1 Abstract 2 - journals.lww.com · 1 1 Abstract 2 3 Background: Although research focused on...
30
1 Abstract 1 2 Background: Although research focused on African Americans with mental illness has been 3 increasing, few studies have addressed gender and age differences in beliefs, attitudes, and 4 coping. 5 Objectives: Examined African American women’s and men’s beliefs about mental illness, 6 attitudes toward seeking mental health services, preferred coping behaviors, and whether these 7 variables differ by gender and age. 8 Methods: An exploratory, cross-sectional survey design was used. Participants were 272 9 community-dwelling African Americans aged 25-72 years. Data analysis included descriptive 10 statistics and general linear regression models. 11 Results: Men and women believed they knew some of the symptoms and causal factors of mental 12 illness. Their attitudes suggested they are not very open to acknowledging psychological 13 problems, are concerned about stigma associated with mental illness, are somewhat open to 14 seeking mental health services, but prefer religious coping. Significant gender and age 15 differences were evident in attitudes and preferred coping. 16 Discussion: Findings can guide future research with this population with a focus on developing 17 reliable beliefs measures for this group, examining the impact of stigma and psychological 18 openness on treatment-seeking, and development of gender- and age- specific mental health 19 interventions. 20 21 Key Words: African Americans, Mental Illness, Beliefs, Coping Behaviors 22 *Manuscript (Including Abstract, References and Figure Legends)
Transcript of 1 Abstract 2 - journals.lww.com · 1 1 Abstract 2 3 Background: Although research focused on...

1
Abstract 1
2
Background: Although research focused on African Americans with mental illness has been 3
increasing, few studies have addressed gender and age differences in beliefs, attitudes, and 4
coping. 5
Objectives: Examined African American women’s and men’s beliefs about mental illness, 6
attitudes toward seeking mental health services, preferred coping behaviors, and whether these 7
variables differ by gender and age. 8
Methods: An exploratory, cross-sectional survey design was used. Participants were 272 9
community-dwelling African Americans aged 25-72 years. Data analysis included descriptive 10
statistics and general linear regression models. 11
Results: Men and women believed they knew some of the symptoms and causal factors of mental 12
illness. Their attitudes suggested they are not very open to acknowledging psychological 13
problems, are concerned about stigma associated with mental illness, are somewhat open to 14
seeking mental health services, but prefer religious coping. Significant gender and age 15
differences were evident in attitudes and preferred coping. 16
Discussion: Findings can guide future research with this population with a focus on developing 17
reliable beliefs measures for this group, examining the impact of stigma and psychological 18
openness on treatment-seeking, and development of gender- and age- specific mental health 19
interventions. 20
21
Key Words: African Americans, Mental Illness, Beliefs, Coping Behaviors22
*Manuscript (Including Abstract, References and Figure Legends)

2
In the U.S. an estimated 57.5 million Americans ages 18 and older experience mental illness 1
each year (Kessler et al., 2005). Although mental illness is an “equal opportunity” illness that 2
strikes regardless of race, ethnicity or gender, some groups appear to experience higher burden 3
associated with mental illness (Williams et al., 2007). For instance, in the U.S. African 4
Americans make up only 12% of the population (40.1 million), yet they make up 7.5 million 5
Americans affected by mental illness (Davis, 2005; US Census Bureau, 2007). Compared to 6
Caucasians, mentally ill African Americans have more chronic disease, higher levels of 7
disability, higher rates of inpatient service use, lower rates of outpatient mental health service 8
use, and more barriers to seeking mental health treatment (Snowden, 2001; USDHHS, 2001; 9
Ward, Clark & Heidrich, 2009; Williams et al., 2007). 10
Although research focused on African Americans with mental illness has been 11
increasing, few studies have addressed gender and age differences in beliefs, attitudes, and 12
coping. Disregarding gender and age ignores within group diversity and can have critical 13
implications for documenting and understanding prevalence, treatment-seeking behaviors 14
(service use), and the potential need for gender- and age-specific treatment. We sought to 15
address this research gap by examining African American’s representations/beliefs about mental 16
illness, attitudes towards seeking mental health services, preferred coping behaviors, and whether 17
these vary by gender and age. 18
The Common Sense Model (CSM) guided this work (Leventhal, Nerenz & Steele, 1984; 19
Petrie, Jago & Devcich, 2007). The CSM postulates that individuals have common sense beliefs/ 20
representations about illnesses that guide how they cope with health threats and illness. A 21
representation is a set of beliefs about the identity/symptoms, cause, timeline, consequences, 22
control/treatment, illness coherence (understanding of the illness), and emotional impact of the 23

3
health threat or illness. Representations are informed by informal (family, friends, and clergy 1
etc.) and formal sources (education, training, and health care providers etc.) of information. 2
Regardless of the source or accuracy of the information, representations influence behaviors 3
chosen to eliminate or control the health threat or illness, i.e., coping responses. 4
Despite their mental illness burden, African Americans have low rates of seeking 5
treatment. This behavioral pattern raises the question of how African American men and women 6
of various ages cope with mental illness. Factors that may impede treatment-seeking such as 7
beliefs about mental illness, attitudes toward seeking mental health services, and preferred 8
coping behaviors have not been examined with a focus on gender or age differences (Ward et al., 9
2009). Such research would resolve the issue of whether there is need for gender- and or age-10
specific outreach and intervention for African Americans, and could guide the development of 11
such efforts. Gender- and age-specific outreach and clinical interventions have the potential to 12
increase treatment-seeking behaviors among African American men and women. 13
Studies examining African Americans beliefs about mental illness and attitudes toward 14
seeking mental health services have shown mixed results. Several studies, including the seminal 15
report Mental Health: Culture, Race and Ethnicity, have shown that African Americans view 16
mental illness as highly stigmatizing, resulting in low treatment-seeking (Gary, 2005; National 17
Mental Health Association, 1998; Thompson-Sanders, Bazile, & Akbar, 2004; USDHHS, 2001). 18
Similarly, a recent qualitative study of attitudes and beliefs about mental health among older 19
African American adults revealed that participants viewed mental illness, particularly depression, 20
as a “weakness and if you had true inner strength you wouldn’t let depression get to you, and 21
then you wouldn’t need to get professional help” (Conner, Copeland, Grote et al., 2010). 22

4
In contrast to the above findings, two studies indicate that African Americans have 1
positive beliefs and attitudes toward seeking mental health services, but these positive beliefs 2
and attitudes do not translate to actually seeking treatment. For instance, in one study of racial 3
differences in beliefs about how the natural course of mental illness relates to perceptions of 4
treatment effectiveness, African Americans compared to Caucasians were more likely to believe 5
that mental health professionals could help individuals with mental illness. However, the African 6
Americans were also more likely to believe that mental health problems could improve on their 7
own (Anglin, Alberti, Link & Phelan, 2008). The belief that mental health problems can resolve 8
on their own seemed to negatively affect use of mental health services as a coping strategy. 9
Similar results were obtained in another study of racial differences in attitudes toward 10
professional mental health care and use of services; African Americans compared to Caucasians 11
had more positive attitudes toward seeking mental services, but were less likely to use services. 12
In other words, having a positive attitude toward seeking mental health services did not result in 13
actual use of mental health services (Diala, Muntaner, Walrath, Nickerson, LaVeist, & Leaf, 14
2000). 15
The research described above suggests that although some African Americans may have 16
positive beliefs and attitudes towards seeking mental health services, they are not seeking or 17
using such services as a way of coping with mental illness. Hence the question, if African 18
Americans are not seeking mental health services how are they actually coping with mental 19
health problems? The limited literature suggests preferred coping is primarily religious (clergy 20
and church family (Chatters, Taylor, Jackson, & Lincoln, 2008; Conner, Copeland, Grote et al., 21
2010; Dessio, Wade, Chao, Kronenberg, Cushman, & Kalmuss, 2004; Ward et al., 2009; Ward & 22
Heidrich, 2009). For instance, in a study examining African American women’s preferred 23

5
coping, Ward and colleges found this group would “definitely” use religious coping to deal with 1
a mental health problem, while indicating they would “probably” seek professional treatment. 2
Similarly, Chatters and colleagues found that more African Americans (90.4%) than non-3
Hispanic Whites (66.7%) reported use of religious coping in dealing with mental health issues 4
(Chatters, Taylor, Jackson, & Lincoln, 2008). In a qualitative study, Connors and colleagues also 5
found high use of religious coping including prayer and developing a relationship with God as 6
ways to cope with depression (Conner, Copeland, Grote et al., 2010). For example, one 7
participant stated “yeah, I um, prayers is the first thing on my list.” 8
Given that religious coping is preferred among African American women (Ward & 9
Heidrich, 2009), do such preferences result in delays in seeking professional help? Whether 10
religious coping can co-exist with seeking professional help has not been explored. In addition, 11
whether use of religious coping is also preferred among African American men is unknown as 12
almost all previous research has involved women. Hence the need for more research exploring 13
gender and age differences in coping behaviors among African American men and women. 14
Given the mixed findings regarding African American’s beliefs and attitudes towards 15
mental illness and seeking mental health services, the limited research on preferred coping 16
among this group, and the scarcity of mental health research with African American men, this 17
study examined the following research questions: 18
1. What are African American women and men’s representations of mental illness? 19
20 2. What are African American women and men’s attitudes toward seeking mental health 21
services? 22
23 3. How do African Americans women and men believe they would cope if faced with 24
mental illness? 25
26

6
4. Are there gender and age differences in attitudes and coping, and does age influence the 1
relationship between gender and attitudes and coping? 2
3
Method 4
Study Design and Sample 5
An exploratory, cross-sectional survey design was used. African American men and women 6
ages 25 to 70 were recruited regardless of history of mental illness, as the primary focus was 7
participants’ beliefs regardless of their experience with mental illness. The desired sample size 8
was based on having power of .80 to detect a difference between men and women of .25 standard 9
deviations in beliefs, attitudes and coping. A sample of 180 participants was required, however 10
due to overwhelming interest in the study the final sample consisted of 272 participants. See 11
Table 1 for demographic characteristics of the sample by gender. 12
Measures 13
Demographic questionnaire. Year of birth, income, marital status, number of children, 14
socioeconomic status, and level of education were collected. 15
Representations of mental illness -- Identity. To assess identity/symptoms associated with mental 16
illness, we used the Brief Symptom Inventory (BSI) which includes 53 symptoms associated with mental 17
illness (Derogatis & Melisaratos, 1983). Response options were changed from a Likert-type scale to 18
dichotomous responses of 1 (yes) or 0 (no) and scores were summed to give a total score. Current 19
research supports construct validity of the BSI with African Americans ( Hoe & Brekke, 2009). The BSI 20
has outstanding internal consistency with a reported alpha of .96, consistent with an alpha of .97 in the 21
present study. 22
Representations of mental illness -- Cause, Timeline, Consequences, Treatment Cure/Control, 23
Illness Coherence, and Emotional Representation. These dimensions of representation were measured 24

7
using the Illness Perception Questionnaire- Revised (IPQ-R), an instrument based on the Common Sense 1
Model (Moss-Morris et al., 2002). The IPQ-R consists of seven subscales Identity, Cause, Timeline, 2
Consequences, Treatment Cure/Control, Illness Coherence, and Emotional Representation. For this study, 3
the BSI was used to assess identity (as described above) because the Identity subscale of the IPQ-R 4
assess individuals’ beliefs about symptoms of physical illnesses rather than symptoms associated 5
with mental illnesses. 6
The 16-item Cause subscale assesses beliefs about factors that may cause mental illness. 7
The 8-item Timeline subscale assesses the degree to which the respondent believes that mental 8
illness has a cyclical course. The 7-item Consequences subscale measures the degree to which 9
outcomes of mental illness for self and others are considered serious and negative. The 11-item 10
Treatment Cure/Control subscale assesses the degree to which the individual believes mental 11
illness is curable or controllable through medical treatment and personal motivation. The 5-item 12
Illness Coherence subscale assesses the extent to which an individual perceives he/she has a 13
good understanding of mental illness. Finally, the 6-item Emotional Representation subscale 14
assesses the degree to which an individual believes he or she is emotionally affected by mental 15
illness. All items have 5-point Likert-type response options ranging from 1 (strongly disagree) to 16
5 (strongly agree) and subscale scores are created by taking a mean of the relevant items. 17
Minor changes were made in IPQ-R wording, consistent with the developers’ suggestions 18
for adapting the scale (Moss-Morris et al., 2002). For example, “My illness will last a long time” 19
was changed to “Mental illness will last a long time.” In previous studies, the IPQ-R has shown 20
good discriminant, known-group, and predictive validity, as well as acceptable internal 21
reliability, with subscale alphas ranging from .79 to .89 (Moss-Morris, et al., 2002). In the 22

8
present study, alphas ranged from .58 to .66, a matter which is discussed further in the discussion 1
and limitations section. 2
Attitudes. Attitudes toward seeking mental health services was measured using the 3
Inventory of Attitude Toward Seeking Mental Health Services (IASMHS). The IASMHS is a 24-4
item measure designed to assess individuals’ attitudes toward seeking professional help for 5
mental health problems (Mackenzie et al., 2004). The IASMHS has 3 subscales: psychological 6
openness, help-seeking propensity, and indifference to stigma. Psychological openness refers to 7
the extent to which individuals are open to acknowledging mental health problems. Help-seeking 8
propensity reflects the extent to which individuals believe they are willing and able to seek 9
professional mental health services. Indifference to stigma reflects the extent to which 10
individuals are concerned about what significant people in their lives might think if they found 11
out the individual was seeking professional help for mental health problems (Mackenzie et al., 12
2004). The items have 5-point response options: disagree (0), somewhat disagree (1), undecided 13
(2), somewhat agree (3), or agree (4). Relevant items are summed to create subscale scores that 14
range from 0-32, with higher scores indicating more psychological openness, help-seeking 15
propensity, and less concern about stigma. Previously reported internal consistencies for the 16
subscales are 0.82 for the psychological openness subscale, 0.76 for the help-seeking propensity 17
subscale, and 0.79 for the indifference to stigma subscale (Mackenzie et al., 2004). In the present 18
study the subscales were acceptable with 0.73 for the psychological openness subscale, 0.81 for 19
the help-seeking propensity subscale, and 0.77 for the indifference to stigma subscale. 20
Coping. Preferred coping was measured using the 14-item Preferred Coping Scale (PCS) 21
(Ward & Heidrich, 2009). The PCS has 4 subscales measuring use of: (a) Professional Help (6 22
items); (b) Informal Support Network (4 items); (c) Religiosity (3 items); and (d) Avoidance (6 23

9
items). Response options range from 1 (definitely not do), 2 (not sure), 3 (might do) to 4 1
(definitely do). Subscale scores were created by taking a mean of the relevant items, with higher 2
scores indicating greater likelihood of coping in that fashion if faced with a mental illness. In 3
previous research with African American individuals, internal consistency alpha coefficients 4
ranged from 0.62 - 0.78 (Ward & Heidrich, 2009). In the present study subscale reliabilities 5
ranged from 0.64 - 0.84. 6
Procedure 7
Approval to conduct this study was obtained from the University Health Sciences 8
Institutional Review Board (IRB). Packets containing informed consent forms, the demographic 9
questionnaire, the IPQ-R, BSI, IASMHS, PCS, researcher-addressed postage-paid envelope, and 10
a $10 gift card were distributed at churches, local African American barber shops and hair 11
salons, the YWCA, community events, and through local advertising in the African American 12
community. In addition, a snowball sampling strategy (Karasz, 2005) was also used by 13
encouraging participants to tell people they knew about the research opportunity. Prospective 14
participants were given the opportunity to complete the packet immediately (in person) or to 15
return it by mail. Participants received assistance with reading or completing the research packet 16
if they requested it. 17
Results 18
To address the first research question which examined African American men and 19
women’s beliefs/representations, each dimension of the CSM using the BSI and the IPQ-R was 20
examined using descriptive statistics and bivariate analyses. On the Identity/Symptoms 21
dimension (BSI scale), the women endorsed an average of 33.8 symptoms (SD=14.8, range= 53) 22
and the men endorsed an average of 31.9 symptoms (SD=14.5, range 53). Seventy-five percent 23

10
or more of participants endorsed the following as symptoms of mental illness: hostility (84.1 %), 1
thoughts of ending your life (78.7 %), suddenly scared for no reason (77.5 %), experiencing 2
spells of terror or panic (76.5 %), and having urges to beat, injure, or harm someone else (76.4 3
%). Least endorsed symptoms were pain in heart or chest (36.7 %), nausea or upset stomach 4
(39.5 %), hot and cold spells (39.6 %) and feeling weak in parts of the body (39.6 %), which 5
suggest most participants did not believe these symptoms were symptoms of mental illness. 6
To understand participant’s beliefs about factors they believed can cause mental illness, 7
descriptive statistics was conducted on 17-item IPQ-R Cause Subscale (CS). Recall that response 8
options were strongly disagree (1), disagree (2), neither agree or disagree (3), agree (4), and 9
strongly agree (5). Mean scores on the CS indicated the women believed mental illness can be 10
caused by the following 7 factors: stress (M=4.0, SD=0.9); trauma (M=4.0, SD=0.9); drug use 11
(M=3.9, SD=1.0); alcohol use (M=3.7, SD=1.1); heredity (M=3.70, SD=1.0); family problems 12
(M=3.7, SD=0.9); and work stress (M=3.6, SD=1.1). The men believed mental illness can be 13
caused by the following 5 factors: alcohol use (M=3.7, SD=1.1); drug use (M=3.6, SD=1.2); 14
trauma (M=3.6, SD=1.2), stress (M=3.6, SD=1.3), and family problems (M=3.3, SD=1.0). 15
Mean scores for the remaining IPQ-R subscales (see Table 2) suggest the women believed 16
mental illness is chronic and cyclic, with negative consequences, but can be controlled. The 17
women’s mean scores were near the midpoint (M=3) for illness coherence and emotional impact 18
suggesting they neither agreed nor disagreed that they have an understanding of mental illness 19
and are emotionally affected by it. The men believed having a mental illness can result in 20
negative consequences. However, the men’s mean scores for the other beliefs subscales were 21
near the midpoint suggesting they neither agreed nor disagreed that mental illness is chronic and 22

11
cyclic, can be controlled, they have an understanding of mental illness or are affected by mental 1
illness. 2
The second research question examined African American women and men’s attitudes 3
toward seeking mental health services. Using descriptive statistics, mean scores on the IASMHS 4
subscales for the women and men respectively were: Psychological Openness (M=18, SD=7.6, 5
range= 32; M=16, SD=6.7, range=31), Help-seeking Propensity (M=24.6, SD=6.1, range=32; 6
M=22.7, SD=6.7, range=29), and Indifference to Stigma (M=18.9, SD=7.5, range=32; M=18.3, 7
SD=7.2, range=28) (see Table 2). These mean scores for both the women and men indicate low 8
psychological openness, some openness to seeking help, and some concerns about stigma. 9
The third research question evaluated African American women and men’s coping if 10
faced with mental illness. On the PCS higher scores (4=definitive use) suggest higher 11
endorsement of a particular coping behavior. Mean scores on the PCS subscales for the women 12
and men respectively were: Professional Coping (women M= 2.8, SD= 0.8, range=3.4; men 13
M=2.8, SD=0.7, range=4), Informal Coping (women M=3.3, SD=0.8, range=2.5; men M=3.3, 14
SD=.08, range=4), Religious Coping (women M=3.5, SD=0.6, range=2.7; men M=3.4, SD=0.8, 15
range=4) and Avoidance Coping (women M=2.8, SD=.97, range=3; men M=2.6, SD=1.1, 16
range=3) (see Table 2 for p-value). The mean score for the women on religious coping indicated 17
they would “definitely use” religious coping, while the men “might use” it. All of the other 18
mean scores on the PCS were closer to the midpoint (M=3) indicating all participants “might 19
use” professional and informal coping, and they were “not sure” if they would use avoidance 20
coping. 21
The fourth question examined gender and age differences in attitudes and preferred 22
coping, and the influence of age on the relationship between gender and attitudes and coping. 23

12
General linear models (GLM) were created to examine differences between gender, age group 1
and attitude and coping. In addition, a gender by age group interaction term was examined to 2
determine if the subscale level differences among age groups differed between the genders. 3
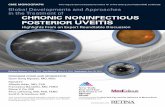
Tables 3 and 4 presents results of the GLM addressing these questions. Overall, an age group 4
effect was evident in psychological openness and help-seeking propensity. Also, an age group by 5
gender interaction was evident in psychological openness. There were no statistically significant 6
gender or age group effects for indifference to stigma. These findings regarding psychological 7
openness indicate that young women were significantly more open than young men, but middle-8
age and older men and women did not differ (see Figure 1). Also, young women had 9
significantly higher propensity for help-seeking than young men, but middle-age and older men 10
and women had higher propensity for help-seeking overall compared to the other groups (see 11
Figure 1). 12
Overall, an age group effect was evident in preferred coping including use of professional 13
help, informal support, and religious coping, but not for avoidance coping. There were no 14
statistically significant gender effects regarding use of professional help, use of informal support, 15
religious coping, or avoidance coping. On the other hand, younger and middle-age men and 16
women compared to older men and women significantly preferred use of professional help, 17
informal support and religious coping (see Figure 1). 18
Discussion 19
The primary aim of this study was to examine African American women and men’s 20
beliefs about mental illness, attitudes towards seeking mental health services, preferred coping 21
behaviors, and whether attitudes and coping varied by gender and age. The findings suggest the 22
women and men believed they knew some of the symptoms and causal factors of mental illness. 23

13
They held beliefs about the timeline, consequences, and controllability of mental illness, were 1
unsure of their own understanding of mental illness, and whether they were emotionally affected 2
by mental illness. However, due to low reliability of five of the IPQ-R subscales (timeline, 3
consequences, controllability, illness coherence and emotional representation) findings of beliefs 4
in these areas should be interpreted cautiously. Regarding attitudes, findings appear to suggest 5
participants are not very open to acknowledging psychological problems, are concerned about 6
the stigma of mental illness, but are somewhat open to seeking mental health services. Religious 7
coping appeared to be the most preferred coping mechanism. Significant gender and age 8
differences were evident in attitudes toward seeking mental health services and preferred coping. 9
Beliefs 10
The findings suggest both female and male participants believed they knew some of the 11
symptoms and causal factors of mental illness and they accurately identified these factors. 12
However, our finding is interesting given contrasting results of several studies. For example, a 13
national survey conducted by the National Mental Health Association (NMHA, 1998), found that 14
63% of African Americans believed depression is a personal weakness. Similarly, Johnson 15
(2000) found African American men believed mental health problems are simply a lack of 16
motivation. In a more recent study Conner and colleagues (2010) found older African American 17
adults believed depression was a sign of weakness and lack of inner strength. The difference in 18
findings with the present study could be attributed to a number of factors including cohort 19
effects, participants’ exposure to mental illness, and possibly increased knowledge of mental 20
illness among our study participants. 21
Low reliability of the IPQ-R subscales (timeline, consequences, controllability, illness 22
coherence and emotional representation) raise questions about use of these subscales with 23

14
African Americans. To our knowledge, only one study (Ward & Heidrich, 2009) has used the 1
IPQ-R with African American women, and that study revealed problems with poor reliability on 2
the timeline and controllability subscales. No study could be located that used the IPQ-R with 3
African American men. Problems with the IPQ-R subscales in the present study combined with 4
results from Ward & Heidrich (2009) warrant further investigations into the IPQ-R, with the goal 5
of developing a more reliable measure to assess African Americans beliefs about mental illness. 6
Attitudes 7
When examining African American women and men’s attitudes towards seeking mental 8
health services, our results suggest they are somewhat willing and able to seek professional 9
mental health services. However, they do not appear to be open to acknowledging mental health 10
problems and they are concerned about what significant people in their lives might think if they 11
found out they were seeking or were to seek professional help for mental health problems. The 12
finding that African American women and men are open to seeking mental health services is 13
consistent with the finding of positive attitudes by Diala et al.2000, but in contrast with most of 14
the current literature which suggest African Americans have negative attitudes toward seeking 15
mental health services (Gary, 2005; National Mental Health Association, 1998; Thompson-16
Sanders et al., 2004; USDHHS, 2001). 17
Our finding that both the women and men had low endorsement of psychological 18
openness might shed light on African Americans treatment-seeking behaviors. African 19
Americans low use of mental health services, historically and presently, has been well 20
documented. In addition, several barriers to seeking mental health services have been postulated 21
in current literature including poor access to care, receipt of poor quality care, low availability of 22
care, and stigma associated with mental illness (USDHHS, 2001). Missing from the treatment-23

15
seeking and barriers literature is the relationship between psychological openness and the 1
decision to seek professional help for mental health problems. Another unanswered question is 2
whether psychological openness influences type of coping responses or whether it influences 3
treatment adherence and patient/client continuity in treatment. In sum, our finding about African 4
American women and men’s low endorsement of psychological openness has implications for 5
future research and treatment. 6
The results regarding concerns about stigma, particularly concerns about significant 7
people finding out that one is seeking mental health services is consistent with current literature 8
on stigma. In fact, the stigma literature suggests concerns about stigma are quite prevalent in the 9
African American community (Gary, 2005; USDHHS, 2001). Our results however, provide new 10
information regarding African American men and stigma. Most of the research on stigma has 11
been gender neutral and has aggregated data and results, with no focus on African American 12
men. However, our findings suggest that stigma is also a concern among African American men, 13
and has the potential to inform gender-specific outreach designed to educate and reduce stigma 14
in the African American community. 15
In sum, our overall findings about attitudes toward mental health services provides more 16
insight about African Americans low use of mental health services and can guide research 17
focusing on improving attitudes to treatment-seeking, increasing treatment-seeking behaviors, 18
and examining gender differences in these areas. 19
Coping Behaviors 20
Our results suggest if faced with a mental illness, the women believed they would 21
“definitely use” religious coping, while the men might use it. Use of religious coping among our 22
female participants is consistent with a number of studies showing the high use of religious 23

16
practices (praying, reading the Bible, and talking to a pastor) to cope with mental health issues 1
(Chatters et al., 2008; Dessio et al., 2004). Our finding that men “might use” religious coping is 2
new and makes a significant contribution to the literature. 3
Consistent with mental health service use literature, our participants seemed apprehensive 4
about seeking professional help (Alegria et al., 2008; Neighbors et al., 2009). Surprisingly they 5
also seemed tentative about using informal support which is inconsistent with current literature, 6
which shows that use of informal support such as family and friends is very common among 7
African American women and men (Broman, 1996; Johnson, 2000; Snowden, 2001). It is 8
possible our participants’ tentativeness about using informal support and seeking professional 9
help might be related to their concern about stigma if significant people in their lives found out 10
they were seeking or were to seek professional help. Lincoln and colleagues (2005), found that 11
among African Americans, social support did not mitigate the effects of stress and was 12
negatively affected by financial strain. Given that 87.8% of our participants’ incomes were 13
below $40,000, it is possible that their tentativeness about use of support network could be 14
related to financial strain. 15
16
Gender and Age Differences in Attitudes and Preferred Coping 17
Given that most of mental health research focusing on African Americans has neglected 18
to examine gender-based differences, and aging research among this group is still in the infancy 19
stage, there is little published information about gender and age differences. Thus, our study 20
results documenting the existence of gender and age differences in attitudes and preferred coping 21
is significant. In particular, the finding that the women were significantly more open to 22
acknowledging psychological problems and seeking professional help compared to the men can 23

17
help guide gender-specific mental health education/outreach to African American men. In 1
addition, the finding of age differences showing that older participants were less psychologically 2
open than young participants, and middle-aged participants were more open to seeking 3
professional help than young participants suggest the need for future research to examine how 4
psychological openness can be increased among older adults and African American men, with 5
the goal of increasing treatment-seeking behaviors. 6
Although there is a small growing body of research examining coping behaviors 7
(Conners et al., 2010; Chatters et al. 2008; Ward & Heidrich, 2009; Ward, Clark & Heidrich, 8
2009) information about gender and age differences in coping behaviors is scant. Thus, our 9
finding that both older and middle-aged participants compared to young participants were less 10
likely to seek professional help to cope with a mental health problem is critical because it sheds 11
light on which subgroups of African Americans are not seeking professional help. 12
In contrast to current literature, we found that older adults compared to young adults were 13
less likely to use informal support and religious coping. A plethora of research suggests that 14
religious coping is very common among older African Americans. For instance, a recent study 15
found older African Americans relied heavily on religious coping. In fact, religious coping was 16
identified as the most culturally accepted strategy for dealing with depression (Conner et al., 17
2010). The difference in findings may be attributed to the diversity with the African American 18
population. Such diversity includes religious beliefs, geographic residence, etc. In addition, it is 19
possible older African Americans are less likely to use informal support due to the impact of 20
morbidity and mortality among their social network. 21
Limitations 22

18
Beliefs about timeline, consequences, illness coherence, and emotional impact should be 1
interpreted cautiously as the internal consistency on these IPQ-R subscales were below 2
acceptable levels (<.70). This is the first report of IPQ-R use with African American males and 3
older African Americans. The low reliability on some of the subscales may indicate lack of 4
validity for use with this population. Another limitation is that no adjustments were made to the 5
type I error rate to account for the multiple models due to the exploratory nature of these 6
analyses. Thus, conclusions were drawn cautiously because some results may be significant due 7
to chance alone. Finally, limits to generalizability of the results should be considered since the 8
sample was drawn primarily from the Midwest. However, the sample did include an inner city / 9
urban sample representative of many inner cities in the U.S. 10
Future Research 11
The findings and limitations of the present study suggest numerous avenues for future 12
research. Given limitations with use of the IPQ-R and the critical need to further examine 13
African Americans beliefs about mental illness, particularly among African American men and 14
older adults, future research in this area focusing on developing a more reliable beliefs measure 15
is critically needed. Also, use of qualitative methodology has the potential to illuminate 16
underlying social and cultural contexts that may influence beliefs, attitudes, and preferred coping 17
strategies in the absence of more reliable measures. 18
Consistent with mental health service use the literature, our participants seemed 19
apprehensive about seeking professional help. However, our finding about attitudes toward 20
mental health services provides more insight about African Americans low use of mental health 21
services and can guide research focusing on improving attitudes about seeking professional help 22
/ treatment-seeking, increasing treatment-seeking behaviors, and examining gender differences in 23

19
these areas. In addition, the finding that older adults are less likely to use informal support and 1
religious coping compared to young adults is contrary to current literature and warrants further 2
investigation. For instance, it is possible that older African Americans have less informal support 3
if death of love ones, illness of loved ones, or their own health issues restrict their social 4
interactions. It is also possible our study results may reflect geographic influences on religious 5
coping. Replication of the present study with African Americans in the southern “Bible belt” 6
might reveal higher levels of religious coping and other coping among older African Americans. 7
Such a study would likely yield meaningful and useful results in addressing the mental health 8
needs of older African American adults. 9
Conclusion 10
To our knowledge, this study is the first to examine African American women and men’s 11
beliefs about mental illness, attitudes toward seeming mental health services, and preferred 12
coping behaviors, with attention to gender and age differences. The findings suggest the men and 13
women believed they knew some of the symptoms and causal factors of mental illness, and they 14
accurately identified these factors. They are not very open to acknowledging psychological 15
problems, are concerned about the stigma of mental illness, but are somewhat open to seeking 16
mental health services. Religious coping appeared to be the most preferred coping strategy. 17
Significant gender and age differences were evident in attitudes toward seeking mental health 18
services and preferred coping. The findings can guide future mental health research with a focus 19
on developing more reliable measures for this group, the impact of psychological openness on 20
seeking professional treatment, and eliminating disparities in mental health care and outcomes 21
for African American women and men, and older African Americans.22

20
References
Alegria M, C. P., Wells K, et al. (2008). Disparity in depression treatment among racial and
ethnic minority populations in the United States. Psychiatric Servervices,59, 1264-1272.
Anglin, D. M., Alberti, P. M., Link, B. G., & Phelan, J. C. (2008). Racial differences in beliefs
about the effectiveness and necessity of mental health treatment. American Journal of
Community Psychology, 42(1-2), 17-24.
Broman, C. L. (1996). Coping with personal problems. In H. W. Neighbors & J. S. Jackson
(Eds.), Mental health in black America (pp. 117–129). Thousand Oaks, CA: Sage.
Chatters, L. M., Taylor, R. J., Jackson, J. S., & Lincoln, K. D. (2008). Religious coping among
African Americans, Caribbean Blacks, and non-Hispanic Whites. Journal of Community
Psychology, 36, 371-386.
Conner, K. O., Copeland, V. C., Grote, N. K., Koeske, G., Rosen, D., Reynolds, C. F., 3rd, &
Brown, C. (2010). Mental health treatment seeking among older adults with depression:
the impact of stigma and race. American Journal of Geriatric Psychiatry, 18(6), 531-543.
Conner, K. O., Copeland, V. C., Grote, N. K., Rosen, D., Albert, S., McMurray, M. L., . . .
Koeske, G. (2010). Barriers to treatment and culturally endorsed coping strategies among
depressed African-American older adults. Aging & Mental Health, 14(8), 971-983.
Davis, K. (2005). Decreasing discrimination and stigma associated with mental illness in the
African American community. U.S. Department of Health and Human Services:
Substance Abuse and Mental Health Services Administration, Center for Mental Health
Services. Retrieved May 15, 2005, from www.stopstigma.samhsa.gov/archtel.htm.
Derogatis, L.R., & Melisaratos, N. (1983). The brief symptom inventory: An introductory report.
Psychological Medicine, 13(3), 595–605.
Dessio, W., Wade, C., Chao, M., Kronenberg, F.,, & Cushman, L. E., & Kalmuss, D. . (2004).
Religion, spirituality, and healthcare choices of African-American women: Results of a
national survey. Ethnicity and Disease, 14(2), 189–197.
Diala, C., Muntaner, C., Walrath, C., Nickerson, K. J., LaVeist, T. A., & Leaf, P. J. (2000).
Racial Differences in Attitudes Toward Professional Mental Health Care and in the Use
of Services. American Journal of Orthopsychiatry, 70(4), 455-464.
Gary, F. A. (2005). Stigma: Barriers to mental health care among ethnic minorities. Issues in
Mental Health Nursing, 26(10), 979-999.

21
Hoe, M., & Brekke, J. (2009). Testing the Cross-Ethnic Construct Validity of the Brief Symptom
Inventory. Research on Social Work Practice, 19(1), 93-103.
Johnson, E. D. (2000). Differences among families coping with serious mental illness: A
qualitative analysis. American Journal of Orthopsychiatry, 70(1), 126-134.
Karasz, A. (2005). Cultural differences in conceptual models of depression. Social Science &
Medicine, 60(7), 1625-1635.
Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005).
Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the
National Comorbidity Survey Replication. Achieve of General Psychiatry, 62(6), 593-
602.
Leventhal, H., Nerenz, D.R., & Steele, D.J. (1984). Illness representations and coping with
health threats. In: A. Baum, S.E. Taylor, & J.E. Singer (Eds.), Handbook of psychology
and health: Social psychological aspects of health. Hillsdale, NJ: Earlbaum.
Lincoln, C., & Taylor. (2005). K.D. Lincoln, L.M. Chatters and R.J. Taylor, Social support,
traumatic events and depressive symptoms among African Americans, Family Relations
54, 501–511.
Mackenzie CS, K. V., Gekoski WL, Macaulay HL. (2004). An adaptation and extension of the
attitudes toward seeking professional psychological help scale. . Journal of Applied
Social Psychology. 34:2410–2435.
Moss-Morris, R., Weinman, J., Petrie, K. J., Horne, R., Cameron, L. D., & Buick, D. (2002). The
revised Illness Perception Questionnaire (IPQ-R). Psychology & Health, 17(1), 1-16.
National Mental Health Association. (1998). Depression in African Americans is not “Just the
Blues”. Retrieved January 29, 2007 from https://www.nmha.
org/newsroom/system/news.vw.cfm?do=vw&rid=43.
Neighbors, H., Woodward, A., T., Bullard, K., M., Ford, B.C., Taylor, R.J., et al. (2008). Mental
health service use among older African Americans: The National Survey of American
Life. The American Journal of Geriatric Psychiatry, 16(12), 948-956.
Petrie, K. J., Jago, L.A., & Devcich, D.A. (2007). The role of illness perceptions in pat ients with
medical conditions. . Current Opinion in Psychiatry, 20(2), 163–167.
U.S. Department of Health and Human Services. (2001). Mental Health: Culture, Race and
Ethnicity—A Supplement to Mental Health: A Report of the Surgeon General. Rockville,
MD: U.S. Department of Health and Human Services, Public Health Service, Office of
the Surgeon General.

22
U.S. Census Bureau. U.S. Department of Commerce, Washington DC. Accessed June 5, 2008.
Available at http://www.census.gov/Press-Release/www/releases/archives/
population/011910.html.
Snowden, L. (2001). Barriers to effective mental health services for African Americans. . Mental
Health Services Research, 3(4), 191-187.
Thompson-Sanders, V. L., Bazile, A., & Akbar, M. (2004). African Americans’ perceptions of
psychotherapy and psychotherapists. Professional Psychology: Research and Practice,
35(1), 19-26.
Ward, E. C., Clark, L. O., & Heidrich, S. (2009). African American women's beliefs, coping
behaviors, and barriers to seeking mental health services. Qualitative Health Research,
19(11), 1589-1601.
Ward, E. C., & Heidrich, S. M. (2009). African American women's beliefs about mental illness,
stigma, and preferred coping behaviors. Research in Nursing & Health, 32(5), 480-492.
Williams, D. R., Gonzalez, H. M., Neighbors, H., Nesse, R., Abelson, J. M., Sweetman, J., &
Jackson, J. S. (2007). Prevalence and Distribution of Major Depressive Disorder in
African Americans, Caribbean Blacks, and Non-Hispanic Whites: Results From the
National Survey of American Life. Achieve General Psychiatry, 64(3), 305-315.

1
Table 1. Characteristics of Study Sample by Gender
Total
N=272 (%) Male
N=158 (%) Female
N=114 (%) χ2 p-value
Age
Young (22-45) 110 (40.4)
66 (41.7)
44 (38.6) Middle (46-59) 95 (34.9)
56 (35.4)
39 (34.2)
Older (60+) 67 (24.6)
36 (22.8)
31 (27.2) 0.699
Socioeconomic Status Working class 139 (52.5)
89 (56.3)
50 (46.7)
Middle to Upper class 67 (25.3)
37 (23.4)
30 (28.0) Retired 59 (22.3)
32 (20.3)
27 (25.2) 0.306
Education level ≤ High school 174 (69.6)
105 (72.4)
69 (65.7)
College 67 (26.8)
39 (26.9)
28 (26.7) Graduate School 9 (3.6)
1 (0.7)
8 (7.6) 0.014
Income level > $40,000 238 (87.8)
144 (91.7)
94 (82.5)
< $40, 001 - $80, 000 33 (12.2)
13(8.3)
20(17.5) 0.021
Insurance type No 108 (41.5)
81 (53.6)
27 (24.8)
Yes 152 (58.5)
70 (46.4)
82 (75.2) 0.001
Diagnosis of mental illness or treatment for mental illness
No 189 (69.7)
114 (72.6)
75 (65.8) Yes 82 (30.3) 43 (27.4) 39 (34.2) 0.228
* note that some subjects did not answer all questions
Table

2
Table 2. Mean Scores of Illness Perception Questionnaire (IPQ-R), Attitudes and Coping Subscales by Gender
N Mean sd min max p-value*
IPQ-R (Beliefs) Identity/Symptoms all 272 32.7 14.6 0.0 53.0
Female 114 33.8 14.8 0.0 53.0
Male 158 31.9 14.5 0.0 53.0 0.178
Cause all 272 3.3 0.6 1.2 4.8
Female 114 3.4 0.6 1.5 4.8
Male 158 3.3 0.7 1.2 4.8 0.135
Timeline all 272 3.4 0.7 1.0 5.0
Female 114 3.6 0.7 1.8 5.0
Male 158 3.4 0.8 1.0 5.0 0.034
Consequences all 272 3.7 0.7 1.2 5.0
Female 114 3.9 0.6 1.8 5.0
Male 158 3.5 0.7 1.2 5.0 *0.001
Control all 272 3.2 0.5 1.4 4.7
Female 114 3.5 0.4 2.5 4.7
Male 158 3.0 0.5 1.4 4.1 *0.001
Illness Coherence all 272 3.0 0.7 1.0 5.0
Female 114 3.0 0.8 1.0 5.0
Male 158 2.9 0.7 1.0 4.8 0.507
Emotional Representation all 272 2.7 0.7 1.0 4.3
Female 114 2.8 0.7 1.0 4.3
Male 158 2.7 0.6 1.0 4.0 0.181
IASMHS (Attitudes) Psychological_openness (sum) all 272 16.9 7.1 0.0 32.0
Female 114 18.0 7.6 0.0 32.0
Male 158 16.0 6.7 0.0 30.9 *0.033
Help-seek propensity (sum) all 272 23.5 6.5 0.0 32.0
Female 114 24.6 6.1 0.0 32.0
Male 158 22.7 6.7 3.0 32.0 *0.019
Indifference to stigma (sum) all 272 18.6 7.3 0.0 32.0
Female 114 18.9 7.5 0.0 32.0
Male 158 18.3 7.2 4.0 32.0 0.554

3
PCS (Coping) Professional help all 272 2.8 0.7 0.0 4.0
Female 114 2.8 0.8 0.6 4.0
Male 158 2.8 0.7 0.0 4.0 0.955
Informal support all 272 3.3 0.8 0.0 4.0
Female 114 3.3 0.8 1.5 4.0
Male 158 3.3 0.8 0.0 4.0 0.964
Religious coping all 272 3.4 0.8 0.0 4.0
Female 114 3.5 0.6 1.3 4.0
Male 158 3.4 0.8 0.0 4.0 0.228
Avoidance all 272 2.7 1.0 0.0 4.0
Female 114 2.8 1.0 0.0 4.0
Male 158 2.6 1.1 0.0 4.0 0.273
*p-value compares female to male

4
Table 3. Results of General Linear Modeling (GLM) of IASMHS (Attitudes N=272)
F-value Numerator DF P-value
Psychological Openness Age group 5.9891 2 0.002880
Gender 2.2659 1 0.133511
Income 0.0001 1 0.990973
Socioeconomic Status 3.3056 1 0.070241
Education 0.0735 1 0.786506
Diagnosis of mental illness 0.4085 1 0.523341
Age group*Gender 3.145 2 0.044778
Help - Seeking Age group 4.2089 2 0.015930
Gender 2.3537 1 0.126247
Income 1.1856 1 0.277263
Socioeconomic Status 2.419 1 0.121138
Education 0.0751 1 0.784297
Diagnosis of mental illness 1.0915 1 0.297152
Age group*Gender 1.7782 2 0.171069
Indifference to Stigma Age group 0.8221 2 0.440709
Gender 0.0069 1 0.933649
Income 0.0031 1 0.955315
Socioeconomic Status 1.2331 1 0.267864
Education 2.2160 1 0.137846
Diagnosis of mental illness 0.2671 1 0.605745
Age group*Gender 1.7539 2 0.175224
Denominator: 250

5
Table 4. Results of General Linear Modeling (GLM) of Preferred Coping Scale, N=272
F-value Numerator DF P-value
Professional Help Age group 4.1873 2 0.016266
Gender 0.7143 1 0.398836
Income 0.3093 1 0.578636
Socioeconomic Status 3.4867 1 0.063035
Education 0.6974 1 0.404453
Diagnosis of mental illness 3.3709 1 0.067544
Age group*Gender 0.1904 2 0.826756
Informal Support Age group 4.5372 2 0.011600
Gender 0.0389 1 0.843709
Income 0.7115 1 0.399742
Socioeconomic Status 0.2254 1 0.635361
Education 0.5993 1 0.439586
Diagnosis of mental illness 0.5608 1 0.454649
Age group*Gender 0.3519 2 0.703701
Religious Age group 4.5512 2 0.011444
Gender 0.9037 1 0.342713
Income 0.8558 1 0.355804
Socioeconomic Status 5.2623 1 0.022623
Education 0.5853 1 0.444955
Diagnosis of mental illness 2.0889 1 0.149625
Age group*Gender 0.2307 2 0.794155
Avoidance Age group 0.9654 2 0.382231
Gender 1.0969 1 0.295966
Income 0.0670 1 0.795952
Socioeconomic Status 0.5865 1 0.444501
Education 0.6517 1 0.420272
Diagnosis of mental illness 0.5954 1 0.441081
Age group*Gender 0.9877 2 0.373888 Denominator: 250

6

1
Figure 1. Graphic display of results of GLM adjusting for covariates
Figure

2