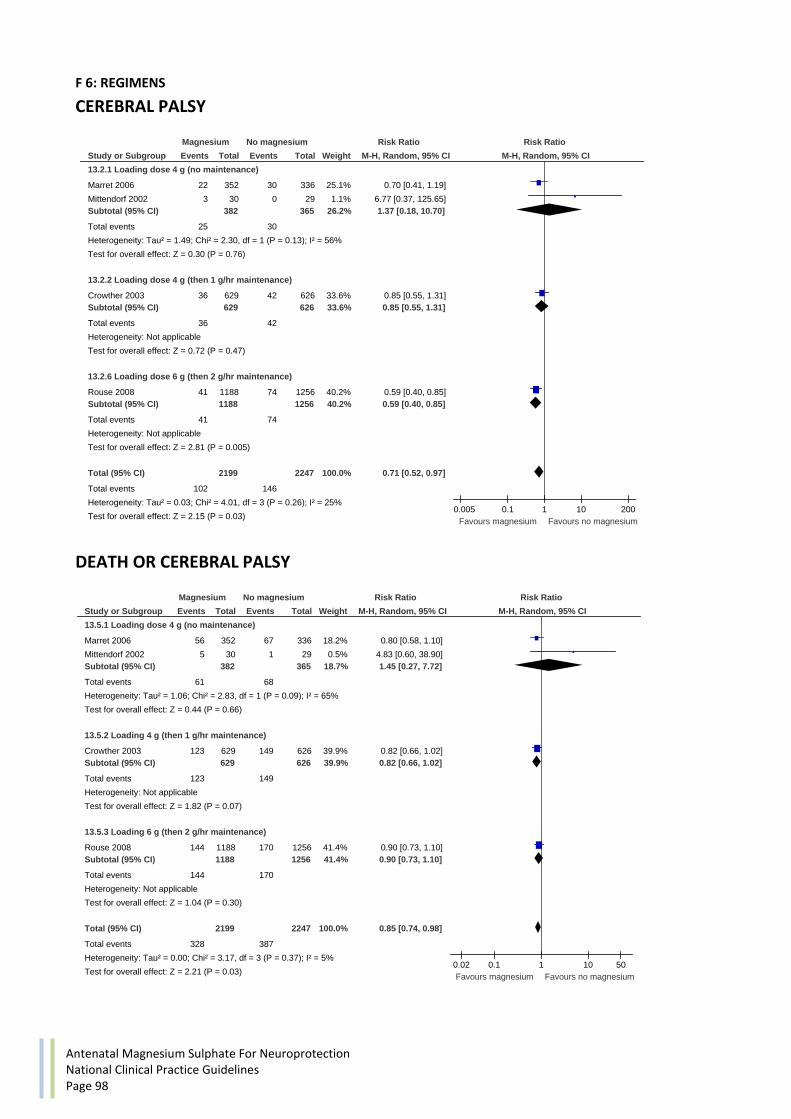
Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 98
F 6: REGIMENS
CEREBRAL PALSY
DEATH OR CEREBRAL PALSY
Study or Subgroup
13.2.1 Loading dose 4 g (no maintenance)
Marret 2006
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 1.49; Chi² = 2.30, df = 1 (P = 0.13); I² = 56%
Test for overall effect: Z = 0.30 (P = 0.76)
13.2.2 Loading dose 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.72 (P = 0.47)
13.2.6 Loading dose 6 g (then 2 g/hr maintenance)
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.81 (P = 0.005)
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.03; Chi² = 4.01, df = 3 (P = 0.26); I² = 25%
Test for overall effect: Z = 2.15 (P = 0.03)
Events
22
3
25
36
36
41
41
102
Total
352
30
382
629
629
1188
1188
2199
Events
30
0
30
42
42
74
74
146
Total
336
29
365
626
626
1256
1256
2247
Weight
25.1%
1.1%
26.2%
33.6%
33.6%
40.2%
40.2%
100.0%
M-H, Random, 95% CI
0.70 [0.41, 1.19]
6.77 [0.37, 125.65]
1.37 [0.18, 10.70]
0.85 [0.55, 1.31]
0.85 [0.55, 1.31]
0.59 [0.40, 0.85]
0.59 [0.40, 0.85]
0.71 [0.52, 0.97]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.005 0.1 1 10 200
Favours magnesium Favours no magnesium
Study or Subgroup
13.5.1 Loading dose 4 g (no maintenance)
Marret 2006
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 1.06; Chi² = 2.83, df = 1 (P = 0.09); I² = 65%
Test for overall effect: Z = 0.44 (P = 0.66)
13.5.2 Loading 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.82 (P = 0.07)
13.5.3 Loading 6 g (then 2 g/hr maintenance)
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.04 (P = 0.30)
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 3.17, df = 3 (P = 0.37); I² = 5%
Test for overall effect: Z = 2.21 (P = 0.03)
Events
56
5
61
123
123
144
144
328
Total
352
30
382
629
629
1188
1188
2199
Events
67
1
68
149
149
170
170
387
Total
336
29
365
626
626
1256
1256
2247
Weight
18.2%
0.5%
18.7%
39.9%
39.9%
41.4%
41.4%
100.0%
M-H, Random, 95% CI
0.80 [0.58, 1.10]
4.83 [0.60, 38.90]
1.45 [0.27, 7.72]
0.82 [0.66, 1.02]
0.82 [0.66, 1.02]
0.90 [0.73, 1.10]
0.90 [0.73, 1.10]
0.85 [0.74, 0.98]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.02 0.1 1 10 50
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 99
F 6: REGIMENS
SUBSTANTIAL GROSS MOTOR DYSFUNCTION
DEATH OR SUBSTANTIAL MOTOR DYSFUNCTION
Study or Subgroup
13.8.1 Loading dose 4 g (no maintenance)
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.80 (P = 0.42)
13.8.2 Loading 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.24 (P = 0.03)
13.8.3 Loading dose 6 g (then 2 g/hr maintenance)
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.15 (P = 0.03)
Total (95% CI)
Total events
Heterogeneity: Chi² = 1.01, df = 2 (P = 0.60); I² = 0%
Test for overall effect: Z = 3.08 (P = 0.002)
Events
18
18
18
18
20
20
56
Total
352
352
629
629
1188
1188
2169
Events
22
22
34
34
38
38
94
Total
336
336
626
626
1256
1256
2218
Weight
24.1%
24.1%
36.4%
36.4%
39.5%
39.5%
100.0%
M-H, Fixed, 95% CI
0.78 [0.43, 1.43]
0.78 [0.43, 1.43]
0.53 [0.30, 0.92]
0.53 [0.30, 0.92]
0.56 [0.33, 0.95]
0.56 [0.33, 0.95]
0.60 [0.43, 0.83]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favours magnesium Favours no magnesium
Study or Subgroup
13.9.1 Loading dose 4 g (no maintenance)
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.09 (P = 0.27)
13.9.2 Loading 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 2.59 (P = 0.010)
13.9.3 Loading dose 6 g (then 2 g/hr maintenance)
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.25 (P = 0.80)
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.01; Chi² = 2.67, df = 2 (P = 0.26); I² = 25%
Test for overall effect: Z = 1.95 (P = 0.05)
Events
52
52
105
105
123
123
280
Total
352
352
629
629
1188
1188
2169
Events
60
60
141
141
134
134
335
Total
336
336
626
626
1256
1256
2218
Weight
21.4%
21.4%
39.8%
39.8%
38.8%
38.8%
100.0%
M-H, Random, 95% CI
0.83 [0.59, 1.16]
0.83 [0.59, 1.16]
0.74 [0.59, 0.93]
0.74 [0.59, 0.93]
0.97 [0.77, 1.22]
0.97 [0.77, 1.22]
0.84 [0.71, 1.00]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 100
F 6: REGIMENS
ANY NEUROLOGICAL IMPAIRMENT
DEVELOPMENT DELAY OR INTELLECTUAL IMPAIRMENT
Study or Subgroup
13.3.1 Loading dose 4g (no maintenance)
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
13.3.2 Loading dose 4 g (then 1g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.31 (P = 0.75)
13.3.3 Loading dose 6g (then 2g/hr maintenance)
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.31 (P = 0.75)
Events
0
193
193
0
193
Total
0
629
629
0
629
Events
0
187
187
0
187
Total
0
626
626
0
626
Weight
100.0%
100.0%
100.0%
M-H, Fixed, 95% CI
Not estimable
1.03 [0.87, 1.21]
1.03 [0.87, 1.21]
Not estimable
1.03 [0.87, 1.21]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium
Study or Subgroup
13.12.1 Loading dose 4 g (no maintenance)
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.88 (P = 0.38)
13.12.2 Loading 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.33 (P = 0.74)
13.12.3 Loading dose 6 g (then 2 g/hr maintenance)
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.09 (P = 0.93)
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.90, df = 2 (P = 0.64); I² = 0%
Test for overall effect: Z = 0.05 (P = 0.96)
Events
57
57
176
176
406
406
639
Total
352
352
629
629
1188
1188
2169
Events
63
63
170
170
427
427
660
Total
336
336
626
626
1256
1256
2218
Weight
9.9%
9.9%
26.2%
26.2%
63.9%
63.9%
100.0%
M-H, Fixed, 95% CI
0.86 [0.62, 1.20]
0.86 [0.62, 1.20]
1.03 [0.86, 1.23]
1.03 [0.86, 1.23]
1.01 [0.90, 1.12]
1.01 [0.90, 1.12]
1.00 [0.91, 1.09]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 101
F 6: REGIMENS
MAJOR NEUROLOGICAL DISABILITY
INTRAVENTRICULAR HAEMORRHAGE
Study or Subgroup
13.4.2 Loading dose 4g (no maintenance)
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
13.4.3 Loading dose 4 g (then 1g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.88 (P = 0.38)
13.4.4 Loading dose 6g (then 2g/hr maintenance)
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.88 (P = 0.38)
Events
0
89
89
0
89
Total
0
629
629
0
629
Events
0
78
78
0
78
Total
0
626
626
0
626
Weight
100.0%
100.0%
100.0%
M-H, Fixed, 95% CI
Not estimable
1.14 [0.86, 1.51]
1.14 [0.86, 1.51]
Not estimable
1.14 [0.86, 1.51]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium
Study or Subgroup
13.14.1 Loading dose 4 g (no maintenance)
Marret 2006
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 0.54, df = 1 (P = 0.46); I² = 0%
Test for overall effect: Z = 1.12 (P = 0.26)
13.14.2 Loading dose 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.06 (P = 0.29)
13.14.6 Loading dose 6 g (then 2 g/hr maintenance)
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.07 (P = 0.28)
Total (95% CI)
Total events
Heterogeneity: Chi² = 3.75, df = 3 (P = 0.29); I² = 20%
Test for overall effect: Z = 0.65 (P = 0.51)
Events
71
13
84
165
165
218
218
467
Total
352
85
437
629
629
1188
1188
2254
Events
82
11
93
148
148
252
252
493
Total
336
80
416
626
626
1256
1256
2298
Weight
17.2%
2.3%
19.5%
30.4%
30.4%
50.1%
50.1%
100.0%
M-H, Fixed, 95% CI
0.83 [0.62, 1.09]
1.11 [0.53, 2.34]
0.86 [0.66, 1.12]
1.11 [0.92, 1.34]
1.11 [0.92, 1.34]
0.91 [0.78, 1.08]
0.91 [0.78, 1.08]
0.96 [0.86, 1.08]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 102
F 6: REGIMENS
INTRAVENTRICULAR HAEMORRHAGE (grade 3/4)
PERIVENTRICULAR LEUKOMALACIA
Study or Subgroup
13.15.1 Loading dose 4 g (no maintenance)
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
13.15.2 Loading dose 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.13 (P = 0.90)
13.15.6 Loading dose 6 g (then 2 g/hr maintenance)
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.71 (P = 0.09)
Total (95% CI)
Total events
Heterogeneity: Chi² = 1.69, df = 1 (P = 0.19); I² = 41%
Test for overall effect: Z = 1.18 (P = 0.24)
Events
0
49
49
23
23
72
Total
0
629
629
1188
1188
1817
Events
0
50
50
38
38
88
Total
0
626
626
1256
1256
1882
Weight
57.6%
57.6%
42.4%
42.4%
100.0%
M-H, Fixed, 95% CI
Not estimable
0.98 [0.67, 1.42]
0.98 [0.67, 1.42]
0.64 [0.38, 1.07]
0.64 [0.38, 1.07]
0.83 [0.62, 1.13]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.2 0.5 1 2 5
Favours magnesium Favours no magnesium
Study or Subgroup
13.16.1 Loading dose 4 g (no maintenance)
Marret 2006
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 0.47, df = 1 (P = 0.50); I² = 0%
Test for overall effect: Z = 0.18 (P = 0.85)
13.16.2 Loading dose 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.14 (P = 0.89)
13.16.6 Loading dose 6 g (then 2 g/hr maintenance)
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.68 (P = 0.50)
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.80, df = 3 (P = 0.85); I² = 0%
Test for overall effect: Z = 0.43 (P = 0.67)
Events
27
1
28
22
22
21
21
71
Total
352
85
437
629
629
1188
1188
2254
Events
28
0
28
21
21
27
27
76
Total
336
80
416
626
626
1256
1256
2298
Weight
37.5%
0.7%
38.1%
27.5%
27.5%
34.3%
34.3%
100.0%
M-H, Fixed, 95% CI
0.92 [0.55, 1.53]
2.83 [0.12, 68.37]
0.95 [0.58, 1.57]
1.04 [0.58, 1.88]
1.04 [0.58, 1.88]
0.82 [0.47, 1.45]
0.82 [0.47, 1.45]
0.93 [0.68, 1.28]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.01 0.1 1 10 100
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 103
F 6: REGIMENS
BLINDNESS
DEAFNESS
Study or Subgroup
13.10.1 Loading dose 4 g (no maintenance)
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.03 (P = 0.97)
13.10.2 Loading 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.00 (P = 1.00)
13.10.3 Loading dose 6 g (then 2 g/hr maintenance)
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.00, df = 1 (P = 0.98); I² = 0%
Test for overall effect: Z = 0.03 (P = 0.98)
Events
1
1
1
1
0
2
Total
352
352
629
629
0
981
Events
1
1
1
1
0
2
Total
336
336
626
626
0
962
Weight
50.5%
50.5%
49.5%
49.5%
100.0%
M-H, Fixed, 95% CI
0.95 [0.06, 15.20]
0.95 [0.06, 15.20]
1.00 [0.06, 15.88]
1.00 [0.06, 15.88]
Not estimable
0.97 [0.14, 6.90]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.02 0.1 1 10 50
Favours magnesium Favours no magnesium
Study or Subgroup
13.11.1 Loading dose 4 g (no maintenance)
Marret 2006
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.51 (P = 0.13)
13.11.2 Loading 4 g (then 1 g/hr maintenance)
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.25 (P = 0.80)
13.11.3 Loading dose 6 g (then 2 g/hr maintenance)
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Tau² = 1.77; Chi² = 2.42, df = 1 (P = 0.12); I² = 59%
Test for overall effect: Z = 0.58 (P = 0.56)
Events
0
0
8
8
0
8
Total
352
352
629
629
0
981
Events
4
4
7
7
0
11
Total
336
336
626
626
0
962
Weight
33.8%
33.8%
66.2%
66.2%
100.0%
M-H, Random, 95% CI
0.11 [0.01, 1.96]
0.11 [0.01, 1.96]
1.14 [0.41, 3.12]
1.14 [0.41, 3.12]
Not estimable
0.51 [0.05, 4.96]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.005 0.1 1 10 200
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 104
Q7: Number of babies in utero
NHMRC Evidence Statement
Key question(s):
Q7: Do improvements to the fetus/infant/child vary by number of babies in utero?
1. Evidence base
Subgroup analysis from 4 RCTs; therefore the comparisons by the number of babies in utero are non-randomised comparisons (level III).
B (Several Level lll studies with low
risk of bias) 2. Consistency
B (Most studies consistent and
inconsistency can be explained)
3. Clinical Impact
Very large A (overall)
4. Generalisability
As for overall. B (Evidence directly generalisable to
target population with some caveats)
5. Applicability
No evidence to suggest that benefit is specific to either single or multiple (up to 4) babies in utero
A (Evidence directly
applicable to Australian
healthcare context) Other factors
In the absence of being able to assess clinical impact, the choices are:
a) To make no recommendation regarding magnesium regimens; b) To make a cautious recommendation that magnesium sulphate be given to women with up to 4
babies in utero; c) To make a recommendation that magnesium sulphate be given to women regardless of plurality.
EVIDENCE STATEMENT MATRIX
Component Rating
Evidence base B
Consistency B
Clinical impact A (overall)
Generalisability B
Applicability A

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 105
RECOMMENDATION
Magnesium sulphate be given to women regardless of plurality. B
UNRESOLVED ISSUES
Individual patient data meta-analysis needed.
IMPLEMENTATION OF RECOMMENDATION
Will this recommendation result in changes in usual care? YES
Are there any resource implications associated with implementing this recommendation?
YES
Will the implementation of this recommendation require changes in the way care is currently organised?
YES
Are the guideline development group aware of any barriers to the implementation of this recommendation?
YES

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 106
F 7: Evidence Tables and Graphs: NUMBER OF BABIES IN UTERO
Study Single Twin Higher order Reported separately
Crowther 2003 Yes Yes Yes (triplet+quad) Single vs multiple
Rouse 2008 Yes Yes No Single vs twin
Marret 2006 Yes Yes Yes (triplet) No
Mittendorf 2002 Yes Yes No No
DEATH
Study or Subgroup
14.1.1 Single
Crowther 2003
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 0.04; Chi² = 2.55, df = 1 (P = 0.11); I² = 61%
Test for overall effect: Z = 0.20 (P = 0.84)
14.1.2 Multiple
Crowther 2003
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 0.47, df = 1 (P = 0.49); I² = 0%
Test for overall effect: Z = 0.53 (P = 0.59)
14.1.3 Mixed
Marret 2006
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 0.45, df = 1 (P = 0.50); I² = 0%
Test for overall effect: Z = 0.59 (P = 0.55)
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 3.70, df = 5 (P = 0.59); I² = 0%
Test for overall effect: Z = 0.70 (P = 0.48)
Events
60
83
143
27
16
43
34
2
36
222
Total
447
950
1397
182
91
273
352
30
382
2052
Events
73
75
148
34
18
52
38
1
39
239
Total
438
985
1423
188
110
298
336
29
365
2086
Weight
29.6%
32.9%
62.5%
13.8%
7.8%
21.6%
15.4%
0.5%
15.9%
100.0%
M-H, Random, 95% CI
0.81 [0.59, 1.10]
1.15 [0.85, 1.55]
0.96 [0.68, 1.37]
0.82 [0.52, 1.30]
1.07 [0.58, 1.98]
0.90 [0.63, 1.31]
0.85 [0.55, 1.32]
1.93 [0.19, 20.18]
0.88 [0.57, 1.35]
0.94 [0.79, 1.12]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.05 0.2 1 5 20
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 107
F 7: NUMBER OF BABIES IN UTERO
CEREBRAL PALSY
DEATH OR CEREBRAL PALSY
Study or Subgroup
14.2.1 Single
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.06 (P = 0.95)
14.2.2 Multiple
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.46 (P = 0.14)
14.2.3 Mixed
Marret 2006
Mittendorf 2002
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 2.85, df = 2 (P = 0.24); I² = 30%
Test for overall effect: Z = 2.81 (P = 0.005)
Total (95% CI)
Total events
Heterogeneity: Chi² = 5.75, df = 4 (P = 0.22); I² = 30%
Test for overall effect: Z = 2.75 (P = 0.006)
Events
29
29
7
7
22
3
41
66
102
Total
447
447
182
182
352
30
1188
1570
2199
Events
28
28
14
14
30
0
74
104
146
Total
438
438
188
188
336
29
1256
1621
2247
Weight
19.5%
19.5%
9.5%
9.5%
21.1%
0.3%
49.5%
71.0%
100.0%
M-H, Fixed, 95% CI
1.01 [0.61, 1.68]
1.01 [0.61, 1.68]
0.52 [0.21, 1.25]
0.52 [0.21, 1.25]
0.70 [0.41, 1.19]
6.77 [0.37, 125.65]
0.59 [0.40, 0.85]
0.65 [0.48, 0.88]
0.71 [0.55, 0.91]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.005 0.1 1 10 200
Favours magnesium Favours no magnesium
Study or Subgroup
14.5.1 Single
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.14 (P = 0.25)
14.5.2 Multiple
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.57 (P = 0.12)
14.5.3 Mixed
Marret 2006
Mittendorf 2002
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 0.02; Chi² = 2.95, df = 2 (P = 0.23); I² = 32%
Test for overall effect: Z = 0.99 (P = 0.32)
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 3.65, df = 4 (P = 0.46); I² = 0%
Test for overall effect: Z = 2.30 (P = 0.02)
Events
89
89
34
34
56
5
144
205
328
Total
447
447
182
182
352
30
1188
1570
2199
Events
101
101
48
48
67
1
170
238
387
Total
438
438
188
188
336
29
1256
1621
2247
Weight
28.3%
28.3%
11.9%
11.9%
17.4%
0.4%
42.0%
59.8%
100.0%
M-H, Random, 95% CI
0.86 [0.67, 1.11]
0.86 [0.67, 1.11]
0.73 [0.50, 1.08]
0.73 [0.50, 1.08]
0.80 [0.58, 1.10]
4.83 [0.60, 38.90]
0.90 [0.73, 1.10]
0.88 [0.68, 1.14]
0.85 [0.75, 0.98]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.02 0.1 1 10 50
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 108
F 7: NUMBER OF BABIES IN UTERO
ANY NEUROLOGICAL IMPAIRMENT
MAJOR NEUROLOGICAL DISABILITY
Study or Subgroup
14.3.1 Single
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.73 (P = 0.47)
14.3.2 Multiple
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.65 (P = 0.52)
14.3.3 Mixed
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Chi² = 0.85, df = 1 (P = 0.36); I² = 0%
Test for overall effect: Z = 0.29 (P = 0.78)
Events
149
149
44
44
0
193
Total
447
447
182
182
0
629
Events
136
136
51
51
0
187
Total
438
438
188
188
0
626
Weight
73.2%
73.2%
26.8%
26.8%
100.0%
M-H, Fixed, 95% CI
1.07 [0.89, 1.30]
1.07 [0.89, 1.30]
0.89 [0.63, 1.26]
0.89 [0.63, 1.26]
Not estimable
1.02 [0.87, 1.21]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium
Study or Subgroup
14.4.1 Single
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.31 (P = 0.19)
14.4.2 Multiple
Crowther 2003
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.56 (P = 0.58)
14.4.3 Mixed
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Not applicable
Total (95% CI)
Total events
Heterogeneity: Chi² = 1.26, df = 1 (P = 0.26); I² = 21%
Test for overall effect: Z = 0.86 (P = 0.39)
Events
71
71
18
18
0
89
Total
447
447
182
182
0
629
Events
56
56
22
22
0
78
Total
438
438
188
188
0
626
Weight
72.3%
72.3%
27.7%
27.7%
100.0%
M-H, Fixed, 95% CI
1.24 [0.90, 1.72]
1.24 [0.90, 1.72]
0.85 [0.47, 1.52]
0.85 [0.47, 1.52]
Not estimable
1.13 [0.85, 1.50]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 109
Q8: Reason for treatment
NHMRC Evidence Statement
Key question(s):
Q8: Do improvements to the fetus/infant/child vary by reason women considered (at less than 30 weeks gestation) to be at risk of preterm birth?
1. Evidence base
Subgroup analysis from 4 RCTs; therefore the comparisons by time magnesium is planned are non-randomised comparisons (level III).
B (Several Level lll studies with low
risk of bias) 2. Consistency
B (Most studies consistent and
inconsistency can be explained)
3. Clinical Impact
Very large A (overall)
4. Generalisability
As for overall. B (Evidence directly generalisable to
target population with some caveats)
5. Applicability
As for overall. A (Evidence directly
applicable to Australian
healthcare context)
Other factors
In the absence of being able to assess clinical impact, the choices are:
a) To make no recommendation regarding reason for treatment with magnesium sulphate; b) To recommend that magnesium be given to all women regardless of whether reason for treatment
is PROM, preterm labour or preterm birth; c) To make a cautious recommendation that magnesium sulphate be only given to women at risk of
preterm birth within 24 hours.
EVIDENCE STATEMENT MATRIX
Component Rating
Evidence base B
Consistency B
Clinical impact A (overall)
Generalisability B
Applicability A

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 110
RECOMMENDATION
Magnesium sulphate be given regardless of reason women considered (at less than 30 weeks’ gestation) to be at risk of preterm birth.
B
UNRESOLVED ISSUES
Individual patient data meta-analysis needed
IMPLEMENTATION OF RECOMMENDATION
Will this recommendation result in changes in usual care? YES
Are there any resource implications associated with implementing this recommendation?
YES
Will the implementation of this recommendation require changes in the way care is currently organised?
YES
Are the guideline development group aware of any barriers to the implementation of this recommendation?
YES

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 111
Q9: Parity Of Women
NHMRC Evidence Statement
Key question(s):
Q9: Do improvements to the fetus/infant/child vary by parity of women?
1. Evidence base
Subgroup analysis from 4 RCTs; therefore the comparisons by parity of women are non-randomised comparisons (level III).
B (Several Level lll studies with low
risk of bias) 2. Consistency
B (Most studies consistent and
inconsistency can be explained)
3. Clinical Impact
Very large A (overall)
4. Generalisability
As for overall. B (Evidence directly generalisable to
target population with some caveats)
5. Applicability
As for overall. A (Evidence directly
applicable to Australian
healthcare context)
Other factors
In the absence of being able to assess clinical impact, the choices are:
a) To make no recommendation regarding giving magnesium sulphate to women based on parity; b) To recommend that magnesium sulphate be given to all women regardless of parity.
EVIDENCE STATEMENT MATRIX
Component Rating
Evidence base B
Consistency B
Clinical impact A (overall)
Generalisability B
Applicability A

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 112
RECOMMENDATION
Magnesium sulphate be given to all women regardless of parity (number of previous births for the woman).
B
UNRESOLVED ISSUES
Individual patient data meta-analysis needed
IMPLEMENTATION OF RECOMMENDATION
Will this recommendation result in changes in usual care? YES
Are there any resource implications associated with implementing this recommendation?
YES
Will the implementation of this recommendation require changes in the way care is currently organised?
YES
Are the guideline development group aware of any barriers to the implementation of this recommendation?
YES

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 113
Q10: Mode Of Birth
NHMRC Evidence Statement
Key question(s):
Q10: Do improvements to the fetus/infant/child vary by mode of birth?
1. Evidence base
Subgroup analysis from 4 RCTs; therefore the comparisons by time magnesium is planned are non-randomised comparisons (level III).
B (Several Level lll studies with low
risk of bias) 2. Consistency
B (Most studies consistent and
inconsistency can be explained)
3. Clinical Impact
Very large A (overall)
4. Generalisability
As for overall. B (Evidence directly generalisable to
target population with some caveats)
5. Applicability
As for overall. A
(Evidence directly applicable to
Australian healthcare context)
Other factors
In the absence of being able to assess clinical impact, the choices are:
a) To make no recommendation regarding giving magnesium sulphate to women based on mode of birth;
b) To recommend that magnesium sulphate be given to all women regardless of mode of birth.
EVIDENCE STATEMENT MATRIX
Component Rating
Evidence base B
Consistency B
Clinical impact A (overall)
Generalisability B
Applicability A

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 114
RECOMMENDATION
Magnesium sulphate be given to all women regardless of mode of birth. B
UNRESOLVED ISSUES
Individual patient data meta-analysis needed.
IMPLEMENTATION OF RECOMMENDATION
Will this recommendation result in changes in usual care? YES
Are there any resource implications associated with implementing this recommendation?
YES
Will the implementation of this recommendation require changes in the way care is currently organised?
YES
Are the guideline development group aware of any barriers to the implementation of this recommendation?
YES

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 115
Appendix F 10: Evidence Table and Graphs: MODE OF BIRTH
Study Caesarean Section Vaginal Birth
Crowther 2003 Yes Yes
Rouse 2008 Yes Yes
Marret 2006 Yes Yes
Mittendorf 2002 No No
CAESAREAN SECTION
VAGINAL BIRTH
Study or Subgroup
Crowther 2003
Marret 2006
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Chi² = 2.55, df = 2 (P = 0.28); I² = 22%
Test for overall effect: Z = 0.01 (P = 0.99)
Events
289
116
417
822
Total
535
286
1096
1917
Events
290
96
448
834
Total
527
278
1145
1950
Weight
35.3%
11.8%
52.9%
100.0%
M-H, Fixed, 95% CI
0.98 [0.88, 1.10]
1.17 [0.95, 1.46]
0.97 [0.88, 1.08]
1.00 [0.93, 1.07]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium
Study or Subgroup
Crowther 2003
Marret 2006
Rouse 2008
Total (95% CI)
Total events
Heterogeneity: Chi² = 2.56, df = 2 (P = 0.28); I² = 22%
Test for overall effect: Z = 0.01 (P = 0.99)
Events
246
170
679
1095
Total
535
286
1096
1917
Events
237
182
697
1116
Total
527
278
1145
1950
Weight
21.6%
16.7%
61.7%
100.0%
M-H, Fixed, 95% CI
1.02 [0.90, 1.17]
0.91 [0.80, 1.03]
1.02 [0.95, 1.09]
1.00 [0.95, 1.06]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.5 0.7 1 1.5 2
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 116
Q11: Combined Effect Of Antenatal Corticosteroids
NHMRC Evidence Statement
Key question(s):
Q11: Do improvements to the fetus/infant/child vary by combined effect of antenatal corticosteroids and magnesium sulphate?
1. Evidence base
Subgroup analysis from 4 RCTs; therefore the comparisons by time magnesium is planned are non-randomised comparisons (level III).
B (Several Level lll studies
with low risk of bias) 2. Consistency
B (Most studies consistent and inconsistency can be
explained) 3. Clinical Impact
Very large A (overall)
4. Generalisability
As for overall. B (Evidence directly
generalisable to target population with some
caveats)
5. Applicability
As for overall. A (Evidence directly
applicable to Australian healthcare context)
Other factors
In the absence of being able to assess clinical impact, the choices are:
a) To make no recommendation regarding giving magnesium sulphate to women receiving antenatal corticosteroids;
b) To recommend that magnesium sulphate be given to all women whether or not antenatal corticosteroids have been given.
EVIDENCE STATEMENT MATRIX
Component Rating
Evidence base B
Consistency B
Clinical impact A (overall)
Generalisability B
Applicability A

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 117
RECOMMENDATION
Magnesium sulphate be given to all women whether or not antenatal corticosteroids have been given.
B
UNRESOLVED ISSUES
Individual patient data meta-analysis needed
IMPLEMENTATION OF RECOMMENDATION
Will this recommendation result in changes in usual care? YES
Are there any resource implications associated with implementing this recommendation?
YES
Will the implementation of this recommendation require changes in the way care is currently organised?
YES
Are the guideline development group aware of any barriers to the implementation of this recommendation?
YES

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 118
Appendix F 11: Evidence Table and Graphs: COMBINED EFFECT OF ANTENATAL CORTICOSTEROIDS
Study High use of antenatal corticosteroids
Crowther 2003 yes
Rouse 2008 yes
Marret 2006 yes
Mittendorf 2002 unknown
DEATH
CEREBRAL PALSY
Study or Subgroup
16.4.1 High
Crowther 2003
Marret 2006
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 3.37, df = 2 (P = 0.19); I² = 41%
Test for overall effect: Z = 0.67 (P = 0.50)
16.4.2 Unknown
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 0.55 (P = 0.58)
Total (95% CI)
Total events
Heterogeneity: Chi² = 3.73, df = 3 (P = 0.29); I² = 20%
Test for overall effect: Z = 0.62 (P = 0.53)
Events
87
34
103
224
2
2
226
Total
629
352
1188
2169
30
30
2199
Events
107
38
96
241
1
1
242
Total
626
336
1256
2218
29
29
2247
Weight
44.6%
16.2%
38.8%
99.6%
0.4%
0.4%
100.0%
M-H, Fixed, 95% CI
0.81 [0.62, 1.05]
0.85 [0.55, 1.32]
1.13 [0.87, 1.48]
0.94 [0.79, 1.12]
1.93 [0.19, 20.18]
1.93 [0.19, 20.18]
0.95 [0.80, 1.12]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.02 0.1 1 10 50
Favours magnesium Favours no magnesium
Study or Subgroup
16.5.1 High
Crowther 2003
Marret 2006
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Chi² = 1.67, df = 2 (P = 0.43); I² = 0%
Test for overall effect: Z = 2.95 (P = 0.003)
16.5.2 Unknown
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.28 (P = 0.20)
Total (95% CI)
Total events
Heterogeneity: Chi² = 4.01, df = 3 (P = 0.26); I² = 25%
Test for overall effect: Z = 2.74 (P = 0.006)
Events
36
22
41
99
3
3
102
Total
629
352
1188
2169
30
30
2199
Events
42
30
74
146
0
0
146
Total
626
336
1256
2218
29
29
2247
Weight
29.0%
21.1%
49.5%
99.7%
0.3%
0.3%
100.0%
M-H, Fixed, 95% CI
0.85 [0.55, 1.31]
0.70 [0.41, 1.19]
0.59 [0.40, 0.85]
0.69 [0.54, 0.88]
6.77 [0.37, 125.65]
6.77 [0.37, 125.65]
0.71 [0.55, 0.91]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Fixed, 95% CI
0.005 0.1 1 10 200
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 119
F 11: COMBINED EFFECT OF ANTENATAL CORTICOSTEROIDS
DEATH OR CEREBRAL PALSY
Study or Subgroup
16.6.1 High
Crowther 2003
Marret 2006
Rouse 2008
Subtotal (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 0.49, df = 2 (P = 0.78); I² = 0%
Test for overall effect: Z = 2.41 (P = 0.02)
16.6.2 Unknown
Mittendorf 2002
Subtotal (95% CI)
Total events
Heterogeneity: Not applicable
Test for overall effect: Z = 1.48 (P = 0.14)
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 3.17, df = 3 (P = 0.37); I² = 5%
Test for overall effect: Z = 2.21 (P = 0.03)
Events
123
56
144
323
5
5
328
Total
629
352
1188
2169
30
30
2199
Events
149
67
170
386
1
1
387
Total
626
336
1256
2218
29
29
2247
Weight
39.9%
18.2%
41.4%
99.5%
0.5%
0.5%
100.0%
M-H, Random, 95% CI
0.82 [0.66, 1.02]
0.80 [0.58, 1.10]
0.90 [0.73, 1.10]
0.85 [0.74, 0.97]
4.83 [0.60, 38.90]
4.83 [0.60, 38.90]
0.85 [0.74, 0.98]
Magnesium No magnesium Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.02 0.1 1 10 50
Favours magnesium Favours no magnesium

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 120
Appendix G: Harms – Maternal; and Fetus, Infant, and Child
Maternal Harms
Effect (95% CI) No of trials
No of women
Trial references Source
CESSATION OF MATERNAL THERAPY
RR 3.12 (2.35 to 4.15) 2 3,293 Crowther 2003; Rouse 2008 Doyle 2009 (CR)
181/1631 (11.1%) vs 59/1672 (3.5%)
RR 1.59 (0.57 to 4.41) 4 310 Cotton 1984; Cox 1990; Fox 1993; Ma 1992;
Crowther 2002 (CR)
8/151 (5.3%) vs 7/159 (4.4%)
RR 2.69 (2.18 to 3.31) 1 10,110 Magpie 2002 Magpie 2002
317/4999 (6.3%) vs 118/4993 (2.4%)
Not reported in any trials Crowther 1998 (CR)
HYPOTENSION
RR 1.90 (1.11 to 3.26) 1 9,992 Magpie 2002 Duley 2003 (CR)
RR 1.51 (1.09 to 2.09) 2 1,626 Crowther 2003; Marret 2006 Doyle 2009 (CR)
RR 3.16 (0.13 to 76.30) 1 156 Cox 1990 Crowther 2002 (CR)
Overall RR 1.63 (1.23 to 2.15) 119/5896 (2.0%) vs 72/5828 (1.2%)
Not reported in any trials Crowther 1998 (CR)
RESPIRATORY DEPRESSION OR OTHER RESPIRATORY PROBLEM
RR 1.98 (1.24 to 3.15) 2 10,667 Magpie 2002; South Africa 1998 Duley 2003 (CR)
RR 1.31 (0.83 to 2.07) 2 3,303 Crowther 2003; Rouse 2008 Doyle 2009 (CR)
Overall RR 1.62 (1.17 to 2.24) 93/6975 (1.3%) vs 57/7005 (0.8%)
RESPIRATORY ARREST
RR 1.02 (0.06 to 16.25) 4 5,411 Crowther 2003; Magpie 2006; Marret 2006; Rouse 2008
Doyle 2009 (CR)
RR 3.16 (0.13 to 76.30) 1 156 Cox 1990 Crowther 2002 (CR)
RR 2.50 (0.49 to 12.88) 1 10,110 Magpie 2002 Duley 2003 (CR)
TENDON REFLEXES (absent or reduced)
RR 1.00 (0.70 to 1.42) 2 10,667 Magpie 2002; South Africa 1998 Duley 2003 (CR)
TACHYCARDIA
RR 0.0 (0.0 to 0.0) 1 35 Cotton 1984 Crowther 2002 (CR)
RR 1.53 (1.03 to 2.29) 1 1,062 Crowther 2003 Doyle 2009 (CR)
RR 1.05 (0.15 to 7.21) 1 133 Rust 1996 Crowther 1998 (CR)
CARDIAC ARREST
RR 0.34 (0.04 to 3.26) 4 5,411 Crowther 2003; Magpie 2006; Marret 2006; Rouse 2008
Doyle 2009 (CR)
RR 0.80 (0.21 to 2.98) 1 10,110 Magpie 2002 Duley 2003 (CR)
CAESAREAN
RR 1.05 (1.01 to 1.10) 6 10,108 Magpie 2002; South Africa 1994; South Africa 1998; Taiwan 1995; Memphis 1997; Tennessee 2001
Duley 2003 (CR)
2528/5082 (49.7%) vs 2370/5026 (47.2%)
RR 1.07 (0.62 to 1.83) 3 281 Cotton 1984; Cox 1990; Fox 1993 Crowther 2002 (CR)
RR 1.00 (0.93 to 1.07) 3 2,323 Crowther 2003; Marret 2006; Rouse 2008
Doyle 2009 (CR)
MORTALITY
RR 0.32 (0.01 to 7.92) 3 2,323 Crowther 2003; Marret 2006; Doyle 2009 (CR)

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 121
Rouse 2008
RR 0.54 (0.26 to 1.10) 2 10,795 Magpie 2002; South Africa 1998 Duley 2003 (CR)
ADMISSION TO ICU
RR 0.89 (0.54 to 1.47) 2 2,606 Crowther 2003; Magpie 2006 (part) Doyle 2009 (CR)
HOSPITAL STAY (days)
MD 0.17 (-0.18 to 0.53) 2 2,606 Crowther 2003; Magpie 2006 (part) Doyle 2009 (CR)
POSTPARTUM HAEMORRHAGE
RR 0.87 (0.67 to 1.12) 2 1,626 Crowther 2003; Marret 2006 Doyle 2009 (CR)
RR 0.96 (0.88 to 1.05) 2 8,909 Magpie 2002; Memphis 1997 Duley 2003 (CR)
ANY SIDE EFFECTS
RR 1.88 (1.11 to 3.20) 1 133 Rust 1996 Crowther 1998 (CR)
RR 5.26 (4.59 to 6.03) 1 9,992 Magpie 2002 Duley 2003 (CR)
1201/4999 (24.0%) vs 228/4993 (4.6%)
FLUSHING
RR 9.38 (7.74 to 11.37) 2 10,127 Magpie 2002; Memphis 1997 Duley 2003 (CR)
NAUSEA/VOMITING
RR 8.88 (5.46 to 14.43) 1 9,992 Magpie 2002 Duley 2003 (CR)
RR 0.73 (0.30 to 1.81) nausea only
1 133 Rust 1996 Crowther 1998 (CR)
RR 0.42 (0.08 to 2.08) vomiting only
1 133 Rust 1996 Crowther 1998 (CR)
DIARRHOEA
RR 7.67 (2.41 to 24.41) 1 133 Rust 1996 Crowther 1998 CR)
ABDOMINAL PAIN
RR 0.0 (0.0 to 0.0) 0 0 0 Crowther 1998 (CR)
CHEST PAIN
RR 0.0 (0.0 to 0.0) 0 0 0 Crowther 1998 (CR)
STROKE
RR 0.50 (0.13 to 2.00) 1 10,110 Magpie 2002 Duley 2003 (CR)
GIVEN CALCIUM GLUCONATE
RR 1.35 (0.63 to 2.88) 2 10,795 Magpie 2002; South Africa 1998 Duley 2003 (CR)
SLURRED SPEECH
RR 3.04 (0.13 to 73.42) 1 135 Memphis 1997 Duley 2003 (CR)
MUSCLE WEAKNESS
RR 11.99 (5.22 to 27.54) 1 9,992 Magpie 2002 Duley 2003 (CR)
DIZZINESS
RR 3.70 (1.84 to 7.42) 1 9,992 Magpie 2002 Duley 2003 (CR)
DROWSINESS/CONFUSION
RR 2.22 (1.01 to 4.87) 1 9,992 Magpie 2002 Duley 2003 (CR)
HEADACHE
RR 2.12 (1.19 to 3.76) 1 9,992 Magpie 2002 Duley 2003 (CR)
PROBLEM AT INJECTION SITE (INTRAMUSCULAR OR INTRAVENOUS)
RR 1.78 (1.52 to 2.08) 1 9,992 Magpie 2002 Duley 2003 (CR)
INDUCTION OF LABOUR
RR 0.99 (0.94 to 1.04) 1 8,774 Magpie 2002 Duley 2003 (CR)
BLOOD TRANSFUSION
RR 0.91 (0.77 to 1.09) 1 8,774 Magpie 2002 Duley 2003 (CR)
RR = risk ratio: MD = mean difference

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 122
Fetus, Infant and Child
Effect (95% CI) No of trials
No of women /infants
Trial references Source
FETAL DEATHS
RR 5.70 (0.28 to 116.87) 3 277 Cotton 1984; Cox 1990; Fox 1993 Crowther 2002 (CR)
RR 0.78 (0.42 to 1.46) 4 4,446 Crowther 2003; Marret 2006 Mittendorf 2002 (neuroprotective); Rouse 2008
Doyle 2009 (CR)
RR 0.99 (0.87 to 1.12) 3 9,961 Magpie 2002; South Africa 1998 South Africa 1994
Duley 2003 (CR)
NEONATAL AND INFANT DEATHS
RR 1.16 (0.94 to 1.42) 1 9,270 Magpie 2002 Duley 2003 (CR)
TOTAL DEATHS (FETAL, NEONATAL AND INFANT)
RR 1.74 (0.63 to 4.77) 3 292 Cotton 1984; Cox 1990; Fox 1993 Crowther 2002 (CR)
RR 0.95 (0.80 to 1.12) 4 4,446 Crowther 2003; Marret 2006; Mittendorf 2002; Rouse 2008
Doyle 2009 (CR)
RR 5.00 (0.25 to 99.16) 1 50 Ricci 1991 Crowther 1998 (CR)
ASSISTED VENTILATION
RR 1.17 (0.61 to 2.24) 1 165 Cox 1990 Crowther 2002 (CR)
NECROTISING ENTEROCOLITIS (NEC)
RR 1.19 (0.33 to 4.29) 3 289 Cotton 1984; Cox 1990; Fox 1993 Crowther 2002 (CR)
ADMISSION TO NEONATAL ICU/SCN
RR 0.49 (0.18 to 1.32) 1 165 Cox 1990 Crowther 2002 (CR)
RR 1.57 (0.76 to 3.24) 1 133 Rust 1996 Crowther 1998 (CR)
RR 1.01 (0.96 to 1.06) 1 8,260 Magpie 2002 Duley 2003 (CR)
APGAR SCORE <7 at 5 MINUTES
RR 1.03 (0.90 to 1.18) 3 4,387 Crowther 2003 Marret 2006 Rouse 2008
Doyle 2009 (CR)
RR 1.02 (0.85 to 1.22) 1 8,260 Magpie 2002 Duley 2003 (CR)
NEONATAL CONVULSIONS
RR 0.80 (0.56 to 1.13) 3 4,387 Crowther 2003 Marret 2006 Rouse 2008
Doyle 2009 (CR)
NEONATAL HYPOTONIA
RR 1.02 (0.77 to 1.36) 1 2,444 Rouse 2008 Doyle 2009 (CR)
CHRONIC LUNG DISEASE (oxygen at 36 days)
RR 1.12 (0.95 to 1.32) 2 1,943 Crowther 2003 Marret 2006
Doyle 2009 (CR)
CHRONIC LUNG DISEASE (oxygen at 28 days)
RR 1.07 (0.94 to 1.22) 1 1,255 Crowther 2003 Doyle 2009 (CR)
INTRAVENTRICULAR HAEMORRHAGE TOTAL
RR 0.86 (0.28 to 2.62) 3 289 Cotton 1984 Cox 1990 Fox 1993
Crowther 2002 (CR)
RR 3.00 (0.13 to 70.30) 1 50 Ricci 1991 Crowther 1998 (CR)
RR 0.96 (0.86 to 1.08) 4 4,552 Crowther 2003 Marret 2006 Mittendorf 2002 Rouse 2008
Doyle 2009 (CR)
INTRAVENTRICULAR HAEMORRHAGE (SEVERE GRADES 3 & 4)

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 123
RR 0.0 1 90 Fox 1993 Crowther 2002 (CR)
RR 0.83 (0.62 to 1.13) 2 3699 Crowther 2003 Rouse 2008
Doyle 2009 (CR)
INTRAVENTRICULAR HAEMORRAGE (SEVERE GRADES 3 & 4) OR PVL
RR 0.0 1 90 Fox 1993 Crowther 2002 (CR)
PERIVENTRICULAR LEUKOMALACIA
RR 0.0 1 90 Fox 1993 Crowther 2002 (CR)
RR 0.93 (0.68 to 1.28) 4 4,552 Crowther 2003 Marret 2006 Mittendorf 2002 Rouse 2008
Doyle 2009 (CR)
NEONATAL LENGTH OF STAY
MD 1.18 (-0.46 to 2.82) days
2 180 Ricci 1991 Rust 1996
Crowther 1998 (CR)
RR 1.02 (0.93 to 1.11) (> 7 days)
1 8,260 Magpie 2002 Duley 2003 (CR)

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 124
Appendix H: Additional Information about Regimens and Monitoring for giving Magnesium Sulphate to Prevent
Eclampsia from Clinical Practice Guidelines and Management Protocols
Condition The Society of Obstetric Medicine of Australia and New Zealand (SOMANZ) recommend magnesium sulphate as the drug of choice for prophylaxis against eclampsia for women with preeclampsia. The World Health Organization (WHO), Royal College of Obstetricians and Gynaecologists (RCOG) and Society of Obstetricians and Gynaecologists of Canada (SOGC) give more cautious recommendations, indicating that treatment with magnesium sulphate is recommended in severe pre-eclampsia. SOGC qualifies this by indicating that magnesium sulphate may be given for women with non-severe preeclampsia. SOGC does not give any guidelines on recommended dosage regimens. RCOG indicates that in cases of less severe disease the decision is less clear and will depend on an individual case assessment. The New South Wales Department of Health is more conservative indicating it is appropriate for use for seizure prophylaxis in a woman who has already had an eclamptic seizure and indicates that the efficacy is less certain for use as a seizure prophylaxis in a woman with severe pre-eclampsia who is at risk of eclampsia (Table H1).
Loading Dose
A loading dose of 4 g of magnesium sulphate is recommended by all those guidelines that specified doses. Administration recommendations for the loading dose vary
when administered by infusion pumps, with both the volume and time of administration differing. However, the syringe pump administration recommendations are
similar. RCOG and SOMANZ do not give any recommendation for the administration of the loading dose in either the infusion or syringe pump. SOMANZ indicate
that it is appropriate that obstetric units determine their own protocols. The Royal Women’s Hospital (Victoria) guidelines do not give any recommendation for the
administration of the loading dose by infusion pump (Table H2).
Maintenance dose
Most of the guidelines consulted who specified doses recommend 1 g of magnesium sulphate per hour as a maintenance dose. SOMANZ is the exception with 1-2 g
of magnesium sulphate per hour recommended as a maintenance dose. All guidelines who specified doses recommend a maintenance period of 24 hrs either after
birth and/or 24 hrs after last seizure. RCOG and SOMANZ do not give any recommendation for the administration of the maintenance dose in either the infusion or
syringe pump. SOMANZ indicate that it is appropriate that obstetric units determine their own protocols. In addition, the South Australian guidelines recommend a
total daily dose not exceeding 30-40 g of magnesium sulphate (Table H3).
Monitoring
SOMANZ recommend monitoring of serum levels of magnesium sulphate, however they indicate that it is appropriate that obstetric units determine their own
protocols for monitoring outcomes. RCOG recommend ‘regular assessment’ but give no indication of timing. The Royal Women’s Hospital (Victoria) guidelines
recommend monitoring for 4 hrs following the discontinuation of the magnesium infusion (Tables H4 and H5).

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 125
Table H.1: Magnesium sulphate recommendation for condition
Guidelines Condition
NSW Seizure prophylaxis in a woman with severe pre-eclampsia who is at risk of eclampsia (although efficacy for this is less certain).
Seizure prophylaxis in a woman who has already had an eclamptic seizure.
The Royal Women’s Hosp, VIC Women with preeclampsia for whom there concern about the risk of eclampsia.
Management of an eclamptic seizure.
SA Pre-eclampsia to prevent eclampsia (prophylaxis).
For eclamptic seizures.
RCOG Consider for severe pre-eclampsia where there is concern about risk of eclampsia.
Women with less severe pre-eclampsia, the decision to use MgSO4 is less clear and depends on the individual case.
Eclampsia for seizures.
SOMANZ Preeclampsia (prevention of eclampsia).
For eclamptic seizures.
WHO To prevent seizure in a woman with severe pre-eclampsia.
Prevention and treatment of eclampsia.
SOGC Eclampsia.
Women with severe pre-eclampsia to prevent eclampsia (prophylaxis).
Consider for women with non-severe pre-eclampsia.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 126
Table H.2 Recommended intravenous (IV) loading dose of magnesium sulphate for treating pre-eclampsia and eclampsia
Guidelines Condition (see Table H.1 for details)
Dosage in Grams (g)
Infusion by infusion pump Infusion by syringe pump Other
Volume MgSO4 Solution concentration
Time Volume
MgSO4 Solution concentration
Time
NSW Pre-eclampsia/ Eclampsia
4 g 108 mL add 8 mL of 50% soln to 100 mL saline
20-30 min 8 mL 9 mL of 50% soln, prime line with 1 mL
15 min
The Royal Women’s Hosp, VIC
Pre-eclampsia 4 g 8 mL 50% soln 15 min
Eclampsia 4 g 8 mL 50% soln 5 min to 10 min
SA Pre-eclampsia 4 g 20 mL 40 mL 50% soln in 60 mL saline
20 min 8 mL 50% soln 20 min
Eclampsia 4 g 20 mL 40 mL 50% soln in 60 mL saline
10 min 8 mL 50% soln 10 min
RCOG Eclampsia 4 g 5-10 min IV by infusion pump
SOMANZ Eclampsia 4 g 10-15 min IV infusion (no details of type)
WHO Pre-eclampsia/ 4 g IV infusion (20% solution) over 5 min
Eclampsia
If blank then this indicates no information for this variable
If separate regimens were given for the different conditions then these are stated, if not stated separately, only one regimen was given for both conditions.
soln=solution
SCOG gives no recommendations on volume or concentration

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 127
Table H.3 Recommended intravenous (IV)* maintenance dose of magnesium sulphate for the treatment of pre-eclampsia and eclampsia
Guideline Condition (see Table H.1 for details)
Dosage in grams (g)
Timing Infusion by infusion pump Infusion by syringe pump Other Time period for continuing maintenance dose
Volume Per hour
MgSO4 Solution concentration
Volume Per hour
MgSO4 Solution concentration
NSW Pre-eclampsia / Eclampsia
1 g per hour
40 mL add 20 mL of MgSO4 50% soln to 380 mL saline
2 mL 50 mL of 50% soln, prime line with 1 mL
At least 24 hrs
The Royal Women’s Hosp, VIC
Pre-eclampsia / Eclampsia
1 g per hour
2 mL 50 mL of 50% soln
At least 24 hrs after birth
SA Pre-eclampsia / Eclampsia
1 g per hour
5 mL 20% soln (40 mL 50% soln in 60 mL saline)
2 mL 50% soln For 24 hrs after last seizure and 24 hr after birth
RCOG Eclampsia 1 g per hour
Later of 24 hrs after last seizure or 24 hrs after birth Unless clinical reason for continuing
SOMANZ Eclampsia 1-2 g per hour
IV infusion (no details of type)
For 24 hrs after last seizure
SCOG gives no recommendations on volume or concentration
*WHO recommends intramuscular maintenance
If blank then this indicates no information for this variable
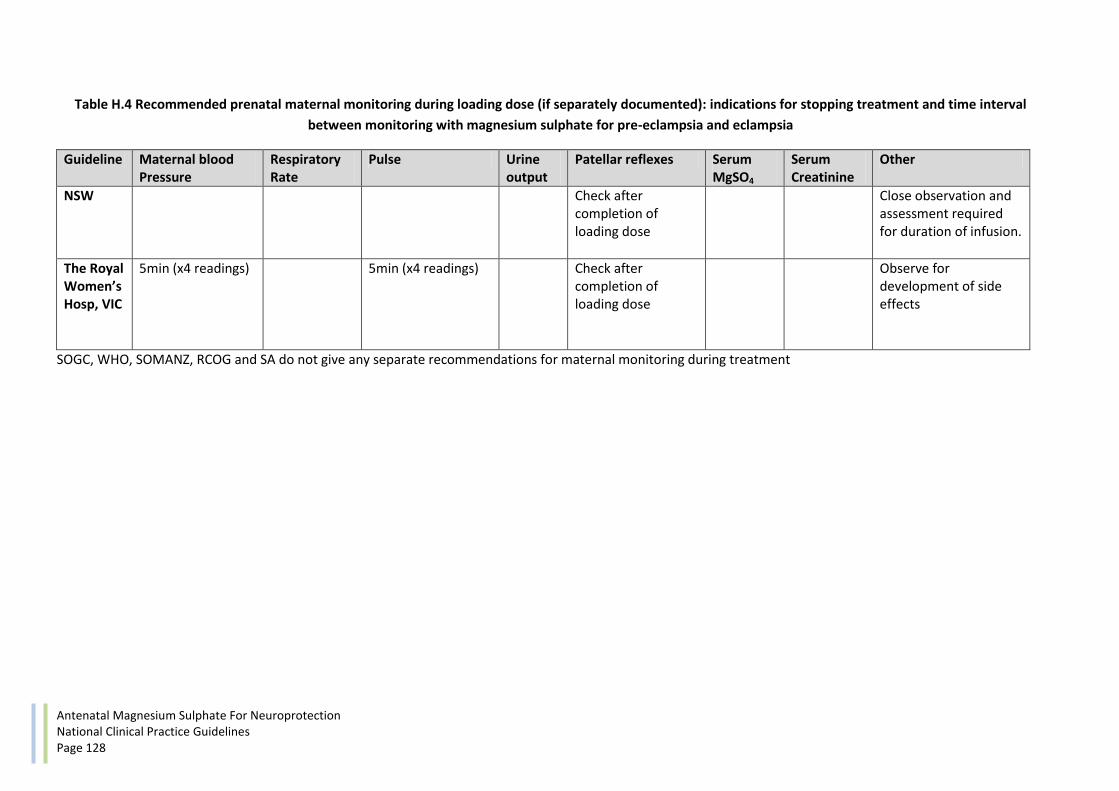
Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 128
Table H.4 Recommended prenatal maternal monitoring during loading dose (if separately documented): indications for stopping treatment and time interval
between monitoring with magnesium sulphate for pre-eclampsia and eclampsia
Guideline Maternal blood Pressure
Respiratory Rate
Pulse Urine output
Patellar reflexes Serum MgSO4
Serum Creatinine
Other
NSW Check after completion of loading dose
Close observation and assessment required for duration of infusion.
The Royal Women’s Hosp, VIC
5min (x4 readings) 5min (x4 readings) Check after completion of loading dose
Observe for development of side effects
SOGC, WHO, SOMANZ, RCOG and SA do not give any separate recommendations for maternal monitoring during treatment

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 129
Table H.5 Recommended prenatal maternal monitoring during maintenance dosage: time interval between monitoring and indications for review or stopping
treatment with magnesium sulphate for pre-eclampsia and eclampsia
Guideline Maternal blood Pressure
Respiratory Rate
Pulse Urine output Serum creatinine
Patellar reflexes
Serum MgSO4 Other
NSW 1-2 hr 1-2 hr, stop if <10 breaths per min
1-2 hr 1-2 hr, Stop if <30 mL for 3 consecutive hrs
2 hrs, Stop if absent
At 1 hr after commencing infusion then as clinically indicated
Where woman’s condition is unstable increase frequency of observation
The Royal Women’s Hosp, VIC
0.5 hr 0.5 hr should be ≥16 per min, review if <12 per min
0.5 hr 1 hr urine, 4 hrs urinary protein Review if <100 mL urine in 4 hrs
1 hr, Review if absent
6 hrs or Request if any of respiratory, urine or reflexes are under review or further seizures or renal impairment.
2 hr temperature **ECG monitoring and anaesthetist aware of woman’s medical condition
SA 1hr 1 hr, stop if <10-12 breaths per min
insert indwelling catheter and monitor 1hrly, if <100 ml over 4 hrs check serum MgSO4
6 hrs, if >100mmol/L check serum MgSO4
Minimum 4 hourly, stop if absent
Test 6 hrly if serum creatinine >100 mmol/L or urine <100 mL over 4 hrs
1hr Pulse SpO2 oximeter **ECG monitoring and anaesthetist on site
SOMANZ YES YES YES YES YES Oxygen saturation
RCOG If respiratory rate depression (no details) give calcium gluconate 1 g over 10 min
Stop if <20 mL/hr Stop if absent
“Magnesium toxicity is unlikely with these regimens and levels do not need to be routinely measured”
WHO Stop or delay if <16 per min
Stop or delay if output is less than 30 mL per hr over preceding 4 hrs
Stop or delay if absent
** for eclamptic seizures only

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 130
Table H.6 Antidote for magnesium sulphate toxicity
Guidelines Antidote
NSW Calcium chloride or calcium gluconate (10 mL of 10% solution) by slow intravenous injection over 3 minutes.
The Royal Women’s Hosp, VIC Calcium gluconate (10 mL of 10% solution over 10 minutes) by slow intravenous injection. The patient requires ECG monitoring during and after administration because of the potential for cardiac arrhythmias. Resuscitation and ventilator support should be available during and after administration of both magnesium sulphate and calcium gluconate.
SA Call for medical assistance, administer oxygen at 8-12 litres, stop infusion, monitor vital signs. Administer Calcium gluconate (10% solution), 10 mL, slowly, IV check electrolytes, creatinine, magnesium sulphate concentrations.
RCOG Calcium gluconate 1 g (10 mL) over 10min can be given if concern over respiratory depression.
WHO Give calcium gluconate 1 g (10 mL of 10% soln) IV slowly over 10 min until respirations satisfactory. Assist ventilation using mask and bag, anaesthetic apparatus or intubation.
SOMANZ and SOGC do not give recommendations of antidote
Table H.7 Details of magnesium sulphate concentrations and effects (taken from The Royal Women’s Hospital, VIC guidelines)
Magnesium sulphate concentrations (mmol/L)
Effects
0.8-1.0 Normal plasma concentrations
1.7-3.5 Therapeutic range
2.5-5.0 ECG changes (P-Q interval prolongation, widen QRS complex)
4.0-5.0 Reduction in deep tendon reflexes
>5.0 Loss of deep tendon reflexes
>7.5 Sinoatrial and atrioventricular blockade. Respiratory paralysis and CNS depression
>12 Cardiac arrest

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 131
References
Guidelines for the management of hypertensive disorders of pregnancy 2008. Society of Obstetric Medicine of Australia and New Zealand (SOMANZ).
The management of severe preeclampsia/eclampsia. Royal College of Obstetricians and Gynaecologists (RCOG) Guideline No. 10(A). March 2006.
Clinical practice guidelines: Diagnosis, evaluation and management of hypertensive disorders of pregnancy. The Society of Obstetricians and Gynaecologists of Canada
(SOGC). Journal of Obstetrics and Gynaecology Canada volume 30 March 2008 supplement 1.
Magnesium sulphate protocol CPG. Magnesium sulphate is the anticonvulsant of choice for preeclampsia prophylaxis and treatment. The Royal Women’s Hospital,
Victoria, Australia. Dec 2009.
Policy directive. Magnesium sulphate (MgSO4) infusion protocol for eclamptic seizure prophylaxis. New South Wales Department of Health, Australia.
Education material for teachers of midwifery. Midwifery education modules -2nd edition. Managing eclampsia. World Health Organization (WHO).
Maternity care in South Australia. Perinatal practice guidelines. Section 6 chapter 96. Magnesium sulphate infusion regimen. 26th Oct 2009.

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 132
Recommended loading dose of magnesium sulphate from trials
Trial Arm of trial Dosage in
Grams (g)
Infusion Other details
Volume MgSO4 solution concentration time type
Rouse 2008 6 g 20-30 min IV infusion
Crowther 2003 4 g 8 mL 16 mmol of 0.5% MgSO4 soln 20 min IV infusion
Marret 2006 4 g 40 mL 0.1g/mL MgSO4 soln 30 min IV infusion Single dose
Mittendorf 2002 Tocolytic 4 g IV infusion
Neuroprotective 4 g Single dose
If blank then this indicates no information for this variable
Recommended maintenance dose of magnesium sulphate from trials
Trial Arm of trial Dosage in
Grams (g)
Infusion Other details
Volume MgSO4 solution concentration time type
Rouse 2008 2 g Per hr IV infusion
Crowther 2003 1 g 2 mL 0.5% MgSO4 soln Per hr IV infusion
Marret 2006 No maintenance dose given
Mittendorf 2002 Tocolytic 2-3 g Per hr IV infusion
Neuroprotective No maintenance dose given
If blank then this indicates no information for this variable

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 133
Recommended prenatal maternal monitoring during magnesium sulphate dosage for fetal, infant and child neuroprotection
Trial Monitoring Cease treatment
Rouse 2008 No details Discontinue if birth had not occurred after 12 hrs and no longer considered imminent
Crowther 2003 Pulse rate, blood pressure, respiratory rate monitored throughout infusion and any maternal adverse events recorded
Stop if respiratory rate decreases more than 4/min below baseline, diastolic blood pressure decreases more than 15mmHg below baseline
Marret 2006 Pulse rate, blood pressure, respiratory rate, tendon reflex and any maternal adverse effects recorded throughout infusion
Stopped at anaesthetist discretion
Mittendorf 2002 Pulse rate, blood pressure/respiratory rate monitored throughout infusion and maternal side effects recorded
Stop if respiratory rate drops below 16/min or if blood pressure drops more than 15mm Hg below baseline

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 134
Appendix I: Public consultation comments and Panel responses
Comment Received Response/Justification
1 Patient information sheets
Information sheets and/or leaflets be designed
and provided which will provide clear and
comprehensive information and explanation of
the treatment and range of side effects so that
women are able to make an informed decision.
Information sheets relevant for consumers will be
prepared and disseminated after the main
guideline documents have been finalised.
2 Information and education for midwives.
A comprehensive strategy be considered to
ensure that midwives can access information and
education regarding the administration of
magnesium sulphate during the antenatal period
for women at high risk of pre term labour.
The clinical practice guidelines provide guidance on
administration of magnesium sulphate during the
antenatal period and will be readily available for
use by midwives in their practice. In addition we
expect that individual centres will already have
individual obstetric unit protocols or develop more
detailed local protocols based on the Guidelines.
3 Patient care during administration of
magnesium sulphate.
During administration of magnesium sulphate the
woman should receive one on one midwifery
care in the birthing suite of a facility (not in an
antenatal or postnatal ward).
When magnesium sulphate is administered the
recommended monitoring under good practice
points should be available. We expect that each
maternity health facility will have their own
protocols regarding models of care.
4 Audit and follow up.
Long term audit and follow up of the women and
babies who have received magnesium sulphate
prior to 30 weeks’ gestation to ensure benefit.
Agree. The Guidelines recommend an audit
process (page 14).
5 Further research.
Further research is prioritised to studying the
impact for women of administration of
magnesium sulphate.
Agree. The priority research recommendations are
given within the guidelines (page 14) and these
focus on outcomes for women and their babies.
6 Monitoring recommendations.
Minimum standards of observations to include:
a. monitoring of oxygen saturation;
a. The Panel consider that monitoring oxygen saturation is not required as a minimum standard – respiratory rate is reduced by magnesium sulphate serum concentrations above the therapeutic range and therefore is an appropriate minimum observation for respiratory depression. Recording respiratory rate has been a standard monitoring requirement for using magnesium sulphate for

Antenatal Magnesium Sulphate For Neuroprotection National Clinical Practice Guidelines Page 135
b. reflexes prior to loading dose to gain
baseline reflex responses; c. temperature; and
d. continuous fetal heart monitoring
pre-eclampsia. b. This has been added to baseline assessment
within the Guidelines. c. The flushing experienced by women with a
magnesium sulphate infusion is not related to a temperature rise. Routine temperature monitoring is therefore not required.
d. The method and frequency of monitoring the fetal heart should be determined by the underlying clinical condition of the woman and her fetus.
7 Gestation at which magnesium sulphate is administered.
Evidence supports a likely benefit in the large group of infants born between 30.0 and 33.6 weeks’ gestation. We would consider 32 weeks’ gestation as a compromise position.
The Panel decided that current evidence to support this wider interpretation is not strong enough for National Clinical Guidelines therefore the recommendations are not open to all gestational ages at this point in time. Further research of higher gestational ages through RCTs and individual patient data (IPD) meta-analysis is needed and in planning stages.
8 Timing of magnesium sulphate administration.
The clinical recommendation and relevant good practices points should be combined to achieve greater clarity and consistency.
The clinical recommendation and good practice points each deal with a different clinical scenario; time to give magnesium sulphate prior to planned birth time; severe fetal and maternal compromise; and birth expected within 4 hours. The Panel considered that the clinical recommendation should stand alone and be supported by separate good practice points.
9 Loading dose regimen for magnesium sulphate.
Clinical recommendation is confusing.
The Panel consider that a statement about no immediate repeat doses is important and appropriate to include within the clinical recommendation.
10 Repeat magnesium sulphate at a later gestation if birth does not occur when magnesium sulphate first administered.
Giving discretion to the ‘attending health professional’.
As evidence about need for repeat doses is presently unclear no firm recommendation can be given. The decision needs to be at the discretion of the attending health professional.
11 Nifedipine administration.
The interaction between magnesium sulphate and nifedipine in relation to hypotension.
We have included additional information about hypotension in monitoring under good practice points.

Antenatal Magnesium SulphatePrior to Preterm Birth for Neuroprotection
of the Fetus, Infant and Child
Antenatal M
agnesium Sulphate Prior to Preterm
Birth for Neuroprotection of the Fetus, Infant and Child
Prepared by the
Antenatal Magnesium Sulphate
For Neuroprotection
Guideline Development Panel
2010
Nati onal Clinical Practi ce Guidelines


















