ادخ مانب - معاونت درمان | اقتصاد...
190
م خدا بنا
Transcript of ادخ مانب - معاونت درمان | اقتصاد...

بنام خدا


ALTERD LEVEL OF CONSCIOUSNESS
ALOCA SIGN NOT A DISEASE
COMA THE LAST STATE OF DEPRESSED CONSCIOUSNESS
کاهش سطح هوشیاری

1) ARAS
2) CEREBRAL HEMISHERERS
PATHOPHYSIOLOGY

Stages of depressed consciousnessManifestationsStage
arousableattention,fullySleepy,poorLethargy
Poor orientationConfusion
Agitated confusion, hallucinations, Delirium autonomic abnormalities(sweating,HR,HTN)
to noxious stimulationArousableObtundation
momentarily with noxious ArousableStupor
stimulation,localizes pain
not localize painUnarousable,doesComa

encephalopathy
The term encephalopathy describes a diffuse disorder of the brain in which at least two of the following symptoms are present
1) altered states of consciousness
2) altered cognition or personality
3) Seizures
Encephalitis is an encephalopathy accompanied by cerebrospinal fluid (CSF) pleocytosis.

ETIOLOGY








EVALUATION
Coma is a medical emergency whose evaluation requires a rapid, comprehensive, and systematic approach. Early identification of the underlying cause of coma can be crucial for patient management and prognosis.

History
The etiology may be apparent from the history, when coma results from the expected progression or complication of a known illness or injury

General examinationAssessing vital signs and the ABCs: airway patency, breathing (ventilation and oxygenation), and circulation, are important for initial stabilization, but may also inform the etiology
dehydration, unusual odors, needle tracts, trauma, or signs of organ system failure
Breathing patterns :Cheyne-Stokes (Cerebral, thalamic, or
hypothalamic modulation of respiration has been lost) , central neurogenic hyperventilation(midbrain lesion ) , Gasping (dysfunction
of the low brainstem-medulla)

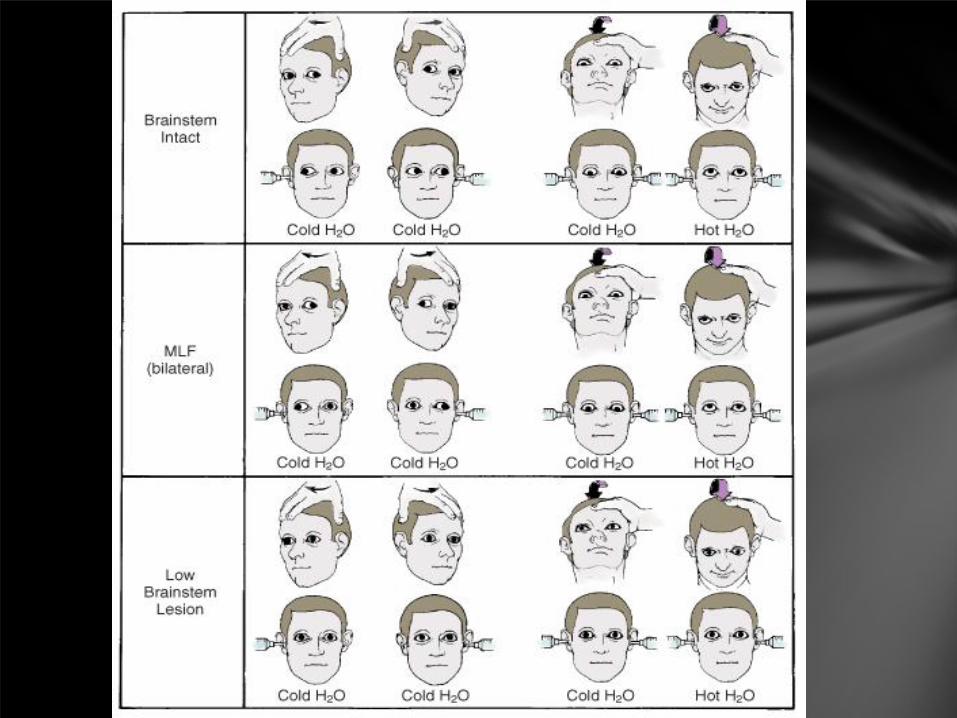
Neurological examination
The neurologic examination in this situation is necessarily brief and is directed at determining whether the pathology is structural or due to metabolic dysfunction (including drug effects and infection). The examiner assesses: Level of consciousness Motor responses Brainstem reflexes(RAS): pupillary light, extraocular, and corneal reflexes


DIAGNOSTIC STUDIES
Laboratory Testing
Neuroimaging
Lumbar puncture
Electroencephalogram

Laboratory Testing
All patients presenting with altered consciousness should undergo a rapid bedside test for blood glucose and basic laboratory testing including: Serum electrolytes, calcium, magnesium, glucose Arterial blood gas, Liver function tests, ammonia Complete blood count Blood urea nitrogen, creatinine ,Urine drug screen ,Blood culture

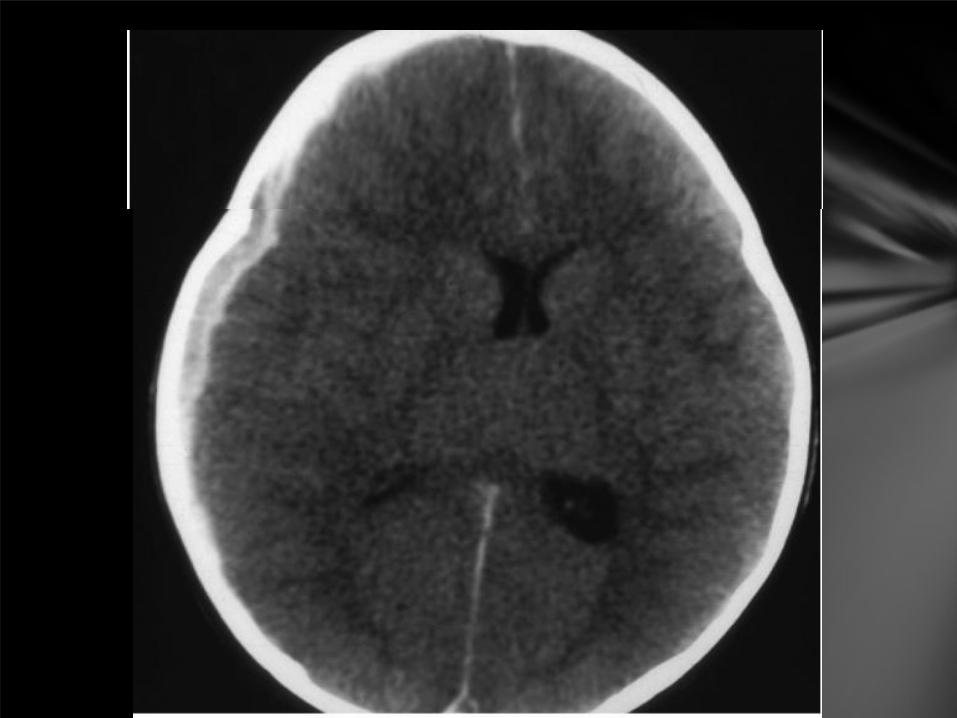
Neuroimaging
Computed tomography (CT) is the initial neuroimaging test of choice to evaluate a child in coma.. CT should be performed immediately when the examination suggests increased intracranial pressure (papilledema, bulging fontanelle in infants, or bradycardia with hypertension) or a transtentorialherniation syndrom

Falx cerebri and tentorium




Lumbar puncture
Urgent evaluation of cerebrospinal fluid (CSF) is required when there is suspected infection of the central nervous system. In a patient with altered level of consciousness, neuroimaging to exclude an intracranial mass lesion is required prior to lumbar puncture (LP) in order to avoid precipitating transtentorial herniation. Coagulation test results should also be obtained beforehand.
Empiric antimicrobial treatment is recommended when the diagnosis of bacterial meningitis or herpes encephalitis is strongly suspected,

Encephalogram
EEG should be performed in children with coma of unknown etiology. It is often the only means of recognizing nonconvulsive status epilepticus (NCSE), especially in patients who are paralyzed.
Periodic epileptiform discharges may occur in NCSE but also in underlying brain injury without seizures. Periodic lateralized epileptiform discharges suggest herpes encephalitis or infarction. Multifocal or generalized periodic discharges can also be seen with metabolic and infectious etiologies and are characteristic of subacute sclerosing panencephalitis.




TREATMENT
Early treatment of coma is generally supportive until a definitive diagnosis is made. An important goal of early treatment is to limit brain injury. Treatments for dangerous etiologies (eg, hypoglycemia, increased intracranial pressure, bacterial meningitis,opioidintoxication) are often initiated empirically, especially if there are suggestive clinical features.

Airway
Establishing a secure airway and providing adequate ventilation may be lifesaving and also may limit neurologic injury. Establishing a secure airway in a patient with coma may be attained by repositioning
the child to open the airway,. Patients with GCS <8 are usually unable to adequately protect their airway and should be intubated.

Breathing
Oxygen saturation should be measured and supplemental oxygen provided. Moderate hyperventilation (target PaCO2 30 to 35 mm Hg) to produce arterial constriction and lower intracranial pressure (ICP) should only be initiated for patients with increased ICP. Extreme hyperventilation has been associated with brain ischemia; the risks of aggressive hyperventilation (PaCO2 <30 mmHg) are only justified in patients with transtentorialherniation
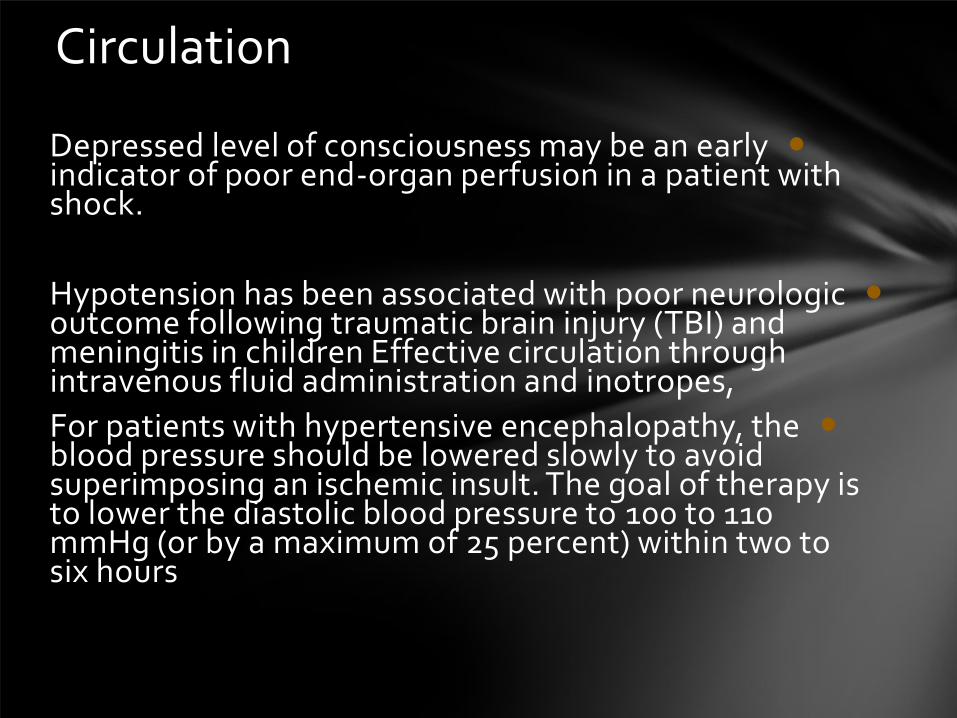
Circulation
Depressed level of consciousness may be an early indicator of poor end-organ perfusion in a patient with shock.
Hypotension has been associated with poor neurologic outcome following traumatic brain injury (TBI) and meningitis in children Effective circulation through intravenous fluid administration and inotropes,
For patients with hypertensive encephalopathy, the blood pressure should be lowered slowly to avoid superimposing an ischemic insult. The goal of therapy is to lower the diastolic blood pressure to 100 to 110 mmHg (or by a maximum of 25 percent) within two to six hours

Glucose
Fingerstick blood sugar and a serum glucose should be checked immediately in the evaluation of a comatose child. Glucose (2.5 mL/kg of 10 percent dextrose solution) should be administered even before test results are known. If hypoglycemia is revealed, then ongoing monitoring and treatment will be needed.

Intracranial pressureWhen increased intracranial pressure (ICP) is suspected based on CT findings, papilledema, split sutures, or a herniation syndrome, emergent treatment is recommended. Increased ICP is assumed when there is coma after head injury. Early interventions to reduce intracranial pressure include treating fever, elevating the head of the bed to 30 degrees above horizontal, moderate hyperventilation (target PaCO2 30 to 35 mmHg) and administering mannitol (0.25 to 1 g/kg IV). Neurosurgery should be consulted.

Seizures
If seizures have occurred diazepam(0.1-0.3 mg/kg), phenytoin (15 to 20 mg/kg phenytoin equivalent IV) should be administered. Recurrent seizures or status epilepticus may increase ICP and may be associated with secondary brain injury and worse neurologic outcome. (don’t forget hypoglycemia&hypocalcemia)
Nonconvulsive status epilepticus should be considered as a diagnosis even when there are no obvious seizure movements.

Infection
Empiric antibiotic and antiviral therapy are recommended if bacterial meningitis (eg, ceftriaxone 100 mg/kg plus vancomycin 60 mg/kg) or viral encephalitis (acyclovir 30 to 60 mg/kg per day,) are among the suspected entities .Blood cultures should be obtained prior to starting antibiotics but initiation of therapy should NOT await lumbar puncture. Therapy should be continued until these conditions have been excluded


Hyperthermia
Hyperthermia (>38.5 degrees C) can contribute to brain damage in cases of ischemia. Fever also increases cerebral metabolism and blood flow, thereby contributing to elevated ICP .Fever should be lowered with antipyretics and/or cooling blankets immediately. Shivering, which can contribute to elevated ICP, should be avoided.

Acid-base and electrolyte imbalance
Electrolyte imbalance may cause or be a complication of coma, and may increase the risk of neurologic injury. Iatrogenic causes of electrolyte derangement may result from resuscitation of patients with hypotonic or large volumes of hypertonic solutions. Resuscitation of patients with cardiovascular compromise should use isotonic solutions only (normal saline or lactated Ringers). Any electrolyte abnormalities should be corrected and monitored.

Antidotes
Antidote use is recommended only in the setting of known or strongly suspected drug overdose Naloxone (.01 to 0.1mg/kg up to 2 mg) is a relatively safe and effective treatment and should be considered when the history suggests possible opiate ingestion. Flumazenil is an antidote for benzodiazepine overdose, but will render benzodiazepines ineffective in the event of a seizure, so it should also be used with caution. Gastric lavage and activated charcoal may be recommended for very recent ingestions.
Agitation
Agitation may increase ICP, interfere with respiratory support, and increase the risk of injury. Significant sedation, however, may obscure the neurologic exam, may contribute to hypotension and hypoventilation, and should be administered only when the benefits of relieving agitation outweigh the need for close neurologic monitoring by exam.



•Seizures represent the abnormal and excessive discharging of the neuralglial network. A diverse group of disturbances of cerebral function or homeostasis can lead to seizures

Epilepsy is defined as recurrent, unprovoked seizures. Epileptic seizures are generally separated on the basis of the mechanism of the electrical phenomena into seizures that arise from one region of the cortex (focal, partial, or localization related) and seizures that arise from both hemispheres simultaneously (generalized)


Status epilepticus •Status epilepticus is defined as ongoing seizure activity for
greater than 30 minutes or repetitive seizures without return
of consciousness for greater than 30 minutes
impending status epilepticus for seizures between 5 and 30 min. The measures used to treat status epilepticus need to be started in any patient with acute seizures that do not stop within a few minutes


ICU ADMISSIONEEG MONITORINGMIDAZOLAM DRIPASSISTED VENTILATION
FLUID THERAPY (judiciously)
HEMODYNAMIC STATESUPPORTIVE CARETREATMENT OF ETIOLOGY

•A complete laboratory evaluation of a child with the new onset of seizures includes a complete blood count; measurement of blood chemistries, including glucose, calcium, sodium, potassium, chloride, bicarbonate, urea nitrogen, creatinine, magnesium, and phosphorus; blood or urine toxicology screening; analysis of CSF; and EEG and brain imaging (MRI).


عالیم و نشانه های نیاز قریب الوقوع به احیا

CNSعالئم و نشانه های مربوط به
،Obtundation دلیزیم ،Agitation آژیتاطیى ، LethargyلتارژیConfusionگیدی

عالئم و نشانه های تنفسی
Nasal)بیی ای پز پزع ، (Grunting)گزاتیگ ، آپ flaring) ، فض تگی ا ظؼیف ،خابدایی (Tachypnea)تذ تفض ، (Retracting)رتزکظیى ،
Poor) ا درری air movement) اطتزیذر، (Stridor) ، خض خض (Wheezing)طی

عالئم و نشانه های قلبی عروقی
، ظؼیف ای بط ، کاردی تاکی ، کاردی بزادی ، (Arrhythmia)آریتویPoor)هیزگی آظت بزگؼت Capillary Refill) ، پاییي خى فؼار

عالئم و نشانه های مربوط به پوست و مخاطها
، طیاس ، تؼزیك ( Pallor)، رگ پزیذگی( Mottling)هؼبک ػذى پطت، خؼکی ( Poor Membrane Turgor)، ترگر ظؼیف ( Diaphoresis)سیاد
( Dry mucous membranes)ططذ هخاطی

فیلم ها


آسپیراسیون جسم خارجی

Foreign Body Airway Obstruction
chocking

FBAO (Choking)
Epidemiology & Recognition
•More than 90% of deaths occur in children < 5 y/o.
•Signs: a sudden onset of respiratory distress with coughing, gagging, stridor, or wheezing

FBAO (Choking) Mild airway
obstruction The child can cough
& make some sounds. Severe airway obstruction The victim cannot cough or
make any sound.

Heimlich maneuver
Conscious Child Standing Conscious or Unconscious Child, Lying


Back Blow & Chest Thrust in an Infant


Unresponsive Victim
Perform CPR but should look into the mouth before giving breaths.
•If you see a foreign body, remove it.
•Do not perform blind finger sweeps because it may push obstructing objects further into the pharynx & may damage the oropharynx.
•Attempt to remove an object only if you can see it in the pharynx.
•Then attempt ventilation & follow with chest compressions.

Finger Sweep Maneuver Administered to an Unconscious Victim of FBAO


Emergency Department Management of Asthma Exacerbations

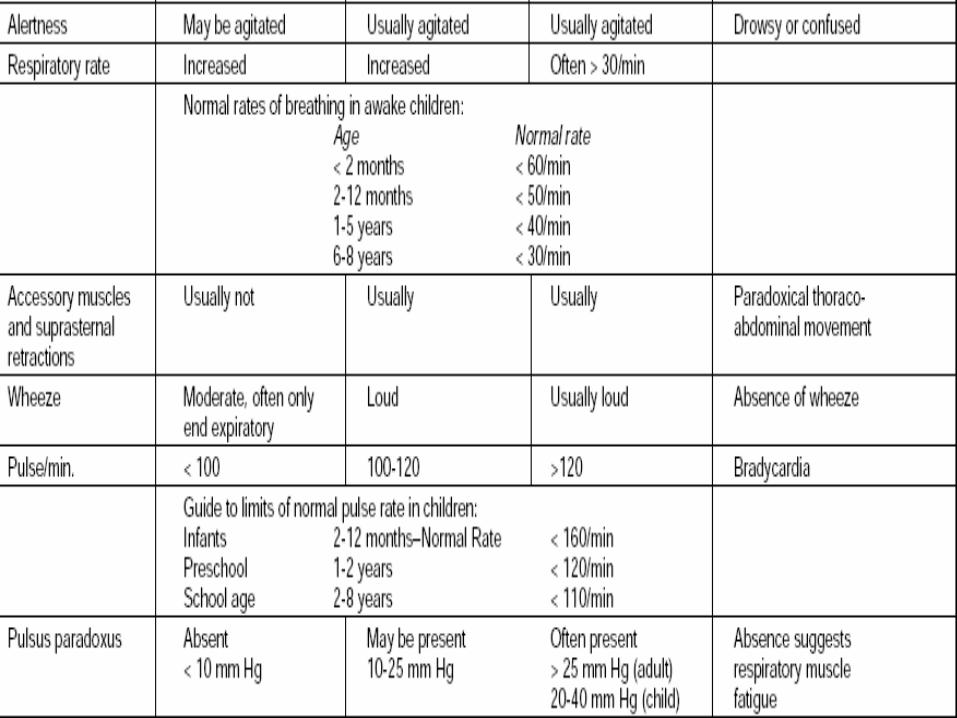
Severity of Asthma Exacerbations


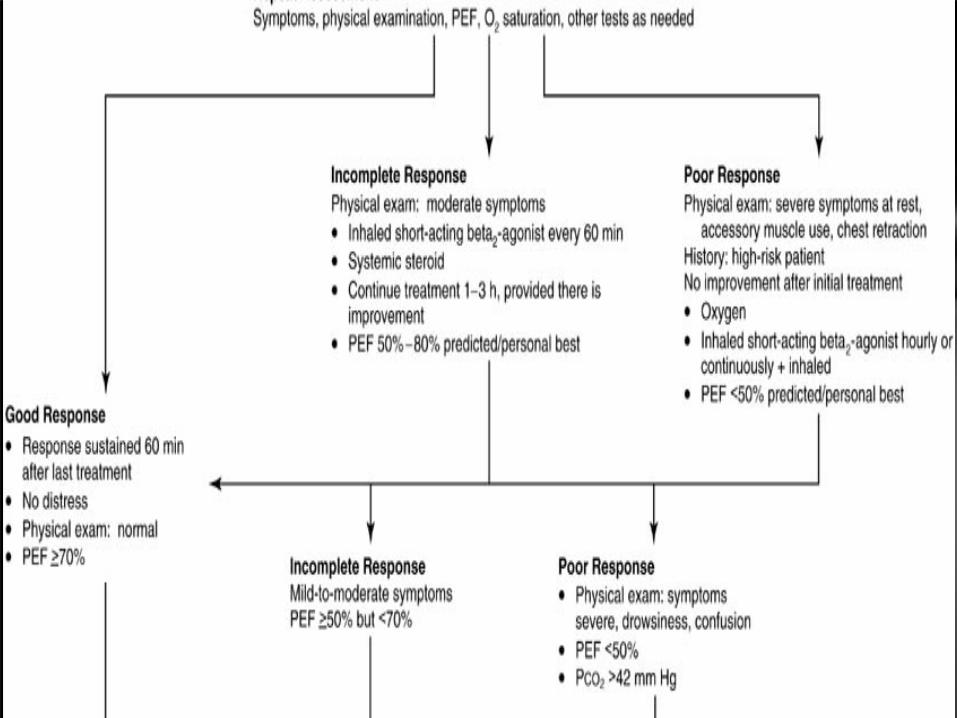
Management of Asthma Exacerbations in Acute Care Setting















Definition of shock
Shock is an acute, complex state of circulatory dysfunction result in failure to deliver sufficient amount of oxygen and other nutrients to meet tissue metabolic demand.

Classification of the cause of shock
Hypovolemic
Cardiogenic
Distributive
Obstructive
Septic
Dissociative

hypovolemic
Blood loss: hemorrhage
Plasma loss: burns, nephrotic syndrome
Water/electrolyte loss: vomiting, diarrhea
( the most common shock in pediatrics )

CARDIOGENIC
Congenital heart disease
Cardiomyopathies: infectious or acquired, dilated or restrictive
Ischemia
Arrhythmias

DISTRIBUTIVE
Anaphylaxis
Neurologic: loss of sympathetic vascular tone secondary to spinal cord or brainstem injury
Drugs

SEPTIC
Hypovolemic: third spacing of fluids into the extracellular, interstitial space
Distributive: early shock with ↓afterload
Cardiogenic: ↓ myocardial function by endotoxins

OBSTRUCTIVE
Tension pneumothorax
Pericardial tamponade
Pulmonary embolism
Anterior mediastinal masses
Critical coarctation of the aorta

DISSOCIATIVE SHOCK
Oxygen not released from hemoglobin(CO poisoning)
Methemoglobinemia



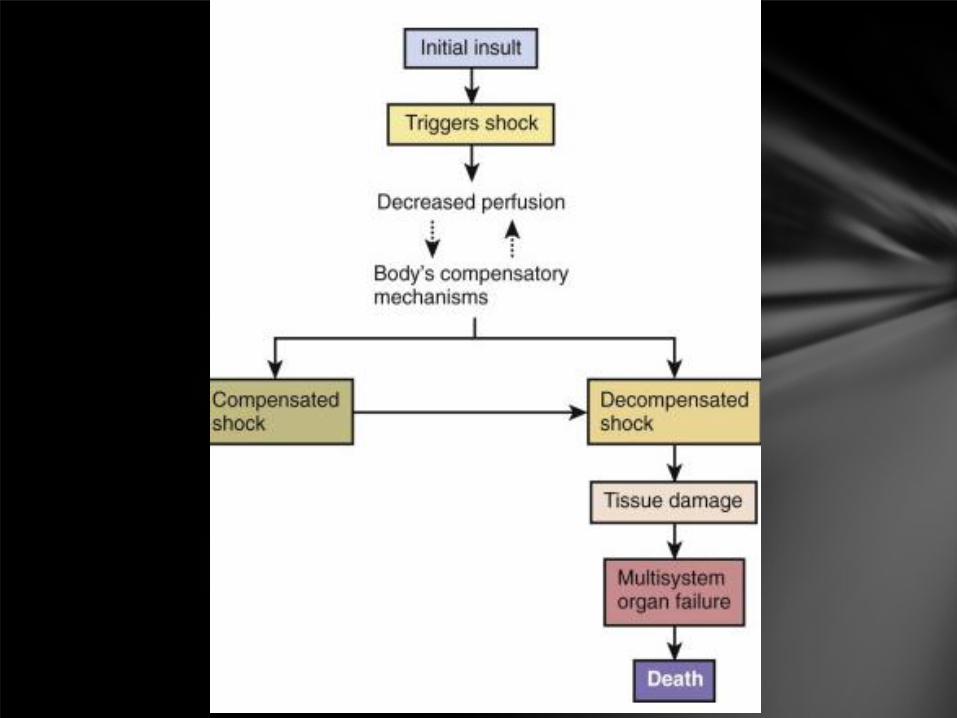
Stages of shockCompensated shock :presence of normal blood pressure by
compensatory mechanism (Hypoperfusion state)
Decompensate shock: fail of compensatory
mechanism. Hypotension and organ dysfunction
Irreversible shock :progression of organ dysfunction
Hypotension definition
Neonate (0-28 days): < 60 mmHg
Infant (1-12 months): < 70 mmHg
Children (1-10 years): < 70 + [2×age (y)] mmHg
>10 years: <90 mmHg

compensation
Increasing cardiac output(↑HR,↑stroke volume ,↑systemic vascular resistance)
increasing oxygen extraction
Redistributing blood flow to the brain, heart, liver & kidneys at the expense of the skin and GI tract & muscles
Increased respiratory rate
renin-angiotensin-aldosterone , ADH , cortisol and catecholamine ,ANF,
Renal excretion of H+ and retention of HCO3− to maintain
normal body pH
Multisystem Organ Dysfunction

Cardiovascular
Despite administration of isotonic intravenous fluid bolus ≥60 mL/kg in 1 hour: Decrease in BP (hypotension) <5th or systolic BP <2 SD below normal for ageOR
Need for vasoactive drug to maintain BP in normal range (dopamine >5 µg/kg/min or dobutamine, epinephrine, or norepinephrine at any dose)OR
Two of the following:
Unexplained metabolic acidosis: base deficit > 5.0 mEq/L
Increased arterial lactate: >2? upper limit of normal
Oliguria: urine output <0.5 mL/kg/hr
Prolonged capillary refill: >5 seC
Core to peripheral temperature gap >3?C

Respiratory
Pao2/Fio2 ratio <300 in absence of cyanotic heart disease or pre-existing lung diseaseOR
Paco2 >65 torr or 20 mm Hg over baseline Paco2
OR
Proven need for >50% Fio2 to maintain saturation ≥92%OR
Need for nonelective invasive or noninvasive mechanical ventilation

Neurologic
GCS score ≤11OR
Acute change in mental status with a decrease in GCS score ≥3 points from abnormal baseline

Hematologic
Platelet count <80,000/mm3 or a decline of 50% in the platelet count from the highest value recorded over the last 3 days (for patients with chronic hematologic or oncologic disorders)OR
INR >2

Renal
Serum creatinine ≥2? upper limit of normal for age or 2-fold increase in baseline creatinine value

Hepatic
Total bilirubin ≥4 mg/dL (not applicable for newborn)
Alanine transaminase level 2? upper limit of normal for age

Systemic inflammatory response syndrome
The presence of at least two of the following four criteria, one of which must be abnormal temperature or leukocyte count:
- Core temperature of > 38.50 C or < 360 c
- Tachycardia
- High respiratory rate
- Lukocyte count elevated or depressed for age

Infection
Suspected or proven infection or a clinical syndrome associated with high probability of infection

Sepsis
SIRS plus a suspected or proven infection

Severe sepsis
Sepsis plus one of the following : cardiovascular organ dysfunction
OR
acute respiratory distress syndrome
OR
two or more other organ dysfunctions
Septic shock
Sepsis and cardiovascular organ dysfunction

Clinical Manifestations
depends in part on the underlying etiology
If unrecognized and untreated, all forms of shock follow a common and untoward progression of clinical signs and irreversible shock and death

Fever

Tachycardia
Each 10 Core temperature rises HR 12 beat/min

Tachypnea
Each 10 Core temperature rises RR 5-10 /min
Poor Perfusion
Mottled or cool extremities
Mental status change
Decreased urine output
Capillary filling > 3 sec
Decreased peripheral (dorsalis pedis or radial )pulses compared to central pulses
Increase in central to peripheral temperature gradient(gap>3 c)

Diagnosis
Shock is diagnosed clinically on the basis of a thorough history and physical exam

Laboratory Findings
Leukocytosis
Identifying an infectious etiology(cultures,analyses of body fluids, imaging,…)
Organ dysfunction detection(renal,hepatic,…)
hematologic abnormalities and electrolyte disturbances(Plt,PT,PTT,FSP,Anemia,↑PMN,↓ Ca, ↓or↑BS,↓Alb,metabolic acidosis,…
Svo2 & serum lactate (marker for the adequacy of oxygen delivery and the effectiveness of therapeutic interventions)

SvO2 or Svco2 & Serum lactate
marker for the adequacy of oxygen delivery and the effectiveness of therapeutic interventions

Oxygen delivery normally exceeds oxygen consumption by threefold. The oxygen extraction ratio is approximately 25%, thus producing a normal of 75-80%. A falling value, as measured by co-oximetry, reflects an increasing oxygen extraction ratio and documents a decrease in oxygen delivery relative to consumption.
Serum lactate measurements

Management
Early recognition and prompt intervention

for each unrecognizedand untreated hour of shock, the mortality rate is estimated to increase twofold.


Fluid administration
isotonic crystalloid solution(NS)
increments of 20 mL/kg
Max 60-80 mL/kg
sometimes require as much as 200 mL/kg

Within the bolus fluid dose
Rales
Gallop rhythm
Hepatomegaly
Increased work of breathing
Increased oxygen need,

Titration of Fluid resuscitation
Untill normalization of:
heart rate (according to age-based heart rates)
urine output (to 1 mL/kg/hr)
capillary refill time (to <2 sec)
mental status

Antibiotics
After cultures provided this does not significantly delay antibiotic administration (2 or more B/C )
Within 1 hour of recognition of sepsis
Broad spectrum
Cover likely organism
High infected tissues penetration
Hospital acquired: know local resistance pattern
3rd-generation cephalosporin or ….

When intubate? Early sepsis:
Respiratory alkalosis from central mediated hyperventilation
Late sepsis:
Hypoxemia
Metabolic acidosis
The decision to intubate and ventilate is based on clinical assessment of:
Increased work of breathing
Hypoventilation
Decreased level of consciousness
Patient in fluid refractory shock should be intubated and ventilated without delay

If no clinical improvement(fluid refractory)
Add vasoactive infusions :
Low dose dopamine (2 to 5 mcg/kg/min) for children who are normotensive
Beta adrenergic dose of dopamine (5 to 10 mcg/kg/min) or norepinephrine for those who are hypotensive and vasodilated
Epinephrine for children who are hypotensive and vasoconstricted despite maximum beta adrenergic doses of dopamine and/or norepinephrine

If catecholamine resistant
after sample for baseline cortisol levels
Patients at risk for adrenal insufficiency:
congenial adrenal hypoplasia
abnormalities of the hypothalamic-pituitary axis
recent therapy with corticosteroids (asthma, rheumatic dis. , malignancies,& IBD
Septic shock with Purpura fulminant

Corticosteroid dose
Recommended dose is a wide range from 2mg/kg /day for stress coverage to 50 mg/kg /day titrated to reversal of shock
Dexamethasone (0.1 mg/kg, maximum 10 mg) may be given as the initial steroid dose in the emergency department since (unlike hydrocortisone) it will not interfere with subsequent testing of adrenal function
Therapeutic goal in emergency room: Capillary refill ≤ 2 secs,
Normal pulses with no differential between the quality of peripheral and central pulses,
Warm extremities,
Urine output >1 mL/kg/h
Normal mental status
Normal blood pressure for age
Normal glucose concentration
Normal ionized calcium concentration.

Transfer to PICU


Monitor CVP in PICU
Attain normal MAP-CVP & SvO2> 70%

What is MAP-CVP CO= (MAP – CVP) / SVR
Q= dp/R,
(Q= Blood flow, dp= perfusion pressure, R=resistance)
MAP – CVP = PP
(PP= Perfusion pressure)
For example: Renal perfusion pressure
Mean renal arterial pressure – mean renal venous pressure
Renal vascular resistant
One goal of shock treatment is to maintain perfusion pressure above the critical point below which blood flow can not effectively maintain in individual organ.

The value of CVP monitoring is doubted. CVP has a very poor correlation with intravascular volume
CVP is influenced not only by intravascular volume and venous return, but by
Venous tone (hypotensive patient can exhibit normal BP due to vasoconstriction)
Intrathoracic pressure
Rt heart function
Myocardial compliance
However low CVP can guide fluid resuscitation
CVP = 10-12 cm H2O
Perfusion pressure (MAP – CVP) > 65 mmHg

• Cold shock with normal blood pressure (High SVR)
• Cold shock with low blood pressure (High SVR)
• Warm shock with low blood pressure (Low SVR)

Cold shock with normal blood pressure (High SVR)
1. Titrate fluid and epinephrine
ScvO2 > 70%, Hb> 10 g/dL
2. If ScvO2 < 70%
Add vasodilator with volume loading
(milrinone, Sodium Nitroprusside)

Cold shock with low blood pressure (High SVR)
1. Titrate fluid and epinephrine
ScvO2 > 70%, Hb> 10 g/dL
2. If still hypotensive consider norepinephrine
3. If ScvO2 still < 70% consider
Dobutamine, milrinone

Warm shock with low blood pressure(Low SVR)
1. Titrate fluid and norepinephrine
ScvO2 > 70% , Hb > 10 gr/dL
2. If still hypotensive add vasopressin
3. If ScvO2 still < 70% consider low dose epinephrine
↓
shock not reversed

Shock not reversed? Persistant catecholamine resistant shock
Rout and correct pericardial effusion pneumothorax, intra-abdominal pressure > 12 mmHg
Goal C.I > 3.3 and < 6.0 L/min/m2
↓
Shock not reversed
↓
Refractory shock : ECMO
successful treatment of septic shock cannot begin in the ICU for patients whopresent to the ED in shock; it must begin at the time of triage in the ED


دهیدراتاسیون
ب احتیاج گذارذ هایغ بز ػال ک ػین هی هاخ بیوارای با گاا دفغ هثل دارین را طبیؼی غیز صرت ب رفت دطت اس هایغ کوبد خبزاىا خزیشی یا اطتفزاؽ اطال در هایغ سیاد
ن را آبی کن یا دیذراتاطیى بایذ گذارذ هایغ بز ػال هارد ایي در هحللای با خراکی طزیك اس تاذ هی آبی کن ایي .کین خبزاى
خراکی تغذی تحول ػذم صرت در ریذی یا ORS هثل خراکی الکتزلیتی.ػد ادام

کدک ػیار اطت فمط هختصزا تؼگی دارد :دیذراتاطیى خفیف.،ترگر پطتی طبیؼی بد گدافتادگی چؼوا ذارد
ػذیذا بی لزار اطت لغ ػذیذ ب هایؼات :دیذراتاطیى هتطط.دارد،ترگرپطتی کاغ یافت چؼواگد افتاد اطت
بی حال اطت، تاائی ػیذى ذارد، ترگر : دیذراتاطیى ػذیذ .پطتی اظحا کاغ یافت چؼوا خیلی گد افتاد اطت

در صرتی ک کدک بز اطاص طبم بذی در دطت ػذیذ طبم بذی ػد بایذ طزیؼا هایغ درهای را با طزػت سیادتز خت خلگیزی اس ػارض
ػزع ػد با تخ ب ایک در ایي هارد بایذ در سهاى کن هیشاى سیادی هایغ ب فزد بذین بایذ هایغ اتخابی ( حذد یک طم حدن خى 20cc/kgحذالل )
اس ظز اطوالرتی طذین شدیک ب خى باػذ در ایي هارد ط ع طزم 30تا 15ریگزریگزالکتات ز -را اطتفاد هی کین ػاهل زهال طالیي
دلیم تا بز طزف ػذى حالت دیذرتاطیى ػذیذ یا ػک یا ایک تا ط بار ایي کار را ادام دین اداه هی دین

در هاردی ک بیوار در ػک وی باػذ یا با درهاى الی اس ػک خارج دطت ایپز اتزهیک ایپ 3ػذ اطت بز اطاص ع طذین بیواراى ب
اتزهیک ایش اتزهیک تمظین بذی هی ػد

دهیدراتاسیون ایزو ناترمیک
کذ دریافت طاػت 24بایذ طی در ایي حالت هیشاى هایغ کلی ک کدک 1/2طاػت ال 8ک در . دیذراتاطیى اطت+ ػاهل هایغ گذارذdeficit+1/3 maintance را هی دین
اگز دیذراتا طیى اس لبل هؼلم ػذ هیشاى کلی هایغ هحاطب ػذ طاػت 8هایؼی را ک ب صرت طزیغ بزای درهاى ػک داد این اس هایغ
. ال کن هی کین
Dw5%1/2 normal salineایي ع دیذراتاطیى ب صرت تیپیک اس هایغدر
3/1- 3/2گاا هی تاین خت طلت کار اس طزم.اطتفاد هی کینوزا پتاطین اطتفاد کین

دهیدراتاسیون هایپو ناترمیک
ب باالداػت باػذ ب ویي ػلت meq/lit75حتوا هایغ تدیش ػذ طذینNormal Salin 1/2حذالل اس طزم Dw5 اطتفاد کین ک حدن کلی
اطت Maintance+Deficitػاهل


دهیدراتاسیون هیپرناتومیک
ب تخ با سیزا اطت هؼکل کدکاى ایي در دیذراتاطیى حذص هیشاى ػلت ویي ب باالطت ایا در خى اطوالریت ایدا در خى باال طذین ب دارد ػزق داخل ب رفتي ب توایل طللی داخل بافتی هیاى هایغ
بیوار یابذ هی کاغ دیزتز ػزلی داخل حدن کدکاى ایي در ػلت ویي.دذ هی ؼاى را ػذیذ دیذرتاطیى ػالئن دیزتز

دهیدراتاسیون هیپرناتومیک
کؼیذ باال اطوالرتی خاطز ب هغشی ػالئن ایداد احتوال کدکاى ایي در اتفاق هغشی طللای بیؼتز دیذراتاطیى هغشی طلی داخل هایغ ػذىاذ دطت ایي اس هغشی طکت خزیشی تزهبس، ػاهل افتذ هی


دهیدراتاسیون هیپرناتومیک
در طی درهاى ایي کدکاى ػال بز کتزل دیذراتاطیى بایذ طزػت اصالذ باػذ چى mEq/kg/h5 /0در رس با طزیؼتز اس mEq/liL 12طذین طزیؼتز اس
فزد دچار ادم هغشی هی ػد ن ادم هغشی ن ػارض هغشی دیگز هی تاذ باػث تؼح طکل ایداد کذ

دهیدراتاسیون هیپرناتومیک
بزابز هایغ 1/25 1/5ایي ػولیات ویؼ هایغ کل ب دطت آهذ ػاهل طاػت کدک هی ػد دیگز یاسی ب 24گذارذ کل هایغ هرد یاس
.تؼییي هایغ گذارذ دیذراتاطیى یظت

NSبتز اس طزم kg20-10اس ظز هیشاى طذین در کدکاى کوتز اس . 1/4DW5% 6تا 4هیلی اکی االى پتاطین ػزع ػد طپض ز 20وزا
mEq/kg/h 0/5طاػت طذین چک ػد در صرتی هیشاى طذین طزیؼتز اس هی کین یا حدن NS 1/2DW5%پائیي افتاد یا هیشاى طذین هایغ را تبذیل ب
.هایغ را کظز هی کین ک ػول ال بتز اطت
پائیي افتاد یا طذین هحلل را mEq/kg/h 0/5حال اگز هیشاى طذین کوتز اس افشایغ هی دین% 20-%10کوتز هی کین یا حدن هایغ را

در ایي هارد اگز بیوار دبار ػالئن دیذراتاطیى ػذیذ را ؼاى داد دیگز اس هایغ زهال cc/kg20طزػت هایغ را سیاد وی کین بلک دبار یک دس
طالیي اظاف هی دین


lower respiratory tract infection
Bronchitis
Bronchiolitis
Pneumonia
Any combination of these

Pneumonitis




Risk factors
Gastroesophageal reflux
Neurologic impairment (aspiration)
Immunocompromised states
Anatomic abnormalities of R. tract
Residence in residential care facilities for handicapped children
Hospitalization,(ICU) or requiring invasive procedures.

CLINICAL MANIFESTATIONS
MOSTLY AGE DEPENDENT
Neonate
fever(may be with subtle sym & sign)
Older infants and children
Fever, chills, tachypnea, cough, malaise, pleuritic chest pain, retractions, apprehension,

Viral pneumonias are associated more often with cough, wheezing, or stridor & fever is less prominent than with bacterial pneumonia
Bacterial pneumonias typically are associated with higher fever, chills, cough, dyspnea, and auscultatory findings of lung consolidation
CLINICAL MANIFESTATIONS
flaring of the alae of the nose, intercostal and subcostal retractions, and grunting
If significant pneumonias : localized crackles and decreased breath sounds
Pleural effusion may cause dullness to percussion
CLINICAL MANIFESTATIONS

LABORATORY AND IMAGING STUDIES
Sputum study
CBC(white blood cell) Viral Or Bacterial
B/C
Rapid viral antigen detection of upper respiratory secretions
Cold agglutinins, may be confirmed by MycoplasmaIgM or more specifically (PCR)

SPECIAL PATIENTS
Patients who are ill and hospitalized
Immunocompromised patients
Patients with recurrent pneumonia
Patients with pneumonia unresponsive to empirical therapy

Bronchoscopy with bronchoalveolar lavage and brush mucosal biopsy
Needle aspiration of the lung
Open lung biopsy

Effusion or empyema, performing a thoracentesis to obtain pleural fluid can be diagnostic and therapeutic

Acute lobar pneumonia of the lingula in a 6-year-old child with high fever, cough, and chest pain

Diffuse viral bronchopneumonia in a 12-year-old boy with cough, fever, and wheezing. Frontal chest radiograph shows bilateral, perihilar, peribronchial thickening and shaggy infiltrate. Focal airspace disease representing consolidation or atelectasis is present in the medial portion of the right upper lobe


Factors Suggesting Need for Hospitalization of Children with Pneumonia

fever, anorexia , poor feeding, headache, symptoms of upper respiratory tract infection, myalgias, arthralgias, tachycardia, hypotension, and various cutaneous signs, such as petechiae, purpura, or an erythematous macular rash. Meningeal irritation is manifested as nuchal rigidity, back pain, Kernig sign , and Brudzinski sign . Increased ICP is suggested by headache, emesis, bulging fontanel or diastasis (widening) of the sutures, oculomotor(anisocoria, ptosis) or abducens nerve paralysis, hypertension with bradycardia, apnea or hyperventilation, decorticate or decerebrate posturing, stupor, coma, or signs of herniation. focal neurologic signs.
Clinical Manifestations

Papilledema is uncommon in uncomplicated meningitis and should suggest a more chronic process, such as the presence of an intracranial abscess, subdural empyema, or occlusion of a duralvenous sinus. Focal neurologic signs usually are due to vascular occlusion. Cranial neuropathies of the ocular, oculomotor, abducens, facial, and auditory nerves may also be due to focal inflammation. Overall, about

Seizures (focal or generalized) due to cerebritis, infarction, or electrolyte disturbances .
Alterations of mental status are common among patients with meningitis and may be due to increased ICP, cerebritis, or hypotension; manifestations include irritability, lethargy, stupor, obtundation, and coma Additional manifestations of meningitis include photophobia and tache c?r?brale, which is elicited by stroking the skin with a blunt object and observing a raised red streak within 30-60 sec.
![Pregnancy Induced Hypertension - معاونت درمانta.mui.ac.ir/sites/ta.mui.ac.ir/files/PIH [Compatibility Mode].pdf · Pregnancy Induced Hypertension ... • Regional anesthesia](https://static.fdocuments.in/doc/165x107/5d61ee1788c993e8748b4afb/pregnancy-induced-hypertension-tamuiacirsitestamuiacirfilespih.jpg)


![Emergency Procedures [DOCUMENT TITLE] Manualhr.csi.edu/handbook/Emergency.pdf · 2019-06-05 · safe to do so. At all times, suspected gas leaks or suspicious odors should be reported](https://static.fdocuments.in/doc/165x107/5e912e857be3fa78fc4a93ab/emergency-procedures-document-title-2019-06-05-safe-to-do-so-at-all-times.jpg)