· Web viewThe Annexes listed below, compliment the main PBC Governance Agreement for 2009/10....
131
Item 8 PBC Gov Sub-Comm (Annex A) The Annexes listed below, compliment the main PBC Governance Agreement for 2009/10. Annexes Annex A PBC Cluster Planning and Performance Management Process (including Commissioning Objectives for 2009/10) Annex B Budgets and Budget Setting Methodology 2009/10 Annex C Incentive Scheme 2009/10 Annex D Business Case for use when seeking Investments Annex E Savings Requirements and Spend 2009/10 Annex F PBC Cluster Governance Arrangements Annex G Roles and Responsibilities Annex H Terms of Reference PBC Accountability Framework - PBC Governance Sub-Committee - PBC Executive Committee - PBC Federation Council - PBC Development Programme Steering Committee - PBC Demand Management Committee Annex I PBC Disputes Resolution Procedure Annex J PBC Governance Agreement Declaration 2009/10 20 May 2009 1
Transcript of · Web viewThe Annexes listed below, compliment the main PBC Governance Agreement for 2009/10....

Item 8 PBC Gov Sub-Comm (Annex A)
The Annexes listed below, compliment the main PBC Governance Agreement for 2009/10.
Annexes
Annex A PBC Cluster Planning and Performance Management Process (including Commissioning Objectives for 2009/10)
Annex B Budgets and Budget Setting Methodology 2009/10
Annex C Incentive Scheme 2009/10
Annex D Business Case for use when seeking Investments
Annex E Savings Requirements and Spend 2009/10
Annex F PBC Cluster Governance Arrangements
Annex G Roles and Responsibilities
Annex H Terms of Reference PBC Accountability Framework
- PBC Governance Sub-Committee- PBC Executive Committee- PBC Federation Council- PBC Development Programme Steering Committee- PBC Demand Management Committee
Annex I PBC Disputes Resolution Procedure
Annex J PBC Governance Agreement Declaration 2009/10
Annex K PBC / Strategic Commissioning Joint Planning Cycle (to be inserted following development through the PBC Development Programme)
20 May 2009 1

ANNEX A
PBC Cluster Planning and Performance Management Process
Practice Based Commissioning Objectives 2009/10
This Practice Based Commissioning (PBC) Commissioning Objectives should be prepared by the PBC Cluster on an annual basis.
Completed Commissioning Objectives must be submitted to the PCT for approval no later than Friday 8 May 2009, having been discussed and agreed upon with all participating practices and signed off by the PBC Cluster Clinical Leads on behalf of all participating practices. There will be no extension to this deadline except in very exceptional circumstances.
On review of the plans on 1 June the PBC Governance Sub-Committee will either:
1. Recommend for approval by the PCT Board – or;
2. Recommend for approval, pending requested further information – or;
3. Not recommend for approval by the Board, in which case reasons will be given to the Cluster, so that resubmission may be made.
A. CONTACT INFORMATION
Practice or PBC Cluster Name
GP or PBC Cluster Clinical Lead Name
Email address
Main contact telephone number
NHS Brent acknowledges this Commissioning Template has been adapted from an original version developed by Brighton and Hove PCT.
20 May 2009 2

B. PRACTICE OR PBC CLUSTER INDICATIVE BUDGET 2009/10
The PBC Cluster is responsible for the following indicative budgets:
Area Value (£)
Acute NHS Hospital Payment by Results,
Accident and Emergency
In-Patient
Out-Patient
Prescribing
Total
The PBC Cluster will monitor activity and finance for the following budgets with the PCT:
Area Value (£)
Direct access (radiology, pathology)
Direct access (other diagnostics including In Health contract)
The PCT is responsible for the following budgets:
Area Value (£)
Acute NHS Hospital – non PBR
Community services
Primary Care Services
Mental health services
Genito-Urinary Medicine (GUM)
Total
20 May 2009 3

ANNEX A: PBC Cluster Planning and Performance Management Process (PBC Objectives 2009/10)
C. PUBLIC HEALTH PROFILE
Describe particular health needs of the practice/locality population and specific disease prevalence rates or admission rates where these are higher than normative levels (compared to rest of London or England) - with reference to the Brent Joint Needs Strategic Analysis. The JNSA is available on the NHS Brent website – click link for further information: http://www.brentpct.org/html/Publications_3448.htm. Also, please refer to the most recent Locality Profile for your Cluster which is designed to guide you more specifically.
Describe any specific needs analysis that has been undertaken in last 24 months or any that is planned in 09/10. This could be either from public/patient surveys or available statistical information.
Other information requirements.
Plans to derive additional information.
20 May 2009 4

D. WHAT ARE THE CLUSTER’S 3–5 YEAR COMMISSIONING GOALS?
Include a longer term vision (3–5 years) for the future nature and shape of services, with specific goals. Goals need to be in alignment with the PCT Commissioning Strategy Plan (CSP) 2008-13, and have outcomes focus. The PCT’s CSP is available on the NHS Brent website. Click here for further information: http://www.brentpct.org/html/Publications_5488.htm. Within this context, Cluster objectives and workstreams will include local innovation to deliver the agreed outcomes.
3-5 Year Cluster Vision:
Goals: Outcomes:
20 May 2009 5

E. WHAT ARE YOUR PLANS TO ENGAGE STAKEHOLDERS?
Identify key stakeholder groups e.g. clinicians, public/patient groups or local government agencies, third sector organisations. Outline plans to engage key stakeholder groups. How will this be reviewed?
Key Stakeholder Groups:
Plans to engage:
Review / feedback processes:
F. PBC INCENTIVE SCHEME PAYMENTS AND INVESTMENT 2009/10
Describe cluster Governance arrangements. Describe the plans for distribution of incentive scheme. Describe the plans for distribution e.g. GP-oriented, Cluster-oriented, or a mix. Itemise investment plans for Cluster level Incentive Scheme payments, indicate plans for establishing a Cluster bank account, and outline the Cluster approval process.
Cluster Governance Arrangements:
Distribution of payments:
Investment plan:
Establishment of bank account:
Cluster Approval Process:
20 May 2009 6

G. COMMISSIONING OBJECTIVES AND WORKSTREAMS
Planning templates have been designed in accordance with the following principles:
Alignment (PCT priorities, outcomes, incentive payments) Enabling local innovation Simplicity Transparency Clarity Outcomes focus (rather than process) Accountability System development
Pre-determined objectives align with NHS Brent’s CSP and Operating Plan, which in turn reflect local and national priorities. Therefore, as well as addressing local health needs, initiatives such as demand management, the WCC Initiatives, the Primary and Community Care Strategy, prescribing, the development of PBC business and engagement systems, and the management of the indicative budget provide the objective subject headings.
Note: Accompanying this document are the Excel sheets – embedded below as a separate document – including templates for each of the following objectives, along with an example of one workstream per objective:
Demand management World Class Commissioning initiatives Ensure financial balance Develop PBC business and processes
Please use these Excel templates to complete your Commissioning Objectives:
20 May 2009 7

PBC CLUSTER SIGN OFF
We are satisfied that the detail in these Commissioning Objectives are correct, robust and deliverable and that all associated services and/or organisations have been consulted and are signed up to the plan.
GP PRACTICE SIGN UP VERIFICATION
Process for and Evidence of GP Practice sign up
Process:
Evidence:
PBC CLUSTER BOARD APPROVAL
Cluster Board Meeting date:
Attendees:
Name Signature Position Date
PCT MANAGEMENT SIGN OFF
Print Name Position Comments DateDirector of Primary Care and Community CommissioningEMTPBC Governance Sub-CommitteePCT Board
PBC GOVERANCE SUB-COMMITTEE COMMENT / FEEDBACK
Date received
Date assessed
Outcome (tick one only)Recommend approval:
Recommend for approval with following requests/caveats:
Recommend not approved for following reasons:
20 May 2009 8

ANNEX B
Budgets and Budget Setting Methodology 2009/2010
1) Budget Scope 09/10 at NHS Brent
2) Background to Healthcare Resource Groups, HRG4 and other 09/10 changes
More detail on the above is shown in Annex B Attachment 3.
3) Budget Methodology – Fair Share v. Historic (actual)
Hospital PbR
Practice budgets are based on 100% historic shares (08/09 activity at 09/10 tariff). Fair shares budgets are due to be calculated and shared for information.
Prescribing
Practice budgets are based on 50% historic and 50% capitation (Age, Sex, temporary resident orientated prescribing units – ASTRO-PUs)
PBC Budget Setting Methodology 2009/10 – PbR
4) Inpatients and Planned Same Day (PSD)20 May 2009
All hospital based care covered by Payment by Results (PbR) including A&E, excluding outpatient diagnostics and procedures
ü
Prescribing ü
Direct access (Pathology, Radiology) Shadow
Diagnostics (including In Health) Shadow
Outpatient Procedures Shadow
Mental Health services To be developed during 09/10
Community services To be developed during 09/10
GUM û
Other non – PBR û
9

Activity
Historic budgets have been set by taking April-December 2008 SUS data (based on HRG 3.5) for inpatients pro-rata to set an expected annual activity level.
Activity at Imperial Healthcare has been increased by 0.7% for projected population growth.
Activity at North West London Hospitals has been increased by £0.8m (1.6%) for projected population growth and seasonal variation. Non-elective activity reductions at NWLH and Imperial have been applied to General Medicine at a net saving of £0.928m (1.8%) due to plans for new patient pathways for intermediate care e.g. Clinicentre.
Pricing
The methodology for pricing activity follows the “Step-by-step guide to the calculation of the 2009-10 national tariff” (DH PbR Team). The 2008/09 HRG3.5 tariff has been uplifted by 1.7% general uplift and an average 3.5% PBR increase (cost shift from MFF).
An increase to specialist top-ups and uplift for CNST (Clinical Negligence Scheme for Trusts) in relevant specialties, notably obstetrics, have also been applied, over all the increase for CNST was £1.2m (1.14%)
5) Outpatients
Activity
Historic budgets have been set by taking April-December 2008 SUS data pro-rata to set an expected annual activity level. Demand management reductions of £0.1m for the planned shift of OP first attendances to primary care have been included in response to planned investments in primary care and community services.
Pricing
2009/10 HRG4 tariffs were applied to the activity by specialty.
6) A & E
Activity is based upon 2008/09 projected outturn and 2009/10 HRGv4 Price.
7) MFF (Market Forces Factor)
Trust specific MFF has been added to the National tariff for the first time in 2009/10. However it is not yet clear whether it is feasible (or appropriate) for MFF to be included within the in-year budget monitoring, hence MFF has not been included in the 2009/10 PBC budgets initially.
8) Scaling to Contract Values
PCT contracts with providers include local developments, population growth, seasonality and other agreed changes. PBC budgets were therefore scaled downwards by 0.02% (£26k) to equal the 09/10 contract values.
9) Budget Setting Methodology – Prescribing
See Annex B Attachment1 for explanation of prescribing budget setting methodology.
10) Resolution of Issues (PbR)
Issues to be resolved Proposed resolution
20 May 2009 10

Activity historically unallocated to Practices.
Set up Practice Unknown budget and allocate costs in year
Data quality issues with direct access, A&E
Incorporate in PBC budgets and provide latest A&E data to PracticesShadow direct access and diagnostic budgets for NWLHT and Imperial in 09/10 and extend as data is available
In Health Diagnostic Develop scheme to utilise In Health Diagnostics contract in 09/10. Include in shadow diagnostic budgets.
11) Approach to management of risk – Acute
• In order to protect Practices from the financial impact of variation in high cost and low volume activity, the Department of Health recommends a PCT-wide risk pool.
• Any activity covered by the risk pool is paid from that central budget instead of the Practice’s own. Practices have collective ownership of any over or underperformance of the risk pool.
• The national guidance suggests that Practices contribute 3-5% of their indicative budget to a risk pool. • In 09/10, the risk pool is proposed at 3.5 % of total Practice budgets (the same as 08/09).
12) Approach to management of risk – Prescribing
• High cost, low volume drugs have a significant and unpredictable impact on Practice budgets.• Removing high cost drugs from Practice budgets and holding in a PCT-wide risk pool gives a
representative and level baseline between Practices.• The list of high cost drugs is based on advice from the PCT Head of Prescribing and agreed with PBC
Leads.• In 2009/10 high cost drug spend is forecast at £4.246m and is included as indicative spend in Practice
budgets. A central risk pool of £0.315m is also held.• As with the acute activity risk pool, Practices have collective ownership of over/under performance of the
high cost drugs risk pool
Approach to measurement and allocation of savings
13) Savings delivered from Cluster commissioning plans (‘freed up resources’)
• Savings will be calculated at the end of the financial year and available for spend in the following financial year on a non recurrent basis in the first year after the saving has been made. Recurrent savings will need to be demonstrated.
• The PCT is committed to ensuring that Practices secure direct benefits from the efficiency savings delivered by participation in PBC and that these ‘freed up resources’ lead to further improvements in local healthcare.
• The approach to freed-up resources is consistent with the guidance from the Department of Health that at least 70% of these resources should be made available to Practices within their indicative budgets for directed reinvestment.
• Preparation of commissioning plans will include drawing up detailed business cases, with a clear and robust framework for the identification of recurrent and non recurrent savings to be agreed with the PCT. See Annexes D & E for business case templates.
• ‘Fortuitous’ savings will not be available for reinvestment.• The PCT reserves the right to withhold the release of savings if savings have been made by stopping
legitimate treatments to patients or as a result of unplanned reasons.
14) Reporting arrangements
• Practices will receive budget summaries during 2009/10 in accordance with a monthly timetable and format agreed with PBC leads.
20 May 2009 11

• The PBC Support Team will work with Practices to refine information and reporting during the year.• Further training in Dr Foster plus targeted analysis is being agreed.• Finance and Information support will be strengthened in 09/10.
15) Incentive Scheme
• Practices participating in PBC are eligible for payments as outlined in the 2009/10 Local Incentive Scheme (LIS).
• The Local Incentive Scheme will pay:- A management allowance on signing off governance agreement of £0.38 per registered patient- A payment of £0.39 per registered patient payable on approval of 09/10 plan- A payment of £1.23 per patient for achievement of Cluster commissioning objectives
• The additional prescribing element of £1 per patient will be based on the existing prescribing scheme.• If Clusters wish to pool their use of the incentive funds, appropriate governance arrangements need to be
in place.• Once these are agreed by the Clusters’ Practices, the PCT will transfer the funds to the Cluster for in-year
management.
16) Financial Governance and Accountability
Financial governance and accountability arrangements will continue to be overseen by the Board sub-committee which will:
• Agree the budget setting methodology• Monitor the risk pool• Review budgetary performance• Review savings achievement• Agree Incentive Scheme payments• Review and approve commissioning plans & business cases (ensuring no conflicts of interest).
20 May 2009 12

Annex B Attachment 1
GP Prescribing Budget 2009/2010
1. GP Prescribing Budgets 2009/20102. Practice Prescribing Budget Setting Method 2009/20103. Practice Budget Setting Methodology steps for 2009/20104. High Cost Drugs (HCDs)5. Timescales for the budgets
1. GP Prescribing Budgets 2009/10
1.1 NHS Brent Prescribing Priority 2009/10Cost effective evidence based prescribing remains a priority in order to ensure appropriate use of the prescribing budget and a financial target based on practices staying within realistic limits of their prescribing budget is included in the Clinical Efficiency Prescribing Incentive scheme (CEPIS) 2009/10 (if Prescribing is included in PBC budget, then the budgetary target does not apply, however, if prescribing is not part of the PBC budget then the financial target is applicable).
1.2 Prescribing Uplift for 2009/2010
For 2009/2010, an uplift of 5% based on December 2008 forecast out turn has been allocated to GP prescribing budget. This uplift includes funds: to manage any risks that arise from changes in list size for in year changes in the prescribing of High Cost drugs (in primary care only) to implement NICE guidance in primary care for implementation of appropriate NSF related prescribing such as Vascular Risk Assessment
To manage the in year (2009/10) growth in primary care high cost drugs spend, a high cost drugs risk pool has been set aside at PCT level – this is out of the 5% uplift.
2. Practice Prescribing Budget Setting Method 2009/2010
Whilst the overall aim of the budget setting methodology must be to achieve fair budgets based on objective assessment of need, it is recognised that it is not possible to achieve this in a totally mechanistic way for a number of reasons.
2.1 Principles
In setting practice prescribing budgets, the PCT should take into account the following underlying principles: Improved quality Increased equity Increased cost effectiveness
2.2 National Recommendation
There is no validated or national/local satisfactory formula which takes into account all the influences on GP prescribing costs at a practice level. To date, the national recommendation has been that prescribing budgets should not be based on or relied upon either on total capitation or total historic budgets, but should be set on a mix of weighted capitation methodology, historic budget patterns and local judgement. The maximum proportion of the budget set on weighted capitation is 50%, as recommended by the validated methodology tool from Prescribing Support Unit (PSU).
It is expected that this formula would not only take into account the historic prescribing patterns of GPs but also recognise the necessity to move towards an allocation that takes into account the need of the patients registered with our GPs and practices receive a “fair share” of the resources available. Currently, this methodology is in line with most other PCTs both nationally and locally.
The nationally accepted capitation weightings is the current needs weighted ASTRO PUs. This is population weighted for differences in prescribing for different age groups, sex and temporary residents) together with the 20 May 2009 13

practice’s Low Income Scheme Index (LISI). LISI is a measure of deprivation based on claims for exemption from the prescription charge on the grounds of low income. It is calculated and distributed by the Prescribing Support Unit (PSU)}. See Annex B Attachment 2.
3. Practice Budget Setting Methodology steps for 2009/2010
The PCT has adopted the Prescribing Support Unit (PSU) methodology (validated tool) for the allocation of prescribing budget to practices. Prescribing budget allocations are based on a 50% historic budget and 50% weighted capitation for 2009/10:
a. The high cost drug budget for primary care (forecast spend) per practice is calculated based on spend at December 08 and is removed from the practice budgets. (Primary HCD are high cost, low volume drugs and have a significant and unpredictable impact on practice budgets- see high cost drugs in Annex B Attachment 2)
b. The historic budget is shared between practices based on their historic budget allocationc. The practice based needs weighted ASTRO-PUs and LISI score are used to share the capitation budget
between practicesd. The 2009/10 practice budget is then calculated by adding the weighted capitation share and historic
share plus the appropriate costs of high cost drugs per practice. In addition to the above, local adjustments need to be made to take into account:
Current variation in practices spend per capitation (low spenders) Practices with nursing homes
Any fortuitous savings made in the prescribing budget in year 2009-10 e.g. reduction in price of generic drugs (category M drugs) or branded drugs (Pharmaceutical Price Regulation Scheme) will not be considered as prescribing savings.
4. High Cost Drugs (HCDs)
At year end (March 2010), each practice’s actual spend on primary care high cost drugs will be confirmed. Where practices have spent less than their allocations, this difference will be deducted from their budget and will be added to the primary care high cost drug risk pool. Where practices have spent more than their allocation, their budgets will be topped up using the primary care high cost drug risk pool.
The HCDs are specialist drugs that are initiated or recommended by secondary care and continued in primary care but have a significant impact on prescribing spend due to their high cost. This list is compiled for budget setting purposes and is not for determining whether a prescriber should take on the responsibility for prescribing.
Please note that this HCDs risk pool does not fund the prescribing of red drugs and PbR excluded drugs. The responsibility for prescribing red drugs lies with the acute trusts (all practices have recently been sent a list). There are special arrangements between the PCT and acute trusts regarding funding of PbR excluded drugs and the funding for this is separate and not part of the prescribing budget. Practices that prescribe these drugs will not be able to claim for additional funds.
20 May 2009 14

Annex B Attachment 2
WeightingsASTRO-PU = age, sex, temporary resident orientated prescribing unit (a more accurate weighting of some of the factors known to influence prescribing costs). This weighting accounts for 35% of variation between practices.
Age Male Values Female Value
0-4 1 0.85-14 1.4 1.2
15-24 1.7 2.125-34 2.0 2.435-44 2.8 3.245-54 4.4 5. 455-64 7.6 7.265-74 10.1 9.675+ 11.8 10.6
Primary Care High Cost drugs
Annex B Attachment 3
Background to Healthcare Resource Groups, HRG4 and other 09/10 changes
20 May 2009
Prescribing costs of the following drugs are adjusted at the end of the financial year. The final list is updated before budget calculations:
Amisulpride, Lanreotide Testosterone Propionate,Anastrozole, Letrozole Testosterone Undecanoate Aripiprazole, Lamivudine, Testosterone,Bicalutamide, Lamotrigine, Tiludronic Acid,Cabergoline, Leuprorelin Acetate Tinzaparin Sodium,Cabergoline, Mazindol, Tizanidine Hydrochloride,Ciclosporin, Modafinil, Tobramycin With Sodium Chloride Colistimethate Sodium, Mycophenolate Mofetil, Tobramycin,,Colistin Sulphate, Mycophenolate Sod, Topiramate,Dalteparin Sodium, Octreotide Acetate Toremifene Citrate,Darbepoetin Alfa, Olanzapine Trientine Dihydrochloride Donepezil Hydrochloride, Ondansetron Triptorelin,,Dornase Alfa, Pancreatin Triptorelin,Enoxaparin, Pergolide Mesilate Epoetin Alfa, Pramipexole,Epoetin Beta, Quetiapine,Exemestane, Quinagolide Hydrochloride,Famciclovir, Riluzole,Famciclovir, Risperidone,Fentanyl Citrate, Risperidone,Fentanyl, Ropinirole,Flutamide, Sevelamer,Galantamine, Sirolimus,Glycopyrronium Bromide, Sodium Clodronate,Glycopyrronium Bromide, Somatropin,Glycopyrronium Bromide, Tacrolimus,Goserelin Acetate, Testosterone Enantate,Granisetron Hydrochloride, Testosterone Esters
15

Healthcare Resource Groups (HRGs) are standard groupings of clinically similar treatments which use comparable levels of healthcare resource. In their most basic form HRGs are groups of ICD-10 diagnoses and OPCS procedures that have similar resource implications.
HRGs offer organisations the ability to understand their activity in terms of the types of patients they care for, and the treatments they undertake. They enable the comparison of activity within and between different organisations and provide an opportunity to benchmark treatments and services to support trend analysis over time.
• HRGs are currently used as a means of determining fair and equitable reimbursement for care services delivered by providers. These consistent 'units of currency' support standardised healthcare commissioning across the service.
• The Casemix Service’s completed major revision, HRG4, is the basis of the 09/10 tariff.
3) What’s new in HRG4?
HRG4 is a major revision increasing the number of groupings from 650 under HRG v3.5 to more than 1,400 and delivers:
A portfolio of new and updated HRG groupings that accurately record patient treatment to reflect current practice and anticipated trends in healthcare
Additional specialty and service coverage, including: Chemotherapy, Radiotherapy, Specialist Palliative Care, Critical Care, Interventional Radiology, High cost drugs, Diagnostic Imaging, Rehabilitation and Multiple Trauma
Setting independence to accurately reflect care given, regardless of where it is delivered Improved complexity and complication splits to better reflect variations in severity ‘Unbundling’ of elements of care that can be identified as additional, exceptional, high-cost or non-routine
treatments: Chemotherapy – regimen and delivery, Radiotherapy – planning and treatment, Interventional Radiology, Diagnostic Imaging (e.g. MRIs/CT), Rehabilitation, Renal Dialysis, Critical Care, Specialist Palliative Care and High cost drugs
Spell based HRGs cover a patient’s whole stay from admission to discharge.
4) Other Changes in 2009/10
• The same price no longer applies to inpatient and day case care. There is a price for inpatient and a separate price for day case care - the planned same day tariff (PSD). In time the PSD will also apply to procedures carried out in outpatient departments.
• A short stay elective tariff (same rate as the PSD) is introduced in 2009-10 to ensure that no perverse financial incentive is introduced between inpatient and day case prices.
• The greater granularity of HRG4 reduces the need for specialised service top ups – these are retained for specialised services for children and orthopaedics only.
• There are more categories of outpatient attendance covering single and multi-professional appointments.
• Diagnostic imaging (with the exception of plain film and equivalents) has been unbundled from outpatient attendance costs and is supported by a non-mandatory tariff.
5) National Tariff Changes in 2009/10
• To reflect changes to pay rates, quality and reform requirements and efficiency requirements the tariff has been increased across the board by 1.7%.
• An extra 7% or £20m has been added to the obstetrics outpatient tariff to support the Maternity Matters aim of reducing late bookings in antenatal care.
• The 1.7% uplift includes an amount (£100m) in respect of increased CNST payments. A further £216m has been added to the prices of individual tariffs.
• Patient Transport Services and the Healthcare Travel Costs Scheme are no longer covered by the national tariff.
• The differential tariff for emergency admissions (which shared the financial impact of increasing numbers equally between providers and commissioners) has been removed.
• The 80/20 payment mechanism for A&E (which funded capacity regardless of activity) has been removed.• Full details of the tariff and the guidance are at the DH website: www.dh.gov.uk/pbr .• More information about HRG4 is available on the NHS Information Centre website: www.ic.nhs.uk 20 May 2009 16

20 May 2009 17

ANNEX CIncentive Scheme 2009/10
Activity Total £ available
% Points
£Allocated
Cluster or GP-Based payment
Terms for Payment
1 Development of approved 09/10 cluster Commissioning Objectives Approved plan with agreed outcomes
19.5 0.39 cluster To be developed according to the templates provided by the PCT and submitted to PCT by 8 May for approval. Recommendation for approval by the PBC Governance Sub Committee on 1 June. To be paid to clusters on approval by June PCT Board.
2 Outcomes of cluster Commissioning Objectives
Quarterly performance monitoring meetings to assess progress against agreed outcomes. Incentive payment to be made, once ratified by the PBC Governance Committee. To be paid to clusters on a quarterly basis.
Demand management 22.5 0.45 cluster Four workstreams; two PCT-wide and two PBC, which contribute to the PCT secondary care activity reductions: New Ops by 811 and reduce emergency admissions by 397.
PBC business systems and engagement development
15 0.3 cluster To be identified through PBC Development Programme. Five workstreams, one to be developed by 8 May as specified on planning templates. Remainder to be developed in-year.
Financial Outcomes. 15 0.3 cluster To be measured at year-end. WCC initiatives 9 0.18 cluster A minimum of one workstream.
Management Allowance Payment will be made at cluster level upon evidence of cluster formation and GP engagement, a signed Governance Agreement by each Cluster, and evidence of satisfactory Governance arrangements in place within each cluster.
Cluster formation articulated and evidence of GP Practice engagement
10 0.2 cluster
Sign off Governance Agreement 9 0.18 cluster
TOTAL 2 100 2 cluster
Prescribing 1 51 1 GP Based upon pre-existing Clinical Efficiency Prescribing Incentive Scheme (detailed on following pages). One-off payment only on achievement of outcomes at year-end to GP Practices.
20 May 2009 18

Annex C: Proposed Incentive Scheme 2009/10 (Prescribing)
Clinical Efficiency Prescribing Incentive Scheme 2009/10
Introduction
The Clinical Efficiency Prescribing Incentive Scheme 2009/10 aims to encourage quality prescribing as well as cost effective prescribing in the selected priority therapeutic areas. The GMS contract, NICE guidelines and new developments in therapy exert considerable upward pressures on costs therefore cost effective evidence based prescribing remains a priority in order to ensure appropriate use of the prescribing budget.
The practices’ achievements in the prescribing targets will be monitored by the Prescribing Team and awards remunerated to practices via the Practice Based Commissioning Incentive Scheme.
Basis of the scheme
There are 13 targets with a total of 55 points in the scheme. The scheme will have two levels of achievement for each prescribing target. The two levels of achievement, rewarded by two levels of points and the value of the award, will be employed to acknowledge the fact that some practices may wish to put more effort into working towards the prescribing targets.
The periods during which the practice’s assessment of the targets is based is detailed in each of the relevant targets eg. The antibiotic targets are assessed in the October 2009-March 2010 period.
We are continuing to drive “clinical efficiency” in prescribing via the scheme this year with the same targets as the previous years and a number of new targets related to NICE guidance, MHRA safety recommendations and repeat prescribing systems. A number of targets reflect the Department of Health “Better Care , Better Value” indicators for PCTs which identify areas for potential improvements in efficiency and form part of a portfolio of NHS performance measures and also areas identified by the National Audit Office as areas for improving cost effective prescribing.
Targets to support Clinical Efficiency and Cost Effective Prescribing
The following targets are included in the scheme:
1. Performance against prescribing budget2. Generic prescribing rate3. Antibiotic prescribing rate4. Top eleven antibiotic prescribing
The revised top eleven NHS Brent antibiotics in line with the main first line antibiotic choices in the Brent and Harrow ‘Management of Infection: Guidance for Primary Care’ revised in December 2008 are:
Amoxicillin Cefalexin Clarithromycin Doxycycline Erythromycin Flucloxacillin Metronidazole Nitrofurantoin
20 May 2009 19

Annex C: Proposed Incentive Scheme 2009/10 (Prescribing)
Penicillin V (also called Phenoxymethylpenicillin) Oxytetracycline/tetracycline Trimethoprim
First line antibiotics excluded from the top eleven list are:
i) Co-amoxiclav (first line for acute pyelonephritis, severe cellulitis, animal bites and human bites)
ii) Ciprofloxacin (first line for acute prostatitis, acute pyelonephritis in penicillin allergy)iii) Azithromycin (for penicillin allergic children with sinusitis/otitis media/pharyngitis/sore
throat/tonsillitis).iv) In line with the national Chlamydia screening programme the use of azithromycin may
increase and if this has a significant impact figures this will be taken into consideration as part of this target.
Cost effective proton pump inhibitor (PPI) prescribing
The prescribing cost rate and the prescribing of low cost PPIs are included in the scheme. The percentage of low cost PPIs is a NHS “Better Care, Better Value” indicator. Generic omeprazole capsules and generic lansoprazole capsules are currently the most cost
effective PPIs available. Generic omeprazole tablets are included as low cost generic PPIs although they are more
expensive than the other generic PPIs available - note that the generic omeprazole 40mg tablets are more than twice as expensive as the omeprazole 40mg capsules (Based on April 2009 Drug Tariff Prices).
Generically prescribed dispersible forms are not classed as low cost PPIs. These should be reserved for those with swallowing difficulties or on PEG feeds.
The PPIs that are only available as branded products are esomeprazole, pantoprazole, rabeprazole, omeprazole dispersible tablets, lansoprazole dispersible tablets and lansoprazole granules.
The National Prescribing Centre has produced a number of useful resources to support the implementation of prescribing and medicines management priorities within the NHS including the review of PPI prescribing which can be accessed via the link below. http://www.npci.org.uk/nsm/nsm/ppis/implement/implement1.php
Oral NSAID prescribing
The prescribing cost rate of NSAIDs is included as a target in the scheme. Further data has been published on the adverse effects of NSAIDs highlighting that the
cardiovascular risks associated with high dose diclofenac and ibuprofen regimens may be associated with a small increased risk of thrombotic events such as heart attack or stroke. The key points from this new data are:- The evidence for diclofenac suggests that it has a thrombotic risk profile similar to that of
at least one coxib (etoricoxib) and possibly others.- There may be a small thrombotic risk for ibuprofen at high doses (e.g. 2400mg/day) but
at low doses epidemiological data do not suggest an increased risk of MI- Naproxen is associated with a lower thrombotic risk than coxibs and epidemiological data
do not suggest an increased risk of MI, however some risk cannot be excluded
Annex C: Proposed Incentive Scheme 2009/10 (Prescribing)
20 May 2009 20

- Ibuprofen, but not rofecoxib, paracetamol, or diclofenac, interferes with aspirin’s ability to irreversibly block COX I enzyme, this might be expected to reduce the protective effect of aspirin on risk for thrombotic events. It would seem prudent to avoid concomitant use of aspirin with ibuprofen until conclusive evidence becomes available to prove otherwise, as there remains uncertainty about whether ibuprofen can negate the effect of aspirin.
- If an NSAID is considered necessary in someone on low dose aspirin then consider using naproxen
Prescribing of NSAIDs and the choice of NSAID should be carefully based on considerations of safety profiles, patient risk factors, side effects (e.g. CV, GI) and patient preference.
The National Prescribing Centre has produced a number of national support materials and a range of resources to support organisations and individuals plan and implement safer ways to prescribe NSAIDs.
The materials collated and presented relate to all NSAIDs but focus, in particular, on safer prescribing of those most commonly used in England and can be accessed on the link below. http://www.npci.org.uk/nsm/nsm/nsaids/library/library_guide_to_nsm.php
Low cost generic statin prescribing
Increasing low cost statin prescribing (prescription items for simvastatin and pravastatin as a percentage of the total number of prescriptions for all statins) is one of the "Better Care, Better Value" indicators.
In NHS Brent, the percentage of statin items prescribed as low cost generic is currently at 73% (July-September 2008) and the national target is 77%.
The National Prescribing Centre has produced support materials to support this work and can be accessed via the link below: http://www.npci.org.uk/nsm/nsm/statins/implement/implement1.php
Prescribing of angiotensin II receptor antagonists
Currently, in NHS Brent the percentage of renin-angiotensin type drugs prescribed as angiotensin II receptor antagonists (AIIRAs) has remained stable at 37%-38% and the national average is currently 28%
The percentage of renin-angiotensin system drugs items for ACE inhibitors and for angiotensin II receptor antagonists is a “Better Care, Better Value “indicator.
NHS Brent spends over £1.6 million per year on AIIRAs which represents 76% of spend on renin-angiotensin type drugs and the percentage of renin-angiotensin type drugs prescribed as AIIRAs is 38% - this is significantly higher than the national average of 28% (as of December 2008).
The aim of this target is to encourage practices to continue the work performed in previous years in reviewing the prescribing of AIIRAs and identify patients where an ACE inhibitor may be more appropriate e.g. in those patients who have not tried an ACE inhibitor first.
Selective serotonin reuptake inhibitor (SSRI) prescribing
This is a new target to monitor the adherence to the locally agreed “Guideline for Pharmacological treatment of Depression in Adults (>18 Years of Age) in Primary Care” produced by the Central & North West London Mental Health Trust, Westminster, Kensington and Chelsea, Brent, Harrow & Hillingdon PCT in March 2007.
These guidelines recommend fluoxetine or citalopram as the first line choice of antidepressants and this target will monitor the percentage of SSRI items that are prescribed as the first line choices.
See Chart 1 illustrating the current pattern of prescribing in GP practices.
Annex C: Proposed Incentive Scheme 2009/10 (Prescribing)
20 May 2009 21

Medicines Reconciliation
NICE and the NPSA have issued guidance to the NHS on how to improve processes that will ensure that any medication patients are taking prior to admission to hospital is documented on admission.
GP practices have an important role to play in ensuring that patient medication records that are passed on to secondary care in response to their patients being admitted, must be accurate and complete. The hospital also has a responsibility to ensure that when patients are discharged, a full and accurate medication record is communicated to the GP.
This audit aims to assess whether the minimum data set for identifying the most accurate list of a patient’s current medicine is communicated on admission and discharge from hospital and any discrepancies are dealt with and resolved.
An audit tool has been provided for practices to use, all results should be submitted using this tool.
Audit on glitazone prescribing
NICE guidance first published guidance on the use of glitazones in 2003 and recent drug safety issues highlighted by the Medicines and Healthcare Products Regulatory Agency (MHRA) in 2008 have required the prescribing of glitazones to be reviewed.
This audit aims to assess adherence to the new safety guidance on cardiovascular risks associated with glitazones and in line with the NICE guidance.
An audit tool has been provided for practices to use, all results should be submitted using this tool.
See Chart 2 illustrating the current pattern of prescribing in GP practices.
Repeat prescribing systems
The National Audit Office report also highlighted the need for robust repeat prescribing systems in minimising the wastage of prescribed medicines.
In addition to this, repeat prescribing is a major part of the work of general practices and as such it is important that it is safe, efficient and user-friendly for both patients and staff.
The repeat prescribing system related target this year aims to bring practice repeat prescribing system policies to a minimum standard to ensure all aspects in the risk management of the process are covered.
A template policy highlighting the issues and points that should be clarified in the policy and new developments such as repeat dispensing and medicines usage reviews are all included.
In practices where the GP processes all repeat prescription requests, as is often the case in single handed practices, it is still recommended that a written practice policy is in place.
Principles of the Clinical Efficiency Prescribing Incentive scheme
1. The Clinical Efficiency Prescribing Incentive Scheme will operate from 1st April 2009 to 31st March 2010 as part of the Practice Based Commissioning Incentive Scheme.
2. NHS Brent reserves the right to withhold payment under the incentive scheme, if savings have been made by stopping legitimate treatments to patients or “windfall” savings such as a significant decrease in list size.
3. The prescribing targets aim to reflect high quality and cost effective prescribing without compromising the needs or care of patients and links clinical and cost-effective performance.
Annex C: Proposed Incentive Scheme 2009/10 (Prescribing)
20 May 2009 22

4. NHS Brent reserves the right to amend the targets or ranges in the light of any unforeseen changes affecting prescribing, such as changes in national or local policy or price for example if there is a significant price reduction within a drug class covered in the scheme that causes a “windfall” achievement of the target.
5. Practice achievements in the prescribing targets will be available around July 2010.6. Awards will be co-ordinated along with the Practice based Commissioning Incentive
Scheme 2009/10.7. An appeals committee consisting of members of the Prescribing & Medicines Management
Committee will be set up in the event of any complaints received about the allocation of points awarded to a practice.
Monitoring of the Scheme
Monitoring of all the prescribing targets except 11, 12 and 13 will be carried out using electronic PACT data analysis at the PCT.
Submissions from the practices using the forms provided are required for targets 11, 12 and 13.
Practices will receive quarterly reports on their progress against the prescribing targets in the scheme. This will include graphs comparing your practice with others across the PCT.As prescribing data is generally available 2 months later, it is envisaged that practices will receive the first quarter report in August 2008.
The tools for auditing and reporting results will be provided by the Prescribing Team.
The deadline for submissions will be 31 March, 2010.
20 May 2009 23

Annex C: Proposed Incentive Scheme 2009/10 (Prescribing)
Clinical Efficiency Prescribing Incentive Scheme 2009/10 Targets
No. Target Description Criteria Achievement V Criteria Excellence V
1 To remain within Practice Prescribing Budget
Spend for 2009/10 to be no more than 2% over budget allocation
1 Spend to be within 2009/10 budget allocation
5
2 Generic Prescribing Percentage of generic items
Monitoring:Level will be measured using ePACT data as an average for Apr 09 to Mar 10This is a DoH / National Audit Office identified area for savings and also one of the London SHA Scorecard indicators for 2009/10
No points if generic rate is below 80%
Rate of 80% and above 1
3 AntibioticsRate of prescribing inItems/1000 Infections STAR PU
Monitoring:
Rate
between 271 and 310Or;
2 Rate of
270 or less3
20 May 2009 24

Level will be measured using ePACT data from Oct 09 to Mar 10This is a DoH/National Audit Office Key Performance Indicator and also one of the London SHA Scorecard indicators for 09/10
Reduce rate by 10% or more compared to same period in previous financial year (Oct 08 to Mar 09)
4 Top 11 Antibiotics Percentage of antibiotic items from NHS Brent formulary of top eleven antibiotics
Monitoring:Level will be measured using ePACT data from Oct 09 to Mar 10Monitoring of the implementation of local antibiotic guidelines – “Management of Infection Guidance for Primary Care”
85 to 89% of antibiotic choice from the Top 11 list
Or
Increase percentage by 5% or more compared to same period in previous financial year (Oct 08 to Mar 09)
2 90% or more of antibiotic choice from the Top 11 list
3
20 May 2009 25

Annex C: Proposed Incentive Scheme 2009/10 (Prescribing)
No. Target Description Criteria Achievement V Criteria Excellence V
5 Proton Pump Inhibitors (PPIs)Prescribing cost (Net Ingredient Cost NIC) per 1000 Gastrointestinal STAR PUs
Monitoring:Level will be measured using ePACT data from Jan to Mar 10
This is a DoH/National Audit Office Key Performance Indicator as part of the “Better Care Better Value Indicators” and also one of the London SHA Scorecard indicators for 09/10
Cost rate between £41 and £48
Or
Reduce cost rate by 20% or more compared to same period in previous financial year (Jan to Mar 09)
2 Cost rate of £40 or less 4
6 Proton Pump Inhibitors (PPIs)Percentage of PPI items prescribed as low cost PPIs
Monitoring:Level will be measured using
Between 90% and 94% of PPI items are generic omeprazole capsules/tablets or generic lansoprazole capsules
1 95% or more PPI items are generic omeprazole tablets/capsules or generic lansoprazole capsules
2
20 May 2009 26

ePACT data from Jan to Mar 10This is a DoH/National Audit Office Key Performance Indicator as part of the “Better Care Better Value Indicators” and also one of the London SHA Scorecard indicators for 09/10
Or Increase percentage by 10% or more compared to same period in previous financial year (Jan to Mar 09)
7 Oral NSAIDsPrescribing cost (Net Ingredient Cost NIC) per 1000 Musculoskeletal STAR PUs
Monitoring:Level will be measured using ePACT data from Jan to Mar 10This is one of the London SHA Scorecard indicators for 09/10
Cost rate between £65 and £112
Or
Reduce cost rate by 10% or more compared to same period in previous financial year (Jan to Mar 09)
2 Cost rate of £64 or less 4
8 Prescribing of Low Cost StatinsPercentage of statin items prescribed as generic simvastatin and generic pravastatin
Monitoring:Level will be measured using ePACT data from Jan to Mar 10This is a DoH/National Audit Office Key Performance
Between 70% and 79% of statin items to be prescribed as generic simvastatin and pravastatin
2 80% or more statin items to be prescribed as generic simvastatin and pravastatin
4
20 May 2009 27

Indicator as part of the “Better Care Better Value Indicators” and also one of the London SHA Scorecard indicators for 09/10
No. Target Description Criteria Achievement V Criteria Excellence V
9 Prescribing of Angiotensin II Receptor Antagonists (AIIRAs)
Percentage of renin-angiotensin type drug items prescribed as AIIRAs
Monitoring:Level will be measured using ePACT data from Jan to Mar 10This is a DoH/National Audit Office Key Performance Indicator as part of the “Better Care Better Value Indicators” and also one of the London SHA Scorecard indicators for 09/10
*Percentage reduction will be calculated from the practice baseline eg. In a practice with 60% AIIRA rate, a 10% reduction would equate to a 6% reduction to 54%
Practice percentage of renin-angiotensin type drug items prescribed as AIIRAs has reduced by 10% to 19%* compared to same period in previous financial year (Jan to Mar 09) where practice percentage is above 28%
3 Practice percentage of renin-angiotensin type drug items prescribed as AIIRAs is below 28%
Or;
Reduced percentage of renin-angiotensin type drug items prescribed as AIIRAs by 20%* or more compared to same period in previous financial year (Jan to Mar 09).
6
20 May 2009 28

10 Selective Serotonin Reuptake Inhibitor (SSRI) Prescribing Citalopram and fluoxetine as a percentage of all SSRI, venlafaxine and mirtazapine items prescribed
Monitoring:Level will be measured using ePACT data from Jan to Mar 10Monitoring of the Implementation of local guidelines – “Guidelines for Pharmacological treatment of Depression in Adults(>18 years of age) in Primary Care”
Between 50% and 59% of items to be prescribed as citalopram or fluoxetine
1 60% or more to be prescribed as citalopram or fluoxetine
3
11 Medicines Reconciliation (NICE/NPSA Guidance – December 2007)Practices to submit results of the audit using the NHS Brent tool. Demonstrates compliance to this NPSA/NICE Guidance and implementation to minimise risks of medication errors
One level of achievement only
Survey or audit to be carried out
8
20 May 2009 29

Annex C: Proposed Incentive Scheme 2009/10 (Prescribing)
No. Target Description Criteria Achievement V Criteria Excellence V
12 Audit on Glitazone Prescribing (NICE Guidance and MHRA Safety Advice)
Practices to submit results of the audit using Brent PCT tool.
Compliance and implementation of both NICE Guidance and MHRA Safety advice
One level of achievement only
Submit results of audit and action plan
6
13 Repeat Prescribing Policy Review
Practices should submit their updated repeat prescribing policy which should incorporate the following:
- Review of the policy/procedure for the security of prescriptions.
- Discharge information regarding communication between primary and
One level of achievement only
Review to be carried out incorporating the various points detailed
6
20 May 2009 30

secondary care.- Controlled drugs.- Training and update on
repeat prescribing – to be given by the prescribing and medicines management team.
- Procedures for blood/pathology tests/results.
The National Audit Office report has highlighted the need for robust repeat prescribing systems in order to minimise the wastage of prescribed medicines.This target aims to target risk management in terms of patient safety.
Total maximum points = 51
20 May 2009 31

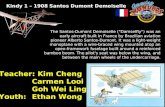
Annex C: Proposed Incentive Scheme 2009/10 (Prescribing)Chart 1
Target 10: Percentage of Citalopram and Fluoxetine Prescribed of all SSRI's, Venlafaxine and Mirtazapine (July-September 2008)
0%
10%
20%
30%
40%
50%
60%
70%
80%
The Eagle E
yeThe V
illage Medical C
entreThe S
tag-Holyrood S
urgeryS
tag Lane Medical C
entreLanfranc M
edical Centre
The Chaplin R
d Surgery
Prem
ier Medical C
entreFalls U
nder Brent P
ctN
easden Medical C
entreP
ark Road S
urgeryC
rest Medical C
entreFreuchen M
edical Centre
Kings E
dge Medical C
entreC
hurch End M
edical Centre
Stanley C
orner Medical C
entreForty W
illows S
urgeryK
enton Medical C
entreB
urnley Practice
The Fryent Way S
urgeryA
ksyr Medical P
racticeA
cton Lane Surgery
The Girton P
racticeP
eel Precinct S
urgeryThe W
illesden Medical C
entreP
reston Medical C
entreW
alm Lane S
urgeryC
halkhill Family P
racticeC
hamberlayne R
d Surgery
Dr S
Ray
Craven P
ark Health C
entreH
azeldene Medical C
entreS
t.Georges M
edical Centre
The Sunflow
er Medical C
entreP
rimary C
are Medical C
entreM
edicareThe W
indmill M
edical Practice
The Law M
edical Group P
racticeS
udbury & A
lperton Medical
Gladstone M
edical Centre
Kilburn P
ark Medical C
entreThe S
urgery Brent Tpct (W
chc)W
embley P
ark Drive M
edicalE
llis Practice
Park H
ouse Medical C
entreThe B
eechcroft Medical C
entreS
t Andrew
s Medical C
entreS
udbury Court S
urgeryThe B
roadway S
urgeryB
rentfield Medical C
entreR
oundwood P
ark Medical
Alperton M
edical Centre
The Sheldon P
racticeC
hichele Road S
urgeryP
reston Road S
urgeryB
uckingham R
d Surgery
The Tudor House M
edicalU
xendon Crescent S
urgeryThe Lonsdale M
edical Centre
Sm
s Medical P
racticeB
rampton H
ealth Centre
Lancelot Medical C
entreS
taverton Surgery
Oxgate G
ardens Surgery
Church Lane S
urgeryThe S
urgeryW
illesden Green S
urgeryFryent M
edical Centre
Willow
Tree Family D
octorsB
lessing Medical C
entreH
arlesden Medical P
racticeThe M
edical Centre
% c
italo
pram
and
fluo
xetin
e pr
escr
ibed
Brent Average = 54%
Incentive Scheme Maximum Points
target ≥ 60%
20 May 2009 32

Annex C: Proposed Incentive Scheme 2009/10 (Prescribing)
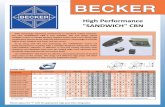
Chart 2
Target 13: Brent PCT Prescribing Cost of Glitazones (April 2006 - Sept 2008)
£95.87£94.80
£101.37
£116.72£117.46
£118.46
£118.87£116.79
£108.59
£103.71
£0.00
£20.00
£40.00
£60.00
£80.00
£100.00
£120.00
£140.00
April-June2006
July-Sep2006
Oct-Dec 2006 Jan-March2007
April-June2007
July-Sep2007
Oct-Dec 2007 Jan-March2008
April-June2008
July-Sep2008
Net
Ingr
edie
nt C
ost p
er 1
000
Endo
crin
e ST
AR
PU
MHRA/CHM advice on rosiglitazone and pioglitazone cardiovascular safety issued in
Dec 2007 and Feb 2008.
20 May 2009 33

ANNEX D
Business Case for use when seeking Investments
Business Case Template
Guidance to help you complete this document is included as hidden text. To see it, click the button on the toolbar or select Tools, Options and the View tab, and in the Formatting Marks section, uncheck the Hidden Text box.
Project Name Project ReferenceSRO (Sponsor)Project ManagerFinancials verified byProject Start date Project completion date
Project Description
Our desired outcome is:
The project objectives that will lead to this outcome are:
KPI Base-line Target
This supports our strategic objectives by:
Benefits
The benefits of delivering this project are:
ANNEX D: Business Case for use when seeking Investments
20 May 2009 34

Options
Good practice relevant to this project includes:
The options that have been considered are:
The preferred option is:
Scope
This project will cover:
This project will not cover:
Delivery
The actions required to deliver the objectives are:
ANNEX D: Business Case for use when seeking Investments
The individuals who will fill the project roles are:Role Dates and FTE Person filling
20 May 2009 35

The dependencies of this project are:
Stakeholders and Governance
The people who need to be involved are:
We will ensure all the necessary interests are represented by:
We discussed the plans with the PBC Executive on (date) and their feedback was:
The actions we took as a result of their feedback were:
ANNEX D: Business Case for use when seeking Investments
Cost
The costs that will be incurred to obtain these benefits are:
20 May 2009 36

The timing of this expenditure will be:
These costs will be met by:
Risks
Risk (to success of project) Likelihood Impact Total
Risks (to the PCT, if the project is not delivered successfully)
Likelihood Impact Total
Risks (to the PCT, of undertaking the project) Likelihood Impact Total
ANNEX D: Business Case for use when seeking Investments
Monitoring and Reporting
The critical success factors for this project are:
The schedule for key project decisions is:Decision Date By
2 – Go live
3 – Project Complete
4 – Benefits Evaluation
The additional control points when the Investment Panel will review progress are:
Control point Date
20 May 2009 37

Document HistoryVersion Status
(Draft or Approved)
Date Author/Editor Details of changes
0.1 Draft Document created1.0 Final1.1 Draft 5/9/08 SD Incorporating PBC Feedback box
and “project start” and “project completion” date.
20 May 2009 38

ANNEX D: Business Case for use when seeking Investments
Business Cases Seeking Investment – Key Stages from early Development to PCT Approval
20 May 2009 39

ANNEX E
PBC Savings Requirements and Spend 2009/10
Paragraph 9.3 of the PBC Governance Agreement describes how freed up resources (FUR) will be generated and be available for PBC re-investment.
PBC Clusters are expected to identify how FUR will be generated by completion of either a business case (where pump-priming investment is required as per Annex D) or savings template (attached in this Annex E where no pump-priming investment is required) which is subject to PCT approval, to enable FUR to be released to the cluster on achievement of the plan.
This section outlines the principal purposes for which non-recurrent PBC savings (FUR) can be utilized by PBC Clusters/practices.
1. Increasing capacity at either cluster or GP practice level
Non-recurrent payments to clinical and non-clinical staff including:
Commissioning or providing alternative services for patients within Brent PCT’s CSP priorities
Creating a range of access options to improve patient access to services e.g. by developing alternative methods of consultation, increasing hours, appointment of additional staff etc.
Encouraging clinical engagement by paying clinical staff to attend meetings and events Supporting high quality care through the commissioning and provision of educational
and training events for staff Increasing quality of practice facilities to support the provision of a greater range of
primary care services (identified through the PCT Primary and Community Care Strategy)
2. Improving engagement and communication with patients, public and local stakeholders
Activities to promote stakeholder engagement or the purchase of material or equipment relating to health education or health promotion for use in the practice. This includes:
Stakeholder events, including cluster patient forums, public/local stakeholder engagement meetings, or expert patient initiatives/programmes
Televisions/Projectors Video players/DVD recorders Audio players/recorders Leaflets and posters Display stands, etc Disseminating health education advice to patients
3. Medical equipment
Material or equipment to be used for the treatment of patients of the practice including:
Diagnostic equipment such as Sphygmomanometers ECG machines Blood testing equipment Sterilisers
ANNEX E - PBC Savings Requirements and Spend 2009/10
20 May 2009 40

Nebulisers Foetal heart detectors Cryothermic probes Defibrillators
4. Improving public areas in practices
The purchase of material or equipment which will enhance the comfort or convenience of patients of the practice. This includes:
a. Furniture, e.g. waiting room seating, surgery couches, etc.b. Furnishings including decorating materials, carpetsc. Security features, e.g. alarms, shutters.d. Heating / air conditioning (excluding maintenance)
5. Improving cluster/practice efficiency
The purchase of computers and related equipment. This includes:
a. Computer hardware 1
b. Computer software 2
c. Fax machinesd. Answering machinese. Photocopiers
1
1. All computer equipment must be purchased through the PCT to ensure system compatibility. A catalogue is available from Brent PCT ICT Department, 020 8795 6676 or [email protected]
2 As above
20 May 2009 41

ANNEX E - PBC Savings Requirements and Spend 2009/10
Savings Template
Guidance to help you complete this document is included as hidden text. To see it, click the button on the toolbar or select Tools, Options and the View tab, and in the Formatting Marks section, uncheck the Hidden Text box.
Project Name PBC Cluster :Project ReferenceSRO (Sponsor) PBC Cluster:Project ManagerFinancials verified byStart date Completion date
Project Description
Our desired outcome is:
The project objectives that will lead to this outcome are:
Key Performance Indicators (KPI)
Base-line
Target
This supports our NHS Brent strategic objectives by:
Benefits ANNEX E - PBC Savings Requirements and Spend 2009/10: Savings Template
20 May 2009 42

The benefits of delivering this project are:
Options
Good practice relevant to this project includes:
Scope
This project will cover:
This project will not cover:
Delivery
The actions required to deliver the objectives are:
ANNEX E - PBC Savings Requirements and Spend 2009/10: Savings Template
Risks
Risk (to success of project) Likelihood Impact Total
20 May 2009 43

Proposed reduction in activity and cost Current Activity
Current Cost
% Saving
Document HistoryVersion Status
(Draft or Approved)
Date Author/Editor Details of changes
20 May 2009 44

ANNEX F
PBC Cluster Governance Arrangements
As each cluster will have their own bank account within 2009/10 into which incentive payments will be made, it is imperative that robust governance arrangements are put in place within each cluster in order to ensure due process, probity, accountability and transparency to both GP Practices and the PCT. These arrangements need to be incorporated within a cluster Governance Agreement between the cluster and GP Practices and signed by all parties. The Governance Agreement needs to include as a minimum the following processes / procedures:
Election and re-election of members to the Cluster Board Process for deciding who will be signatories for the bank account Approval process for payments to be made from bank account Separation of responsibilities between payments and reconciliation Reporting of expenditure to Cluster Board Arrangements for at least quarterly publication of transactions from bank account to
Cluster practices and PCT Clear roles and responsibilities in relation to handling monies. Process for agreeing incentive payments to be made to GP practices. Determination of funds to be maintained at cluster level to support cluster management
and attendance at meetings. Agreement of management expenditure items that will qualify for re-imbursement.
Cluster financial arrangements will be subject to internal audit within the first year in order to ensure due diligence.
Managing PBC Incentive Scheme funds
The purpose of creating a separate PBC bank account is to ensure the PBC cluster is able to draw upon funding to support its management activities and infrastructure expenditure. The Practice Based Commissioning (PBC) Cluster Lead is responsible for establishing a separate PBC bank account for receipt of the PBC Incentive Scheme funding.
Banking Procedures
It is a local decision as to how many and which PBC Cluster members are allowed to requisition funds from the PBC bank account, however there should be a minimum of two signatories on cheques and any withdrawals by other means. The aim should be to balance the availability of PBC Cluster members with the need for proper financial control.
The following PBC bank account details should be submitted in writing to the PCT PBC Manager:
Account name Account number Sort code Authorised signatories
If the PBC Cluster members change, the Cluster Lead must submit a new list of authorised signatories. The PCT advises PBC Clusters to maintain an electronic cash book/file to record all receipts and payments into the PBC bank account. At the month end the electronic cash book/file will be reconciled with the PBC bank statement. Copies of the reconciliations will be
ANNEX F: PBC Cluster Governance Arrangements
20 May 2009 45

provided to the appropriate PCT finance lead monthly. This information will be made available on request to PCT Officers for governance and audit requirements, including compliance with PCT Standing Financial Instructions (SFIs) and Standing Orders (SO). Annex E provides guidance on principal purposes for the available funds.
Managing PBC budgets
The PCT will provide finance leads to support each PBC Cluster/practice to manage their indicative PBC budget and associated activity. The specific named leads will be notified in year.
During 2009/10, all PBC Clusters/practices will receive the following reports according to an agreed format, on a pre-determined date each month:
Data validation file (at General Practice level) Activity and expenditure report (at General Practice level and PBC Cluster level)
In addition, all PBC Clusters/practices will be issued with a login and password and receive training in the Dr Foster application https://da.drfoster.co.uk. Additional support will be made available by PCT staff. Refer to Annex I for further details on PBC support arrangements.
20 May 2009 46

ANNEX G
Roles and Responsibilities
PCT Responsibilities and Support for Commissioning
The PCT is committed to supporting PBC activities and to working with practice based commissioners to provide the tools and support they need to effectively fulfil their commissioning responsibilities.
Responsibilities
The schedule on the following pages details, as part of this agreement, the specific responsibilities of the PCT and practices in relation to PBC in 2009/10. The schedule covers Financial Management, Information Management, contract negotiation and performance management, strategic commissioning, and public health.
PBC Development Team
In order to support these commitments and to enhance the level of commissioning support to PBC the PCT will continue to provide a PBC development team within the Primary and Community Commissioning Directorate. A second PBC development manager was appointed during 2008/09 and this team will be further strengthened by the appointment of a WTE assistant director who will focus on the development of PBC in 2009/10. The assistant director will be accountable to the Director of Primary and Community Commissioning. The team will be supported by one PBC Development administrator/PA. The PCT will continue to support PBC through its funding of five cluster-based PBC administrators (job description is included in this annex), who will be line-managed by their cluster-based management leads, and accountable to the PCT through the PBC Development Managers, and will thus be subject to a joint (PBC/PCT) annual appraisal.
The PBC Development Team has a specific remit to support and ensure the full and effective development of PBC in Brent and to ensure cluster delivery of:
Cluster Objectives to include:
- Demand management initiatives to create more and better local services in reducing demand on secondary care
- Manage within financial balance- Develop PBC systems and processes- Contribute to CSP priorities
In addition, support will be offered from the following directorates:
Finance, as part of its restructuring plan for 2009/10, has appointed an Assistant Director with lead responsibilities for PBC who will work with the PBC Development Team to provide finance support and advice, attendance at meetings and a consistent reporting schedule which meets the needs of the clusters. The department will continue to offer a Finance Lead for each cluster to provide financial and activity analytical support.
20 May 2009 47

ANNEX G – Roles and Responsibilities
Public Health. Under the proposed restructure for NHS Brent Public Health will appoint a new Assistant Director of Regeneration and PBC. This post will share responsibility with the other assistant directors within Public Health for offering consultation on health needs assessment, health intelligence, evidence based health care, development of quality care, general leadership and strategic overview and advice on health promotion. This consultation will be equivalent to three sessions, or one and a half days per week.
Strategic commissioning will provide support for the development of community and primary care based pathways. Their work plan will be agreed by practice based commissioners.
Information, as part of its restructuring plan for 2009/10, will appoint a PBC Information Manager and a PBC Analyst to capture, manage, analyse and communicate data regarding PBC using the Dr. Foster system.
PBC Responsibilities and Support for Commissioning
Representing Practice Based Commissioning in Brent, the Federation Council is committed to supporting PBC activities and to working with both the PCT and the wider health community in order to effectively fulfil its responsibilities. To this end, each Federation Council member will be by appointed on an annual basis and their performance subject to review before reappointment.
Note: For particular reference to practice based commissioners’ roles and responsibilities, please refer to:
Service Level Agreement of the Federation Council and NHS Brent (Annex G) PBC Executive Committee Terms of Reference (Annex H) Federation Council’s Code of Conduct (Annex H) Federation Council’s Portfolio of Responsibilities (Annex H)
Meetings
2. The Federation Council, comprising two leads from each cluster, will continue to meet once monthly. It is hoped that this will enable PBC leads more influence in planning, SLA negotiating and monitoring, and in the development of new pathways. A basic Service Level Agreement is included on the pages to come for quick reference.
3. The PBC Executive Committee, comprising PBC representation from Federation Councillors and cross-directorate PCT membership including Finance, Strategic Commissioning, Public Health, and Primary and Community Commissioning, will continue to meet monthly. The Director of Primary and Community Commissioning will chair the meeting.
4. The PBC Executive Committee meets monthly to:
Consider draft PBC budget methodology Review main SLAs Review joint arrangements with the local authority Review health needs assessment and strategy
ANNEX G – Roles and Responsibilities
20 May 2009 48

Review in year performance of all aspects of PBC plans Oversee demand management plans Review existing pathways Consider development of new pathways Review adequacy of PCT support Oversee the PBC Development Programme
20 May 2009 49

PCT Responsibilities PBC Responsibilities PCT support Volume of PCT Support
Fina
ncia
l Man
agem
ent
Maintain financial balance annually Hold indicative budgets - responsibility for ensuring a break-even, or surplus position. Inform PCT of kind of reports required.
Respond to PBC information reporting request.
Provide a named finance lead for each cluster.
Provide PBC leads with monthly financial and activity reports
Meet practice based commissioners at least monthly , to review progress and budget performance
Undertake a full budget holder role in relation to:
Agreeing / monitoring budgets. Coding and paying invoices. Support SLA negotiations with Trusts. Validation of financial information and forecasting
financial position. Ensuring significant budget variances are
promptly identified, and appropriately reported.
Hold indicative budgets therefore responsible for monitoring budget spend and taking action, which may include establishing a recovery plan, if budgets are overspent.
Disseminate and discuss financial activity reports within clusters to GPs and other clinical colleagues.
The PCT will provide PBC leads with monthly financial and activity reports to a pre agreed timetable and in a format requested by PBC.
20 May 2009 50

PCT Responsibilities PBC Responsibilities PCT support Volume of PCT Support
Issuing Standard Financial Instructions and Standing Orders, and monitor compliance.
Comply with Trust Standard Financial Instructions (SFIs) and Standing Orders (SOs).
All documentation including guidance on PCT intranet or PCT website and made explicit as to whereabouts.
Providing financial assessment and input into PBC commissioning and provider plans.
Producing annual commissioning plans. PBC Development Team.
Info
rmat
ion
Man
agem
ent Monthly validation of contract activity. Ascertain which areas are most worthy of time
spent in view of payback. Monthly validation of contract activity at agreed cost threshold/ clinical areas.
To agree with practice based commissioners a robust validation process including validation areas.
Liaison with Trusts in relation to disputed activity on SUS.
Liaison with GP Practices and PCT SLA Team on clinical validation issues to be raised with providers.
PCT Information Team will collate queries from practice based commissioners on a monthly basis and liaise with Trusts to resolve.
20 May 2009 51

PCT Responsibilities PBC Responsibilities PCT support Volume of PCT Support
Produce monthly information pack in pre agreed format with PBCers for practice based commissioners:
Interrogate information from Dr Foster and hospital data to inform service redesign initiatives.
Provide suitable training for practice based commissioners to utilise Dr Foster.
Production of statutory information returns to the Department of Health e.g. Operating Plan, LDP Trajectories.
n/a n/a
SLA
Neg
otia
tion
and
Man
agem
ent
Produce annual Operating Plan (Commissioning Plan) for the PCT.
Produce PBC Plans in alignment with Operating plan and CSP.
PBC Team strategic commissioning, finance and information teams.
Negotiate, agree and manage SLAs with identified acute trusts in line with national and local planning guidance.
Identification of changes required in SLAs
PBC representation at in-year monitoring meetings with Providers
PBC Team strategic commissioning, finance and information teams.
20 May 2009 52

PCT Responsibilities PBC Responsibilities PCT support Volume of PCT Support
Promote and support collaborative working with partner PCTs in line with London-wide lead commissioning arrangements.
n/a n/a
Ensure that appropriate activity / finance performance management arrangements are in place for all commissioned services.
Identify commissioning/ contracting leads for acute and community contacts plus any new providers through Any Willing Provider or other procurement processes.
PBC Development team.
Perf
orm
ance
Man
agem
ent
Ensure appropriate systems in place to monitor host Trust non-financial performance against relevant national and local targets – e.g. waiting times, infection rates etc.
PBC representation at in-year monitoring meetings with Providers.
Understand the impact of performance against targets for consortia / practice population.
Strategic Commissioning
Report performance against targets to relevant PCT and SHA. Ensure reports sent through to relevant personnel.
Through PBC reps – ensure 2 way communications.
n/a
20 May 2009 53

PCT Responsibilities PBC Responsibilities PCT support Volume of PCT Support
Agree plans to address performance variance against targets with Trust as required.
Leads to participate n/a
Stra
tegi
c co
mm
issi
onin
g
PEC and PBC Exec to agree annual clinical and service redesign priorities following PCT liaison with practice based commissioners.
Leading service and pathway redesign to achieve demand managementImplementing the Primary and community care strategy.
Strategic commissioning support. Primary care strategy and development support.
PCT attendance at practice based commissioner meetings (by invitation).
Performance Management of demand management and primary and community strategy implementation and CSP priorities.
To develop and implement cluster commissioning objectives.
PBC Development team, finance, PH and strategic commissioning.
Ensure all procurements follow PCT guidance and due diligence.
Follow PCT guidance and ensure due diligence and ensure transparent audit trail.
Provide procurement expertise and advice.
20 May 2009 54

PCT Responsibilities PBC Responsibilities PCT support Volume of PCT Support
Invo
lvin
g Pe
ople
Supporting community liaison and engagement to develop a two-way dialogue to inform commissioning plans and needs assessments.
To work with the PCT’s PPI Team and the PBC Team and PBC development programme to draw up an action plan for actively engaging patients, the public and local stakeholders across the Cluster.
To ensure that systematic processes are in place to capture and measure the patient experience of services commissioned and/or provided.
Advice provided by PCT PPI Team.
Publ
ic H
ealth
To assess the health needs of the people of Brent and at cluster level by improving and updating cluster profiles.
To assess the health needs of their populations – by using available data on the health and health needs and asking questions where there are gaps.
Public Health team will work with practice based commissioners to profile practice/consortia populations to establish patterns of disease, inequalities etc.
20 May 2009 55

PCT Responsibilities PBC Responsibilities PCT support Volume of PCT Support
To ensure that services commissioned are informed by health need, are clinically and cost effective, and reduce health inequalities.
To ensure that services commissioned:
Meet the identified health needs of the local population.
Are of proven clinical effectiveness. Result in demonstrable improvements in
the health of their population and reductions in health inequalities.
The Public Health team will work with clusters to develop mechanisms for monitoring outcomes at a local level and identification of metrics that are meaningful at a local level.
The Public Health team will provide advice in carrying out Equality Impact Assessment on new service developments, policies etc.
The Public Health team will profile cluster populations to provide ethnic monitoring data to enable equity of access of services to be monitored.
20 May 2009 56

ANNEX G – Roles and Responsibilities Continued (Federation Council / NHS Brent SLA)
The Federation Council - Service Level Agreement between NHS Brent and the Practice Based Commissioning Executive Committee
1 Introduction
1.1 Practice Based Commissioning (PBC) has been introduced nationally as one of the mechanisms to improve patient care by involving front line clinicians in commissioning decisions. Within NHS Brent, a Practice Based Commissioning Executive (PBCE) will continue to provide a clinically led forum to oversee the implementation of PBC in Brent. The Practice Based Commissioning Executive will comprise PCT Officers and Brent Federation Council representatives, as mentioned in Annex G.
2 General Information
2.1 The Agreement is made between NHS Brent (The Commissioner) and the Practice Based Commissioning Executive Federation Member (The Provider), AN Other.
3 Definitions
3.1 The Organisation: NHS Brent
3.1.1 The Commissioner: NHS Brent’s Primary Care and CommunityCommissioning Directorate
3.1.1.1 The Provider: Practice Based Commissioning Executive Federation Member, AN Other.
4 Purpose and Period of the Agreement
4.1 The purpose of the Agreement is to set out the responsibilities of the Organisation, Commissioner and the Provider.
4.2 The Agreement is renewable on an annual basis, and upon review of performance, unless terminated earlier in accordance with the provision below, or varied in accordance with the provision below.
5 Responsibilities of NHS Brent
5.1 To maintain current Terms of Reference for the Practice Based Commissioning Executive as set out in Schedule 1 (Note: For the purposes of this Governance Agreement, please refer to Annex H: Terms of Reference).
5.2 To organise the Practice Based Commissioning Executive monthly meetings.
5.3 To provide agreed information within mutually agreed time scales.
5.4 The Organisation will employ appropriately qualified and experienced Practice Based Commissioning Executive Federation Members to maintain the Service.
20 May 2009 57

ANNEX G – Roles and Responsibilities Continued (Federation Council / NHS Brent SLA)
5.5 Practice Based Commissioning Executive Federation Members will also receive written confirmation of their role and the expectations of the Organisation as specified in Schedule 3 (Note: For the purposes of this Governance Agreement, please refer to Annex H: Terms of Reference - Portfolio of responsibilities for Practice Based Commissioning Federation Members).
5.6 Practice Based Commissioning Executive Federation Members should be offered suitable training and support to enable them to carry out their role effectively.
5.7 All Practice Based Commissioning Executive Federation Members will have been appropriately vetted by their Cluster and the Organisation and hold accredited qualifications where appropriate. It is the responsibility of the Clusters and the Organisation to judge the suitability of Practice Based Commissioning Executive Federation Members.
6 Responsibilities of the Service
6.1 To be available for a minimum of 2.5 days per month, equivalent to five 3-hour sessions to carry out responsibilities and duties of the role in accordance with paragraph 5.5.
6.2 To attend and contribute at meetings, including Practice Based Commissioning Executive monthly meetings, SLA contract review and monitoring meetings, PCT-led meetings and other PBC relevant events as required.
6.3 To take on a portfolio of lead responsibilities covering specific SLAs, care groups and pathways as specified in Schedule 3 (Note: For the purposes of this Governance Agreement, please refer to Annex H: Terms of Reference - Portfolio of responsibilities for Practice Based Commissioning Federation Members).
6.4 To read, review and comment on documents, reports and data within agreed timescales.
6.5 To maintain active and positive communication with the PCT, Federation Council, Clusters and General Practices on all PBC related developments.
6.6 To satisfy the Federation Council Code of Conduct as set out in Schedule 2 (Note: For the purposes of this Governance Agreement, please refer to Annex H: Terms of Reference – Federation Council Code of Conduct).
6.7 To satisfy performance standards as set out in Schedule 1(Note: For the purposes of this Governance Agreement, please refer to Annex H: Terms of Reference – Practice Based Commissioning Executive Committee Terms of Reference).
7 Funding
7.1 Funding is for a specific period as set out in paragraph 4.2.
20 May 2009 58

ANNEX G – Roles and Responsibilities Continued (Federation Council / NHS Brent SLA)
7.2 The annual contract value per individual Practice Based Commissioning Executive Federation Member will not exceed £12,000 per annum (excluding on-costs).
7.3 Payment will be made monthly on a basis of 1/12 th of annual contract value subject to satisfactory performance standards.
7.4 It is a requirement of the Agreement that the Provider immediately informs the Commissioner of any significant change(s) in its circumstances, which may materially affect the ability of the Provider to supply the Services covered by this Agreement.
7.5 NHS Brent has the right to suspend funding in the event of:
7.5.1 A failure on the Provider to fulfil the terms of this Agreement.
8 Equal Opportunities
8.1 The Organisation is required to have an Equal Opportunities Policy outlining principles of Equal Opportunities.
8.2 The Organisation will ensure their recruitment procedure for any new Practice Based Commissioning Executive Federation Members will adhere to the equal opportunities policy.
9 Health And Safety
9.1.1 The Organisation is required to have a written policy on Health and Safety and this should be made available on request.
10 Confidentiality
10.1 The Organisation and its staff may be receiving personal and confidential information from service users. The Organisations’ staff must not disclose any information which comes into their possession in the course of providing the Service except as may be required by law, or where the express consent of the individual concerned, has been obtained. This includes information acquired through complaints procedures.
10.2 The Organisation will ensure policies and procedures are in place to prevent unauthorised disclosures. Disclosure of information which has not been authorised will be considered as a serious breach of the terms of this Agreement and could result in the suspension of payment and as outlined in paragraph 7.5 or termination of the Agreement as outlined in paragraph 14.
11 Statutory Requirements
11.1 The Organisation shall conform to all existing and new legislation which may be applicable to this Agreement.
Variations in the Terms of the Agreement
20 May 2009 59

ANNEX G – Roles and Responsibilities Continued (Federation Council / NHS Brent SLA)
11.2 Variations in the terms of this Agreement will be agreed by the Commissioner and Provider and subsequently confirmed in writing by NHS Brent. Variations to the Agreement will require a minimum of 28 days notice.
12 Performance Management
12.1.1 The Director of Primary Care and Community Commissioning will review the level of performance by the Provider during individual quarterly review meetings.
12.2 If the Commissioner believes that a Practice Based Commissioning Executive Federation Member(s) level of performance is unsatisfactory has broken the terms of this Agreement it will provide details of the issue to the cluster board or consortia management for action.
12.2.1 Should a Practice Based Commissioning Cluster / Consortia agree unanimously that their nominated Federation Council representative’s level of performance is unsatisfactory, they have the right to request their removal from the Federation Council and subsequently Practice Based Commissioning Executive.
13 Termination of the Agreement
13.1 The Agreement may be terminated immediately by the Commissioner with the agreement of the PCT Chief Executive in the event of any of the following:
13.1.1 A permanent cessation of the Provider.13.1.2 A persistent failure to fulfil the terms of the Agreement.13.1.3 A serious breach of the terms of the Agreement.13.1.4 The performance of the Provider is unsatisfactory and documented to be so.13.1.5 There is a substantial change to the service which the Commissioner has not
approved.
13.2 The Agreement can otherwise only be terminated by either party on written notice of three months.
14 Additional Notes
14.1 NHS Brent must protect the public finances under its jurisdiction and so may use the information the Organisation has provided under this Agreement to prevent and detect fraud. NHS Brent may also share this information for the same purposes with other organisations.
14.2 The Organisation is expected to consult with PCT officers about any publicity, whether adverse or positive for any work funded through PCT Service Level Agreements. The Organisation is expected to take full advice on the handling of such matters from the PCT’s Communications department.
15 Schedules
The following Schedules form part of this Agreement (Refer to Annex H: Terms of Reference):
20 May 2009 60

ANNEX G – Roles and Responsibilities Continued (Federation Council / NHS Brent SLA)
15.1.1 Schedule 1: Practice Based Commissioning Executive Terms of Reference (Note: For the purposes of this Governance Agreement, please refer to Annex H: Terms of Reference – Practice Based Commissioning Executive Committee Terms of Reference)
15.1.2 Schedule 2: Federation Council Code of Conduct (Note: For the purposes of this Governance Agreement, please refer to Annex H: Terms of Reference – Federation Council Code of Conduct)
15.1.3 Schedule 3: Portfolio of responsibilities for Practice Based Commissioning Executive Federation Members (Note: For the purposes of this Governance Agreement, please refer to Annex H: Terms of Reference - Portfolio of responsibilities for Practice Based Commissioning Federation Members)
16 Declaration
16.1 I have read and fully understand this Agreement. I have undertaken appropriate consultation within my respective organisation and I am empowered to agree the terms and conditions which have been negotiated.
17 Signed on behalf of NHS Brent
SIGNATURE
NAME Jo Ohlson
POSITION Director of Primary Care and Community Commissioning
DATE
18 Signed on behalf of Practice Based Commissioning Executive
SIGNATURE
NAME
PBC CLUSTER
DATE
April, 2009
20 May 2009 61

ANNEX G: Roles and Responsibilities Continued – Job Profile PBC Administrator (cluster-based)
Job Profile: Practice Based Commissioning Administrator
Post: Practice Based Commissioning AdministratorResponsible to: Practice Based Commissioning Cluster Lead Accountable to: Director Primary and Community Care CommissioningLocality base: Practice Based Commissioning Cluster GP Practice Band: 5Hours: 37.5 Hours Profile
The post holder will be responsible for supporting the cluster board and the individual GP practices with the development and project management of Practice Based Commissioning, demand management initiatives and the implementation of integrated pathways of care across Brent. The post holder will be required to support the PBC Cluster and the Cluster Lead in the successful implementation of Practice Based Commissioning.
This role requires excellent, co-ordination and organisational skills to ensure inclusive decision making is achieved and nationally determined timescales and targets are met at a local level.
High-level partnership working and communication skills are also essential in ensuring the best outcome is delivered for the Cluster and the PCT.
The post holder will assist the PBC Cluster lead to write business cases and manage them through the approval process. Upon PCT approval, the post holder will ensure the PBC Cluster works effectively to implement the business cases and will also be required to produce regular progress reports to the cluster lead and cluster at scheduled meetings.
The post holder will ensure a PBC dataset is received and acted upon and that activity is monitored and fed back in an appropriate and timely manner to the cluster members. The post holder will work closely with clusters and practices commissioning managers to ensure intelligence and data from practices is used to inform the strategic commissioning function as required.
Key Responsibilities and Duties
1. Support the cluster lead in coordinating complex projects such as care pathways, linking in with the appropriate individuals and organisations, and providing support to practices to modernise and implement the service developments and Primary Care Schemes arising from the Primary and Community Care Strategy and other Government and local targets.
2. Support the Cluster in the planning and coordination of PCT led initiatives coordinating steering groups, project management process and timetable.
20 May 2009 62

ANNEX G: Roles and Responsibilities Continued – Job Profile PBC Administrator (cluster-based)
3. Support the cluster to produce regular activity reports and evidence from the practices within the cluster as required by the PCT in developing the performance management framework.
4. Set up and maintain systems to monitor and evaluate the implementation of approved commissioning objectives.
5. To lead the co-ordination of information and the preparation of the cluster commissioning plan.
6. To produce reports for the clusters using excel and power point, clinical systems and Dr Foster for Cluster papers, Board Papers, Presentations and Project Management Reports.
7. To work closely with the Performance and Information team and produce data as required; producing monitoring reports including graphs, timelines, and data tables that summarise progress against key actions and project future performance.
8. To co-ordinate the cluster budget management review process. Enabling budgets to be understood and reviewed by the PBC leads and practices within the cluster.
9. Develop and implement a framework for agreeing practice savings plans and managing the end of year process of establishing the level of savings to be available after assessment of the tPCT’s risk pool.
10. Ensure that services which practices plan to provide under PBC, have robust business plans which support them.
11. Responsible for ensuring that PBC leads have a suitable system in place for managing their indicative financial budgets for PBC.
12. Maintain systems to monitor performance figures, for the Department of Health, when necessary.
13. To communicate frequently and receive and deal with all incoming communications ensuring that they are answered quickly and politely.
14. To support and encourage practices to develop an understanding of data systems such as Dr Foster, EMIS, VISION, etc to provide activity reports. Retrieval and validation of data i.e. public health statistics or activity reports.
Administrative Responsibilities
1. The post holder must demonstrate the ability to be a team member within a multi-disciplinary setting and to contribute effectively from an administrative standpoint.
2. The post holder must deliver an effective and highly competent level of administrative support to the Cluster.
3. Create excellent working relationships and promote regular liaison between GP surgeries working closely with practice managers, general practitioners, other health or social care workers, allied healthcare professionals, patients, carers and stakeholders as required.
4. Networking with external agencies. 5. Co-ordination of and attendance at regular cluster meetings relevant to
20 May 2009 63

ANNEX G: Roles and Responsibilities Continued – Job Profile PBC Administrator (cluster-based)
the work of P and local education. This includes circulation of papers, preparation of agendas, taking minutes, book venues, facilities and catering as required.
6. Drafting of written correspondence. 7. To prepare and type letters which involve explaining complex issues to
practices and clusters, reports and spreadsheets using the appropriate IT package.
8. Being aware of other operational systems within the service and covering colleagues’ absence.
9. To support the teams in developing effective administrative systems.
General
This job description is a reflection of the current requirements of the post. As the Primary Care Trust is an evolving organization the duties may change over time. Any significant change will be discussed with the post holder before implementation.
Notifying Cluster Lead of any time management issue which is affecting your ability to achieve deadlines.
The post holder will be required to carry out any other duties, as defined by the cluster lead to ensure smooth and effective working within the team.
Confidentiality
The post holder must observe and maintain the confidentiality of information relating to patients, staff cluster, practices and other Trust business in accordance with the Data Protection Act (1984, 1998).
Health and Safety
Employees must be aware of their responsibilities under the Health & Safety at Work Act (1974), to ensure the agreed safety procedures are carried out to maintain a safe environment for employees and visitors. Equal Opportunities
The aim of the Trust’s policy is to ensure that no job applicant or employee is discriminated against either directly or indirectly on the grounds of race, colour, creed, sex, disability, marital status, age nationality or ethnic origin. The Trust commits itself to promote equal opportunities and will keep under review its policies, procedures and practices to ensure that all users and providers of its service are treated according to their needs. The policy applies to all staff working within the Trust.
20 May 2009 64

Person Specification
Experience
Essential
A minimum of 3 years’ experience at administration or middle management level
Evidence of effective partnership working with NHS and/or Local authority partner organisations
Partnership working between NHS organisations Broad experience as an administrator or manager Understanding of commissioning budgets or budget management
responsibility Project management
Desirable
Strategic planning A minimum of 2 years’ experience in primary care development (ideally
general practice) or commissioning roles
Qualifications and Knowledge
Essential
Degree educated or equivalent Competence in software packages word processing and Excel spreadsheets, Evidence of continuing professional development Understanding of relationships between NHS and its partners. Understanding of the current and future direction for commissioning in the
NHS, the reform agenda and commissioningDesirable
Experience of working with EMIS, VISION, Dr Foster Up-to-date knowledge of relevant legislation plans and guidance Current thinking in relation to good governance in the NHS
Skills
Essential
Project management skills
20 May 2009 65

Excellent analytical and report writing ability. Ability to develop effective relationships across primary care. Management of administrative processes with excellent organisational
abilities Evidence of effective prioritisation and time management skills Ability to work unsupervised and represent the organisation Ability to manage workload and meet deadlines consistently Minute taking
Desirable
Balance conflicting and competing interests
Personal Attributes
Essential
Excellent ability to communicate to a wide range of people Authority and self belief Enthusiasm Effective team player Determination
October 2008
20 May 2009 66

ANNEX H
Terms of Reference
On the following pages are terms of reference for each of the major stakeholder groups currently serving practice based commissioning at NHS Brent. Also included is an organisational chart showing accountability and lines of communication among these groups and as they relate to the NHS Brent’s Board of Directors.
Terms of Reference included are:
PBC Governance Sub-Committee
PBC Executive Committee
PBC Federation Council
PBC Development Programme Steering Committee
PBC Demand Management Committee
These terms of reference describe the purpose and structure of each committee and document how the scope of each charter will be defined, developed, and verified. They also name the stakeholders, roles and responsibilities of each.
20 May 2009 67

20 May 2009 68

ANNEX H: Terms of Reference (PBC Governance Sub-Committee)
Practice Based Commissioning Governance Sub-Committee
Terms of Reference
1. Constitution
The PBC Governance Sub-Committee is established as a Committee of the PCT Board and has no executive powers other than those specifically delegated in these terms of reference as set out in paragraph 7.
2. Chair
The Chair shall be a Non-Executive Director of the PCT.
3. Membership
The membership shall be:
Non-Executive Directors x 2 Director of Primary Care and Community Commissioning Professional Executive Committee (PEC) Co-Chair Director of Public Health Director of Finance Director of Strategic Commissioning LMC as an observer Directors may designate representatives as necessary
4. Frequency
Meetings shall normally be bi-monthly but will be kept under review and will have a more frequent pattern as required.
5. Quorum
A quorum shall be a Non-Executive Director and two Directors.
6. Authority
The Committee is authorised by the Board to consider any activity within its terms of reference. The Panel is authorised by the Board to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary.
7. Responsibilities
Practice based commissioning places primary care professionals, working alongside secondary care clinicians and other primary and allied health professionals, at the heart of decision making to commission services for their local population. PCTs continue to be legally responsible for finances and contracting with providers, the overall commissioning strategy and for the
ANNEX H: Terms of Reference (PBC Governance Sub-Committee)
20 May 2009 69

implementation of PBC. By devolving indicative budgets to practices that treat and refer patients, GPs and other primary care professionals are being encouraged to manage referrals and to commission and redesign services in a way that are cost effective and convenient for patients.
7.1 The responsibilities of this Committee are as follows:
1. To oversee PBC development process.
2. To authorize and monitor the PBC development, local Governance Agreement and ensure its alignment with national guidance and local policies, including the Commissioning Strategic Plan and PCT Operating Plan. Ensure sufficient time to consult and ensure ownership within the development of the Governance Agreement.
3. To authorise PBC budget methodology and receive appropriate in year reports on PBC/Clusters performance.
4. To oversee monitoring of PBC/Clusters performance in year including receiving exception reports and reports on corrective action.
5. To assure the process of assessment and approval of practices'/ consortia annual commissioning plans and business cases.
6. To oversee the delivery of the PBC local incentive scheme for 2008/09 and the approval of practice payments under this scheme.
7. To ensure value for money and clinical corporate governance arrangements are sound and appropriate in agreeing any proposals for service change.
8. To provide guidance on public consultation, conflicts of interest and tendering requirements resulting from proposed service changes.
9. To promote PBC within the PCT and stakeholders.
10. To advise the PCT Board of PBC and resource implications for commissioning support and infrastructure and to ensure alignment with the PCT’s priorities and objectives.
7.2 In order to fulfil those responsibilities the committee will:
1. Receive and review reports from officers on the above.
2. Review and agree budget methodology.
3. Approve a planning cycle for PBC commissioning aligned with NHS London’s overall timetable.
4. Approve a process for approving for business cases including assessment criteria.
5. Approve the criteria and mechanisms by which commissioning plans are assessed and approved and assure the Board these criteria and mechanisms are adhered to.
20 May 2009 70

ANNEX H: Terms of Reference (PBC Governance Sub-Committee)
6. Approve delegation arrangements as required to ensure the business cycle is completed in a timely manner. For the approval of commissioning plans between planned PBC Governance meetings, the PBC Governance Committee Chair, a second Non-Executive Director and the Director of Finance and Performance can make decisions based on a report from the assessment panel.
7. Provide minutes and committee reports to the PCT Board detailing the decision-making of the group.
8. Notify Brent Local Medical Committee of committee assessments and decisions and requests from other representative committees if appropriate.
9. Provide advice and to identify possible support for business cases from other existing independent contractors with a view to them being considered by the relevant practice based commissioners.
10. Take all reasonable steps to ensure any potential conflicts of interest within the above processes are identified and addressed appropriately.
8. Reporting Arrangements
In making decisions on behalf of the PCT Board, the Committee should record all decisions in writing, including the reasons and criteria used in its decision making. The Committee should report to the PCT Board on a regular basis. An annual report should be submitted to the Board.
March 2009
20 May 2009 71

ANNEX H: Terms of Reference (PBC Executive Committee)
Practice Based Commissioning Executive Committee
Terms of Reference
Introduction
Practice Based Commissioning (PBC) has been introduced nationally as one of the mechanisms to improve patient care by:
1. Encouraging a greater variety and choice of services for patients.2. Providing care in settings that are closer to home and more convenient for patients.3. Making more efficient use of services.4. Involving front line clinicians in commissioning decisions.
And it involves:
1. The agreement of indicative PCT commissioning budgets for GP practices and professionals based on transparent principles.
2. The design of new clinically led service pathways and models and the implementation of these.
Within Brent Teaching PCT a Practice Based Commissioning Executive (PBCE) has been established to support the achievement of these objectives by providing a clinically led forum with significant clinical and managerial input from practicing primary care professionals. The Executive’s role is:
1. To oversee the implementation of PBC and support practices to work together to develop, provide and commission high quality services for people registered with the GPs in Brent.
2. To provide a collaborative structure for cost-effective commissioning and provision of services by co-ordinating the plans and views of practices.
3. To facilitate pooling of budgets and risk sharing arrangements in line with PCT financial rules.
4. To agree on behalf of practices the framework and policies for the ongoing development of PBC in Brent.
Objectives
The Executive will:
1. Take responsibility for the development and implementation of PBC in Brent:
a. Review health needs assessment and commissioning strategy to inform PBC commissioning objectives and developments. (Responsibility for approving, PBC commissioning objectives and business plans, lies with the PBC Governance Committee),
b. Review of individual business plans to identify Brent wide initiatives and priorities.
c. Identification of opportunities for service redesign across Brent.
20 May 2009 72

ANNEX H: Terms of Reference (PBC Executive Committee)
d. Oversight of the individual work streams required to achieve the business plans.
e. Development of the operational policies for the implementation of the commissioning plans and associated models of care and pathways. This covers practice and partner organisation responsibilities.
f. Development of plans and business cases for the management of savings/freed-up resources/overspends and recommend these to the PBC Governance Committee.
g. Development and agreement of new models of care and service specifications for discussion with the PEC.
h. Review of compliance with agreed care pathways/service models and of PBC performance (activity, finance and demand/capacity), developing remedial action plans and support as required.
i. Provide a forum for the PCT to obtain the views of Practice Based Commissioners in relation to its strategic commissioning function.
2. Develop the detailed organizational development support plan for practice teams to ensure they become effective PB Commissioners.
3. Ensure effective arrangements for PPI in PBC to ensure that practice and service plans reflect the views and aspirations of users.
4. Support practices/groups of practices to implement effective governance arrangements for any inter-practice services.
5. Identify commissioning risks and issues for services not covered by PBC and agree plans for these with the PCT/relevant bodies.
6. Provide a forum for monitoring of new service models and of SLAs/contracts.
7. Provide a forum for effective liaison between practice based commissioners and other commissioning agencies across Brent.
8. Provide regular reports on the progress and achievements of PBC.
9. Act as the main decision making body for all issues in relation to PBC across Brent in line with the statutory functions of the PEC and PCT Board. For example:
a. Advising on infrastructure systems required to successfully support Practice Based Commissioners.
b. Ensuring the provision by the PCT of information to practices to support them with PBC and supporting practices to use and interpret this.
c. Holding practice based commissioners to account for their management of relevant NHS resources in line with agreed accountability frameworks, national targets, Health Care commission assessments and local agreements.
d. Making recommendations to the PEC for the use of Pooled/Freed Up Resources.
20 May 2009 73

e. Negotiating the timescale and format for devolution of further budgets to practices and for movement to “fair share” budgets on behalf of practices. This will include impact assessment and addressing local health inequalities.
f. Development and agreeing on behalf of practices plans to manage financial risk.
ANNEX H: Terms of Reference (PBC Executive Committee)
Relationships
The Executive has 4 main relationships:
1. It is accountable to the PBC Governance Committee and thereby to the PCT Board.2. It is accountable to local people as the commissioner of services.3. It reports on its work to its constituent practices and uses the Brent GP Federation
Council as a reference group as required.4. It will promote effective communication with constituent GP practices, primary care
teams, PEC, and the GP Federation Council.
Under Practice Based Commissioning, PCTs remain accountable for all the funds allocated to them for ensuring fair access to services for their populations. The PCT will retain responsibility for accountability agreements with practices for the delivery of services that meet all national and local quality standards, specifically in relation to budgets and service re-design priorities.
Membership
The Commissioning Executive is a joint committee of the Federation Council and PCT Executive members and comprises two Federation representatives or equivalent per PBC Cluster / Consortia, maximum 10 Federation members or equivalent.
The Commissioning Executive will include officers from the PCT (Directors of Finance, Primary Care Commissioning, and Strategic Commissioning) also representatives from the local authority. The Executive will discuss the need for the co-option of other representatives.
Whilst Federation Council members represent a constituency and bring an important professional/constituency perspective, as Commissioning Executive members they are expected to take a corporate view of the tasks they undertake.
Nominations to the Federation Council
Each PBC Cluster / Consortia will be expected to nominate two PBC representatives to sit on the Federation Council and subsequently the Commissioning Executive.
Nominees will be assessed against an agreed set of competencies / person specification.
Nominations will be ratified by the Director of Primary Care and Commissioning and the PEC Chair.
Federation Council members will be representatives of their PBC Cluster and not of their individual practice or individual profession.
Terms of Office
20 May 2009 74

The term of office for an Executive member will initially be from 25 th June 2008 to 24th June 2009. The PCT will review the joint working of the Federation and Commissioning Executive and will make a decision on the future of the Executive at least three months prior to the 24 th
June 2009.
ANNEX H: Terms of Reference (PBC Executive Committee)
RemunerationThe remuneration of Federation Council members of the Commissioning Executive will be £12,000 per annum (excluding on-costs).
Mode of Operation
The Commissioning Executive will meet on the last Wednesday afternoon of every month. It may agree to meet more frequently by agreement or at the request of the PBC Governance Committee or PCT Board- for example to agree a significant strategic decision or because the PCT has sought guidance on a particular issue.
Should a position on the Federation Council become vacant, the nomination process above will apply for the relevant Cluster / Consortia.
The Executive will ensure that it has open and transparent processes to ensure that members can see the basis on which decisions are taken and will also ensure there are regular communications with members to inform and disseminate their decisions.
The agenda, minutes and papers from each meeting will be made available and published on Brent’s intranet system.
Quorum
The Executive will be quorate when all Clusters / Consortia are represented and two Executive Directors are present.
Where a decision is required and consensus cannot be reached, voting may be required (refer to PEC guidance).
An 80% attendance record will be expected of all Commissioning Executive members as a minimum, unless there are extenuating circumstances that have been agreed with the Director of Primary Care and Community Commissioning and the Federation Council. If a member fails to meet this requirement, it will be addressed by the Federation Council and PCT Executive.
Specific Roles
Chair
The Director of Primary Care and Community Commissioning and the Director of Strategic Commissioning have responsibility for chairing Executive meetings on an alternate basis.
Agenda Setting
20 May 2009 75

The agendas will be agreed by the rotating Chair of the Federation Council and the Assistant Director of Primary Care Commissioning. Final approval will be given by the Director of Primary Care and Community Commissioning and / or the Director of Strategic Commissioning.
ReviewThese terms of reference will be kept under review annually
September 2008 (Version 4)
20 May 2009 76

ANNEX H: Terms of Reference (Federation Council Code of Conduct)
Brent Federation of Practiced Based Commissioners
Council Code of Conduct
Introduction
At the inaugural seminar of the new council it was agreed that council members would adhere to mutually agreed code of conduct and their work would support the following values.
Values
Patient focus and benefit Health improvement Respect for each other Confidentiality Transparency /openness Probity Communication Flexibility Innovation Honesty Democracy Commitment Developing Local leadership Mutual support for equal and effective contributions Growing aspirations
Duties
Members of the Council will also serve as members of the PCT Commissioning Executive.
They will attend all meetings and development sessions where possible, and preferably give advance warning of non-availability.
Each member has been allocated to take a lead commissioning role and will also act as back up on another commissioning role.
Each member will be expected to attend at least 80% of all meetings/sessions unless there are extenuating circumstances which have been agreed with the council and the PCT.
Members will be expected to read papers and communicate regularly and promptly between meetings checking their preferred e-mail address and post.
Members will be accountable to the council and their nominating cluster/consortium for their Federation role, and to the PCT CEO for their commissioning executive role.
20 May 2009 77

ANNEX H: Terms of Reference (Federation Council Code of Conduct)
Responsibilities
Members will make decisions that promote the Council and Cluster / Consortium values.
Members will make decisions that support financial balance. All members have a responsibility to support the communication systems
within the federation. Members will respect the confidentiality and sensitivity of information they
may see in their role. Members will make decisions based on the information presented and
declare any personal interest at the outset. Members will declare any new personal interests as they arise if there is any
potential conflict with their federation role. Members will hold honest and open debates but will support all federation
decisions once reached whatever their personal view. Members will not discuss detail of council debates outside the council, unless
with explicit council approval. Members will treat each other with respect and listen and acknowledge each
others’ views. Views of each member have equal weight.
July 2008
20 May 2009 78

ANNEX H: Terms of Reference (Federation Council – Portfolio of Responsibilities)
Portfolio of Responsibilities for
Practice Based Commissioning Federation Members
Name: A N Other
PBC Cluster: Anytown
Portfolio of responsibilities
1. To act as the Service Level Agreement lead for Process, Systems and Governance.
2. To provide Service Level Agreement support for Mental Health services.
3. To provide Service Level Agreement support for Community Services.
4. To provide PBC support for the development of Community Pathways, specifically gynaecology services.
5. To provide PBC support for the development of the Primary Care Strategy.
6. To provide PBC support for the development of World Class Commissioning.
Responsibilities
Members will make decisions that promote the Council and Cluster / Consortium values.
Members will make decisions that support financial balance. All members have a responsibility to support the communication systems
within the federation. Members will respect the confidentiality and sensitivity of information they
may see in their role. Members will make decisions based on the information presented and
declare any personal interest at the outset. Members will declare any new personal interests as they arise if there is any
potential conflict with their federation role. Members will hold honest and open debates but will support all federation
decisions once reached whatever their personal view. Members will not discuss detail of council debates outside the council, unless
with explicit council approval. Members will treat each other with respect and listen and acknowledge each
others’ views. Views of each member have equal weight.
July 2008
20 May 2009 79

ANNEX H: Terms of Reference (PBC Development Programme Steering Committee)
PBC Development Programme Steering Committee
Terms of Reference
1. Introduction and Context
Within the broader context of the Department of Health’s Practice Based Commissioning Development Support Framework, NHS Brent has been awarded a Practice Based Commissioning (PBC) Development Programme, led by NHS Alliance and Humana. This will take place from February – November 2009.
2. Aim of the Steering Group
The steering group will oversee the shaping and development of the PBC Development Programme, ensuring the priority development needs in relation to PBC of both the PCT and the clusters are identified and addressed. In addition it will ensure there is appropriate engagement and communication and will monitor its performance from inception to delivery. It will hold the Programme Leads to account.
2. Objectives and Deliverables
To approve the development implementation plan.
To monitor performance of the Development Programme against the implementation plan from the appointment of the Programme Leads through to the completion of the project through regular progress reports from the Program Leads.
To ensure the necessary engagement and communications within the programme
To provide perspective, advice and guidance to the Program Leads on PCT and cluster priorities in relation to the diagnostic phase feedback and the subsequent programme.
To facilitate access for the Programme Leads to the to key PBC stakeholder communities.
To receive and approve the final report of the project.
To participate in the dissemination of outcomes from the project and to be advocates in implementing the recommendations of the programme.
3. Working Principles:
Ensure that the program’s emphasis is on ‘active learning’, based on solving real problems to ensure that PCT / PBC teams acquire, practice and embed the skills and knowledge that is directly relevant to their job roles.
20 May 2009 80

ANNEX H: Terms of Reference (PBC Development Programme Steering Committee)
Ensure cross-cluster engagement in programme development and implementation.
Within the PCT, ensure cross-directorate engagement in programme development and implementation.
Align to NHS Brent priorities as set out in the Department of Health’s PBC Development Support Framework.
Ensure PCT/PBC cross-cluster cohesion and consistency in the approach to implementation of each phase of the program.
Focus on areas of greatest practical impact first.
4. Frequency
The Group will meet bi-monthly.
5. Membership
The following membership is proposed:
1. Gill Kelly: (interim) Asst. Director of Primary and Community Care Commissioning
2. Julie Wood: NHS Alliance3. Tim Taylor: Assistant Director of Finance4. Charles Allan: Director of Human Resources5. Simon Bowen: Public Health6. Eliza Tudor: PBC Manager 7. Carole Amobi: PEC Co-Chair / Manish Prasad: PEC Co-Chair8. Ethie Kong: Harness Cluster Lead 9. Rhiannon Lloyd: Kingsbury Cluster Lead10. Samantha Sharkey: Willesden Cluster Lead
The programme will receive the following operational support:
1. One Program Lead from NHS Alliance2. One Support Lead from Humana3. One cluster PBC Administrator (to be identified)4. Others as specified
6. Chair
Assistant Director of Primary Care and Community Commissioning: Gill Kelly (interim)
7. Reporting Structure
Reports to the PBC Executive Committee and PBC Governance Sub-Committee for information. Accountable to the EMT.
8. Attendance and Nominated Deputies
Members and those listed as being in attendance will be expected to routinely attend meetings and to contribute to the discussion and feedback to the clusters in driving forward the PBC Development Programme. A nominated deputy should attend where a member or someone listed as being in attendance cannot attend.
20 May 2009 81

ANNEX H: Terms of Reference (PBC Development Programme Steering Committee)
9. Quorum
The minimum quorum of members present at the meeting will be four, of which must include:
Julie Wood: NHS Alliance / Humana Gill Kelly, Assistant Director Primary and Community Care Commissioning One PBC Manager One Cluster Lead / Federation member
March 2009
20 May 2009 82

ANNEX H: Terms of Reference (Demand Management Sub-Committee)
Demand Management Sub-Committee of the PBC Executive Committee
Terms of Reference 2009/10
Version Control
Status Group / Committee Date Draft PBC Exec 25/2/09Draft v 5 Demand management Group 17/3/09Draft/Final v 6 PBC Exec 25/3/09
1. Aim of the Sub Committee
To ensure appropriate PBC leadership and engagement within the development and implementation of the NHS Brent Demand Management Plan. To ensure progress towards care outside hospital through the implementation of care pathways and appropriate investments in sustainable community and primary care based solutions.
2. Programme Ownership
Programme to be owned and driven by the PBC Executive with management support from the PCT.
3. Objectives
• develop a clear work programme to achieve the shifts in care identified within the CSP and reflected in contracts with acute hospitals – see Annexe A for details of required 2009/10 activity shifts
• consider other high impact interventions which could effect the desired outcomes
• identify human and other resource requirements across the plan, enabling the activities to be successfully achieved
• agree milestones and outcomes to track progress against plans• identify and manage risks to achievement
4. Working Principles
• align work to NHS Brent priorities as set out in the CSP and Annual Operating Plan
• focus on areas of greatest impact initially• ensure cross cluster engagement in plan development and
implementation (clinical and public/patient)• ensure cohesion and consistency in the plans developed and
implemented across the clusters to maximise economies of scale• PCT managers to provide support to PBC and work collaboratively• identify evidence based solutions
5. Workstreams
Each workstream will be led by a PBC clinician or manager. Staff on the workstream will be drawn from acute/ primary / community commissioning, PH, finance,
20 May 2009 83

ANNEX H: Terms of Reference (Demand Management Steering Committee)
information. Each workstream will be supported by a PBC Administrator. The task of each workstream group will be to identify 3 priorities to tackle in the first instance.
The following workstream groups will be formed:
5.1 Data Analysis: Lead Jenny Poole, supported by Simon Bowen, Vijay Patel, Caroline Kerby, Sandeep Prashar, and admin.
• agree Dr Foster training needs• provide targeted and specific Dr Foster training and support to PCT and
PBC personnel• secure additional support from Dr Fosters for clusters• determine specific data analyses required• conduct PCT wide acute activity data analysis and by cluster
5.2 Non elective: Lead: Jahan Mahmoodi, supported by acute commissioner, Simon Bowen, Finance, Jeevan Jayanthan, PBC manager.
i) A and E
• establish reasons for the Accident and Emergency standardised admission rate (SAR) 19% increase from 07/08 – 08/09
• GPs to utilise community based options for referral (e.g. CCS, CCT) as alternative to AAU admission at CMH
• establish which GP Practices are outside the norm – for all providers and address
• identify heavy user patients and work with clusters/GPs to establish remedial actions including communication strategies
ii) In-patient demand management
Conduct analysis to determine the following:
• high cost high volume activity by cluster and establish reasons for growth• intermediate care HRGs with high levels of excess bed days and
emergency HRGs presenting to secondary care to determine potential areas for hub and spoke primary / community based service development via NHSI Opportunity Locator
• admissions to AAU of those discharged within 24 hours
On the basis of the analysis develop / implement /agree:
• complete EARLI to identify patients at high risk of admission and put in place plans to improve community based co-ordination and management
service models and provision for district nursing and community matrons in the Provider Arm contract to enhance community capacity.
• intermediate care pathway
5.3 Out-patient demand management: Lead: Sarah Basham, supported by Simon Bowen, Caroline Kerby, Acute Commissioning, Finance, Information, Edward Coker.
20 May 2009 84

Conduct analysis to determine the following:
ANNEX H: Terms of Reference (Demand Management Steering Committee)
specific reasons for growth/change in gynaecology, cardiology, orthopaedics, ENT, diabetic medicine, clinical haematology, geriatric medicine, max fax, urology, respiratory medicine.
OP: IP conversion rates by specialty out-patient ambulatory care sensitive (ACS) conditions presenting to
secondary care by cluster to determine potential areas for hub and spoke primary / community based service development.
onward referral pattern and prevalence from community pathways those OP specialties with most potential to shift activity from secondary to
primary care via NHSI Opportunity Locator review of anti-coagulation services
On the basis of the analysis develop / implement /agree:
proposals for highest spend out-patient procedures: TandO, dermatology, gynaecology, general surgery, urology, cardiology
referral protocols and plans for provision of services identified via opportunity locator and ACS conditions within hub and spoke primary / community based service development
• 12 month pilot physiotherapy service to reduce referrals to TandO via any willing provider in Kilburn Cluster. If referral reduction targets achieved (10% reduction in 2009/10 and 20% reduction in 20010/11), ascertain potential to roll out across all clusters and implement.
improvements to community pathways commission new anti-coagulation service
5.4 Diagnostics Lead: Rhiannon Lloyd, supported by Caroline Davidson, Jenny Poole, and Natasha
work with In-Health to expand the range and location of diagnostic tests develop referral protocols for GPs to refer ultra sound and MRI to In-
Health GPs to start referring to In-Health and stop referring to direct access
diagnostics at NWP and CMH develop referral protocols for GPs for all diagnostics that support
management of patients in primary care
5.5 Acute Contract Management Lead: Caroline Kerby supported by Jahan Mahmoodi, Jasoda Manji.
Understand and influence the acute contract e.g. data validation, new referrals, follow up ratios, data validation etc. and also the contract business terms. Some activities to consider would include:
spread data validation process to 90 % GP Practices Contract challenges: ensure resolution and feedback to clusters avoid payment of repeat new referrals to same OP specialties investigate penalties for non compliance (include discharge letters) understand impact of HRG 4 on contract and budget setting agree outpatient pathways which set out when treatment is complete or
being shared with primary care
6. Required Information for Transfer to Primary Care
20 May 2009 85

ANNEX H: Terms of Reference (Demand Management Steering Committee)
The following information will b required in order for services to be provided in primary care:
evidence that re-provision in primary care better meets patient needs target group for new service location for delivery pathway including referrals, appointments, and follow ups informatics, data validation and communication systems funding levels, sources and VFM audit and review equality impact assessment
7. Outcomes
a PCT wide plan according to with quantified service reductions which form measurable outcomes and which is owned by all clusters
clear and deliverable demand management sections of five cluster commissioning plans with quantified outcomes for reduction of secondary care activity
at least two agreed pathways implemented across all five clusters in 2009/10 evidenced achievement of agreed activity reductions in secondary care
8. PCT Management Support
The PBC leads commit to identify the resources required to deliver the agreed workstreams and the PCT commits to release staff of the appropriate level of seniority to support the demand management plans. Membership of the demand management group and workstreams will include acute and primary care commissioners, public health physicians, finance managers, information managers, prescribing managers etc. The relative roles will be included as part of the PBC Governance Agreement.
9. Frequency
The Sub Committee will meet monthly on the third Tuesday each month from 09:30 hrs 11:30 hrs.
10. Membership
The following membership is proposed:-
2 x management Federation leads 3 x clinical Federation leads AD Primary and Community Care Commissioning 2 x PBC Manager Deputy Director Finance Head of Acute Commissioning Heal of information Public Health Consultant Cluster administrators
11. Chair
20 May 2009 86

ANNEX H: Terms of Reference (Demand Management Steering Committee)
Nominated Federation Lead(s): In the first instance J Poole and C Kerby will co-chair.
12. Reporting Structure
Reports to the PBCE. Delivery Plans and exceptional reports will be provided.
13. Attendance and Nominated Deputies
Members and those listed as being in attendance will be expected to routinely attend meetings and to contribute to the discussion and feedback to other clusters in driving forward the demand management plan. A nominated deputy must attend where a member or someone listed as being in attendance cannot attend. 14. Quorum
The minimum quorum of members present at the meeting will be four, of which must include :-
2 Federation leads 2 PCT managers
15. Review of Terms of Reference
The function and Terms of Reference for the Sub Committee will be reviewed annually. Next review end of March 2010.
20 May 2009 87

ANNEX H: Terms of Reference (Demand Management Steering Committee)
Appendix A
2009/10 acute contract demand management activity shifts and schemes
NHS BRENTDEMAND MANAGEMENT SCHEMES 2009/10
Specialty
How reduction in trust activity will be achieved Current trust
activity
Earliest starting point for
new (09/10)
capacity
In year reduction in trust’s activity (09/10)
NEL WCC Intermediate Care Initiative
Modelling of HRG reduction has been based upon the DH Ambulatory Sensitive Conditions (HRG analysis attached).NHS Brent has committed to the following community schemes planned to reduce emergency admissions:
Enhanced CCT Acute care at home (Clinicenta) Enhanced end of life care (Clinicenta) Improved intermediate care and reablement Improved community nursing infrastructure to support improved management of people at
home
Oct 09 397 FCE
AandE attendan
ces
Subject to business case approval, NHS Brent intends to procure a new model of urgent care at CMH. The model of care has been developed with clinicians from acute and primary care. The current reduction in AandE activity is based upon a 24/7 service taking minor ailments and injuries.
Oct 09 21,639(10,819 Minors/10,819
Std)
1st OPs Improved primary care pathways and referral protocols Oct 09 1st OPs
20 May 2009 88

Trauma and Orthopaedics.Ophthalmology.Cardiology.Dermatology.Gynaecology.
PBC clusters will reduce referrals to acute care through the introduction of care pathways; referral protocols; peer audits; skills directories etc
163 162 162 162 162
Total 811
General Surgery
PSD Elective procedures (day cases)
Anticipated changes in patient choice based upon new market entrant (Clinicenta)
Oct 09 60
General Surgery
PSD Elective procedures (outpatients)
Anticipated changes in patient choice based upon new market entrant (Clinicenta)
Oct 09 160
20 May 2009 89

ANNEX I
PBC Disputes Resolution Procedures
Within the ‘Practice Based Commissioning Practical Implementation’3 guidance published by the Department of Health, the Strategic Health Authority is required to ensure robust arbitration processes are in place.
“A dispute resolution procedure may be invoked by either party to the contract if there is a failure to agree. This may occur either before or after the PBC Governance Agreement is agreed. The disputes procedure has three stages negotiation and mediation followed by adjudication if the dispute remains unsettled.”4
1. Negotiation
“The negotiation period must be formally invoked and represents the formalisation of a difference of opinion as a dispute. Either party may trigger the 15 operational day negotiation period by making a written negotiation offer to the other.”5
Negotiators: PBC Leads and the Assistant Director of Primary Care and Community Commissioning.
2. Mediation
“At the mediation stage the decision about the solution to the dispute remains with the parties in dispute”6. The two parties are assisted to come to a resolution through a meeting convened by the PCT and will be managed by the Director of Primary Care and Community Commissioning. “In order to invoke the mediation the two parties concerned must submit to the mediators a position statement that describes the precise points over which they disagree. If the mediators are satisfied that the nature of the dispute has been adequately documented, they will invite the parties to describe their own solution to the dispute. The parties will have five working days to comment on the other party’s position. The mediators will challenge and test and at the end of this time will invite the parties to agree.”7
3. Adjudication
If a dispute cannot be resolved at the mediation stage, the Director of Primary and Community Care Commissioning will make a recommendation to the Chief Executive of Brent PCT whose decision shall be final and binding on both parties.
3 Practice Based Commissioning: Practical Implementation, Department of Health, Nov 20064 Guidance on the Standard NHS Contract for Community Services, Department of Health, Dec 20085 As above6 As above7 As above
20 May 2009 90

ANNEX J
PBC Governance Agreement Declaration 2009/10
The Cluster confirms that the following GP Practices have been consulted, and have signed up to the Cluster Governance Agreement:
GP PRACTICE ENGAGEMENT & SIGN UP TO CLUSTER ARRANGEMENTS
Evidence of GP Practice sign up to the Cluster arrangement:
GP Practices participating in PBC Cluster:
Process:
Evidence:
Cluster Governance Agreement / arrangements (between cluster & GP Practices) :
The Cluster, on behalf of all participating GP Practices, confirms acceptance of the PBC Governance Agreement, management of the PBC Budget, implementation of agreed commissioning objectives, active involvement in the performance management process, and being party to the PBC Incentive Scheme for 2009/10.
Cluster lead: Cluster Lead:
Signature:
Date:
Signature:
Date:
Upon receipt of the signed Governance Agreement by the PBC Cluster Leads, the PCT will confirm approval of the final cluster membership.
Please send the completed PBC Governance Agreement declaration to [email protected] or [email protected] by May 2009
20 May 2009 91

PCT MANAGEMENT SIGN OFF
The Director of Primary Care Commissioning, on behalf of the PCT confirms acceptance of the PBC Governance Agreement, provision of indicative PBC Budgets, provision of PCT support to clusters to achieve agreed commissioning objectives and to develop a proactive performance management process, underpinned by a PBC Incentive Scheme for 2009/10.
Name Jo Ohlson
Position Director of Primary Care and Community Commissioning
Signature:
Date:
20 May 2009 92