1 Pandemic Flu H1N1 Terry L Dwelle MD MPHTM CPH FAAP.
64
1 Pandemic Flu Pandemic Flu H1N1 H1N1 Terry L Dwelle MD MPHTM Terry L Dwelle MD MPHTM CPH FAAP CPH FAAP
-
Upload
nicholas-campbell -
Category
Documents
-
view
214 -
download
0
Transcript of 1 Pandemic Flu H1N1 Terry L Dwelle MD MPHTM CPH FAAP.
1
Pandemic FluPandemic FluH1N1H1N1
Terry L Dwelle MD MPHTM Terry L Dwelle MD MPHTM CPH FAAPCPH FAAP

2
Pandemic Influenza – General Pandemic Influenza – General InformationInformation
Pandemic is a worldwide epidemicWe can expect several pandemics in
the 21st century

3
H1N1 (Swine Origin Influenza H1N1 (Swine Origin Influenza Virus)Virus)
33,902 cases in the US (estimate is that there have been 1 million cases in the US)
3663 hospitalizations (10.8%, 0.36% of estimated cases in the US) 170 deaths (0.5% of identified cases and 4.6% of those hospitalized,
0.017% of estimated cases in the US) Genetically this H1N1 is linked to the 1918-19 strain Currently we are seeing almost totally H1N1 circulating Majority of the cases are in children and young adults Majority of hospitalized patients have underlying conditions (asthma
being the most common, others include chronic lung disease, DM, morbid obesity, neurocognitive problems in children and pregnancy).
There have been over 50 outbreaks in camps Southern hemisphere – currently seeing substantial disease from
H1N1 that is cocirculating with seasonal influenza. There has been some strain on the health systems in some situations.
About 30% of infected individuals are asymptomatic (study from Peru)
4
H1N1 in PregnancyH1N1 in PregnancyApril 15 to May 18, 2009 – 34 confirmed or April 15 to May 18, 2009 – 34 confirmed or
probable cases of H1N1 in pregnant probable cases of H1N1 in pregnant women reported to the CDCwomen reported to the CDC
11/34 (32%) were admitted to hospital11/34 (32%) were admitted to hospitalGeneral population hospitalization rate General population hospitalization rate
7.6%7.6%6 deaths – pneumonia and acute 6 deaths – pneumonia and acute
respiratory distress syndromerespiratory distress syndromePromptly treat pregnant women with Promptly treat pregnant women with
H1N1 infection with antiviralsH1N1 infection with antivirals
Lancet on line, July 29, 2009
5
Pandemic Influenza - ImpactPandemic Influenza - Impact
A moderate pandemic may exceed A moderate pandemic may exceed the capacity of hospitals to provide the capacity of hospitals to provide inpatient careinpatient care
6
Pandemic Influenza - Pandemic Influenza - EpidemiologyEpidemiology
Pandemics occur in waves Pandemics occur in waves The order in which communities will be The order in which communities will be
affected will likely be erraticaffected will likely be erratic Some individuals will be asymptomatically Some individuals will be asymptomatically
infectedinfected A person is most infectious just prior to A person is most infectious just prior to
symptom onsetsymptom onset Influenza is likely spread most efficiently by Influenza is likely spread most efficiently by
cough or sneeze droplets from an infected cough or sneeze droplets from an infected person to others within a 3 foot circumferenceperson to others within a 3 foot circumference
7
Pandemic Influenza - Pandemic Influenza - ResponseResponseWe don’t look at pandemic flu as a We don’t look at pandemic flu as a
separate disease to be dealt with in a separate disease to be dealt with in a different way from regular seasonal different way from regular seasonal influenzainfluenza
Influenza response toolboxInfluenza response toolboxSocial distancing and infection control measureSocial distancing and infection control measureVaccineVaccineAntiviral medicationsAntiviral medications
The most effective way to prevent The most effective way to prevent mortality is by social distancingmortality is by social distancing
8
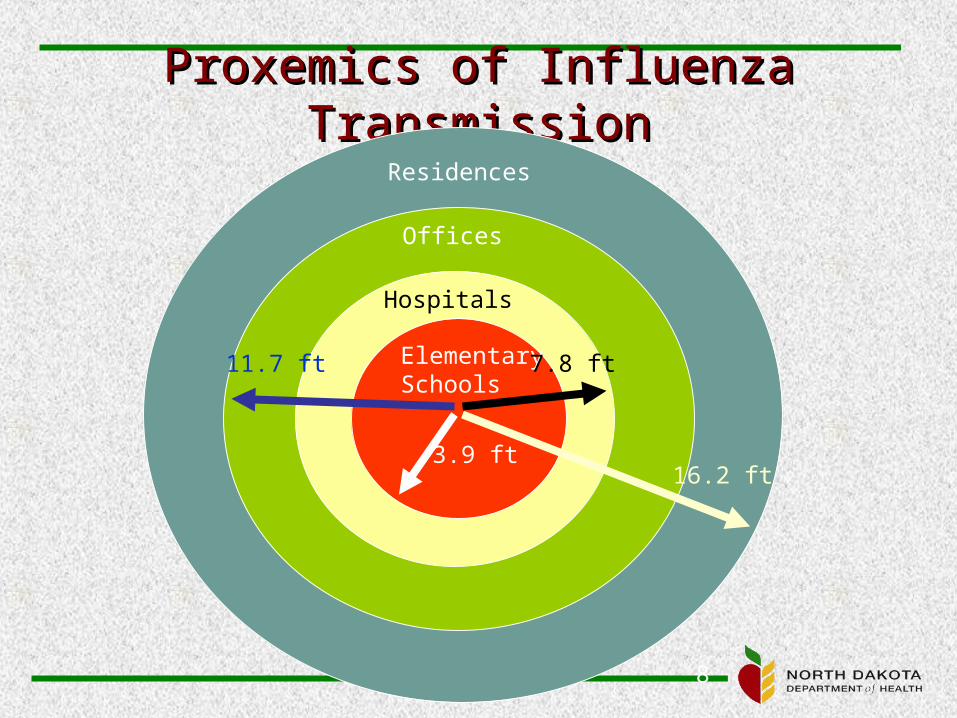
Proxemics of Influenza Proxemics of Influenza TransmissionTransmission
Elementary Schools
Hospitals
Offices
Residences
3.9 ft
7.8 ft11.7 ft
16.2 ft

9
Goals of Influenza PlanningGoals of Influenza Planning
-20
0
20
40
60
80
100
120
5 10 15 20 25 30 35 40 45 50 55 60
No Intervention
With InterventionCases
Day
Goals•Delay outbreak peak•Decompress peak burden on hospitals and infrastructure•Diminish overall cases and health impacts
10
IsolationIsolation From From
www.cdc.gov/h1n1flu/guidance_homecare.htm
Data from 2009Data from 2009Most fevers lasted 2-4 daysMost fevers lasted 2-4 days90% of household transmissions occurred within 5 90% of household transmissions occurred within 5
days of onset of symptoms in the 1days of onset of symptoms in the 1stst case caseRequires 3-5 days of isolation (different from the 7 Requires 3-5 days of isolation (different from the 7
days previously used for influenza). The rule here days previously used for influenza). The rule here is isolation for 24 hours after resolution of the fever is isolation for 24 hours after resolution of the fever without the use of fever-reducing medications.without the use of fever-reducing medications.
Consider closing a school or business for a Consider closing a school or business for a minimum of 5 days which should move the minimum of 5 days which should move the infected into the area of much lower nasal infected into the area of much lower nasal shedding and contagion. shedding and contagion.

11
Unstressed Hospital and Clinic Unstressed Hospital and Clinic Surge North DakotaSurge North Dakota
8.36
4.18
2.792.09
1.67
0
1
2
3
4
5
6
7
8
9
10 20 30 40 50
100% CapHosp / ILI
Regional ILI rate
Clinic Caution 16.5
Clinic Crisis 21
X
12
Pan Flu AntiviralsPan Flu Antivirals
Terry L Dwelle MD MPTHM Terry L Dwelle MD MPTHM CPH FAAPCPH FAAP
13
Intervention - AntiviralsIntervention - Antivirals
Antivirals (Tamiflu and Relenza) will be used primarily for treatment not prophylaxisND will have approximately 160,000 treatment
courses available for a pandemic (25% of the population)
Distribution flowNormalNormal + Supplementation (from the state
cache, some prepositioned with LPHU’s) Points of Distribution
14
Antiviral Treatment – H1N1Antiviral Treatment – H1N1
Sensitive to zanamivir (Relenza) and oseltamivir Tamilflu but resistant to amantadine and rimantadine
Some circulating seasonal Influ A viruses may be resistant to oseltamivir – consider combination treatment with oseltamivir and amantidine or rimantidine
Uncomplicated febrile illness due to H1N1 does not require treatment
Treatment is recommended forAll hospitalized patients with confirmed, probable or
suspected H1N1High risk patients for complicationswww.cdc.gov/h1n1flu/recommendations.htm
15
High risk groups for High risk groups for complicationscomplications
< 5yo (highest risk is < 2yo)< 5yo (highest risk is < 2yo) Adults Adults >> 65yo 65yo Persons with the following conditionsPersons with the following conditions
AsthmaAsthma Other chronic pulmonary diseasesOther chronic pulmonary diseases Cardiovascular disease (except hypertension)Cardiovascular disease (except hypertension) Renal, hepatic, hematological (including sickle cell disease), Renal, hepatic, hematological (including sickle cell disease),
neurologic, neuromuscular, metabolic (including diabetes neurologic, neuromuscular, metabolic (including diabetes mellitus)mellitus)
Immunosuppression including that caused by medication or Immunosuppression including that caused by medication or by HIVby HIV
Pregnant womenPregnant women < 19yo receiving long-term aspirin therapy< 19yo receiving long-term aspirin therapy Residents of nursing homes and other chronic care facilitiesResidents of nursing homes and other chronic care facilities
www.cdc.gov/h1n1flu/recommendations.htm
16
Treatment guidanceTreatment guidance
Start treatment as soon as possible Start treatment as soon as possible after onset of symptoms after onset of symptoms Best if started before 48 hours from Sx Best if started before 48 hours from Sx
onsetonsetStill may be some benefit in Rx after 48 Still may be some benefit in Rx after 48
hourshoursDuration – 5 daysDuration – 5 daysDoses – H1N1 same as for seasonal fluDoses – H1N1 same as for seasonal flu
www.cdc.gov/h1n1flu/recommendations.htm
17
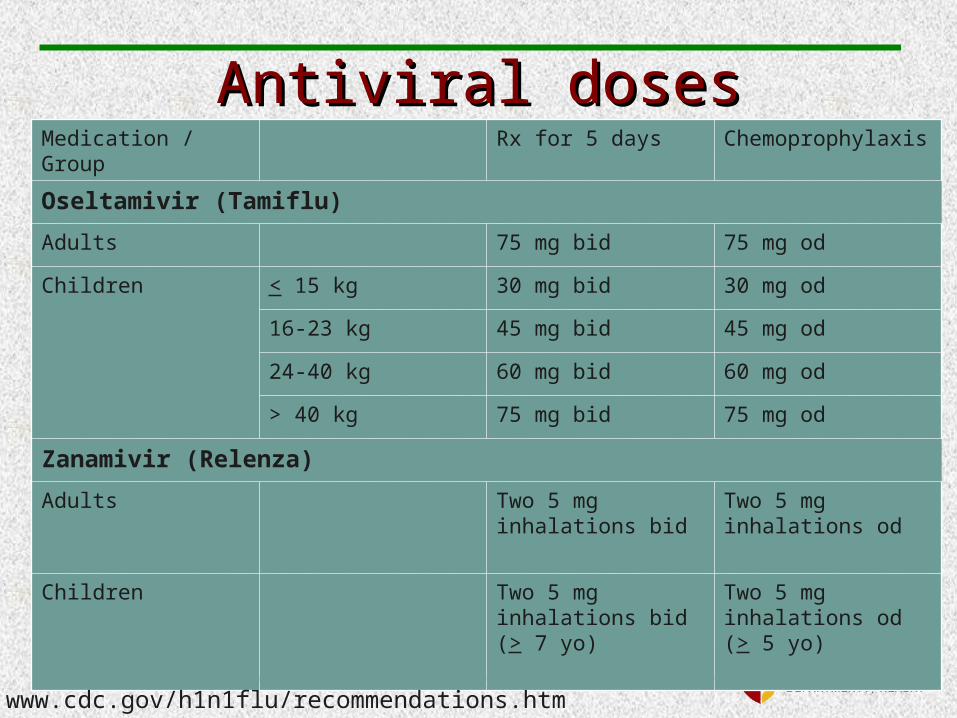
Antiviral dosesAntiviral dosesMedication / Group Rx for 5 days Chemoprophylaxis
Oseltamivir (Tamiflu)
Adults 75 mg bid 75 mg od
Children < 15 kg 30 mg bid 30 mg od
16-23 kg 45 mg bid 45 mg od
24-40 kg 60 mg bid 60 mg od
> 40 kg 75 mg bid 75 mg od
Zanamivir (Relenza)
Adults Two 5 mg inhalations bid
Two 5 mg inhalations od
Children Two 5 mg inhalations bid (> 7 yo)
Two 5 mg inhalations od (> 5 yo)
www.cdc.gov/h1n1flu/recommendations.htm
18
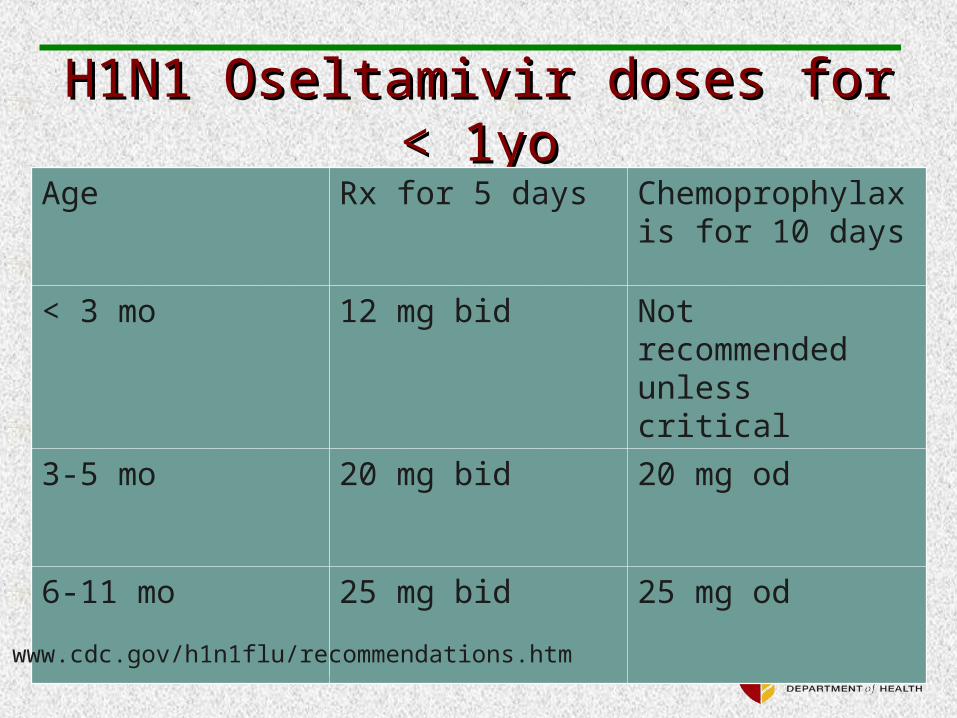
H1N1 Oseltamivir doses for < H1N1 Oseltamivir doses for < 1yo1yo
Age Rx for 5 days Chemoprophylaxis for 10 days
< 3 mo 12 mg bid Not recommended unless critical
3-5 mo 20 mg bid 20 mg od
6-11 mo 25 mg bid 25 mg od
www.cdc.gov/h1n1flu/recommendations.htm
19
ProphylaxisProphylaxisClose contact of cases (confirmed,
probable or suspected) who are at high-risk for complications
Health care personnel, public health workers, or first responders who have unprotected close contact to a case (confirmed, probable or suspect) during the infectious period (24 hours before to 24 hours after becoming afebrile)
www.cdc.gov/h1n1flu/recommendations.htm
20
Close contactClose contactCare for or live with a person who is a Care for or live with a person who is a
confirmed, probable or suspect caseconfirmed, probable or suspect caseHaving been in a setting where there is Having been in a setting where there is
a high likelihood of contact with a high likelihood of contact with respiratory droplets and or other bodily respiratory droplets and or other bodily fluidsfluids
Activities like kissing, embracing, Activities like kissing, embracing, sharing of eating/drinking utensils, sharing of eating/drinking utensils, physical examination physical examination
www.cdc.gov/h1n1flu/recommendations.htm

21
Pregnant womenPregnant women
Treatment – oseltamivir preferredTreatment – oseltamivir preferredProphylaxis – zanamivir Prophylaxis – zanamivir
www.cdc.gov/h1n1flu/recommendations.htm
Vaccination StrategyVaccination Strategy
Molly Sander, MPHMolly Sander, MPH
Immunization Program Immunization Program ManagerManager

Pharmacists and VaccinationND Law 43-15-01: “Immunization
and vaccination by injection of an individual who is more than eighteen years of age, upon an order by a physician or nurse practitioner authorized to prescribe such a drug or by written protocol with a physician or nurse practitioner”

Pharmacists and Vaccination ND Rule: 61-04-11
Obtain and maintain a license to practice pharmacy issued by the North Dakota state board of pharmacy;
Successfully complete a board-approved twenty-hour course of study and examination pertaining to the administration of medications by injection…;
Obtain and maintain current certication in cardiopulmonary resuscitation or basic cardiac life support;
Complete an application process adopted by the board and provide required documentation;
Maintain continuing competency to retain the certicate of authority. A minimum of six hours of the thirty-hour requirement for continuing education, every two years, must be dedicated to this area of practice.

Pharmacists and Vaccination ND Rule: 61-04-11
Requirements of physician or nurse practitioner order for a pharmacist to administer injections. The order must be written, received electronically or if received orally be reduced to writing, and must contain at a minimum the:• Identity of the physician or nurse practitioner issuing
the order;• Identity of the patient to receive the injection;• Identity of the medication or vaccine, and dose, to
be administered; and• Date of the original order and the dates or schedule,
if any, of each subsequent administration.
Pharmacists and Vaccination ND Rule: 61-04-11
A physician or nurse practitioner may prepare a written protocol governing the administration of medications by injection with an authorized pharmacist for a specic period of time or purpose.
Notication of administration must be made to the ordering physician or nurse practitioner and other authorities as required by law and rule.
Every record, including notication, which is required to be made under this section, must be kept by the administering pharmacist and by the pharmacy when in legal possession of the drugs administered for at least two years from the date of administration.
• NDIIS
Pharmacists and VaccinationND Rule: 61-04-11
Pharmacists may administer medications by injection within a licensed North Dakota pharmacy or at a location within North Dakota specically identied in a written protocol.
The pharmacy shall maintain a current policy and procedural manual related to the administration of medications by injection.
VaccineVaccineSeparate novel H1N1 influenza
vaccine from seasonal trivalent vaccine.
45 million doses in mid-OctoberFollowed by 20 million doses per week
there after.Five manufacturers: same age
indications as seasonal vaccine.Both injectable and intranasal vaccine
will be available.Assume 2 doses required for
everyone, separated by 3 to 4 weeks.

ACIP RecommendationsACIP RecommendationsPregnant women because they are at higher
risk of complications and can potentially provide protection to infants who cannot be vaccinated;
Household contacts and caregivers for children younger than 6 months of age because younger infants are at higher risk of influenza-related complications and cannot be vaccinated. Vaccination of those in close contact with infants less than 6 months old might help protect infants by “cocooning” them from the virus;

ACIP RecommendationsACIP RecommendationsHealthcare and emergency
medical services personnel because infections among healthcare workers have been reported and this can be a potential source of infection for vulnerable patients. Also, increased absenteeism in this population could reduce healthcare system capacity; Include public health personnel
ACIP RecommendationsACIP RecommendationsAll people from 6 months through 24
years of age Children from 6 months through 18 years
of age because many cases of novel H1N1 influenza are in children and they are in close contact with each other in school and day care settings, which increases the likelihood of disease spread, and
Young adults 19 through 24 years of age because many cases of novel H1N1 influenza are in these healthy young adults and they often live, work, and study in close proximity, and they are a frequently mobile population; and,
ACIP RecommendationsACIP RecommendationsPersons aged 25 through 64 years who
have health conditions associated with higher risk of medical complications from influenza. Chronic pulmonary disease, including asthmaCardiovascular diseaseRenal, hepatic, neurological/neuromuscular, or
hematologic disordersImmunosuppressionMetabolic disorders, including diabetes mellitus
ACIP RecommendationsACIP Recommendations Once the demand for vaccine for the
prioritized groups has been met at the local level, programs and providers should also begin vaccinating everyone from the ages of 25 through 64 years.
Current studies indicate that the risk for infection among persons age 65 or older is less than the risk for younger age groups. However, once vaccine demand among younger age groups has been met, programs and providers should offer vaccination to people 65 or older.

ACIP RecommendationsACIP Recommendations If demand exceeds supply (not expected):
pregnant women, people who live with or care for children
younger than 6 months of age, health care and emergency medical
services personnel with direct patient contact,
children 6 months through 4 years of age, and
children 5 through 18 years of age who have chronic medical conditions.
DistributionDistributionH1N1 vaccine purchased from
manufacturers by the federal government.
Vaccine is allocated to states based on population.North Dakota will receive 0.208%
H1N1 vaccine will be distributed through a third party distributor (McKesson)Will also ship ancillary supplies.
• Alcohol pads, syringes, needles, sharps containers
EnrollmentEnrollmentProviders are required to sign an
enrollment form in order to receive H1N1 vaccine.CDC is creating a standardized form. It is
currently unavailable.Enrollment requirements unknown,
but most likely include:Proper storage and handling: 35 ° – 46° FFollowing of ACIP recommendationsReporting of doses administered?
Administration FeeAdministration Fee The federal government will set a
maximum administration fee.Most likely at the Medicare rate:
$18.45/dose in North Dakota. (Different than Medicaid fee cap for VFC:$13.90)
Cannot charge for the cost of the vaccine, as it is free from the federal government.
Administration fee may be billed to patient, Medicaid, Medicare, private insurance, etc.
Local public health units cannot refuse to vaccinate based on inability to pay.Private providers will probably be able to
refuse vaccination if patient is unable to pay.

NDIISThe North Dakota Immunization
Information System (NDIIS) is a confidential, population-based, computerized information system that attempts to collect vaccination data about all North Dakotans.
Healthcare providers, pharmacists, local public health units, schools, and childcares may have access to the NDIIS.

NDIISNDIISThe NDIIS will be used to track doses
administered.Similar data entry to other vaccines, but
includes high-risk groups for vaccination.
Doses administered must be reported to CDC by the state on a weekly basis.Report each Tuesday for the previous week.
Contact the NDDoH at 701.328.3386 or toll-free at 800.472.2180 if interested in obtaining access.
Strategies for VaccinationStrategies for VaccinationCheck with local public health unit
to determine local strategies.Mass Immunization ClinicsSchool Clinics:
• Recommended by CDC• Good way to capture children
Vaccination similar to seasonal influenza vaccination. (private and public mix)

Vaccine Information Statements
A VIS must be given with each dose.
2009-2010 seasonal VIS are available at www.cdc.gov/vaccines/pubs/vis/default.htm.
H1N1 VIS not yet available.
VAERS Remember to report
vaccine adverse events for both seasonal and H1N1.
http://vaers.hhs.gov/
VAERS module will be available in NDIIS.Same fields as
VAERS form.Pre-populated with
demographic and vaccine information from NDIIS.
Contact InformationContact Information
Molly Sander, MPH, Program Manager 328-4556
Abbi Pierce, MPH, Surveillance Coordinator
328-3324 Keith LoMurray,
IIS Sentinel Site Coordinator 328-2404
Tatia Hardy, VFC Coordinator 328-2035
Kim Weis, MPH, AFIX Coordinator 328-2385

Community Mitigation and
Infection Control
Kirby Kruger, State Kirby Kruger, State Epidemiologist, Division Epidemiologist, Division
DirectorDirector
of Disease Controlof Disease Control

Community MitigationCommunity Mitigation
SchoolsSchoolsChildcare settingsChildcare settingsHealthcare settingsHealthcare settingsBusinessesBusinessesGeneral PublicGeneral Public
Home careHome care

Community MitigationCommunity Mitigation
Isolation or exclusionVoluntary and passive24 hours after fever subsides and not using fever
reducing medication
Hand hygieneRespiratory etiquette
Exclusion Period - time ill people Exclusion Period - time ill people should be away from othersshould be away from others
Applies to settings in which the majority of the people are not at increased risk for complicationsGeneral public
Does NOT apply to health care settingsStaffVisitors
Antivirals not considered with exclusion
Schools Current ConditionsSchools Current Conditions
Ill staff and students to stay homeFever of ≥ 100° F with cough and/or sore throat
Ill staff and students to be separated from others while waiting to go homeProper infection control for staff that are caring
for ill students Hand hygiene and respiratory etiquette Routine Cleaning Early treatment of high risk individuals Consideration of selective school dismissal

Schools – more severe Schools – more severe conditonsconditons
Active Screening High risk students and staff stay home Quarantine if household members are sick Increase distance between people at school Extend isolation periods - use 7 day period or 24
hours after fever, whichever is longer School dismissal
ReactivePreemptive
Childcare SettingsChildcare Settings
Guidance still under revisionSimilar to schoolsFor settings with very young children
(< 5 years) Consideration the longer exclusion
period

Infection ControlInfection ControlHealthcare FacilitiesHealthcare Facilities
CDC still recommending airborne precautions (N95) with all encounters with patients with ILI
HICPACHas endorsed standard precautions plus
droplet precautionsWHO – same as HICPACNDDoH Similar to HICPAC and WHO
BusinessesBusinesses Review or develop business continuity plans Provide education for employees Promote vaccination Review leave policies with employees
Non-punitive
Encourage sick employees to stay home Promote hand hygiene and respiratory etiquette Increase distances between employees and
employees and the public Implement telecommuting and staggered shifts if
possible
General PublicGeneral Public Hand hygiene and respiratory etiquette Avoiding large public gatherings Stay home while ill with a fever Seek medical care or treatment if indicated
High risk groupSigns of more severe illness
Prepare to be at home for 7-10 days How to care for ill family members Infection control in the home
HomecareHomecare Infection control Drink plenty of clear fluids OTC medications (no aspirin) Monitor fever and other symptoms When to seek medical care
Difficulty breathing or chest painPurple or blue color in lipsSevere vomiting Signs of dehydration (dizzy, low urine output, no tears,
loss of elasticity in skin)Less responsive than usual or confusion

Infection Control in the Infection Control in the HomeHome
Place ill person in a private room try to designate one bathroom for ill person
Have ill person wear a surgical mask No visitors One non-pregnant person should provide care Caregiver should consider wearing mask Caregiver should consider N95 if assisting with
respiratory treatment Hand hygiene and respiratory etiquette for
household Use paper towels to dry hands

Surveillance, Testing Surveillance, Testing and Reportingand Reporting
Kirby Kruger, State Kirby Kruger, State Epidemiologist, Division Epidemiologist, Division
DirectorDirector
of Disease Controlof Disease Control

What have we seen in ND?What have we seen in ND?
Laboratory SurveillanceLaboratory SurveillanceSentinel PhysiciansSentinel PhysiciansSyndromic SurveillanceSyndromic SurveillanceFollow-up of random sample of Follow-up of random sample of
children under the age of 18children under the age of 18School absenteeism reportsSchool absenteeism reportsOutbreak SupportOutbreak Support
SurveillanceSurveillance
HospitalizationsHospitalizationsWork with Infection Control NursesWork with Infection Control NursesParticipate in the Emerging Infections Participate in the Emerging Infections
ProgramProgramUse of RedBat to gather Hospitalization dataUse of RedBat to gather Hospitalization dataUse of HC StandardUse of HC Standard
School absenteeism ratesSchool absenteeism ratesIncrease the number of schools that reportIncrease the number of schools that reportMonitor school closuresMonitor school closures
SurveillanceSurveillance
Outbreak SupportOutbreak SupportIncrease the number of facilities that Increase the number of facilities that
can report outbreaks and receive free can report outbreaks and receive free testingtesting
SurveillanceSurveillance
TestingTesting Limited testing in all areas of North Dakota Limited testing in all areas of North Dakota
where novel H1N1 has not been where novel H1N1 has not been demonstrateddemonstratedTesting will be stopped once ongoing transmission is Testing will be stopped once ongoing transmission is
likely (2-5 positive tests)likely (2-5 positive tests)Current restriction on testing Current restriction on testing
• Ward, Cass and Burleigh CountiesWard, Cass and Burleigh Counties
All areas can continue to test for novel All areas can continue to test for novel H1N1 in hospitalized patients in which H1N1 in hospitalized patients in which H1N1 infection has not been ruled outH1N1 infection has not been ruled out
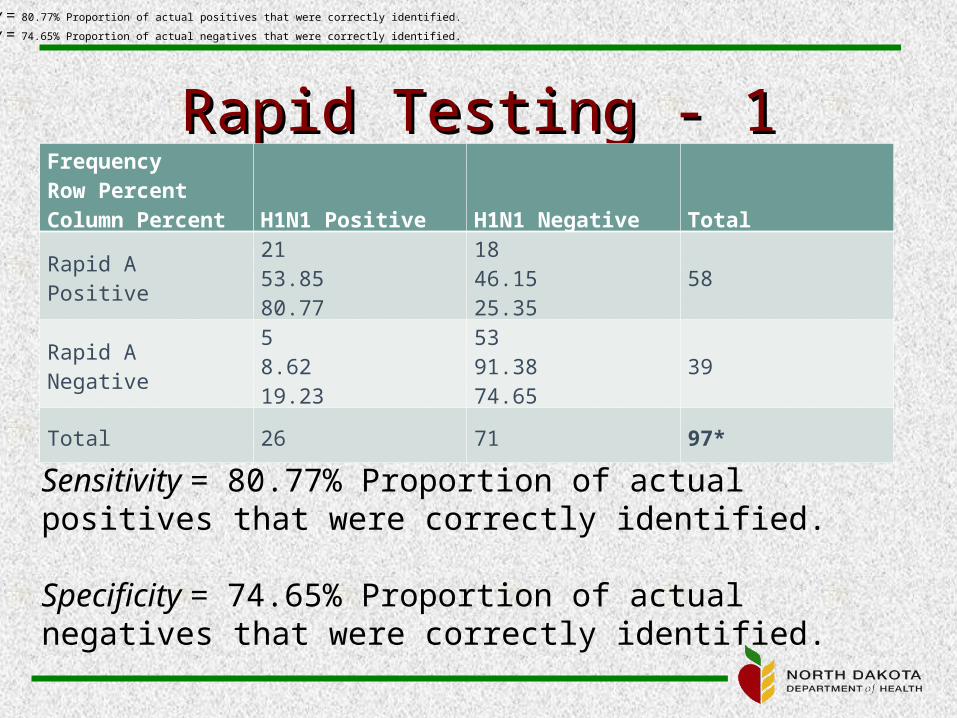
Rapid Testing - 1Rapid Testing - 1FrequencyRow PercentColumn Percent H1N1 Positive H1N1 Negative Total
Rapid A Positive2153.8580.77
1846.1525.35
58
Rapid A Negative58.6219.23
5391.3874.65
39
Total 26 71 97*
Sensitivity = 80.77% Proportion of actual positives that were correctly identified.
Specificity = 74.65% Proportion of actual negatives that were correctly identified.
Sensitivity = 80.77% Proportion of actual positives that were correctly identified.
Specificity = 74.65% Proportion of actual negatives that were correctly identified.
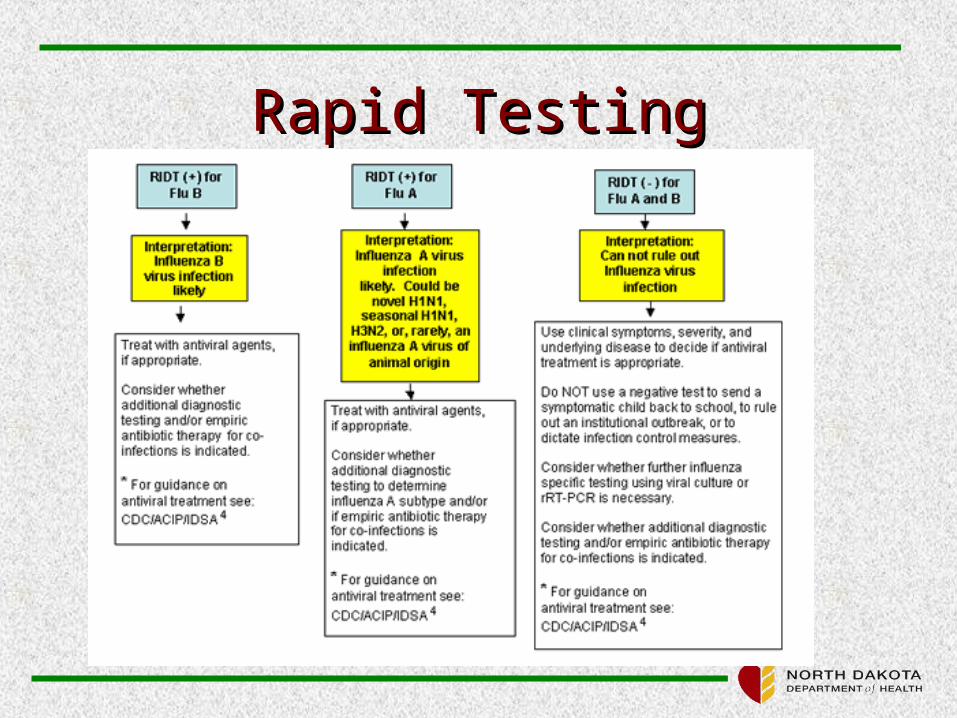
Rapid TestingRapid Testing

ResourcesResources
NDDoH flu web-page (updated every Wednesday)http://www.ndflu.com/
CDC flu web-pagehttp://www.cdc.gov/flu/http://www.cdc.gov/flu/