
11,12
57
Inflammation. Etiology. Vascular changes. Cellular events in inflammation. Acute inflammation. Morphologic patterns.
Transcript of 11,12
Inflammation. Etiology. Vascular changes. Cellular events in inflammation.
Acute inflammation. Morphologic
patterns.
Questions Inflammation. Definition. Basis. Etiology
and pathogenesis. Nomenclature. Acute inflammation: tissue response.
Mediators in acute inflammation. Type of cells in the focus of acute
inflammation. Consequences of acute inflammation.
Patterns of acute inflammation.

Inflammation A protective response intended to
eliminate the initial cause of cell injury as well as the necrotic cells and tissues resulting from the original insult.
Inflammation is a beneficial host response to foreign invaders and necrotic tissue, but it is itself capable of causing tissue damage.

General Features of Inflammation
The main components of inflammation are a vascular reaction and a cellular response, activated by mediators that are derived from plasma proteins and various cells.
The phases of the inflammatory process are: Tissue injury, degeneration and necrosis Acute inflammation Inactivation and removal of the agent
Restitutio (repair) Scar /chronic inflammation

Inflammation
Acute inflammation rapid in onset and of short duration, lasting up to few
days characterized by fluid and plasma protein exudation
and predominantly neutrophilic leukocyte accumulation
= exudative inflammation
Chronic inflammation longer duration (days to years) characterized by lymphocytes and macrophages influx
and vascular proliferation and fibrosis (scarring) = productive inflammation

Acute inflammation
The external manifestations of inflammation, often called its cardinal signs, result from the vascular changes and cell recruitment: heat (calor), redness (rubor), and swelling (tumor). pain (dolor) and loss of function (functio laesa)

Causes of acute inflammation
Microbial infections pyogenic bacteria, viruses
Hypersensitivity reactions parasites, tubercle bacilli
Physical agents trauma, ionising radiation, heat, cold
Chemicals corrosives, acids, alkalis, reducing agents,
bacterial toxins Tissue necrosis
ischaemic infarction

Inflammation /Nomenclature
Related to organ localization + itis Pleura –pleuritis Myocardium – myocarditis Cystis – cystitis
Exceptions Pneumonia, angina

ACUTE INFLAMMATION Acute inflammation is a
rapid response to injury or microbes and other foreign substances that is designed to deliver leukocytes and plasma proteins to sites of injury.
The principal leukocytes in acute inflammation are neutrophils (polymorphonuclear leukocytes).
Granulocytes, Neutrophilic granulocytesPolymorph

Role of the neutrophil polymorph
The neutrophil polymorphs = acute inflammatory infiltrate Movement Adhesion to micro-organisms Phagocytosis Intracellular killing of micro-
organisms Oxygen-dependent
mechanisms –RAS Oxygen-independent
mechanisms

ACUTE INFLAMMATION Acute inflammation has 3
major components: Vascular changes:
alterations in vessel caliber resulting in increased blood flow (vasodilation) and (increased vascular permeability).
Cellular events: emigration of the leukocytes from
the microcirculation and accumulation in the focus of injury (cellular recruitment and activation).
Mediators, derived from plasma proteins and cells

Vascular Reactions in Acute Inflammation
Vasoconstriction (for seconds) Vasodilation is induced by chemical
mediators such as histamine is the cause of erythema and stasis of blood flow.
Increased vascular permeability by histamine, kinins and other mediators that
produce gaps between endothelial cells, by direct or leukocyte-induced endothelial injury,
and by increased passage of fluids through the
endothelium

Exudates
Exudates increased vascular permeability allows
plasma proteins and leukocytes to enter sites of infection or tissue damage;
fluid leak through blood vessels results in edema.
Exudates v/s transudates Exudate - in inflammation because of
increased vascular permeability as a result of increased interendothelial spaces.
Transudates - when fluid leaks out because of increased hydrostatic pressure or decreased osmotic pressure.

Responses of Lymphatic Vessels
In inflammation, lymph flow is increased and helps drain edema fluid from the extravascular space
In severe inflammatory reactions, especially to microbes, the lymphatics may transport the offending agent. lymphangitis and lymphadenitis
Inflamed lymph nodes are often enlarged, because of hyperplasia of the lymphoid follicles and increased numbers of lymphocytes and phagocytic cells lining the sinuses of the lymph nodes = reactive, or inflammatory, lymphadenitis.
For clinicians, the presence of red streaks near a skin wound is a sign of an infection in the wound.

Cellular Events Leukocyte Recruitment
Leukocytes are recruited from the blood into the extravascular tissue to the site of infection or tissue injury, and are activated.
Leukocyte Activation- to perform their functions ingest offending agents, kill bacteria and other microbes,
and eliminate necrotic tissue and foreign substances. they may induce tissue damage and prolong
inflammation, since the leukocyte products that destroy microbes can also injure normal host tissues.
key to the normal function of leukocytes in host defense is to ensure that they are recruited and activated only when needed

Leukocyte Recruitment – a multiple steps
process Margination, adhesion, and rolling along the vessel wall Firm adhesion to the endothelium Transmigration between endothelial cells; Migration in interstitial tissues toward a chemotactic
stimulus mediated by the binding of complementary adhesion molecules on
leukocytes and endothelial surfaces – selectins, integrins Chemical mediators-chemoattractants

Leukocyte Activation
Stimuli for activation microbes, products of necrotic cells, and
several mediators opsonization
components of the microbes and dead cells, or host proteins, (opsonins), that coat microbes and target them for phagocytosis
Leu express on their surface different kinds of receptors
receptors for opsonins that facilitate rapid phagocytosis of the coated microbes
Fc receptor for IgG, complement receptors 1 and 3, and C1q (collectins).

Leukocyte Activation Stimuli for activation
microbes, products of necrotic cells, and several mediators
Leu express on their surface different kinds of receptors and engagement of these receptors by microbial products or by various mediators of inflammation induces leukocyte activation
Leukocyte functions: Phagocytosis of particles
an early step in the elimination of harmful substances. Production of substances that destroy phagocytosed
microbes and remove dead tissues lysosomal enzymes and reactive oxygen and nitrogen
species. Production of mediators that amplify the
inflammatory reaction- arachidonic acid metabolites, cytokines.

Leukocyte Effector Mechanisms
The culmination of the phagocytosis of microbes is killing and degradation of the ingested particles. Destruction is caused by free radicals (ROS,
NO) and lysosomal enzymes leukocyte NADPH oxidase (phagocyte oxidase) -
superoxide ion and hydrogen peroxide lysosomes of neutrophils (called azurophilic
granules) -enzyme myeloperoxidase (MPO) - hypochlorous radical.
Enzymes and ROS may damage normal tissues

CHEMICAL MEDIATORS OF INFLAMMATION
Cell-derived mediators - produced locally by cells at the site of inflammation
In intracellular granules and are rapidly secreted upon cellular activation (e.g., histamine in mast cells) or are synthesized de novo in response to a stimulus (e.g., prostaglandins and cytokines).
Plasma-protein-derived mediators- circulating in the plasma (typically synthesized by the liver) as inactive precursors that are activated at the site of inflammation
complement proteins, kinins, which undergo proteolytic cleavage to acquire their biologic activities.
Once activated and released from the cell, mediators are inactivated by enzymes, eliminated or inhibited

The principal chemical mediators of inflammation
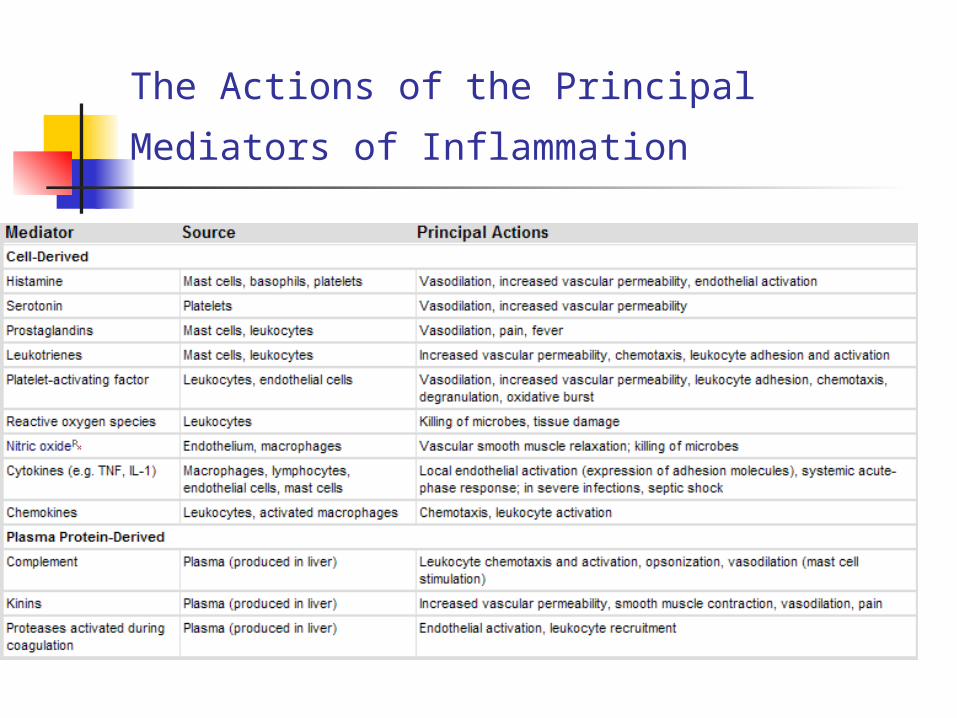
The Actions of the Principal Mediators of
Inflammation

Major Cell-derived Mediators of Inflammation
Vasoactive amines -histamine, serotonin main effects vasodilation and increased vascular permeability
Arachidonic acid metabolites -prostaglandins and leukotrienes-derived from cell membrane phospholipids
involved in vascular reactions, leukocyte chemotaxis, and other reactions of inflammation; antagonized by lipoxins
Cytokines -proteins produced by many cell types (TNF, IL-1, chemokines)
mediate multiple effects -leukocyte recruitment and migration; Reactive oxygen species (O2, superoxide, H2O2, peroxide, OH-,
hydroxyl radical)-released from neutrophils and macrophages
role in microbial killing, tissue injury Nitric oxide
vasodilation, microbial killing Lysosomal enzymes –myeloperoxidase, lysozyme (bact.), acid
hydrolases, lactoferrin, lysozyme, alkaline phosphatase, proteases – collagenase, elastases
neutrophils and monocytes role in microbial killing, tissue injury

HISTAMINE
Mast Cells, basophils Powerful
vasodilatator Vasoactive “amine”
inceases vascular permeability

SEROTONIN
5HT, 5-Hydroxy-Tryptamine)
Platelets and Enterochromaffin Cells
Vasoactive mediator, with effects similar to those of histamine
Evokes NO synthetase

Arachidonic Acid (AA) Metabolites(EICOSANOIDS)
Affect a variety of biologic processes, including inflammation and hemostasis.
Leukocytes, mast cells, endothelial cells, and platelets are the major sources of AA metabolites in inflammation.
= Products derived from the metabolism of AA AA is a 20-carbon polyunsaturated fatty acid, a
component of cell membrane phospholipids. It is released from these phospholipids via cellular
phospholipases, activated by mechanical, chemical, or physical stimuli, or by inflammatory mediators (C5a).
AA metabolism - 2 enzymatic pathways: Cyclooxygenase prostaglandins and thromboxanes, lipoxygenase leukotrienes and lipoxins

Arachidonic Acid (AA) Metabolites
(EICOSANOIDS)
Effects Prostaglandins, thromboxanes
Pain, fever, clotting Leukotrienes
Chemotaxis, vasoconstriction, increased Permeability
Lipoxins Inhibit chemotaxis, vasodilatation,
counteract actions of leukotrienes

Platelet-Activating Factor (PAF)
It is generated from the membrane phospholipids of many cells
• neutrophils, monocytes, basophils, endothelial cells, and platelets
Activate platelets Vasoconstriction and
bronchoconstriction Vasodilation and increased
vascular permeability

CYTOKINES/CHEMOKINES
Proteins produced by many cells – TNFα, IL-1,interferon-γ (IFN-γ) Lymphocytes, macrophages.
Numerous roles in acute and chronic inflammation
CHEMOKINES are small proteins (>40)
act primarily as chemoattractants for different subsets of leukocytes

FREE RADICALS
Synthesized via the NADPH oxidase (phagocyte oxidase) pathway and are released from neutrophils and macrophages
O2 – (SUPEROXIDE) H2O2 (PEROXIDE) OH- (HYDROXYL RADICAL)
Very destructive within lysosomes they function to destroy phagocytosed
microbes and necrotic cells At higher levels -responsible for tissue injury

NITRIC OXIDE
Synthesized from arginine by endothelial cells (type
III nitric oxide synthase, eNOS)
by macrophages (type II NO synthase,iNOS)
Effects Vasodilation
reduces platelet and leukocyte adhesion
NO produced in phagocytes is cytotoxic to microbes.

Lysosomal enzymes The lysosomal granules of neutrophils and
monocytes contain many molecules that can mediate acute inflammation.
Myeloperoxidase Lysozyme (Bact.) Acid Hydrolases Lactoferrin Lysozyme Alkaline Phosphatase Proteases – collagenase, elastases
The potentially damaging effects of lysosomal enzymes are checked by antiproteases present in the serum and tissue fluids-α1-antitrypsin, α2-macroglobulin.

Plasma Protein-Derived Mediators of Inflammation
Complement proteins, >20 proteins
Coagulation proteins Activated factor XII triggers the clotting, kinin
and complement cascades, and activates the fibrinolytic system, production of fibrin
Kinins (bradykinin) Produced by proteolytic cleavage of precursors; increased permeability, Smooth muscle
contraction (non vascular), pain
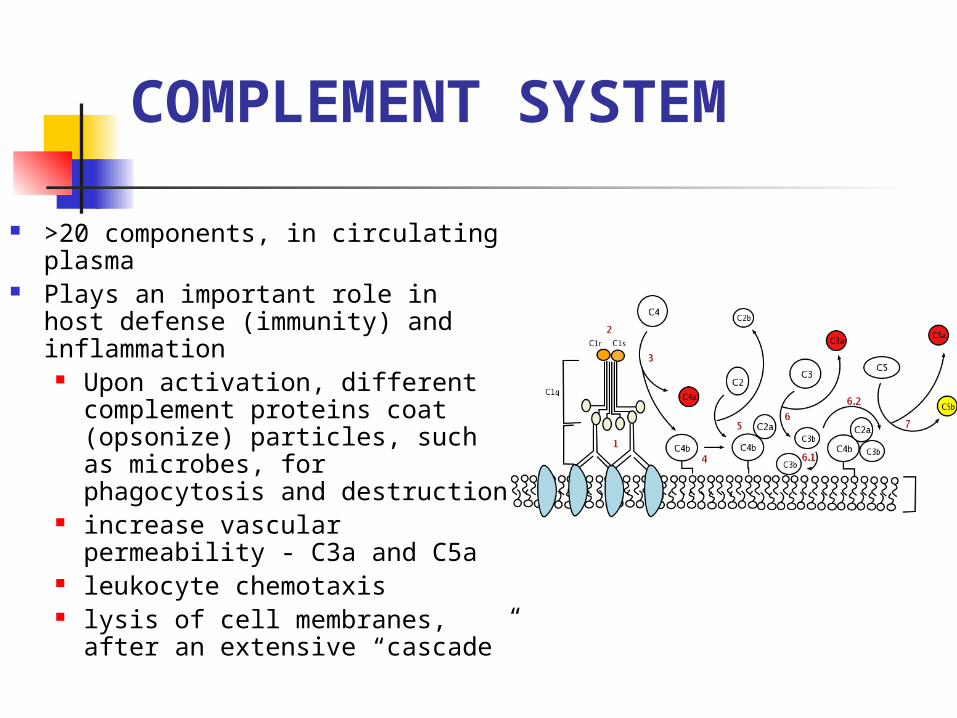
COMPLEMENT SYSTEM
>20 components, in circulating plasma
Plays an important role in host defense (immunity) and inflammation
Upon activation, different complement proteins coat (opsonize) particles, such as microbes, for phagocytosis and destruction
increase vascular permeability - C3a and C5a
leukocyte chemotaxis lysis of cell membranes, after
an extensive “cascade”

Outcomes of acute inflammation
Resolution, Healing by
scarring (fibrosis), Chronic
inflammation
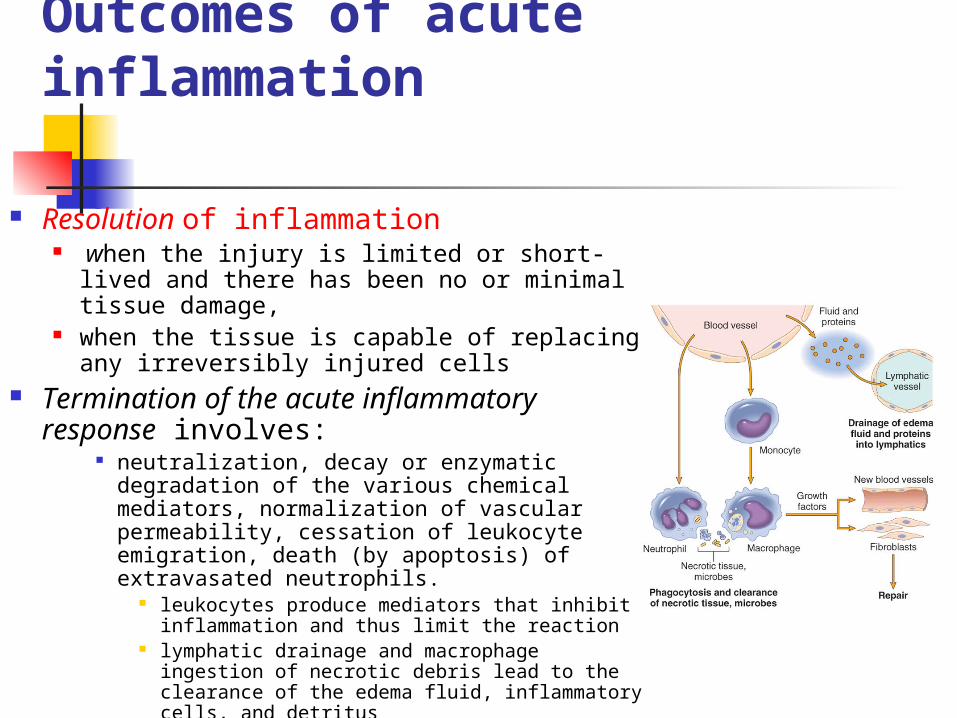
Outcomes of acute inflammation
Resolution of inflammation when the injury is limited or short-lived
and there has been no or minimal tissue damage,
when the tissue is capable of replacing any irreversibly injured cells
Termination of the acute inflammatory response involves:
neutralization, decay or enzymatic degradation of the various chemical mediators, normalization of vascular permeability, cessation of leukocyte emigration, death (by apoptosis) of extravasated neutrophils.
leukocytes produce mediators that inhibit inflammation and thus limit the reaction
lymphatic drainage and macrophage ingestion of necrotic debris lead to the clearance of the edema fluid, inflammatory cells, and detritus

Outcomes of Acute Inflammation
Progression to chronic inflammation - if the offending agent is not removed In some instances, signs of chronic inflammation
may be present at the onset of injury (e.g., in viral infections or immune responses to self-antigens).
Scarring or fibrosis - after substantial tissue destruction or when inflammation occurs in tissues that do not regenerate. Extensive fibrinous exudates may not be completely
absorbed and are organized by ingrowth of connective tissue, with resultant fibrosis.
The usual outcome of abscess formation is scarring because of the underlying tissue destruction

ACUTE INFLAMMATION-Summary
Initial reaction of tissue to injury Vascular component: dilatation of vessels Exudative component: vascular leakage
of protein-rich fluid Neutrophil polymorph -the characteristic
cell recruited to the tissue Outcome - resolution, suppuration (e.g.
abscess), organisation, or progression to chronic inflammation

Morphologic patterns of acute inflammation

MORPHOLOGIC PATTERNS OF ACUTE INFLAMMATION
Distinctive morphologic patterns depend on: the severity of the inflammatory response, its
specific cause and the particular tissue Serous inflammation Catarrhal inflammation Fibrinous inflammation Haemorrhagic inflammation Suppurative (purulent) inflammation Putrefactive (gangrenous) inflammation
Importance to know the morphologic patterns often associated with different eliciting stimuli and
clinical situations.

Serous inflammation Characterized by the outpouring of a watery,
relatively protein and cells-poor fluid Depending on the site of injury, the fluid derives
either from the serum or from the secretions of mesothelial cells lining the peritoneal, pleural, and pericardial cavities.
Location Skin - viruses Mesothelial linings (serosa) of peritoneal, pleural,
and pericardial cavities Fluid in a serous cavity is called an effusion
Mucosa of GIT, respiratory tract (rhinitis) Catarrhal inflammation – mucous + epithelial cells
Liver, myocardium

Serous inflammation Skin blister -from a burn or
viral infection a serous effusion
accumulated either within or immediately beneath the epidermis of the skin
Outcome of serous inflammation
Recovery Exceptions
Serous meningitis Cholera - dehydratation burns

Fibrinous inflammation Occurs as a consequence of more severe
injuries, resulting in greater vascular permeability and the exudate is rich of fibrinogen converts to fibrin
Location Serous cavities
Pericarditis, pleuritis, peritonitis Mucosa of respiratory tract
Diphtheria of the larynx Lobar pneumonia –alveoli
Mucosa of gastrointestinal tract Histologically, the accumulated
extravascular fibrin appears as an eosinophilic meshwork of threads
Cor villosum Weigert staining– violet-blue reaction

Fibrinous inflammation
Two types Superficial – easy removing of fibrin,
without loss of tissue Serous cavities Lobar pneumonia (crupousa) Diphtheria of larynx
Deep –pseudomembraneous, necrosis of sub lying epithelium
Diphtheria of tonsils C. difficile

Pneumonia crouposa

Pericarditis fibrinosa

Pleuritis fibrinosa

Outcome of fibrinous inflammation
Resolution exudates may be degraded by fibrinolysis, and the
accumulated debris may be removed by macrophages, resulting in restoration of the normal tissue structure
Organization the failure to completely remove the fibrin results in the
ingrowth of fibroblasts and blood vessels, leading ultimately to scarring that may have significant clinical consequences
organization of a fibrinous pericardial exudate forms dense fibrous scar tissue that bridges or obliterates the pericardial space and restricts myocardial function
Pneumonia crouposa – carnification, pneumosclerosis Death
Diphtheria of larynx – asphyxia Intoxication – peritonitis, pneumonia crouposa

Suppurative (purulent) inflammation
Characterized by the presence of large amounts of purulent exudate (pus) consisting of neutrophils, macrophages, necrotic cells, and edema fluid
Yellowish colour to grey Staphylococci induce most often suppuration =
pyogenic. Two types
Local (focal collections of pus) – abscesses Directly, by seeding of pyogenic organisms into a tissue
hair follicle - fulunculus, carbunculus Ductullar way - bronchi, bile ducts Hemaetogenic- several organs
by secondary infections (suppuration) Diffuse – phlegmone
No localization of the suppuration, neutrophils + tissue decay Adipose tissue-panniculitis
Empyema – in cavities Gall bladder, pleura

Bronchopneumonia
Purulent inflammation. A, Multiple bacterial abscesses in the lung B. The abscess contains neutrophils and cellular debris, and is surrounded by congested blood vessels.

Pneumonia lobularis

Nephritis purulenta

Leptomeningitis purulenta
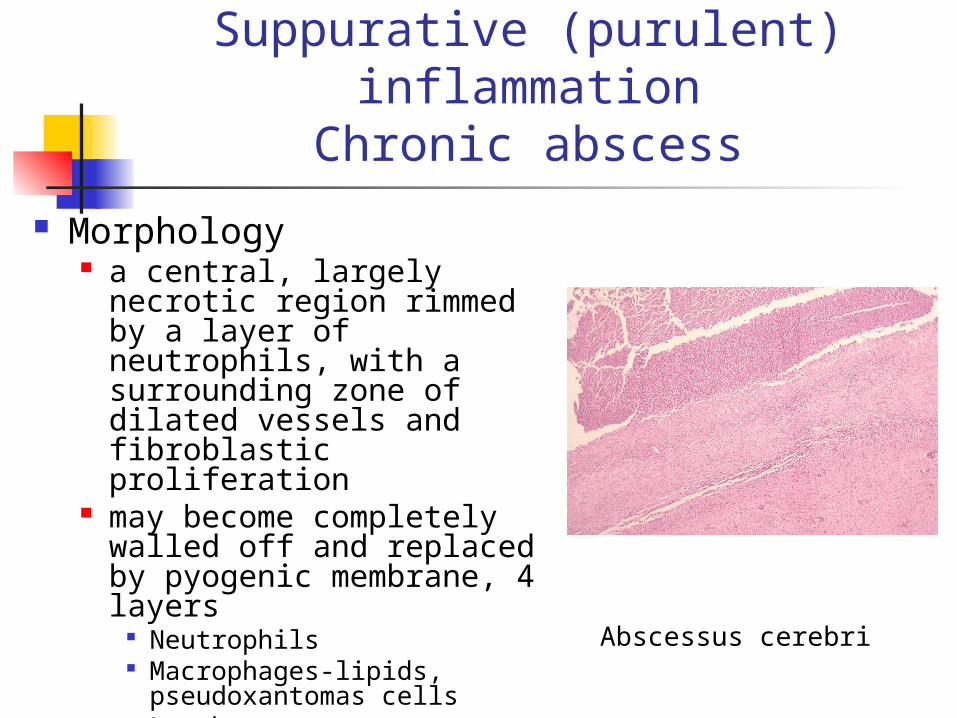
Suppurative (purulent) inflammation
Chronic abscess
Morphology a central, largely necrotic
region rimmed by a layer of neutrophils, with a surrounding zone of dilated vessels and fibroblastic proliferation
may become completely walled off and replaced by pyogenic membrane, 4 layers
Neutrophils Macrophages-lipids,
pseudoxantomas cells Lymphocytes connective tissue capsule
Abscessus cerebri
Outcome of suppurative inflammation
Local factors Bile stasis, lithiasis
General condition of the patient immunity diabetes
Local effects Break in the cavities
Suppurative peritonitis Systemic effects-generalization of the
inflammation Sepsis
Pyaemia-multiple abscesses

Haemorrhagic inflammation
Characterized by increased erythodiapedesis due to vascular wall injury
Often combined fibrinohaemorrhagic Vasotropic agents- viruses
Grippe – rhinitis, tracheitis, pharyngitis hemorrhagic fever Pestis Anthrax
Impaired coagulation Thrombocytopenia Vit C

Ulcerative inflammation An ulcer is a local defect (or
excavation), of the surface of an organ or tissue -necrotic tissue
Ulceration can occur only when tissue necrosis and inflammation exist on or near a surface:
inflammatory necrosis of the mucosa of the mouth, stomach, intestines, or genitourinary tract;
tissue necrosis and subcutaneous inflammation of the lower extremities
Peptic ulcer of the stomach, duodenum - acute and chronic inflammation coexist.
acute stage - intense polymorphonuclear infiltration and vascular dilation in the margins of the defect.
Chronic stage - the margins and base of the ulcer develop scarring with accumulation of lymphocytes, macrophages, and plasma cells.


















![Design of Computer Integrated Manufacturing …mpmpjournal.iaun.ac.ir/article_558243_369e11b06fe...following 3 categories [11,12] : 1) Stand-alone systems, such as machining centers](https://static.fdocuments.in/doc/165x107/5ed1aea1ef23f6521d32737c/design-of-computer-integrated-manufacturing-following-3-categories-1112-.jpg)