#12, 13, 14 cardiovascular
75
NURS 216 Spring 2013 Dr. Smith
Transcript of #12, 13, 14 cardiovascular

NURS 216 Spring 2013
Dr. Smith

Reading You must read Chapter 17 for review of the structure
and normal function of the cv system. Slides 5-20 in this lecture should be review from A&P and we will only briefly discuss them.
We will discuss most parts of Chapter 18 except for HTN in special populations.
We will discuss most parts of Chapter 19 except for heart disease in infants and children.

Objectives Review important concepts of cardiovascular anatomy:
layers of the heart, valves, electrical conducting system
Review important concepts of cardiovascular physiology: mechanical function, hemodynamics, regulation of cardiac output and blood flow
Review components of the systemic circulation and blood vessels

Discuss disorders of arterial function: artherosclerosis, peripheral arterial disorders, aneurysms and dissections
Discuss control of blood pressure and hypertension
Discuss disorders of venous function: varicose veins and venous thrombosis
Discuss coronary heart disease: chronic and acute
Discuss pericardial, myocardial, endocardial, and valvular disorders
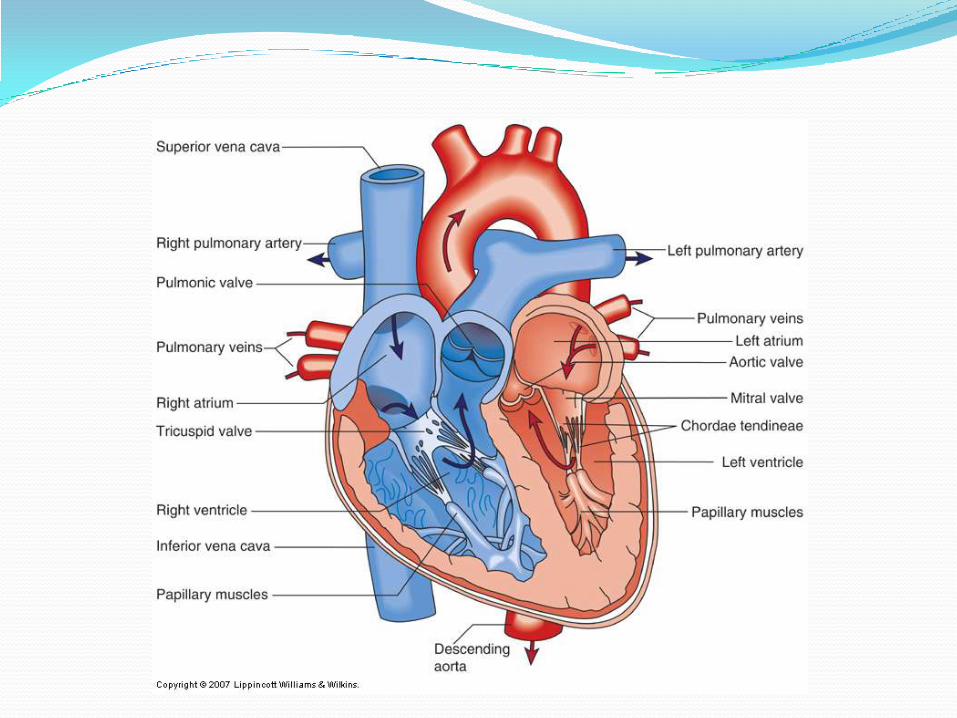

Mechanical Functions The heart’s job is to pump blood throughout the
circulatory system
Cardiac muscle is similar to skeletal, with addition of intercalated disks
Atria and ventricles must be coordinated and healthy to achieve ideal blood flow and circulation

Pulmonary circulation:
smaller volume,
low pressure
Systemic circulation:
larger volume,
high pressure

Arterial vs. Venous System Difference in type and thickness of layers
Vascular smooth muscle
Arterial system: high-pressure “resistance” vessels, blood moves through b/c of pressure pulsations from LV
Venous system: low-pressure “capacitance” vessels, blood moves through by muscle pumps
-valves
-effects of gravity
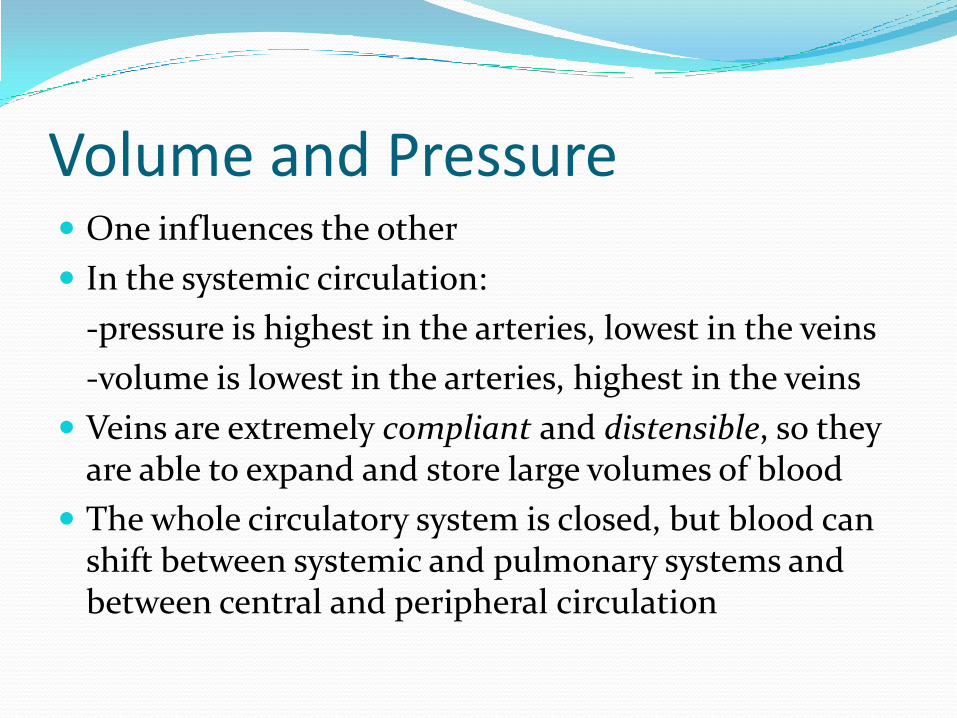
Volume and Pressure One influences the other
In the systemic circulation:
-pressure is highest in the arteries, lowest in the veins
-volume is lowest in the arteries, highest in the veins
Veins are extremely compliant and distensible, so they are able to expand and store large volumes of blood
The whole circulatory system is closed, but blood can shift between systemic and pulmonary systems and between central and peripheral circulation

Pressure, Resistance, and Flow Blood flow (cardiac output) = Δ pressure/resistance
-higher pressure gradient means more blood flow
-higher resistance means less blood flow
Resistance is affected by radius of the vessel and blood viscosity
Ideally, blood flow is laminar, not turbulent
Laplace law: P = T/r may restate: T = P*r
Intraluminal
pressureWall
tension
Vessel
radius

Layers of the Heart

Coronary Arteries
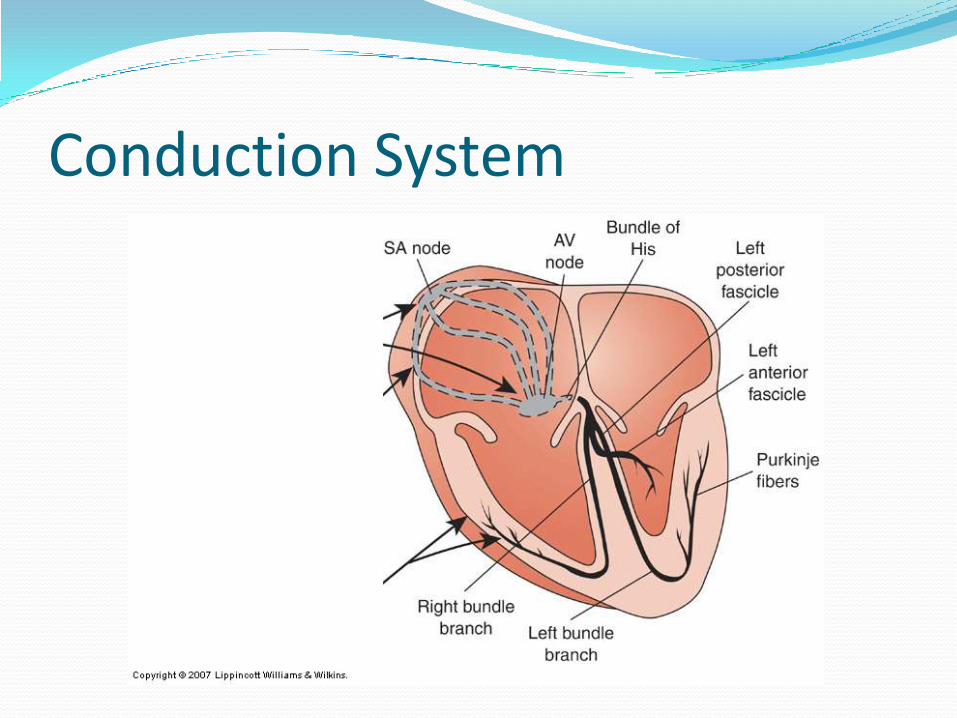
Conduction System

Electrocardiogram (EKG or ECG)

Cardiac Cycle During systole, AV valves are closed, semilunar valves open,
and ventricles eject their blood into the pulmonary arteries and aorta
During diastole, semilunar valves are closed, AV valves open, and atria drop blood down into ventricles
At end of diastole, there is an “atrial kick”
End Diastolic Volume (EDV) = volume in ventricles at end of diastole
End Systolic Volume (ESV) = volume at end of systole
Stroke Volume (SV) = EDV-ESV usually ~ 70 mL
Ejection fraction (EF) = SV/EDV usually ~ 60-70%

Cardiac Output Determinants Cardiac output (CO) = SV x HR, measured in L/min
-varies greatly with metabolic demands, activity
-anywhere from 4 to 8 L/min
Preload = EDV, “volume work” or “prestretch”
-to a limit, higher preloads cause a stronger contraction (due to arrangement of muscle fibers)
Afterload = pressure that LV must overcome to pump blood into aorta “pressure work” (blood pressure)
Contractility = increased strength of contraction independent of preload

Control of Cardiovascular Function CV system is innervated by the autonomic nervous
system (ANS)
Effects of sympathetic and parasympathetic systems
Vagus nerve
SNS is the main controller of blood vessels
Autoregulation in the tissue beds
-histamine, serotonin, kinins, prostaglandins
Endothelial control
-nitrous oxide (NO), angiotensin II

Arterial Disorders Hyperlipidemia and atherosclerosis (central)
Peripheral arterial problems
Aneurysms and dissections (usually central)

Atherosclerosis The development of fibrous, fatty lesions in the intima
of large and medium-sized arteries (aorta, coronary arteries, cerebral arteries)
MOST COMMON CAUSE OF CORONARY HEART DISEASE!!!
Vessels become narrowed, blood flow decreases, leads to ischemia (chronic)
A portion of the lesion or plaque can break off and completely block blood flow (acute)

Atherosclerosis Why? Response-to-injury hypothesis
The intima is damaged (HTN + high LDL = danger)
Injury to the endothelium changes the permeability and causes an inflammatory response
Monocytes and platelets are attracted to the injury
Monocytes and oxidized LDL molecules burrow under intima
Lesion under intima grows, core may become necrotic, may harden due to calcium deposits
Thrombosis, hemorrhage, or rupture of fibrous cap may occur

Hyperlipidemia Types of lipoproteins are
categorized by the amount of fat (density)
“bad” and “good”
Levels affected by diet, activity level, and liver function

Hypercholesterolemia Specifically, too-high levels of LDL or Total Cholesterol
Primary (familial) or secondary
Measure with a fasting lipid profile/panel
Treat with diet, exercise, then medications
More aggressive depending on other CHD risk factors
Goal levels:
-LDL <100 mg/dL
-TC < 200
-HDL > 60

Atherosclerosis Always monitor risk factors, work with patient to
improve/reduce them
If patient develops s/sx:
-exercise/stress test
-cardiac catheterization
May need angioplasty, stents, or coronary artery bypass grafting (CABG)



CHD Risk Factors Biologic: male gender, increasing age, family history
Modifiable: hyperlipidemia, hypertension, smoking, diabetes mellitus, obesity, sedentary lifestyle
Negative risk factor: high HDL-C

Peripheral Arterial Disease Can also have atherosclerosis in peripheral arteries,
often superficial femoral and popliteal
Same risk factors as CHD
Blood flow to the extremity is reduced
Intermittent claudication
Diagnose by signs of hypoxia in limb, palpation of pulses, ultrasound
Address risk factors, avoid injury, medications
May need a stent

Aneursyms and Dissections Atrophy or weakness of the medial layer causes a
dilation of the artery
Can occur in any artery of the body, commonly abdominal aorta
Degeneration caused by atherosclerosis, connective tissue disorders, increased blood pressure around a stenotic area
Example types: berry, fusiform, saccular, dissection

Aneursyms and Dissections Increasing radius at the weakened spot increases
tension inside artery (LaPlace Law)
Danger of eventual rupture
Abdominal aortic aneurysm:
-usually over age 50, increase with age
-often asymptomatic, possible pulsating mass
Aortic dissection:
-most common site is the ascending aorta
-rupture, hemorrhage into vessel wall
-abrupt, intense pain, BP quickly falls – usu FATAL


Blood Pressure definitions BP is measured in an
artery, usually the brachial
Measured in mmHg
BP is the pressure inside an artery caused by the movement of blood through it
BP = CO * PVR

Short-Term Regulation of BP Neural
-baroreceptors: pressure sensors, in carotids and aortic arch
-chemoreceptors: chemical sensors, in carotids and aortic arch
Humoral
-RAA System (renin is released by the kidneys)
-vasopressin/ADH: released in response to decreased BP or increased osmolality of blood

RAA System Renin release stimulated by:
-increased SNS activity
-decreased BP, ECF volume, or ECF Na concentration
Renin changes to angiotensin I in the blood, then into angiotensin II in the lungs
Angiotensin II effects:
-vasoconstriction of arterioles (short-term control)
-stimulates aldosterone release, causing Na and water retention (longer-term control)
Long-Term Regulation of BP Mainly by the kidneys via their control of ECF volume
ECF excess causes higher rates of Na and H2O excretion
ECF deficit causes lower rates of Na and H2O excretion
Many blood pressure medications work through changing kidney function
Essential Hypertension Aka “primary” HTN, accounts for 90-95% of HTN
Normal BP = <120 and <80
HTN = >140 or >90
Biological risk factors:
Lifestyle risk factors:
Criteria for HTN diagnosis: at least 2 separate readings
Treatments: lifestyle modifications, medications

Manifestations of Hypertension “the silent killer”
Major risk factor for atherosclerosis
Increases workload of the LV
Target Organ Damage
Heart: LVH (LV hypertrophy), angina, MI, prior stents/CABG, heart failure
TIA or strokes in brain
Chronic kidney disease
Peripheral vascular disease
retinopathy

Secondary Hypertension d/t another condition, correcting that condition often
improves BP
Kidney disease
Excess aldosterone or glucocorticoids
Pheochromocytoma – tumor usually in the adrenal medulla
Coarctation of the aorta
Malignant HTN

http://www.biij.org/2006/2/e11/
3D reconstruction of CT angiography of an
infant with coarctation of the aorta

Orthostatic Hypotension AKA postural
hypotension
SNS reflexes don’t work properly
BP quickly drops, decreasing CBF -> dizziness & syncope
With position change, see BP drop and HR increase

Orthostatic Hypotension Causes Reduced blood volume
Medications
Aging
Immobility, extended bed rest
Autonomic nervous system dysfunction
Treatment depends on identifying a cause

Coronary Arteries
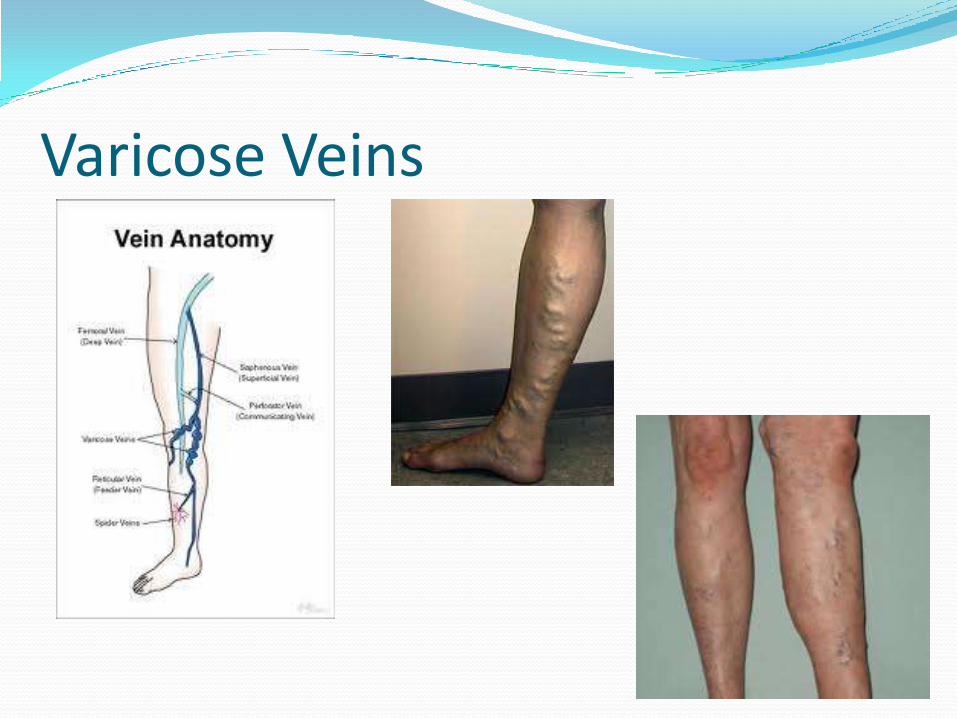
Venous Disorders – Varicose Veins Legs contain superficial and deep veins
Varicose veins – dilated, enlarged superficial veins
Occur due to impaired or blocked flow in deep veins, increased pressure is superficial veins
More common after age 50, in obese persons & women
Long-term increased venous pressures eventually weaken valves, worsening the vein distension
Support stockings, surgical repair
Varicose Veins

Chronic Venous Insufficiency Commonly caused by reflux/backflow through
damaged veins
Worsened by prolonged standing
s/sx: varicose veins, tissue congestion, edema, eventual impaired nutrient delivery to tissues (necrosis, dermatitis, stasis ulcers, thin/shiny skin)
Most common in lower legs

Venous Disorders - DVTs Deep Vein Thrombosis (DVT)
Risk factors: blood stasis, vessel wall injury, increased coagulability (Virchow’s triad)
-what clinical conditions could lead to these risk factors?
May be asymptomatic when small, but gradually tend to increase in size
S/sx: pain, swelling, tenderness (usually unilateral, often in calf)
Complications?


Pericardial Disorders Pericardial effusion
-accumulation of fluid in the pericardial cavity
-can compress heart, lower SV
-diagnose with ultrasound/echo
-pericardiocentesis
-cardiac tamponade
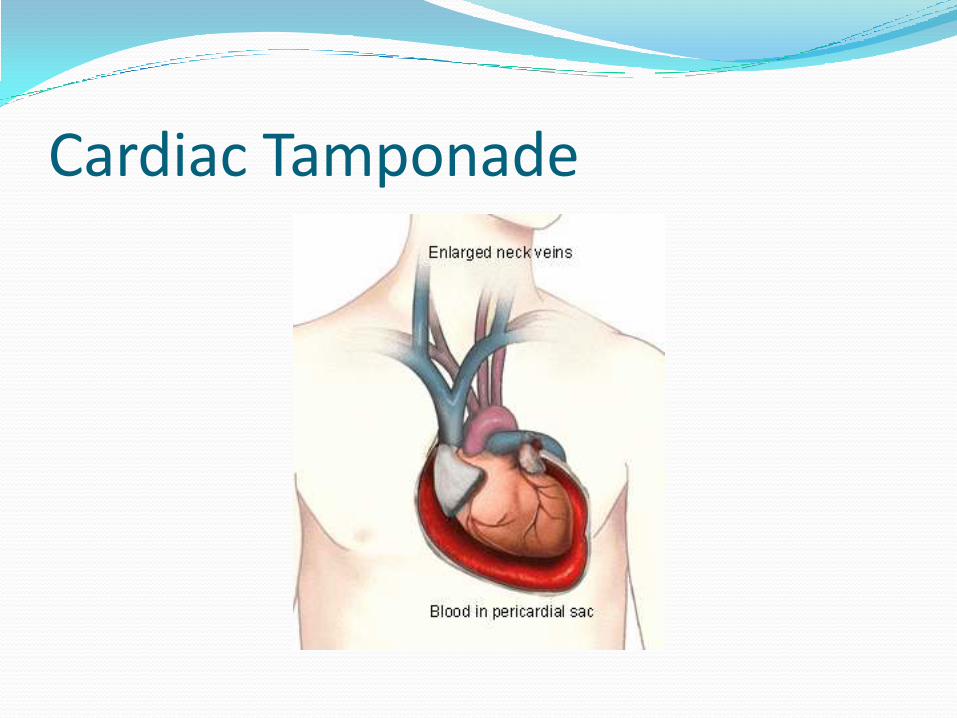
Cardiac Tamponade

Pericarditis Acute – can be after infections or trauma
-increased capillary permeability allows exudate into pericardial cavity
-S/sx: chest pain, pericardial friction rub, EKG changes
Chronic – exudate may remain for months, years
-often due to systemic diseases
-symptoms usually minimal
-still needs to be monitored

Coronary Heart Disease Heart disease due to impaired coronary blood flow,
usually d/t atherosclerosis
-stable plaque (usually leads to ischemia/angina)
-unstable plaque (often leads to MI)
CHD (MIs, heart failure, etc) is the leading cause of death in the United States for men and women
Projected costs of CHD in 2010: 316.4 billion (direct and indirect) (CDC data)

Coronary Arteries

An Oxygen Problem The balance between myocardial oxygen supply and
demand must be maintained!
Demand influenced by: HR, contractility, muscle mass, ventricular wall tension (afterload)
Supply influenced by: coronary blood flow, O2 carrying capacity, vascular resistance
Remember that blood flow (perfusion) is necessary for oxygen delivery
Effect of reduced oxygen: ischemia
Effect of absent/acute lack of oxygen: infarction

Myocardial Ischemia Ischemia occurs when O2 demand is greater
than supply
O2 shortage forces myocardium to use anaerobic metabolism -> pain (angina pectoris)
Mild increases in HR and BP usually occur before chest pain – the SNS is compensating
Possible EKG changes
All changes are reversible if O2 supply is restored

Angina Pectoris Stable – predictable onset, pain is constricting,
pressure-like, subsides with rest or medication
Silent – ischemia without angina
Variant or vasospastic – due to spasmodic narrowing of the coronary arteries, unpredictable, often at night, often associated with cocaine use

Acute Coronary Syndromes AKA myocardial infarction, “heart attack”
Sudden blockage of one or more coronary arteries stops blood flow to a part of the myocardium
The myocardium quickly begins to die: infarction/necrosis
MIs are most common in the LV
Locations: Anterior, inferior, lateral, septal
LOCATION AND SIZE OF INFARCT DEPEND ON LOCATION OF CORONARY ARTERY BLOCKAGE

Signs and Symptoms of an MI Angina pectoris, chest pressure, possibly
radiating down left arm
Diaphoresis
Nausea
Women often experience non-traditional symptoms!

Diagnosis of an MI Blood markers: cardiac enzymes (troponin)
EKG changes (ST elevation – “STEMI”)
Cardiac catheterization
Treatment:
-medications
-reperfusion (usually angioplasty and/or stent)

Myocardial InfarctionLeft main
coronary
artery
Left anterior
descending
coronary
artery (LAD)

Zones of necrosis and ischemia

Effects of an MI Reduced contractility & compliance
Abnormal wall motion
Reduced SV & EF
dysrhythmias
These changes combine to depress overall ventricular function
Severity depends on:
-function of the uninvolved myocardium
-collateral circulation
-general compensation of the cardiovascular system
Compensatory Mechanisms SNS will react to < CO and cause vasoconstriction of
systemic arteries and veins
SNS also causes > HR and > contractility (HR and BP usually maintained)
Kidneys retain Na and water
The increased preload increases ventricular contractility to a point (Frank Starling)
The body’s compensations for decreased ventricular function are limited
The ventricles (LV) gradually dilate and hypertrophy due to increased volume and workload

Worst-Case Scenario Outcomes Cardiogenic shock – when MI affects > 40% of LV, the
severe drop in systemic and cardiac circulation causes death
Papillary muscle rupture – usually affects mitral valve
Cardiac rupture – the necrotic area of the ventricle wall ruptures, leads to massive bleeding into pericardium
MIs often result in heart failure

Myocardial Disorders All the other causes of myocardial dysfunction besides
CHD
Myocarditis: inflammation of myocardium, usually d/t infection
-wide variation of s/sx
-diagnose by EKG changes, cardiac enzymes, biopsy
Cardiomyopathies
-primary and secondary
-dilated, hypertrophic, restrictive
Hypertrophic Cardiomyopathies(HCM) Ventricular wall enlargement “enlarged heart”, walls
become stiff and less compliant -> heart failure
Common in young adults, cause of sudden cardiac death
A primary type of cardiomyopathy, genetic
Variation in S/sx and prognosis
-dyspnea, chest pain, fatigue – worse with exertion
-arrhythmias
Medication and surgical treatments

Dilated Cardiomyopathies(DCM) Pathogenesis: a gradual enlargement (dilation) of the
ventricle chambers (left ventricle) -> heart failure EF drops to 40% or lower A primary type of cardiomyopathy, caused by:
-infectious myocarditis-alcohol/drug abuse-NMS diseases-genetic, idiopathic
S/sx: dyspnea on exertion (DOE), othopnea, weakness, edema, dysrhythmias
Treatment focuses on preventing further damage, maintaining heart function, possible transplant


Infective Endocarditis Rare but life-threatening
Often d/t bacteria that invade the endocardium and valves -> common cause of valve disorders
Staphylococci, streptococci, enterococci
Requires an already-damaged endocardium and an organism gaining entry into the circulatory system
Vegetations often develop on heart valves
Pt may have systemic infection s/sx, heart murmur
Risk factors: heart disease, IV drug use
Diagnose with blood cultures, echo

Acute Rheumatic Fever Multisystem inflammatory disease that may occur
after group A β-hemolytic streptococcal pharyngitis
Theory is that the infection causes a systemic autoimmune response
Rheumatic Heart Disease (RHD) is the cardiac manifestation of RF, may involve all three layers of the heart
Autoantibodies react with host tissue – cause damage to the valves, both stenosis and regurgitation
Progression is gradual

Valvular Heart Disease A problem with any of the four heart valves creates
abnormal blood flow and increases cardiac work
Normal valves allow unidirectional and unimpededblood flow
Regurgitation: valve doesn’t close properly and allows backflow – creates volume work
Stenosis: valve opening is restricted, preventing forward flow – creates pressure work
Both problems can occur together in the same valve
Regurg or stensosis cause murmurs

Pathogenesis of Valve Disease Destruction by infective endocarditis (ex: rheumatic
fever)
Connective tissue defects
Rupture of papillary muscles
Damage from an MI
Congenital malformations (mitral valve prolapse)
Mitral and aortic valves most commonly affected
Manifestation variables: valve involved, severity of damage, rapidity of onset, any compensatory mechanisms

Mitral Valve Stenosis Resistance to blood flow from LA->LV, LA must
work harder
Pressure from LA backs up into pulmonary circulation, pulmonary pressures rise
Increased pressure may travel through pulmonary system to the RV -> RV hypertrophy -> R heart failure
Sx appear at ~50% stenosis
Increasing exertional dyspnea, tachycardia, atrial dysrhythmias

Mitral Regurgitation During systole, some blood flows backward into LA
instead of all moving forward through aortic valve
Causes: RHD, mitral valve prolapse
LA dilates to accommodate backflow, eventually fails and pressures in pulmonary circuit rise -> L heart failure
LV will become dilated and hypertrophied
Acute mitral regurg usually fatal

Aortic Stenosis Narrowed aortic valve obstructs blood flow into aorta
from LV during systole
Pressure work -> LV hypertrophy
Compensation works for a while
Sx begin at ~50% narrowing
Angina, syncope, LV failure
Loud systolic murmur
Onset of sx: 5 year survival
Usually fatal before causing right heart failure