18_Elbow Trauma.ppt
42
ELBOW TRAUMA
-
Upload
drcoolcat2000 -
Category
Documents
-
view
22 -
download
4
Transcript of 18_Elbow Trauma.ppt

ELBOW TRAUMA

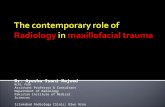
RADIAL HEAD FRACTURES

MASON CLASSIFICATION

NON-OP TREATMENT
Indications:– Mason 1– Mason 2
Tx: Sling for comfortImmobilization no more than 2 weeks to
prevent elbow stiffness!Fracture displacement and nonunion is usually
asymtomatic and inconsequential (Ring - CORR 2002, Cobb – Orthopedics 1998)

OPERATIVE INDICATIONS
Traditionally 1) >2 mm displacement
2) >30% of joint involvement
Most Importantly: Blocked forearm rotation Mason 3 fracture (displaced comminuted)

OPERATIVE TX OPTIONS
ExcisionORIFArthroplasty

RADIAL HEAD EXCISION
Isolated radial head fracture – No Essex-Lopresti lesion– No terrible triad– No MCL injury
In older patients with limited functional demands

ORIF
Mason type 2: 15/15 had satisfactory resultMason type 3 with 2-3 fragments: 1/12
nonunionMason type 3 with >3 fragments: 13/14 had
unsatisfactory results(Ring JBJS Am 2002)
If >3 fragments, consider arthroplasty

ARTHROPLASTY
N=1680% good or excellent results at 2.8y f/uEarly mobilization important for
satisfactory outcome(Bain JBJS Am 2005)







SURGICAL ANATOMY
Pronation of forearm translates PIN 1 cm away from operative field
Safe zone of lateral radius: Proximal 38 mm Supination decreases safe zone to 22 mm
(Diliberti JBJS Am 2000)

IMPLANT PLACEMENT ON RADIAL HEAD
110° safe zone on lateral aspect to prevent impingement in sigmoid notch
Make horizontal marks in forearm in neutral, pronation and supination
Limits:– Anterior: ½ distance from between mark in neutral
and supination– Posterior: 2/3 distance from between mark in neutral
and pronation
(Corresponds to region between Listers tubercle and radial styloid)

PROXIMAL ULNA FRACTURES


PROXIMAL ULNA FRACTURES: Treatment Options
Plating Tension Band


TENSION BAND (Macko JBJS Am 1985)
Most common complication: Prominent hardware
Indication: Transverse fracture with no comminution



PLATING (Bailey JOT 2001)
22/25 good or excellent results20% requested plate removal





CORONOID FRACTURES

CORONOID FRACTURE: Morrey and Regan ClassificationType 1: Avulsion of the tip of the processType 2: 50% of the processType 3: >50% of the process

CORONOID FRACTURES Type 1: Sutures around the fragment Type 2: Sutures through drill holes in ulna Type 3: Screws
Small fragments associated with more challenging injury pattern!

CORONOID FRACTURE: O’Driscoll’s Classification

ELBOW DISLOCATIONS

ELBOW STABILIZERS
1) Lateral collateral ligament
2) Coronoid
3) Radial head

ELBOW DISLOCATION
Non-op or Radial head excision + CastGood results if no coronoid fractureRadial head was ultimate determinant of
outcome with many radial head resections needed to restore forearm rotation(Broberg & Morrey CORR 1987)

TERRIBLE TRIAD
1) Elbow dislocation
2) Coronoid fracture
3) Radial head fracture

CURRENT MANAGEMENT
Radial head ORIF or arthroplastyCoronoid fixation
If still unstable (dislocation with 30° Ext)

LCL + MCL REPAIR

CROSS PINS

EX-FIX

HINDGED BRACE