18-Cromwell Cases NLA with Summary Baltimore Onsite 9-21-13 · CAPD HIV (HAART) Glucocorticoids...
47
Diagnostic Dilemmas Case Based Interactive Session Diagnostic Dilemmas Case Based Interactive Session William Cromwell, MD, FAHA, FNLA Diplomate, American Board of Clinical Lipidology Chief Medical Officer LipoScience, Inc. Chief Lipoprotein and Metabolic Disorders Institute Adjunct Associate Professor Wake Forest University School of Medicine William Cromwell, MD, FAHA, FNLA Diplomate, American Board of Clinical Lipidology Chief Medical Officer LipoScience, Inc. Chief Lipoprotein and Metabolic Disorders Institute Adjunct Associate Professor Wake Forest University School of Medicine
Transcript of 18-Cromwell Cases NLA with Summary Baltimore Onsite 9-21-13 · CAPD HIV (HAART) Glucocorticoids...

Diagnostic DilemmasCase Based Interactive Session
Diagnostic DilemmasCase Based Interactive Session
William Cromwell, MD, FAHA, FNLA
Diplomate, American Board of Clinical Lipidology
Chief Medical OfficerLipoScience, Inc.
ChiefLipoprotein and Metabolic Disorders Institute
Adjunct Associate ProfessorWake Forest University School of Medicine
William Cromwell, MD, FAHA, FNLA
Diplomate, American Board of Clinical Lipidology
Chief Medical OfficerLipoScience, Inc.
ChiefLipoprotein and Metabolic Disorders Institute
Adjunct Associate ProfessorWake Forest University School of Medicine

William Cromwell, MD, FAHA, FNLADisclosures
William Cromwell, MD, FAHA, FNLADisclosures

54 year-old male presents for evaluated of hypertriglyceridemia. o Triglyceride in 1987 was 500 mg/dL.
o Multiple fasting lipid profiles since that time show:Total Cholesterol 280 – 350 mg/dLTriglycerides 400 – 460 mg/dLHDL Cholesterol 35 – 42 mg/dL
o Prior medical therapy includes:Atorvastatin 40 mg daily and Fish oil 2000 mg daily
(DHA+EPA content unknown)o No current lipid lowering medications.
o Diet is a described as “low carbohydrate” diet.
o No routine physical activity
Case RYCase RY

He was evaluated for an episode of chest pain in May 2007 with cardiac enzymes and stress echocardiogram which were unremarkable. Chest pain was felt to be due to gastroesophagealreflux. He is able to engage in activities of choice without complaints.
Past Medical History: Elevated BP (no diagnosis of HTN)
GERDCurrent Medications: None
Family History: Unremarkable Review of Systems: Unremarkable,
Weight unchanged x 6 months
Case RYCase RY

PE: BP 138/86 Pulse 74 Wt 212 lb Ht 68” Waist 38” BMI 32.2Otherwise unremarkable
Case RYCase RY
Baseline
Total-C 300 mg/dL TG 390 mg/dLHDL-C 42 mg/dL LDL-C 178 mg/dLNon HDL-C 258 mg/dL
TSH, LFT, Creatinine all WNLFBS 105 mg/dL
“Low Carb” DietNo Exercise Regimen
What Lipoprotein AbnormalityIs Present?
Is increased lipoprotein related CHD risk present?
What lipid / lipoprotein targets are appropriate?

■ Normal■ Hypoalpha-
lipoproteinemia
■ Complete (FHC)or partial LPLdeficiencyassociated witha secondaryfactor
■ Complete LPLdeficiency
(FHC)■ Primary apoC-II
deficiency
■ Familial dysbeta-lipoproteinemia(type III)
■ Hepatic lipasedeficiency
■ (Primary causeassociated witha secondaryfactor)
Apo B > 75 mg/dL
Apo B < 75 mg/dL
TC:Apo B> 2.4
TC:Apo B < 2.4
■ FamilialhyperTG
■ Partial LPLdeficiency
■ FH■ Polygenic■ FDB■ PCSK9deficiency■ ARH deficiency■ CYP7A1deficiency■ Hypoalphalipo-proteinemia
■ FCH■ β-Sitosterolemia
Normal Chylo + VLDL Chylo Chylo + VLDL Remnants
VLDL LDL VLDL + LDL
NormoTG< 133 mg/dL
TG:Apo B > 8.8
NormoApo B< 120 mg/dL
TG:Apo B < 8.8
HyperTG> 133 mg/dL
NomoTG> 133 mg/dL
HyperApo B> 120 mg/dL
Hyper TG> 133 mg/dL
PrimaryCauses
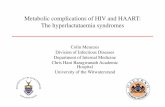
Algorithm for Differential Diagnosis of HypertriglyceridemiaAlgorithm for Differential Diagnosis of Hypertriglyceridemia
Abbreviations: apo, apolipoprotein; ARH, autosomal recessive hypercholesterolemia; CAPD, continuous ambulatory peritoneal dialysis; Chylo, chylomicrons; CP7A1, cytochrome P450 7A1; DM2, diabetes mellitus type 2; dysbeta; dysbetalipoproteinemia; FCH, familial combined hyperlipidemia; FDB, familial defective apoB; FH, familial hypercholesterolemia; FHC, familial hyperchylomicronemia; HAART, highly active antiretroviral therapy; LPL, lipoprotein lipase; PCOS, polycystic ovary syndrome; SLE, systemic lupus erythematosus; TC, total cholesterol; TG, triglyceride.
de Graaf J et al. Nat Clin Pract Endocrinol Metab 2008;4:608-18.
Lipoproteins

Apo B > 75 mg/dL
Apo B < 75 mg/dL
TC:Apo B > 2.4
TC:Apo B < 2.4
Normal Chylo + VLDL Chylo Chylo + VLDL Remnants
VLDL LDL VLDL + LDL
NormoTG< 133 mg/dL
TG:Apo B > 8.8
NormoApo B< 120 mg/dL
TG:Apo B< 8.8
HyperTG> 133 mg/dL
NomoTG> 133 mg/dL
HyperApo B> 120 mg/dL
Hyper TG> 133 mg/dL
SecondaryCauses
■ Normal ■ DM2■ Metabolic
syndrome■ Abdominal
obesity■ Alcohol■ Glucocorticoids■ Estrogens■ Chronic renal
failure■ Pregnancy
■ SLE withacquired apoC-IIdeficiency
■ DM2■ Metabolic
syndrome■ Abdominal
obesity■ Alcohol■ Hyperthyroidism■ Glucocorticoids■ Chronic renal
failure
■ DM2■ Metabolic
syndrome■ Abdominal
obesity■ Alcohol■ Glucocorticoids■ Estrogens■ Chronic renal
failure■ Hemodialysis
■ Nephroticsyndrome
■ Hypothyroidism■ Anabolic
steroids
■ DM2■ Metabolic
syndrome■ Abdominal
obesity■ Nephrotic
syndrome■ Cholestasis■ SLE, PCOS,
CAPD■ HIV (HAART)■ Glucocorticoids■ Antipsychotic
drugs■ Pregnancy 3rd
trimester
Abbreviations: apo, apolipoprotein; ARH, autosomal recessive hypercholesterolemia; CAPD, continuous ambulatory peritoneal dialysis; Chylo, chylomicrons; CP7A1, cytochrome P450 7A1; DM2, diabetes mellitus type 2; dysbeta; dysbetalipoproteinemia; FCH, familial combined hyperlipidemia; FDB, familial defective apoB; FH, familial hypercholesterolemia; FHC, familial hyperchylomicronemia; HAART, highly active antiretroviral therapy; LPL, lipoprotein lipase; PCOS, polycystic ovary syndrome; SLE, systemic lupus erythematosus; TC, total cholesterol; TG, triglyceride.
de Graaf J et al. Nat Clin Pract Endocrinol Metab 2008;4:608-18.
Lipoproteins
Algorithm for Differential Diagnosis of HypertriglyceridemiaAlgorithm for Differential Diagnosis of Hypertriglyceridemia

Apo B > 75 mg/dL
Apo B < 75 mg/dL
TC:Apo B > 2.4
TC:Apo B < 2.4
Normal Chylo + VLDL Chylo Chylo + VLDL Remnants
VLDL LDL VLDL + LDL
NormoTG< 133 mg/dL
TG:Apo B > 8.8
NormoApo B< 120 mg/dL
TG:Apo B < 8.8
HyperTG> 133 mg/dL
NomoTG> 133 mg/dL
HyperApo B> 120 mg/dL
Hyper TG> 133 mg/dL
Apo B = 81 mg/dL ■ Familial dysbeta-lipoproteinemia(type III)
■ Hepatic lipasedeficiency
■ (Primary causeassociated witha secondaryfactor)
PrimaryCauses
SecondaryCauses
■ DM2■ Metabolic
syndrome■ Abdominal
obesity■ Alcohol■ Hyperthyroidism■ Glucocorticoids■ Chronic renal
failure
TC = 300 mg/dL TC:Apo B = 3.7
TG = 390 mg/dLTG:Apo B = 4.93
Apo E phenotype = E2/E2
Case RYCase RYWhat Lipoprotein Abnormality Is Present?What Lipoprotein Abnormality Is Present?

2 Major Risk Factors (age, low HDL-C)10-year Framingham Risk Score = 12% (moderately high risk)
What additional evaluation should be considered?
A. hs-CRP test?B. Non-Invasive Imaging?
(Coronary Calcium Score, CIMT)C. Other testing?
Case RYCase RYWhat Is The Patients Cardiovascular Risk?What Is The Patients Cardiovascular Risk?

2 Major Risk Factors (age, low HDL-C)10-year Framingham Risk Score = 12% (moderately high risk)
Additional Results:
hs-CRP = 4.710-year Reynolds Risk Score = 10% (moderately high risk)
Coronary Calcium Score = 1310 (>95th percentile)10-year MESA Risk Score = 30% (CHD Risk Equivalent)Lp(a) = 15
Overall CHD Risk = Very High Risk
Case RYCase RYWhat Is The Patients Cardiovascular Risk?What Is The Patients Cardiovascular Risk?

Overall CHD Risk = Very High Risk
Goals: Baseline:
LDL-C: < 70 mg/dL 178 mg/dLnon HDL-C: < 100 mg/dL 258 mg/dLTG: < 150 mg/dL 390 mg/dLOptionalApo B: < 70 mg/dL 81 mg/dL
Case RYCase RYWhat Are The Appropriate Targets of Therapy?What Are The Appropriate Targets of Therapy?

Clinical Intervention
Therapeutic Lifestyle ChangesWeight Optimization Mediterranean Eating Pattern
25% calories from fat, low refined carbohydrates
Exercise 45 minutes, 5 days per week
Pharmacologic Therapy
Atorvastatin 40mg dailyFenofibrate 160 mg daily
Case RYCase RYWhat Management Options Should Be Considered?What Management Options Should Be Considered?

Overall CHD Risk = Very High Risk
Goals: Baseline: 6 months(24 lb loss)
LDL-C: < 70 mg/dL 178 mg/dL 73 mg/dLnon HDL-C: < 100 mg/dL 258 mg/dL 104 mg/dLTG: < 150 mg/dL 390 mg/dL 142 mg/dLOptional Apo B: < 70 mg/dL 81 mg/dL 55 mg/dL
Case RYCase RYResponse To TherapyResponse To Therapy

Therapy
Baseline 6 Month
Atorvastatin40 mg
Fenofibrate 160 mg
TLC (24# Wt Loss)
Total-C (mg/dL) 300 146
TG (mg/dL) 390 142HDL-C (mg/dL) 42 45
LDL-C (mg/dL) [Goal < 70 mg/dL] 178 73
% Change vs. Baseline 58%
Non HDL-C[Goal < 100 mg/dL] 258 104
Apo B (mg/dL)[Goal < 70 mg/dL] 81 55
% Change vs. Baseline 32%
Summary Case RYSummary Case RY

Case RYCase RYWhat Management Options Should Be Considered?What Management Options Should Be Considered?
Clinical Intervention
Therapeutic Lifestyle ChangesWeight Optimization Mediterranean Eating Pattern
25% calories from fat, low refined carbohydrates
Exercise 45 minutes, 5 days per week
Pharmacologic Therapy Adjustment?

Therapy
Baseline 6 Month
Atorvastatin40 mg
Fenofibrate 160 mg
TLC (24# Wt Loss)
1 Year
Atorvastatin40 mg
TLC (57# Wt Loss)
Total-C (mg/dL) 300 146 142
TG (mg/dL) 390 142 54HDL-C (mg/dL) 42 45 75
LDL-C (mg/dL) [Goal < 70 mg/dL] 178 73 64
% Change vs. Baseline 35% 64%
Non HDL-C[Goal < 100 mg/dL] 258 104 67
Apo B (mg/dL)[Goal < 70 mg/dL] 81 55 40
% Change vs. Baseline 32% 51%
Summary Case RYSummary Case RY


17 year-old male presents for evaluated of hyperlipidemia.
Patient first became aware of abnormal serum lipids at approximately age 8 when laboratory studies showed total cholesterol > 300 mg/dL.
o Multiple lipid profiles since that performed (details incomplete):
Total Cholesterol 350 – 420 mg/dLo No medical therapy to date.
o Diet is a described as “low fat” diet.
o Exercise consist of playing lacrosse and cross country running 75 minutes of sustained physical activity, 5 times per week.
Case MGCase MG

Past Medical History: HyperlipidemiaCurrent Medications: None
Family History: Father – hyperlipidemia (elevated TC, TG)CHD (CABG x 4 at age 40)
Mother – hyperlipidemia (elevated TC)
No information regarding other family membersNo siblings
Review of Systems: Unremarkable, Weight unchanged x 6 months
Case MGCase MG

PE: BP 118/74 Pulse 68 Wt 146.4 lb Ht 68.5” Waist 30” BMI 21.9Otherwise unremarkable
Case MGCase MG
Baseline
Total-C 311 mg/dL TG 163 mg/dLHDL-C 37 mg/dL LDL-C 241 mg/dLNon HDL-C 274 mg/dL
TSH, LFT, FBS, Creatinine all WNL
“Low Fat” DietExercise 75 Minutes, 5 x week
What Lipoprotein AbnormalityIs Present?
Is increased lipoprotein related CHD risk present?
What lipid / lipoprotein targets are appropriate?

Apo B > 75 mg/dL
Apo B < 75 mg/dL
TC:Apo B > 2.4
TC:Apo B < 2.4
Normal Chylo + VLDL Chylo Chylo + VLDL Remnants
VLDL LDL VLDL + LDL
NormoTG< 133 mg/dL
TG:Apo B > 8.8
NormoApo B< 120 mg/dL
TG:Apo B < 8.8
HyperTG> 133 mg/dL
NomoTG> 133 mg/dL
HyperApo B> 120 mg/dL
Hyper TG> 133 mg/dL
Apo B = 205 mg/dL PrimaryCauses
SecondaryCauses
TG = 163 mg/dL
Case MGCase MGWhat Lipoprotein Abnormality Is Present?What Lipoprotein Abnormality Is Present?
■ FCH■ β-Sitosterolemia ■ DM2
■ Metabolic syndrome■ Abdominal obesity■ Nephrotic syndrome■ Cholestasis■ SLE, PCOS, CAPD■ HIV (HAART)■ Glucocorticoids■ Antipsychotic drugs■ Pregnancy 3rd trimester

Nomogram to Diagnose Familial Combined HyperlipidemiaNomogram to Diagnose Familial Combined Hyperlipidemia
Adapted from Veerkamp MJ, et al. Circulation 2004;109:2980-2985.

Total Cholesterol and Triglyceride PercentilesNational Health and Nutrition Examination Survey 1999‐2006Total Cholesterol and Triglyceride PercentilesNational Health and Nutrition Examination Survey 1999‐2006
Total Cholesterol 1(mg/dL)
Percentiles
White Male Age 10th 25th 50th 75th 90th 95th
12‐17 122 136 154 174 195 212Patient MG 311 (99th percentile)
Triglyceride 2(mg/dL)
Percentiles
White Male Age 10th 25th 50th 75th 90th 95th
17 45 58 80 114 164 210Patient MG 163 (90th percentile)
1. Circulation. 2009;119:1108-11152. J Pediatrics 2009;155:S6.e15-26

163 mg/dL90th
7 points
311 mg/dL99th 4 points
205 mg/dL 5.5 points
16.5 points
Nomogram to Diagnose Familial Combined HyperlipidemiaNomogram to Diagnose Familial Combined Hyperlipidemia
Adapted from Veerkamp MJ, et al. Circulation 2004;109:2980-2985.

10 year versus lifetime assessment?
What additional evaluation should be considered?
A. hs-CRP test?B. Non-Invasive Imaging?
(CIMT)C. Other testing?
Case MGCase MGWhat Is The Patients Cardiovascular Risk?What Is The Patients Cardiovascular Risk?

Additional Results:hs-CRP = 0.46
CIMT = mean CIMT 0.636, Max CIMT 0.7371.523 mm plaque L Bulb, 1.601 mm plaque R Bulb
Lp(a) = 10LDL-P = > 3500 nmol/L
Absorptive Biomarkers = HyperabsorberCampesterol (5.4 ug/mL), Sitosterol (4.5 ug/mL), Cholestanol (4.2 ug/mL)
Lifetime CHD Risk = Very High Risk
Case MGCase MGWhat Is The Patients Cardiovascular Risk?What Is The Patients Cardiovascular Risk?

Lifetime CHD Risk = Very High Risk
Goals: Baseline:
LDL-C: < 70 mg/dL 241 mg/dLnon HDL-C: < 100 mg/dL 274 mg/dLTG: < 150 mg/dL 163 mg/dLOptionalLDL-P: < 800 nmol/L > 3500 nmol/L
Case MGCase MGWhat Are The Appropriate Targets of Therapy?What Are The Appropriate Targets of Therapy?

Therapeutic Lifestyle Changes?
Pharmacologic Therapy?
Case MGCase MGWhat Management Options Should Be Considered?What Management Options Should Be Considered?

Clinical Intervention
Therapeutic Lifestyle ChangesMediterranean Eating Patternlow saturated fat, low refined carbohydrates
Maintain Exercise
Pharmacologic Therapy
Rosuvastatin 20mg daily
Case MGCase MGWhat Management Options Should Be Considered?What Management Options Should Be Considered?

Overall CHD Risk = Very High Risk
Goals: Baseline: 3 months(Wt stable)
LDL-C: < 70 mg/dL 241 mg/dL 104 mg/dLnon HDL-C: < 100 mg/dL 274 mg/dL 130 mg/dLTG: < 150 mg/dL 163 mg/dL 104 mg/dLOptional LDL-P: < 800 nmol/L >3500 nmol/L 1992 nmol/L
Case MG
Response to Therapy
Case MG
Response to Therapy

Therapy
Baseline 3 Month
Rosuvastatin20 mg
TLC (Wt Stable)
Total-C (mg/dL) 311 175
TG (mg/dL) 163 129HDL-C (mg/dL) 37 45
LDL-C (mg/dL) [Goal < 70 mg/dL] 241 104
% Change vs. Baseline 57%
Non HDL-C[Goal < 100 mg/dL] 274 104
LDL-P (nmol/L)[Goal < 800 nmol/L] > 3500 1992
% Change vs. Baseline 43%
Summary Case MGSummary Case MG

Case MGCase MGWhat Management Options Should Be Considered?What Management Options Should Be Considered?
Clinical Intervention
Therapeutic Lifestyle ChangesMediterranean Eating Patternlow saturated fat, low refined carbohydrates
Maintain Exercise
Pharmacologic Therapy Adjustment?

Therapy
Baseline 3 Month
Rosuvastatin20 mg
TLC (Wt Stable)
3 Month
Rosuvastatin20 mg
Ezetimibe 10 mg
TLC (Wt Stable)
Total-C (mg/dL) 311 175 93
TG (mg/dL) 163 129 79HDL-C (mg/dL) 37 45 45
LDL-C (mg/dL) [Goal < 70 mg/dL] 241 104 32
% Change vs. Baseline 57% 87%
Non HDL-C[Goal < 100 mg/dL] 274 104 48
LDL-P (nmol/L)[Goal < 800 nmol/L] > 3500 1992 704
% Change vs. Baseline 43% 80%
Summary Case MGSummary Case MG


37 year-old male presents for evaluated of hypercholesterolemia.
Patient first became aware of abnormal serum lipids at approximately age 30 when laboratory studies showed total cholesterol > 200 mg/dL.
o Rare lipid profiles performed since that time (details unknown).
o No medical therapy to date.o Diet is a described as “moderation” diet.
o Exercise consist of 75 minutes of sustained physical activity, 5-7 times per week. Patient is an Army Ranger.
Case PKCase PK

Past Medical History: Hyperlipidemia
Current Medications: NoneFamily History: Father – CHD (stent x 2 at age 45)
Paternal GF – CHD (fatal MI age 48)
Information regarding siblings unknownReview of Systems: Unremarkable,
Weight unchanged x 6 months
Case PKCase PK

PE: BP 128/74 Pulse 62 Wt 205 lb Ht 75.5” Waist 35” BMI 25.3Otherwise unremarkable
Case PKCase PK
Baseline
Total-C 209 mg/dL TG 123 mg/dLHDL-C 55 mg/dL LDL-C 129 mg/dLNon HDL-C 154 mg/dL
TSH, LFT, FBS, Creatinine all WNL
“Moderation” DietExercise 75 Min, 5-7 x week
What Lipoprotein AbnormalityIs Present?
Is increased lipoprotein related CHD risk present?
What lipid / lipoprotein targets are appropriate?

Apo B > 75 mg/dL
Apo B < 75 mg/dL
TC:Apo B > 2.4
TC:Apo B < 2.4
Normal Chylo + VLDL Chylo Chylo + VLDL Remnants
VLDL LDL VLDL + LDL
NormoTG< 133 mg/dL
TG:Apo B > 8.8
NormoApo B< 120 mg/dL
TG:Apo B < 8.8
HyperTG> 133 mg/dL
NomoTG> 133 mg/dL
HyperApo B> 120 mg/dL
Hyper TG> 133 mg/dL
Apo B = 103 mg/dLTG = 123 mg/dL
Case PKCase PKWhat Lipoprotein Abnormality Is Present?What Lipoprotein Abnormality Is Present?

1 Major Risk Factor (family history)10-year Framingham Risk Score = 2.8% (low risk)
What additional evaluation should be considered?
A. hs-CRP test?B. Non-Invasive Imaging?
(Coronary Calcium Score, CIMT)C. Other testing?
Case PKCase PKWhat Is The Patients Cardiovascular Risk?What Is The Patients Cardiovascular Risk?

1 Major Risk Factor (family history)10-year Framingham Risk Score = 2.8% (low risk)
Additional Results:
hs-CRP = 2.710-year Reynolds Risk Score = 3.6% (low risk)
CIMT = mean CIMT 0.582, Max CIMT 0.764 (unremarkable)1.723 mm plaque L Bulb, 2.201 mm plaque RICA
Lp(a) = 270
LDL-P = 1580 nmol/L
Lifetime CHD Risk = Very High Risk
Case PKCase PKWhat Is The Patients Cardiovascular Risk?What Is The Patients Cardiovascular Risk?

Lifetime CHD Risk = Very High Risk
Goals: Baseline:
LDL-C: < 70 mg/dL 129 mg/dLnon HDL-C: < 100 mg/dL 154 mg/dLTG: < 150 mg/dL 123 mg/dLOptionalLDL-P: < 800 nmol/L 1580 nmol/L
Case PKCase PKWhat Are The Appropriate Targets of Therapy?What Are The Appropriate Targets of Therapy?

Therapeutic Lifestyle Changes?
Pharmacologic Therapy?
Case PKCase PKWhat Management Options Should Be Considered?What Management Options Should Be Considered?

Clinical Intervention
Therapeutic Lifestyle ChangesMediterranean Eating Patternlow saturated fat, low refined carbohydrates
Maintain Exercise
Pharmacologic Therapy
Simvastatin 20mg dailyNiaspan 1000mg daily
Case PKCase PKWhat Management Options Should Be Considered?What Management Options Should Be Considered?

Overall CHD Risk = Very High Risk
Goals: Baseline: 4 months(15# Wt Loss)
LDL-C: < 70 mg/dL 129 mg/dL 89 mg/dLnon HDL-C: < 100 mg/dL 154 mg/dL 111 mg/dLTG: < 150 mg/dL 123 mg/dL 69 mg/dLOptional LDL-P: < 800 nmol/L 1580 nmol/L 792 nmol/L
Case PK
Response to Therapy
Case PK
Response to Therapy

Therapy
Baseline 4 Month
Simvastatin20 mg
Niaspan1000 mg
TLC (15# Wt Loss)
Total-C (mg/dL) 209 166
TG (mg/dL) 123 69HDL-C (mg/dL) 55 48
LDL-C (mg/dL) [Goal < 70 mg/dL] 129 104
% Change vs. Baseline 19%
Non HDL-C[Goal < 100 mg/dL] 154 118
LDL-P (nmol/L)[Goal < 800 nmol/L] 1580 792
% Change vs. Baseline 50%
Summary Case MGSummary Case MG

Case PKCase PKWhat Management Options Should Be Considered?What Management Options Should Be Considered?
Clinical Intervention
Therapeutic Lifestyle ChangesMediterranean Eating Patternlow saturated fat, low refined carbohydrates
Maintain Exercise
Pharmacologic Therapy Adjustment?

o Type III Dyslipoproteinemia, Metabolic Syndrome. o Apo E2/E2 and “second hit” resulting in increased VLDL (insulin
resistance)
o Familial Combined Hyperlipidemia, Sterol Hyperabsorption
o FCH – mixed overproduction / clearance defect
Increased apoB containing lipoproteins that may manifest as one of 3 lipid phentypes (high TG, high Cholesterol, both high)
o Hyperabsorption of plant sterols / stanols
o Elevated Lp(a) with relative elevation of LDL particle number
Case RYCase RY
Case MGCase MG
Case PKCase PK
SummarySummary