#{188}. /7
32
Transcript of #{188}. /7


#{188}. /7
r7�
Forsuppoft&e blood thempy,consider the IBM blood cellseparator and processors.
They make quite a team.
(I,’
4’
/
2997 blood cellseparator.

�IlI1*’ #{149}.�
S
a.
/
For blood bankers, oncolo-gists, pathologists and hema-tologists, the IBM 2997 blood cellseparatorand the IBM 2991 bloodcellprocessors are a logical choice.
The IBM 2997 provides� � high yields ofplatelets, leukocytess’ ‘ � and plasma at low extracorporeal
volume.Because you’re con-
cerned enough about patient sen-sitization to use HLA-matched
granulocytes and platelets,you’ll also want to use leukocyte-poor red cell units. These are
easily prepared on the IBM2991 blood cell processors.Using leukocyte-poor red cellunits can lessen the chance ofadverse transfusion reactions.
Both of the 2991models do an excellent job ofwashing red blood cells,includ-ing thawed cells. They alsoreduce microaggregates andsalvage red cells fromoxygenators after surgery
The 2997 and the 2991use disposable plastic supplies,have built-insafety features andare easyto use.
If you’d like to find out.more about what our 2997 bloodcell separator and our 2991 bloodcell processors can do for you,call IBM DIRECT toll-free8001631-5582 (in New Jersey8001352-4960), or write to us, IBMBiomedical Systems, P0. Box 10,Dept. MA, Princeton, NJ 08540.
processormode/i.
p
2991 blood ce/lprocessor model2.
- - -- - -
- - - - -- - --- - - - - -
- - - -
- . -
Biomedical Systems
Th15 On�
I�UI�III�III�I�II�flhUhI�IIUIIIllhIII�IllII�ID7NW- 06K- P2OZ

1. VAND EXTRACTS
#{149}DETECTION OF ASAS 2 MIU* OF HUMAN
perML IN SERUM
#{149}RAPIDS QUANT1TATION REQUIRESLESS ThAN 21/2 HOURS - FASTERQUALITATIVE ASSAY USEFUL INRESEARCH COLUMN MONITORING
#{149}SIMPLE TO PERFORM -
HEMAGGLUTINATION INHIBITIONMETHOD - UTILIZES MICROTITEREQUIPMENT
ANTI HUMAN ERYTHROPOIETIN SERUMANTI HUMAN ERYTHROPOIETIN SERUM IS PRODUCED IN COATS AGAINSTPARTIALLY PURIFIED HUMAN URINARY ERYTHROPOEITIN. THE PURITY, TITERAND MONOSPECIFICITY ARE DETERMINED USING QUANTITATIVE PRECIPITINTECHNIQUES, IMMUNOELECTROPHORESIS AND HEMACCLUTINATION INHI-BITION. NON-SPECIFIC ANTIBODIES ARE REMOVED. NO CROSS REACTIVITYWITH 14 MAJOR SERUM PROTEINS.

A Subsidiary of Harcourt Brace Jovanovich, Publishers
B ODThe Journal of
The American Society of Hematology
Blood: The Journal of The American Society of
Hematology (ISSN 0006-497 1) is published month-
ly, in two volumes per year. Second class postage paid
at New York, N.Y., and at additional mailing offices.
Editorial correspondence should be addressed to:
Dr. Paul A. Marks, Editor
BLOOD
Columbia University College
of Physicians and Surgeons
701 W. 168 St.
New York, N. Y. 10032
Other correspondence (copyediting, production,
subscriptions, changes of address, etc.) should be
addressed to:
Mr. Kenneth Brown, Managing Editor
BLOOD
Grune & Stratton, Inc.
1 1 1 Fifth Ave.
New York, N. Y. 10003
Subscription rates: $66.00 per year within the
United States; foreign, $70.00 per year. Students,
Research Fellows, Interns, and Residents may receive
a reduced subscription rate: $49.00 per year within the
United States; foreign, $53.00 per year. A letter giving
qualifying data must accompany such orders. Single
copies: U.S., $8.50; foreign, $9.00. Subscriptions are
accepted on a calendar-year basis. Prices are subject
to change. Back-issue and back-volume prices are
those in current effect.
Change-of-address notices, including both the
subscriber’s old and new address, should be sent to the
publisher at least one month in advance.
Advertising Representative: Charles C. Cunning-
ham, Inc., P.O. Box 308, Park Ridge, New Jersey
07656, telephone (201) 391-3210.
Agents for Great Britain: Academic Press, Inc.
(London) Limited, 24-28 Oval Road, London NW1
7DX, England. Agents for Australia and New
Zealand: Harcourt Brace Jovanovich Group (Austra-
ha) Pty. Ltd., P.O. Box 300, North Ryde, N.S.W.
21 13, Australia.
The appearance of the code at the bottom of the
first page of an article in this journal indicates the
copyright owner’s consent that copies of the article
may be made for personal or internal use, or for the
personal or internal use of specific clients. This
consent is given on the condition, however, that the
copier pay the stated per-copy fee through the Copy-
right Clearance Center, Inc. for copying beyond that
permitted by Sections 107 or 108 of the U.S. Copy-
right law. This consent does not extend to other kinds
of copying, such as copying for general distribution,
for advertising or promotional purposes, for creating
new collective works, or for resale. Absence of the code
indicates that the material may not be processed
through the Copyright Clearance Center.
Postmaster: Send 3579 to 300 West Chestnut St.,
Ephrata, Pa. 17522. Return postage guaranteed.
The American Society of Hematology certifies that the continuing medical education offering provided by
BLOOD, The Journal ofthe American Society ofHematology, meets the criteriafor up to 22 hours ofcredit in
Category 5(a)for the Physician’s Recognition Award ofthe American Medical Association.
© 1980, Grune & Stratton, Inc. 1 1 1 Fifth Avenue, New York 10003

Bone MarrowSampling System
TM
PATENT PENDING
Filtration system for concentrating marrow tissuein the management of hematological disorders.
Features of PrepacellTM (PatentPending) System:
. Clinically tested in over 100 patients
#{149}FDA Registered
. Eliminates dry tap situations inbone marrow aspirations
#{149}System designed and tested by aHematologist
#{149}Sterile and completely disposable
#{149}Syringe and filter fused into asingle airtight unit.
#{149}Unit is easily dismantled exposingmarrow tissue on filter pad
#{149}Luer lock on unit for needle
attachment
D � El Applied Medical Devices, Inc.7346 SOUTH ALTON WAYSUITE KENGLEWOOD, COLORADO 60112(303) 773-6513800-525-7626

POSTDOCTORAL FELLOWSHIP IN
BLOOD BANKING, AMERICAN RED
CROSS, WASHINGTON, D.C. AVAIL- JUNIOR FACULTY POSITION available
ABLE JULY 1, 1981. REQUIREMENTS University of California, San Francisco,Department of Medicine and Cancer
INCLUDE M.D. DEGREE, LICENSE TO Research Institute, to direct adult bone
PRACTICE MEDICINE IN STATE OR marrow transplantation unit and related
TERRITORY OF U.S. AND EITHER U.S. research program. Candidate must beboard certified in hematology or oncology.
CITIZENSHIP OR PERMANENT RESI- Salary commensurate with previous experi-
DENTS VISA. SEND C.V., BIBLIOGRA- ence. Inquiries to Stephen B. Shohet, M.D.,
PHY NAMES OF FOUR REFERENCES Director, Cancer Research Institute,, 1282-M, University of California, San Fran-
TO KRIS MURAWSKI, M.D., AMERI- cisco, CA 94143. An Equal Opportunity
CAN RED CROSS BLOOD SERVICES, and Affirmative Action Employer.
1730 “E” STREET, N.W., WASHING-
TON, D.C. 20006 EOE M/F
rvMan, Cancer and Immunity
A.J. CochranUniversity Deportment of Pathology, Western Infirmary, Glasgo w, Scotland
1978, 2O6pp. 0.12.177550.X
Evidence has been accumulating during the last decade to suggest that some cancerpatients react against their tumours,�and that the immune system is involved in thisreaction. In this book, studies in vivo and in vitro, which demonstrate such interactions,
are critically discussed. These include assessments of membrane characteristics of tumourcells, the different classes of tumour-associated antigens, the immunological reactions tosuch antigens and the mechanisms whereby tumour cells may survive and proliferate inthe presence of established anti-tumour immunity. Also considered are the more clinicalaspects, detection and quantification of immune responses to tumour cells and the effectsof conventional forms of treatment of cancer on such responses. The utility of immuno-logical assessment in cancer diagnosis, prognosis, treatment planning and monitoring theclinically tumour free individual is discussed. Whereas much of the previously publishedwork on this subject has devoted attention to studies in animals, in this volume theauthor concentrates on studies in Man.
“The best parts of this book are those which deal with Dr Cochran ‘s extensive research onthis subject, for we are following an explorer on his own voyages ofdiscovery. When he isrecounting his own work the book is vivid, well illustrated, and written in a strong andeager prose which carries the reader along with little effort. The o ther sections of thebook also have many virtues. “ British Medical Journal, Jan. 1979
Academic Press London New York San FranciscoA Subsidiary of Harcourt Brace Jovanovich, Publishers24-28 Oval Road, London NW!, England.
�rLl Fifth Avenue, New York, NY 10003, USA APL 0001

FROM PARKE-DAVIS RESEARCH
A BREAKTHROUGHIN THE TREATMENT OF
A MAJORVIRAL DISEASE
1

�‘ ...� : . #{149}f�’ . , .�- ,‘; � .-‘
© 1979 Wamer-Lambert Company
Parenteral
(vidarabinefor
infusion)

N�=1O
80-
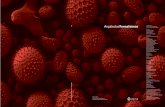
Fig. I Morbidity and mortality in biopsy-proved Herpes simplex
virus encephalitis
NIAIDSTUDY N=18
100-
0 ALIVE, NO OR MINORSEQUELAE
I ALIVE, MODERATESEOUELAE
U ALIVE, SEVERESEQUELAE
U DEAD
‘National Instituteof Allergy andInfectious Diseases-adapted from Whitley, at at’
U)
z
� 60-
z 40-UiC)
UiQ.
20-
VIRA-A’ PLACEBO’THERAPY
‘P - 0.03 AT DAY 30
Early diagnosis and treatment are essential
A significant contributionin reducinS mortality of patients withHerpes simplex virus encephalitis
Controlled studies indicate that VIRA-A
(vidarabine for infusion) reduced the
mortality caused by Herpes simplex
virus encephalitis from 70% to 28%
(Chi-square analyses, P 0.03) (Fig. 1).1
Of 28 patients who were brain-biopsy
positive for Herpes simplex virus,
18 received VIRA-A and 10 received
1
There is a direct relationship between
the outcome of therapy and the state of
consciousness at the time that VIRA-A
therapy is initiated. Once the comatose
state is reached in the patient with
Herpes simplex virus encephalitis,
therapy may be futile.’ In the same
double-blind placebo-controlled study of
VIRA-A, over half the comatose patients
died in spite of active drug therapy,
and all the survivors were severelyneurologically debilitated. But no deaths
occurred among lethargic patients
treated with VIllA-A, and six of seven
survivors had only minor or moderate
neurologic complications.’
After localization of an intracerebral
lesion by brain scan, electroencepha-
lography, and/or computerized axialtomography, brain biopsy is required to
confirm the etiologic diagnosis by means
of viral isolation in cell cultures. Detec-
tion of Herpes simplex virus in the
biopsied brain tissue can also be reliably
done by specific fluorescent antibody
techniques.
Recommended Dosage:ISmg/kg/dayfor lOdays
Note: There are no clinical studies
available to indicate that VIRA-A
(vidarabine for infusion) is effective in
the management of encephalitis due to
varicella-zoster or vaccinia viruses.
VIRA-A is not effective against RNA
viral or adenoviral infections. It is also
not effective against bacterial or fungal
infections. There are no clinical data to
indicate efficacy against cytomegalovirus,
vaccinia virus, or smallpox virus.
Some degree of immunocompetence
must be present in order for VIRA-A to
achieve clinical response.
Please see following page for completeprescribing information, includingcontraindkations, warnings, precautions,and adverse reactions. �

LA.�ATO9.ESAC
.
are among the malignancies that have responded to Adriamycin
Among the other disseminated neoplastic conditions
that have responded to Adriamycin are Hodgkin’sdisease. breast carcinoma. acute lymphoblastic leukemia.
acute myeloblastic leukemia, Wilms’ tumor, bone andsoft tissue sarcomas, neuroblastoma, ovarian
carcinoma, transitional cell bladder carcinoma, thyroidcarcinoma, and bronchogenic lung carcinoma inwhich the small cell histologic type is the most responsive
compared to other cell types. Adriamycin shouldbe administered only under the direction of specialistsqualified in the administration of such drugs.
Severe local tissue necrosis will occur if there is
extravasation during administration.Severe irreversible myocardial toxicity with delayed
congestive failure often unresponsive to any cardiacsupportive therapy may be encountered as total dosageapproaches 550 mg/m2. This toxicity may occur atlower cumulative doses in patients with prior mediastinalirradiation or on concurrent cyclosphosphamide therapy.
The incidence of bone marrow depression is high.
Hematopoietic toxicity may limit dosage.In patients with impaired hepatic function, dosage
should be reduced.For information on the use OfADRIAMYCIN, call collect:(614) 764-8100.
(Photomicrographs courtesy of Dr. J.E. Ultrnann and Dr. R.S. Stein)
1 #{149} S TM
Auriamvcin(doxorubicin�hydroch1oride)for InjectionFOR INTRAVENOUS USE ONLY10 mg and 50 mg vials
For complete prescribing information, please see the following page.
Noduiar iymphoma - poorly differen-
tiated lymphocytic. The cells are
lymphocytes with marked nuclear
variations. Nuclei are round to oval.
and show indentation and
Diffuse lymphoma - histiocytic.
Larger cells than in poorly differen-
tiated type. Nuclei vary in size.
Prominent. large nucleoli are
present in some cells.
Although the cells are probably
transformed lymphocytes.
histiocytic lymphoma” remains
the standard terminology.
or eceivea f reec opyo ft her eview,N on-Hodgkin’sI �mphomas:A
B riefI ntroductiont oT heirE valuationa ndM anagement,fillo uta ndm ailt hisc oupont o:A
driaL aboratories.I nc.P
0.B ox1 6529.C olumbus.O hio4 3216A
tt:P .M cCarthy�
Dr.
Street Address
City State Zip

PARKE-DAVISPD-JA-2690-2-P (4-80)
Parenteral
�i1RkAMdaraL�nefor infusion)
A significant contribution to medicineFULL PRESCRIBING INFORMATION
Description. Vira-A for infusion (ara-A, vidarabine, adenine arabinoside) is a sterile anti-viral drug for intravenous administration only Vira-A (Vidarabine for Infusion) is a purinenucleoside obtained from fermentation cultures of Streptoinyces anbbiot;cus Each millili-ter of suspension contains 200 milligrams of vidarabine monohydrate equivalent to 1874milligrams of vidarabine. Each milliliter contains 0.1 milligram Phemerol� lbenzethoniumchloride) as a preservative: sodium phosphate, USP. 1 8 milligrams, and sodiumbiphosphate. USP, 4.8 milligrams. as buftering agents. Hydrochloric acid may have beenadded to adjust pH Vira-A is a white, crystalline solid with this empirical formulaCH3NsO3.H�O The molecular weight is 285.2: the solubility is 0.45 mgml at 25CC: andthe melting point ranges from 26O� to 270C. The chemical name is 9-j�-D-arabinofur-anosyladenine monohydrate, with the following structural formula.Clinical Pharmacology. Following intravenous admin-istration. Vira-A is rapidly deaminaled mb arabinosyl-hypoxanthine lAra-Hx). the principal metabolite. which NH2Is promptly distributed into the tissues. Peak Ara-Hxand Ara-A plasma levels ranging from 3 to 6 pg/mI and N.�0 2 to 0 4 �g/ml. respectively. are attained after slow in-travenous infusion of Vira-A doses of 10 mg/kg of body I Iweight. These levels reflect the rate of infusion and .s� Nshow no accumulation across time The mean half-life Nof Ara-Hx is 3 3 hours Ara-Hx penetrates into the cere-brospinal fluid (CSF) to give a CSF/plasma ratio of ap-proximately 13. HO-CH2 ‘H20
Excretion of Vira-A is principally via the kidneys.Urinary excretion is constant over 24 hours Forty-oneto 53’� of the daily dose is recovered in the urine as H OHAra-Hx with 1 to 3� appearing as the parent corn-pound. There is no evidence of fecal excretion of drug H Hor rnetabolites. In patients with impaired renal function OH HAra-Hx may accumulate in the plasma and reach levelsseveral-told higher than those described above.Microbiology. Wa-A possessesin vitro andin vivoantiviral activity against Herpesvirus simplex Herpes simplex viruxf types 1 and 2.
The antiviral mechanism of action has not yet been established. The drug ix converted intonucleofidex which appear to be involved with the inhibition of viral replication. In KB cells in-fected with Herpes simplex virus type 1 . Vira-A inhibits viral DNA synthesis. I/ira-A ix rapidlydeaminated to Ara-Hx. the principal metabolite, in cell cultures, laboratory animals, andhumans.
Ara-Hx also possessesin vitro antiviral activity but this activity ix significantly less than theactivity of Vira-A.Indications and Usage. Vira-A is indicated in the treatment of Herpes simplex virus en-cephalitis. Controlled studies indicate that Vira-A therapy will reduce the mortality caused byHerpes simplex virus encephalitis from 70 to 28� Vira-A therapy does not appear to altermorbidity and resulting serious neurological sequelae in the comatose patient. Therefore.early diagnosis and treatment are essential.
Herpes simplex virus encephalitis should be suspected in patients with a history of anacute febrile encephalopathy associated with disordered mentation, altered level of con-sciousness and focal cerebral signs
Studies which may support the suspected diagnosis include examination of cerebrospinalfluid and localization of an intra-cerebral lesion by brain scan, electroencephalography orcomputerized axial tomography (CAT)
Brain biopsy is required in order to confirm the etiological diagnosis by means of viral isola-ion in cell cultures
Detection of Herpes simplex virus in the biopsied brain tissue can also be reliably done byspecific fluorescent antibody techniques Detection of Herpes virus-like particles by electronmicroscopy or detection of intranuclear inclusions by histopathologic techniques only pro-vides a presumptive diagnosis
There are no reports available to indicate that Vira-A for infusion is effective in the manage-ment of encephalitis due to varicella-zoster or vaccinia viruses Vira-A us not effective againstinfections caused by adenovirus or RNA viruses It is also not effective against bacterial orfungal infections There are no data to support efficacy of Wa-A against cytomegalovirus.vaccinia virus, or smallpox virus.Contraindications. Wa-A is contraindicated in patients who develop hypersensitivity reac-tions to it
Warnings. Vira-A should not be administered by the intramuscular or subcutaneous routebecause of its low solubility and poor absorption.Precautions. Treatment should be discontinued in the patient with a brain biopsy negative forHerpes simplex virus in cell culture.
Special care should be exercised when administering \Iira-A to patients susceptible to fluidoverloading or cerebral edema. Examples are patients with CNS infections and impaired re-nal function
Patients with impaired renal function. such as post-operative renal transplant recipients.may have a slower rate of renal excretion of Ara-Hx Therefore. the dose of Vira-A may needto be adjusted according to the severity of impairment. These patients should be carefullymonilored
Patients with imoaired liver function should also be observed for possible adverse effectsAlthough clear evidence of adverse experience in humans from simultaneous Vira-A
and allopurinol administration has not been reported. laboratory studies indicate that al-lopurinol may interfere with Vira-A metabolism Therefore. caution is recommended whenadministering Vira-A to patients receiving allopurinol
Appropriate hematologic tests are recommended during �uira-A administration since he-moglobin. hematocrit. white blood cells. and platelets may be depressed during therapy
Some degree of immunocompetence must be present in order for Vira-A to achieve clinicalresponse
Usage in Pregnancy: Vira-A given parenterally is teratogenic in rats and rabbits. Doses of5 mg/kg or higher given intramuscularly to pregnant rabbits during organogenesis inducedfetal abnormalities Doses of 3 mg/kg or less did not induce teratogenic changes in pregnantrabbits. ‘(ira-A doses ranging from 30 to 250 mg/kg were given intramuscularly to pregnantrats during organogenesis. signs of maternal toxicity were induced at doses of 100 mg/kg orhigher and frank fetal anomalies were found at doses of 150 to 250 mg/kg
A safe dose for the human embryo or fetus has not been establishedConsequently. the use of Vira-A in pregnant patients should be limited to life-threatening
illnesses where the possible benefits outweigh the potential risks involvedIt is not known whether Vira-A is excreted in human milk As a general rule. nursing should
not be undertaken while a patient is under treatment since many drugs are excreted in hu-man milk However. Vira-A is rapidly deaminated in the gastrointestinal tractAdverse Reactions. The principal adverse reactions involve the gastrointestinal tract andare anorexia. nausea. vomiting, and diarrhea These reactions are mild to moderate. and sel-dom require termination of Vira-A therapy
CNS disturbances have been occasionally reported at therapeutic doses These aretremor. dizziness. hallucinations, confusion. psychosis. and ataxia
Hematologic clinical laboratory changes noted in controlled and uncontrolled studies werea decrease in hemoglobin or hematocrit, white blood cell count. and platelet count. SGOTelevations were also observed. Other changes occasionally observed were decreases inreticutocyte count and elevated total bilirubin.
Other symptoms which have been reported are weight loss. malaise. pruritus. rash, hema-ternesis. and pain at the intection site.Overdosage. Acute massive overdose of the intravenous form has been reported withoutany serious evidence of adverse effect. Acute water overloading would pose a greater threattothe patientthan Wa-A. due to its low solubility Doses of Vira-A over 20 mg/kg/day canproduce bone marrow depression with concomitant thrombocytopenia and leukopenia If amassive overdose of the intravenous form occurs. hematologic, liver. and renal functionsshould be carefully monitored
Acute massive oral ingestion is not expected to be toxic because drug absorption from thegastrointestinal tract is minimal. The oral LD5, for Vira-A is greater than 5.020 mg/kg in miceand rats.Dosageand Administration. CAUTION-THE CONTENTS OF THE VIAL MUST BEDILUTED IN AN APPROPRIATE INTRAVENOUS SOLUTION PRIOR TO ADMINISTRA-TION. RAPID OR BOLUS INJECTION MUST BE AVOIDED
Dosage. Herpes simplex virus encephalitis-15 mgi kg/day for 10 days.Method ofPreparation. Each vial contains 200 mg of Vira-A per ml of suspension. The
solubility of Vira-A in intravenous infusion fluids is limited Each one mg of Vira-A requires2.22 ml of intravenous infusion fluid for complete solubilization Therefore. each one liter ofintravenous infusion fluid will solubilize a maximum of 450 mg of Wa-A.
Any appropriate intravenous solution is suitable for use as a diluent EXCEPT biologic orcolloidal fluids (e.g . blood products. protein solutions. etc
Shake the Vira-A vial well to obtain a homogeneous suspension before measuring andtransferring.
Prepare the Vira-A solution for intravenous administration by aseptically transferring theproper dose of Vira-A into an appropriate intravenous infusion fluid. The intravenous infusionfluid used to prepare the Vira-A solution may be prewarmed to 35’ to 40’C (95#{176}to 100’F) tofacilitate solution of the drug following its transference Depending on the dose to be given,more than one liter of intravenous infusion fluid may be required. Thoroughly agitate the pre-pared admixture until completely clear Complete solubilization of the drug. as indicated by acompletely clear solution, is ascertained by careful visualinspection Final filtration with an in-line membrane filter (0.45 p pore size or smaller) is necessary
Once in solution. the drug has been found to be chemically stable at room temperature (be-low 86#{176}F(for at least two weeks. Dilution should be made just prior to administration andused at least within 48 hours. Subsequent agitation. shaking. or inversion of the bottle is un-necessary once the drug is completely in solution
Administration. Using aseptic technique. slowly infuse the total daily dose by intravenousinfusion IPrepared as discussed abovel at a constant rate over a 12. to 24-hour periodHow Supplied. N 0071-4150-08(Steri-Vial5 4150) Vira-A )Vidarabine for Infusion), a sterilesuspension containing 200 mg/mI. is supplied in 5-mi Steri’Vials. packages of 10Animal Pharmacology and Toxicity. Acute Toxicity: The intraperitoneal LD5( for Vira-Aranged from 3,890 to 4,500 mg/kg in mice, and from 2.239 to 2,512 mg/kg in rats, suggestinga low order of toxicity to a single parenteral dose Hepatic megalocytosis was observed inrats after single. intraperitoneal inlections at doses near and exceeding the LD50 value. Thehepatic megalocytosix appeared to regress completely over several months Acute intrave-nous LD50 values could not be obtained because of the limited solubility of Vira-A.
Subacute Toxicity. Rats. dogs. and monkeys have been given daily intramuscular injec-tions of Vira-A as a 20% suspension for 28 days. These animal species showed dose relateddecreases in hemoglobin. hematocrit. and lymphocytes Bone marrow depression was alsoobserved in monkeys. Except for localized, inlection-site injury and weight gain inhibition orloss. rats tolerated daily doses up to 150 mg/kg. and dogs tolerated daily doses up to 50 mg/kg Megalocytosix was not seen in the rats dosed by the intramuscular route for 28 days.Rhesus monkeys were particularly sensitive to Vira-A Daily intramuscular doses of 15 mg/kgwere tolerable. but doses of 25 mg/kg or higher induced progressively severe clinical signs ofCNS toxicity. Three monkeys given slow intravenous infusions of V’ira-A in solution at a doseof 15 mg/kg daily for 28 days had no significant adverse reactions.
Tumorigenicity. Chronic parenteral )IM) studies of vidarabine have been conducted inmice and rats.
In the mouse study, there was a statistically significant increase in liver tumor incidenceamong the vidarabine-treated females In the same study. some vidarabine-treated malemice developed kidney neoplasia. No renal tumors were found in the vehicle-treated controlmice or the vidarabine-treated female mice.
In the rat study. intestinal. testicular. and thyroid neoplasia occurred with greater frequencyamong the vidarabine-treated animals than in the vehicle-treated controls The increases inthyroid adenoma incidence in the high-dose (50 mg/kg) males and the low-dose (30 mg/kg)females were statistically significant
Hepatic megalocytosis. associated with vidarabirie treatment. has been found in short- andlong-term rodent (rat and mouse) studies It is not clear whether or not this represents apreneoplastic change
Mutagenicity. Results ofin vitro experiments indicate that vidarabine can be incorporatedinto mammalian DNA and can induce mutation in mammalian cells mouse L5178Y cell line).Thus farm vivo studies have not been as conclusive. but there is some evidence (dominantlethal assay in mice) that vidarabine may be capable of producing mutagenic effects in malegerm cells.
It has also been reported that vidarabine causes chromosome breaks and gaps whenadded to human leukocytesin vitro While the significance of these effects in terms of muta-genicity is not fully understood. there is a well-known correlation between the ability of van-ous agents to produce such effects and their ability to produce heritable genetic damage
YH
Reference: 1 Whitley RJ. Soong S-j Doiin R. et al. Adenine arabinoside therapy of biopsy-proved henpex’simplex encephalitis National Institute of Allergy and Infectious DiseasesCollaborative Antiviral Study. N EnglJ Med 297.289-294. August 11, 1977.
PARKE-DAVIS
Division of Warner-Lambert CompanyMorris Plains, NJ 07950

WARNINGS1. Severe local tissue necrosis will occur f there is extravasation during administration
Adriamycin must not be given by the intramuscular or subcutaneous route.
2. Serious irreversible myocardial toxicity with delayed congestive failure often unrespon-sive to any cardiac supportive therapy may be encountered as total dosage approaches550 mg/m’. This toxicity may occur at lower cumulative doses in patients with priormediastinal irradiation or on concurrent cyclophosphamide therapy
3. Dosage should be reduced in patients with impaired hepatic function
4. Severe myelosuppression may occur
5. Adriamycin should be administered only under the supervision of a physician who isexperienced in the use of cancer chemotherapeutic agents.
Adria LaboratorIes Inc.
ADRIAMYCIN “ (doxorubicin hydrochloride) for Injection
FOR INTRAVENOUS USE ONLY
DESCRIPTiONDoxorubicin is a cytofoxic anthracyctine antibiotic isolated from cultures of Seepiomyces peucelxJs
var. raestis It is supplied in the hydrochloride form as a freeze�dnied powder containing lactose.
CUNICAL PHARMACOLOGYThough not completely elucidated, the mechanism of action of doxorubscin is related to its ability
to bind to DNA and inhibit nucleic acid synthesis. Cell culture studies have demonstrated rapid cellpenetration and peninucleolar chromatin Landing. rapid inhibition of mitotic activity and nucleic acid
synthesis. mutagenesis and chromosomal aberrations. Animal studies have shown activity fl a
spectrum of experimental tumors, immunosuppression, carcinogenic properties in rodents, inductionof a variety of toxic effects. including delayed and progressive cardiac toxicity in rabbits. myelosup-pression in all species and atrophy to testes in rats and dogs.
Pharmacokinetic studies show the ntravenous administration of normal or radiolabeled Adnia-mycin (doxorubicin hydrochloride) for Injection is followed by rapid plasma clearance and significanttissue binding. Urinary excretion. as determined by fluorimetric methods. accounts for approxi-mafely 4-5% of the administered dose in five days. Biltary excretion represents the major excretion
route, 40-50% of the administered dose being recovered in the b,Ie or the feces in seven daysImpairment of liver function results in slower excretion. and. consequently. increased retention and
accumulation in plasma and tissues. Adriamycin does not cross the blood brain barrier
INDICATiONSAdniamycin has been used successfully to produce regression in disseminated neoplasfic condi-
tions such as acute lymphoblaslic leukemia, acute myeloblastic leukemia. Wilms’ tumor. neuroblas-toma. soft tissue and bone sarcomas. breast carcinoma. ovarian carcinoma. transitional cell bladdercarcinoma, thyroid carcinoma. tymphomas of both Hodgkin and non-Hodgkin types and bronchogeniccarcinoma in which the small cell histologic type is the most responsive compared to other celltypes. A number of other solid tumors have also shown some responsiveness but in numbers toolimited to iustifv specific recommendation. Studies to date have shown malignant melanoma. kidneycarcinoma. large bowel carcinoma. brain tumors and mefastases to the central nervous system notto be significantly responsive to Adriamycin therapy.
CONTRAINDICAT1ONSAdniamycin therapy should not be started in patients who have marked myelosuppression induced
by previous treatment with other antitumor agents or by radiotherapy. Conclusive data are notavailable on pre-existing heart disease as a co-factor of increased risk of Adriamycin inducedcardiac toxicity. Preliminary data suggest fhat in such cases cardiac toxicity may occis at doseslower than the recommended cumulative limit It is therefore not recommended to start AdniamycinIn such cases Adniarnycin treatment is contraindicated in patients who received previous treatmentwith complete cumulative doses of Adriamycin and/or daunorubicin.
WARNINGSSpecial attention must be given to the cardiac toxicity exhibited by Adriamycin. Although
uncommon, acute left ventricular failure has occurred. particularly in patients who have receivedtotal dosage of the drug exceeding the currently recommended limit of 550 mg/m’ This limitappeans to be lower (400 mg/rn’) in patients who received radiotherapy to the mediaslinal area orconcomitant therapy with other potentially cardiotoxic agents such as cyclophosphamide The totaldose of Adniamycin administered to the individual patient should also take into account a previous orconcomitant therapy with related compounds such as daunorubicin. Congestive heart failure and/orcardiomyopathy may be encountered several weeks after discontinuation of Adriamycin therapy
Cardiac failure is often not favorably affected by presentty known medical or physical therapy forcardiac support. Early clinical diagnosis of drug induced heart failure appears to be essential for
successful treatment with digitalis. diuretics. low salt diet and bed rest. Severe cardiac toxicity mayoccur precipitously without antecedent EKG changes. A baseline EKG and EKGs performed prior toeach dose or course after 300 mg/rn’ cumulative dose has been given is suggested Transient EKGchanges consisting of T�wave flattening, S-T depression and ai-rhythmias lasting for up to two weeksafter a dose or course of Adriamycin are presently not considered indications for suspension ofAdniamycin therapy. Adriamycin cardiomyopathy has been reported to be associated with a per-sistent reduction in the voltage of the CR5 wave, a prolongation of the systolic time interval and areduction of the ejection fraction as determined by echocardiography or radionuclide angiography.None of these tests have yet been confirmed to consistently identify those individual patients thatare approaching their maximally tolerated cumulative dose of Adria’nycin. If test results indicatechange in cardiac function associated with Adriamycin the benefit of continued therapy must becarefully evaluated against the risk of producing irreversible cardiac damage.
Acute life-threatening arrhythmias have been reported to occur during or within a few hours afterAdriamycin administration.
There is a high incidence of bone marrow depression. primarily of leukocytes, requiring carefulhematologic monitoring. With the recommended dosage schedule, leukopenia is usually transient.reaching its nadir at 10-14 days after treatment with recovery usually occurring by the 21st day.White blood cell counts as low as 1000/mm’ are to be expected during treatment with appropriatedoses of Adniamycin. Red blood cell and platelet levels should also be monitored since they may alsobe depressed Hematologie toxicity may require dose reduction or suspension or delay of Adniamycintherapy Persistent severe myelosuppression may result in superintection or hemorrhage.
Adniamycin may potentiate the toxicity of other anticancer therapies. Exacerbation of cyclophos-phamide induced hemorrhagic cystitis and enhancement of the hepatotoxicity of 6-mercaptopurinehave been reported. Radiation induced toxicity to the myocardium. mucosae. skin and liver havebeen reported to be increased by the administration of Adriamycin.
Toxicity to recommended doses of Adrianycin is enhanced by hepatic impairment: therefore. priorto the individual dosing, evaluation of hepatic function is recommended using conventional clinicallaboratory tests such as SGOT. SGPT. alkaline phosphatase and bilirubin (See Dosage and Adminis.tration)
On intravenous administration of Adniamycin extravasation may occur with or without an
accompanying stinging or burning sensation and even if blood returns well on aspiration of theinfusion needle. It any signs or symptoms of extravasation have occurred the injection or infusionshould be immediately terminated and restarted in another vein.
Adriamycin and retated compounds have also been shown to have mutagenic and carcinogenicproperties when tested in experimental models.
� use of Adriamycin in pregnancy has not been established. AdniamycinIs embryotoxic and teratogenic in rats and embryotoxic and abortifacient in rabbits. Therefore. the
benefits to the pregnant patient should be carefully weighed against the potential toxicity to fetusand embryo. The possible adverse effects on fertility in males and females in humans or expenimen-fal animals have not been adequately evaluated.
PRECAUTIONSInitial treatment with Adrialtycin requires close observation of the patient and extensive labora-
lory monitoring. It is recommended, therefore. that patients be hospitalized at least during the firstphase of the treatment.
Like other cytotoxic drugs, Mriarnycin may induce hyperuricemia secondary to rapid lysis ofneoplastic cells The clinician should monitor the patients blood uric acid level and be prepared touse such supportive and pharmacologic measures as might be necessary to control this problem
Adriamycin imparts a red coloration to the urine for 1-2 days after administration and patientsshould be advised to expect this during active therapy.
Adriamycin is not an anti-microbial agent.
ADVERSE REACTiONSDose limiting toxicities of therapy are myelosuppression and cardiotoxicity (see Warnings( Other
reactions reported are:Cutaneous-Reversible complete alopecia occurs in most cases. Hyperpigmentation of nailbeds
and dermal creases. primarily in children, have been reported in a few cases. Recall of skin reactiondue to prior radiotherapy has occurred with Adriamycin administration.
Gastrointestinal-Acute naisea and vomiting occurs frequently and may be severe This may bealleviated by antiemetic therapy. Mucositis (stomatitis and esophagitis) may occur 5-10 days afteradministration. The effect may be severe leading to ulceration and represent a site of origin forsevere infections. The dose regimen consisting of administration of Adriamycin on three successivedays results in the greater incidence and severity of mucositis. Anorexia and diarrhea have beenoccasionally reported.
Vascular-Phlebosclerosis has been reported especially when small veins are used or a singlevein is used for repeated administration. Facial flushing may occur if the injection is given toorapidly
!�Q.�A! - Severe cellulitis, vesication and tissue necrosis will occur if Adriamycin is extravasatedduring administration. Erythematous streaking along the vein proximal to the site of the injection hasbeen reported. (See Dosage and Administration.)
Hypersensitivity - Fever, chills � urticaria have been reported occasionally Anaphylaxis mayoccur A case of apparent cross sensitivity to lincomycin has been reported.
Qiti�.t - Conjunctivitis and lacrimation occur rarely.
DOSAGE AND ADMINiSTRATIONCare in the administration of Adriamycin will reduce the chance of perivenous infiltration It may
also decrease the chance of local reactions such as urticaria and erythentatous streaking.The recommended dosage schedule is 60�75 mg/rn’ as a single intravenous injection adminis-
fered at 21�day intervals. The lower dose should be given to patients with madequate marrowreserves due to old age. or prior therapy. or neoplastic marrow infiltration. An alternative doseschedule is 30 mg/rn’ on each of three successive days repeated every 4 weeks. Adriamycin dosagemust be reduced if the bilirubin is elevated as follows: Serum Bilirubin 1.2-3.0 mg/lOU mi-give /�
normal dose, > 3 mg/tOO mI-give ‘/4 normal dose.Preparation of Solution: Adriamycin � rog vials and 50 mg vials should be reconstituted with 5 ml
and 25 ml respectively of Sodium Chloride injection U.S.P. or Sterile Water for injection U.S.P. to givea final concentration of 2 m9/mI of doxorubicin hydrochloride. An appropriate volume of air shouldbe withdrawn from the vial during reconstitution to avoid excessive pressure build-up. Bactenio-static diluents are not recommended.
Skin reactions associated with Adriamycin have been reported. Caution in the handling andpreparation of the powder add solution must be exercised and the use of gloves is recommended. IfAdniamycin powder or solution contacts the skin or mucosae. immediately wash thoroughly with
soap and water.After adding the diluent, the vial should be shaken and the contents allowed to dissolve. The
reconstituted solution is stable for 24 hours at room temperature and 48 hours under refrigeration(4�1O�C). It should be protected from exposure to sunlight and any unused solution should bediscarded.
It is recommended that Adriamycin be slowly administered into the tubing of a freely runningintravenous infusion of Sodium Chloride Injection U.S.P. or 5% Dextrose Injection U.S.P. The tubingshould be attached to a Butterfly needle inserted preferably into a large vein. It possible. avoid veinsin extremities with compromised venous or lymphatic drainage. The rate of administration isdependent on the size of the vein and the dosage. However the dose should be administered in notless than 3 to 5 minutes. Local erythematous streaking along the vein as well as facial flushing maybe indicative of too rapid an administration. A horning or stinging sensation may be indicative ofperivenous infiltration and the infusion should be immediately terminated and restarted in another
vein. Perivenous infiltration may occur painlessly. If it is known or suspected that subcutaneousextravasation has occurred local infiltration with an injectable corticosteroid and flooding the sitewith normal saline has been reported to lessen the local reaction. The area should subsequently befrequently examined and plastic surgery consuftation should be obtained. If ulceration begins, earlywide excision of the involved area should be considered
Adniamycin should not be mixed with heparin or 5-fluorouracil since it has been reported thatthese drugs are incompatible to the extent that a precipitate may form. Until specific compafibilitydata are available. it is not recommended that Adriamycin be mixed with other drugs.
Adriamycin has been used in combination with other approved chemotherapeutic agents. Thoughevidence is available that at least in some types of neoplastic disease combination chemotherapy issuperior to single agents. the benefits and risks of such therapy have not yet been fully elucidated
HOW SUPPLIEDADRIAMYCIN “ (doxorubicin hydrochloride) for Injection is available in two sizes:10 mg-Each vial contains 10 mg of doxorubscin HCI and 50 mg of lactose U.S.P as a sterile
red-orange Iyo#{216}tilizedpowder. Packaged and supplied in 1O�vial cartons NDC 38242-874�1O50 mg-Each vial contains 50 mg of doxorubicin HCI and 250 mg of lactose U.S.P. as a sterile
red-orange lyophilized powder. Packaged and supplied in a single vial cartonNDC 38242-875-50.
‘Rudolph. R. et al: Skin Ulcers Due to Adriwnycin. Cancer 38:1087-1094. Sept.. 1976.
8740102-1/80
�.�r:I�n � Distributed by Adria Laboratories Inc., Columbus. Ohio 43215._______________Manufactured by: Farmitalia Carlo Erba SpA.. Italy.
LA�ATO9ESAC
R.vis.d January 1980

NOWAVAILABLE FROMIVES LABORATORIES
VIALS, containing 20 mg daunorubicin equivalent
ID(DAUNORUBICINHCI) for injection
FOR REMISSION INDUCTION IN ACUTENONLYMPHOCYTIC LEUKEMIA (MYELOGENOUS,
MONOCYTIC, ERYTHROID) IN ADULTS
in 1980 ives Labo�aio�’es inc

*adapfurj from Wiernik and SerpickFor Brief Summary, please seefollowing page.
Ceru bidi ne#{174}daunorubicin HCI),
a salt of an anthracyclinecytotoxic antibiotic, has beenunder clinical investigationsince 1965In the past 12 years, the Cancer and LeukemiaGroup B (CALGB) has treated 2,500 patientswith acute nonlymphocytic leukemia (ANLL)�using Cerubidine alone or in combinationwith other agents. In these and other exten-siVe studies2-� it has emerged as the singlemost effective agent in the treatment of ANLL’and is in part responsibleforthe improve-ments in complete remission rate and sur-vival time that have been achieved in patientswith ANLL�
Complete remission ratesof 40% to 50% when used as asingle agentThe table below compares the response totherapy with daunorubicin alone to that of acombination of prednisone, vincristine,6-mercaptopurine, and methotrexate (POMP).With daunorubicin a complete remissionrate of 50% was achieved in a median of 19days; with POMP, the complete remission ratewas 28% and took a median of 64 days. Add i-tionally, the median survival of responders todaunorubicin therapy was greater than thatof nonresponders.3
Complete remission ratesof 53% to 65% when combinedwith cytosine arabinosideIn one study, the CALGB achieved an overallcomplete remission rate of 53% in 208 pa-tients with ANLL-57% in patients less than60 years of age-usingthe “7 and 3” induc-tion regimen of seven consecutive days ofcytosine arabinoside and three consecutivedays of Cerubidine� With the same inductionregimen the Baltimore Cancer ResearchCenter achieved a complete remission rateof 63% in 30 patients and concluded thatthis combination “� . . achieves remissionmore rapidly and effectively than anywe pre-viously studied�’4The UCLA Acute LeukemiaStudy Group, using high-dose, sequential,seven-day courses of cytosine arabinoside,thioguanine, and cerubidine, achieved acomplete remission rate of 79%�
Should be administeredonly by physicianswith experience inleukemia chemotherapySevere myelosuppression occurs at thera-peutic doses. Contraindicated in patientswith preexistingdrug-induced bone marrowsuppression unless the benefit warrants therisk. Preexisting heart disease and previoustherapy with doxorubicin are cofactors ofincreased risk of daunorubicin-inducedcardiac toxicity, and the benefit to riskratio should be weighed before startingdaunorubici n.

CERUBIDINE#{174}(DAUNORUBICIN HCI) for injection
for remission induction in acute nonlymphocytic leukemia (myelogenous, monocytic, erythroid) in adults
WARNINGS1 . Cerubidine must be given into a rapidly flowing intravenous in-fusion. It must never be given by the intramuscular or subcuta-neous route. Severe local tissue necrosis will occur if there isextravasation during administration.2. Myocardial toxicity manifested in its most severe form by p0-tentially fatal congestive heart failure may be encountered whentotal cumulative dosage exceeds 550 mg/m2. This may occur ei-ther during therapy or several months after termination of therapy.Treatment with digitalis, diuretics, sodium restriction and bed restis indicated.3. Severe myelosuppression occurs when used in therapeuticdoses.4. It is recommended that Cerubidine be administered only byphysicians who are experienced in leukemia chemotherapy andin facilities with laboratory and supportive resources adequate tomonitor drug tolerance and protect and maintain a patient com-promised by drug toxicity. The physician and institution must becapable of responding rapidly and completely to severe hemor-rhagic conditions, and/or overwhelming infection.5. Dosage should be reduced in patients with impaired hepatic orrenal functton.
Warnings: Therapy should not be started in patients with preexistingdrug-induced bone marrow suppression unless the benefit warrantsthe risk. Preexisting heart disease and previous therapy with doxoru-bicin increase the risk of Cerubidine-induced cardiac toxicity; thebenefit to risk ratio should be weighed before starting Cerubidine insuch patients.
Bone Marrow-Cerubidine is a potent bone marrow suppressant.Suppression will occur in all patients given a therapeutic dose of thisdrug.
Cardiac Effects-At total cumulative doses less than 550 mg/m2,acute congestive heart failure is seldom encountered, but rare in-stances of pericarditis-myocarditis, not dose-related, have been re-ported; at cumulative doses exceeding 550 mg/m2, the incidence ofdrug-induced congestive heart failure increases. This limit appearslower, 400 mg/m2, in patients who received radiation therapy that en-compassed the heart; the total dose administered should also takeinto account any previous or concomitant therapy with other poten-tially cardiotoxic agents or related compounds such as doxorubicin.Although there is no reliable method for predicting acute congestiveheart failure, certain changes in the electrocardiogram and a de-crease in the systolic ejection fraction from pretreatment baselinemay help to recognize those patients at greatest risk; a decreaseequal to or greater than 30% in limb lead ORS voltage has been as-sociated with a significant risk of drug-induced cardiomyopathy. Anelectrocardiogram and/or determination of systolic ejection fractionshould be performed before each course of Cerubidine; if one ofthese predictive parameters occurs, the benefit of continued therapymust be weighed against the risk of producing cardiac damage. Earlyclinical diagnosis of drug-induced congestive heart failure appears tobe essential for successful treatment with digitalis, diuretics, sodiumrestriction, and bed rest.
Evaluation of Hepatic and Renal Function-Since significant hepaticor renal impairment can enhance the toxicity of the recommendeddoses of Cerubidine, hepatic and renal functions should be evalu-ated with conventional clinical laboratory tests prior to administration.
Pregnancy-Cerubidine can cause fetal harm when administered to
a pregnant woman; patients using this drug during pregnancy, or whobecome pregnant while taking this drug, should be apprised of thepotential hazard to the fetus.
Extravasation atlnjection Site-Extravasation of Cerubidine at thesite of intravenous administration can cause severe local tissuenecrosis.
Precautions: Therapy with Cerubidine requires close observationof the patient and extensive chemical and laboratory monitoring.Hyperuricemia secondary to rapid lysis of leukemic cells may beinduced; blood uric acid levels should be monitored and appropriatetherapy initiated if hyperuricemia develops. Appropriate measuresmust be taken to control any systemic infection before beginningtherapy with Cerubidine. Therapy with Cerubidine may transientlyimpart a red coloration to the urine , and patients should be advisedto expect this.
Pregnancy Category D: See Warnings Section.
Adverse Reactions : Dose-limiting toxicity includes myelosuppres-sion and cardiotoxicity (see Warnings). Other reactions include: Cu-taneous-Reversible alopecia in most patients. Gastrointestinal-Acute nausea and vomiting, usually mild, and antiemetic therapymay be of some help; mucositis, three to seven days after adminis-tration; diarrhea. Local- If extravasation occurs during administra-tion, tissue necrosis can result atthe site. Acute Reactions-Fever,chills, skin rash.
Consult direction circular before prescribing.
References1 . Data on file, Ives Laboratories.2. Freireich EJ, Keating MJ, Gehan EA, et al: Therapy of acute mye-logenous leukemia. Cancer 42 (August suppl): 874-882, 1978.3, Wiernik PH, Serpick AA: A randomized clinical trial of daunorubi-cm and a combination of prednisone, vincristine, 6-mercaptopurine,and methotrexate in adult acute nonlymphocytic leukemia. CancerRes 32:2023-2026, 1972.4. Chang P. Wiernik PH, Lichtenfeld JL, Schiffer CA: Levamisole (L),cytosine arabinoside (Ara-C), and daunorubicin (DNR) inductiontherapy of adult acute nonlymphocytic leukemia (ANLL), abstracted(C-254). Proc AACR ASCO 19:370, 1978.5. Gale RP, Cline MJ: High remission-induction rate in acute myeloidleukaemia. Lancet 1:497-499, 1977.
IVES LABORATORIES INC.New York, NY 10017DEDICATED TOIMPROVING THE QUALITY OF LIFE THROUGH MEDICINE’

BLOOD-THE JOURNAL OF THE ASH xxi
ADJUVANTRAPYOF
CANCER HEdited by STEPHEN E. JONES, M.D.
and SYDNEY E. SALMON, M.D.
Among the important developments pre-
sented ar the favorable results in adju-
vant chemotherapy in early breast cancer
which were clearly confirmed by many stud-
ies and suggest efficacy in postmenopausal
as well as premenopausal women. Other
papers reflect the progress made and the
ongoing work in the areas of; hematologic
malignancies, genitourinary tumors, osteo-
sarcoma, childhood tumors, head and neck,
thyroid, and brain tumors, ovarian cancer,
melanoma and soft tissue sarcoma, lung
cancer, and gastrointestinal tumors. This
volume comprises the edited proceedings
of the Second International Conference on
the Adjuvant Therapy of Cancer, held in
March 1979.1979, 624 pp., ISBN.’ 0-8089-1213-5
GS 0074
GRUNE & STRATTONA Subsidiary of llarcoiirt Briar-c’ Jot’anoticli, Pi,bljsI,r’,-.�
I I I FIFTH AVENUE, NEW YORK, N.Y. 1000324-28 OVAL ROAD, LONDON NWI 7DX

.‘
Inte ronEditor-in-Chief: ION GRESSER
Board of Editors: KARl CANTELL,EDWARD DeMAEYER, MAURICE LANDY,
MICHEL REVEL, and JAN VILCEKVolume 1,
CONTENTS: K. Cantell, WHY IS INTERFERON NOT
IN CLINICAL USE TODAY? Introduction. How do
you make Large Quantities of Human Interferon?Purification and Safety. Pharmacokinetics andTreatment Schedules. Accumulating Clinical Data.How can Interferon be used Most Effectively? Whyis Interferon not in Clinical Use Today? Will Inter-
feron be in Clinical Use Tomorrow? W. E. StewartII, VARIED BIOLOGIC EFFECTS OF INTERFERON.
Introductory and Historical Aspects. Some of theThings Interferon Can do. Defining Interferon. R. M.
Friedman, INTERFERONS: INTERACTIONS WITH
CELL SURFACES. Introduction. The Cell Surfacein the Establishment of Antiviral State. Alterationsin the Plasma Membrane as a Consequence of In-terferon Binding. Discussion. E. De Maeyer and
J. Do Maeyer-Guignard, CONSIDERATIONS ON
MOUSE GENES INFLUENCING INTERFERON PRO-
DUCTION AND ACTION. Introduction. What are theIf Loci? In Depth Study of If-i. Evidence for GenesInfluencing the Interaction of Interferon and the
Immune System. Scope for Future Research. M.
Revel, MOLECULAR MECHANISMS INVOLVED INTHE ANTIVIRAL EFFECTS OF INTERFERON. Stud-
ies of the Antiviral Effect of Interferon in Intact
Cells: the SV4O System. Studies in Cell-free Sys-tems: Interferon-Induced Translation Regulation.
The Interferon Receptor and Early Events in Inter-
feron’s Action.
References appear at the end of each chapter.1980, 176 pp., $23.00
ISBN: 0-12-302250-9
Send payment with order and save postage and handlingcharge.
Prices are subject to change without notice.
ACADEMIC PRESS, INC.A Subsidiary of Harcourt Brace Jovanovich, Publishers
111 FIFTH AVENUE, NEW YORK, N.Y. 1000324-28 OVAL ROAD, LONDON NW1 7DX
GS 0100
.4



for automatic friarvesting of specificcomponents ina continuous flow
sealless systemThe CS-3000TM Blood Cell Separator represents asignificant advance in blood processing. It allowsautomatic collection of blood components fortherapeutic or research purposes.
A built-in microcomputer controls each operationas well as provides continuous monitoring ofinstrument safety alarms and automaticadjustment of blood pumps and centrifuge tomaximize the efficiency of component collection.
Designed to protect both donor and patientR Continuous flow, closed system without rotating sealsreduces the threat of contamination or leaks duringblood processing.$ Programmed automatic instrument shutdown underabnormal operating conditions further assuresdonor/patient safety.
. Low extracorporeal volume reduces risk of problems
associated with donor hypovolemia.
Designed to improve operator convenienceand efficiencyU Automated collection procedures assure highcomponent yields while minimizing operator time.
. Simple to set up and operate.
. Mobile unit may be used in donor room or atpatient’s bedside.

(� Copyright 1980 Traveno� Laboratories. Inc All rights reserved
New from Fenwal Laboratories“.1
BLOOD CELLSEPARATOR
For fully automatic, high yield harvestingof blood components
1 The ready-to-use.disposable
Apheresis KIt fIts easilyinto the CS-30001MSeparator. Themonitor assemblyshown here containsseveral safety andalarm monitorIngsystems.
4 During theprocedure. the
monitor assembly andmicrocomputercontinuously check forabnormal conditions.
2 The collection andseparation
containers, which arepart of the ApheresisKit, are placed in theirrespective holders. Thesystem is automaticallyprimed and the properfunction of variousmonitors and alarmsystems is verified priorto each procedure.
5 The continuous flowseparation
procedure is relativelyrapid. As an example,the time required toharvest a therapeuticdose of plateletsranges from 90 to 120minutes
1) Blood processing is�J activated by thepress of a button. Eachcollection procedure iscarried out undermicrocomputer control.A manual mode ofoperation is availablewhen desired.
6 At the completion ofthe procedure, the
collection container isremoved from theApheresis Kit. Thecollected componentmay then be stored oradministered to therecipient directly fromthe collection container.
Brief StatementThere are no known contraindications for use of the �S�3OOO’� Blood Cell Separator to har�
vest blood components Platelets should not be harvested for subsequent transfusion if the
donor has recently ingested aspirin or other drugs known to adversely affect platelet functionApheresis procedures in other than normal healthy donors should be undertaken only
under supervision of a qualified physician who has evaluated each patient and prescribedthat use of the instrument is necessary:�: FENWAL LABORATORIES
]�, DlVI�ON OFTRAVENOL LABORATORIES, INC.DEERFIELD. ILLINOIS. USA 60015

CELLULAR and
MOLECULAR REGULATIONof HEMOGLOBIN SWITCHING
Edited byG. STAMATOYANNOPOLOUS, M.D.
and ARTHUR W. NIENHUIS, M.D.
Based on the proceedings of a conference heldon Hemoglobin S�t’itc’1ziiig in Seattle, June 1978
SECTIONS: DEVELOPMENTAL HEMO-
GLOBINS IN MAN AND ANIMAL MOD-
ELS. Human Fetal Hemoglobin. Physiology of
Hemoglobin Switching. Hemoglobins in Early
Development. HEMOGLOBIN SWITCHING
AND ERYTHROID CELL DIFFERENTIA-
TION. Regulation of Erythropoiesis. Hemo-
globin Switching in Culture. Commitment and
Biochemical Differentiation of Erythroid Cells.
MOLECULAR BIOLOGY OF HEMOGLO-
BIN SWITCHING. Organization of Globin
Genes. Globin mRNA Structure. Metabolism
of Globin mRNA. Control of Globin Gene
Expression./979, 797 pp.. I.SBN 0-8089-0611-7
GRUNE & STRATTONA .‘ri,b.siilia,� of IIa,uoiirt 1lI.(l(�(’ JOI1l�1OI’i(ll , Piibli.sIie,’.s
111 FIFTH AVENUE. NEWYORK. N.Y. 10003
24-28 OVAL ROAD. LONDON NWI 71)X
GS 0041



xxx BLOOD-THE JOURNAL OF THE ASH
PROGRESS IN HEMO STASISAND THROMBOSIS
VOLUME 4
Edited by THEODORE H. SPAET, M.D.
Volume 4 presents the first intensive discussion ofa rational approach to gastrointestinal bleedingand its management, an examination of variousfunctions of platelet contractile proteins not hith-erto characterized systematically, and an explana-tion of how membrane properties influence plateletfunction. Other highlights are thorough discussionsof the role of prostaglandins in platelet functionand of transport through endothelial cells.
CONTENTS: M. Frojmovic, Rheo-optical Studiesof Platelet Structure and Function. G. D. Wilner,The Molecular Basis for Measurement of Circu-lating Fibrinogen Derivatives. S. I. Shattil andR. A . Cooper, The Role of Membrane Lipid Corn-position, Organization, and Fluidity in HumanPlatelet Function. A . P. Kaplan, Initiation of theIntrinsic Coagulation and Fibrinolytic Pathwaysof Man: The Role of Surfaces, Hageman Factor,Prekallikrein, High Molecular Weight Kininogen,and Factor XI. I. M. Gerrard and J. G. White,Prostaglandins and Thromboxanes:” Middle Men”Modulating Platelet Function in Hemostasis andThrombosis. H. Chien, Transport Across ArterialEndothelium. D. A. Gilbert et al., The Nonsurg-ical Management of Acute Nonvariceal UpperGastrointestinal Bleeding. R. I. Friedman andE. R. Burns, The Role of Platelets in the Prolif-erative Response of the Injured Artery. L. Harker,Platelet Survival. T. Pollard and R. F. Adeistein,Platelet Contractile Proteins. S. F. Shapiro, Pro-thrombin.
1978, 432 pp., iSBN: 0-8089-1096-5
GS 0076
GRUNE & STRATTONA Subsidiary of Harcourt Brace Jovanovich, Publishers
I I1 FIFTH AVENUE, NEW YORK, N.Y. 1000324-28 OVAL ROAD, LONDON NW! 7DX

Immuneul rs
Tran r FactorEdited by AMANULLAH KHAN, CHARLES H. KIRKPATRICK and N. 0. HILL
The Third International Symposium on Transfer Factor, held onOctober 12-14, 1978, at Wadley Institute of Molecular Medicine,Dallas, Texas.
Serving as a forum for investigators interested in transfer factor topresent and discuss their work, the meeting consisted of full lengthpresentations and a poster session. Ample time was provided fordiscussion following each paper and general discussion at the end ofeach session. The papers submitted for the meeting, the postersessions, and the discussions are included in this volume.
Transfer factor, a dialyzable component of Ieukocyte lysates, hasbeen shown to affect cellular immunity in many in vivo and in vitrotests. This substance has proven useful in immunodeficiencydiseases, viral illnesses, fungal and parasitic diseases. There arealso reports of its usefulness in malignant diseases. The spectrum ofclinical trials ranges from phase I studies to randomized controlledtrials. This volume by leading researchers presents the state of theart in testing for transfer factor and its various components,preparation, purification, and characterization of the molecules,animal models for testing transfer factor activity, and clinicalinvestigations.1979, 750 pp. ISBN: 0-12-406060-9
AP 7854
Academic Press, Inc.A Subsidiary of Harcourt Brace Jovanovich, Publishers
1 1 1 FIFTH AVENUE, NEW YORK, N.Y. 1000324-28 OVAL ROAD, LONDON NW1 7DX

THE JOURNAL SPACE SAVER!
Now, yourjournals can become an attractive, permanent part of
your, professional library. These famous Jesse Jones volume files,
especially designed to keep your copies ofGrune and Stratton journals
orderly, readily accessible for future reference-guard against soiling,
tearing, wear or misplacement of copies.
Each library case is designed in simulated leather with its spine
embossed in 16-k gold lettering with the title ofthejournal and a gold
transfer so you can record the volume and year.
Reasonably priced, too. Only $4.95 each, 3 for $14.00, 6 for $24.00.
Satisfaction unconditionally guaranteed or money refunded. Only
U.S. orders accepted.
To: Jesse Jones Box Corp.
P.O. Box 5120Dept. GS
Philadelphia, Penns�’1vania 1914 1
Please send me _______________________G&S Library Cases at $Journal(s)
cime
(Please Print)
Address
(;it�’__________________________________ State ZipNote: Allow 3 weeks for delivery

BLOOD-THE JOURNAL OF THE ASH xxxiii
(Continued on following page)
INFORMATION FOR CONTRIBUTORS
SUBMITTING THE MANUSCRIPT
BLOOD, The Journal of the American Society of Hematology,
provides an international forum for the publication of original
articles, in English, describing basic laboratory and clinical inves-
tigations encompassed in the broad discipline of hematology.
The scope of the journal covers all aspects of hematology,
including disorders of leukocytes, both benign and malignant,
erythrocytes, platelets, hemostatic mechanisms, and immunolo-
gy, as well as major developments in clinical laboratory diagnosis
and blood banking.
Manuscripts are accepted for consideration on the condition
that they are contributed solely to BLOOD. No substantial part of
a paper may have been or may be published elsewhere, except
for an abstract of 500 words or less. Manuscripts will be
critically reviewed by the Editor or an Associate Editor with
appropriate independent referees drawn from the Editorial Board
and other experts. Authors may recommend appropriate review-
ers or may indicate individuals they wish excluded from the
review process. Insofar as possible the Editor and Associate
Editors will incorporate these suggestions in the review process.
Acceptance of papers for publication is based upon the originality
of the observation or investigation, the quality of the work
described, and the clarity of the presentation. Papers will ordi-
narily be published in the order in which they are finally accepted
for publication and not in the order of submission.
Acknowledgments to other investigators for advice, assist-
ance, and data must be substantiated by written authorization to
the Editor-in-Chief specifically granting permission to the authors
for such citations.
Concise Reports: BLOOD will consider for rapid editorial
review and decision concise reports of original investigations of
scientific importance within the broad discipline of hematology in
order to speed up the publication process for accepted manu-
scripts that meet the criteria for Concise Reports. Such manu-
scripts must represent original and definitive studies and include
adequate description of experimental methods, documentation
of findings, and references to the literature. The Editors will
provide decisions on such manuscripts within three weeks of
receipt at the BLOOD Office. These decisions will not be
accompanied by detailed reviewers’ comments such as are
returned with manuscripts handled in the ordinary manner.
Papers deemed not suitable for rapid publication as Concise
Reports may be resubmitted for consideration as regular manu-
scripts. Request for consideration as a Concise Report should be
made in the author’s covering letter upon submission. Concise
Reports cannot exceed 1 0 typed pages, including tables,
figures, and references (count 2 graphs or 1 photomicrograph as
a typed page). Authors must accept the responsibility of
conforming to the instructions in ‘ ‘Information for Contribu-
tors. �‘
Letters to the Editor: Letters to the Editor are welcomed
and will be published if appropriate. They should be typewritten,
double spaced, and generally, should not be more than two
typewritten pages in length.
Editorials, Brief Reviews: Editorials and Brief Reviews may
be solicited by the Editors, and may be submitted for considera-
tion without solicitation. These manuscripts must be prepared in
a manner appropriate for any other papers and will be reviewed
as are original articles submitted for consideration.
Articles, editorials, letters to the editor, and other text mate-
rial in BLOOD represent the opinions of the authors and do not
reflect the opinions of the American Society of Hematology, the
publisher, or the institution with which the author is affiliated,unless the contrary is clearly specified.
In order to comply with the requirements of the insurance
carrier, authors of accepted manuscripts and letters will be
requested to provide the following signed statement: ‘ ‘The
writer/author represents and warrants that his/her part of the
work as submitted will in no way violate any copyright, or any
other right, and will contain nothing libelous or otherwise
unlawful.”
Submit papers, with a $50.00 check, money order, or
institutional purchase order to cover the cost of manuscript
handling, to:
Dr. Paul A. Marks, Editor
BLOOD
Columbia University College of Physicians
and Surgeons
701 West 168 Street
NewYork, N.Y. 10032
Receipt of a manuscript will be acknowledged by a card
bearing the name and address of the Editor or Associate Editor
who is assigned responsibility for the review process. All further
correspondence concerning the manuscript should be addressed
to the responsible Editor or Associate Editor.
Papers reporting human experimentation will be reviewed in
accordance with the precepts established by the Helsinki Decla-
ration. Copies of this declaration may be obtained by writing to
the American Medical Association, 535 North Dearborn Street,
Chicago, Ill. 606 10. Such papers must include a statement that
the human investigations were performed after approval by a
local Human Investigations Committee and in accord with an
assurance filed with and approved by the Department of Health,
Education, and Welfare where appropriate.
All manuscripts dealing with recombinant DNA research must
include a description of the physical and biologic containment
procedures practiced to aid and forewarn others who might
consider repeating the work, in accord with the National Insti-
tutes of Health Guidelines for Research Involving Recombinant
DNA Molecules.
Authors submitting a manuscript do so on the understanding
that if it is accepted for publication, copyright in the article,
including the right to reproduce the article in all forms and media,
shall be assigned exclusively to the Publisher. The Publisher will
not refuse any reasonable request by the author for permission to
reproduce any of his or her contributions to the journal.

xxxiv BLOOD-THE JOURNAL OF THE ASH
(Continued from preceding page)
PREPARING THE MANUSCRIPT
The original and two complete copies of the manuscript must
be submitted. Manuscripts must be typewritten, double or triple
spaced on good quality 8’/2-by-1 1-inch white paper with margins
of at least one inch. Please do not use erasable bond.
The first page of the manuscript should contain the following
information: ( 1 ) title of the paper; (2) authors’ names; (3) name
of institution in which work was done; (4) acknowledgments for
research support; (5) name and address of the author to whom
communications regarding the manuscript should be directed;
(6) a short title, not to exceed 40 characters (including spaces),
to be used as a running title.
The second page should contain an abstract of 200 words or
less, summarizing the reason for the study, the methods used,
the results, and the major conclusions. Do not include a
summary at the end of the paper. The remainder of the paper
should be written as concisely as possible.
PREPARING ILLUSTRATIONS
AND TABLES
Tables and illustrations must be cited in order in the text using
arabic numerals. All line drawings should be submitted as clear,
glossy, black and white photographs. Legible copies may be
used with the duplicate manuscripts. Photomicrographs and
other photographic illustrations must be submitted in duplicate;
copies are not acceptable. Legends for illustrations should be
typewritten, double spaced, on a separate sheet, and included at
the end of the manuscript. A legend must accompany each
illustration. Contributors will pay all charges involved in process-
ing and printing of color photographs.
Figures, especially charts, graphs, and line drawings, are
generally reduced in size for publication (consult a recent issue of
the journal for examples). To maintain legibility it is important
that all numbers, letters, and symbols be large enough originally
so that when reduced they will remain at least Y,2 inch (2 mm)
high (i.e. , approximately the same size as used for this line of
type). Figures not properly prepared will have to be returned to
the contributor for revision or will be relettered by the printer and
the cost charged to the contributor.
Each table should be typed on a separate sheet and appro-
priately numbered. Legends should be typed on the same sheets
as the tables.
REFERENCES
References should be compiled at the end of the article
according to the order of citation in the text. They should be
typewritten, double spaced under the heading REFERENCES.
Abbreviations for titles of medical periodicals should conform to
those used in the latest edition of Index Medicus. (A � ‘List of
Journals Indexed in Index Medicus’ ‘ -with abbreviations-is
obtainable from the Superintendent of Documents, U . S. Govern-
ment Printing Office, Washington, D.C. 20402, at a modest
charge.) References to abstracts and Letters to Editors must be
identified as such. Inclusive page numbers of references are not
required.
Personal communications and references to publications in
press by authors other than those submitting the paper must be
substantiated by a letter from the investigator(s) concerned
confirming the data or observations and granting the authors
permission to cite the material.
EXAMPLES OF REFERENCES
Journal article, one author:
1 . Beutler E: The effect of methemoglobin formation on
sickle cell disease. J Clin Invest 40: 1 856, 1961
Journal article, two or more authors:
2. Karpatkin 5, Charmatz A: Heterogeneity of human platel-
ets. Ill. Glycogen metabolism in platelets of different sizes. Br J
Haematol 19:135, 1970
Journal article, in press:
3. O’Malley JE, Eisenberg L: The hyperkinetic syndrome.
Semin Psychiatry (in press)
Complete book:
4. Lillie RD: Histopathologic Technic and Practical Histo-
chemistry (ed 3). New York, Blakiston, 1965, p 39
Chapter of book:
5. Moore G, Minowada J: Human hemopoietic cell lines: A
progress report, in Fames P (ed): Hemic Cells In Vitro, vol 4.
Baltimore, Williams & Wilkins, 1969, p 100
Chapter of book that is part of published meeting:
6. Natvig JB, Kunkel HG, Gedde-DahI T Jr: Genetic studies of
the heavy chain sub-groups of G 9lobulin, in Killander J (ed):
Gamma Globulins, Proceedings of the Third Nobel Symposium.
New York, Wiley, 1967
Chapter of book that is part of unpublished meeting:
7. Polliak A: A morphologic study of the lymphoproliferative
lesions induced by excess vitamin A. First Meeting, European
Division, International Society of Hematology, Milan, 197 1 , p
181
Abstract:
8. Curnutte JT, Karnovsky ML, Babior BM: Manganese-
dependent NADPH oxidation by a particulate preparation from
guinea pig granulocytes: An alternative interpretation. Clin Res
23:271A, 1975 (Abstr)
Letter to the Editor:
9. Seeler RA: Sickle cell anemia monthly variations. Blood
47:879, 1976 (Letter)
PROOFREADING
Contributors are provided with galley proofs and are asked to
proofread them for typesetting errors. Important changes in data
are allowed, but authors will be charged for excessive alterations
in proof. Galley proofs should be returned within 48 hours.
REPRINTS
Reprints of articles can be furnished to contributors when
ordered in advance of publication. An order form, showing cost
of reprints, is sent with proofs. Individuals wishing to obtain
reprints of an article that appeared in BLOOD can do so by
contacting the author at the address given in the journal.
ANNOUNCEMENTS
Announcements of meetings, conferences, and the like that
are of interest to the readership of BLOOD should be sent to the
Editor at least three months before the first day of the month of
issue. These items should be as concise as possible. When
considered appropriate, they will be published as promptly as
possible, subject to the availability of space in the journal.